
Models and Algorithms for the Refinement of Therapeutic Approaches for Retinal Diseases

Abstract
:1. Introduction
2. Materials and Methods
2.1. Mathematical Models
2.2. Numerical Methods
2.3. Mathematical Functionals for Drug Comparison
3. Results
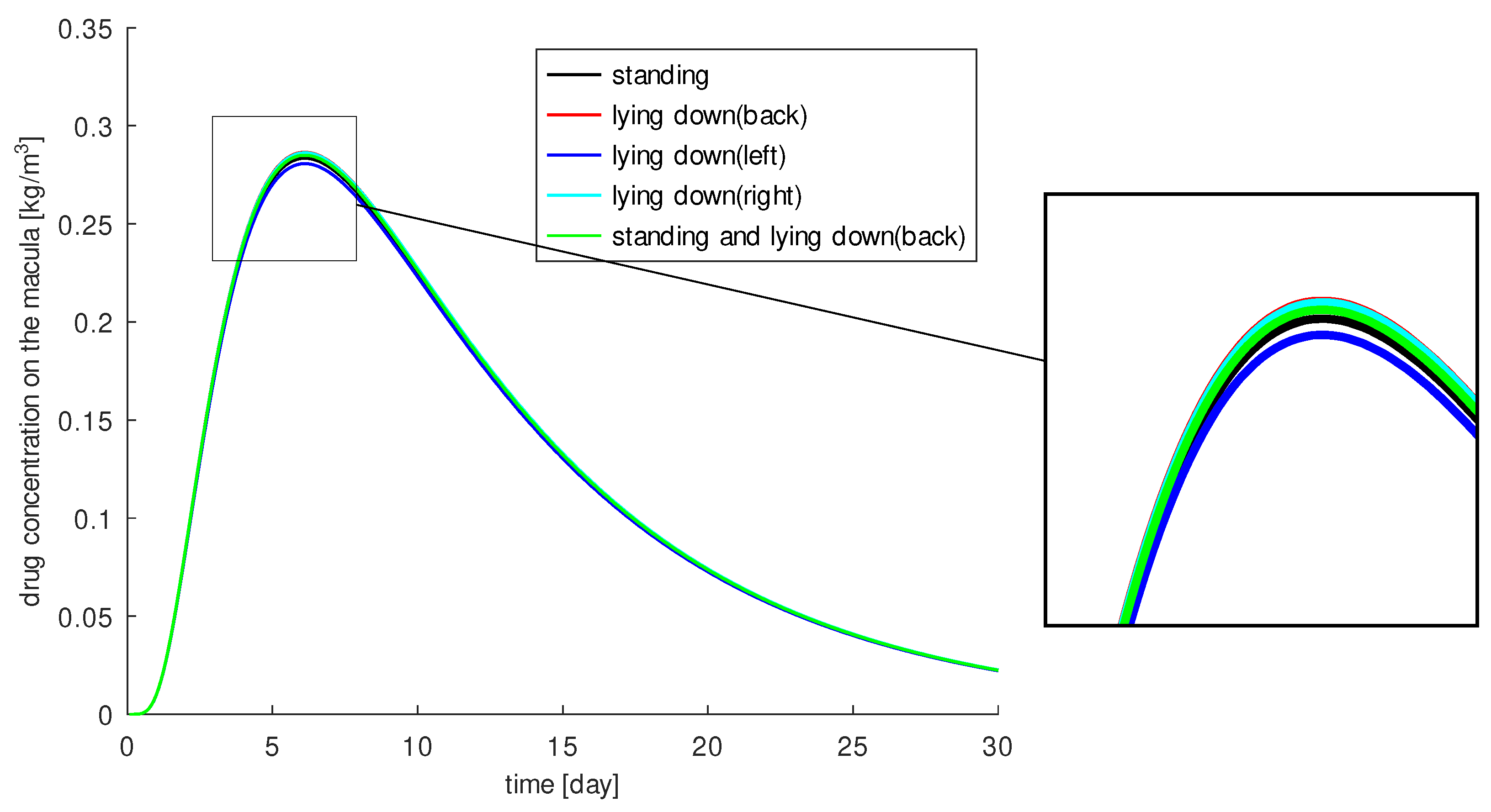
3.1. The Influence of Gravity on Drug Distribution
- The patient stands (over the total time).
- The patient lies on the back.
- The patient lies sideways on the left side.
- The patient lies sideways on the right side.
- The patient stands half the day and lies on the back for the rest of the day.
