

Differentiating Fordyce Spots from Their Common Simulators Using Ultraviolet-Induced Fluorescence Dermatoscopy—Retrospective Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carli, P.; de Giorgi, V.; Chiarugi, A.; Nardini, P.; Weinstock, M.A.; Crocetti, E.; Stante, M.; Giannotti, B. Addition of dermoscopy to conventional naked-eye examination in melanoma screening: A randomized study. J. Am. Acad. Dermatol. 2004, 50, 683–689. [Google Scholar] [CrossRef] [PubMed]
- Vestergaard, M.E.; Macaskill, P.; Holt, P.E.; Menzies, S.W. Dermoscopy compared with naked eye examination for the diagnosis of primary melanoma: A meta-analysis of studies performed in a clinical setting. Br. J. Dermatol. 2008, 159, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Kapsokalyvas, D.; Bruscino, N.; Alfieri, D.; de Giorgi, V.; Cannarozzo, G.; Cicchi, R.; Massi, D.; Pimpinelli, N.; Pavone, F.S. Spectral morphological analysis of skin lesions with a polarization multispectral dermoscope. Opt. Express 2013, 21, 4826–4840. [Google Scholar] [CrossRef] [PubMed]
- Suhai, B.; Horváth, G. How well does the Rayleigh model describe the E-vector distribution of skylight in clear and cloudy conditions? A full-sky polarimetric study. J. Opt. Soc. Am. A Opt. Image Sci. Vis. 2004, 21, 1669–1676. [Google Scholar] [CrossRef] [PubMed]
- Mojeski, J.A.; Almashali, M.; Jowdy, P.; Fitzgerald, M.E.; Brady, K.L.; Zeitouni, N.C.; Colegio, O.R.; Paragh, G. Ultraviolet imaging in dermatology. Photodiagnosis Photodyn. Ther. 2020, 30, 101743. [Google Scholar] [CrossRef]
- Tang, J.; Ran, Y. Polarized and ultraviolet dermoscopy for the diagnosis of dermatophytosis of vellus hair. IJDVL 2020, 86, 607. [Google Scholar]
- Szepetiuk, G.; Piérard-Franchimont, C.; Quatresooz, P.; Piérard, G.E. Physico-biological foundation of skin fluorescence--review. Pathol. Biol. 2012, 60, 380–386. [Google Scholar] [CrossRef] [PubMed]
- Pietkiewicz, P.; Navarrete-Dechent, C. Scabies mite is bright green under UV dermatoscopy. Dermatol. Pract. Concept 2023, 13, e2023135. [Google Scholar] [CrossRef]
- Al-Nasiri, M.; Navarrete-Dechent, C.; Korecka, C.; Salwowska, N.; Goldust, M.; Pietkiewicz, P. Ultraviolet reflectance dermatoscopy of trichobacteriosis axillaris reveals peripilar yellow-green luminescent concretions. Dermatol. Pract. Concept 2023, 13. Online ahead of print. [Google Scholar] [CrossRef]
