
Plasma Fibrinogen as a Predictor of Perioperative-Blood-Component Transfusion in Major-Nontraumatic-Orthopedic-Surgery Patients: A Cohort Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
Statistics
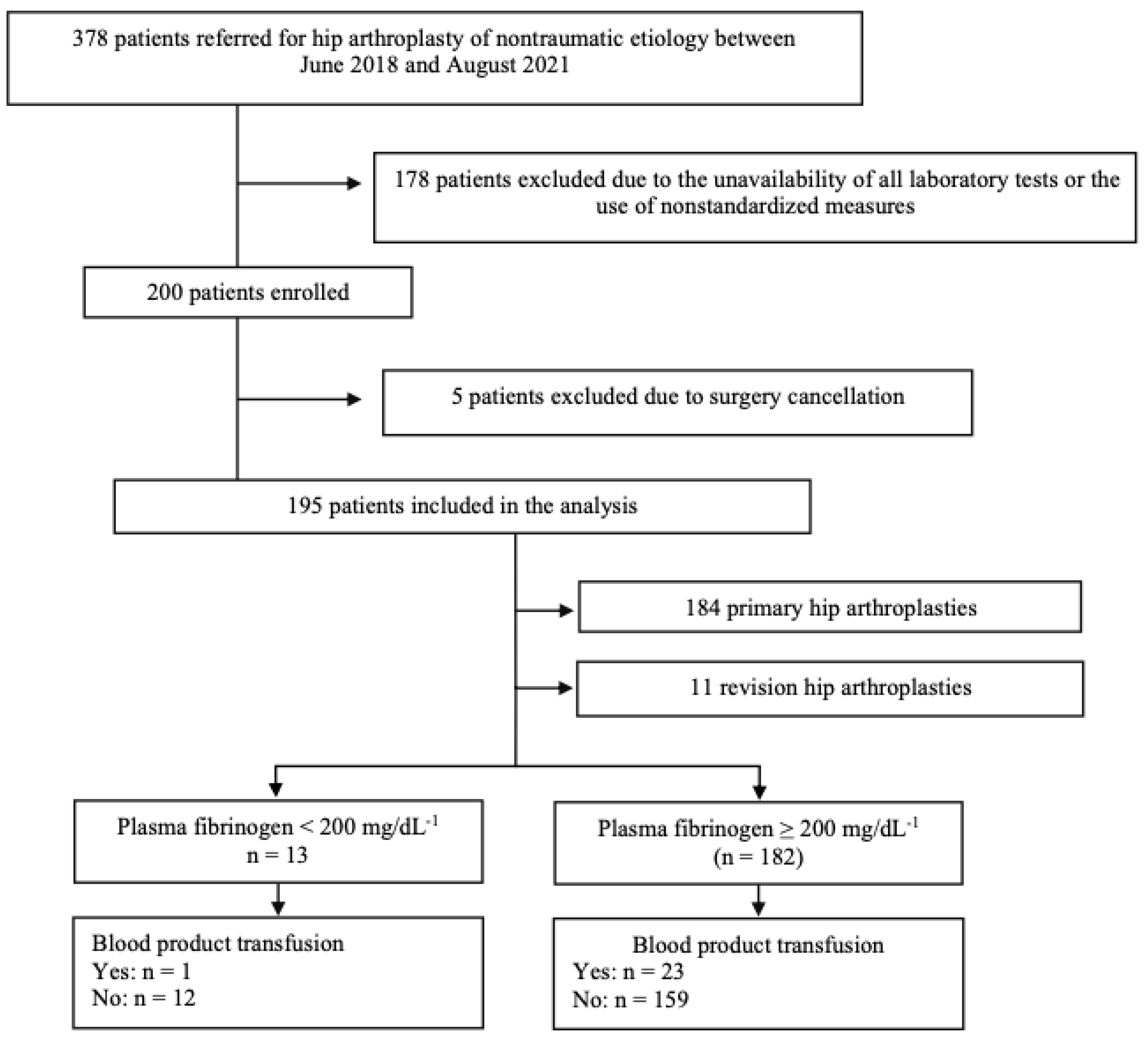
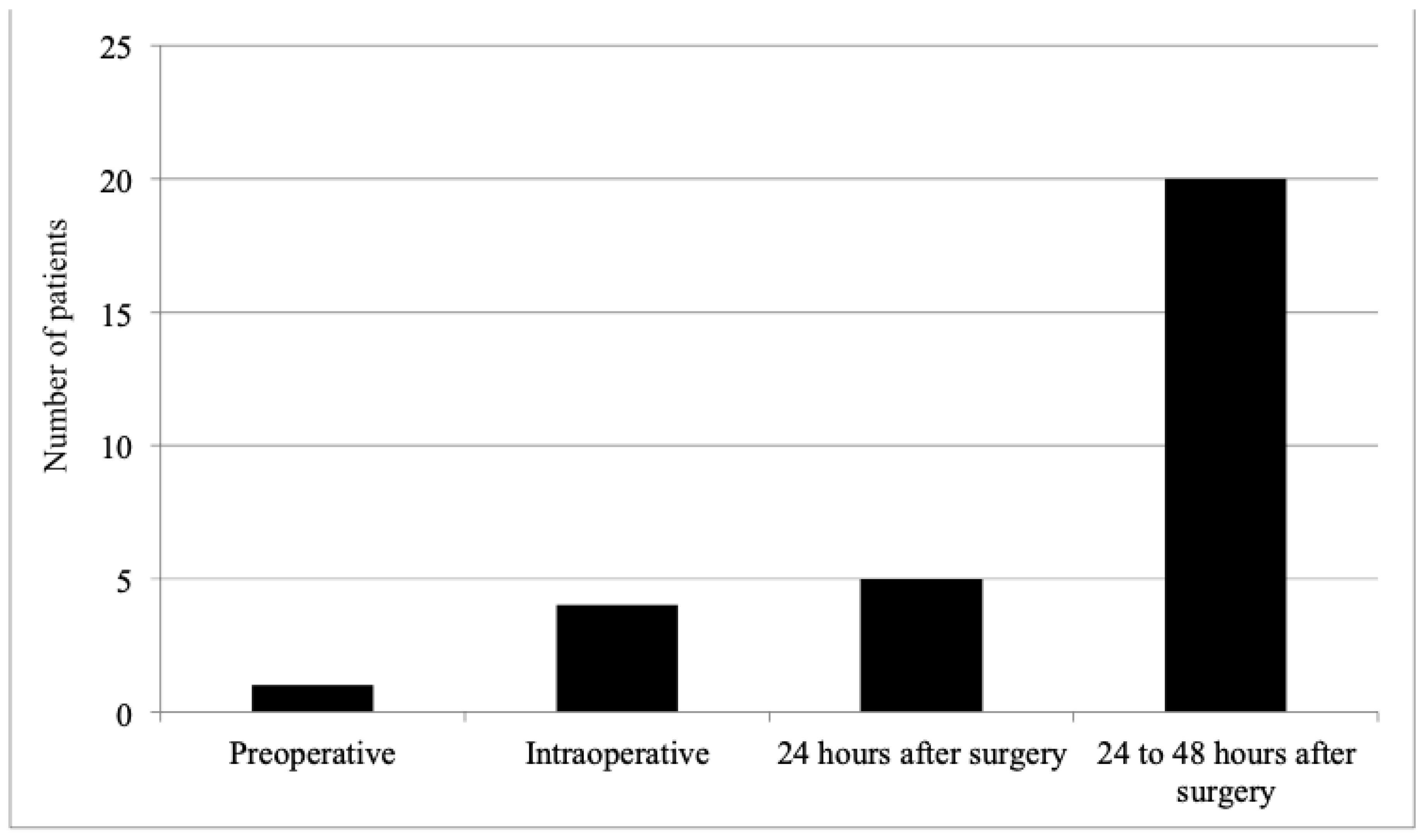
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wei, N.; Jia, Y.; Wang, X.; Zhang, Y.; Yuan, G.; Zhao, B.; Wang, Y.; Zhang, K.; Zhang, X.; Pan, Y.; et al. Risk Factors for Postoperative Fibrinogen Deficiency after Surgical Removal of Intracranial Tumors. PLoS ONE 2015, 10, e0144551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simurda, T.; Snahnicanova, Z.; Loderer, D.; Sokol, J.; Stasko, J.; Lasabova, Z.; Kubisz, P. Fibrinogen Martin: A Novel Mutation in FGB (Gln180Stop) Causing Congenital Afibrinogenemia. Semin. Thromb. Hemost. 2016, 42, 455–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simurda, T.; Stanciakova, L.; Stasko, J.; Dobrotova, M.; Kubisz, P. Yes or no for secondary prophylaxis in afibrinogenemia? Blood Coagul. Fibrinolysis 2015, 26, 978–980. [Google Scholar] [CrossRef] [PubMed]
- Charbit, B.; Mandelbrot, L.; Samain, E.; Baron, G.; Haddaoui, B.; Keita, H.; Sibony, O.; Mahieu-Caputo, D.; Hurtaud-Roux, M.F.; Huisse, M.G.; et al. The decrease of fibrinogen is an early predictor of the severity of postpartum hemorrhage. J. Thromb. Haemost. 2007, 5, 266–273. [Google Scholar] [CrossRef]
- Hagemo, J.S.; Stanworth, S.; Juffermans, N.P.; Brohi, K.; Cohen, M.; Johansson, P.I.; Roislien, J.; Eken, T.; Naess, P.A.; Gaarder, C. Prevalence, predictors and outcome of hypofibrinogenaemia in trauma: A multicentre observational study. Crit Care 2014, 18, R52. [Google Scholar] [CrossRef] [Green Version]
- Yang, L.; Vuylsteke, A.; Gerrard, C.; Besser, M.; Baglin, T. Postoperative fibrinogen level is associated with postoperative bleeding following cardiothoracic surgery and the effect of fibrinogen replacement therapy remains uncertain. J. Thromb. Haemost. 2013, 11, 1519–1526. [Google Scholar] [CrossRef]
