
Multisystem Inflammatory Syndrome in Adults Associated with Recent Infection with COVID-19


Abstract
:1. Introduction
- Serious involvement of the heart: myo-, pericarditis, dilatation or aneurysm of the coronary arteries, or new dysfunction of the right or left ventricle, atrioventricular block II.-III. degree or ventricular tachycardia;
- rash and nonpurulent conjunctivitis.
- Newly developed neurological signs and symptoms: encephalopathy in a patient without previous cognitive deficit, convulsions, meningeal symptoms, peripheral neuropathy;
- Shock or hypotension not caused by medication (sedation);
- Abdominal pain, vomiting, diarrhea;
- Thrombocytopenia.
- Elevated value of at least two of the following: C-reactive protein (CRP), ferritin, IL-6, erythrocyte sedimentation rate, procalcitonin (PCT);
- Positive test for SARS-CoV-2 during illness using RT-PCR, serology, or antigen detection.
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Viner, R.M.; Whittaker, E. Kawasaki-like disease: Emerging complication during the COVID-19 pandemic. Lancet 2020, 395, 1741–1743. [Google Scholar] [CrossRef] [PubMed]
- Pérez, A.; Torregrosa, I.; D’Marco, L.; Juan, I.; Terradez, L.; Solís, M.Á.; Moncho, F.; Carda-Batalla, C.; Forner, M.J.; Gorriz, J.L. IgAdominant infection-associated glomerulonephritis following SARS-CoV-2 infection. Viruses 2021, 13, 587. [Google Scholar] [CrossRef] [PubMed]
- Licciardi, F.; Pruccoli, G.; Denina, M.; Parodi, E.; Taglietto, M.; Rosati, S.; Montin, D. SARSCoV-2–induced Kawasaki-like hyperinfammatory syndrome: A novel COVID phenotype in children. Pediatrics 2020, 146, e20201711. [Google Scholar] [CrossRef] [PubMed]
- CDC. Multisystem Inflammatory Syndrome in Adults (MIS-A)—Case Definition. Available online: https://www.cdc.gov/mis-c/mis-a/hcp.html (accessed on 11 May 2021).
- Cheung, E.W.; Zachariah, P.; Gorelik, M.; Boneparth, A.; Kernie, S.G.; Orange, J.S.; Milner, J.D. Multisystem Inflammatory Syndrome Related to COVID-19 in Previously Healthy Children and Adolescents in New York City. JAMA 2020, 324, 294–296. [Google Scholar] [CrossRef] [PubMed]
- Chau, V.Q.; Giustino, G.; Mahmood, K.; Oliveros, E.; Neibart, E.; Oloomi, M.; Moss, N.; Mitter, S.S.; Contreras, J.P.; Croft, L.; et al. Cardiogenic shock and hyperinflammatory syndrome in young males with COVID-19. Circ. Heart Fail. 2020, 13, e007485. [Google Scholar] [CrossRef] [PubMed]
- Patel, P.; DeCuir, J.; Abrams, J.; Campbell, A.P.; Godfred-Cato, S.; Belay, E.D. Clinical characteristics of multisystem inflammatory syndrome in adults: A systematic review. JAMA Netw. Open 2021, 4, e2126456. [Google Scholar] [CrossRef] [PubMed]
- Behzadi, F.; Ulloa, N.A.; Danckers, M. Multisystem inflammatory syndrome in adults: A case report and review of the literature. J. Med. Case Rep. 2022, 16, 102. [Google Scholar] [CrossRef] [PubMed]
