
Recent Advances in Ultrasound Breast Imaging: From Industry to Clinical Practice
 , , , , , and
, , , , , and 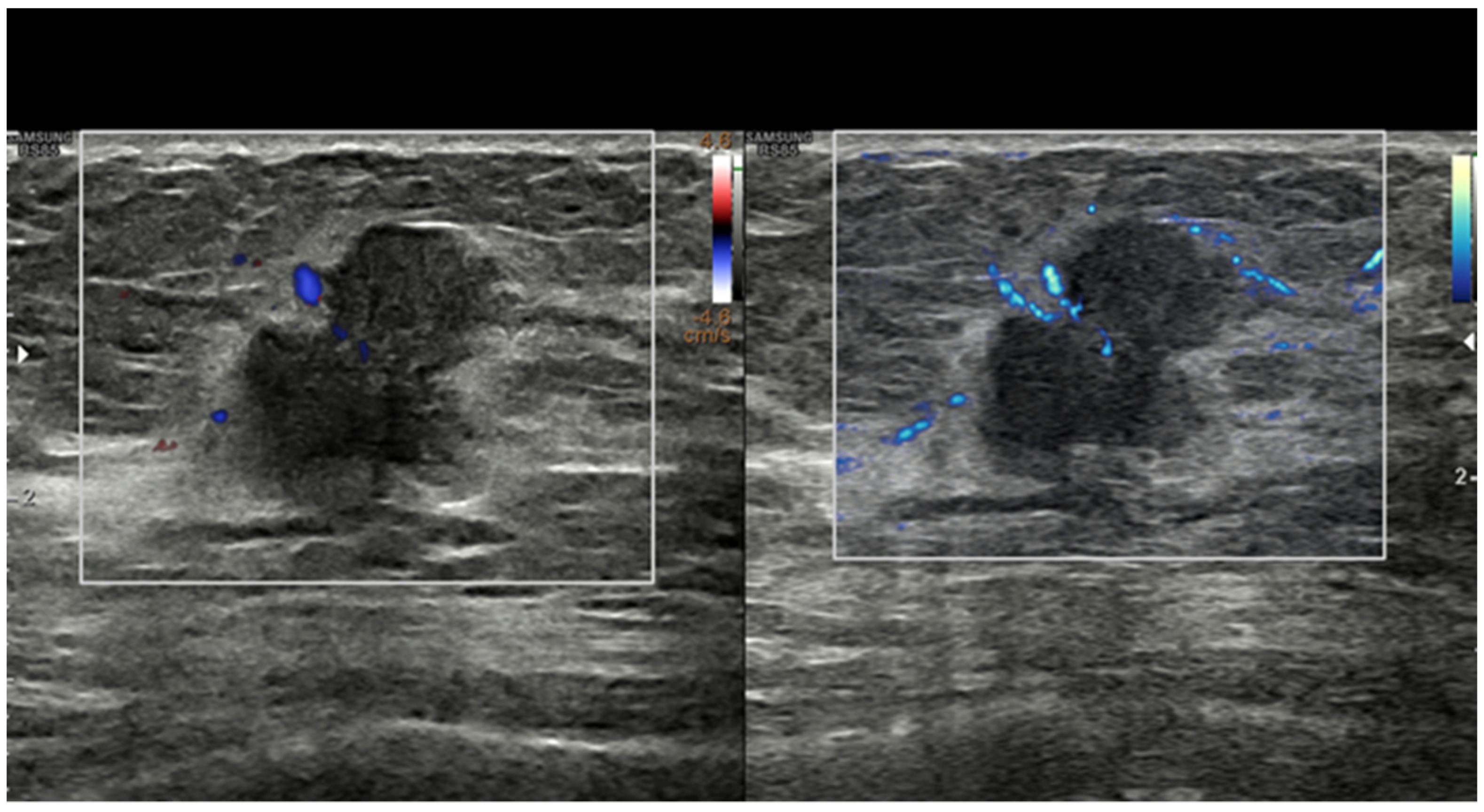{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction—Where Do We Come from?
2. Technological Developments—What the Industry Has Made Available to Us
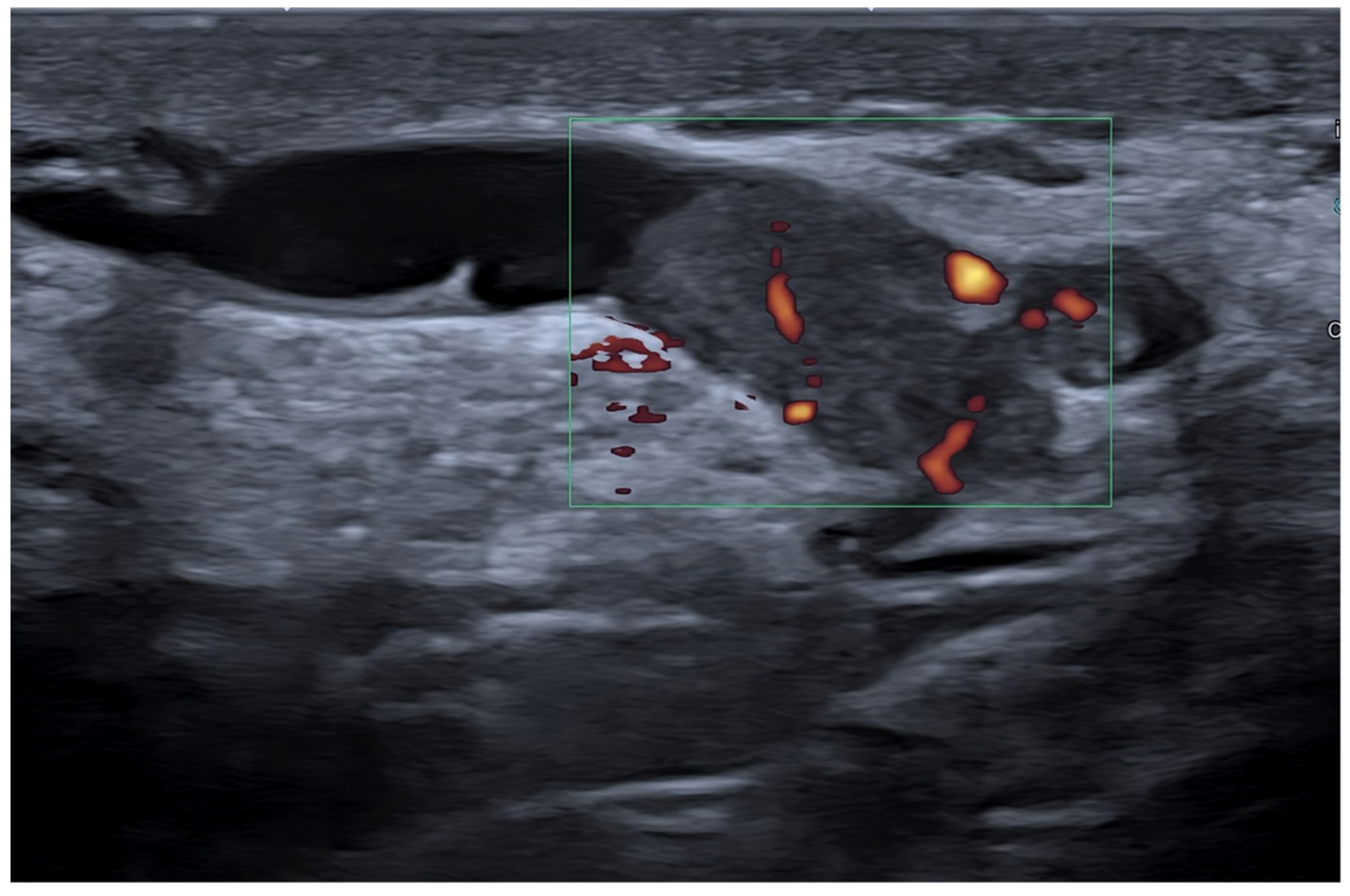
2.1. Conventional Doppler Techniques and New Microvasculature Imaging Techniques
2.2. High-Frequency Transducers
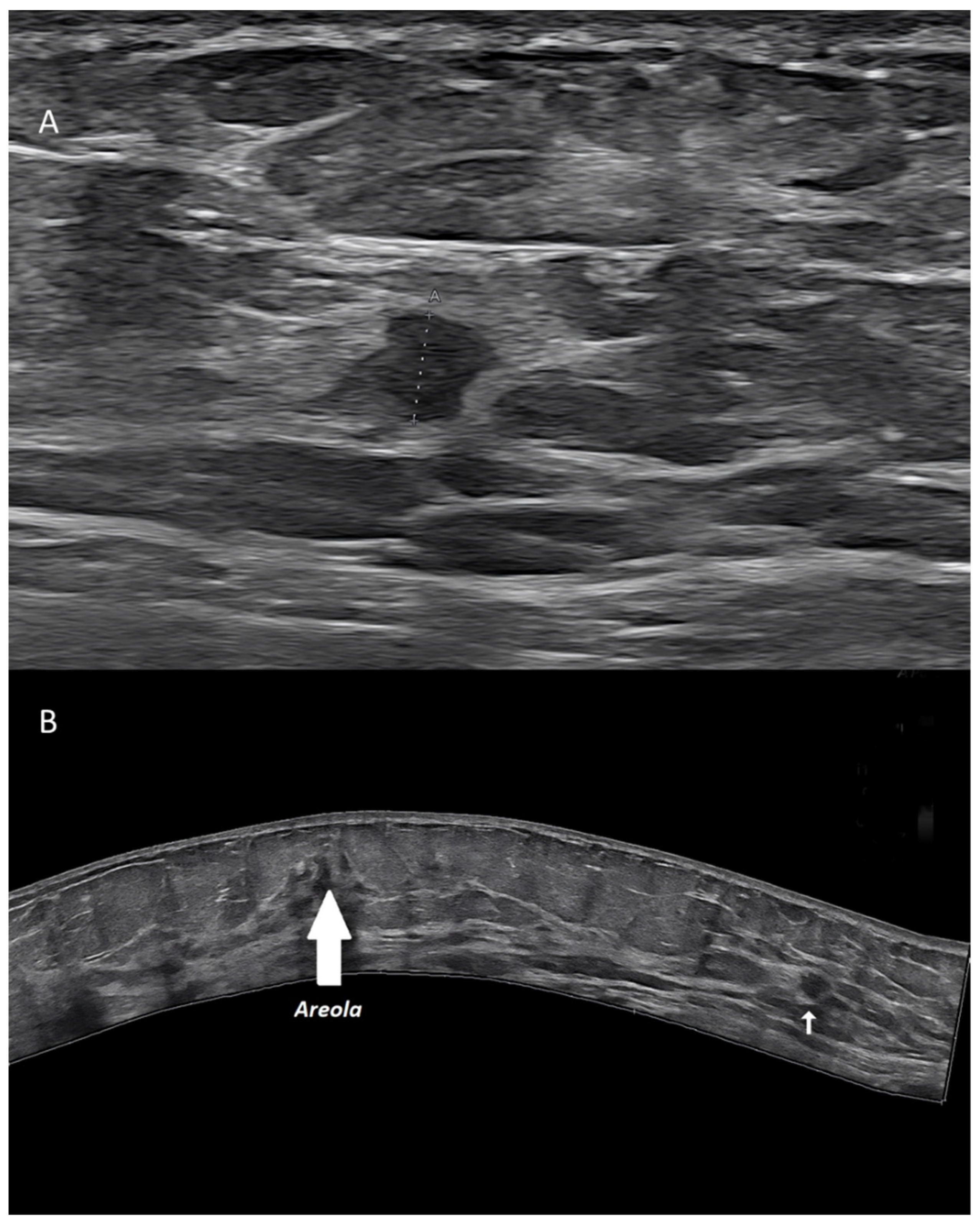
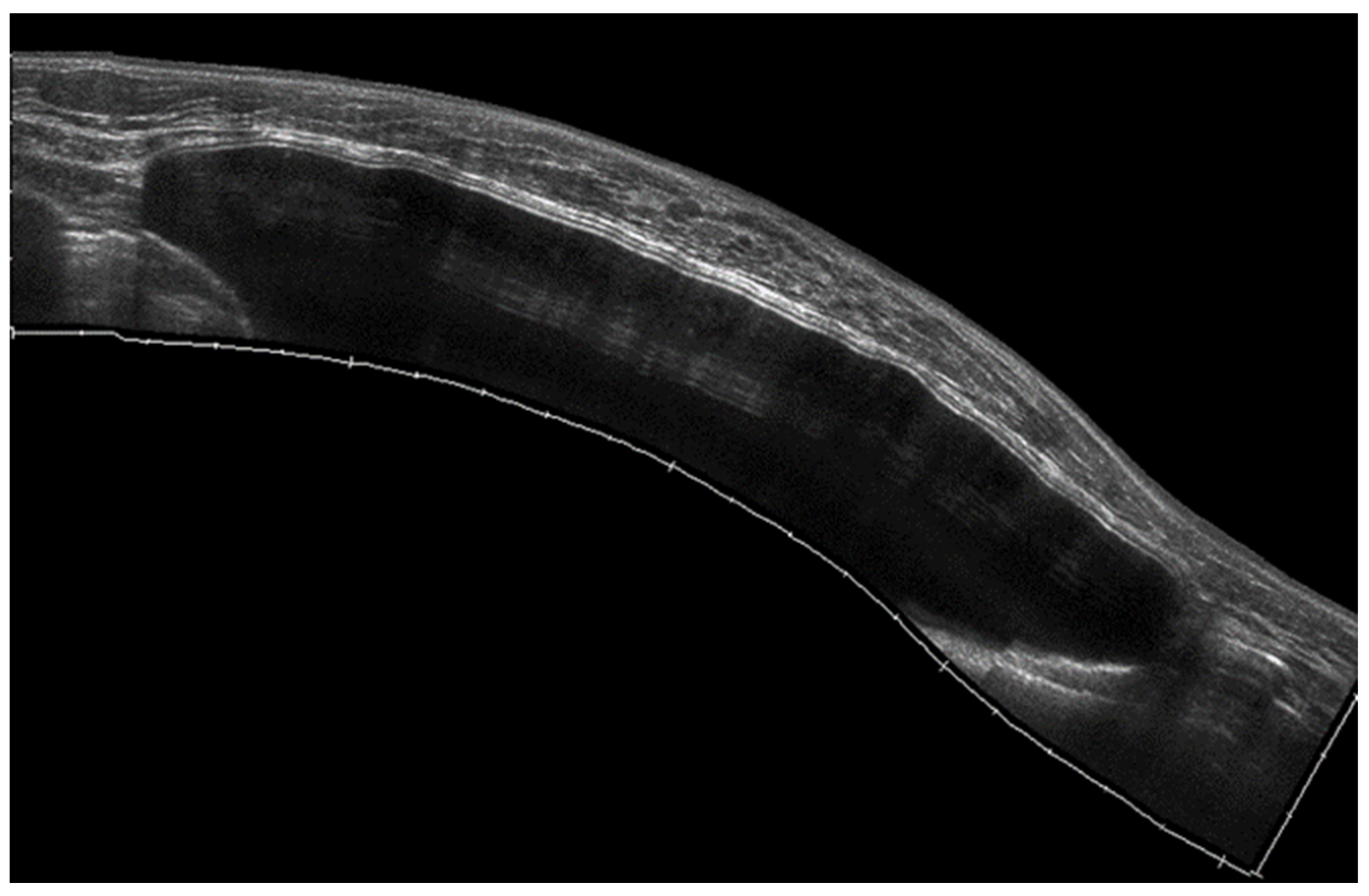
2.3. Extended Field-of-View Scanning
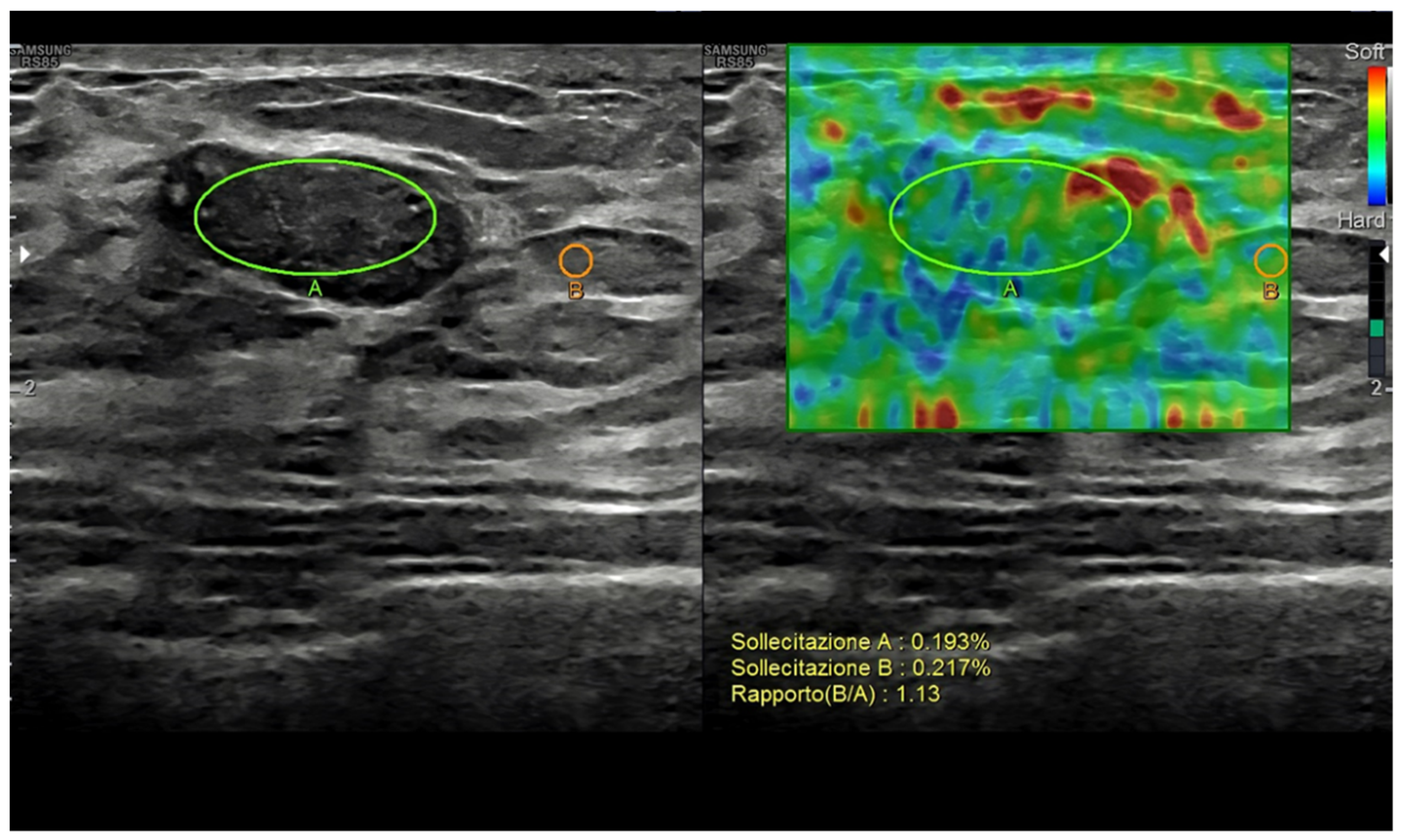
2.4. Elastography
2.5. Contrast-Enhanced Ultrasound
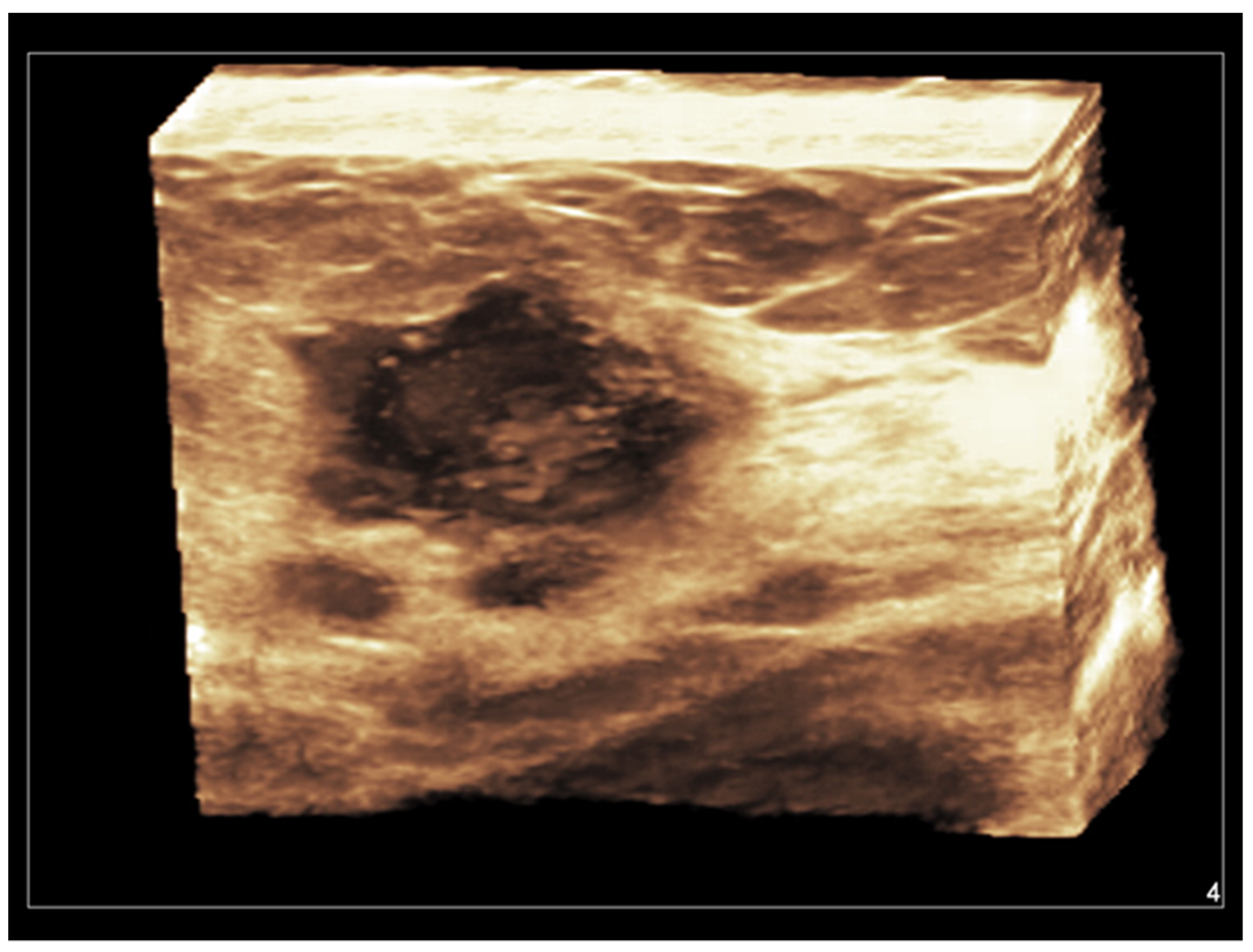
2.6. Three-Dimensional Ultrasound
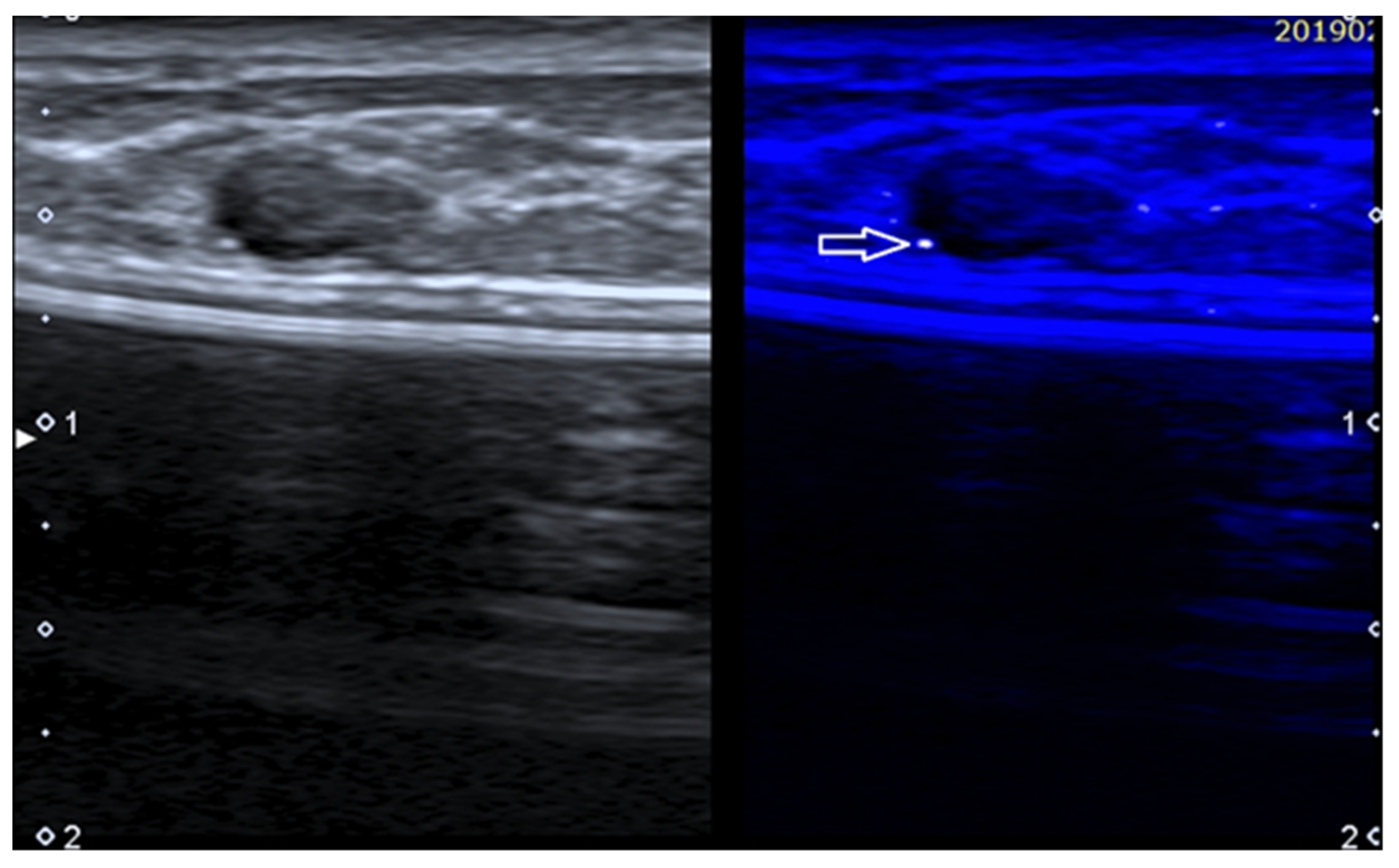
2.7. MicroPure
2.8. Automated Breast Ultrasound
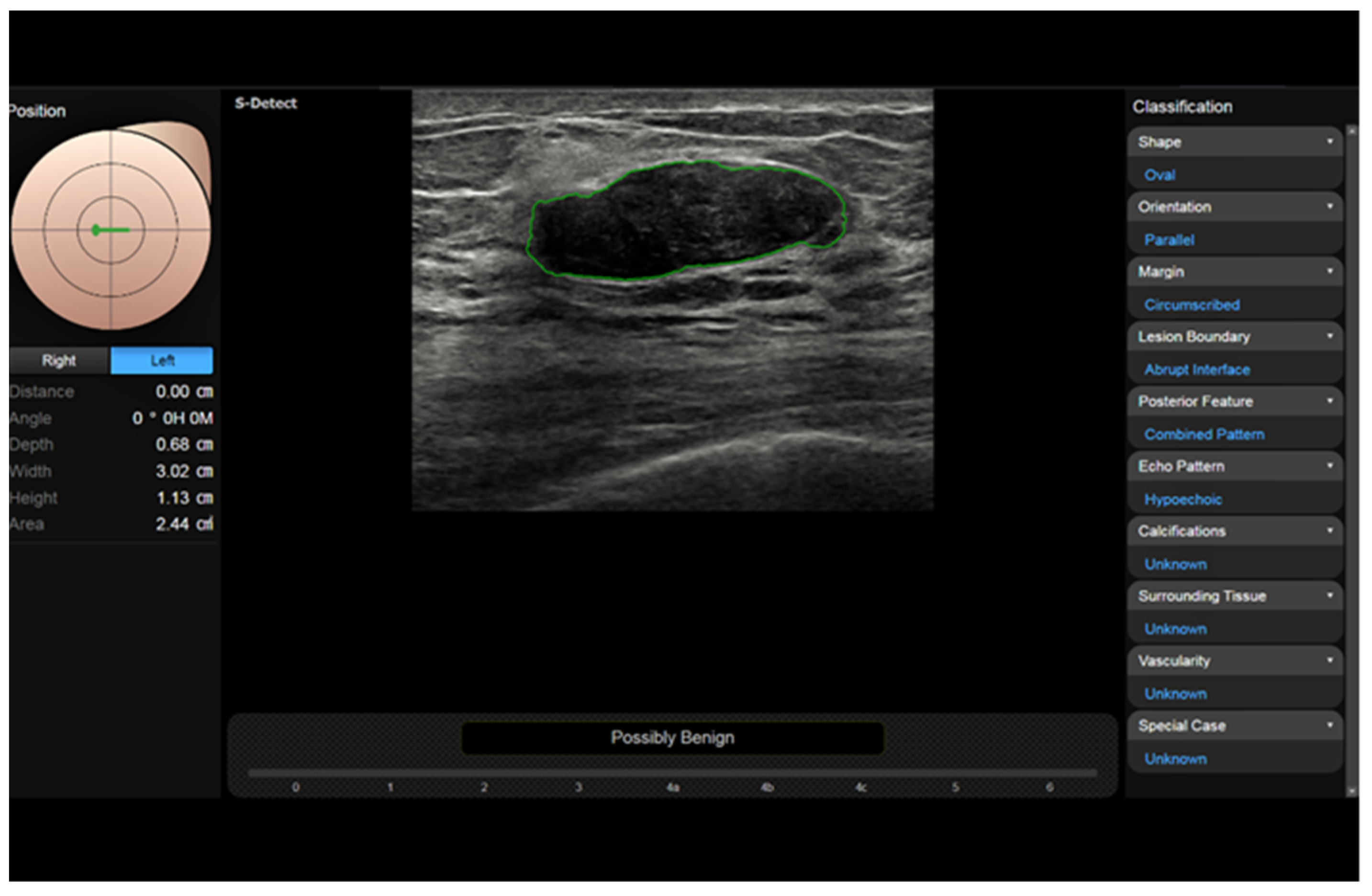
2.9. Computer-Assisted Diagnosis—S-Detect
2.10. Ultrasound Nomograms
2.11. Images Fusion and Virtual Navigation
3. Changing Clinical Scenarios—The Current Impact of US in Breast Practice
3.1. Primary Ultrasound
3.2. Complementary Ultrasound
3.3. Second-Look Ultrasound
4. Conclusions—Not Everything That Glitters Is Gold
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dodd, G.D. Present status of thermography, ultrasound and mammography in breast cancer detection. Cancer 1977, 39, 2796–2805. [Google Scholar] [CrossRef]
- Sickles, E.A.; Filly, R.A.; Callen, P.W. Breast cancer detection with sonography and mammography: Comparison using state-of-the-art equipment. Am. J. Roentgenol. 1983, 140, 843–845. [Google Scholar] [CrossRef]
- Dempsey, P.J. The History of Breast Ultrasound. J. Ultrasound Med. 2004, 23, 887–894. [Google Scholar] [CrossRef]
- Agarwal, M.; van der Pol, C.B.; Patlas, M.N.; Udare, A.; Chung, A.D.; Rubino, J. Optimizing the radiologist work environment: Actionable tips to improve workplace satisfaction, efficiency, and minimize burnout. Radiol. Med. 2021, 126, 1255–1257. [Google Scholar] [CrossRef] [PubMed]
- Albano, D.; Stecco, A.; Micci, G.; Sconfienza, L.M.; Colagrande, S.; Reginelli, A.; Grassi, R.; Carriero, A.; Midiri, M.; Lagalla, R.; et al. Whole-body magnetic resonance imaging (WB-MRI) in oncology: An Italian survey. Radiol. Med. 2020, 126, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.A.; Samy, M.; Ali, A.M.; Hassan, R.A. Architectural distortion outcome: Digital breast tomosynthesis-detected versus digital mammography-detected. Radiol. Med. 2021, 127, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Argalia, G.; Ventura, C.; Tosi, N.; Campioni, D.; Tagliati, C.; Tufillaro, M.; Cucco, M.; Svegliati Baroni, G.; Giovagnoni, A. Comparison of point shear wave elastography and transient elastography in the evaluation of patients with NAFLD. Radiol. Med. 2022, 127, 571–576. [Google Scholar] [CrossRef]
- Argalia, G.; Tarantino, G.; Ventura, C.; Campioni, D.; Tagliati, C.; Guardati, P.; Kostandini, A.; Marzioni, M.; Giuseppetti, G.M.; Giovagnoni, A. Shear wave elastography and transient elastography in HCV patients after direct-acting antivirals. Radiol. Med. 2021, 126, 894–899. [Google Scholar] [CrossRef] [PubMed]
- Grani, G.; Lamartina, L.; Biffoni, M.; Giacomelli, L.; Maranghi, M.; Falcone, R.; Ramundo, V.; Cantisani, V.; Filetti, S.; Durante, C. Sonographically Estimated Risks of Malignancy for Thyroid Nodules Computed with Five Standard Classification Systems: Changes over Time and Their Relation to Malignancy. Thyroid 2018, 28, 1190–1197. [Google Scholar] [CrossRef]
- American College of Radiology ACR-BI-RADS-Ultrasound. ACR Breast Imaging Reporting and Data System, Breast Imaging Atlas; American College of Radiology: Reston, VA, USA, 2003. [Google Scholar]
- Hooley, R.J.; Scoutt, L.M.; Philpotts, L.E. Breast ultrasonography: State of the art. Radiology 2013, 268, 642–659. [Google Scholar] [CrossRef]
- Brizi, M.G.; Perillo, F.; Cannone, F.; Tuzza, L.; Manfredi, R. The role of imaging in acute pancreatitis. Radiol. Med. 2021, 126, 1017–1029. [Google Scholar] [CrossRef] [PubMed]
- Catalano, O.; Wortsman, X. Dermatology ultrasound. imaging technique, tips and tricks, high-resolution anatomy. Ultrasound Q. 2020, 36, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Catalano, O.; Varelli, C.; Sbordone, C.; Corvino, A.; De Rosa, D.; Vallone, G.; Wortsman, X. A bump: What to do next? ultrasound imaging of superficial soft-tissue palpable lesions. J. Ultrasound 2020, 23, 287–300. [Google Scholar] [CrossRef]
- Catalano, O.; Mattace Raso, M.; D’Aiuto, M.; Illiano, L.A.; Saturnino, P.P.; Siani, A. Additional role of colour Doppler ultrasound imaging in intracystic breast tumours. Radiol. Med. 2009, 114, 253–266. [Google Scholar] [CrossRef] [PubMed]
- Chang, R.F.; Huang, S.F.; Moon, W.K.; Lee, Y.H.; Chen, D.R. Solid Breast Masses: Neural Network Analysis of Vascular Features at Three-dimensional Power Doppler US for Benign or Malignant Classification. Radiology 2007, 243, 56–62. [Google Scholar] [CrossRef] [Green Version]