3.2. Optimal Injection Position
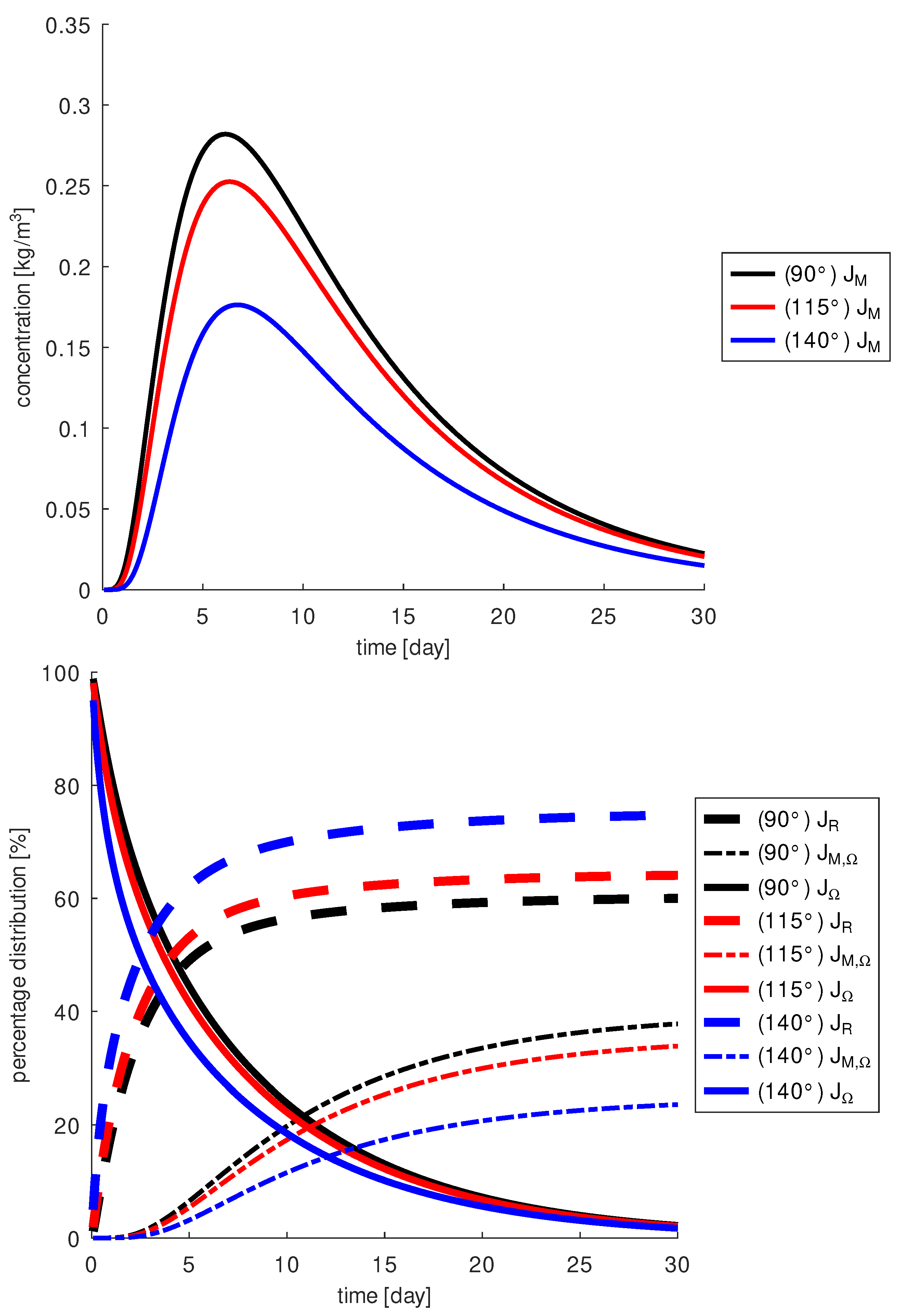
3.3. Optimal Injection Angle
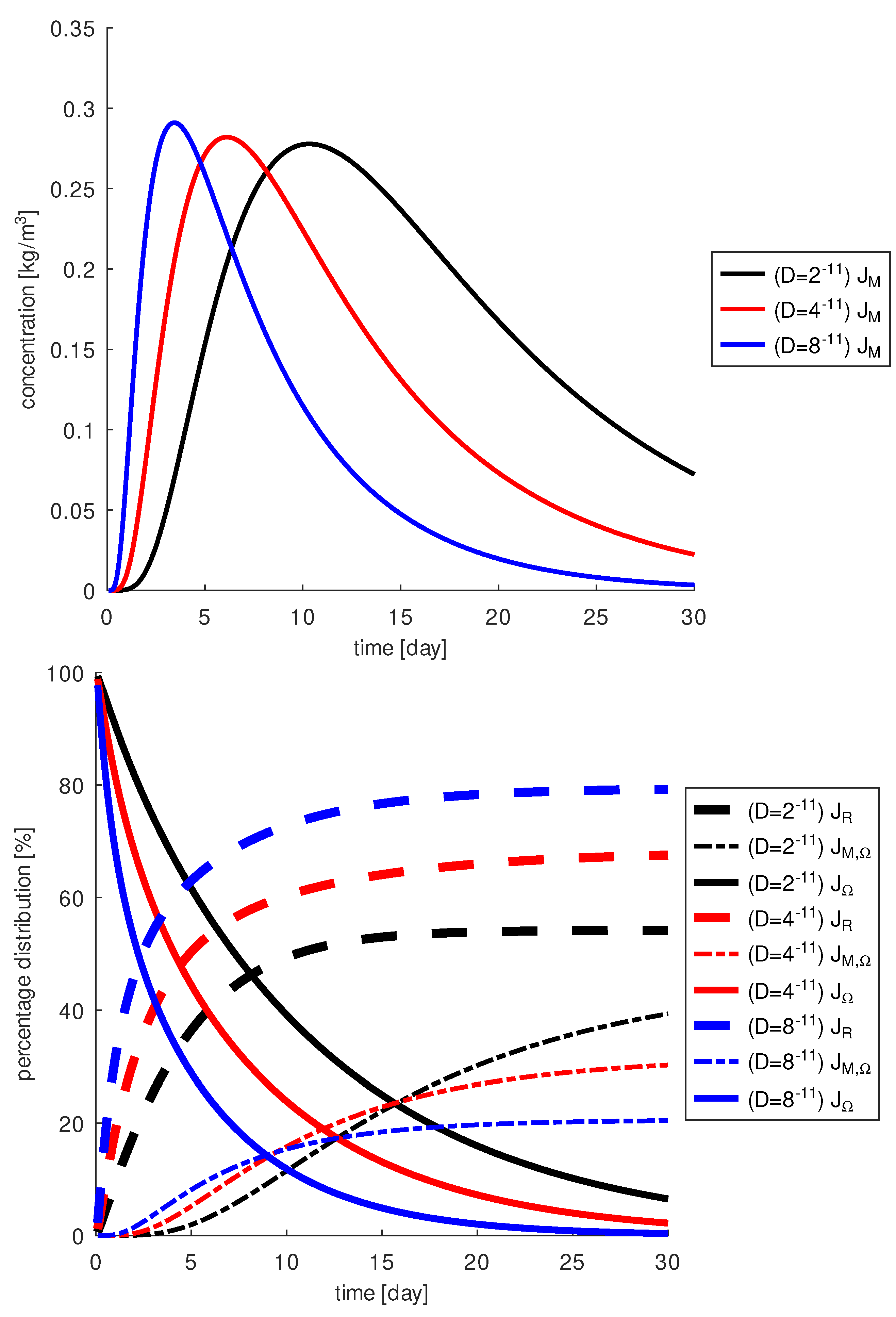
3.4. The Influence of the Diffusion Coefficient on Drug Distribution
4. Discussion
5. Conclusions
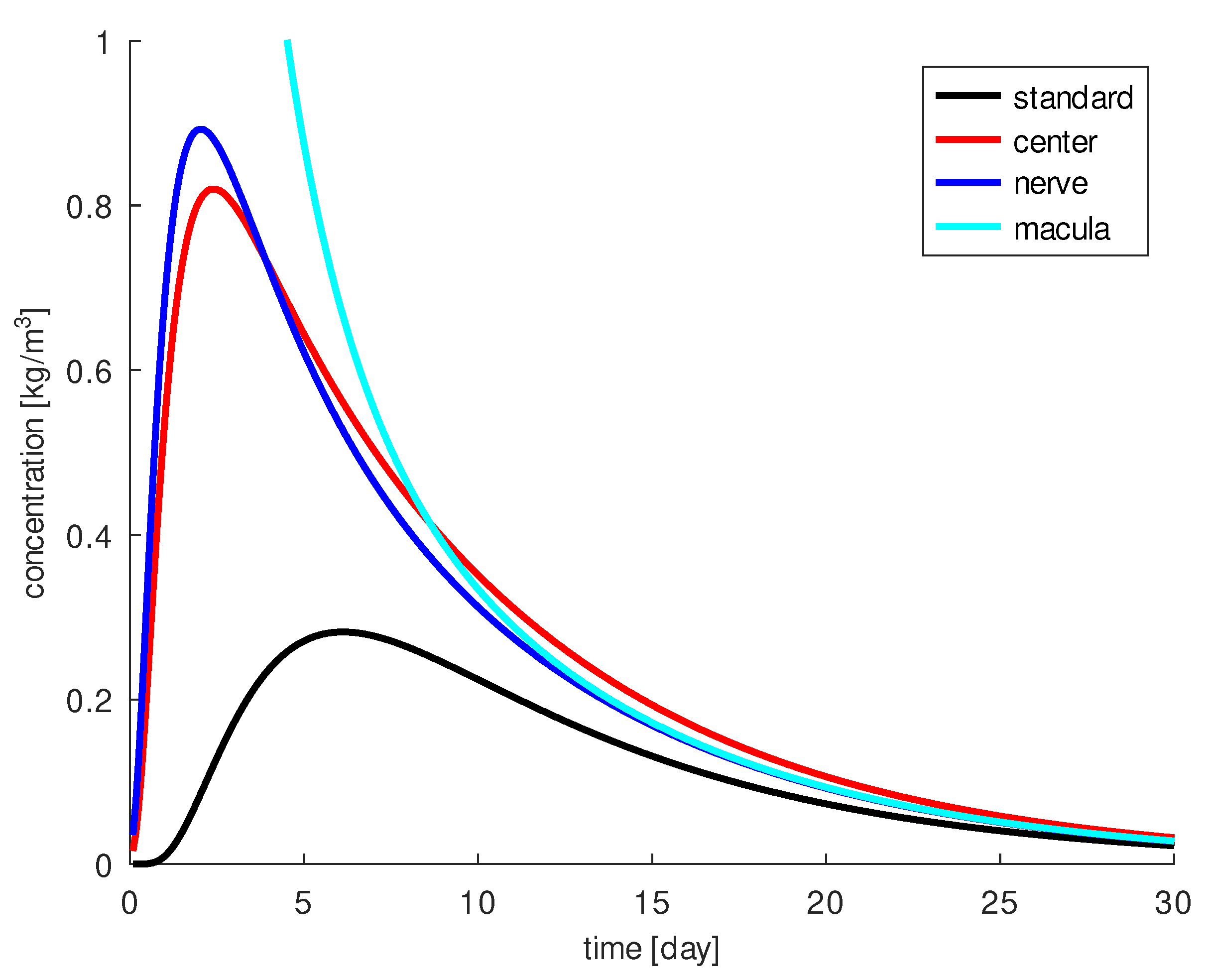