- Fordyce, J.A. A peculiar affection of the mucous membrane of the lips and oral cavity. J. Cutan Dis. 1896, 14, 413–419. [Google Scholar] [CrossRef]
- Tsuji, T.; Yamauchi, R. Areolar sebaceous hyperplasia with a Fordyce’s spot-like lesion. J. Dermatol. 1994, 21, 524–526. [Google Scholar] [CrossRef] [PubMed]
- Belinchón, I.; Aguilar, A.; Tardío, J.; Gallego, M.A. Areolar sebaceous hyperplasia: A case report. Cutis 1996, 58, 63–64. [Google Scholar]
- Mansur, A.T.; Aydingoz, I.E. Unilateral buccal fordyce spots with ipsilateral facial paralysis: A sign of neuro-sebaceous connection? Acta Derm. Venereol. 2012, 92, 177–178. [Google Scholar] [CrossRef]
- Errichetti, E.; Piccirillo, A.; Viola, L.; Ricciuti, F.; Ricciuti, F. Areolar sebaceous hyperplasia associated with oral and genital Fordyce spots. J. Dermatol. 2013, 40, 670. [Google Scholar] [CrossRef]
- Lester, R.A.; Torgerson, R.R.; Sandhu, N.P. Rare presentation of sebaceous hyperplasia. BMJ Case Rep. 2014, 2014, bcr2014204025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montalvo, N.; Tapia, V.; Padilla, H.; Redrobán, L. Heterotopic sebaceous glands in the esophagus, a very rare histopathological diagnosis: A case report and review of the literature. Clin. Case Rep. 2016, 5, 89–92. [Google Scholar] [CrossRef] [PubMed]
- Kansky, A.A.; Didanovic, V.; Dovsak, T.; Brzak, B.L.; Pelivan, I.; Terlevic, D. Epidemiology of oral mucosal lesions in Slovenia. Radiol. Oncol. 2018, 52, 263–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.; Lam, J.M. A teenage boy with asymptomatic papules on his upper lip. Paediatr. Child Health 2018, 23, 499–500. [Google Scholar] [CrossRef]
- Thirunavukkarasu, B.; Nada, R.; Dawra, S.; Sinha, S.K. Ectopic sebaceous glands in oesophagus. BMJ Case Rep. 2019, 12, e232736. [Google Scholar] [CrossRef]
- Le, A.; Amin, M.; Cappell, M.S. Case Report of a Proposed, Novel, Endoscopic ‘Whitehead Pimple’ Sign of Ectopic Esophageal Sebaceous Glands Based on Their Mimicking the Dermatologic and Histopathologic Characteristics of Cutaneous Whitehead Pimples/Closed Comedones. Dig. Dis. Sci. 2019, 64, 2049–2053. [Google Scholar] [CrossRef]
