
Predicting Overall Survival with Deep Learning from 18F-FDG PET-CT Images in Patients with Hepatocellular Carcinoma before Liver Transplantation

Abstract
:1. Introduction
2. Materials and Methods
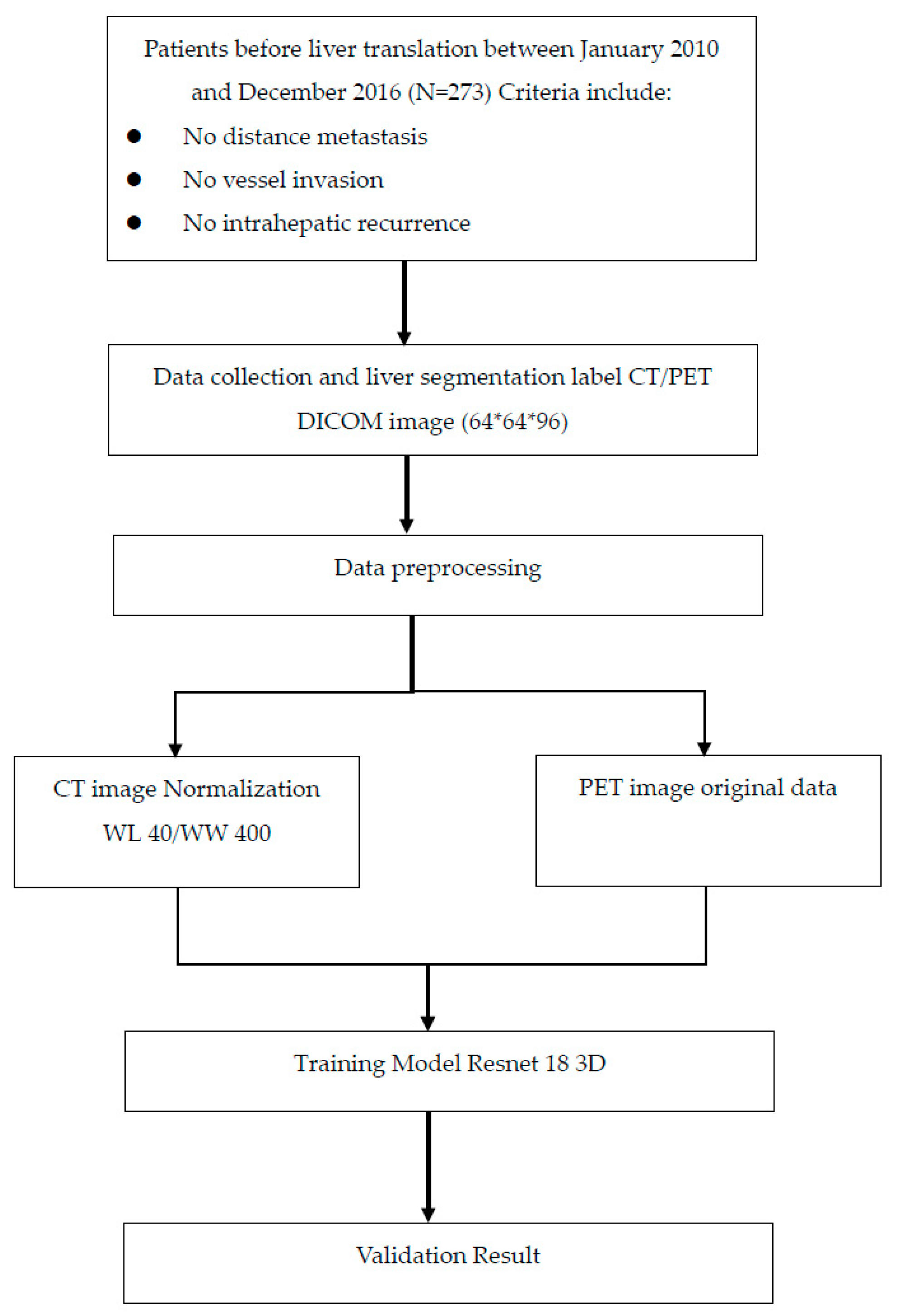
2.1. Data Source
2.2. Study Participants
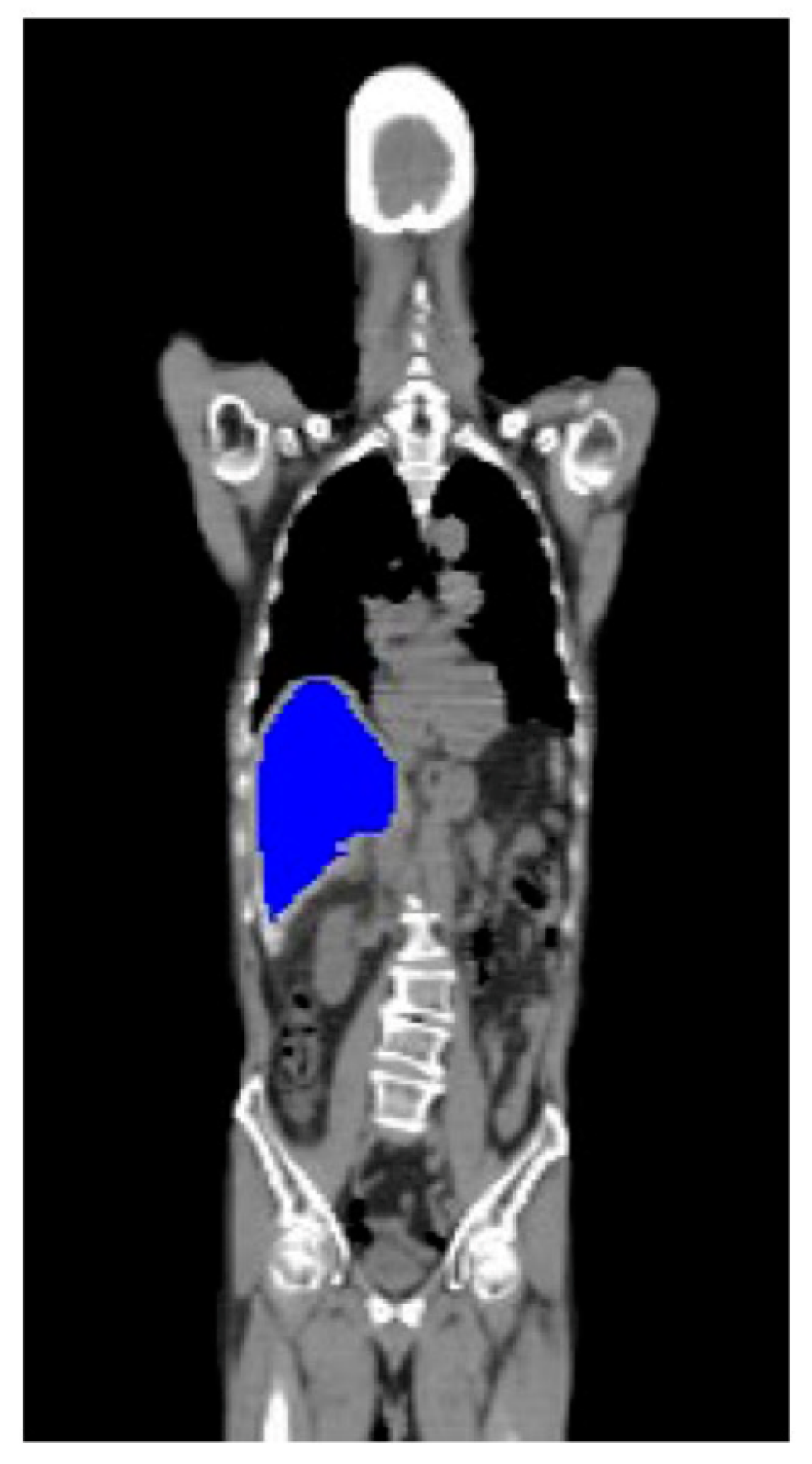
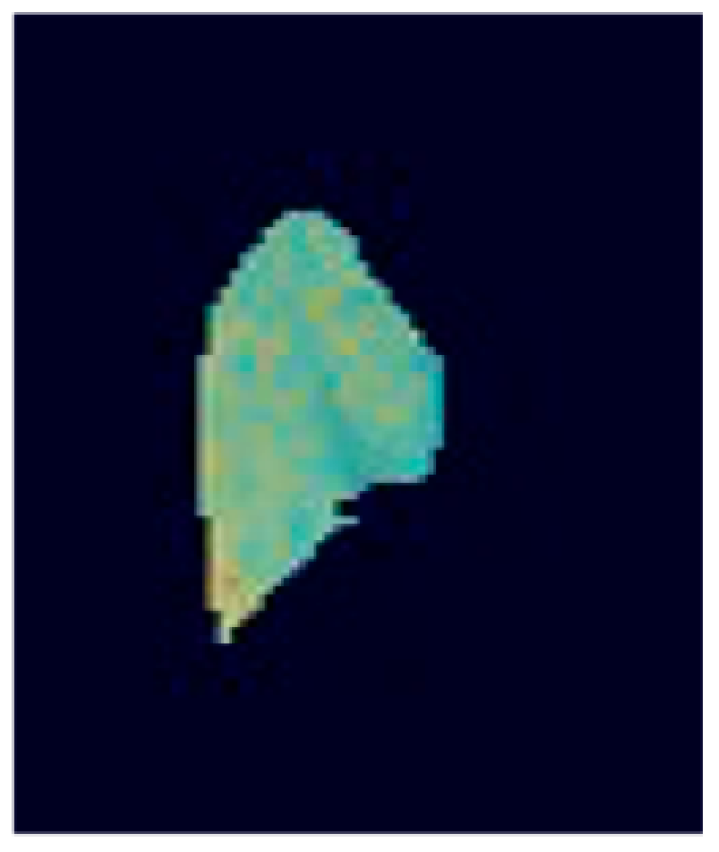
2.3. Image Preprocessing
2.4. Deep Learning Model
2.5. Statistics and Assessment Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Methods | Training Set | Multiple Endpoints | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Fold | AUC | TP | TN | FP | FN | Specificity | Sensitivity | Accuracy | |