- Oberweis, B.S.; Cuff, G.; Rosenberg, A.; Pardo, L.; Nardi, M.A.; Guo, Y.; Dweck, E.; Marshall, M.; Steiger, D.; Stuchin, S.; et al. Platelet aggregation and coagulation factors in orthopedic surgery. J. Thromb. Thrombolysis 2014, 38, 430–438. [Google Scholar] [CrossRef]
- Lee, J.H.; Han, S.B. Patient Blood Management in Hip Replacement Arthroplasty. Hip Pelvis 2015, 27, 201–208. [Google Scholar] [CrossRef] [Green Version]
- Bouzat, P.; Ageron, F.X.; Charbit, J.; Bobbia, X.; Deras, P.; Nugues, J.B.D.; Escudier, E.; Marcotte, G.; Leone, M.; David, J.S. Modelling the association between fibrinogen concentration on admission and mortality in patients with massive transfusion after severe trauma: An analysis of a large regional database. Scand. J. Trauma Resusc. Emerg. Med. 2018, 26, 55. [Google Scholar] [CrossRef]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gotzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; Initiative, S. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Int. J. Surg. 2014, 12, 1500–1524. [Google Scholar] [CrossRef] [Green Version]
- Clauss, A. Rapid physiological coagulation method in determination of fibrinogen. Acta Haematol. 1957, 17, 237–246. [Google Scholar] [CrossRef] [PubMed]
- Rourke, C.; Curry, N.; Khan, S.; Taylor, R.; Raza, I.; Davenport, R.; Stanworth, S.; Brohi, K. Fibrinogen levels during trauma hemorrhage, response to replacement therapy, and association with patient outcomes. J. Thromb. Haemost. 2012, 10, 1342–1351. [Google Scholar] [CrossRef] [PubMed]
- Costa, M.; Dalmau, A.; Sabate, A.; Koo, M.; Aparicio, I.; Contreras, L. Low plasma fibrinogen levels and blood product transfusion in liver transplantation. Minerva Anestesiol. 2014, 80, 568–573. [Google Scholar] [PubMed]
- Charbonneau, H.; Pasquie, M.; Mayeur, N. Preoperative plasma fibrinogen level and transfusion in cardiac surgery: A biphasic correlation. Interact. Cardiovasc. Thorac. Surg. 2020, 31, 622–625. [Google Scholar] [CrossRef]
- Guan, X.; Gong, M.; Wang, X.; Zhu, J.; Liu, Y.; Sun, L.; Zhang, H. Low preoperative fibrinogen level is risk factor for neurological complications in acute aortic dissection. Medicine 2018, 97, e10830. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.Y.; Shim, J.K.; Song, J.W.; Kim, E.K.; Kwak, Y.L. Impact of preoperative fibrinogen concentration on postoperative outcome in patients who received dual antiplatelet therapy in proximity to off-pump coronary bypass surgery. Circ. J. 2014, 78, 1661–1666. [Google Scholar] [CrossRef] [Green Version]