- Mazumder, M.A.; Narula, A.S.; Gulati, S.; Shehwar, D.; Mir, I.M. Post-COVID Multisystem Inflammatory Syndrome-Adult (MIS-A) Presenting with Rhabdomyolysis and AKI. Indian J. Nephrol. 2022, 32, 629–632. [Google Scholar] [CrossRef]
- Kobe, H.; Ito, A.; Ishida, T. COVID-19-induced adult multisystem inflammatorysyndrome and fatal acute limb ischaemia. Respirol. Case Rep. 2021, 10, e0886. [Google Scholar] [CrossRef] [PubMed]
- Taylor, F.B., Jr.; Toh, C.H.; Hoots, K.W.; Wada, H.; Levi, M. Towards definition, clinical and laboratory criteria, and a scoring system for disseminated intravascular coagulation. Thromb. Haemost. 2001, 86, 1327–1330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vogel, T.P.; Top, K.A.; Karatzios, C.; Hilmers, D.C.; Tapia, L.I.; Moceri, P.; Giovannini-Chami, L.; Wood, N.; Chandler, R.E.; Klein, N.P.; et al. Multisystem inflammatory syndrome in children and adults (MIS-C/A): Case definition & guidelines for data collection, analysis, and presentation of immunization safety data. Vaccine 2021, 39, 3037–3049. [Google Scholar] [CrossRef] [PubMed]
- Lidder, A.K.; Pandit, S.A.; Lazzaro, D.R. An adult with COVID-19 kawasaki-like syndrome and ocular manifestations. Am. J. Ophthalmol. Case Rep. 2020, 20, 100875. [Google Scholar] [CrossRef] [PubMed]
- Tung-Chen, Y.; Algora-Martín, A.; Rodríguez-Roca, S.; Díaz de Santiago, A. COVID-19 multisystemic inflammatory syndrome in adults: A not to be missed diagnosis. BMJ Case Rep. 2021, 14, e241696. [Google Scholar] [CrossRef] [PubMed]
- Uwaydah, A.K.; Hassan, N.M.M.; Abu Ghoush, M.S.; Shahin, K.M.M. Adult multisystem inflammatory syndrome in a patient who recovered from COVID-19 postvaccination. BMJ Case Rep. 2021, 14, e242060. [Google Scholar] [CrossRef] [PubMed]
- Hékimian, G.; Kerneis, M.; Zeitouni, M.; Cohen-Aubart, F.; Chommeloux, J.; Bréchot, N.; Mathian, A.; Lebreton, G.; Schmidt, M.; Hié, M.; et al. Coronavirus disease 2019 acute myocarditis and multisystem inflammatory syndrome in adult intensive and cardiac care units. Chest 2021, 159, 657–662. [Google Scholar] [CrossRef] [PubMed]
- DeCuir, J.; Baggs, J.; Melgar, M.; Patel, P.; Wong, K.K.; Schwartz, N.G.; Morris, S.B.; Godfred-Cato, S.; Belay, E.D. Identification and description of patients with multisystem inflammatory syndrome in adults associated with SARS-CoV-2 infection using the Premier Healthcare Database. Epidemiol. Infect. 2022, 150, e26. [Google Scholar] [CrossRef] [PubMed]
- Yao, Q.; Waley, L.; Liou, N. Adult presentation of multisystem inflammatory syndrome (MIS) associated with recent COVID-19 infection: Lessons learnt in timely diagnosis and management. BMJ Case Rep. 2021, 14, e243114. [Google Scholar] [CrossRef] [PubMed]
- Kunal, S.; Ish, P.; Sakthivel, P.; Malhotra, N.; Gupta, K. The emerging threat of multisystem inflammatory syndrome in adults (MIS-A) in COVID-19: A systematic review. Heart Lung. 2022, 54, 7–18. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 24 February 2022).
