
Replacing Endoscopy with Magnetic Resonance Enterography for Mucosal Activity Assessment in Terminal Ileal Crohn’s Disease: Are We There Yet?

Abstract
:1. Introduction
2. MRE Parameters That Correlate with Disease Activity
2.1. Bowel Wall Thickness
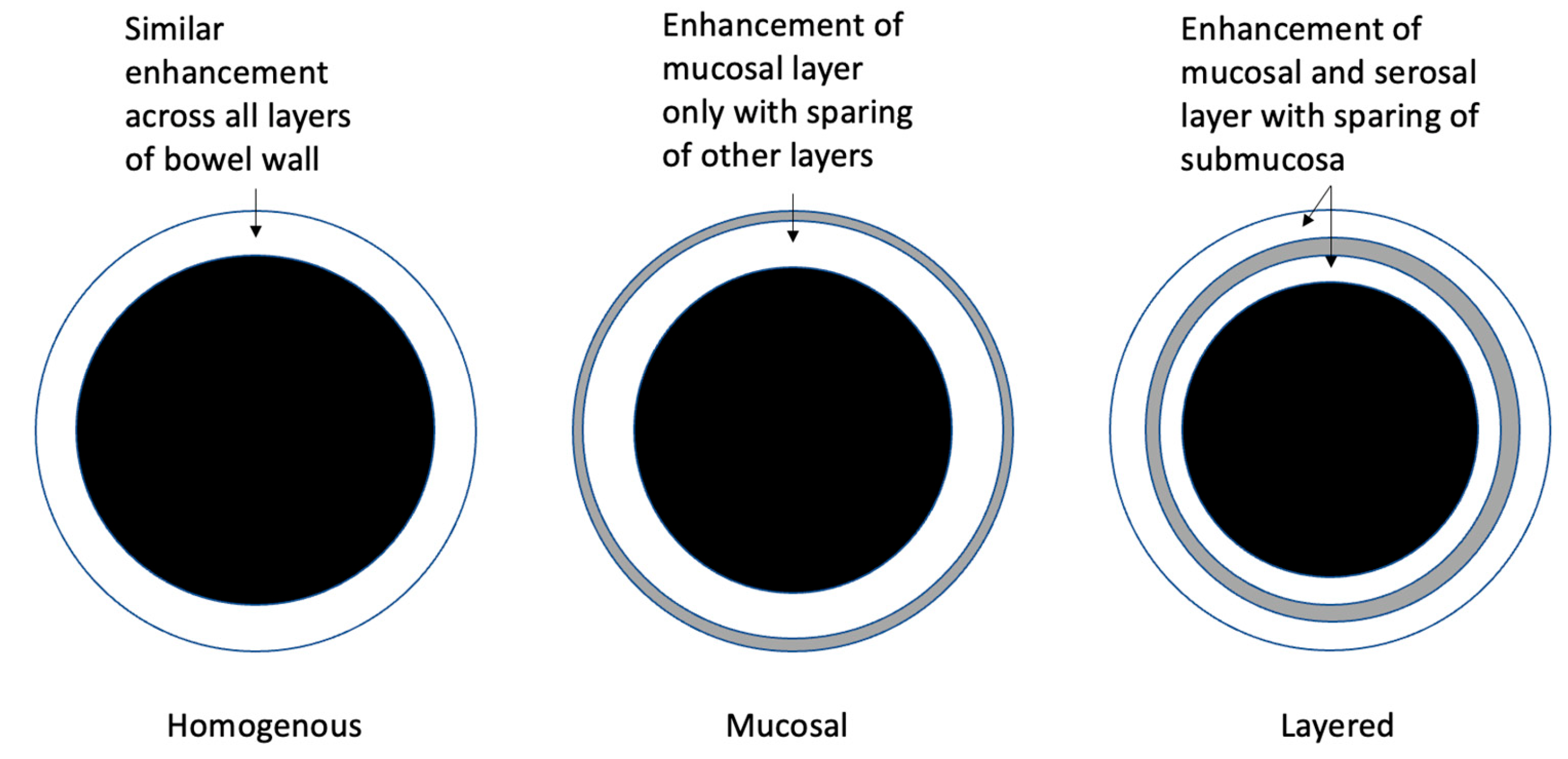
2.2. Bowel Wall Contrast Enhancement
2.3. T2 Mural Signal Intensity/Intramural Oedema
2.4. Ulceration
2.5. Diffusion-Weighted Imaging
2.6. Stenosis and Pre-Stenotic Dilatation
2.7. Motility Sequence Assessment/Cine Sequences
2.8. Fibrofatty Proliferation/Creeping Fat
2.9. Mesenteric Vascularity (Comb Sign)
2.10. Inflammatory Lymph Nodes
2.11. Abscess Detection
2.12. Enteric Fistula
3. Overall Accuracy of MRE for Detection of SMALL Bowel CD Activity
4. The Utility of MRE Indices for Evaluation of CD Activity at MUCOSAL Level

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Index/Modality | Study Design | N = | Reference Index | Parameters Included | Segment Assessed | Formula | Statistical Assessment | Bowel Prep./Rectal Water Instilled? | External Validation? |
|---|---|---|---|---|---|---|---|---|---|---|
| Rimola et al. [10] | MaRIA/MRE | R | 50 | C (CDEIS) | BWT RCE Oedema Ulceration | TI AC TC DC SC Rectum | MaRIA (segmental) = 1.5 × BWT (mm) + 0.02 × RCE + 5 × oedema + 10 × ulceration MaRIA (global) = sum of all segments | Correlation with CDEIS: r = 0.82 Detection of disease activity (ileum and large bowel): AUC = 0.891, sensitivity = 0.81, specificity 0.89 | Yes/Yes | Yes [47,56] |
| Steward et al. [26] | CDMI/MRE | R | 16 | Histology (AIS) | BWT Mural T2 score | TI | CDMI = 1.79 + 1.34 mural thickness + 0.94 mural T2 score | Correlation with histology (AIS): Kendalls tau = 0.40, 95% CI (0.11–0.64) Detection of active TI disease using cut off >4.1: AUC 0.77, sensitivity 81% (95% CI (54–96)), specificity 70% (35–93) | No/No | Yes [47] |
| Steward et al. [26] | London Index/MRE | R | 12 | Histology (AIS) | BWT Mural T2 score Perimural T2 signal Contrast enhancement | TI | London Index = mural thickness + mural T2 score + perimural T2 signal + contrast enhancement | Detection of active TI disease using cut off >3: AUC 0.83, sensitivity 87% (61–98), specificity 70% (35–93) | No/No | Yes [46] |
| Buisson et al. [48] | Clermont/MRE | P | 31 | MRE (MaRIA) | BWT Ulcers Oedema ADC | TI | Clermont = −1.321 × ADC (mm2/s) + 1.646 × wall thickening + 8.306 × ulcers + 5.613 × oedema + 5.039 | No difference found between original MaRIA score (R² = 0.998) and Clermont score (R² = 0.989) | No/No | Yes [56] |
| Ordas et al. [19] | sMaRIA/MRE | R | 98D 37V | C (CDEIS) | BWT oedema Perienteric fat stranding Ulcers | TI AC TC DC SC Rectum | sMaRIA (segmental) = 1 (1 × thickness >3 mm) + (1 × oedema) + (1 × fat stranding) + (2 × ulcers) sMaRIA (global) = addition of all segments | Correlation with CDEIS: r = 0.83 Detection of disease activity (ileum and large bowel): AUC = 0.91, sensitivity 90%, specificity 81% | Yes/Yes | Yes [57] |
| Thierry et al. | Nancy/MRE | P | 20 | C (CDEIS) | Ulceration Parietal oedema BWT differentiation between (sub) mucosa and muscularis propria Rapid contrast enhancement, DWI hyperintensity | TIRCTCLCSCRectum | Nancy Index (segmental) = ulceration + parietal oedema + BWT + differentiation between (sub)mucosa and muscularis propria + rapid contrast enhancement + DWI hyperintensity 1 point for each parameter present. Maximum 6 points. | Detection of disease activity: AUC 0.80, sensitivity 92%, specificity 68% | No/No | Yes [52] |
| Score | Active Disease | Severe Disease |
|---|---|---|
| MaRIA (segmental) | ≥7 | ≥11 |
| sMaRIA (segmental) | >1 | >2 |
| Clermont (segmental) | >8.4 | ≥12.5 |
| Nancy (segmental) | ≥2 | |
| CDMI | ≥4.1 | |
| London Index | >3 |
5. The Utility of MRE to Assess Response to Therapy at Mucosal Level Either via Individual MRE Parameters or MRE Indices
6. The Utility of MRE for Detection of Post-Operative Recurrence in CD
7. Persistently Abnormal MRE Findings in the Setting of Normal Endoscopy
8. The Impact of Concurrent Fibrosis on the Utility of MRE in the Assessment of Mucosal Activity in CD
9. Limitations of MRE