- Schachner, L.A.; Hansen, R.C. Pediatric Dermatology; Elsevier Health Sciences: Philadelphia, PA, USA, 2011; p. 1808. [Google Scholar]
- Baeder, F.M.; Pelino, J.E.P.; de Almeida, E.R.; Duarte, D.A.; Santos, M.T.B.R. High-power diode laser use on Fordyce granule excision: A case report. J. Cosmet. Dermatol. 2010, 9, 321–324. [Google Scholar] [CrossRef]
- Lee, J.H.; Lee, J.H.; Kwon, N.H.; Yu, D.S.; Kim, G.M.; Park, C.J.; Lee, J.D.; Kim, S.Y. Clinicopathologic Manifestations of Patients with Fordyce’s Spots. Ann. Dermatol. 2012, 24, 103–106. [Google Scholar] [CrossRef] [Green Version]
- Elston, D.M.; Meffert, J. Photo quiz. What is your diagnosis? Fordyce Spots. Cutis 2001, 68, 24–49. [Google Scholar] [PubMed]
- Radhakrishnan, S.; Agarwal, D.C. Fordyce spots masquerading as penile warts. Med. J. Armed Forces India 2016, 72, 384–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwata, K.; Katsuda, Y. Somatic symptoms after sexual behavior with fear of four sexually transmitted diseases: A proposal of novel disorder. J. Family Med. Prim. Care 2016, 5, 706–708. [Google Scholar] [CrossRef]
- Flinck, A.; Paludan, A.; Matsson, L.; Holm, A.K.; Axelsson, I. Oral findings in a group of newborn Swedish children. Int. J. Paediatr. Dent. 1994, 4, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Arun Babu, T.; Vijayadevagaran, V.; Carounanidy, U. Congenital intraoral Fordyce spots. Arch Dis. Child. Fetal. Neonatal. Ed. 2016, 101, F252. [Google Scholar] [CrossRef]
- Ramachandran, S.; Kalra, S.; Shaw, S.C. Fordyce Spots in a Neonate. Indian Pediatr. 2022, 59, 91. [Google Scholar] [PubMed]
- Gaballah, K.Y.; Rahimi, I. Can presence of oral Fordyce’s granules serve as a marker for hyperlipidemia? Dent. Res. J. (Isfahan) 2014, 11, 553–558. [Google Scholar] [PubMed]
- De Felice, C.; Parrini, S.; Chitano, G.; Gentile, M.; Dipaola, L.; Latini, G. Fordyce granules and hereditary non-polyposis colorectal cancer syndrome. Gut 2005, 54, 1279–1282. [Google Scholar] [CrossRef] [Green Version]
