
CD24 Gene Expression as a Risk Factor for Non-Alcoholic Fatty Liver Disease
Abstract
:1. Introduction
2. Subjects and Methods
2.1. Liver Stiffness Measurement (LSM) and Controlled Attenuation Parameter (CAP)
2.2. Sample Collection
2.3. CD24 Gene Expression by Quantitative Real Time-PCR (qRT-PCR):
2.4. Reverse Transcription for cDNA Synthesis and Quantitative Real-Time PCR (RTqPCR)
| Primer | Primer Sequence |
| CD24 Forward primer | 5′-ACC CAC GCA GAT TTA TTC CA-3′ |
| CD24 Reverse primer | 5′-ACC ACG AAG AGA CTG GCT GT-3′ |
| β-actin Forward primer | 5′-TGA GCG CGG CTA CAG CTT-3′ |
| β-actin Reverse primer | 5′-TCC TTA ATG TCA CGC ACG ATT T-3′ |
2.5. Statistical Analysis
3. Results
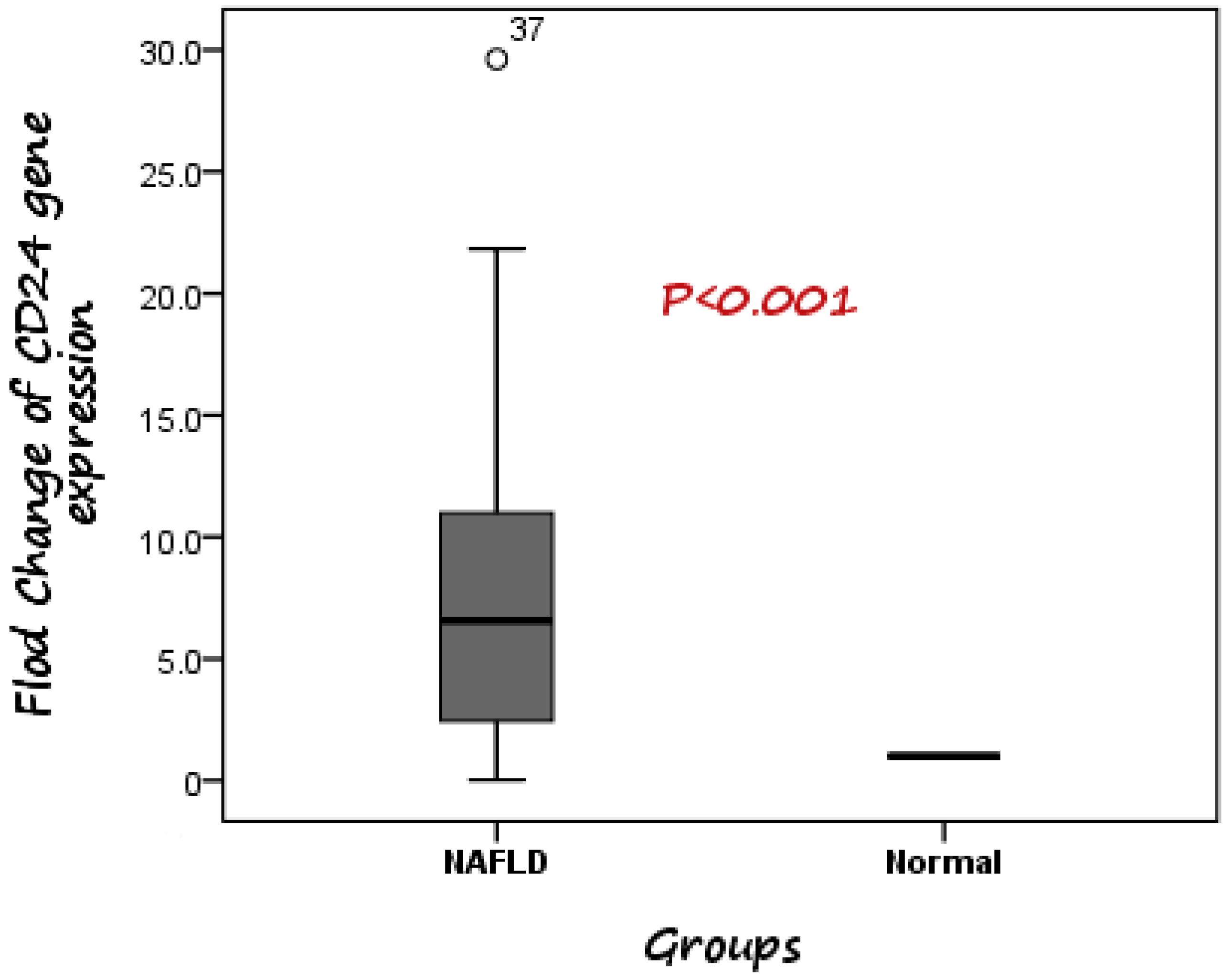
3.1. Evaluation of the Diagnostic Accuracy of CD24 Gene Expression for Distinguishing Patients with NAFLD from Healthy Controls
3.2. Correlation between Different Non-Invasive Fibrosis Markers and CD24 Gene Expression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sherif, Z.A. The rise in the prevalence of nonalcoholic fatty liver disease and hepatocellular carcinoma. In Nonalcoholic Fatty Liver Disease—An Update; Intechopen: Lodon, UK, 2019. [Google Scholar]
- Hirose, S.; Matsumoto, K.; Tatemichi, M.; Tsuruya, K.; Anzai, K.; Arase, Y.; Shiraishi, K.; Suzuki, M.; Ieda, S.; Kagawa, T. Nineteen-year prognosis in japanese patients with biopsy-proven nonalcoholic fatty liver disease: Lean versus overweight patients. PLoS ONE 2020, 15, e0241770. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Marchesini, G.; Pinto-Cortez, H.; Petta, S. Epidemiology of nonalcoholic fatty liver disease and nonalcoholic steatohepatitis: Implications for liver transplantation. Transplantation 2019, 103, 22–27. [Google Scholar] [CrossRef]
- Albhaisi, S.; Sanyal, A.J. Gene-environmental interactions as metabolic drivers of nonalcoholic steatohepatitis. Front. Endocrinol. 2021, 12, 498. [Google Scholar] [CrossRef]
- Seko, Y.; Yamaguchi, K.; Itoh, Y. The genetic backgrounds in nonalcoholic fatty liver disease. Clin. J. Gastroenterol. 2018, 11, 97–102. [Google Scholar] [CrossRef] [Green Version]
- Lisiansky, V.; Kraus, S.; Naumov, I.; Kazanov, D.; Nabiochtchikov, I.; Toledano, O.; Leshno, M.; Avivi, D.; Dotan, I.; Arber, N.; et al. Role of cd24 polymorphisms in the susceptibility to inflammatory bowel disease. Int. J. Biol. Mrk. 2014, 29, 5000072. [Google Scholar]