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ng, S.C.; Shi, H.Y.; Hamidi, N.; Underwood, F.E.; Tang, W.; Benchimol, E.I.; Panaccione, R.; Ghosh, S.; Wu, J.C.; Chan, F.K.; et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: A systematic review of population-based studies. Lancet 2017, 390, 2769–2778. [Google Scholar] [CrossRef]
- Voderholzer, W.A.; Beinhoelzl, J.; Rogalla, P.; Murrer, S.; Schachschal, G.; Lochs, H.; Ortner, M.A. Small bowel involvement in Crohn’s disease: A prospective comparison of wireless capsule endoscopy and computed tomography enteroclysis. Gut 2005, 54, 369–373. [Google Scholar] [CrossRef] [PubMed]
- Argüelles-Arias, F.; Rodríguez-Oballe, J.; Duarte-Chang, C.; Castro-Laria, L.; García-Montes, J.M.; Caunedo-Álvarez, A.; Herrerías-Gutiérrez, J.M. Capsule endoscopy in the small bowel Crohn’s disease. Gastroenterol. Res. Pract. 2014, 2014, 529136. [Google Scholar] [CrossRef]
- Peyrin-Biroulet, L.; Loftus, E.V.; Colombel, J.F.; Sandborn, W.J. Long-term complications, extraintestinal manifestations, and mortality in adult Crohn’s disease in population-based cohorts. Inflamm. Bowel Dis. 2011, 17, 471–478. [Google Scholar] [CrossRef]
- Gajendran, M.; Loganathan, P.; Catinella, A.P.; Hashash, J.G. A comprehensive review and update on Crohn’s disease. Dis. Mon. 2018, 64, 20–57. [Google Scholar] [CrossRef]
- Maaser, C.; Sturm, A.; Vavricka, S.R.; Kucharzik, T.; Fiorino, G.; Annese, V.; Calabrese, E.; Baumgart, D.C.; Bettenworth, D.; Borralho Nunes, P.; et al. ECCO-ESGAR Guideline for Diagnostic Assessment in IBD Part 1: Initial diagnosis, monitoring of known IBD, detection of complications. J. Crohn’s Colitis 2019, 13, 144–164. [Google Scholar] [CrossRef] [Green Version]
- Turner, D.; Ricciuto, A.; Lewis, A.; D’Amico, F.; Dhaliwal, J.; Griffiths, A.M.; Bettenworth, D.; Sandborn, W.J.; Sands, B.E.; Reinisch, W.; et al. STRIDE-II: An Update on the Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) Initiative of the International Organization for the Study of IBD (IOIBD): Determining Therapeutic Goals for Treat-to-Target strategies in IBD. Gastroenterology 2021, 160, 1570–1583. [Google Scholar] [CrossRef] [PubMed]
- Peyrin-Biroulet, L.; Sandborn, W.; Sands, B.E.; Reinisch, W.; Bemelman, W.; Bryant, R.V.; D’Haens, G.; Dotan, I.; Dubinsky, M.; Feagan, B.; et al. Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE): Determining Therapeutic Goals for Treat-to-Target. Am. J. Gastroenterol. 2015, 110, 1324–1338. [Google Scholar] [CrossRef] [PubMed]
- Börsch, G.; Schmidt, G. Endoscopy of the terminal ileum. Diagnostic yield in 400 consecutive examinations. Dis. Colon Rectum 1985, 28, 499–501. [Google Scholar] [CrossRef] [PubMed]
- Rimola, J.; Rodriguez, S.; García-Bosch, O.; Ordás, I.; Ayala, E.; Aceituno, M.; Pellisé, M.; Ayuso, C.; Ricart, E.; Donoso, L.; et al. Magnetic resonance for assessment of disease activity and severity in ileocolonic Crohn’s disease. Gut 2009, 58, 1113–1120. [Google Scholar] [CrossRef] [Green Version]
- Guglielmo, F.F.; Anupindi, S.A.; Fletcher, J.G.; Al-Hawary, M.M.; Dillman, J.R.; Grand, D.J.; Bruining, D.H.; Chatterji, M.; Darge, K.; Fidler, J.L.; et al. Small Bowel Crohn Disease at CT and MR Enterography: Imaging Atlas and Glossary of Terms. Radiographics 2020, 40, 354–375. [Google Scholar] [CrossRef] [PubMed]
- Bruining, D.H.; Zimmermann, E.M.; Loftus, E.V.; Sandborn, W.J.; Sauer, C.G.; Strong, S.A.; Society of Abdominal Radiology Crohn’s Disease-Focused Panel. Consensus Recommendations for Evaluation, Interpretation, and Utilization of Computed Tomography and Magnetic Resonance Enterography in Patients With Small Bowel Crohn’s Disease. Radiology 2018, 286, 776–799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zappa, M.; Stefanescu, C.; Cazals-Hatem, D.; Bretagnol, F.; Deschamps, L.; Attar, A.; Larroque, B.; Tréton, X.; Panis, Y.; Vilgrain, V.; et al. Which magnetic resonance imaging findings accurately evaluate inflammation in small bowel Crohn’s disease? A retrospective comparison with surgical pathologic analysis. Inflamm. Bowel Dis. 2011, 17, 984–993. [Google Scholar] [CrossRef]
- Rimola, J.; Planell, N.; Rodríguez, S.; Delgado, S.; Ordás, I.; Ramírez-Morros, A.; Ayuso, C.; Aceituno, M.; Ricart, E.; Jauregui-Amezaga, A.; et al. Characterization of inflammation and fibrosis in Crohn’s disease lesions by magnetic resonance imaging. Am. J. Gastroenterol. 2015, 110, 432–440. [Google Scholar] [CrossRef]