- Llitjos, J.-F.; Leclerc, M.; Chochois, C.; Monsallier, J.-M.; Ramakers, M.; Auvray, M.; Merouani, K. High incidence of venous thromboembolic events in anticoagulated severe COVID-19 patients. J. Thromb. Haemost. 2020, 18, 1743–1746. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Day of Hospitalization | 1. | 3. | 5. | 6. | 8. | 13. | 17. |
|---|---|---|---|---|---|---|---|
| Monitored Parameter | |||||||
| C-reactive protein (CRP) (mg/L) | 82.06 | 128.1 | 172.2 | 115.1 | 63.6 | 8.2 | 0.69 |
| Procalcitonin (PCT) (ug/L) | 0.24 | 0.73 | 1.19 | 0.73 | 0.34 | 0.05 | 0.04 |
| Interleukin-6 (IL-6) (ng/L) | 42.13 | 328.1 | 65.6 | 7.68 | 3.96 | 1.5 | 2.3 |
| Lactate (mmol/L) | 2.67 | 2.17 | 1.88 | 1.58 | 1.44 | 2.08 | 1.74 |
| Creatinekinase (ukat/L) | 1.2 | 1.5 | 0.8 | 0.52 | 0.41 | 0.15 | 1.2 |
| Creatine kinase-MB (ukat/L) | 0.17 | 0.14 | 0.16 | 0.19 | 0.20 | 0.29 | 0.22 |
| Troponin T (ug/L) | 0.003 | 0.007 | 0121 | 0.077 | 0.041 | 0.028 | 0.005 |
| White blood cell (×109/L) | 6.36 | 3.26 | 4.80 | 7.21 | 9.55 | 7.26 | 8.79 |
| Neutrophils (%) | 82.6 | 82.1 | 91 | 91.7 | 93.2 | 89.2 | 77.9 |
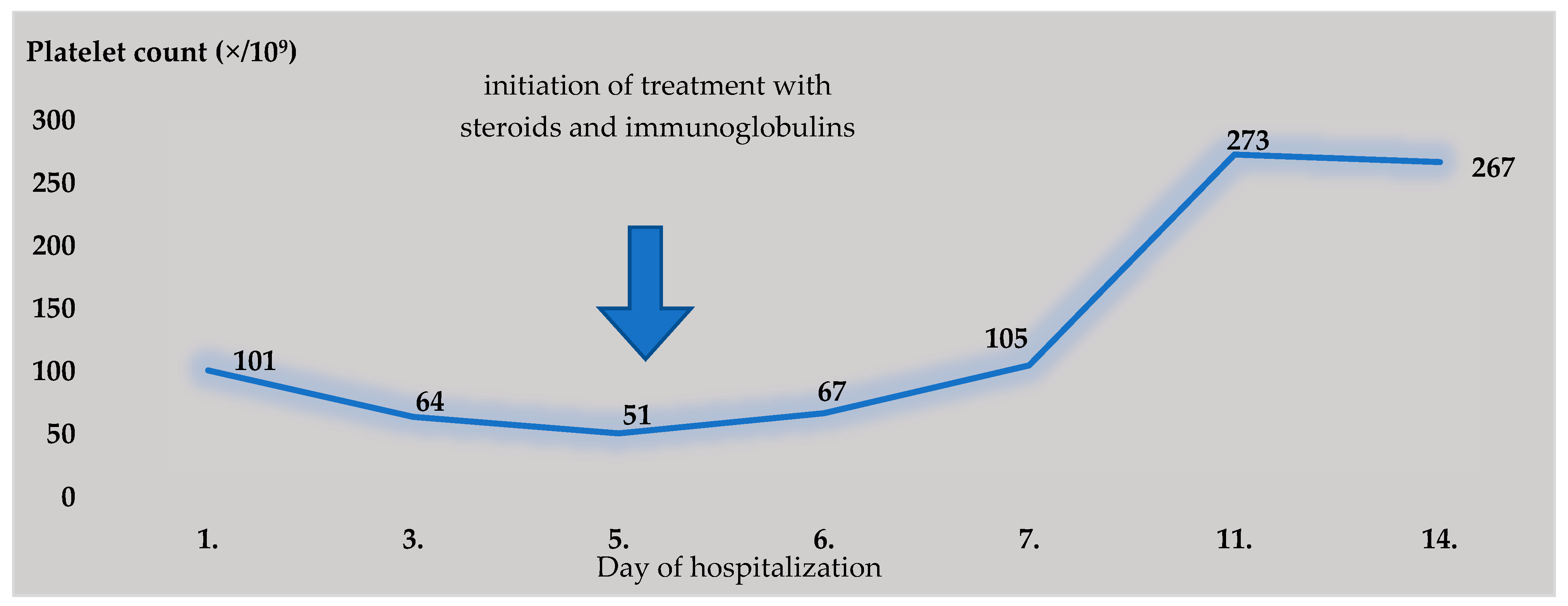
| Platelets (×109/L) | 101 | 64 | 51 | 67 | 105 | 273 | 267 |