- Chiti, G.; Grazzini, G.; Flammia, F.; Matteuzzi, B.; Tortoli, P.; Bettarini, S.; Pasqualini, E.; Granata, V.; Busoni, S.; Messserini, L.; et al. Gastroenteropancreatic neuroendocrine neoplasms (GEP-NENs): A radiomic model to predict tumor grade. Radiol. Med. 2022, 127, 928–938. [Google Scholar] [CrossRef]
- Di Serafino, M.; Vallone, G. The role of point of care ultrasound in radiology department: Update and prospective. A statement of Italian college ultrasound. Radiol. Med. 2021, 126, 636–641. [Google Scholar] [CrossRef]
- Horvath, E.; Cuitiño, M.J.; Pinochet, M.A.; Sanhueza, P. Color Doppler in the study of the breast: How do we perform it? Rev. Chil. Radiol. 2011, 17, 19–27. [Google Scholar]
- Granata, V.; Simonetti, I.; Fusco, R.; Setola, S.V.; Izzo, F.; Scarpato, L.; Vanella, V.; Festino, L.; Simeone, E.; Ascierto, P.A.; et al. Management of cutaneous melanoma: Radiologists challenging and risk assessment. Radiol. Med. 2022, 127, 899–911. [Google Scholar] [CrossRef]
- Granata, V.; Faggioni, L.; Grassi, R.; Fusco, R.; Reginelli, A.; Rega, D.; Maggialetti, N.; Buccicardi, D.; Frittoli, B.; Rengo, M.; et al. Structured reporting of computed tomography in the staging of colon cancer: A Delphi consensus proposal. Radiol. Med. 2022, 127, 21–29. [Google Scholar] [CrossRef]
- Granata, V.; Grassi, R.; Fusco, R.; Setola, S.V.; Belli, A.; Ottaiano, A.; Nasti, G.; La Porta, M.; Danti, G.; Cappabianca, S.; et al. Intrahepatic cholangiocarcinoma and its differential diagnosis at MRI: How radiologist should assess MR features. Radiol. Med. 2021, 126, 1584–1600. [Google Scholar] [CrossRef] [PubMed]
- Cappabianca, S.; Granata, V.; Di Grezia, G.; Mandato, Y.; Reginelli, A.; Di Mizio, V.; Grassi, R.; Rotondo, A. The role of nasoenteric intubation in the MR study of patients with Crohn’s disease: Our experience and literature review. Radiol. Med. 2010, 116, 389–406, English, Italian. [Google Scholar] [CrossRef]
- Granata, V.; Fusco, R.; De Muzio, F.; Cutolo, C.; Setola, S.V.; Grassi, R.; Grassi, F.; Ottaiano, A.; Nasti, G.; Tatangelo, F.; et al. Radiomics textural features by MR imaging to assess clinical outcomes following liver resection in colorectal liver metastases. Radiol. Med. 2022, 127, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Granata, V.; Fusco, R.; De Muzio, F.; Cutolo, C.; Setola, S.V.; Dell’Aversana, F.; Grassi, F.; Belli, A.; Silvestro, L.; Ottaiano, A.; et al. Radiomics and machine learning analysis based on magnetic resonance imaging in the assessment of liver mucinous colorectal metastases. Radiol. Med. 2022, 127, 763–772. [Google Scholar] [CrossRef]
- Sansone, M.; Marrone, S.; Di Salvio, G.; Belfiore, M.P.; Gatta, G.; Fusco, R.; Vanore, L.; Zuiani, C.; Grassi, F.; Vietri, M.T.; et al. Comparison between two packages for pectoral muscle removal on mammographic images. Radiol. Med. 2022, 127, 848–856. [Google Scholar] [CrossRef]
- Gabelloni, M.; Faggioni, L.; Cioni, D.; Mendola, V.; Falaschi, Z.; Coppola, S.; Corradi, F.; Isirdi, A.; Brandi, N.; Coppola, F.; et al. Extracorporeal membrane oxygenation (ECMO) in COVID-19 patients: A pocket guide for radiologists. Radiol. Med. 2022, 127, 369–382. [Google Scholar] [CrossRef]
- Ossola, C.; Curti, M.; Calvi, M.; Tack, S.; Mazzoni, S.; Genesio, L.; Venturini, M.; Genovese, E.A. Role of ultrasound and magnetic resonance imaging in the prognosis and classification of muscle injuries in professional football players: Correlation between imaging and return to sport time. Radiol. Med. 2021, 126, 1460–1467. [Google Scholar] [CrossRef] [PubMed]
- Bakdik, S.; Arslan, S.; Oncu, F.; Durmaz, M.S.; Altunkeser, A.; Eryilmaz, M.A.; Unlu, Y. Effectiveness of Superb Microvascular Imaging for the differentiation of intraductal breast lesions. Med Ultrason. 2018, 20, 306–312. [Google Scholar] [CrossRef] [Green Version]
- Cai, S.-M.; Wang, H.-V.; Zhang, X.-Y.; Zhang, L.; Zhu, Q.-L.; Li, J.-C.; Sun, Q.; Jiang, Y.-X. The Vascular Index of Superb Microvascular Imaging Can Improve the Diagnostic Accuracy for Breast Imaging Reporting and Data System Category 4 Breast Lesions. Cancer Manag. Res. 2020, 12, 1819–1826. [Google Scholar] [CrossRef] [Green Version]
- Corvino, A.; Varelli, C.; Cocco, G.; Corvino, F.; Catalano, O. Seeing the unseen with superb microvascular imaging: Ultrasound depiction of normal dermis vessels. J. Clin. Ultrasound 2022, 50, 121–127. [Google Scholar] [CrossRef]
- Corvino, A.; Varelli, C.; Catalano, F.; Cocco, G.; Delli Pizzi, A.; Boccatonda, A.; Corvino, F.; Basile, L.; Catalano, O. Use of high-frequency transducers in breast sonography. J. Pers. Med. 2022, 12, 1960. [Google Scholar] [CrossRef]
- Corvino, A.; Catalano, O.; Varelli, C.; Cocco, G.; Delli Pizzi, A.; Corvino, F.; Tafuri, D.; Caruso, M. Non-glandular findings on breast ultrasound. Part II: A pictorial review of chest wall lesions. J. Ultrasound 2023, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Lee, H.J.; Ko, K.H.; Park, A.Y.; Koh, J.; Jung, H.K. New Doppler imaging technique for assessing angiogenesis in breast tumors: Correlation with immunohistochemically analyzed microvessels density. Acta Radiol. 2018, 59, 1414–1421. [Google Scholar] [CrossRef]