- Ponti, G.; Meschieri, A.; Pollio, A.; Ruini, C.; Manfredini, M.; Longo, C.; Mandel, V.D.; Ciardo, S.; Tomasi, A.; Giannetti, L.; et al. Fordyce granules and hyperplastic mucosal sebaceous glands as distinctive stigmata in Muir-Torre syndrome patients: Characterization with reflectance confocal microscopy. J. Oral Pathol. Med. 2015, 44, 552–557. [Google Scholar] [CrossRef] [Green Version]
- Fernandez-Flores, A.; Rodríguez Peralto, J.L. Mismatch Repair Protein Expression in Fordyce Granules. Appl. Immunohistochem. Mol. Morphol. 2017, 25, 209–212. [Google Scholar] [CrossRef] [PubMed]
- Chern, P.L.; Arpey, C.J. Fordyce spots of the lip responding to electrodesiccation and curettage. Dermatol. Surg. 2008, 34, 960–962. [Google Scholar] [PubMed]
- Pallua, N.; Stromps, J.P. Micro-punch technique for treatment of Fordyce spots: A surgical approach for an unpleasant condition of the male genital. J. Plast. Reconstr. Aesthet. Surg. 2013, 66, e8–e11. [Google Scholar] [CrossRef] [PubMed]
- Plotner, A.N.; Brodell, R.T. Treatment of Fordyce spots with bichloracetic acid. Dermatol. Surg. 2008, 34, 397–399; discussion 399. [Google Scholar]
- Kim, Y.J.; Kang, H.Y.; Lee, E.S.; Kim, Y.C. Treatment of Fordyce spots with 5-aminolaevulinic acid-photodynamic therapy. Br. J. Dermatol. 2007, 156, 399–400. [Google Scholar] [CrossRef]
- Richey, D.F. Aminolevulinic acid photodynamic therapy for sebaceous gland hyperplasia. Dermatol. Clin. 2007, 25, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Gold, M.H.; Bradshaw, V.L.; Boring, M.M.; Bridges, T.M.; Biron, J.A.; Lewis, T.L. Treatment of sebaceous gland hyperplasia by photodynamic therapy with 5-aminolevulinic acid and a blue light source or intense pulsed light source. J. Drugs Dermatol. 2004, 3 (Suppl. S6), S6–S9. [Google Scholar]
- Ahn, G.R.; Park, S.J.; Lee, C.K.; Kim, B.J. A case of successful treatment of Fordyce spots with a single insulated microneedle radiofrequency device. Dermatol. Ther. 2019, 32, e13026. [Google Scholar] [CrossRef]
- Ryu, S.I.; Jeong, J.Y.; Kim, K.E.; Ryu, H.J. Fordyce Spots Treated by an Intralesional Insulated Microneedle Radiofrequency Device. Dermatol. Surg. 2021, 47, 1021–1022. [Google Scholar] [CrossRef]
- Mutizwa, M.M.; Berk, D.R. Dichotomous long-term response to isotretinoin in two patients with fordyce spots. Pediatr. Dermatol. 2014, 31, 73–75. [Google Scholar] [CrossRef] [PubMed]