- Smith, N.C.; Fairbridge, N.A.; Pallegar, N.K.; Christian, S.L. Dynamic upregulation of cd24 in pre-adipocytes promotes adipogenesis. Adipocyte 2015, 4, 89–100. [Google Scholar] [CrossRef] [Green Version]
- Huang, S.; Sun, C.; Hou, Y.; Tang, Y.; Zhu, Z.; Zhang, Z.; Zhang, Y.; Wang, L.; Zhao, Q.; Chen, M.G.; et al. A comprehensive bioinformatics analysis on multiple gene expression omnibus datasets of nonalcoholic fatty liver disease and nonalcoholic steatohepatitis. Sci. Rep. 2018, 8, 7630. [Google Scholar] [CrossRef] [PubMed]
- Feng, J.; Wei, T.; Cui, X.; Wei, R.; Hong, T. Identification of key genes and pathways in mild and severe nonalcoholic fatty liver disease by integrative analysis. Chronic Dis. Transl. Med. 2021, 7, 276–286. [Google Scholar] [CrossRef] [PubMed]
- Angulo, P.; Hui, J.M.; Marchesini, G.; Bugianesi, E.; George, J.; Farrell, G.C.; Enders, F.; Saksena, S.; Burt, A.D.; Bida, J.P.; et al. The nafld fibrosis score: A noninvasive system that identifies liver fibrosis in patients with nafld. Hepatology 2007, 45, 846–854. [Google Scholar] [CrossRef]
- Calès, P.; Lainé, F.; Boursier, J.; Deugnier, Y.; Moal, V.; Oberti, F.; Hunault, G.; Rousselet, M.C.; Hubert, I.; Laafi, J.; et al. Comparison of blood tests for liver fibrosis specific or not to nafld. J. Hepatol. 2009, 50, 165–173. [Google Scholar] [CrossRef] [Green Version]
- Newsome, P.N.; Sasso, M.; Deeks, J.J.; Paredes, A.; Boursier, J.; Chan, W.-K.; Yilmaz, Y.; Czernichow, S.; Zheng, M.-H.; Wong, V.W.-S. Fibroscan-ast (fast) score for the non-invasive identification of patients with non-alcoholic steatohepatitis with significant activity and fibrosis: A prospective derivation and global validation study. Lancet Gastroenterol. Hepatol. 2020, 5, 362–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mansour, A.M.; Bayoumy, E.M.; ElGhandour, A.M.; El-Talkawy, M.D.; Badr, S.M.; Ahmed, A.E.-M. Assessment of hepatic fibrosis and steatosis by vibration-controlled transient elastography and controlled attenuation parameter versus non-invasive assessment scores in patients with non-alcoholic fatty liver disease. Egypt. Liver J. 2020, 10, 1–10. [Google Scholar] [CrossRef]
- Zeng, F.; Zhang, Y.; Han, X.; Zeng, M.; Gao, Y.; Weng, J. Predicting non-alcoholic fatty liver disease progression and immune deregulations by specific gene expression patterns. Front. Immunol. 2020, 11, 609900. [Google Scholar] [CrossRef]
- Brea, A.; Puzo, J. Non-alcoholic fatty liver disease and cardiovascular risk. Int. J. Cardiol. 2013, 167, 1109–1117. [Google Scholar] [CrossRef]