- Coimbra, A.; Rimola, J.; Cuatrecasas, M.; De Hertogh, G.; Van Assche, G.; Vanslembrouck, R.; Glerup, H.; Nielsen, A.H.; Hagemann-Madsen, R.; Bouhnik, Y.; et al. Magnetic Resonance Enterography and Histology in Patients With Fibrostenotic Crohn’s Disease: A Multicenter Study. Clin. Transl. Gastroenterol. 2022, 13, e00505. [Google Scholar] [CrossRef]
- Capozzi, N.; Ordás, I.; Fernandez-Clotet, A.; Castro-Poceiro, J.; Rodríguez, S.; Alfaro, I.; Sapena, V.; Masamunt, M.C.; Ricart, E.; Panés, J.; et al. Validation of the Simplified Magnetic Resonance Index of Activity [sMARIA] Without Gadolinium-enhanced Sequences for Crohn’s Disease. J. Crohn’s Colitis 2020, 14, 1074–1081. [Google Scholar] [CrossRef]
- Ordás, I.; Rimola, J.; Rodríguez, S.; Paredes, J.M.; Martínez-Pérez, M.J.; Blanc, E.; Arévalo, J.A.; Aduna, M.; Andreu, M.; Radosevic, A.; et al. Accuracy of magnetic resonance enterography in assessing response to therapy and mucosal healing in patients with Crohn’s disease. Gastroenterology 2014, 146, 374–382.e1. [Google Scholar] [CrossRef] [PubMed]
- Rimola, J.; Ordás, I.; Rodriguez, S.; García-Bosch, O.; Aceituno, M.; Llach, J.; Ayuso, C.; Ricart, E.; Panés, J. Magnetic resonance imaging for evaluation of Crohn’s disease: Validation of parameters of severity and quantitative index of activity. Inflamm. Bowel Dis. 2011, 17, 1759–1768. [Google Scholar] [CrossRef]
- Ordás, I.; Rimola, J.; Alfaro, I.; Rodríguez, S.; Castro-Poceiro, J.; Ramírez-Morros, A.; Gallego, M.; Giner, À.; Barastegui, R.; Fernández-Clotet, A.; et al. Development and Validation of a Simplified Magnetic Resonance Index of Activity for Crohn’s Disease. Gastroenterology 2019, 157, 432–439. [Google Scholar] [CrossRef] [Green Version]
- Sato, H.; Tamura, C.; Narimatsu, K.; Shimizu, M.; Takajyo, T.; Yamashita, M.; Inoue, Y.; Ozaki, H.; Furuhashi, H.; Maruta, K.; et al. Magnetic resonance enterocolonography in detecting erosion and redness in intestinal mucosa of patients with Crohn’s disease. J. Gastroenterol. Hepatol. 2015, 30, 667–673. [Google Scholar] [CrossRef]
- Jairath, V.; Ordas, I.; Zou, G.; Panes, J.; Stoker, J.; Taylor, S.A.; Santillan, C.; Horsthuis, K.; Samaan, M.A.; Shackelton, L.M.; et al. Reliability of Measuring Ileo-Colonic Disease Activity in Crohn’s Disease by Magnetic Resonance Enterography. Inflamm. Bowel Dis. 2018, 24, 440–449. [Google Scholar] [CrossRef] [PubMed]
- Bellini, D.; Rivosecchi, F.; Panvini, N.; Rengo, M.; Caruso, D.; Carbone, I.; Ferrari, R.; Paolantonio, P.; Laghi, A. Layered enhancement at magnetic resonance enterography in inflammatory bowel disease: A meta-analysis. World J. Gastroenterol. 2019, 25, 4555–4566. [Google Scholar] [CrossRef] [PubMed]
- Punwani, S.; Rodriguez-Justo, M.; Bainbridge, A.; Greenhalgh, R.; De Vita, E.; Bloom, S.; Cohen, R.; Windsor, A.; Obichere, A.; Hansmann, A.; et al. Mural inflammation in Crohn disease: Location-matched histologic validation of MR imaging features. Radiology 2009, 252, 712–720. [Google Scholar] [CrossRef] [PubMed]
- Knuesel, P.R.; Kubik, R.A.; Crook, D.W.; Eigenmann, F.; Froehlich, J.M. Assessment of dynamic contrast enhancement of the small bowel in active Crohn’s disease using 3D MR enterography. Eur. J. Radiol. 2010, 73, 607–613. [Google Scholar] [CrossRef]
- Tielbeek, J.A.; Ziech, M.L.; Li, Z.; Lavini, C.; Bipat, S.; Bemelman, W.A.; Roelofs, J.J.; Ponsioen, C.Y.; Vos, F.M.; Stoker, J. Evaluation of conventional, dynamic contrast enhanced and diffusion weighted MRI for quantitative Crohn’s disease assessment with histopathology of surgical specimens. Eur. Radiol. 2014, 24, 619–629. [Google Scholar] [CrossRef] [PubMed]
- Steward, M.J.; Punwani, S.; Proctor, I.; Adjei-Gyamfi, Y.; Chatterjee, F.; Bloom, S.; Novelli, M.; Halligan, S.; Rodriguez-Justo, M.; Taylor, S.A. Non-perforating small bowel Crohn’s disease assessed by MRI enterography: Derivation and histopathological validation of an MR-based activity index. Eur. J. Radiol. 2012, 81, 2080–2088. [Google Scholar] [CrossRef] [PubMed]
- Sinha, R.; Verma, R.; Verma, S.; Rajesh, A. MR enterography of Crohn disease: Part 2, imaging and pathologic findings. AJR Am. J. Roentgenol. 2011, 197, 80–85. [Google Scholar] [CrossRef] [Green Version]
