
Artificial Intelligence for Evaluation of Retinal Vasculopathy in Facioscapulohumeral Dystrophy Using OCT Angiography: A Case Series

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Neurological Examination
2.3. Ophthalmological Assessment
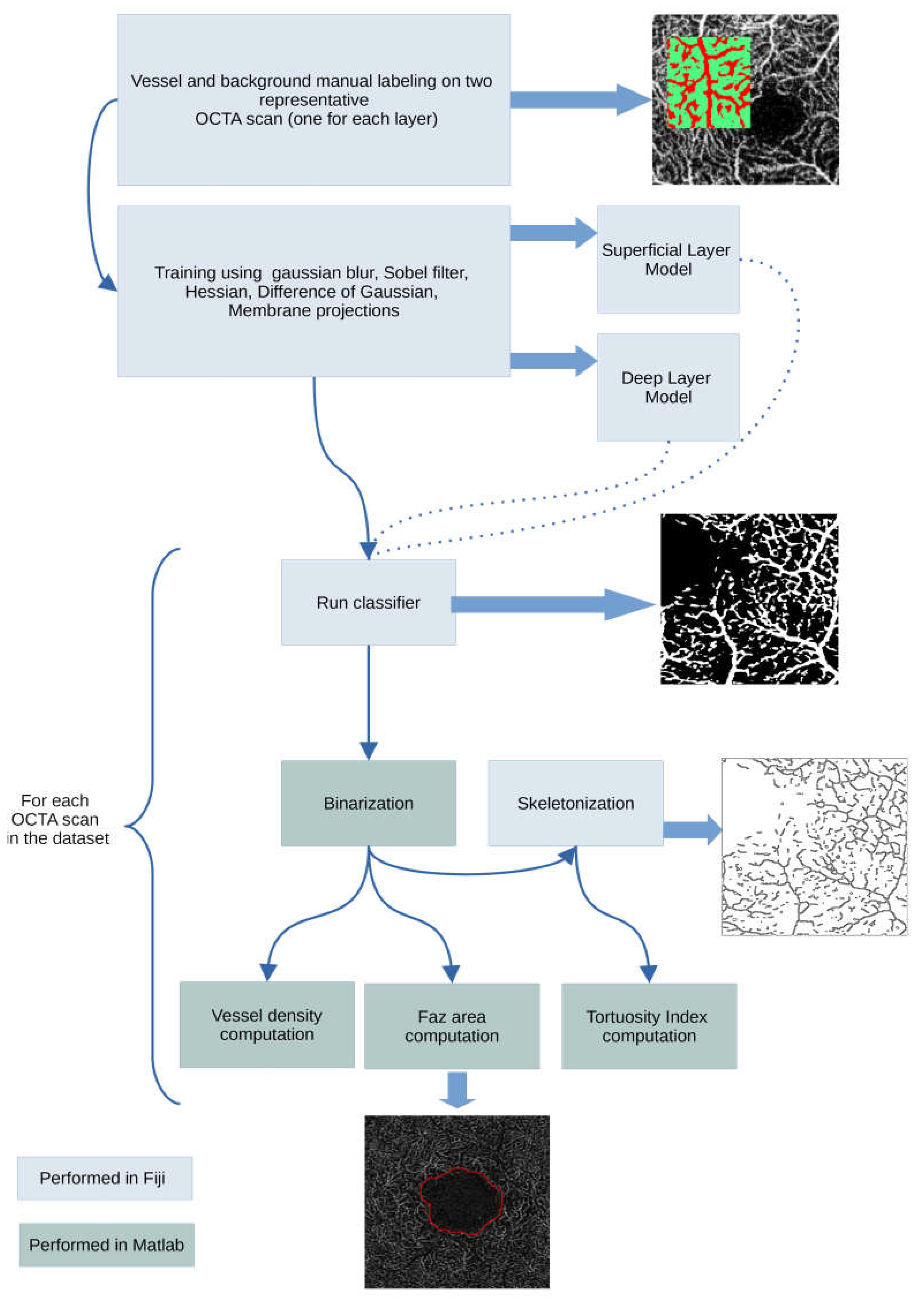
2.4. OCT-A Image Processing
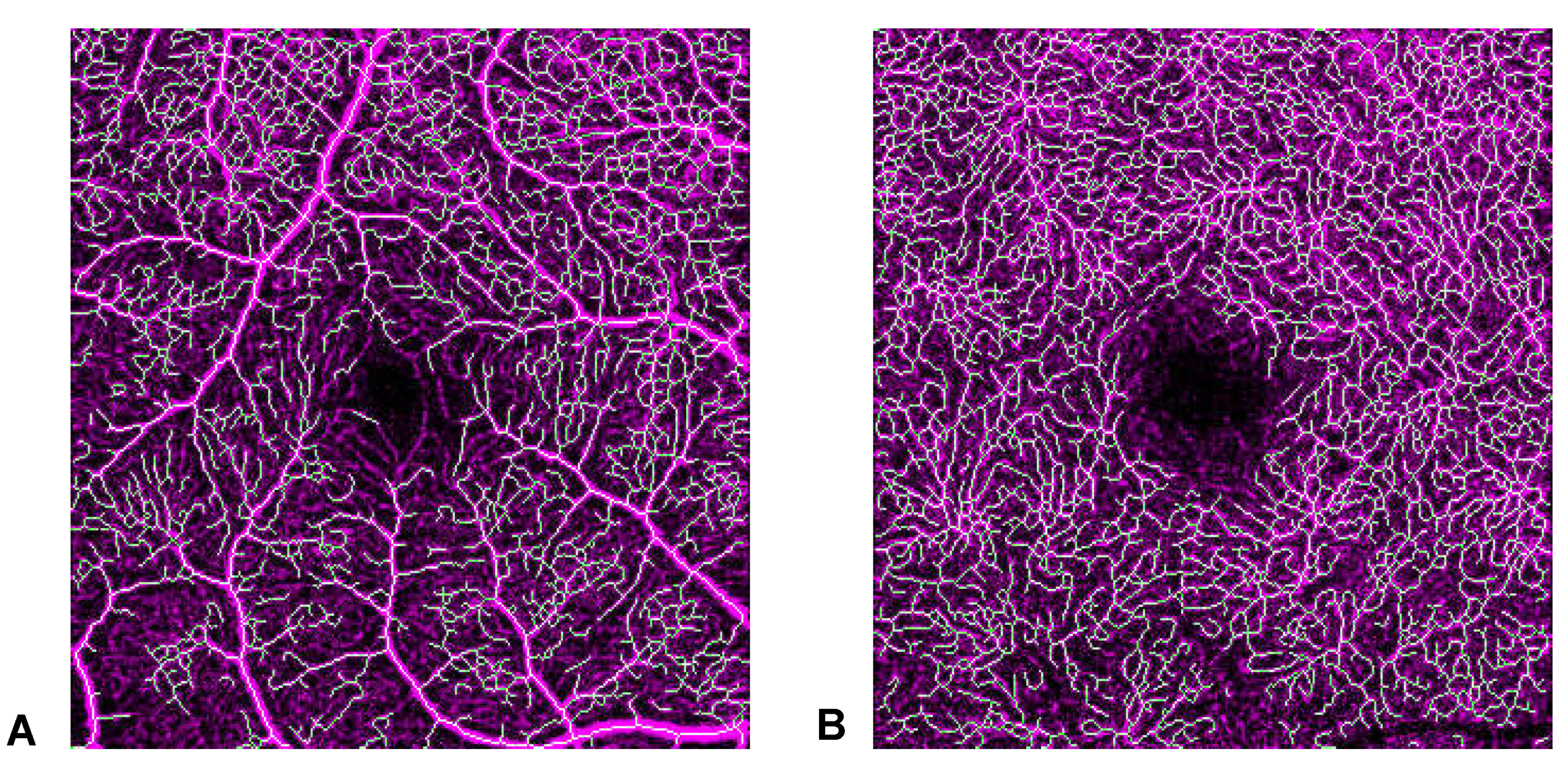
2.4.1. Tortuosity Index (TI)
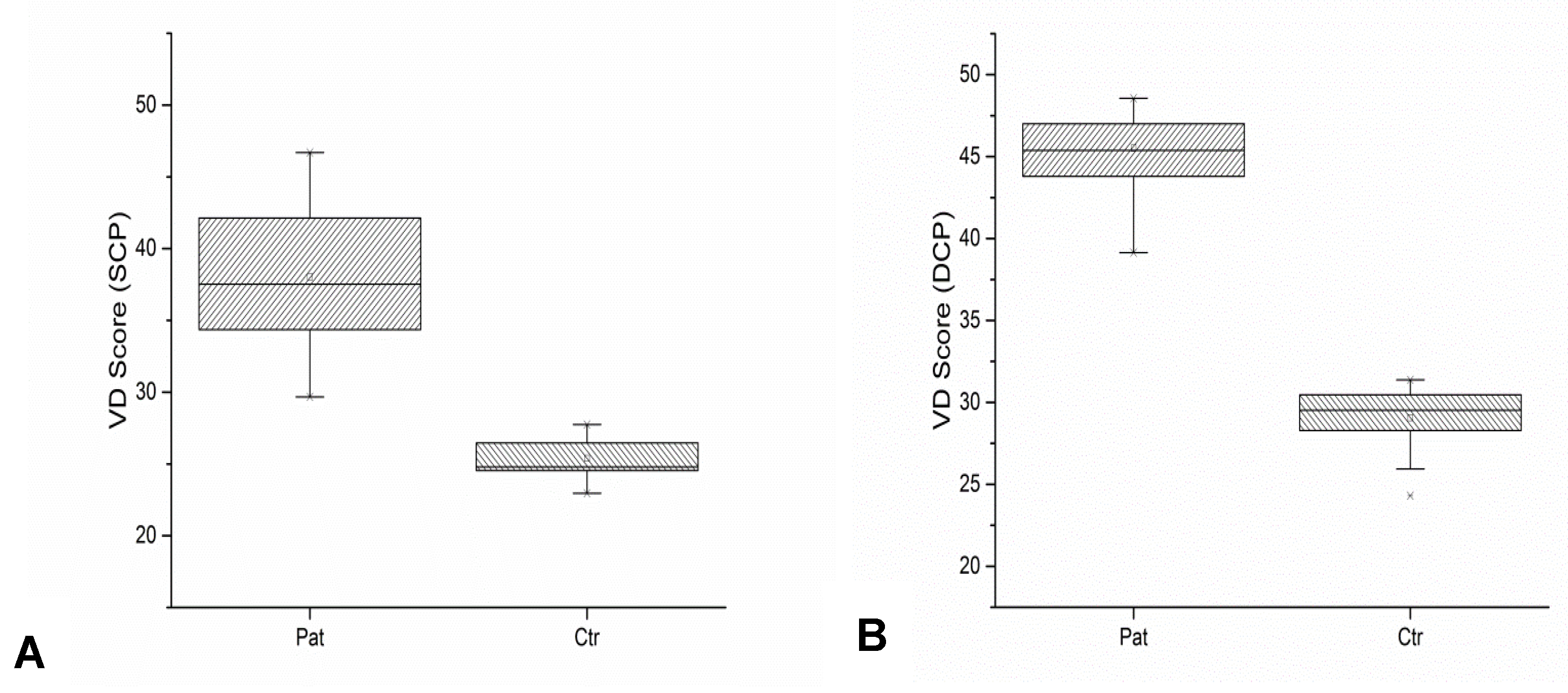
2.4.2. Vessel Density Score (VD Score)
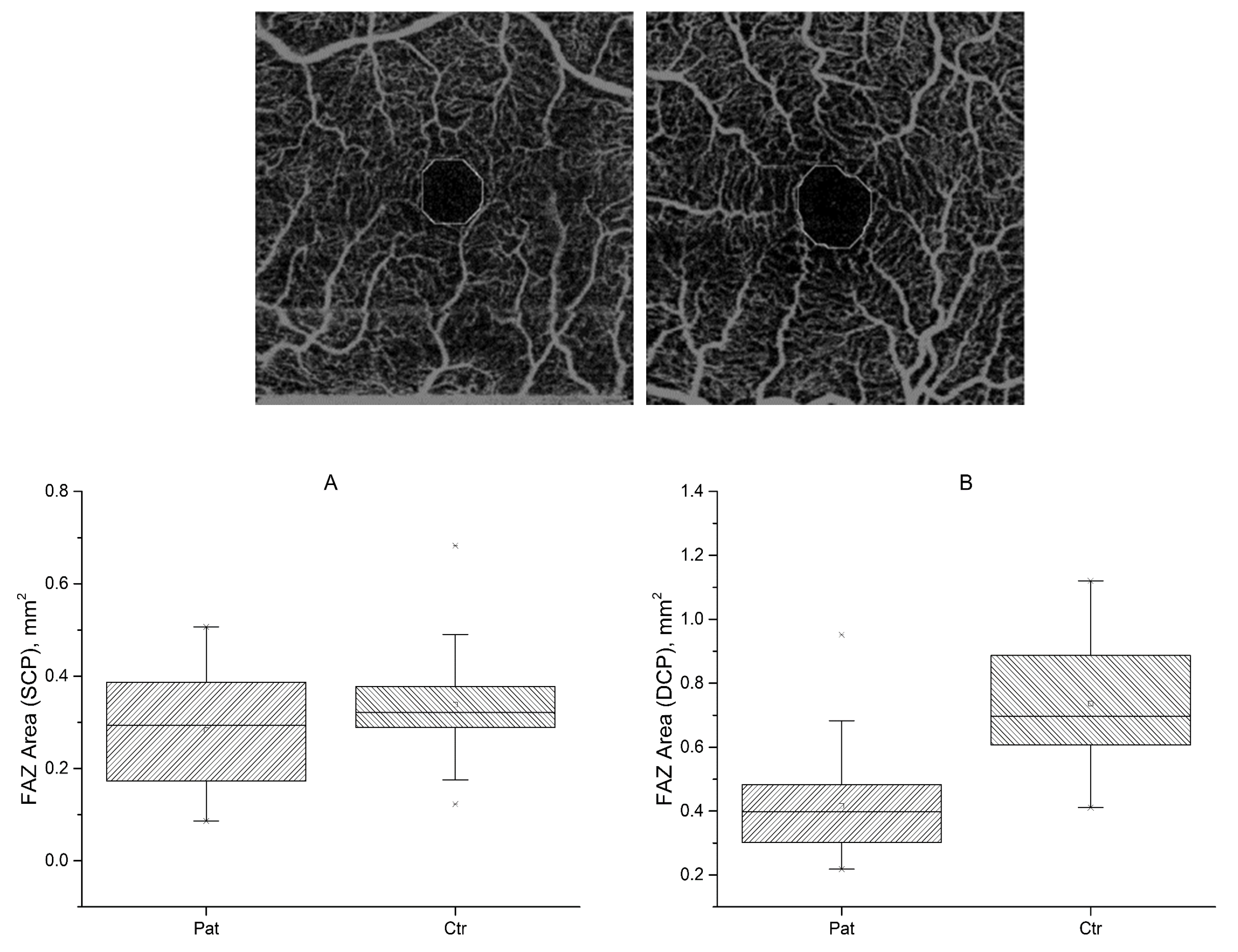
2.4.3. FAZ Area
2.5. Statistical Analysis
3. Results
3.1. Population
3.2. Ophthalmological Examination
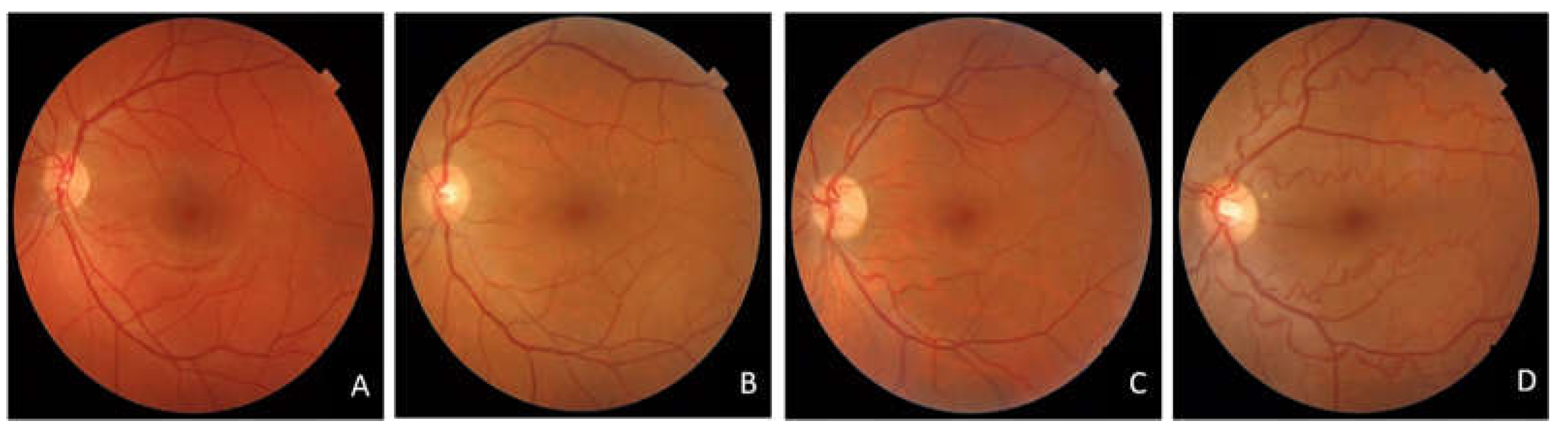
3.2.1. Colour Fundus Photography
3.2.2. Optical Coherence Tomography Angiography
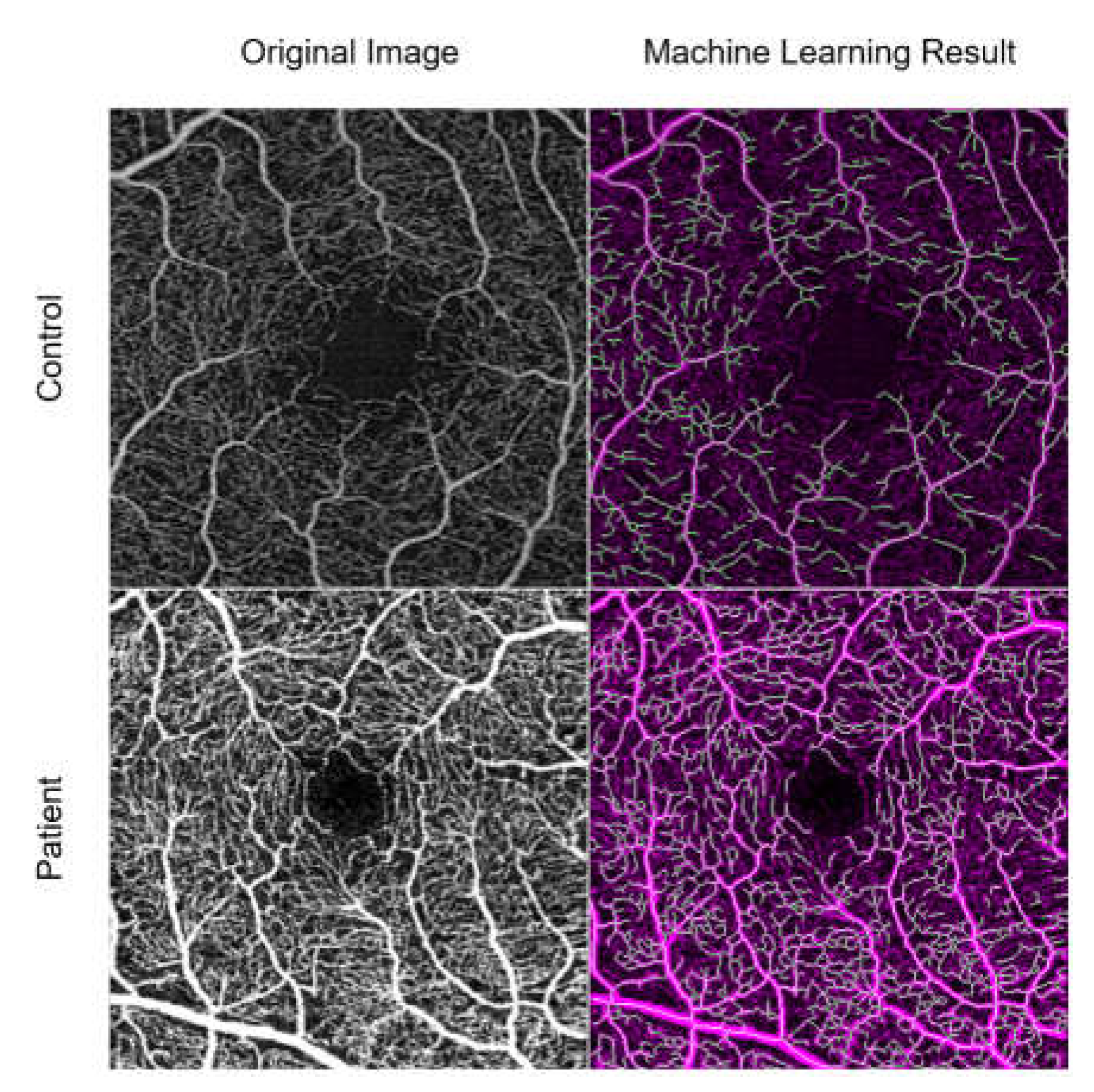
3.3. Machine Learning Results
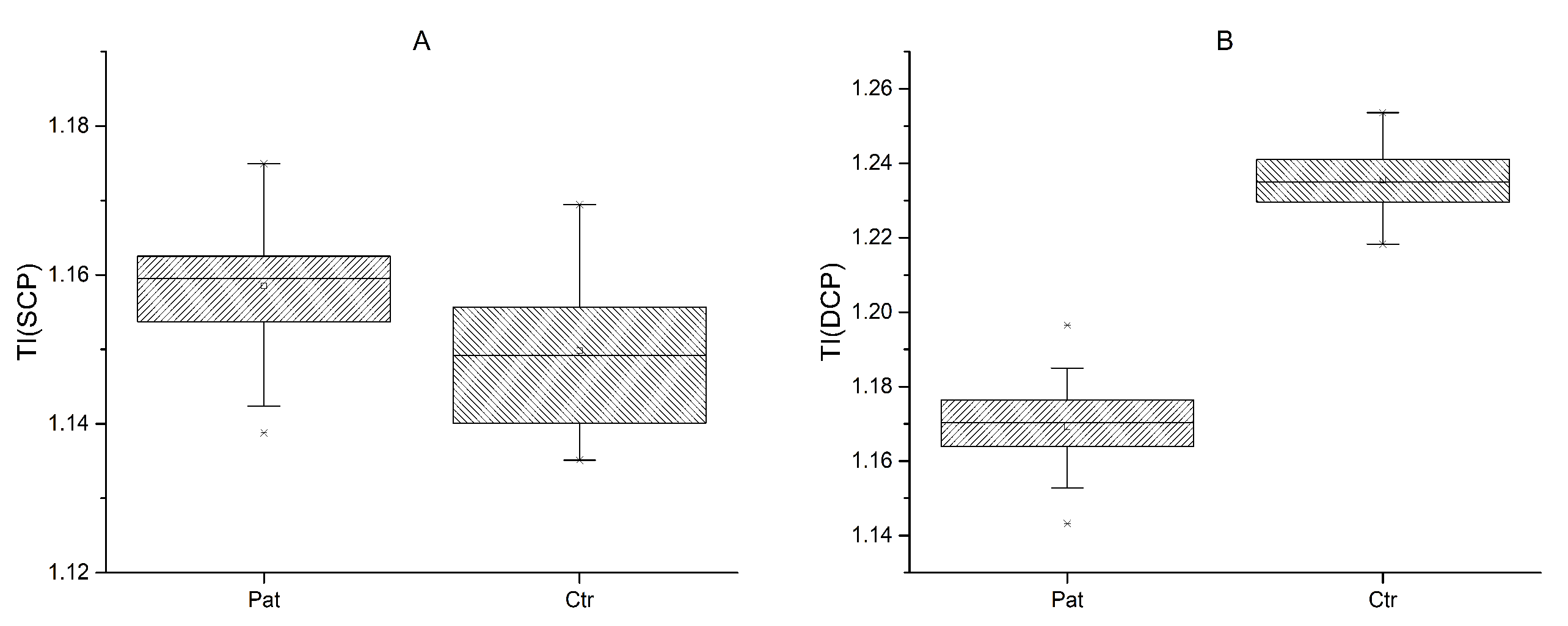
3.3.1. Tortuosity Index
3.3.2. Vessel Density Score