- Handiani, F.; Sadati, M.S. Isotretinoin-induced regression of Fordyce spots in a patient with acne: The first report. G Ital. Dermatol. Venereol. 2015, 150, 343–344. [Google Scholar] [PubMed]
- Kim, S.K.; Do, J.E.; Kang, H.Y.; Lee, E.S.; Kim, Y.C. Combination of topical 5-aminolevulinic acid-photodynamic therapy with carbon dioxide laser for sebaceous hyperplasia. J. Am. Acad. Dermatol. 2007, 56, 523–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jakhar, D.; Kaur, I. Mucoscopy of Fordyce’s Spots on Lips. Indian Dermatol. Online J. 2019, 10, 498–499. [Google Scholar] [CrossRef]
- Errichetti, E.; Zalaudek, I.; Kittler, H.; Apalla, Z.; Argenziano, G.; Bakos, R.; Blum, A.; Braun, R.P.; Ioannides, D.; Lacarrubba, F.; et al. Standardization of dermoscopic terminology and basic dermoscopic parameters to evaluate in general dermatology (non-neoplastic dermatoses): An expert consensus on behalf of the International Dermoscopy Society. Br. J. Dermatol. 2020, 182, 454–467. [Google Scholar] [CrossRef]
- Arrazola, P.; Mullani, N.A.; Abramovits, W. DermLite II: An innovative portable instrument for dermoscopy without the need of immersion fluids. Skinmed 2005, 4, 78–83. [Google Scholar] [PubMed]
- Thoreson, W.B.; Dacey, D.M. Diverse Cell Types, Circuits, and Mechanisms for Color Vision in the Vertebrate Retina. Physiol. Rev. 2019, 99, 1527–1573. [Google Scholar] [CrossRef] [PubMed]
- Hammond, B.R.; Renzi-Hammond, L. Individual variation in the transmission of UVB radiation in the young adult eye. PLoS ONE 2018, 13, e0199940. [Google Scholar] [CrossRef]
- Dyer, J.M.; Foy, V.M. Revealing The Unseen: A Review of Wood’s Lamp in Dermatology. J. Clin. Aesthet. Dermatol. 2022, 15, 25–30. [Google Scholar]
- Ruiz-Pino, M.; Foronda-García-Hidalgo, C.; Alarcón-Blanco, P.; Gutiérrez-Fernández, J. Male genitourinary infections by Corynebacterium glucuronolyticum. A review and clinical experience. Rev. Esp. Quimioter. 2019, 32, 479–484. [Google Scholar]
- Asawanonda, P.; Taylor, C.R. Wood’s light in dermatology. Int. J. Dermatol. 1999, 38, 801–807. [Google Scholar] [CrossRef] [PubMed]