| D-dimer (mg/L) | 0.43 | 1.5 | 1.48 | 2.26 | 2.40 | 1.96 | 0.46 |
| NTproBNP (ng/L) | 122 | * | 5438 | 8730 | 3709 | * | 125 |
| Biological Material | Result | |
|---|---|---|
| PCR SARS-CoV-2 | Nasopharyngeal Swab | Pozit. Ct 32.2 Pozit. Ct 35.2 * |
| Anti-Epstein-Barr virus antibodies | serum | IgM negat./IgG pozit |
| Anti-Cytomegalovirus antibodies | serum | IgM negat./IgG negat. * |
| Anti-HIV virus antibodies | serum | negat. |
| Anti-Chlamydia pneumoniae antibodies | serum | IgM/IgA/IgG negat. |
| Anti-Mycoplasma pneumoniae antibodies | serum | IgM/IgA/IgG negat. |
| Hepatitis B surface antigen | serum | negat. |
| anti-Hepatitis C antibodies | serum | negat. |
| Anti-Herpes simplex 1,2 antibodies | serum | IgM negat./IgG pozit. |
| Anti-Francisella tularensis antibodies | serum | negat. |
| Anti-Leptospira icterohemoragiae antibodies | serum | negat. |
| Candida/Aspergillus antigen | serum | negat. |
| antigen Legionella pneumophila/Streptococcus pneumoniae | urine | negat. |
| PCR Influenza A/B | nasopharyngeal swab | negat. |
| adeno, rota, noroviruses antigen | stool | negat. |
| stool/rectal swab culture | stool | negat. |
| urine culture | urine | sterile * |