3.3.3. Foveal Avascular Zone
4. Discussion
Considerations of AI and Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tawil, R.; Kissel, J.T.; Heatwole, C.; Pandya, S.; Gronseth, G.; Benatar, M. Evidence-based guideline summary: Evaluation, diagnosis, and management of facioscapulohumeral muscular dystrophy: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology and the Practice Issues Review Panel of the American Association of Neuromuscular & Electrodiagnostic Medicine. Neurology 2015, 85, 357–364. [Google Scholar]
- De Simone, A.M.; Pakula, A.; Lek, A.; Emerson, C.P., Jr. Facioscapulohumeral Muscolar Dystrophy. Compr. Physiol. 2017, 7, 1229–1279. [Google Scholar]
- Tasca, G.; Monforte, M.; Ottaviani, P.; Pelliccioni, M.; Frusciante, R.; Laschena, F.; Ricci, E. Magnetic resonance imaging in a large cohort of facioscapulohumeral muscular dystrophy patients: Pattern refinement and implications for clinical trials. Ann. Neurol. 2016, 79, 854–864. [Google Scholar] [CrossRef] [PubMed]
- Monforte, M.; Laschena, F.; Ottaviani, P.; Bagnato, M.R.; Pichiecchio, A.; Tasca, G.; Ricci, E. Tracking muscle wasting and disease activity in facioscapulohumeral muscular dystrophy by qualitative longitudinal imaging. J. Cachexia Sarcopenia Muscle 2019, 10, 1258–1265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzsimons, R.B.; Gurwin, E.B.; Bird, A.C. Retinal vascular abnormalities in facioscapulohumeral muscular dystrophy. A general association with genetic and therapeutic implications. Brain 1987, 110, 631–648. [Google Scholar] [CrossRef] [PubMed]
- Padberg, G.W.; Brouwer, O.F.; De Keizer, R.J.; Dijkman, G.; Wijmenga, C.; Grote, J.J.; Frants, R.R. On the significance of retinal vascular disease and hearing loss in facioscapulohumeral muscular dystrophy. Muscle Nerve 1995, 2, 73–80. [Google Scholar] [CrossRef] [Green Version]