- Park, A.Y.; Seo, B.K. Up-to-date Doppler techniques for breast tumor vascularity: Superb microvascular imaging and contrast-enhanced ultrasound. Ultrasonography 2018, 37, 98–106. [Google Scholar] [CrossRef] [Green Version]
- Park, A.Y.; Kwon, M.; Woo, O.H.; Cho, K.R.; Park, E.K.; Cha, S.H.; Song, S.E.; Lee, J.-H.; Cha, J.; Son, G.S.; et al. A Prospective Study on the Value of Ultrasound Microflow Assessment to Distinguish Malignant from Benign Solid Breast Masses: Association between Ultrasound Parameters and Histologic Microvessel Densities. Korean J. Radiol. 2019, 20, 759–772. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.-C.; Zhang, Y.; Deng, S.-H.; Jiang, Q. Diagnostic Performance of Superb Microvascular Imaging (SMI) Combined with Shear-Wave Elastography in Evaluating Breast Lesions. Experiment 2018, 24, 5935–5942. [Google Scholar] [CrossRef]
- BBarile, A. Correction to: Some thoughts and greetings from the new Editor-in-Chief. Radiol. Med. 2021, 126, 1377. [Google Scholar] [CrossRef]
- Catalano, O.; Corvino, A.; Basile, L.; Catalano, F.; Varelli, C. Use of new microcirculation software allows the demonstration of dermis vascularization. J. Ultrasound 2022, 1–6. [Google Scholar] [CrossRef]
- Sivakumaran, L.; Alturkistani, H.; Lerouge, S.; Bertrand-Grenier, A.; Zehtabi, F.; Thérasse, É.; Roy-Cardinal, M.-H.; Bhatnagar, S.; Cloutier, G.; Soulez, G. Strain Ultrasound Elastography of Aneurysm Sac Content after Randomized Endoleak Embolization with Sclerosing vs. Non-sclerosing Chitosan-based Hydrogels in a Canine Model. J. Vasc. Interv. Radiol. 2022, 33, 495–504. [Google Scholar] [CrossRef] [PubMed]
- Bartolotta, T.V.; Orlando, A.A.M.; Dimarco, M.; Zarcaro, C.; Ferraro, F.; Cirino, A.; Matranga, D.; Vieni, S.; Cabibi, D. Diagnostic performance of 2D-shear wave elastography in the diagnosis of breast cancer: A clinical appraisal of cutoff values. Radiol. Med. 2022, 127, 1209–1220. [Google Scholar] [CrossRef]
- Ding, S.-S.; Liu, C.; Zhang, Y.-F.; Sun, L.-P.; Xiang, L.-H.; Liu, H.; Fang, Y.; Ren, W.-W.; Zhao, H.; Sun, X.-M.; et al. Contrast-enhanced ultrasound in the assessment of Crohn’s disease activity: Comparison with computed tomography enterography. Radiol. Med. 2022, 127, 1068–1078. [Google Scholar] [CrossRef]
- Elia, D.; Fresilli, D.; Pacini, P.; Cardaccio, S.; Polti, G.; Guiban, O.; Celletti, I.; Kutrolli, E.; De Felice, C.; Occhiato, R.; et al. Can strain US-elastography with strain ratio (SRE) improve the diagnostic accuracy in the assessment of breast lesions? Preliminary results. J. Ultrasound 2020, 24, 157–163. [Google Scholar] [CrossRef]
- Hyodo, R.; Takehara, Y.; Naganawa, S. 4D Flow MRI in the portal venous system: Imaging and analysis methods, and clinical applications. Radiol. Med. 2022, 127, 1181–1198. [Google Scholar] [CrossRef]
- Ruan, S.-M.; Huang, H.; Cheng, M.-Q.; Lin, M.-X.; Hu, H.-T.; Huang, Y.; Li, M.-D.; Wang, W. Shear-wave elastography combined with contrast-enhanced ultrasound algorithm for noninvasive characterization of focal liver lesions. Radiol. Med. 2022, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ruscitti, P.; Esposito, M.; Gianneramo, C.; Di Cola, I.; De Berardinis, A.; Martinese, A.; Tochap, G.N.; Conforti, A.; Masciocchi, C.; Cipriani, P.; et al. Nail and enthesis assessment in patients with psoriatic disease by high frequency ultrasonography: Findings from a single-centre cross-sectional study. Radiol. Med. 2022, 127, 1400–1406. [Google Scholar] [CrossRef] [PubMed]
- Salaffi, F.; Carotti, M.; Di Matteo, A.; Ceccarelli, L.; Farah, S.; Villota-Eraso, C.; Di Carlo, M.; Giovagnoni, A. Ultrasound and magnetic resonance imaging as diagnostic tools for sarcopenia in immune-mediated rheumatic diseases (IMRDs). Radiol. Med. 2022, 127, 1277–1291. [Google Scholar] [CrossRef] [PubMed]
- Ventura, C.; Baldassarre, S.; Cerimele, F.; Pepi, L.; Marconi, E.; Ercolani, P.; Floridi, C.; Argalia, G.; Goteri, G.; Giovagnoni, A. 2D shear wave elastography in evaluation of prognostic factors in breast cancer. Radiol. Med. 2022, 127, 1221–1227. [Google Scholar] [CrossRef]
- Youk, J.H.; Gweon, H.M.; Son, E.J. Shear-wave elastography in breast ultrasonography: The state of the art. Ultrasonography 2017, 36, 300–309. [Google Scholar] [CrossRef] [Green Version]
- Barr, R.G.; Nakashima, K.; Amy, D.; Cosgrove, D.; Farrokh, A.; Schafer, F.; Bamber, J.C.; Castera, L.; Choi, B.I.; Chou, Y.-H.; et al. WFUMB guidelines and recommendations for clinical use of ultrasound elastography: Part 2, breast. Ultrasound Med. Biol. 2015, 41, 1148–1160. [Google Scholar] [CrossRef] [Green Version]
- Barr, R.G. Future of breast elastography. Ultrasonography 2019, 38, 93–105. [Google Scholar] [CrossRef] [Green Version]