- Geck, M.J.; Singh, D.; Gunn, H.; Stokes, J.K.; Truumees, E. Is Preoperative Fibrinogen Testing Associated With Total Blood Loss in Adolescent Idiopathic Scoliosis Correction? Spine Deform. 2017, 5, 381–386. [Google Scholar] [CrossRef]
- Verlicchi, F.; Desalvo, F.; Zanotti, G.; Morotti, L.; Tomasini, I. Red cell transfusion in orthopaedic surgery: A benchmark study performed combining data from different data sources. Blood Transfus. 2011, 9, 383–387. [Google Scholar] [CrossRef]
- Carling, M.S.; Jeppsson, A.; Eriksson, B.I.; Brisby, H. Transfusions and blood loss in total hip and knee arthroplasty: A prospective observational study. J. Orthop. Surg. Res. 2015, 10, 48. [Google Scholar] [CrossRef] [Green Version]
- Simurda, T.; Kubisz, P.; Dobrotova, M.; Necas, L.; Stasko, J. Perioperative Coagulation Management in a Patient with Congenital Afibrinogenemia during Revision Total Hip Arthroplasty. Semin. Thromb. Hemost. 2016, 42, 689–692. [Google Scholar] [CrossRef] [Green Version]
- Song, K.; Pan, P.; Yao, Y.; Jiang, T.; Jiang, Q. The incidence and risk factors for allogenic blood transfusion in total knee and hip arthroplasty. J. Orthop. Surg. Res. 2019, 14, 273. [Google Scholar] [CrossRef] [Green Version]
- Carling, M.S.; Zarhoud, J.; Jeppsson, A.; Eriksson, B.I.; Brisby, H. Preoperative plasma fibrinogen concentration, factor XIII activity, perioperative bleeding, and transfusions in elective orthopaedic surgery: A prospective observational study. Thromb. Res. 2016, 139, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Browne, J.A.; Adib, F.; Brown, T.E.; Novicoff, W.M. Transfusion rates are increasing following total hip arthroplasty: Risk factors and outcomes. J. Arthroplast. 2013, 28, 34–37. [Google Scholar] [CrossRef] [PubMed]
- Carling, M.S.; Jeppsson, A.; Wessberg, P.; Henriksson, A.; Baghaei, F.; Brisby, H. Preoperative fibrinogen plasma concentration is associated with perioperative bleeding and transfusion requirements in scoliosis surgery. Spine 2011, 36, 549–555. [Google Scholar] [CrossRef] [PubMed]