| PET + CT | Fold 1 | 0.817 | 45 | 5 | 2 | 3 | 0.93750 | 0.71429 | 0.90909 |
| Fold 2 | 0.707 | 42 | 4 | 4 | 5 | 0.89362 | 0.50000 | 0.83636 | |
| Fold 3 | 0.851 | 45 | 4 | 4 | 2 | 0.95745 | 0.50000 | 0.89091 | |
| Fold 4 | 0.915 | 42 | 5 | 2 | 5 | 0.89362 | 0.71429 | 0.87037 | |
| Fold 5 | 0.657 | 40 | 3 | 4 | 7 | 0.85106 | 0.42857 | 0.79630 | |
| mean | 0.789 | 214 | 21 | 16 | 22 | 0.90665 | 0.57143 | 0.86061 | |
| CT | Fold 1 | 0.783 | 44 | 4 | 3 | 4 | 0.91667 | 0.57143 | 0.87273 |
| Fold 2 | 0.702 | 43 | 3 | 5 | 4 | 0.91489 | 0.37500 | 0.83636 | |
| Fold 3 | 0.840 | 46 | 4 | 4 | 1 | 0.97872 | 0.50000 | 0.90909 | |
| Fold 4 | 0.830 | 45 | 4 | 3 | 2 | 0.95745 | 0.57143 | 0.90741 | |
| Fold 5 | 0.561 | 44 | 1 | 6 | 3 | 0.93617 | 0.14286 | 0.83333 | |
| mean | 0.743 | 222 | 16 | 21 | 14 | 0.94078 | 0.43214 | 0.87179 | |
References
- El-Serag, H.B. Hepatocellular carcinoma. N. Engl. J. Med. 2011, 365, 1118–1127. [Google Scholar] [CrossRef] [PubMed]
- Parkin, D.M.; Bray, F.; Ferlay, J.; Pisani, P. Estimating the world cancer burden: Globocan 2000. Int. J. Cancer 2001, 94, 153–156. [Google Scholar] [CrossRef] [PubMed]
- Cause of Death Statistics. Available online: http://www.mohw.gov.tw/EN/Ministry/Statistic.aspx?f_list_no=474&fod_list_no=3443 (accessed on 18 June 2016).