- Luo, S.; Yao, G.; Hong, Z.; Zhang, S.; Wang, W.; Zhang, J.; Zhang, Y.; Wu, J.; Zhang, L.; Cheng, H.; et al. Qualitative Classification of Shear Wave Elastography for Differential Diagnosis Between Benign and Metastatic Axillary Lymph Nodes in Breast Cancer. Front. Oncol. 2019, 9, 533. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Chang, J.M.; Cho, N.; Koo, H.R.; Yi, A.; Kim, S.J.; Youk, J.H.; Son, E.J.; Choi, S.H.; Kook, S.H.; et al. Practice guideline for the performance of breast ultrasound elastography. Ultrasonography 2013, 33, 3–10. [Google Scholar] [CrossRef]
- Sezgin, G.; Coskun, M.; Apaydin, M.; Sari, A.A. The role of rare breast cancers in the false negative strain elastography results. Radiol. Med. 2021, 126, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Trombadori, C.M.L.; D’Angelo, A.; Ferrara, F.; Santoro, A.; Belli, P.; Manfredi, R. Radial Scar: A management dilemma. Radiol. Med. 2021, 126, 774–785. [Google Scholar] [CrossRef]
- Kapetas, P.; Woitek, R.; Clauser, P.; Bernathova, M.; Pinker, K.; Helbich, T.H.; Baltzer, P.A. A Simple Ultrasound Based Classification Algorithm Allows Differentiation of Benign from Malignant Breast Lesions by Using Only Quantitative Parameters. Mol. Imaging Biol. 2018, 20, 1053–1060. [Google Scholar] [CrossRef] [Green Version]
- De Muzio, F.; Grassi, F.; Dell’Aversana, F.; Fusco, R.; Danti, G.; Flammia, F.; Chiti, G.; Valeri, T.; Agostini, A.; Palumbo, P.; et al. A Narrative Review on LI-RADS Algorithm in Liver Tumors: Prospects and Pitfalls. Diagnostics 2022, 12, 1655. [Google Scholar] [CrossRef]
- Catalano, O.; Sandomenico, F.; Vallone, P.; Setola, S.V.; Granata, V.; Fusco, R.; Lastoria, S.; Mansi, L.; Petrillo, A. Contrast-Enhanced Ultrasound in the Assessment of Patients with Indeterminate Abdominal Findings at Positron Emission Tomography Imaging. Ultrasound Med. Biol. 2016, 42, 2717–2723. [Google Scholar] [CrossRef]
- Granata, V.; Grassi, R.; Fusco, R.; Setola, S.; Belli, A.; Piccirillo, M.; Pradella, S.; Giordano, M.; Cappabianca, S.; Brunese, L.; et al. Abbreviated MRI Protocol for the Assessment of Ablated Area in HCC Patients. Int. J. Environ. Res. Public Heal. 2021, 18, 3598. [Google Scholar] [CrossRef] [PubMed]
- Barretta, M.L.; Catalano, O.; Setola, S.V.; Granata, V.; Marone, U.; Gallipoli, A.D. Gallbladder metastasis: Spectrum of imaging findings. Abdom. Imaging 2011, 36, 729–734. [Google Scholar] [CrossRef]
- Granata, V.; Fusco, R.; Catalano, O.; Avallone, A.; Palaia, R.; Botti, G.; Tatangelo, F.; Granata, F.; Cascella, M.; Izzo, F.; et al. Diagnostic accuracy of magnetic resonance, computed tomography and contrast enhanced ultrasound in radiological multimodality assessment of peribiliary liver metastases. PLoS ONE 2017, 12, e0179951. [Google Scholar] [CrossRef] [Green Version]
- Granata, V.; Castelguidone, E.D.L.D.; Fusco, R.; Catalano, O.; Piccirillo, M.; Palaia, R.; Izzo, F.; Gallipoli, A.D.; Petrillo, A. Irreversible electroporation of hepatocellular carcinoma: Preliminary report on the diagnostic accuracy of magnetic resonance, computer tomography, and contrast-enhanced ultrasound in evaluation of the ablated area. Radiol. Med. 2015, 121, 122–131. [Google Scholar] [CrossRef] [PubMed]
- Chou, C.-P.; Huang, J.-S.; Wang, J.-S.; Pan, H.-B. Contrast-enhanced ultrasound features of breast capillary hemangioma: A case report and review of literature. J. Ultrasound 2022, 25, 103–106. [Google Scholar] [CrossRef] [PubMed]
- Guo, R.; Lu, G.; Qin, B.; Fei, B. Ultrasound Imaging Technologies for Breast Cancer Detection and Management: A Review. Ultrasound Med. Biol. 2018, 44, 37–70. [Google Scholar] [CrossRef]
- Faccioli, N.; Santi, E.; Foti, G.; D’Onofrio, M. Cost-effectiveness analysis of including contrast-enhanced ultrasound in management of pancreatic cystic neoplasms. Radiol. Med. 2022, 127, 349–359. [Google Scholar] [CrossRef] [PubMed]
- Fresilli, D.; Di Leo, N.; Martinelli, O.; Di Marzo, L.; Pacini, P.; Dolcetti, V.; Del Gaudio, G.; Canni, F.; Ricci, L.I.; De Vito, C.; et al. 3D-Arterial analysis software and CEUS in the assessment of severity and vulnerability of carotid atherosclerotic plaque: A comparison with CTA and histopathology. Radiol. Med. 2022, 127, 1254–1269. [Google Scholar] [CrossRef] [PubMed]
- Sofia, C.; Solazzo, A.; Cattafi, A.; Chimenz, R.; Cicero, G.; Marino, M.A.; D’Angelo, T.; Manti, L.; Condorelli, E.; Ceravolo, G.; et al. Contrast-enhanced voiding urosonography in the assessment of vesical-ureteral reflux: The time has come. Radiol. Med. 2021, 126, 901–909. [Google Scholar] [CrossRef]
- Varghese, B.A.; Lee, S.; Cen, S.; Talebi, A.; Mohd, P.; Stahl, D.; Perkins, M.; Desai, B.; Duddalwar, V.A.; Larsen, L.H. Characterizing breast masses using an integrative framework of machine learning and CEUS-based radiomics. J. Ultrasound 2022, 25, 699–708. [Google Scholar] [CrossRef]
- Jia, K.; Li, L.; Wu, X.J.; Hao, M.J.; Xue, H.Y. Contrast-enhanced ultrasound for evaluating the pathologic response of breast cancer to neoadjuvant chemotherapy. Medicine 2019, 98, e14258. [Google Scholar] [CrossRef]