- Dohan, A.; Taylor, S.; Hoeffel, C.; Barret, M.; Allez, M.; Dautry, R.; Zappa, M.; Savoye-Collet, C.; Dray, X.; Boudiaf, M.; et al. Diffusion-weighted MRI in Crohn’s disease: Current status and recommendations. J. Magn. Reson. Imaging 2016, 44, 1381–1396. [Google Scholar] [CrossRef] [Green Version]
- Choi, S.H.; Kim, K.W.; Lee, J.Y.; Kim, K.J.; Park, S.H. Diffusion-weighted Magnetic Resonance Enterography for Evaluating Bowel Inflammation in Crohn’s Disease: A Systematic Review and Meta-analysis. Inflamm. Bowel Dis. 2016, 22, 669–679. [Google Scholar] [CrossRef]
- Rimola, J.E. Cross-Sectional Imaging in Crohn’s Disease, 1st ed.; Springer International Publishing: Cham, Switzerland, 2019. [Google Scholar]
- Rimola, J.; Capozzi, N. Differentiation of fibrotic and inflammatory component of Crohn’s disease-associated strictures. Intest. Res. 2020, 18, 144–150. [Google Scholar] [CrossRef]
- Takenaka, K.; Ohtsuka, K.; Kitazume, Y.; Nagahori, M.; Fujii, T.; Saito, E.; Naganuma, M.; Araki, A.; Watanabe, M. Comparison of magnetic resonance and balloon enteroscopic examination of the small intestine in patients with Crohn’s disease. Gastroenterology 2014, 147, 334–342.e3. [Google Scholar] [CrossRef]
- Bettenworth, D.; Bokemeyer, A.; Baker, M.; Mao, R.; Parker, C.E.; Nguyen, T.; Ma, C.; Panés, J.; Rimola, J.; Fletcher, J.G.; et al. Assessment of Crohn’s disease-associated small bowel strictures and fibrosis on cross-sectional imaging: A systematic review. Gut 2019, 68, 1115–1126. [Google Scholar] [CrossRef] [Green Version]
- Wnorowski, A.M.; Guglielmo, F.F.; Mitchell, D.G. How to perform and interpret cine MR enterography. J. Magn. Reson. Imaging 2015, 42, 1180–1189. [Google Scholar] [CrossRef] [PubMed]
- Menys, A.; Butt, S.; Emmanuel, A.; Plumb, A.A.; Fikree, A.; Knowles, C.; Atkinson, D.; Zarate, N.; Halligan, S.; Taylor, S.A. Comparative quantitative assessment of global small bowel motility using magnetic resonance imaging in chronic intestinal pseudo-obstruction and healthy controls. Neurogastroenterol. Motil. 2016, 28, 376–383. [Google Scholar] [CrossRef]
- Menys, A.; Puylaert, C.; Tutein Nolthenius, C.E.; Plumb, A.A.; Makanyanga, J.; Tielbeek, J.A.; Pendse, D.; Brosens, L.A.; Rodriguez-Justo, M.; Atkinson, D.; et al. Quantified Terminal Ileal Motility during MR Enterography as a Biomarker of Crohn Disease Activity: Prospective Multi-Institution Study. Radiology 2018, 289, 428–435. [Google Scholar] [CrossRef]
- Dreja, J.; Ekberg, O.; Leander, P.; Månsson, S.; Ohlsson, B. Volumetric analysis of small bowel motility in an unselected cohort of patients with Crohn’s disease. Neurogastroenterol. Motil. 2020, 32, e13909. [Google Scholar] [CrossRef] [PubMed]
- Coffey, J.C.; Byrnes, K.G.; Walsh, D.J.; Cunningham, R.M. Update on the mesentery: Structure, function, and role in disease. Lancet Gastroenterol. Hepatol. 2022, 7, 96–106. [Google Scholar] [CrossRef]
- Rimola, J.; Alfaro, I.; Fernández-Clotet, A.; Castro-Poceiro, J.; Vas, D.; Rodríguez, S.; Masamunt, M.C.; Ordás, I.; Ricart, E.; Panés, J. Persistent damage on magnetic resonance enterography in patients with Crohn’s disease in endoscopic remission. Aliment. Pharm. 2018, 48, 1232–1241. [Google Scholar] [CrossRef] [PubMed]
- Colombel, J.F.; Solem, C.A.; Sandborn, W.J.; Booya, F.; Loftus, E.V.; Harmsen, W.S.; Zinsmeister, A.R.; Bodily, K.D.; Fletcher, J.G. Quantitative measurement and visual assessment of ileal Crohn’s disease activity by computed tomography enterography: Correlation with endoscopic severity and C reactive protein. Gut 2006, 55, 1561–1567. [Google Scholar] [CrossRef] [Green Version]
- Panés, J.; Bouzas, R.; Chaparro, M.; García-Sánchez, V.; Gisbert, J.P.; Martínez de Guereñu, B.; Mendoza, J.L.; Paredes, J.M.; Quiroga, S.; Ripollés, T.; et al. Systematic review: The use of ultrasonography, computed tomography and magnetic resonance imaging for the diagnosis, assessment of activity and abdominal complications of Crohn’s disease. Aliment. Pharm. 2011, 34, 125–145. [Google Scholar] [CrossRef]
- Taylor, S.A.; Mallett, S.; Bhatnagar, G.; Baldwin-Cleland, R.; Bloom, S.; Gupta, A.; Hamlin, P.J.; Hart, A.L.; Higginson, A.; Jacobs, I.; et al. Diagnostic accuracy of magnetic resonance enterography and small bowel ultrasound for the extent and activity of newly diagnosed and relapsed Crohn’s disease (METRIC): A multicentre trial. Lancet Gastroenterol. Hepatol. 2018, 3, 548–558. [Google Scholar] [CrossRef]