- Cherqui, D.; Laurent, A.; Mocellin, N.; Tayar, C.; Luciani, A.; Van Nhieu, J.T.; Decaens, T.; Hurtova, M.; Memeo, R.; Mallat, A.; et al. Liver resection for transplantable hepatocellular carcinoma: Long-term survival and role of secondary liver transplantation. Ann. Surg. 2009, 250, 738–746. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL clinical practice guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heimbach, J.K.; Kulik, L.M.; Finn, R.S.; Sirlin, C.B.; Abecassis, M.M.; Roberts, L.R.; Zhu, A.X.; Murad, M.H.; Marrero, J.A. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology 2018, 67, 358–380. [Google Scholar] [CrossRef] [Green Version]
- Vitale, A.; Cucchetti, A.; Qiao, G.L.; Cescon, M.; Li, J.; Ramirez Morales, R.; Frigo, A.C.; Xia, Y.; Tuci, F.; Shen, F.; et al. Is resectable hepatocellular carcinoma a contraindication to liver transplantation? A novel decision model based on “number of patients needed to transplant” as measure of transplant benefit. J. Hepatol. 2014, 60, 1165–1171. [Google Scholar] [CrossRef]
- Clavien, P.A.; Lesurtel, M.; Bossuyt, P.M.; Gores, G.J.; Langer, B.; Perrier, A. Recommendations for liver transplantation for hepatocellular carcinoma: An international consensus conference report. Lancet Oncol. 2012, 13, e11–e22. [Google Scholar] [CrossRef] [Green Version]
- Kornberg, A.; Freesmeyer, M.; Bärthel, E.; Jandt, K.; Katenkamp, K.; Steenbeck, J.; Sappler, A.; Habrecht, O.; Gottschild, D.; Settmacher, U. 18F-FDG-uptake of hepatocellular carcinoma on PET predicts microvascular tumor invasion in liver transplant patients. Am. J. Transpl. 2009, 9, 592–600. [Google Scholar] [CrossRef]
- Kornberg, A.; Küpper, B.; Thrum, K.; Katenkamp, K.; Steenbeck, J.; Sappler, A.; Habrecht, O.; Gottschild, D. Increased 18F-FDG uptake of hepatocellular carcinoma on positron emission tomography independently predicts tumor recurrence in liver transplant patients. Transpl. Proc. 2009, 41, 2561–2563. [Google Scholar] [CrossRef] [PubMed]
- Cascales Campos, P.; Ramirez, P.; Gonzalez, R.; Febrero, B.; Pons, J.A.; Miras, M.; Sanchez Bueno, F.; Robles, R.; Parrilla, P. Value of 18-FDG-positron emission tomography/computed tomography before and after transarterial chemoembolization in patients with hepatocellular carcinoma undergoing liver transplantation: Initial results. Transpl. Proc. 2011, 43, 2213–2215. [Google Scholar] [CrossRef] [PubMed]
- Yoh, T.; Seo, S.; Ogiso, S.; Kawai, T.; Okuda, Y.; Ishii, T.; Taura, K.; Higashi, T.; Nakamoto, Y.; Hatano, E.; et al. Proposal of a new preoperative prognostic model for solitary hepatocellular carcinoma incorporating 18F-FDG-PET imaging with the ALBI grade. Ann. Surg. Oncol. 2018, 25, 542–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitamura, K.; Hatano, E.; Higashi, T.; Narita, M.; Seo, S.; Nakamoto, Y.; Yamanaka, K.; Nagata, H.; Taura, K.; Yasuchika, K.; et al. Proliferative activity in hepatocellular carcinoma is closely correlated with glucose metabolism but not angiogenesis. J. Hepatol. 2011, 55, 846–857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeng, L.B.; Changlai, S.P.; Shen, Y.Y.; Lin, C.C.; Tsai, C.H.; Kao, C.H. Limited value of 18F-2-deoxyglucose positron emission tomography to detect hepatocellular carcinoma in hepatitis B virus carriers. Hepatogastroenterology 2003, 50, 2154–2156. [Google Scholar]
- Kamaleshwaran, K.K.; Kashyap, R.; Bhattacharya, A.; Mittal, B.R. Solitary sternal metastasis from hepatocellular carcinoma detected by F-18 FDG PET/CT. Indian J. Nucl. Med. 2013, 28, 28–29. [Google Scholar] [PubMed] [Green Version]