- Ciardullo, S.; Oltolini, A.; Cannistraci, R.; Muraca, E.; Perseghin, G. Sex-related association of nonalcoholic fatty liver disease and liver fibrosis with body fat distribution in the general us population. Am. J. Clin. Nutr. 2022, 115, 1528–1534. [Google Scholar] [CrossRef] [PubMed]
- Lonardo, A.; Nascimbeni, F.; Ballestri, S.; Fairweather, D.; Win, S.; Than, T.A.; Abdelmalek, M.F.; Suzuki, A. Sex differences in nonalcoholic fatty liver disease: State of the art and identification of research gaps. Hepatology 2019, 70, 1457–1469. [Google Scholar] [CrossRef] [PubMed]
- Hossain, N.; Afendy, A.; Stepanova, M.; Nader, F.; Srishord, M.; Rafiq, N.; Goodman, Z.; Younossi, Z. Independent predictors of fibrosis in patients with nonalcoholic fatty liver disease. Clin. Gastroenterol. Hepatol. 2009, 7, 1224–1229. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease-meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [Green Version]
- Abouzid, M.R.; Ali, K.; Elkhawas, I.; Elshafei, S.M. An overview of diabetes mellitus in Egypt and the significance of integrating preventive cardiology in diabetes management. Cureus 2022, 14, e27066. [Google Scholar] [CrossRef]
- Lonardo, A.; Bellentani, S.; Argo, C.K.; Ballestri, S.; Byrne, C.D.; Caldwell, S.H.; Cortez-Pinto, H.; Grieco, A.; Machado, M.V.; Miele, L.; et al. Epidemiological modifiers of non-alcoholic fatty liver disease: Focus on high-risk groups. Dig. Liver Dis. 2015, 47, 997–1006. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.H.; Cho, Y.; Lee, B.W.; Park, C.Y.; Lee, D.H.; Cha, B.S.; Rhee, E.J. Nonalcoholic fatty liver disease in diabetes. Part i: Epidemiology and diagnosis. Diabetes Metab. J. 2019, 43, 31–45. [Google Scholar] [CrossRef]
- Tomah, S.; Hamdy, O.; Abuelmagd, M.M.; Hassan, A.H.; Alkhouri, N.; Al-Badri, M.R.; Gardner, H.; Eldib, A.H.; Eid, E.A. Prevalence of and risk factors for non-alcoholic fatty liver disease (nafld) and fibrosis among young adults in Egypt. BMJ Open Gastroenterol. 2021, 8, e000780. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.-R.; Hsu, H.-C. Cloning and expression of CD24 gene in human hepatocellular carcinoma: A potential early tumor marker gene correlates with p53 mutation and tumor differentiation. Cancer Res. 1995, 55, 4717. [Google Scholar] [PubMed]
- Jackson, D.; Waibel, R.; Weber, E.; Bell, J.; Stahel, R.A. Cd24, a signal-transducing molecule expressed on human b cells, is a major surface antigen on small cell lung carcinomas. Cancer Res. 1992, 52, 5264–5270. [Google Scholar]