- Qiu, Y.; Mao, R.; Chen, B.L.; Li, X.H.; He, Y.; Zeng, Z.R.; Li, Z.P.; Chen, M.H. Systematic review with meta-analysis: Magnetic resonance enterography vs. computed tomography enterography for evaluating disease activity in small bowel Crohn’s disease. Aliment. Pharm. 2014, 40, 134–146. [Google Scholar] [CrossRef]
- Liu, W.; Liu, J.; Xiao, W.; Luo, G. A Diagnostic Accuracy Meta-analysis of CT and MRI for the Evaluation of Small Bowel Crohn Disease. Acad. Radiol. 2017, 24, 1216–1225. [Google Scholar] [CrossRef] [PubMed]
- Rozendorn, N.; Amitai, M.M.; Eliakim, R.A.; Kopylov, U.; Klang, E. A review of magnetic resonance enterography-based indices for quantification of Crohn’s disease inflammation. Ther. Adv. Gastroenterol. 2018, 11, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Kumar, S.; Parry, T.; Mallett, S.; Bhatnagar, G.; Plumb, A.; Walsh, S.; Scott, N.; Tandon, R.; Chong, H.; du Parcq, J.; et al. Diagnostic performance of magnetic resonance enterography disease activity indices compared with a histological reference standard for adult terminal ileal Crohn’s disease: Experience from the METRIC trial. J. Crohn’s Colitis 2022, 16, 1531–1539. [Google Scholar] [CrossRef]
- Tielbeek, J.A.; Makanyanga, J.C.; Bipat, S.; Pendsé, D.A.; Nio, C.Y.; Vos, F.M.; Taylor, S.A.; Stoker, J. Grading Crohn disease activity with MRI: Interobserver variability of MRI features, MRI scoring of severity, and correlation with Crohn disease endoscopic index of severity. Am. J. Roentgenol. 2013, 201, 1220–1228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buisson, A.; Joubert, A.; Montoriol, P.F.; Da Ines, D.; Ines, D.D.; Hordonneau, C.; Pereira, B.; Garcier, J.M.; Bommelaer, G.; Petitcolin, V. Diffusion-weighted magnetic resonance imaging for detecting and assessing ileal inflammation in Crohn’s disease. Aliment. Pharm. 2013, 37, 537–545. [Google Scholar] [CrossRef]
- Hordonneau, C.; Buisson, A.; Scanzi, J.; Goutorbe, F.; Pereira, B.; Borderon, C.; Da Ines, D.; Montoriol, P.F.; Garcier, J.M.; Boyer, L.; et al. Diffusion-weighted magnetic resonance imaging in ileocolonic Crohn’s disease: Validation of quantitative index of activity. Am. J. Gastroenterol. 2014, 109, 89–98. [Google Scholar] [CrossRef]
- Puylaert, C.A.J.; Nolthenius, C.J.T.; Tielbeek, J.A.W.; Makanyanga, J.C.; Rodriguez-Justo, M.; Brosens, L.A.A.; Nio, C.Y.; Pendsé, D.A.; Ponsioen, C.Y.; Vos, F.M.; et al. Comparison of MRI Activity Scoring Systems and Features for the Terminal Ileum in Patients With Crohn Disease. AJR Am. J. Roentgenol. 2019, 212, W25–W31. [Google Scholar] [CrossRef]
- Oussalah, A.; Laurent, V.; Bruot, O.; Bressenot, A.; Bigard, M.A.; Régent, D.; Peyrin-Biroulet, L. Diffusion-weighted magnetic resonance without bowel preparation for detecting colonic inflammation in inflammatory bowel disease. Gut 2010, 59, 1056–1065. [Google Scholar] [CrossRef] [PubMed]
- Thierry, M.L.; Rousseau, H.; Pouillon, L.; Girard-Gavanier, M.; Baumann, C.; Lopez, A.; Danese, S.; Laurent, V.; Peyrin-Biroulet, L. Accuracy of Diffusion-weighted Magnetic Resonance Imaging in Detecting Mucosal Healing and Treatment Response, and in Predicting Surgery, in Crohn’s Disease. J. Crohn’s Colitis 2018, 12, 1180–1190. [Google Scholar] [CrossRef] [PubMed]
- Kitazume, Y.; Fujioka, T.; Takenaka, K.; Oyama, J.; Ohtsuka, K.; Fujii, T.; Tateisi, U. Crohn Disease: A 5-Point MR Enterocolonography Classification Using Enteroscopic Findings. Am. J. Roentgenol. 2019, 212, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Pariente, B.; Mary, J.Y.; Danese, S.; Chowers, Y.; De Cruz, P.; D’Haens, G.; Loftus, E.V.; Louis, E.; Panés, J.; Schölmerich, J.; et al. Development of the Lémann index to assess digestive tract damage in patients with Crohn’s disease. Gastroenterology 2015, 148, 52–63.e3. [Google Scholar] [CrossRef] [PubMed]
- Rimola, J.; Alvarez-Cofiño, A.; Pérez-Jeldres, T.; Ayuso, C.; Alfaro, I.; Rodríguez, S.; Ricart, E.; Ordás, I.; Panés, J. Comparison of three magnetic resonance enterography indices for grading activity in Crohn’s disease. J. Gastroenterol. 2017, 52, 585–593. [Google Scholar] [CrossRef] [Green Version]