- Mion, S.; Duval, B.; Besnard, T.; Darne, B.; Mouton, C.; Jecker, O.; Labrousse, L.; Remy, A.; Zaouter, C.; Ouattara, A. U-shaped relationship between pre-operative plasma fibrinogen levels and severe peri-operative bleeding in cardiac surgery. Eur. J. Anaesthesiol. 2020, 37, 889–897. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, M.; Ternstrom, L.; Hyllner, M.; Baghaei, F.; Nilsson, S.; Jeppsson, A. Plasma fibrinogen level, bleeding, and transfusion after on-pump coronary artery bypass grafting surgery: A prospective observational study. Transfusion 2008, 48, 2152–2158. [Google Scholar] [CrossRef]
- Kindo, M.; Hoang Minh, T.; Gerelli, S.; Perrier, S.; Meyer, N.; Schaeffer, M.; Bentz, J.; Announe, T.; Mommerot, A.; Collange, O.; et al. Plasma fibrinogen level on admission to the intensive care unit is a powerful predictor of postoperative bleeding after cardiac surgery with cardiopulmonary bypass. Thromb. Res. 2014, 134, 360–368. [Google Scholar] [CrossRef]
- Geck, M.J.; Singh, D.; Gunn, H.; Stokes, J.K.; Truumees, E. Relationship Between Preoperative Plasma Fibrinogen Concentration, Perioperative Bleeding, and Transfusions in Elective Adult Spinal Deformity Correction. Spine Deform. 2019, 7, 788–795. [Google Scholar] [CrossRef]
- Alagha, S.; Songur, M.; Avci, T.; Vural, K.; Kaplan, S. Association of preoperative plasma fibrinogen level with postoperative bleeding after on-pump coronary bypass surgery: Does plasma fibrinogen level affect the amount of postoperative bleeding? Interact. Cardiovasc. Thorac Surg. 2018, 27, 671–676. [Google Scholar] [CrossRef]
- Nakamura, Y.; Ishikura, H.; Kushimoto, S.; Kiyomi, F.; Kato, H.; Sasaki, J.; Ogura, H.; Matsuoka, T.; Uejima, T.; Morimura, N.; et al. Fibrinogen level on admission is a predictor for massive transfusion in patients with severe blunt trauma: Analyses of a retrospective multicentre observational study. Injury 2017, 48, 674–679. [Google Scholar] [CrossRef]