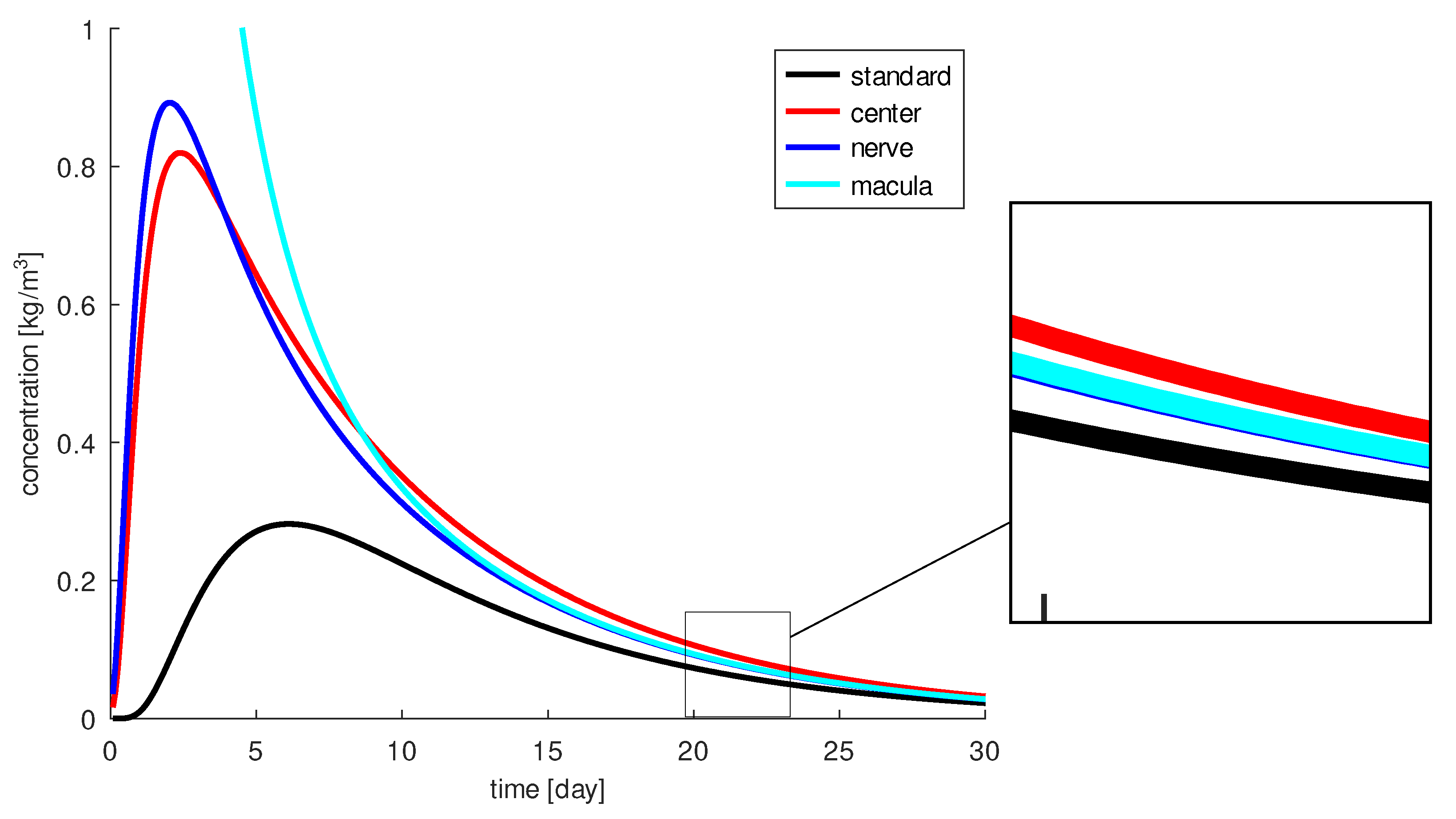
- When the drug is injected centrally into the vitreous, a certain amount of the drug reaches the macula the longest. This can be interesting for longer acting drugs, e.g., aflibercept. Otherwise, a large portion of the drug escapes through the retina.