- Raife, T.J.; Lager, D.J.; Kemp, J.D.; Dick, F.R. Expression of cd24 (ba-1) predicts monocytic lineage in acute myeloid leukemia. Am. J. Clin. Pathol. 1994, 101, 296–299. [Google Scholar] [CrossRef]
- Senner, V.; Sturm, A.; Baur, I.; Schrell, U.H.; Distel, L.; Paulus, W. Cd24 promotes invasion of glioma cells in vivo. J. Neuropathol. Exp. Neurol. 1999, 58, 795–802. [Google Scholar] [CrossRef] [Green Version]
- Kristiansen, G.; Denkert, C.; Schlüns, K.; Dahl, E.; Pilarsky, C.; Hauptmann, S. Cd24 is expressed in ovarian cancer and is a new independent prognostic marker of patient survival. Am. J. Pathol. 2002, 161, 1215–1221. [Google Scholar] [CrossRef] [Green Version]
- Jing, X.; Cui, X.; Liang, H.; Hao, C.; Yang, Z.; Li, X.; Yang, X.; Han, C. Cd24 is a potential biomarker for prognosis in human breast carcinoma. Cell. Physiol. Biochem. 2018, 48, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Rodeheffer, M.S.; Birsoy, K.; Friedman, J.M. Identification of white adipocyte progenitor cells in vivo. Cell 2008, 135, 240–249. [Google Scholar] [CrossRef] [Green Version]
- Bai, X.F.; Li, O.; Zhou, Q.; Zhang, H.; Joshi, P.S.; Zheng, X.; Liu, Y.; Wang, Y.; Zheng, P.; Liu, Y. Cd24 controls expansion and persistence of autoreactive t cells in the central nervous system during experimental autoimmune encephalomyelitis. J. Exp. Med. 2004, 200, 447–458. [Google Scholar] [CrossRef] [Green Version]
- Huby, T.; Gautier, E.L. Immune cell-mediated features of non-alcoholic steatohepatitis. Nat. Rev. Immunol. 2021, 5, 1–15. [Google Scholar] [CrossRef]
- Chatterjee, A.; Basu, A.; Das, K. Hepatic transcriptome signature correlated with homa-ir explains early nonalcoholic fatty liver disease pathogenesis. Ann. Hepatol. 2020, 19, 472–481. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Wang, R.; Xiong, S.; Wang, X.; Zhao, Z.; Bai, S.; Cheng, B. Cancer-associated fibroblasts promote the stemness of cd24(þ) liver cells via paracrine signaling. J. Mol. Med. 2019, 97, 243–255. [Google Scholar] [CrossRef] [PubMed]
- Hafez, M.M.; Abdel-Hafez, L.J.M.; Jamil, L.; Ibrahim, S.M. Association between cluster of differentiation 24 (cd24) polymorphism, talin-1 gene expression and hepatocellular carcinoma prevalence in Egyptian population. Arch. Med. Sci. 2021. Available online: https://repository.msa.edu.eg/xmlui/handle/123456789/123454701 (accessed on 13 August 2021). [CrossRef]