- Navarrete-Dechent, C.; Uribe, P.; Marghoob, A. Ink-enhanced dermoscopy is a useful tool to differentiate acquired solitary plaque porokeratosis from other scaly lesions. J. Am. Acad. Dermatol. 2019, 80, e137–e138. [Google Scholar] [CrossRef] [PubMed]
- Zaar, O.; Polesie, S.; Navarrete-Dechent, C.; Errichetti, E.; Akay, B.N.; Jaimes, J.; Cabo, H.; Sabban, E.C.; Paoli, J. Dermoscopy of porokeratosis: Results from a multicentre study of the International Dermoscopy Society. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 2091–2096. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, B.B.; Shishak, M. An approach to venerophobia in males. Indian J. Sex Transm. Dis. AIDS 2017, 38, 103–106. [Google Scholar]
- Sonthalia, S.; Errichetti, E. Dermoscopy—Not just for diagnosis and not just for Dermatologists! Kathmandu Univ. Med. J. (KUMJ) 2017, 15, 1–2. [Google Scholar] [PubMed]
- Micali, G.; Lacarrubba, F. Augmented diagnostic capability using videodermatoscopy on selected infectious and non-infectious penile growths. Int. J. Dermatol. 2011, 50, 1501–1505. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No | Age | Sex | Ethnicity | Site | Clinical Presentation of Fordyce Spots | Context |
|---|---|---|---|---|---|---|
| 1 | 33 | M | Caucasian | Upper lip | Flat, poorly defined yellow-white papules grouped along the vermilion | STI suspect |
| 2 | 38 | M | Caucasian | Upper lip | Palpable, elevated well-defined yellowish papules grouped bilaterally in the vicinity of labial commissure of the mouth | Incidental finding |
| 3 | 33 | M | Caucasian | Upper lip | Slightly elevated, well-defined yellow-white papules grouped above the tubercle of the lip | STI suspect |
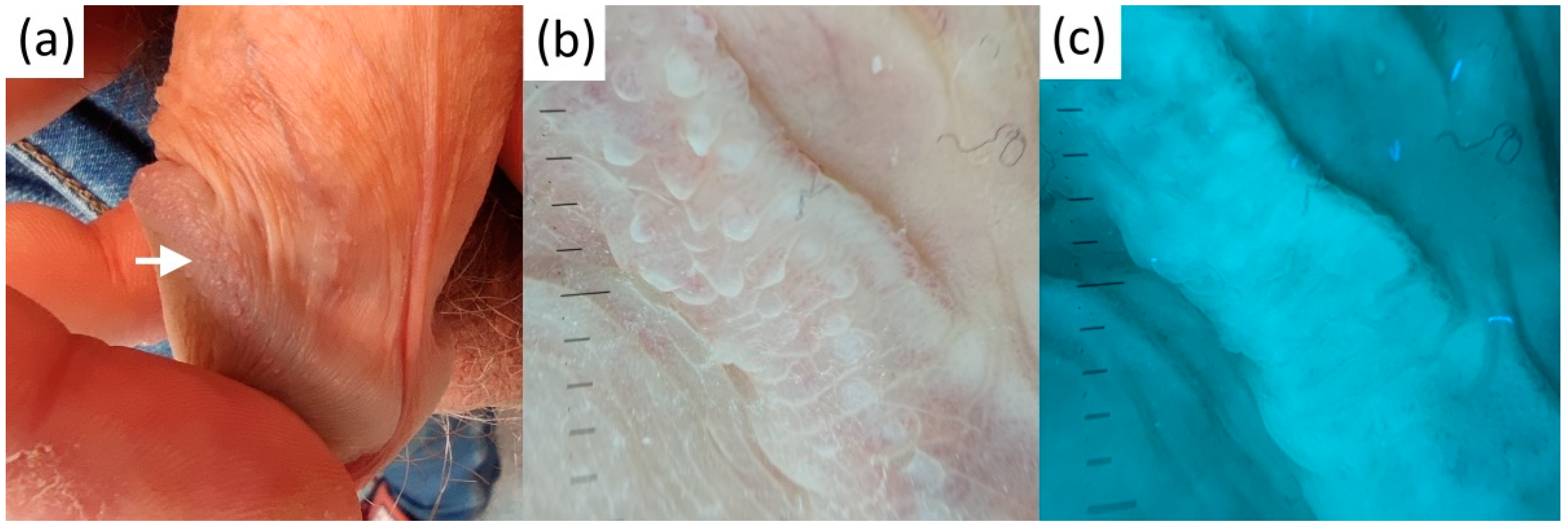
| 4 | 23 | M | Caucasian | Foreskin | Slightly elevated, well-defined yellow-white papules grouped bilaterally in the proximity of frenulum | STI suspect |
| 5 | 35 | M | Caucasian | Upper lip | Flat, poorly defined yellow-white papules grouped along the vermilion | Incidental finding |
| 6 | 28 | M | Caucasian | Foreskin | Slightly elevated, poorly defined scant yellow-white papules located bilaterally in the proximity of frenulum | Incidental finding |
| 7 | 30 | M | Caucasian | Foreskin | Slightly elevated, poorly defined scant yellow-white papules located bilaterally in the proximity of frenulum | Incidental finding |