- Caruso, A.; D’Incà, R.; Scarpa, M.; Manfrin, P.; Rudatis, M.; Pozza, A.; Angriman, I.; Buda, A.; Sturniolo, G.C.; Lacognata, C. Diffusion-weighted magnetic resonance for assessing ileal Crohn’s disease activity. Inflamm. Bowel Dis. 2014, 20, 1575–1583. [Google Scholar] [CrossRef]
- Williet, N.; Jardin, S.; Roblin, X. The Simplified Magnetic Resonance Index of Activity (MARIA) for Crohn’s Disease Is Strongly Correlated With the MARIA and Clermont Score: An External Validation. Gastroenterology 2020, 158, 282–283. [Google Scholar] [CrossRef]
- Tielbeek, J.A.; Löwenberg, M.; Bipat, S.; Horsthuis, K.; Ponsioen, C.Y.; D’Haens, G.R.; Stoker, J. Serial magnetic resonance imaging for monitoring medical therapy effects in Crohn’s disease. Inflamm. Bowel Dis. 2013, 19, 1943–1950. [Google Scholar] [CrossRef] [PubMed]
- Stoppino, L.P.; Della Valle, N.; Rizzi, S.; Cleopazzo, E.; Centola, A.; Iamele, D.; Bristogiannis, C.; Stoppino, G.; Vinci, R.; Macarini, L. Magnetic resonance enterography changes after antibody to tumor necrosis factor (anti-TNF) alpha therapy in Crohn’s disease: Correlation with SES-CD and clinical-biological markers. BMC Med. Imaging 2016, 16, 37. [Google Scholar] [CrossRef] [Green Version]
- Minordi, L.M.; Larosa, L.; Belmonte, G.; Scaldaferri, F.; Poscia, A.; Gasbarrini, A.; Manfredi, R. Crohn’s disease activity before and after medical therapy evaluated by MaRIA score and others parameters in MR Enterography. Clin. Imaging 2020, 62, 1–9. [Google Scholar] [CrossRef]
- Rimola, J.; Fernàndez-Clotet, A.; Capozzi, N.; Rojas-Farreras, S.; Alfaro, I.; Rodríguez, S.; Masamunt, M.C.; Ricart, E.; Ordás, I.; Panés, J. Pre-treatment magnetic resonance enterography findings predict the response to TNF-alpha inhibitors in Crohn’s disease. Aliment. Pharm. 2020, 52, 1563–1573. [Google Scholar] [CrossRef]
- Gordic, S.; Bane, O.; Kihira, S.; Peti, S.; Hectors, S.; Torres, J.; Cho, J.; Colombel, J.F.; Taouli, B. Evaluation of ileal Crohn’s disease response to TNF antagonists: Validation of MR enterography for assessing response. Initial results. Eur. J. Radiol. Open 2020, 7, 100217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, R.; Mintz, A.; Lin, M.; Mhlanga, J.; Chiplunker, A.; Salter, A.; Ciorba, M.; Deepak, P.; Fowler, K. Magnetic resonance enterography features of small bowel Crohn’s disease activity: An inter-rater reliability study of small bowel active inflammation in clinical practice setting. Br. J. Radiol. 2019, 92, 20180930. [Google Scholar] [CrossRef] [PubMed]
- Buisson, A.; Pereira, B.; Goutte, M.; Reymond, M.; Allimant, C.; Obritin-Guilhen, H.; Bommelaer, G.; Hordonneau, C. Magnetic resonance index of activity (MaRIA) and Clermont score are highly and equally effective MRI indices in detecting mucosal healing in Crohn’s disease. Dig. Liver Dis. 2017, 49, 1211–1217. [Google Scholar] [CrossRef] [PubMed]
- Buisson, A.; Hordonneau, C.; Goutte, M.; Scanzi, J.; Goutorbe, F.; Klotz, T.; Boyer, L.; Pereira, B.; Bommelaer, G. Diffusion-weighted magnetic resonance enterocolonography in predicting remission after anti-TNF induction therapy in Crohn’s disease. Dig. Liver Dis. 2016, 48, 260–266. [Google Scholar] [CrossRef]
- Rutgeerts, P.; Geboes, K.; Vantrappen, G.; Kerremans, R.; Coenegrachts, J.L.; Coremans, G. Natural history of recurrent Crohn’s disease at the ileocolonic anastomosis after curative surgery. Gut 1984, 25, 665–672. [Google Scholar] [CrossRef] [Green Version]
- Rutgeerts, P.; Geboes, K.; Vantrappen, G.; Beyls, J.; Kerremans, R.; Hiele, M. Predictability of the postoperative course of Crohn’s disease. Gastroenterology 1990, 99, 956–963. [Google Scholar] [CrossRef]
- Dasharathy, S.S.; Limketkai, B.N.; Sauk, J.S. What’s New in the Postoperative Management of Crohn’s Disease? Dig. Dis. Sci. 2022, 67, 3508–3517. [Google Scholar] [CrossRef]
- Sailer, J.; Peloschek, P.; Reinisch, W.; Vogelsang, H.; Turetschek, K.; Schima, W. Anastomotic recurrence of Crohn’s disease after ileocolic resection: Comparison of MR enteroclysis with endoscopy. Eur. Radiol. 2008, 18, 2512–2521. [Google Scholar] [CrossRef]