- Robert, F.; Pelletier, J. Exploring the impact of single-nucleotide polymorphisms on translation. Front. Genet. 2018, 9, 507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kristiansen, G.; Machado, E.; Bretz, N.; Rupp, C.; Winzer, K.J.; König, A.K.; Moldenhauer, G.; Marmé, F.; Costa, J.; Altevogt, P. Molecular and clinical dissection of cd24 antibody specificity by a comprehensive comparative analysis. Lab. Investig. 2010, 90, 1102–1116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shapira, S.; Kazanov, D.; Dankner, R.; Fishman, S.; Stern, N.; Arber, N. High expression level of pparγ in cd24 knockout mice and gender-specific metabolic changes: A model of insulin-sensitive obesity. J. Pers. Med. 2021, 11, 50. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | NAFLD Group (N = 40) | Control Group (N = 40) | p-Value | |
|---|---|---|---|---|
| Groups | ||||
| Age (Yrs.) | 42.18 ± 11.14 | 29.65 ± 6.63 | <0.001 ** | |
| Gender a | 0.061 | |||
| Male/Female | 10/30 | 18/22 | ||
| Percentage of Male | (25%) | (45%) | ||
| Hypertension a | 0.006 ** | |||
| Absent | 33 (82.5%) | 40 (100%) | ||
| Present | 7 (17.5%) | 0 (0%) | ||
| Diabetes a | <0.001 ** | |||
| Absent | 20 (50%) | 40 (100%) | ||
| Oral hypoglycemic | 9 (22.5%) | 0 (0%) | ||
| on insulin | 11 (27.5%) | 0 (0%) | ||
| Family history of diabetes a | 1.000 | |||
| No | 31 (77.5%) | 31 (77.5%) | ||
| Yes | 9 (22.5%) | 9 (22.5%) | ||
| Family history of liver diseases a | 0.805 | |||
| No | 28 (70%) | 29 (72.5%) | ||
| Yes | 12 (30%) | 11 (27.5%) | ||
| BMI (kg/m2) | 32.42 ± 3.59 | 23.66 ± 1.3 | <0.001 ** | |
| Waist circumference (cm) | 117.9 ± 9.4 | 74.3 ± 6.8 | <0.001 ** | |
| Mid-arm circumference (cm) | 31.8 ± 4.3 | 25.5 ± 1.5 | <0.001 ** | |
| Ultrasound finding a | ||||
| Enlarged liver size | 25 (62.5%) | 0 (0%) | <0.001 ** | |
| Laboratory variables | ||||
| Fasting blood glucose (mg/dL) | 122.6 ± 40.97 | 96.03 ± 7.77 | <0.001 ** | |
| HB (g/dL) | 11.56 ± 1.4 | 12.81 ± 1.06 | <0.001 ** | |
| Platelets count (103/µL) | 236 ± 72.78 | 260.63 ± 56.79 | 0.096 | |
| Total leucocytic count (103/µL) | 6.79 ± 1.91 | 7.24 ± 1.7 | 0.273 | |
| ALT (U/L) | 47.9 ± 18.3 | 30.6± 4.9 | <0.001 ** | |
| AST (U/L) | 33.55 ± 14.9 | 23.6 ± 4.6 | <0.001 ** | |
| Total bilirubin (mg/dL) | 0.76 ± 0.24 | 0.68 ± 0.2 | 0.132 | |
| ALP (U/L) | 155.7± 37.5 | 115.02± 15.2 | <0.001 ** | |
| GGT (U/L) | 91.1± 64.2 | 34.5± 9.2 | <0.001 ** | |
| Total Protein (g/dL) | 8.1± 0.2 | 7.9± 0.24 | 0.007 ** | |