- Trojan, J.; Schroeder, O.; Raedle, J.; Baum, R.P.; Herrmann, G.; Jacobi, V.; Zeuzem, S. Fluorine-18 FDG positron emission tomography for imaging of hepatocellular carcinoma. Am. J. Gastroenterol. 1999, 94, 3314–3319. [Google Scholar] [CrossRef]
- Lin, C.Y.; Chen, J.H.; Liang, J.A.; Lin, C.C.; Jeng, L.B.; Kao, C.H. 18F-FDG PETor PET/CT for detecting extra-hepatic metastases or recurrent hepatocellular carcinoma: A systematic review and meta-analysis. Eur. J. Radiol. 2012, 81, 2417–2422. [Google Scholar] [CrossRef]
- Lee, J.W.; Paeng, J.C.; Kang, K.W.; Kwon, H.W.; Suh, K.S.; Chung, J.K.; Lee, M.C.; Lee, D.S. Prediction of tumor recurrence by 18F-FDG PET in liver transplantation for hepatocellular carcinoma. J. Nucl. Med. 2009, 50, 682–687. [Google Scholar] [CrossRef] [Green Version]
- Anderson, G.S.; Brinkmann, F.; Soulen, M.C.; Alavi, A.; Zhuang, H. FDG positron emission tomography in the surveillance of hepatic tumors treated with radiofrequency ablation. Clin. Nucl. Med. 2003, 28, 192–197. [Google Scholar] [CrossRef]
- Hatano, E.; Ikai, I.; Higashi, T.; Teramukai, S.; Torizuka, T.; Saga, T.; Fujii, H.; Shimahara, Y. Preoperative positron emission tomography with fluorine-18-fluorodeoxyglucose is predictive of prognosis in patients with hepatocellular carcinoma after resection. World J. Surg. 2006, 30, 1736–1741. [Google Scholar] [CrossRef]
- Higashi, T.; Hatano, E.; Ikai, I.; Nishii, R.; Nakamoto, Y.; Ishizu, K.; Suga, T.; Kawashima, H.; Togashi, K.; Seo, S.; et al. FDG PET as a prognostic predictor in the early post-therapeutic evaluation for unresectable hepatocellular carcinoma. Eur. J. Nucl. Med. Mol. Imaging 2010, 37, 468–482. [Google Scholar] [CrossRef]
- Büchler, P.; Krause, B.; Witt, U.; Gottschild, D.; Friess, H. Patients with non-[18F] fludeoxyglucose-avid advanced hepatocellular carcinoma on clinical staging may achieve long-term recurrence-free survival after liver transplantation. Liver Transpl. 2012, 18, 53–61. [Google Scholar]
- Hou, J.; Jia, X.; Xie, Y.; Qin, W. Integrative Histology-Genomic Analysis Predicts Hepatocellular Carcinoma Prognosis Using Deep Learning. Genes 2022, 13, 1770. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Zhou, K.; Wang, Z.; Xiao, R. Generative Consistency for Semi-Supervised Cerebrovascular Segmentation from TOF-MRA. IEEE Trans. Med. Imaging, 2022; 42, 346–353, online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Welker, M.W.; Bechstein, W.O.; Zeuzem, S.; Trojan, J. Recurrent hepatocellular carcinoma after liver transplantation—An emerging clinical challenge. Transpl. Int. 2013, 26, 109–118. [Google Scholar] [CrossRef]
- Sotiropoulos, G.C.; Molmenti, E.P.; Lösch, C.; Beckebaum, S.; Broelsch, C.E.; Lang, H. Meta-analysis of tumor recurrence after liver transplantation for hepatocellular carcinoma based on 1198 cases. Eur. J. Med. Res. 2007, 12, 527–534. [Google Scholar]
- Rodríguez-Perálvarez, M.; Luong, T.V.; Andreana, L.; Meyer, T.; Dhillon, A.P.; Burroughs, A.K. A systematic review of microvascular invasion in hepatocellular carcinoma: Diagnostic and prognostic variability. Ann. Surg. Oncol. 2013, 20, 325–339. [Google Scholar] [CrossRef]
- Verna, E.C.; Patel, Y.A.; Aggarwal, A.; Desai, A.P.; Frenette, C.; Pillai, A.A.; Salgia, R.; Seetharam, A.; Sharma, P.; Sherman, C.; et al. Liver transplantation for hepatocellular carcinoma: Management after the transplant. Am. J. Transpl. 2020, 20, 333–347. [Google Scholar] [CrossRef]
- Liang, W.; Wu, L.; Ling, X.; Schroder, P.M.; Ju, W.; Wang, D.; Shang, Y.; Kong, Y.; Guo, Z.; He, X. Living donor liver transplantation versus deceased donor liver transplantation for hepatocellular carcinoma: A meta-analysis. Liver Transpl. 2012, 18, 1226–1236. [Google Scholar] [CrossRef]