- Longmuir, S.Q.; Mathews, K.D.; Longmuir, R.A.; Joshi, V.; Olson, R.J.; Abràmoff, M.D. Retinal but not venous tortuosity correlates with facioscapulohumeral muscular dystrophy severity. J. AAPOS 2010, 14, 240–243. [Google Scholar] [CrossRef]
- Shields, C.L.; Zahler, J.; Falk, N.; Furuta, M.; Eagle, R.C.; Espinosa, L.E.; Fischer, P.R.; Shields, J.A. Neovascular glaucoma from advanced Coats disease as the initial manifestation of facioscapulohumeral dystrophy in a 2-year-old child. Arch. Opthalmol. 2007, 125, 840–842. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Murphy, O.; Caldito, N.G.; Calabresi, P.A.; Saidha, S. Emerging Applications of Optical Coherence Tomography Angiography (OCTA) in neurological research. Eye Vis. 2018, 5, 11. [Google Scholar] [CrossRef]
- Spaide, R.F.; Klancnik, J.M., Jr.; Cooney, M.J. Retinal Vascular Layers Imaged by Fluorescein Angiography and Optical Coherence Tomography Angiography. JAMA Ophthalmol. 2015, 133, 45–50. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.; Lee, M.; Chung, H.; Kim, H.C. Quantification of retinal vessel tortuosity in diabetic retinopathy using optical coherence tomography angiography. Retina 2018, 38, 976–985. [Google Scholar] [CrossRef] [PubMed]
- Spaide, R.F.; Fujimoto, J.G.; Waheed, N.K.; Sadda, S.R.; Staurenghi, G. Optical coherence tomography angiography. Prog. Retin. Eye Res. 2018, 64, 1–55. [Google Scholar] [CrossRef]
- Goselink, R.J.; Schreur, V.; van Kernebeek, C.R.; Padberg, G.W.; van der Maarel, S.M.; van Engelen, B.G.; Erasmus, C.E.; Theelen, T. Ophthalmological findings in facioscapulohumeral dystrophy. Brain Commun. 2019, 1, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Ricci, E.; Galluzzi, G.; Deidda, G.; Cacurri, S.; Colantoni, L.; Merico, B.; Piazzo, N.; Servidei, S.; Vigneti, E.; Pasceri, V.; et