| INR | 1.05 ± 0.1 | 1.0 ± 0.0 | 0.003 ** | |
| Serum Albumin (g/dL) | 3.8 ± 0.38 | 3.8 ± 0.3 | 0.939 | |
| Cholesterol (mg/dL) | 150.88 ± 32.4 | 101.65 ± 19.76 | <0.001 ** | |
| Triglycerides (mg/dL) | 168.5 ± 44.15 | 143.9 ± 29.7 | 0.005 ** | |
| LDL (mg/dL) | 133.7 ± 34.6 | 104.02 ± 16.1 | <0.001 ** | |
| HDL (mg/dL) | 48.4 ± 15.5 | 55 ± 12.7 | 0.04 * | |
| Variable | NAFLD Group (N = 40) | p-Value | Control Group (N = 40) | p-Value | |||
|---|---|---|---|---|---|---|---|
| Groups | Male N = 10 | Female N = 30 | Male N = 18 | Female N = 22 | |||
| Age (Yrs.) | 44.8 ± 9.1 | 41.3 ± 11.7 | 0.396 | 28.5 ± 4.7 | 30.59 ± 7.8 | 0.305 | |
| Hypertension | 0.338 | - | |||||
| Absent | 7 (70%) | 26 (86.7%) | 18 (100%) | 22 (100%) | |||
| Present | 3 (30%) | 4 (13.3%) | 0 (0%) | 0 (0%) | |||
| Diabetes | 0.322 | - | |||||
| Absent | 7 (70%) | 13 (43.3%) | 18 (100%) | 22 (100%) | |||
| Oral hypoglycemic | 1 (10%) | 8 (26.7%) | 0 (0%) | 0 (0%) | |||
| on insulin | 2 (20%) | 9 (30%) | 0 (0%) | 0 (0%) | |||
| Family history of diabetes | 0.827 | 0.970 | |||||
| No | 8 (80%) | 23 (76.7%) | 14 (77.8%) | 17 (77.3%) | |||
| Yes | 2 (20%) | 7 (23.3%) | 4 (22.2%) | 5 (22.7%) | |||
| Family history of liver diseases | 0.231 | 0.173 | |||||
| No | 9 (90%) | 19 (63.3%) | 11 (61.1%) | 18 (81.8%) | |||
| Yes | 1 (10%) | 11 (36.7%) | 7 (38.9%) | 4 (18.2%) | |||
| BMI (kg/m2) | 32.51 ± 3.1 | 32.39 ± 3.8 | 0.929 | 23.95 ± 1.1 | 23.4 ± 1.33 | 0.183 | |
| Laboratory variables | |||||||
| Fasting blood glucose (mg/dL) | 108.7 ± 38.9 | 127.23 ± 41.2 | 0.220 | 93.78 ± 6.3 | 97.86 ± 8.5 | 0.098 | |
| HB (g/dL) | 12.72 ± 1.03 | 11.17 ± 1.3 | 0.001 ** | 12.9 ± 0.99 | 12.7 ± 1.1 | 0.572 | |
| Platelets count (103/µL) | 252.3 ± 73.3 | 230.57± 73.03 | 0.421 | 270.9 ± 64.8 | 252.2 ± 49.3 | 0.305 | |
| Total leucocytic count (103/µL) | 7.18 ± 1.69 | 7.07 ± 1.9 | 0.875 | 6.7 ± 1.2 | 7.3 ± 1.83 | 0.253 | |
| ALT (U/L) | 60.7 ± 18.6 | 43.7 ± 16.4 | 0.009 * | 29.9± 5.1 | 31 ± 4.8 | 0.489 | |
| AST (U/L) | 44.7 ± 18.9 | 29.8 ± 11.4 | 0.038 * | 22.8 ± 3.9 | 24.3 ± 5 | 0.312 | |
| Total bilirubin (mg/dL) | 0.82 ± 0.25 | 0.74 ± 0.24 | 0.331 | 0.69 ± 0.2 | 0.66 ± 0.2 | 0.605 | |
| ALP (U/L) | 156.4± 40.4 | 155.5 ± 37.2 | 0.949 | 117.3± 15 | 113.1 ± 15.4 | 0.390 | |
| GGT (U/L) | 111.1± 61.9 | 84.4 ± 64.5 | 0.259 | 35.6± 10.3 | 33.5 ± 8.3 | 0.488 | |
| Total Protein (g/dL) | 8.1± 0.34 | 8.04± 0.23 | 0.574 | 7.8± 0.24 | 7.9 ± 0.24 | 0.277 | |