| Clostridioides difficile-toxin A/B, antigen | stool | negat. |
| blood culture | blood | sterile * |
| Brighton Collaboration Case Definition | Patient from Our Case Report |
|---|---|
| Age | |
| Age <21 years (MIS-C) or ≥21 years (MIS-A) | 22 |
| Fever | |
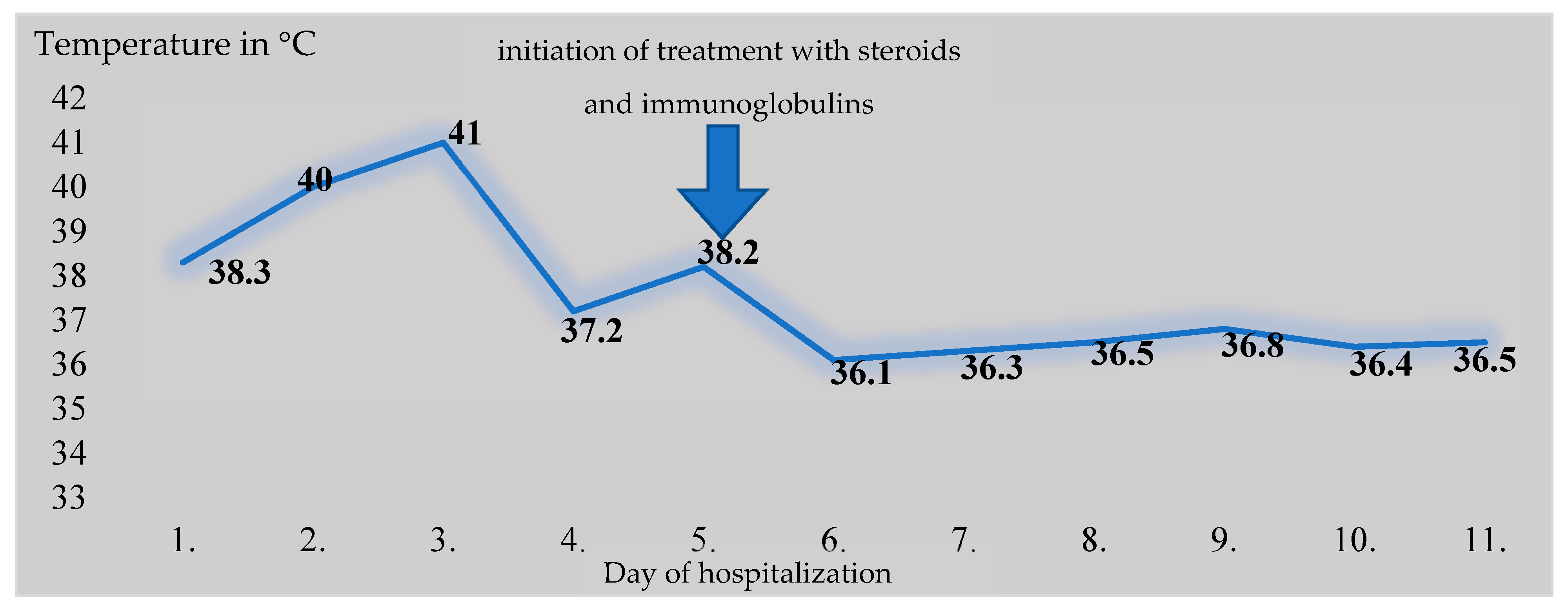
| ≥3 Consecutive days | 6 |
| ≥2 Clinical features | |
| Mucocutaneous | Nonpurulent conjunctivitis, maculopapular exanthema on the chest |
| Gastrointestinal | Diarrhea, vomiting, and abdominal pain |
| Shock/hypotension | Hypotension, clinical signs of shock |
| Neurologic | Headaches |
| Laboratory markers of inflammation | |
| Elevated CRP | 172.2 mg/L (maximal value) |
| Erythrocyte sedimentation rate | 20 mm (after 1 h)/35 mm (after 2 h) |
| Elevated ferritin | 556 ug/L (maximal value) |
| Elevated procalcitonin | 1.19 ug/L (maximal value) |
| ≥2 Measures of disease activity | |
| Elevated BNP or NTproBNP or Troponin T | NTproBNP: 8730 ng/L; Troponin T: 0.121 ug/L (maximal value) |
| Neutrophilia, lymfophenia, or thrombocytopenia | Neutrophils: 93.2%; Lymphocyte 3.30%; Platelets 51 × 109/L |
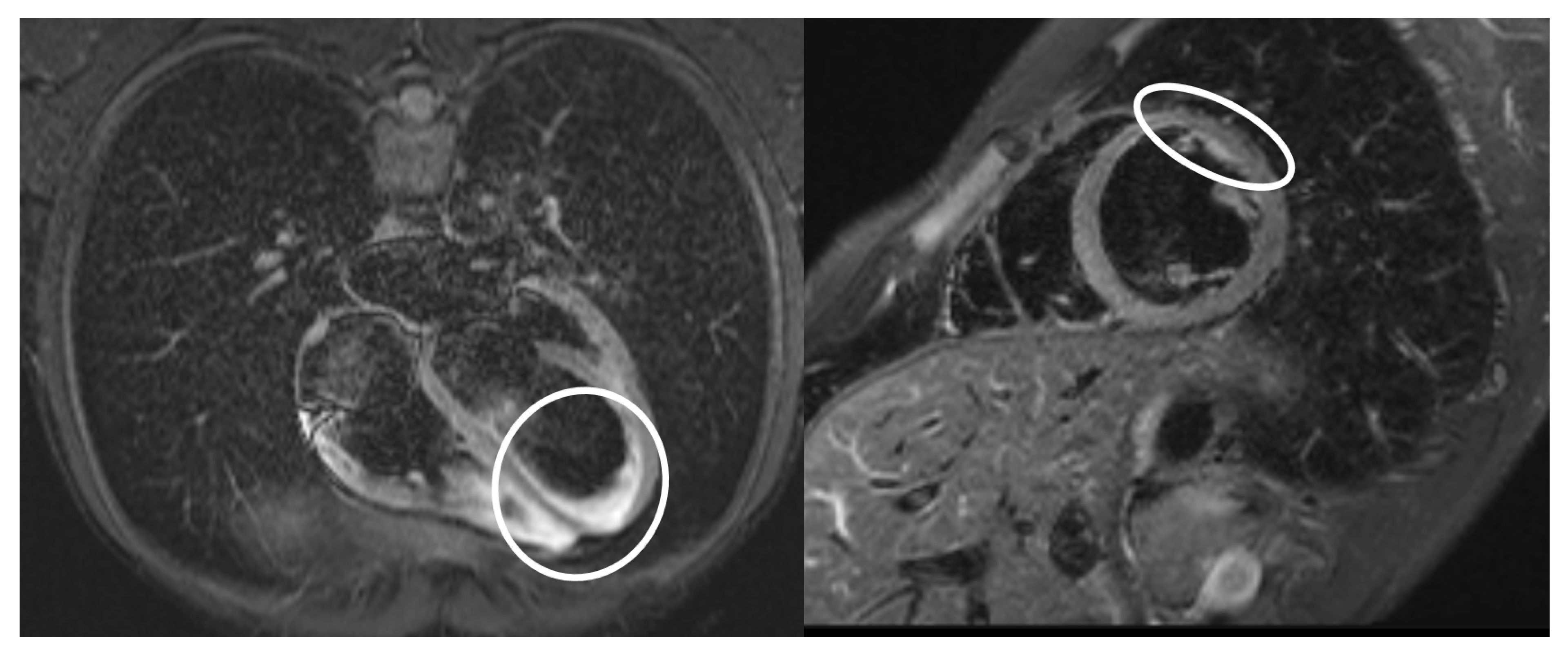
| Echocardiographic evidence of cardiac involvement or physical sigmata of heart failure | Pericardial effusion |