- Umemura, T.; Nakamura, Y.; Nishida, T.; Hoshino, K.; Ishikura, H. Fibrinogen and base excess levels as predictive markers of the need for massive blood transfusion after blunt trauma. Surg. Today 2016, 46, 774–779. [Google Scholar] [CrossRef] [PubMed]
- Notani, N.; Miyazaki, M.; Kanezaki, S.; Ishihara, T.; Sakamoto, T.; Abe, T.; Kataoka, M.; Tsumura, H. Fibrinogen level on admission is a predictive marker of the need for massive blood transfusion after pelvic fracture. Am. J. Emerg. Med. 2020, 38, 789–793. [Google Scholar] [CrossRef] [PubMed]
- Vetter, T.R.; Schober, P.; Mascha, E.J. Diagnostic Testing and Decision-Making: Beauty Is Not Just in the Eye of the Beholder. Anesth. Analg. 2018, 127, 1085–1091. [Google Scholar] [CrossRef] [PubMed]
- Ray, P.; Le Manach, Y.; Riou, B.; Houle, T.T. Statistical evaluation of a biomarker. Anesthesiology 2010, 112, 1023–1040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eusebi, P. Diagnostic accuracy measures. Cerebrovasc. Dis. 2013, 36, 267–272. [Google Scholar] [CrossRef]
- Alzahrani, A.; Othman, N.; Bin-Ali, T.; Elfaraidi, H.; Al Mussaed, E.; Alabbas, F.; Sedick, Q.; Albatniji, F.; Alshahrani, Z.; Asiri, M.; et al. Routine Preoperative Coagulation Tests in Children Undergoing Elective Surgery or Invasive Procedures: Are They Still Necessary? Clin. Med. Insights Blood Disord. 2019, 12, 1179545X18821158. [Google Scholar] [CrossRef]
- Fowler, A.; Perry, D.J. Laboratory monitoring of haemostasis. Anaesthesia 2015, 70 (Suppl. S1), 68-e24. [Google Scholar] [CrossRef] [PubMed]
- Thiruvenkatarajan, V.; Pruett, A.; Adhikary, S.D. Coagulation testing in the perioperative period. Indian J. Anaesth. 2014, 58, 565–572. [Google Scholar] [CrossRef]
- Jagow, D.M.; Yacoubian, S.V.; Yacoubian, S.V. Complete blood count before and after total hip or knee arthroplasty. J. Orthop. Surg. 2015, 23, 209–212. [Google Scholar] [CrossRef]
- Spahn, D.R.; Muñoz, M.; Klein, A.A.; Levy, J.H.; Zacharowski, K. Patient Blood Management: Effectiveness and Future Potential. Anesthesiology 2020, 133, 212–222. [Google Scholar] [CrossRef]
- Hulley, S.B. Designing Clinical Research, 4th ed.; Wolters Kluwer/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013. [Google Scholar]