| Serum Albumin (g/dL) | 3.8 ± 0.37 | 3.8 ± 0.39 | 0.962 | 3.8 ± 0.34 | 3.8 ± 0.26 | 0.489 | |
| Cholesterol (mg/dL) | 158 ± 22.4 | 148.5 ± 35.15 | 0.429 | 105.1 ± 22.1 | 98.8 ± 17.6 | 0.323 | |
| Triglycerides (mg/dL) | 146.3 ± 52.4 | 175.83 ± 39.3 | 0.066 | 152.2 ± 25.8 | 137.14 ± 31.5 | 0.112 | |
| LDL (mg/dL) | 128.4± 34.2 | 135.5 ± 35.2 | 0.582 | 105.11± 17 | 103.9 ± 15.7 | 0.811 | |
| HDL (mg/dL) | 46.5 ± 20.17 | 49± 14.02 | 0.665 | 52.4 ± 6.5 | 57.09 ± 15.9 | 0.253 | |
| Group I Total NAFLD Patients N = 40 | Fibrosis Stage (F0) N = 30 | Fibrosis Stage (F1) N = 10 | p-Value | |
|---|---|---|---|---|
| Fibroscan (kPa) | ||||
| Mean ± SD | 5.1 ± 0.99 | 4.7 ± 0.67 | 6.5 ± 0.3 | <0.001 ** |
| Range | 3.8–6.9 | 3.8–5.9 | 6.2–6.9 | |
| CAP (dB/m) | ||||
| Mean ± SD | 263.9 ± 11.61 | 260.4 ± 10.9 | 274.2 ± 6.44 | <0.001 ** |
| Range | 242–286 | 242–286 | 265–286 | |
| FAST score | ||||
| Mean ± SD | 0.203 ± 0.139 | 0.2377 ± 0.14 | 0.099 ± 0.09 | 0.001 ** |
| Range | 0.04–0.47 | 0.05–0.47 | 0.04–0.25 | |
| NAFLD fibrosis score | 0.147 | |||
| Mean ± SD | −1.37 ± 1.38 | −1.19 ± 1.4 | −1.92 ± 1.01 | |
| Range | −4.1–1.22 | −4.1–1.22 | −3.2–0.33 | |
| FIB 4 | ||||
| Mean ± SD | 0.919 ± 0.46 | 0.96 ± 0.5 | 0.81 ± 0.28 | 0.376 |
| Range | 0.33–2.39 | 0.33–2.39 | 0.36–1.14 |
| Parameters | CD24 Gene Expression | |
|---|---|---|
| r | p-Value | |
| Kpa (kPa) | −0.070 | 0.677 |
| CAP(dB/m) | −0.050 | 0.764 |
| FAST | −0.006 | 0.970 |
| NFS | 0.356 | 0.001 ** |
| FIB-4 | 0.090 | 0.432 |
| Variables | Coefficient | Sig. | Odds Ratio |
|---|---|---|---|
| age | 0.695 | 0.999 | 2.003 |
| sex | −8.443 | 0.999 | 0.000 |
| DM | 27.061 | 1.000 | 565,692,536,831.086300 |
| BMI | −5.426 | 0.997 | 227.262 |
| Fold change of CD24 | 1.372 | 1.000 | 3.943 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amin, M.A.; Ragab, H.M.; Abd El Maksoud, N.; Elaziz, W.A. CD24 Gene Expression as a Risk Factor for Non-Alcoholic Fatty Liver Disease. Diagnostics 2023, 13, 984. https://doi.org/10.3390/diagnostics13050984
Amin MA, Ragab HM, Abd El Maksoud N, Elaziz WA. CD24 Gene Expression as a Risk Factor for Non-Alcoholic Fatty Liver Disease. Diagnostics. 2023; 13(5):984. https://doi.org/10.3390/diagnostics13050984
Chicago/Turabian StyleAmin, Mona A., Halla M. Ragab, Nabila Abd El Maksoud, and Wafaa Abd Elaziz. 2023. "CD24 Gene Expression as a Risk Factor for Non-Alcoholic Fatty Liver Disease" Diagnostics 13, no. 5: 984. https://doi.org/10.3390/diagnostics13050984