| 8 | 43 | M | Caucasian | Upper lip | Flat, poorly defined yellow-white papules grouped unilaterally in the vicinity of left labial commissure of the mouth | Incidental finding |
| 9 | 40 | M | Caucasian | Foreskin | Slightly elevated, poorly defined scant yellow-white papules located bilaterally in the proximity of frenulum | STI suspect |
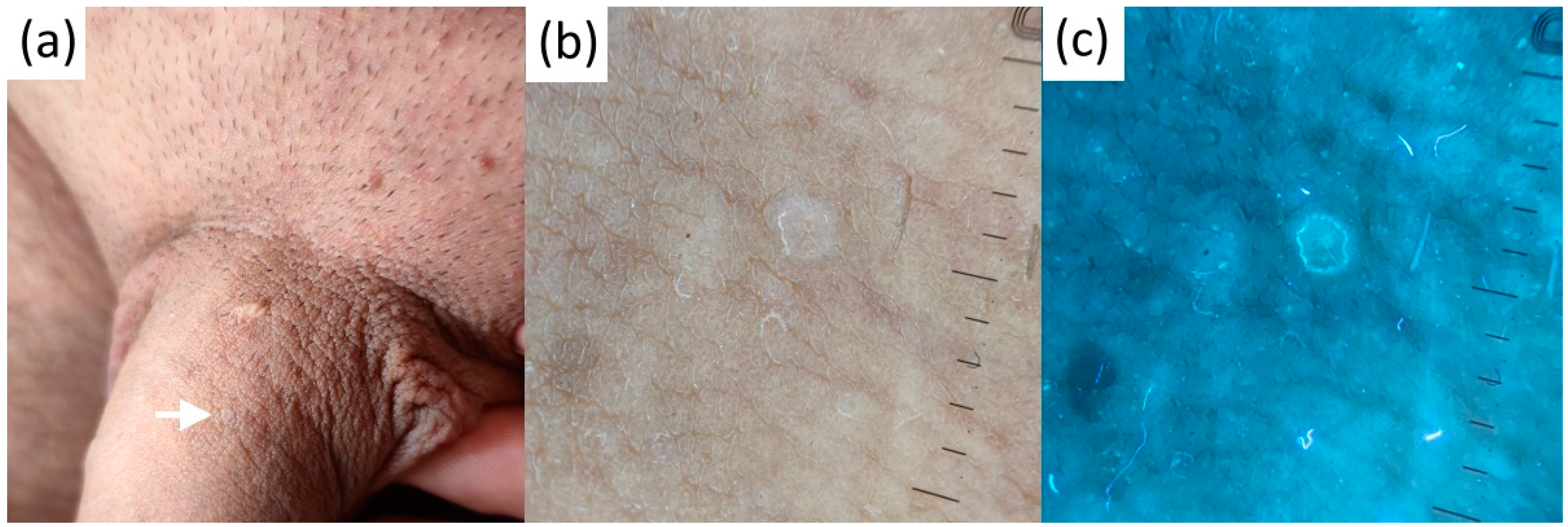
| 10 | 29 | M | Caucasian | Glans | Slightly elevated, poorly defined scant yellow-white papules clustered on the left dorsal surface | Incidental finding |
| 11 | 31 | M | Caucasian | Glans | Elevated, well-defined yellow-white papules clustered on the mid-dorsal surface | STI suspect |
| 12 | 34 | F | Caucasian | Upper lip | Elevated, well-defined yellow-white papules grouped along the vermilion | Incidental finding |
| No | Age | Sex | Ethnicity | Site | Diagnosis/Clinical Presentation | Context |
|---|---|---|---|---|---|---|
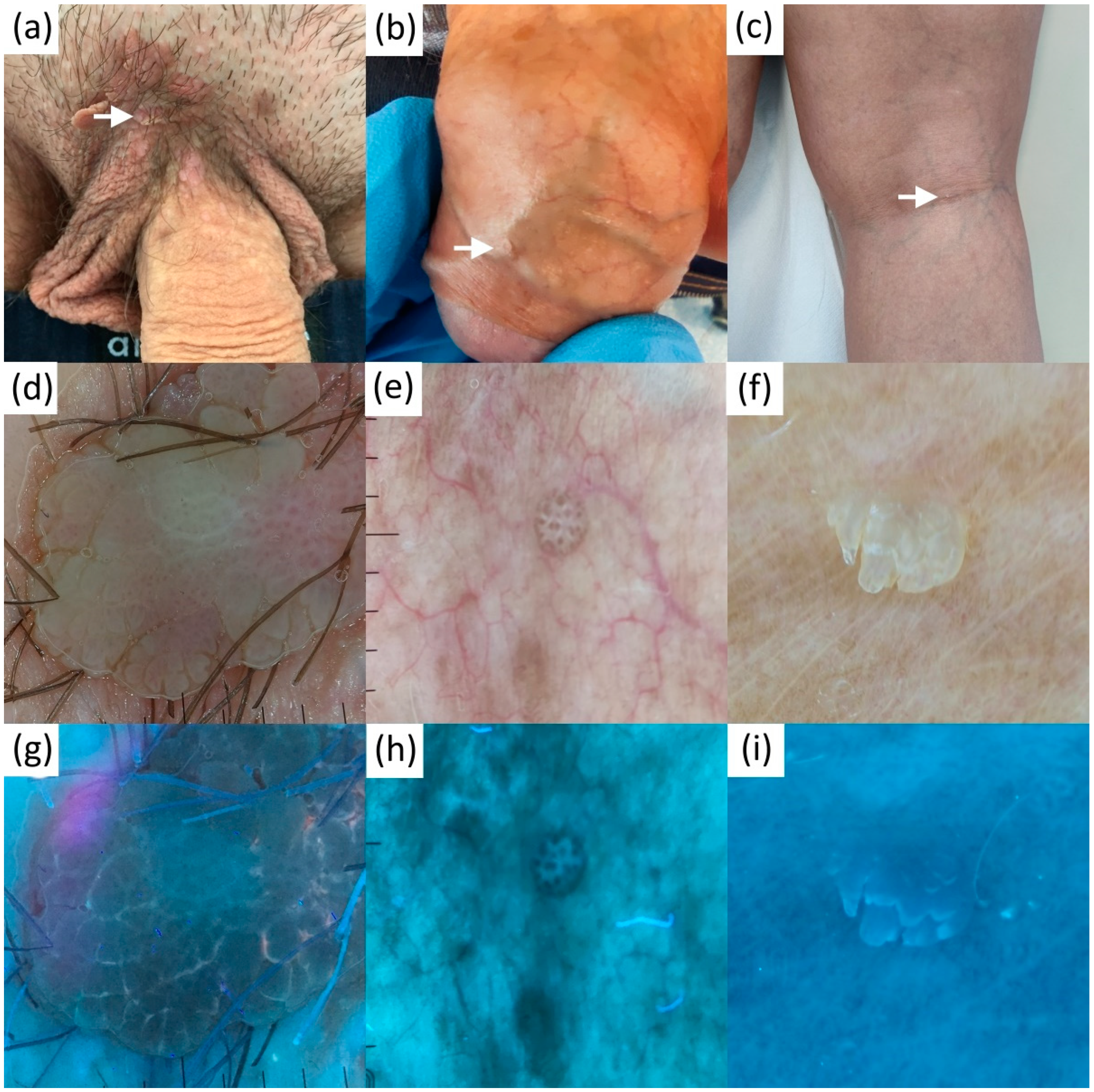
| 1 | 47 | M | Caucasian | Glans | Genital lichen planus/slightly elevated whitepapules and annular lesions on the glans | STI suspect |
| 2 | 23 | M | Caucasian | Glans | Genital lichen planus/coalescing flat-top papules on the glans and foreskin | STI suspect |
| 3 | 9 | F | Caucasian | Pubis | Molluscum contagiosum/solitary umbilicatedpapule | Incidental finding |
| 4.1 | 6 | M | Caucasian | Neck | Molluscum contagiosum/multiple disseminated umbilicated papules | Incidental finding |
| 4.2 | 6 | M | Caucasian | Neck | Molluscum contagiosum/multiple disseminated umbilicated papules | Incidental finding |
| 4.3 | 6 | M | Caucasian | Scalp | Molluscum contagiosum/solitary umbilicatedpapule | Incidental finding |
| 5.1 | 41 | M | Caucasian | Pubis | Molluscum contagiosum/multiple disseminated and grouped umbilicated papules | STI suspect |
| 5.2 | 41 | M | Caucasian | Pubis | Molluscum contagiosum/multiple disseminated and grouped umbilicated papules | STI suspect |
| 5.3 | 41 | M | Caucasian | Pubis | Molluscum contagiosum/multiple disseminated and grouped umbilicated papules | STI suspect |
| 5.4 | 41 | M | Caucasian | Pubis | Molluscum contagiosum/multiple disseminated and grouped umbilicated papules | STI suspect |