- Goldaracena, N.; Gorgen, A.; Doyle, A.; Hansen, B.E.; Tomiyama, K.; Zhang, W.; Ghanekar, A.; Lilly, L.; Cattral, M.; Galvin, Z.; et al. Live donor liver transplantation for patients with hepatocellular carcinoma offers increased survival vs. deceased donation. J. Hepatol. 2019, 70, 666–673. [Google Scholar] [CrossRef]
- Fernandez-Sevilla, E.; Allard, M.A.; Selten, J.; Golse, N.; Vibert, E.; Sa Cunha, A.; Cherqui, D.; Castaing, D.; Adam, R. Recurrence of hepatocellular carcinoma after liver transplantation: Is there a place for resection? Liver Transpl. 2017, 23, 440–447. [Google Scholar] [CrossRef] [Green Version]
- Ho, C.M.; Lee, C.H.; Lee, M.C.; Zhang, J.F.; Chen, C.H.; Wang, J.Y.; Hu, R.H.; Lee, P.H. Survival After Treatable Hepatocellular Carcinoma Recurrence in Liver Recipients: A Nationwide Cohort Analysis. Front. Oncol. 2021, 10, 616094. [Google Scholar] [CrossRef]
- De’Angelis, N.; Landi, F.; Carra, M.C.; Azoulay, D. Managements of recurrent hepatocellular carcinoma after liver transplantation: A systematic review. World J. Gastroenterol. 2015, 21, 11185–11198. [Google Scholar] [CrossRef]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [Green Version]
- Potdar, K.; Pardawala, T.S.; Pai, C.D. A Comparative Study of Categorical Variable Encoding Techniques for Neural Network Classifiers. Int. J. Comput. Appl. 2017, 175, 7–9. [Google Scholar] [CrossRef]
- van Timmeren, J.E.; Cester, D.; Tanadini-Lang, S.; Alkadhi, H.; Baessler, B. Radiomics in medical imaging—"how-to guide and critical reflection. Insights Imaging 2020, 11, 91. [Google Scholar] [CrossRef]
- Puttagunta, M.; Ravi, S. Medical image analysis based on deep learning approach. Multimed. Tools Appl. 2021, 80, 24365–24398. [Google Scholar] [CrossRef]
- Conrad, G.R.; Sinha, P. Narrow time-window dual-point 18F-FDG PET for the diagnosis of thoracic malignancy. Nucl. Med. Commun. 2003, 24, 1129–1137. [Google Scholar] [CrossRef] [PubMed]
- Schillaci, O.; Travascio, L.; Bolacchi, F.; Calabria, F.; Bruni, C.; Cicciò, C.; Guazzaroni, M.; Orlacchio, A.; Simonetti, G. Accuracy of early and delayed FDG PET-CT and of contrast-enhanced CT in the evaluation of lung nodules: A preliminary study on 30 patients. Radiol. Med. 2009, 114, 890–906. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.M.; Huang, G.; Sun, X.G.; Liu, J.J.; Chen, T.; Shi, Y.P.; Wan, L.R. Optimizing delayed scan time for FDG PET: Comparison of the early and late delayed scan. Nucl. Med. Commun. 2008, 29, 425–430. [Google Scholar] [CrossRef]
- Fiz, F.; Masci, C.; Costa, G.; Sollini, M.; Chiti, A.; Ieva, F.; Torzilli, G.; Viganò, L. PET/CT-based radiomics of mass-forming intrahepatic cholangiocarcinoma improves prediction of pathology data and survival. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 3387–3400. [Google Scholar] [CrossRef]
- Haider, S.; Danish, M.S.; Sharma, R. Assessing energy efficiency of Indian paper industry and influencing factors: A slack-based firm-level analysis. Energy Econ. 2019, 81, 454–464. [Google Scholar] [CrossRef]
- Mirmozaffari, M.; Yazdani, M.; Boskabadi, A.; Dolatsara, H.A.; Kabirifar, K.; Golilarz, N.A. A novel machine learning approach combined with optimization models for eco-efficiency evaluation. Appl. Sci. 2020, 10, 5210. [Google Scholar] [CrossRef]
- Fartoux, L.; Decaens, T. Contribution of biomarkers and imaging in the management of hepatocellular carcinoma. Clin. Res. Hepatol. Gastroenterol. 2011, 35, S21–S30. [Google Scholar] [CrossRef] [PubMed]