- Pagana, K.; Pagana, T.; Pagana, T. Mosby’s Diagnostic and Laboratory Test Reference, 15th ed.; Elsevier, Inc: Philadelphia, PA, USA, 2020. [Google Scholar]



{kind=link}
{kind=link}
| Blood-Product Transfusion | |||||
|---|---|---|---|---|---|
| Clinical-Epidemiological Characteristics | Total (n = 195) | No (n = 171) | Yes (n = 24) | p-Value | |
| Age (years) | 62.2 (11.2) | 61.7 (11.3) | 65.6 (10.3) | 0.119 ‡ | |
| Sex | Female | 91 (46.7%) | 76 (83.5%) | 15 (16.5%) | |
| Male | 104 (53.3%) | 95 (91.3%) | 9 (8.7%) | 0.126 § | |
| Race | White | 194 (99.5%) | 170 (87.6%) | 24 (12.4%) | |
| Mixed | 1 (0.5%) | 1 (100.0%) | 0 (0.0%) | 1.000 § | |
| BMI * | 27.7 (4.4) | 27.9 (4.5) | 26.8 (4.2) | 0.259 ¶ | |
| ASA-PS † | 1 | 35 (17.9%) | 31 (88.6%) | 4 (11.4%) | |
| 2 | 148 (75.9%) | 132 (89.2%) | 16 (10.8%) | ||
| 3 | 12 (6.2%) | 8 (66.7%) | 4 (33.3%) | 0.073 ** | |
| Blood-Product Transfusion | |||||
|---|---|---|---|---|---|
| Preoperative Laboratory Tests | Total (n = 195) | No. (n = 171) | Yes (n = 24) | p-Value | |
| Fibrinogen (mg/dL−1) | 315 (83) | 316 (83) | 310 (79) | 0.745 § | |
| Hemoglobin (g/dL−1) | 13.9 (1.3) | 14.0 (1.2) | 13.1 (1.8) | 0.028 § | |
| Hematocrit (%) | 41.6 (4.1) | 42.1 (3.9) | 39.1 (5.1) | 0.006 ¶ | |
| Platelets (count) | 230,756 (61,063) | 229,371 (61,298) | 240,625 (59,689) | 0.327 ¶ | |
| Coagulation | PT * (seconds) | 12.2 (1.5) | 12.1 (1.5) | 12.7 (1.5) | 0.093 ¶ |
| APTT † (seconds) | 28.7 (6.5) | 28.8 (6.7) | 27.4 (4.8) | 0.291 ¶ | |
| INR ‡ | 1.0 (0.1) | 1.0 (0.1) | 1.1 (0.1) | 0.449 ¶ | |
| Test Feature | Results * |
|---|---|
| Sensitivity | 4.17% (95%CI: 0.11–21.12%) |
| Specificity | 92.98% (95%CI: 88.06–96.32%) |
| Positive predictive value | 7.69% (95%CI: 1.12–37.99%) |
| Negative predictive value | 87.36% (95%CI: 86.30–88.35%) |
| Accuracy | 82.05% (95%CI: 75.93–87.17%) |
| Positive likelihood ratio | 0.59 (95%CI: 0.08–4.36) |
| Negative likelihood ratio | 1.03 (95%CI: 0.94–1.13) |
| Absolute risk (fibrinogen < 200 mg/dL−1) (A) | 7.69% (95%CI: 1.37–33.31%) |
| Absolute risk (fibrinogen ≥ 200 mg/dL−1) (B) | 12.64% (95%CI: 8.57–18.25%) |
| Relative risk (A/B) | 0.608 (95%CI: 0.089–4.158) |
| Blood-Product Transfusion | |||||