al. Progress in the molecular diagnosis of facioscapulohumeral muscular dystrophy and correlation between the number of KpnI repeats at the 4q35 locus and clinical phenotype. Ann. Neurol. 1999, 45, 751–757. [Google Scholar] [CrossRef]
- Van Overveld, P.G.; Enthoven, L.; Ricci, E.; Rossi, M.; Felicetti, L.; Jeanpierre, M.; Winokur, S.T.; Frants, R.R.; Padberg, G.W.; Van Der Maarel, S.M. Variable hypomethylation of D4Z4 in facioscapulohumeral muscular dystrophy. Ann. Neurol. 2005, 58, 569–576. [Google Scholar] [CrossRef]
- Armstrong, R.A. Statistical guidelines for the analysis of data obtained from one or both eyes. Ophthalmic Physiol. Opt. 2013, 33, 7–14. [Google Scholar] [CrossRef]
- Schindelin, J.; Arganda-Carreras, I.; Frise, E.; Kaynig, V.; Longair, M.; Pietzsch, T.; Preibisch, S.; Rueden, C.; Saalfeld, S.; Schmid, B.; et al. Fiji: An open-source platform for biological-image analysis. Nat. Methods 2012, 9, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Sage, D.; Prodanov, D.; Tinevez, J.Y.; Schindelin, J. MIJ: Making Interoperability Between ImageJ and Matlab Possible. In ImageJ User & Developer Conference (IUDC’12), Mondorf-les-Bains; Grand Duchy of Luxembourg: Luxembourg, 2012. [Google Scholar]
- Hiner, M.C.; Rueden, C.T.; Eliceiri, K.W. ImageJ-MATLAB: A bidirectional framework for scientific image analysis interoperability. Bioinformatics 2017, 33, 629–630. [Google Scholar] [CrossRef] [Green Version]
- Arganda-Carreras, I.; Kaynig, V.; Rueden, C.; Schindelin, J.; Cardona, A.; Seung, H.S.; Ezzat, M.; Hiner, M.; Freydiere, P. Trainable_Segmentation: Release v3.1.2. Zenodo 2016, 59290. [Google Scholar]
- Software—Artificial Intelligence Institute: University of Waikato. Available online: https://ai.waikato.ac.nz/software (accessed on 23 February 2023).