- Mirpouya, M.; Elham, S.; Mohammad, K.S.; Kamyar, K.; Reza, Y.; Tayyebeh, A.G. A novel artificial intelligent approach: Comparison of machine learning tools and algorithms based on optimization DEA Malmquist productivity index for eco-efficiency evaluation. Int. J. Energy Sect. Manag. 2021, 15, 523–550. [Google Scholar]
- Mirza-Aghazadeh-Attari, M.; Ambale Venkatesh, B.; Aliyari Ghasabeh, M.; Mohseni, A.; Madani, S.P.; Borhani, A.; Shahbazian, H.; Ansari, G.; Kamel, I.R. The Additive Value of Radiomics Features Extracted from Baseline MR Images to the Barcelona Clinic Liver Cancer (BCLC) Staging System in Predicting Transplant-Free Survival in Patients with Hepatocellular Carcinoma: A Single-Center Retrospective Analysis. Diagnostics 2023, 13, 552. [Google Scholar] [CrossRef]
- Mirmozaffari, M.; Shadkam, E.; Khalili, S.M.; Yazdani, M. Developing a novel integrated generalised data envelopment analysis (DEA) to evaluate hospitals providing stroke care services. Bioengineering 2021, 8, 207. [Google Scholar] [CrossRef]
- Mirmozaffari, M.; Yazdani, R.; Shadkam, E.; Khalili, S.M.; Tavassoli, L.S.; Boskabadi, A. A novel hybrid parametric and non-parametric optimisation model for average technical efficiency assessment in public hospitals during and post-COVID-19 pandemic. Bioengineering 2021, 9, 7. [Google Scholar] [CrossRef]
- Lisson, C.S.; Lisson, C.G.; Mezger, M.F.; Wolf, D.; Schmidt, S.A.; Thaiss, W.M.; Tausch, E.; Beer, A.J.; Stilgenbauer, S.; Beer, M.; et al. Deep neural networks and machine learning radiomics modelling for prediction of relapse in mantle cell lymphoma. Cancers 2022, 14, 2008. [Google Scholar] [CrossRef]
- Mirmozaffari, M.; Yazdani, R.; Shadkam, E.; Khalili, S.M.; Mahjoob, M.; Boskabadi, A. An integrated artificial intelligence model for efficiency assessment in pharmaceutical companies during the COVID-19 pandemic. Sustain. Oper. Comput. 2022, 3, 156–167. [Google Scholar] [CrossRef]
- Ripani, D.; Caldarella, C.; Za, T.; Rossi, E.; De Stefano, V.; Giordano, A. Progression to Symptomatic Multiple Myeloma Predicted by Texture Analysis-Derived Parameters in Patients Without Focal Disease at 18F-FDG PET/CT. Clin. Lymphoma Myeloma Leuk. 2021, 21, 536–544. [Google Scholar] [CrossRef]
- Mirmozaffari, M.; Yazdani, R.; Shadkam, E.; Tavassoli, L.S.; Massah, R. VCS and CVS: New combined parametric and non-parametric operation research models. Sustain. Oper. Comput. 2021, 2, 36–56. [Google Scholar] [CrossRef]
- Bowen, S.R.; Chapman, T.R.; Borgman, J.; Miyaoka, R.S.; Kinahan, P.E.; Liou, I.W.; Sandison, G.A.; Vesselle, H.J.; Nyflot, M.J.; Apisarnthanarax, S. Measuring total liver function on sulfur colloid SPECT/CT for improved risk stratification and outcome prediction of hepatocellular carcinoma patients. EJNMMI Res. 2016, 6, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Xu, X.; Weng, S.; Yan, C.; Chen, J.; Ye, R. CT image-based texture analysis to predict microvascular invasion in primary hepatocellular carcinoma. J. Digit. Imaging 2020, 33, 1365–1375. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.C.; Chen, C.L.; Wang, C.C.; Lin, C.C.; Yong, C.C.; Wang, S.H.; Liu, Y.W.; Lin, T.L.; Lee, W.F.; Lin, Y.H.; et al. Combination of FDG-PET and UCSF Criteria for Predicting HCC Recurrence After Living Donor Liver Transplantation. Transplantation 2016, 100, 1925–1932. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.D.; Kim, S.H.; Kim, Y.K.; Kim, C.; Kim, S.K.; Han, S.S.; Park, S.J. (18)F-FDG-PET/CT predicts early tumor recurrence in living donor liver transplantation for hepatocellular carcinoma. Transpl. Int. 2013, 26, 50–60. [Google Scholar] [CrossRef]