| 6 | 28 | M | Caucasian | Glans | Penile pearly papules/multiple white papuleslocated on the corona of the penis | STI suspect |
| 7 | 43 | M | Caucasian | Glans | Penile pearly papules/multiple white papuleslocated on the corona of the penis | Incidental finding |
| 8 | 31 | M | Caucasian | Glans | Penile pearly papules/multiple white papuleslocated on the corona of the penis | STI suspect |
| 9.1 | 45 | F | Caucasian | Popliteal fossa | Viral wart/solitary hyperkeratotic skin-colored papule | Incidental finding |
| 9.2 | 45 | F | Caucasian | Upper leg | Viral wart/solitary hyperkeratotic skin-colored papule | Incidental finding |
| 10 | 21 | M | Caucasian | Areola | Viral wart/solitary hyperkeratotic skin-colored papule | Incidental finding |
| 11 | 47 | M | Caucasian | Foreskin | Viral wart/solitary skin-colored papule | STI suspect |
| 12 | 35 | M | Caucasian | Penile shaft | Viral wart/multiple disseminated skin-colored papules | STI suspect |
| 13 | 44 | M | Caucasian | Pubis | Viral wart/multiple disseminated skin-colored papules | STI suspect |
| 14 | 32 | M | Caucasian | Penile shaft | Genital porokeratosis/disseminated scaly papules in the genital area | STI suspect |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pietkiewicz, P.; Navarrete-Dechent, C.; Goldust, M.; Korecka, K.; Todorovska, V.; Errichetti, E. Differentiating Fordyce Spots from Their Common Simulators Using Ultraviolet-Induced Fluorescence Dermatoscopy—Retrospective Study. Diagnostics 2023, 13, 985. https://doi.org/10.3390/diagnostics13050985
Pietkiewicz P, Navarrete-Dechent C, Goldust M, Korecka K, Todorovska V, Errichetti E. Differentiating Fordyce Spots from Their Common Simulators Using Ultraviolet-Induced Fluorescence Dermatoscopy—Retrospective Study. Diagnostics. 2023; 13(5):985. https://doi.org/10.3390/diagnostics13050985
Chicago/Turabian StylePietkiewicz, Paweł, Cristian Navarrete-Dechent, Mohamad Goldust, Katarzyna Korecka, Verce Todorovska, and Enzo Errichetti. 2023. "Differentiating Fordyce Spots from Their Common Simulators Using Ultraviolet-Induced Fluorescence Dermatoscopy—Retrospective Study" Diagnostics 13, no. 5: 985. https://doi.org/10.3390/diagnostics13050985