- If the drug is injected closer to the macula, a higher concentration arrives there, but for a shorter period of time. This can be interesting for an intensified initial treatment, e.g., for the treatment of a thick edema.
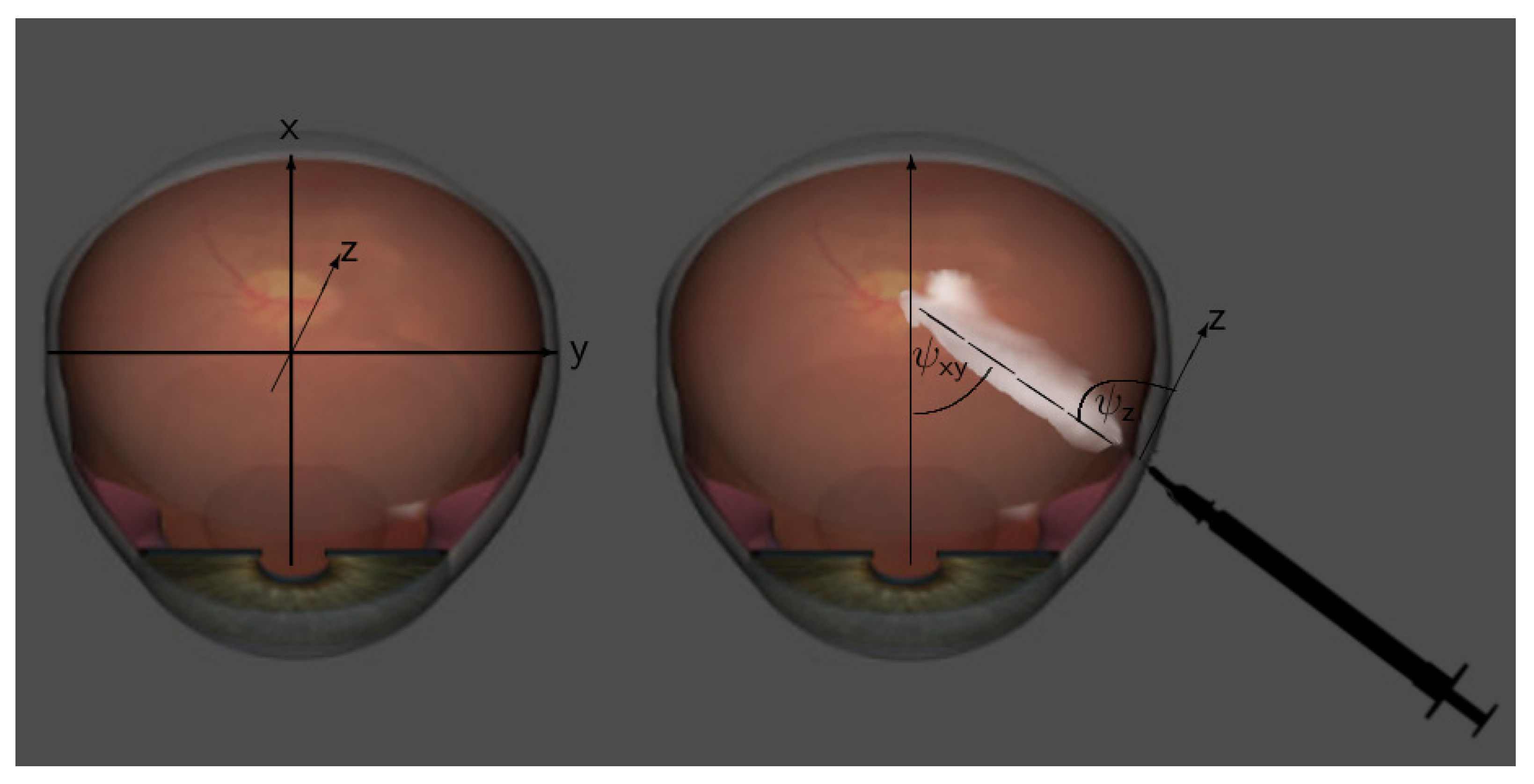
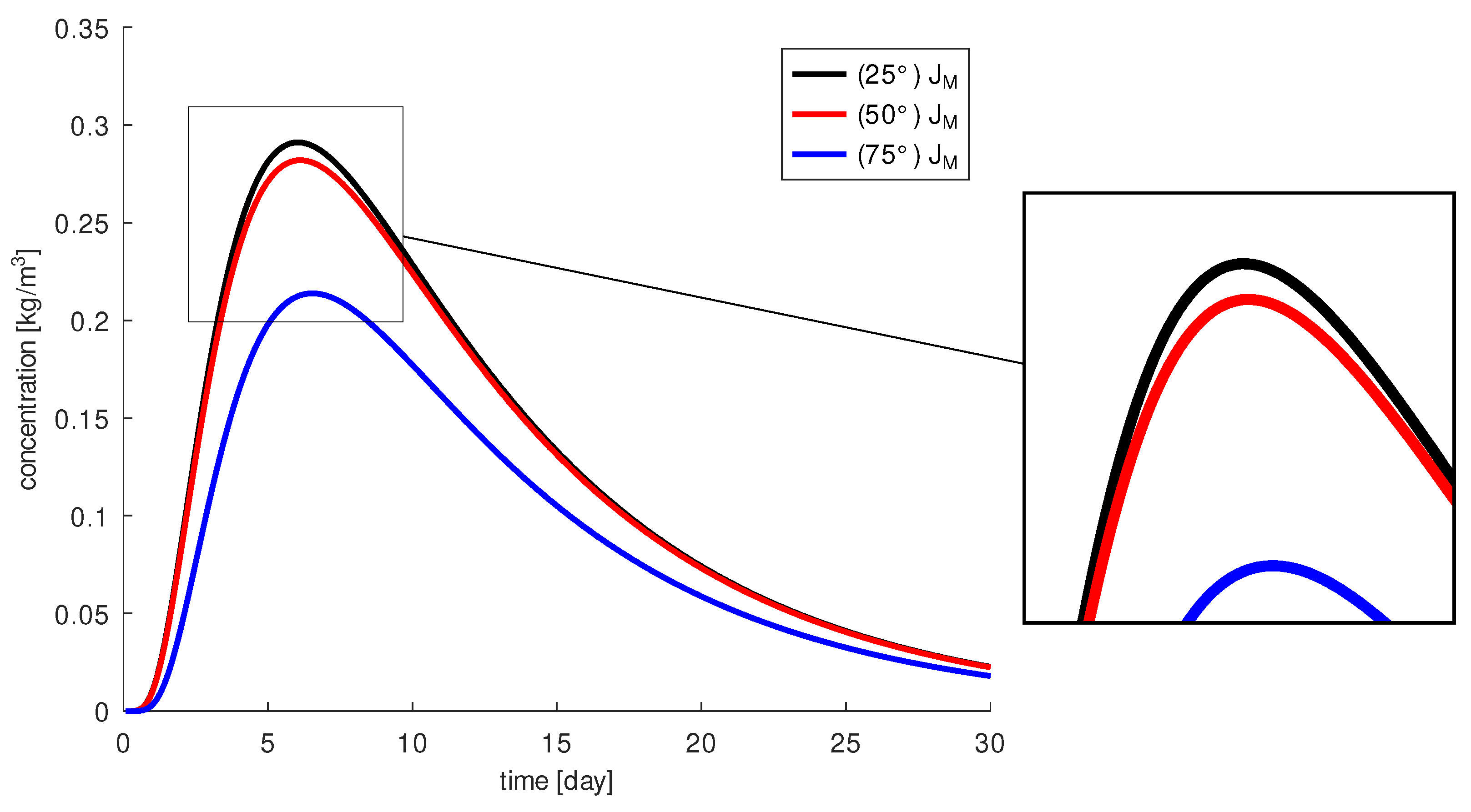
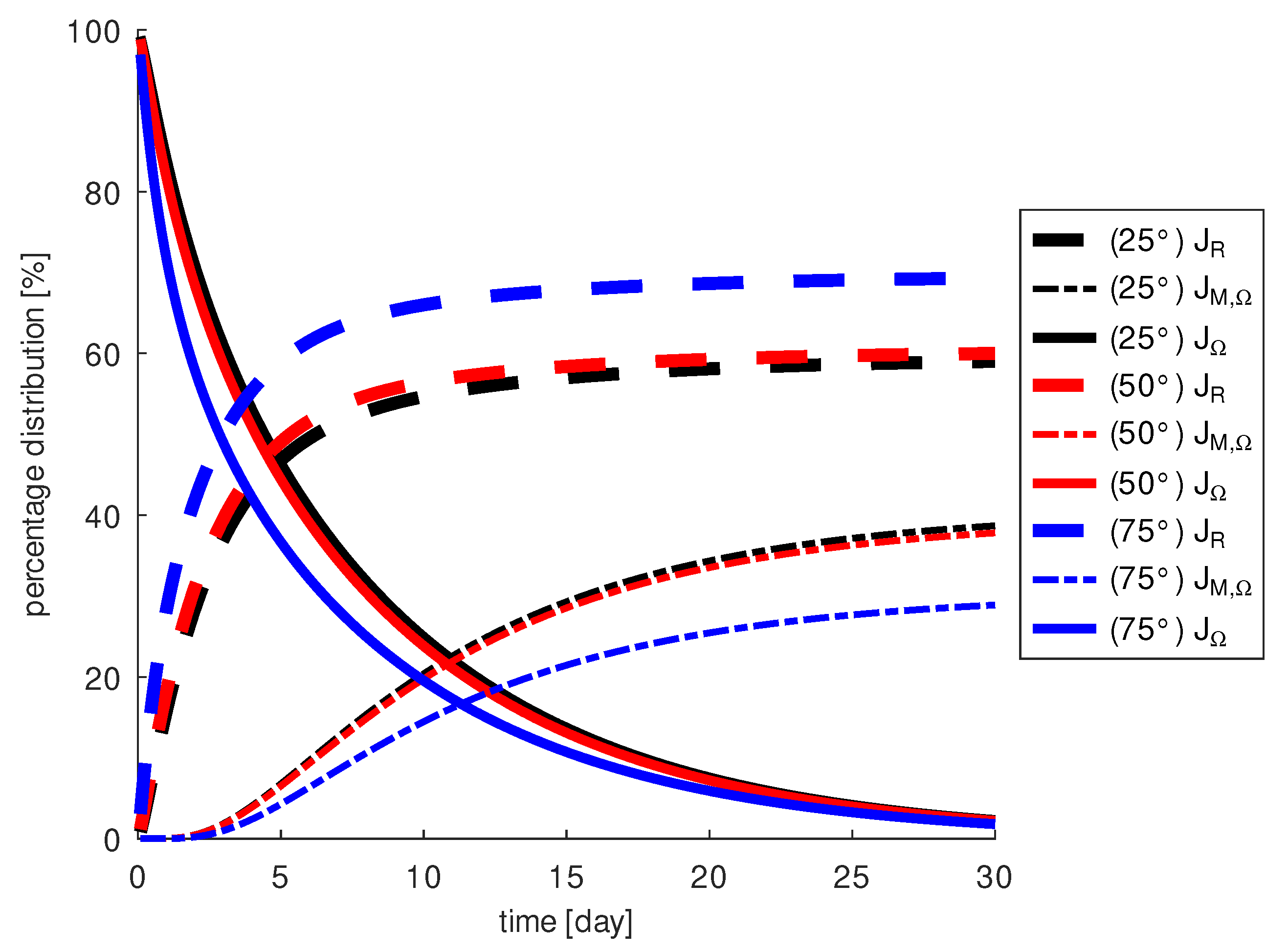
- The needle should be oriented in the direction of the macula. An unfavorable insertion angle can lead to a loss of up to 38% of the drug at the macula.
- A larger diffusion coefficient for the drug, a lighter molecule, results in a higher drug concentration at the macula, but on average over 30 days, it results in a lower drug concentration at the macula because more drug also escapes through the retina more quickly.