- Koilakou, S.; Sailer, J.; Peloschek, P.; Ferlitsch, A.; Vogelsang, H.; Miehsler, W.; Fletcher, J.; Turetschek, K.; Schima, W.; Reinisch, W. Endoscopy and MR enteroclysis: Equivalent tools in predicting clinical recurrence in patients with Crohn’s disease after ileocolic resection. Inflamm. Bowel Dis. 2010, 16, 198–203. [Google Scholar] [CrossRef]
- Yung, D.E.; Har-Noy, O.; Tham, Y.S.; Ben-Horin, S.; Eliakim, R.; Koulaouzidis, A.; Kopylov, U. Capsule Endoscopy, Magnetic Resonance Enterography, and Small Bowel Ultrasound for Evaluation of Postoperative Recurrence in Crohn’s Disease: Systematic Review and Meta-Analysis. Inflamm. Bowel Dis. 2017, 24, 93–100. [Google Scholar] [CrossRef] [Green Version]
- Bachour, S.P.; Shah, R.S.; Lyu, R.; Nakamura, T.; Shen, M.; Li, T.; Dane, B.; Barnes, E.L.; Rieder, F.; Cohen, B.; et al. Test Characteristics of Cross-sectional Imaging and Concordance With Endoscopy in Postoperative Crohn’s Disease. Clin. Gastroenterol. Hepatol. 2022, 20, 2327–2336.e4. [Google Scholar] [CrossRef]
- Schaefer, M.; Laurent, V.; Grandmougin, A.; Vuitton, L.; Bourreille, A.; Luc, A.; Clerc-Urmes, I.; Orry, X.; Frampas, E.; De Billy, M.; et al. A Magnetic Resonance Imaging Index to Predict Crohn’s Disease Postoperative Recurrence: The MONITOR Index. Clin. Gastroenterol. Hepatol. 2022, 20, e1040–e1049. [Google Scholar] [CrossRef] [PubMed]
- Geyl, S.; Guillo, L.; Laurent, V.; D’Amico, F.; Danese, S.; Peyrin-Biroulet, L. Transmural healing as a therapeutic goal in Crohn’s disease: A systematic review. Lancet Gastroenterol. Hepatol. 2021, 6, 659–667. [Google Scholar] [CrossRef]
- Lafeuille, P.; Hordonneau, C.; Vignette, J.; Blayac, L.; Dapoigny, M.; Reymond, M.; Rouquette, O.; Sollelis, E.; Boube, M.; Magnin, B.; et al. Transmural healing and MRI healing are associated with lower risk of bowel damage progression than endoscopic mucosal healing in Crohn’s disease. Aliment. Pharm. 2021, 53, 577–586. [Google Scholar] [CrossRef]
- Nehra, A.K.; Sheedy, S.P.; Wells, M.L.; VanBuren, W.M.; Hansel, S.L.; Deepak, P.; Lee, Y.S.; Bruining, D.H.; Fletcher, J.G. Imaging Findings of Ileal Inflammation at Computed Tomography and Magnetic Resonance Enterography: What do They Mean When Ileoscopy and Biopsy are Negative? J. Crohn’s Colitis 2020, 14, 455–464. [Google Scholar] [CrossRef]
- Fernandes, S.R.; Rodrigues, R.V.; Bernardo, S.; Cortez-Pinto, J.; Rosa, I.; da Silva, J.P.; Gonçalves, A.R.; Valente, A.; Baldaia, C.; Santos, P.M.; et al. Transmural Healing Is Associated with Improved Long-term Outcomes of Patients with Crohn’s Disease. Inflamm. Bowel Dis. 2017, 23, 1403–1409. [Google Scholar] [CrossRef]
- Sauer, C.G.; Middleton, J.P.; McCracken, C.; Loewen, J.; Braithwaite, K.; Alazraki, A.; Martin, D.R.; Kugathasan, S. Magnetic Resonance Enterography Healing and Magnetic Resonance Enterography Remission Predicts Improved Outcome in Pediatric Crohn Disease. J. Pediatr. Gastroenterol. Nutr. 2016, 62, 378–383. [Google Scholar] [CrossRef]
- Buisson, A.; Hordonneau, C.; Goutorbe, F.; Allimant, C.; Goutte, M.; Reymond, M.; Pereira, B.; Bommelaer, G. Bowel wall healing assessed using magnetic resonance imaging predicts sustained clinical remission and decreased risk of surgery in Crohn’s disease. J. Gastroenterol. 2019, 54, 312–320. [Google Scholar] [CrossRef]
- Cosnes, J.; Bourrier, A.; Nion-Larmurier, I.; Sokol, H.; Beaugerie, L.; Seksik, P. Factors affecting outcomes in Crohn’s disease over 15 years. Gut 2012, 61, 1140–1145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thia, K.T.; Sandborn, W.J.; Harmsen, W.S.; Zinsmeister, A.R.; Loftus, E.V. Risk factors associated with progression to intestinal complications of Crohn’s disease in a population-based cohort. Gastroenterology 2010, 139, 1147–1155. [Google Scholar] [CrossRef] [Green Version]
- Louis, E.; Collard, A.; Oger, A.F.; Degroote, E.; Aboul Nasr El Yafi, F.A.; Belaiche, J. Behaviour of Crohn’s disease according to the Vienna classification: Changing pattern over the course of the disease. Gut 2001, 49, 777–782. [Google Scholar] [CrossRef] [Green Version]
- Alfredsson, J.; Wick, M.J. Mechanism of fibrosis and stricture formation in Crohn’s disease. Scand. J. Immunol. 2020, 92, e12990. [Google Scholar] [CrossRef]