- Bin, L.; Huihui, Y.; Weiping, Y.; Changyuan, W.; Qinghong, Q.; Weiyu, M. Value of three-dimensional ultrasound in differentiating malignant from benign breast tumors. A systematic review and meta-analysis. Ultrasound Q. 2019, 35, 68–73. [Google Scholar] [CrossRef]
- Satake, H.; Ishigaki, S.; Ito, R.; Naganawa, S. Radiomics in breast MRI: Current progress toward clinical application in the era of artificial intelligence. Radiol. Med. 2021, 127, 39–56. [Google Scholar] [CrossRef] [PubMed]
- Rossi, F.; Lambertini, M.; Brunetti, N.; De Giorgis, S.; Razeti, M.G.; Calabrese, M.; Tagliafico, A.S. Muscle mass loss in breast cancer patients of reproductive age (≤45 years) undergoing neoadjuvant chemotherapy. Radiol. Med. 2022, 1–9. [Google Scholar] [CrossRef]
- Fiaschetti, V.; Ubaldi, N.; De Fazio, S.; Ricci, A.; Maspes, F.; Cossu, E. Digital tomosynthesis spot view in architectural distortions: Outcomes in management and radiation dose. Radiol. Med. 2022, 1–14. [Google Scholar] [CrossRef]
- Clauser, P.; Londero, V.; Como, G.; Girometti, R.; Bazzocchi, M.; Zuiani, C. Comparison between different imaging techniques in the evaluation of malignant breast lesions: Can 3D ultrasound be useful? Radiol. Med. 2014, 119, 240–248. [Google Scholar] [CrossRef]
- Park, A.Y.; Seo, B.K.; Cho, K.R.; Woo, O.H. The utility of MicroPure™ ultrasound technique in assessing grouped microcalcifications without a mass on mammography. J. Breast Cancer 2016, 19, 83–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Zelst, J.C.; Mann, R.M. Automated three-dimensional breast US for screening: Technique, artifacts, and lesion characterization. Radio Graph. 2018, 38, 663–683. [Google Scholar] [CrossRef]
- Zanotel, M.; Bednarova, I.; Londero, V.; Linda, A.; Lorenzon, M.; Girometti, R.; Zuiani, C. Automated breast ultrasound: Basic principles and emerging clinical applications. Radiol. Med. 2018, 123, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Schiaffino, S.; Gristina, L.; Tosto, S.; Massone, E.; De Giorgis, S.; Garlaschi, A.; Tagliafico, A.; Calabrese, M. The value of coronal view as a stand-alone assessment in women undergoing automated breast ultrasound. Radiol. Med. 2020, 126, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Barr, R.G.; DeVita, R.; Destounis, S.; Manzoni, F.; De Silvestri, A.; Tinelli, C. Agreement between an automated volume breast scanner and hand held ultrasound for diagnostic breast examinations. J. Ultrasound. Med. 2017, 36, 2087–2092. [Google Scholar] [CrossRef] [Green Version]
- Brem, R.F.; Tabár, L.; Duffy, S.W.; Inciardi, M.F.; Guingrich, J.A.; Hashimoto, B.E.; Lander, M.R.; Lapidus, R.L.; Peterson, M.K.; Rapelyea, J.A.; et al. Assessing Improvement in Detection of Breast Cancer with Three-dimensional Automated Breast US in Women with Dense Breast Tissue: The SomoInsight Study. Radiology 2015, 274, 663–673. [Google Scholar] [CrossRef] [Green Version]
- D’Angelo, A.; Orlandi, A.; Bufi, E.; Mercogliano, S.; Belli, P.; Manfredi, R. Automated breast volume scanner (ABVS) compared to handheld ultrasound (HHUS) and contrast-enhanced magnetic resonance imaging (CE-MRI) in the early assessment of breast cancer during neoadjuvant chemotherapy: An emerging role to monitoring tumor response? Radiol. Med. 2021, 126, 517–526. [Google Scholar] [CrossRef] [PubMed]
- Girometti, R.; Zanotel, M.; Londero, V.; Bazzocchi, M.; Zuiani, C. Comparison between automated breast volume scanner (ABVS) versus hand-held ultrasound as a second look procedure after magnetic resonance imaging. Eur. Radiol. 2017, 27, 3767–3775. [Google Scholar] [CrossRef]
- Coppola, F.; Faggioni, L.; Regge, D.; Giovagnoni, A.; Golfieri, R.; Bibbolino, C.; Miele, V.; Neri, E.; Grassi, R. Artificial intelligence: Radiologists’ expectations and opinions gleaned from a nationwide online survey. Radiol. Med. 2021, 126, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Nardone, V.; Reginelli, A.; Grassi, R.; Boldrini, L.; Vacca, G.; D’Ippolito, E.; Annunziata, S.; Farchione, A.; Belfiore, M.P.; Desideri, I.; et al. Delta radiomics: A systematic review. Radiol. Med. 2021, 126, 1571–1583. [Google Scholar] [CrossRef]
- Tadayyon, H.; Gangeh, M.; Sannachi, L.; Trudeau, M.; Pritchard, K.; Ghandi, S.; Eisen, A.; Look-Hong, N.; Holloway, C.; Wright, F.; et al. A priori prediction of breast tumour response to chemotherapy using quantitative ultrasound imaging and artificial neural networks. Oncotarget 2019, 10, 3910–3923. [Google Scholar] [CrossRef] [PubMed]
- Vicini, S.; Bortolotto, C.; Rengo, M.; Ballerini, D.; Bellini, D.; Carbone, I.; Preda, L.; Laghi, A.; Coppola, F.; Faggioni, L. A narrative review on current imaging applications of artificial intelligence and radiomics in oncology: Focus on the three most common cancers. Radiol. Med. 2022, 127, 819–836. [Google Scholar] [CrossRef] [PubMed]
- Simonetti, I.; Bruno, F.; Fusco, R.; Cutolo, C.; Setola, S.V.; Patrone, R.; Masciocchi, C.; Palumbo, P.; Arrigoni, F.; Picone, C.; et al. Multimodality Imaging Assessment of Desmoid Tumors: The Great Mime in the Era of Multidisciplinary Teams. J. Pers. Med. 2022, 12, 1153. [Google Scholar] [CrossRef]