- Ludemann, L.; Grieger, W.; Wurm, R.; Wust, P.; Zimmer, C. Glioma assessment using quantitative blood volume maps generated by T1-weighted dynamic contrast-enhanced magnetic resonance imaging: A receiver operating characteristic study. Acta Radiol. 2006, 47, 303–310. [Google Scholar] [CrossRef]
- Obuchowski, N.A. Receiver operating characteristic curves and their use in radiology. Radiology 2003, 229, 3–8. [Google Scholar] [CrossRef]
- Metz, C.E. Basic principles of ROC analysis. Semin Nucl. Med. 1978, 8, 283–298. [Google Scholar] [CrossRef]
- Schraiber, L.D.S.; de Mattos, A.A.; Zanotelli, M.L.; Cantisani, G.P.C.; Brandão, A.B.M.; Marroni, C.A.; Kiss, G.; Ernani, L.; Marcon, P.D.S. Alpha-fetoprotein Level Predicts Recurrence After Transplantation in Hepatocellular Carcinoma. Medicine 2016, 95, e2478. [Google Scholar] [CrossRef]
- Takada, Y.; Kaido, T.; Shirabe, K.; Nagano, H.; Egawa, H.; Sugawara, Y.; Taketomi, A.; Takahara, T.; Wakabayashi, G.; Nakanishi, C.; et al. LTx-PET study group of the Japanese Society of Hepato-Biliary-Pancreatic Surgery and the Japanese Liver Transplantation Society. Significance of preoperative fluorodeoxyglucose-positron emission tomography in prediction of tumor recurrence after liver transplantation for hepatocellular carcinoma patients: A Japanese multicenter study. J. Hepatobiliary Pancreat Sci. 2017, 24, 49–57. [Google Scholar]
- McHugh, P.P.; Gilbert, J.; Vera, S.; Koch, A.; Ranjan, D.; Gedaly, R. Alpha-fetoprotein and tumour size are associated with microvascular invasion in explanted livers of patients undergoing transplantation with hepatocellular carcinoma. HPB 2010, 12, 56–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]

| Total | |
|---|---|
| n = 273 | |
| Age (years, mean ± SD) | 55.773 ± 8.138 |
| Gender | |
| Male | 212 (77.7) |
| Female | 61 (22.3) |
| BCLC Classification | |
| 0 | 1 (0.4) |
| A | 119 (43.6) |
| B | 89 (32.6) |
| C | 40 (14.7) |
| D | 24 (8.8) |
| Milan criteria | |
| within | 127 (46.5) |
| beyond | 146 (53.5) |
| UCSF criteria | |
| within | 147 (53.8) |
| beyond | 126 (46.2) |
| CLIP Score | |
| 0 | 61 (22.3) |
| 1 | 105 (38.5) |
| 2 | 48 (17.6) |
| 3 | 37 (13.6) |
| 4 | 17 (6.2) |
| >4 | 5 (1.8) |
| Child–Pugh Classification | |
| Stage A | 167 (61.2) |
| Stage B | 81 (29.7) |
| Stage C | 25 (9.2) |
| Okuda staging system | |
| Ⅰ | 162 (59.3) |
| Ⅱ | 91 (33.3) |
| Ⅲ | 20 (7.3) |
| MELD Score | |
| <10 | 134 (49.1) |
| 10–19 | 96 (35.2) |
| 20–29 | 35 (12.8) |
| 30–39 | 6 (2.2) |
| >39 | 2 (0.7) |
| Pretransplant AFP, ng/mL | |
| <20 | 139 (50.9) |
| 20–200 | 74 (27.1) |
| >200 | 60 (22.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, Y.-C.; Wu, K.-C.; Chang, C.-J.; Chen, Y.-J.; Wang, K.-P.; Jeng, L.-B.; Kao, C.-H. Predicting Overall Survival with Deep Learning from 18F-FDG PET-CT Images in Patients with Hepatocellular Carcinoma before Liver Transplantation. Diagnostics 2023, 13, 981. https://doi.org/10.3390/diagnostics13050981
Lai Y-C, Wu K-C, Chang C-J, Chen Y-J, Wang K-P, Jeng L-B, Kao C-H. Predicting Overall Survival with Deep Learning from 18F-FDG PET-CT Images in Patients with Hepatocellular Carcinoma before Liver Transplantation. Diagnostics. 2023; 13(5):981. https://doi.org/10.3390/diagnostics13050981
Chicago/Turabian StyleLai, Yung-Chi, Kuo-Chen Wu, Chao-Jen Chang, Yi-Jin Chen, Kuan-Pin Wang, Long-Bin Jeng, and Chia-Hung Kao. 2023. "Predicting Overall Survival with Deep Learning from 18F-FDG PET-CT Images in Patients with Hepatocellular Carcinoma before Liver Transplantation" Diagnostics 13, no. 5: 981. https://doi.org/10.3390/diagnostics13050981