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 3D | three dimensions |
| AMD | Age-related macular degeneration |
| CG | Conjugated gradient |
| deal.ii | Differential equations analysis library |
| FEM | Finite element method |
| GMRES | Generalized minimal residual method |
| ILU | Incomplete lower-upper |
| OCT | Optical coherence tomography |
| RPE | Retinal pigment epithelium |
| US | Ultrasound |
| VEGF | Vascular endothelial growth factor |
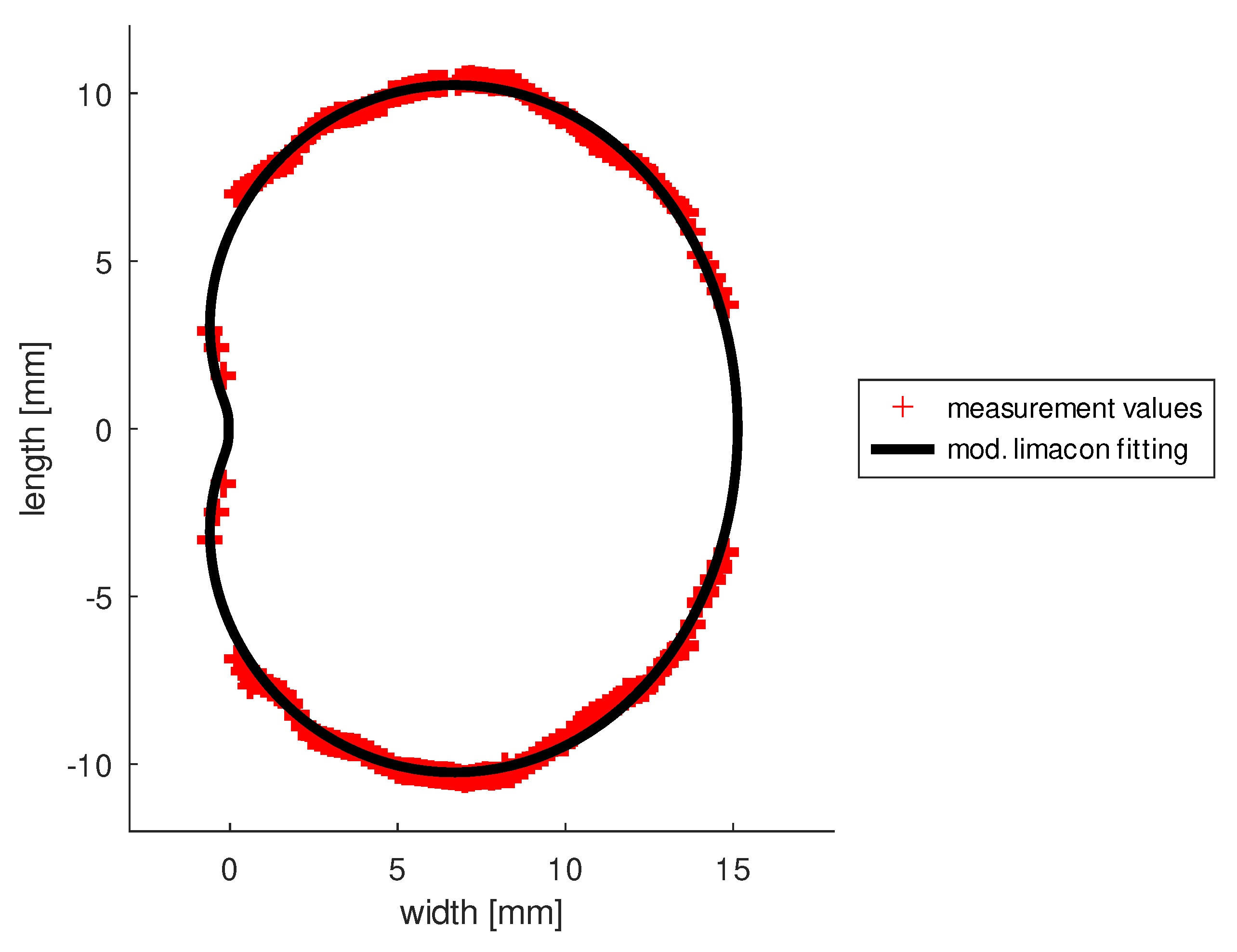
Appendix A. Ultrasound Data

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| x | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| −0.2 | 1.7 | 1.67 | 1.74 | 1.58 | 1.67 | 1.65 | 1.56 | 1.73 | 1.55 | 1.63 | 1.59 | 1.59 |
| −0.4 | 2.5 | 2.2 | 2.5 | 2.5 | 2.47 | 2.59 | 2.49 | 2.46 | 2.45 | 2.5 | 2.43 | 2.58 |
| −0.6 | 3.0 | 3.15 | 3.21 | 3.3 | 3.4 | 3.5 | 3.15 | 3.37 | 3.65 | 3.21 | 3.3 | 3.2 |
| −0.8 | 4.6 | 4.68 | 4.64 | 4.97 | 4.95 | 5.3 | 4.99 | 4.98 | 4.89 | 5.2 | 4.97 | 4.89 |
| −1 | 5.0 | 5.1 | 4.87 | 5.02 | 5.12 | 5.4 | 5.01 | 5.15 | 4.9 | 5.5 | 5 | 4.9 |
| −1.2 | 5.1 | 5.21 | 4.9 | 5.3 | 5.33 | 5.48 | 5.15 | 5.2 | 5.08 | 5.51 | 5.2 | 5.2 |
| −1.4 | 5.2 | 5.35 | 5.13 | 5.46 | 5.68 | 5.52 | 5.37 | 5.32 | 5.12 | 5.59 | 5.38 | 5.4 |
| −1.6 | 5.3 | 5.4 | 5.25 | 5.56 | 5.9 | 5.7 | 5.43 | 5.43 | 5.38 | 5.74 | 5.53 | 5.67 |
| −1.8 | 5.5 | 5.62 | 5.49 | 5.68 | 6.08 | 5.84 | 5.61 | 5.59 | 5.48 | 5.89 | 5.6 | 5.7 |
| −1.6 | 6.2 | 6.5 | 5.9 | 6.6 | 6.41 | 6.35 | 6 | 5.98 | 5.9 | 6.55 | 6.02 | 6.3 |
| −1.4 | 6.1 | 6.3 | 6.01 | 6.34 | 6.15 | 6.06 | 5.89 | 5.7 | 5.39 | 6.2 | 5.9 | 6.02 |
| −1.2 | 6.4 | 6.68 | 6.38 | 6.67 | 6.39 | 6.31 | 6.22 | 6.13 | 5.99 | 6.46 | 6.24 | 6.21 |
| −1 | 6.5 | 6.69 | 6.49 | 6.76 | 6.58 | 6.59 | 5.47 | 6.3 | 6.39 | 6.69 | 6.44 | 6.38 |
| −0.8 | 6.5 | 6.7 | 6.52 | 6.8 | 6.61 | 6.6 | 5.82 | 6.42 | 6.44 | 6.71 | 6.49 | 6.43 |
| −0.6 | 6.6 | 6.79 | 6.62 | 6.84 | 6.7 | 6.74 | 6.26 | 6.52 | 6.48 | 6.79 | 6.57 | 6.5 |
| −0.4 | 6.7 | 6.84 | 6.74 | 6.85 | 6.79 | 6.83 | 6.52 | 6.64 | 6.63 | 6.83 | 6.71 | 6.78 |
| −0.2 | 6.8 | 6.92 | 6.89 | 6.97 | 6.89 | 6.88 | 6.73 | 6.87 | 6.79 | 6.89 | 6.84 | 6.86 |
| 0.2 | 7.0 | 7.12 | 7.08 | 7.22 | 7.09 | 7.12 | 7.11 | 7.14 | 7.03 | 7.12 | 7.13 | 7.13 |