- Granata, V.; Fusco, R.; Avallone, A.; De Stefano, A.; Ottaiano, A.; Sbordone, C.; Brunese, L.; Izzo, F.; Petrillo, A. Radiomics-Derived Data by Contrast Enhanced Magnetic Resonance in RAS Mutations Detection in Colorectal Liver Metastases. Cancers 2021, 13, 453. [Google Scholar] [CrossRef]
- Granata, V.; Fusco, R.; Risi, C.; Ottaiano, A.; Avallone, A.; De Stefano, A.; Grimm, R.; Grassi, R.; Brunese, L.; Izzo, F.; et al. Diffusion-Weighted MRI and Diffusion Kurtosis Imaging to Detect RAS Mutation in Colorectal Liver Metastasis. Cancers 2020, 12, 2420. [Google Scholar] [CrossRef]
- Wilding, R.; Sheraton, V.M.; Soto, L.; Chotai, N.; Tan, E.Y. Deep learning applied to breast imaging classification and segmentation with human expert intervention. J. Ultrasound 2022, 25, 659–666. [Google Scholar] [CrossRef]
- Ciritsis, A.; Rossi, C.; Eberhard, M.; Marcon, M.; Becker, A.S.; Boss, A. Automatic classification of ultrasound breast lesions using a deep convolutional neural network mimicking human decision-making. Eur. Radiol. 2019, 29, 5458–5468. [Google Scholar] [CrossRef]
- Zeng, D.; Xu, M.; Liang, J.-Y.; Cheng, M.-Q.; Huang, H.; Pan, J.-M.; Huang, Y.; Tong, W.-J.; Xie, X.-Y.; Lu, M.-D.; et al. Using new criteria to improve the differentiation between HCC and non-HCC malignancies: Clinical practice and discussion in CEUS LI-RADS 2017. Radiol. Med. 2021, 127, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Jiang, M.; Li, C.-L.; Luo, X.-M.; Chuan, Z.-R.; Lv, W.-Z.; Li, X.; Cui, X.-W.; Dietrich, C.F. Ultrasound-based deep learning radiomics in the assessment of pathological complete response to neoadjuvant chemotherapy in locally advanced breast cancer. Eur. J. Cancer 2021, 147, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Ilesanmi, A.E.; Chaumrattanakul, U.; Makhanov, S.S. Methods for the segmentation and classification of breast ultrasound images: A review. J. Ultrasound 2021, 24, 367–382. [Google Scholar] [CrossRef]
- Scapicchio, C.; Gabelloni, M.; Barucci, A.; Cioni, D.; Saba, L.; Neri, E. A deep look into radiomics. Radiol. Med. 2021, 126, 1296–1311. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.-G.; Zhou, L.-Q.; Xu, J.-W.; Wang, J.-Y.; Wei, Q.; Deng, Y.-B.; Cui, X.-W.; Dietrich, C.F. Artificial intelligence in breast ultrasound. World J. Radiol. 2019, 11, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Bartolotta, T.V.; Orlando, A.; Cantisani, V.; Matranga, D.; Ienzi, R.; Cirino, A.; Amato, F.; Di Vittorio, M.L.; Midiri, M.; Lagalla, R. Focal breast lesion characterization according to the BI-RADS US lexicon: Role of a computer-aided decision-making support. Radiol. Med. 2018, 123, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Bartolotta, T.V.; Orlando, A.A.M.; Spatafora, L.; Dimarco, M.; Gagliardo, C.; Taibbi, A. S-Detect characterization of focal breast lesions according to the US BI RADS lexicon: A pictorial essay. J. Ultrasound 2020, 23, 207–215. [Google Scholar] [CrossRef]
- Bartolotta, T.V.; Orlando, A.A.M.; Di Vittorio, M.L.; Amato, F.; Dimarco, M.; Matranga, D.; Ienzi, R. S-Detect characterization of focal solid breast lesions: A prospective analysis of inter-reader agreement for US BI-RADS descriptors. J. Ultrasound 2020, 24, 143–150. [Google Scholar] [CrossRef]
- Zhao, C.; Xiao, M.; Jiang, Y.; Liu, H.; Wang, M.; Wang, H.; Sun, Q.; Zhu, Q. Feasibility of computer-assisted diagnosis for breast ultrasound: The results of the diagnostic performance of S-detect from a single center in China. Cancer Manag. Res. 2019, 11, 921–930. [Google Scholar] [CrossRef] [Green Version]
- Di Segni, M.; de Soccio, V.; Cantisani, V.; Bonito, G.; Rubini, A.; Di Segni, G.; Lamorte, S.; Magri, V.; De Vito, C.; Migliara, G.; et al. Automated classification of focal breast lesions according to S-detect: Validation and role as a clinical and teaching tool. J. Ultrasound 2018, 21, 105–118. [Google Scholar] [CrossRef] [Green Version]
- Chiao, J.-Y.; Chen, K.-Y.; Liao, K.Y.-K.; Hsieh, P.-H.; Zhang, G.; Huang, T.-C. Detection and classification the breast tumors using mask R-CNN on sonograms. Medicine 2019, 98, e15200. [Google Scholar] [CrossRef]
- Gao, Y.; Luo, Y.; Zhao, C.; Xiao, M.; Ma, L.; Li, W.; Qin, J.; Zhu, Q.; Jiang, Y. Nomogram based on radiomics analysis of primary breast cancer ultrasound images: Prediction of axillary lymph node tumor burden in patients. Eur. Radiol. 2021, 31, 928–937. [Google Scholar] [CrossRef] [PubMed]
- Fausto, A.; Rizzatto, G.; Preziosa, A.; Gaburro, L.; Washburn, M.J.; Rubello, D.; Volterrani, L. A new method to combine contrast-enhanced magnetic resonance imaging during live ultrasound of the breast using volume navigation technique: A study for evaluating feasibility, accuracy and reproducibility in healthy volunteers. Eur. J. Radiol. 2012, 81, e332–e337. [Google Scholar] [CrossRef]
- Kucukkaya, F.; Aribal, E.; Tureli, D.; Altas, H.; Kaya, H. Use of a Volume Navigation Technique for Combining Real-Time Ultrasound and Contrast-Enhanced MRI: Accuracy and Feasibility of a Novel Technique for Locating Breast Lesions. Am. J. Roentgenol. 2016, 206, 217–225. [Google Scholar] [CrossRef]