| ECG changes consistent with myocarditis | Sinus tachycardia and bigeminal ventricular extrasystoles |
| SARS-CoV-2 | |
| Laboratory confirmed SARS-CoV-2 infection or | Yes—PCR SARS-CoV-2 pozit. ct 32.2; ct 35.2 |
| Personal historyof suspected COVID-19 within 12 weeks or | Yes |
| Close contact with known COVID-19 case within 12 week | Probably yes |
| OR | |
| SARS-CoV-2 vaccination | Yes—1 dose before 1 year |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zahornacky, O.; Porubčin, Š.; Rovnakova, A.; Jarcuska, P. Multisystem Inflammatory Syndrome in Adults Associated with Recent Infection with COVID-19. Diagnostics 2023, 13, 983. https://doi.org/10.3390/diagnostics13050983
Zahornacky O, Porubčin Š, Rovnakova A, Jarcuska P. Multisystem Inflammatory Syndrome in Adults Associated with Recent Infection with COVID-19. Diagnostics. 2023; 13(5):983. https://doi.org/10.3390/diagnostics13050983
Chicago/Turabian StyleZahornacky, Ondrej, Štefan Porubčin, Alena Rovnakova, and Pavol Jarcuska. 2023. "Multisystem Inflammatory Syndrome in Adults Associated with Recent Infection with COVID-19" Diagnostics 13, no. 5: 983. https://doi.org/10.3390/diagnostics13050983