- Breiman, L. Random Forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Minnella, A.M.; Barbano, L.; Verrecchia, E. Macular impairment in Fabry disease: A morpho-functional assessment by swept-source OCT angiography and Focal Electroretinography. Investig. Opthalmol. Vis. Sci. 2019, 60, 2667–2675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savastano, M.C.; Gambini, G.; Cozzupoli, G.M.; Crincoli, E.; Savastano, A.; De Vico, U.; Culiersi, C.; Falsini, B.; Martelli, F.; Minnella, A.M.; et al. Retinal capillary involvement in early post-COVID-19 patients: A healthy controlled study. Graefe’s Arch. Clin. Exp. Ophthalmol. 2021, 259, 2157–2165. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Wang, J.C.; Zeng, R.; Katz, R.; Vavvas, D.G.; Miller, J.W.; Miller, J.B. Quantitative Comparison Of Microvascular Metrics On Three Optical Coherence Tomography Angiography Devices In Chorioretinal Disease. Clin. Ophthalmol. 2019, 13, 2063–2069. [Google Scholar] [CrossRef] [Green Version]
- Yu, J.; Jiang, C.; Wang, X.; Zhu, L.; Gu, R.; Xu, H.; Jia, Y.; Huang, D.; Sun, X. Macular perfusion in healthy Chinese: An optical coherence tomography angiogram study. Investig. Ophthalmol. Vis. Sci. 2015, 56, 3212–3217. [Google Scholar] [CrossRef]
- Gómez-Ulla, F.; Cutrin, P.; Santos, P.; Fernandez, M.; Abraldes, M.; Abalo-Lojo, J.M.; Gonzalez, F. Age and gender influence on foveal avascular zone in healthy eyes. Exp. Eye Res. 2019, 189, 107856. [Google Scholar] [CrossRef]
- Osborne, R.J.; Welle, S.; Venance, S.L.; Thornton, C.A.; Tawil, R. Expression profile of FSHD supports a link between retinal vasculopathy and muscular dystrophy. Neurology 2007, 68, 569–577. [Google Scholar] [CrossRef] [PubMed]
- Tasca, G.; Pescatori, M.; Monforte, M.; Mirabella, M.; Iannaccone, E.; Frusciante, R.; Cubeddu, T.; Laschena, F.; Ottaviani, P.; Ricci, E. Different molecular signatures in magnetic resonance imaging-staged facioscapulohumeral muscular dystrophy muscles. PLoS ONE 2012, 7, 38779. [Google Scholar] [CrossRef]
- Fitzsimons, R.B. Retinal vascular disease and the pathogenesis of facioscapulohumeral muscular dystrophy. A signalling message from Wnt? Neuromuscul. Disord. 2011, 21, 263–271. [Google Scholar] [CrossRef]
- Freiberg, F.J.; Pfau, M.; Wons, J.; Wirth, M.A.; Becker, M.D.; Michels, S. Optical coherence tomography angiography of the foveal avascular zone in diabetic retinopathy. Graefe’s Arch. Clin. Exp. Ophthalmol. 2016, 254, 1051–1058. [Google Scholar] [CrossRef] [Green Version]
- Martelli, F.; Giacomozzi, C. Tortuosity Index Calculations in Retinal Images: Some Criticalities Arising from Commonly Used Approaches. Information 2021, 2, 466. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients with FSHD (N) | 33 |
| Female (%), male (%) | 54, 46 |
| Age (years), mean (SD; range) | 50.4 (17.4; 13–76) |
| EcoRI fragment (kB), mean (SD; range) | 22.3 (6.1; 10–35) |
| CSS (0–10), median (IQR; range) | 3.5 (1; 1.5–5) |
| aCSS, median (SD; range) | 148.1 (60.9; 46.2–333.3) |
| Eyes with retinal arteries tortuosity (%) | 71 |
| Eyes with mild, moderate, severe tortuosity (%) | 26, 38, 9 |
| Tortuosity Index | Vessel Density Score | Faz Area | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Controls | Patients | Controls | Patients | Controls | Patients | ||||
| Mean ± SD | p | Mean ± SD | p | Mean ± SD | p | ||||
| Superficial Capillary Plexus | 1.15 ± 0.01 | 1.16 ± 0.01 | <0.001 | 25.40 ± 1.58 | 38.03 ± 4.32 | =0.0001 | 0.34 ± 0.13 | 0.29 ± 0.12 | =0.123, n.s.s.* |
| Deep Capillary Plexus | 1.24 ± 0.01 | 1.17 ± 0.01 | =0.05 | 29.07 ± 1.88 | 45.52 ± 2.37 | =0.0004 | 0.79 ± 0.26 | 0.40 ± 0.16 | =0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maceroni, M.; Monforte, M.; Cariola, R.; Falsini, B.; Rizzo, S.; Savastano, M.C.; Martelli, F.; Ricci, E.; Bortolani, S.; Tasca, G.; et al. Artificial Intelligence for Evaluation of Retinal Vasculopathy in Facioscapulohumeral Dystrophy Using OCT Angiography: A Case Series. Diagnostics 2023, 13, 982. https://doi.org/10.3390/diagnostics13050982
Maceroni M, Monforte M, Cariola R, Falsini B, Rizzo S, Savastano MC, Martelli F, Ricci E, Bortolani S, Tasca G, et al. Artificial Intelligence for Evaluation of Retinal Vasculopathy in Facioscapulohumeral Dystrophy Using OCT Angiography: A Case Series. Diagnostics. 2023; 13(5):982. https://doi.org/10.3390/diagnostics13050982
Chicago/Turabian StyleMaceroni, Martina, Mauro Monforte, Rossella Cariola, Benedetto Falsini, Stanislao Rizzo, Maria Cristina Savastano, Francesco Martelli, Enzo Ricci, Sara Bortolani, Giorgio Tasca, and et al. 2023. "Artificial Intelligence for Evaluation of Retinal Vasculopathy in Facioscapulohumeral Dystrophy Using OCT Angiography: A Case Series" Diagnostics 13, no. 5: 982. https://doi.org/10.3390/diagnostics13050982