- Papalexis, N.; Parmeggiani, A.; Facchini, G.; Miceli, M.; Carbone, G.; Cavallo, M.; Spinnato, P. Current concepts in the diagnosis and treatment of adhesive capsulitis: Role of diagnostic imaging and ultrasound-guided interventional procedures. Radiol. Med. 2022, 127, 1390–1399. [Google Scholar] [CrossRef]
- Crisan, D.; Wortsman, X.; Alfageme, F.; Catalano, O.; Badea, A.; Scharffetter-Kochanek, K.; Sindrilaru, A.; Crisan, M. Ultrasonography in dermatologic surgery: Revealing the unseen for improved surgical planning. JDDG J. der Dtsch. Dermatol. Ges. 2022, 20, 913–926. [Google Scholar] [CrossRef] [PubMed]
- Moschetta, M.; Sardaro, A.; Nitti, A.; Telegrafo, M.; Maggialetti, N.; Scardapane, A.; Brunese, M.C.; Lavelli, V.; Ferrari, C. Ultrasound evaluation of ductal carcinoma in situ of the breast. J. Ultrasound 2021, 25, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Stavros, A.T.; Thickman, D.; Rapp, C.L.; Dennis, M.A.; Parker, S.H.; Sisney, G.A. Solid breast nodules: Use of sonography to distinguish between benign and malignant lesions. Radiology 1995, 196, 123–134. [Google Scholar] [CrossRef] [Green Version]
- Deandrea, S.; Cavazzana, L.; Principi, N.; Luconi, E.; Campoleoni, M.; Bastiampillai, A.J.; Bracchi, L.; Bucchi, L.; Pedilarco, S.; Piscitelli, A.; et al. Screening of women with aesthetic prostheses in dedicated sessions of a population-based breast cancer screening programme. Radiol. Med. 2021, 126, 946–955. [Google Scholar] [CrossRef]
- Fusco, R.; Petrillo, A.; Catalano, O.; Sansone, M.; Granata, V.; Filice, S.; D’Aiuto, M.; Pankhurst, Q.; Douek, M. Procedures for location of non-palpable breast lesions: A systematic review for the radiologist. Breast Cancer 2014, 21, 522–531. [Google Scholar] [CrossRef]
- Nori, J.; Bicchierai, G.; Amato, F.; De Benedetto, D.; Boeri, C.; Vanzi, E.; Di Naro, F.; Bianchi, S.; Miele, V. A new technique for the histological diagnosis of Paget’s disease of the breast using a semiautomated core needle biopsy with a 14-gauge needle. Radiol. Med. 2021, 126, 936–945. [Google Scholar] [CrossRef] [PubMed]
- Panzironi, G.; Moffa, G.; Galati, F.; Pediconi, F. Ultrasound-guided 8-Gauge vacuum-assisted excision for selected B3 breast lesions: A preliminary experience. Radiol. Med. 2022, 127, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Petrillo, A.; Di Giacomo, R.; Esposito, E.; Vallone, P.; Setola, S.V.; Raso, M.M.; Granata, V.; Barretta, M.L.; Siani, C.; Rinaldo, C.; et al. Preoperative localisation of nonpalpable breast lesions using magnetic markers in a tertiary cancer centre. Eur. Radiol. Exp. 2022, 6, 28. [Google Scholar] [CrossRef]
- Bellardita, L.; Colciago, R.R.; Frasca, S.; De Santis, M.C.; Gay, S.; Palorini, F.; La Rocca, E.; Valdagni, R.; Rancati, T.; Lozza, L. Breast cancer patient perspective on opportunities and challenges of a genetic test aimed to predict radio-induced side effects before treatment: Analysis of the Italian branch of the REQUITE project. Radiol. Med. 2021, 126, 1366–1373. [Google Scholar] [CrossRef]
- Carbonaro, L.A.; Rizzo, S.S.; Schiaffino, S.; Mainini, A.P.; Berger, N.; Trimboli, R.M.; Sardanelli, F. Biennial screening mammography: How many women ask for more? Estimate of the interval mammogram rate in an organised population-based screening programme. Radiol. Med. 2021, 126, 200–205. [Google Scholar] [CrossRef]
- Caruso, M.; Catalano, O.; Bard, R.; Varelli, C.; Corvino, F.; Caiazzo, C.; Corvino, A. Non-glandular findings on breast ultrasound. Part I: A pictorial review of superficial lesions. J. Ultrasound 2022, 25, 783–797. [Google Scholar] [CrossRef] [PubMed]
- Maio, F.; Tari, D.U.; Granata, V.; Fusco, R.; Grassi, R.; Petrillo, A.; Pinto, F. Breast Cancer Screening during COVID-19 Emergency: Patients and Department Management in a Local Experience. J. Pers. Med. 2021, 11, 380. [Google Scholar] [CrossRef]
- Neri, E.; Granata, V.; Montemezzi, S.; Belli, P.; Bernardi, D.; Brancato, B.; Caumo, F.; Calabrese, M.; Coppola, F.; Cossu, E.; et al. Structured reporting of x-ray mammography in the first diagnosis of breast cancer: A Delphi consensus proposal. Radiol. Med. 2022, 127, 471–483. [Google Scholar] [CrossRef]
- Deandrea, S.; Sardanelli, F.; Calabrese, M.; Ferré, F.; Vainieri, M.; Sestini, E.; Caumo, F.; Saguatti, G.; Bucchi, L.; Cataliotti, L. Provision of follow-up care for women with a history of breast cancer following the 2016 position paper by the Italian Group for Mammographic Screening and the Italian College of Breast Radiologists by SIRM: A survey of Senonetwork Italian breast centres. Radiol. Med. 2022, 127, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Granata, V.; Bicchierai, G.; Fusco, R.; Cozzi, D.; Grazzini, G.; Danti, G.; De Muzio, F.; Maggialetti, N.; Smorchkova, O.; D’Elia, M.; et al. Diagnostic protocols in oncology: Workup and treatment planning. Part 2: Abbreviated MR protocol. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 6499–6528. [Google Scholar] [CrossRef]