|---|---|---|---|---|---|
| Variable | Total (n = 195) | No. (n = 171) | Yes (n = 24) | p-Value | |
| Surgical technique (n) | THA * | 184 (94.4%) | 165 (89.7%) | 19 (10.3%) | |
| Revision THA | 11 (5.6%) | 6 (54.5%) | 5 (45.5%) | 0.005 § | |
| Operative time (minutes) | 120.2 (30.3) | 117.0 (26.7) | 143.1 (42.8) | 0.001 ¶ | |
| Anesthetic technique (n) | Neuraxial | 188 (96.4%) | 165 (87.8%) | 23 (12.2%) | |
| General | 5 (2.6%) | 4 (80.0%) | 1 (20.0%) | ||
| Other | 2 (1.0%) | 2 (100.0%) | 0 (0.0%) | 0.757 ** | |
| Antifibrinolytic therapy (n) | Yes, intravenous | 188 (96.4%) | 165 (87.8%) | 23 (12.2%) | |
| Yes, intra-articular | 4 (2.1%) | 3 (75.0%) | 1 (25.0%) | ||
| No | 3 (1.5%) | 3 (100.0%) | 0 (0.0%) | 0.601 ** | |
| Hospitalization (n) | ICU † | 4 (2.1%) | 1 (25.0%) | 3 (75.0%) | |
| PACU ‡ | 191 (97.9%) | 170 (89.0%) | 21 (11.0%) | 0.006 § | |
| Postoperative hemoglobin (g/dL−1) | 10.5 (1.5) | 10.8 (1.3) | 8.61 (1.6) | <0.001 ¶ | |
| Postoperative hematocrit (%) | 31.5 (4.3) | 32.2 (3.9) | 26.3 (3.7) | <0.001 †† | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pagnussatt Neto, E.; Lopes da Costa, P.D.; Gurgel, S.J.T.; Schmidt Azevedo, P.; Modolo, N.S.P.; do Nascimento Junior, P. Plasma Fibrinogen as a Predictor of Perioperative-Blood-Component Transfusion in Major-Nontraumatic-Orthopedic-Surgery Patients: A Cohort Study. Diagnostics 2023, 13, 976. https://doi.org/10.3390/diagnostics13050976
Pagnussatt Neto E, Lopes da Costa PD, Gurgel SJT, Schmidt Azevedo P, Modolo NSP, do Nascimento Junior P. Plasma Fibrinogen as a Predictor of Perioperative-Blood-Component Transfusion in Major-Nontraumatic-Orthopedic-Surgery Patients: A Cohort Study. Diagnostics. 2023; 13(5):976. https://doi.org/10.3390/diagnostics13050976
Chicago/Turabian StylePagnussatt Neto, Eugenio, Paula Daniele Lopes da Costa, Sanderland J. Tavares Gurgel, Paula Schmidt Azevedo, Norma S. Pinheiro Modolo, and Paulo do Nascimento Junior. 2023. "Plasma Fibrinogen as a Predictor of Perioperative-Blood-Component Transfusion in Major-Nontraumatic-Orthopedic-Surgery Patients: A Cohort Study" Diagnostics 13, no. 5: 976. https://doi.org/10.3390/diagnostics13050976