- Rieder, F.; Latella, G.; Magro, F.; Yuksel, E.S.; Higgins, P.D.; Di Sabatino, A.; de Bruyn, J.R.; Rimola, J.; Brito, J.; Bettenworth, D.; et al. European Crohn’s and Colitis Organisation Topical Review on Prediction, Diagnosis and Management of Fibrostenosing Crohn’s Disease. J. Crohn’s Colitis 2016, 10, 873–885. [Google Scholar] [CrossRef]
- Wilkens, R.; Hagemann-Madsen, R.H.; Peters, D.A.; Nielsen, A.H.; Nørager, C.B.; Glerup, H.; Krogh, K. Validity of Contrast-enhanced Ultrasonography and Dynamic Contrast-enhanced MR Enterography in the Assessment of Transmural Activity and Fibrosis in Crohn’s Disease. J. Crohn’s Colitis 2018, 12, 48–56. [Google Scholar] [CrossRef] [Green Version]
- Wagner, M.; Ko, H.M.; Chatterji, M.; Besa, C.; Torres, J.; Zhang, X.; Panchal, H.; Hectors, S.; Cho, J.; Colombel, J.F.; et al. Magnetic Resonance Imaging Predicts Histopathological Composition of Ileal Crohn’s Disease. J. Crohn’s Colitis 2018, 12, 718–729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.H.; Mao, R.; Huang, S.Y.; Sun, C.H.; Cao, Q.H.; Fang, Z.N.; Zhang, Z.W.; Huang, L.; Lin, J.J.; Chen, Y.J.; et al. Characterization of Degree of Intestinal Fibrosis in Patients with Crohn Disease by Using Magnetization Transfer MR Imaging. Radiology 2018, 287, 494–503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pellino, G.; Nicolai, E.; Catalano, O.A.; Campione, S.; D’Armiento, F.P.; Salvatore, M.; Cuocolo, A.; Selvaggi, F. PET/MR Versus PET/CT Imaging: Impact on the Clinical Management of Small-Bowel Crohn’s Disease. J. Crohn’s Colitis 2016, 10, 277–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moy, M.P.; Sauk, J.; Gee, M.S. The Role of MR Enterography in Assessing Crohn’s Disease Activity and Treatment Response. Gastroenterol. Res. Pract. 2016, 2016, 8168695. [Google Scholar] [CrossRef]
- Bohra, A.; Vasudevan, A.; Kutaiba, N.; Van Langenberg, D.R. Challenges and Strategies to Optimising the Quality of Small Bowel Magnetic Resonance Imaging in Crohn’s Disease. Diagnostics 2022, 12, 2533. [Google Scholar] [CrossRef] [PubMed]
- Ilangovan, R.; Burling, D.; George, A.; Gupta, A.; Marshall, M.; Taylor, S.A. CT enterography: Review of technique and practical tips. Br. J. Radiol. 2012, 85, 876–886. [Google Scholar] [CrossRef] [Green Version]
- Bohra, A.; Van Langenberg, D.R.; Vasudevan, A. Intestinal Ultrasound in the Assessment of Luminal Crohn’s Disease. Gastrointest. Disord. 2022, 4, 24. [Google Scholar] [CrossRef]
- Petruzziello, C.; Calabrese, E.; Onali, S.; Zuzzi, S.; Condino, G.; Ascolani, M.; Zorzi, F.; Pallone, F.; Biancone, L. Small bowel capsule endoscopy vs. conventional techniques in patients with symptoms highly compatible with Crohn’s disease. J. Crohn’s Colitis 2011, 5, 139–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]





| Parameter | Active Inflammatory CD | Fibrostenosing CD | Ideal Imaging Sequence to Detect Individual Parameter |
|---|---|---|---|
| BWT > 3 mm | ü | ü | T1- and T2-weighted sequences |
| Bowel wall contrast enhancement | ü | ü | T1-weighted sequences |
| T2 mural signal intensity/intramural oedema | ü | T2- and diffusion-weighted sequences | |
| Ulceration | ü | T2-weighted sequences | |
| Increased apparent diffusion coeffienct signal | ü | ü | T2-weighted and T1-weighted post-contrast sequences |
| Fibrofatty proliferation/creeping | ü | ü | T1- and T2-weighted sequences |
| Reduced intestinal motility | ü | ü | T1- and T2-weighted sequences |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bohra, A.; Vasudevan, A.; Kutaiba, N.; Van Langenberg, D.R. Replacing Endoscopy with Magnetic Resonance Enterography for Mucosal Activity Assessment in Terminal Ileal Crohn’s Disease: Are We There Yet? Diagnostics 2023, 13, 1061. https://doi.org/10.3390/diagnostics13061061
Bohra A, Vasudevan A, Kutaiba N, Van Langenberg DR. Replacing Endoscopy with Magnetic Resonance Enterography for Mucosal Activity Assessment in Terminal Ileal Crohn’s Disease: Are We There Yet? Diagnostics. 2023; 13(6):1061. https://doi.org/10.3390/diagnostics13061061
Chicago/Turabian StyleBohra, Anuj, Abhinav Vasudevan, Numan Kutaiba, and Daniel Ross Van Langenberg. 2023. "Replacing Endoscopy with Magnetic Resonance Enterography for Mucosal Activity Assessment in Terminal Ileal Crohn’s Disease: Are We There Yet?" Diagnostics 13, no. 6: 1061. https://doi.org/10.3390/diagnostics13061061