- Leung, J.W. Second-look ultrasound: Only for biopsy or more? Eur. J. Radiol. 2012, 81, s87–s89. [Google Scholar] [CrossRef] [PubMed]
- Sansone, M.; Grassi, R.; Belfiore, M.P.; Gatta, G.; Grassi, F.; Pinto, F.; La Casella, G.V.; Fusco, R.; Cappabianca, S.; Granata, V. Radiomic features of breast parenchyma: Assessing differences between FOR PROCESSING and FOR PRESENTATION digital mammography. Insights Into Imaging 2021, 12, 147. [Google Scholar] [CrossRef]
- Fusco, R.; Granata, V.; Pariante, P.; Cerciello, V.; Siani, C.; Di Bonito, M.; Valentino, M.; Sansone, M.; Botti, G.; Petrillo, A. Blood oxygenation level dependent magnetic resonance imaging and diffusion weighted MRI imaging for benign and malignant breast cancer discrimination. Magn. Reson. Imaging 2020, 75, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Fusco, R.; Granata, V.; Raso, M.M.; Vallone, P.; De Rosa, A.; Siani, C.; Di Bonito, M.; Petrillo, A.; Sansone, M. Blood Oxygenation Level Dependent Magnetic Resonance Imaging (MRI), Dynamic Contrast Enhanced MRI, and Diffusion Weighted MRI for Benign and Malignant Breast Cancer Discrimination: A Preliminary Experience. Cancers 2021, 13, 2421. [Google Scholar] [CrossRef] [PubMed]
- Girometti, R.; Linda, A.; Conte, P.; Lorenzon, M.; De Serio, I.; Jerman, K.; Londero, V.; Zuiani, C. Multireader comparison of contrast-enhanced mammography versus the combination of digital mammography and digital breast tomosynthesis in the preoperative assessment of breast cancer. Radiol. Med. 2021, 126, 1407–1414. [Google Scholar] [CrossRef]
- Catalano, O.; Raso, M.M.; Petrillo, A.; D’Errico, A.G. Extended field of view in breast sonography. Ultraschall Med 2011, 32, 198–202. [Google Scholar] [CrossRef] [PubMed]
- Petralia, G.; Zugni, F.; Summers, P.E.; Colombo, A.; Pricolo, P.; Grazioli, L.; Colagrande, S.; Giovagnoni, A.; Padhani, A.R.; On behalf of the Italian Working Group on Magnetic Resonance. Whole-body magnetic resonance imaging (WB-MRI) for cancer screening: Recommendations for use. Radiol. Med. 2021, 126, 1434–1450. [Google Scholar] [CrossRef]
- Petrillo, A.; Catalano, O.; Fusco, R.; Filice, S.; Vallone, P.; Setola, S.; Granata, V.; Raiano, C.; Avino, F.; Di Bonito, M.; et al. Optical imaging of the breast: Evaluation of deoxyhemoglobin concentration alteration in 166 patients with suspicious breast lesions. Eur. Radiol. Exp. 2018, 2, 8. [Google Scholar] [CrossRef]
- Lohitvisate, W.; Pummee, N.; Kwankua, A. Mammographic and ultrasonographic features of triple-negative breast cancer compared with non-triple-negative breast cancer. J. Ultrasound 2022, 1–8. [Google Scholar] [CrossRef]
- Cellina, M.; Gibelli, D.; Martinenghi, C.; Giardini, D.; Soresina, M.; Menozzi, A.; Oliva, G.; Carrafiello, G. Non-contrast magnetic resonance lymphography (NCMRL) in cancer-related secondary lymphedema: Acquisition technique and imaging findings. Radiol. Med. 2021, 126, 1477–1486. [Google Scholar] [CrossRef]
- Fusco, R.; Sansone, M.; Granata, V.; Di Bonito, M.; Avino, F.; Catalano, O.; Botti, G.; Petrillo, A. Use of Quantitative Morphological and Functional Features for Assessment of Axillary Lymph Node in Breast Dynamic Contrast-Enhanced Magnetic Resonance Imaging. BioMed Res. Int. 2018, 2018, 2610801. [Google Scholar] [CrossRef] [PubMed]
- Nicosia, L.; Bozzini, A.C.; Palma, S.; Montesano, M.; Signorelli, G.; Pesapane, F.; Latronico, A.; Bagnardi, V.; Frassoni, S.; Sangalli, C.; et al. Contrast-Enhanced Spectral Mammography and tumor size assessment: A valuable tool for appropriate surgical management of breast lesions. Radiol. Med. 2022, 127, 1228–1234. [Google Scholar] [CrossRef] [PubMed]
- Romanucci, G.; Mercogliano, S.; Carucci, E.; Cina, A.; Zantedeschi, E.; Caneva, A.; Benassuti, C.; Fornasa, F. Diagnostic accuracy of resection margin in specimen radiography: Digital breast tomosynthesis versus full-field digital mammography. Radiol. Med. 2021, 126, 768–773. [Google Scholar] [CrossRef] [PubMed]











Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Catalano, O.; Fusco, R.; De Muzio, F.; Simonetti, I.; Palumbo, P.; Bruno, F.; Borgheresi, A.; Agostini, A.; Gabelloni, M.; Varelli, C.; et al. Recent Advances in Ultrasound Breast Imaging: From Industry to Clinical Practice. Diagnostics 2023, 13, 980. https://doi.org/10.3390/diagnostics13050980
Catalano O, Fusco R, De Muzio F, Simonetti I, Palumbo P, Bruno F, Borgheresi A, Agostini A, Gabelloni M, Varelli C, et al. Recent Advances in Ultrasound Breast Imaging: From Industry to Clinical Practice. Diagnostics. 2023; 13(5):980. https://doi.org/10.3390/diagnostics13050980
Chicago/Turabian StyleCatalano, Orlando, Roberta Fusco, Federica De Muzio, Igino Simonetti, Pierpaolo Palumbo, Federico Bruno, Alessandra Borgheresi, Andrea Agostini, Michela Gabelloni, Carlo Varelli, and et al. 2023. "Recent Advances in Ultrasound Breast Imaging: From Industry to Clinical Practice" Diagnostics 13, no. 5: 980. https://doi.org/10.3390/diagnostics13050980