| 0.4 | 7.1 | 7.15 | 7.22 | 7.34 | 7.23 | 7.24 | 7.21 | 7.26 | 7.17 | 7.3 | 7.24 | 7.22 |
| 0.6 | 7.2 | 7.23 | 7.31 | 7.49 | 7.35 | 7.39 | 7.32 | 7.47 | 7.26 | 7.41 | 7.42 | 7.34 |
| 0.8 | 7.3 | 7.37 | 7.44 | 7.53 | 7.48 | 7.49 | 7.51 | 7.54 | 7.39 | 7.53 | 7.53 | 7.48 |
| 1 | 7.4 | 7.49 | 7.58 | 7.61 | 7.59 | 7.56 | 7.62 | 7.64 | 7.58 | 7.67 | 7.66 | 7.57 |
| 1.2 | 7.5 | 7.6 | 7.63 | 7.72 | 7.7 | 7.63 | 7.71 | 7.81 | 7.82 | 7.76 | 7.8 | 7.79 |
| 1.4 | 7.7 | 7.78 | 7.74 | 7.83 | 7.89 | 7.74 | 7.86 | 7.94 | 7.92 | 7.88 | 7.89 | 7.85 |
| 1.6 | 7.7 | 7.82 | 7.85 | 7.9 | 7.93 | 7.8 | 7.92 | 7.98 | 7.99 | 7.94 | 7.96 | 7.96 |
| 1.8 | 8.0 | 8.05 | 8.09 | 8.18 | 8.23 | 8.12 | 8.34 | 8.28 | 8.26 | 8.19 | 8.22 | 8.3 |
| 2 | 8.3 | 8.42 | 8.44 | 8.51 | 8.57 | 8.59 | 8.64 | 8.62 | 8.5 | 8.49 | 8.58 | 8.6 |
| 2.2 | 8.7 | 8.78 | 8.83 | 8.88 | 8.89 | 8.92 | 8.94 | 8.91 | 8.86 | 8.84 | 8.95 | 8.98 |
| 2.4 | 8.9 | 8.89 | 9.12 | 9.19 | 9.2 | 9.16 | 9.08 | 9.08 | 9.18 | 9.18 | 9.2 | 9.21 |
| 2.6 | 9.1 | 9.16 | 9.21 | 9.27 | 9.26 | 9.22 | 9.19 | 9.2 | 9.24 | 9.23 | 9.27 | 9.26 |
| 2.8 | 9.2 | 9.24 | 9.32 | 9.33 | 9.28 | 9.29 | 9.26 | 9.25 | 9.26 | 9.29 | 9.34 | 9.31 |
| 3 | 9.2 | 9.31 | 9.39 | 9.37 | 9.35 | 9.32 | 9.36 | 9.3 | 9.32 | 9.34 | 9.39 | 9.38 |
| 3.2 | 9.3 | 9.37 | 9.42 | 9.4 | 9.41 | 9.38 | 9.43 | 9.37 | 9.39 | 9.38 | 9.42 | 9.41 |
| 3.4 | 9.3 | 9.42 | 9.46 | 9.47 | 9.46 | 9.42 | 9.48 | 9.43 | 9.45 | 9.44 | 9.48 | 9.48 |
| 3.6 | 9.4 | 9.46 | 9.5 | 9.51 | 9.49 | 9.46 | 9.52 | 9.47 | 9.5 | 9.49 | 9.52 | 9.5 |
| 3.8 | 9.4 | 9.5 | 9.52 | 9.54 | 9.53 | 9.49 | 9.53 | 9.5 | 9.53 | 9.52 | 9.52 | 9.51 |
| 4 | 9.5 | 9.62 | 9.62 | 9.63 | 9.62 | 9.59 | 9.63 | 9.59 | 9.63 | 9.63 | 9.63 | 9.61 |
| 4.2 | 9.6 | 9.7 | 9.72 | 9.74 | 9.72 | 9.72 | 9.74 | 9.71 | 9.74 | 9.77 | 9.76 | 9.74 |
| 4.4 | 9.7 | 9.82 | 9.84 | 9.85 | 9.84 | 9.85 | 9.86 | 9.82 | 9.86 | 9.88 | 9.84 | 9.84 |
| 4.6 | 9.8 | 9.94 | 9.95 | 9.96 | 9.94 | 9.96 | 9.98 | 9.94 | 9.97 | 9.99 | 9.95 | 9.93 |
| 4.8 | 9.9 | 10.0 | 10.0 | 10.0 | 10.0 | 10.0 | 10.0 | 10.0 | 10.0 | 10.1 | 10.0 | 10.0 |
| 5 | 10.1 | 10.1 | 10.1 | 10.1 | 10.1 | 10.2 | 10.2 | 10.2 | 10.1 | 10.1 | 10.2 | 10.1 |
| 5.2 | 10.1 | 10.2 | 10.2 | 10.2 | 10.1 | 10.2 | 10.2 | 10.2 | 10.2 | 10.1 | 10.2 | 10.2 |
| 5.4 | 10.1 | 10.2 | 10.2 | 10.2 | 10.1 | 10.2 | 10.2 | 10.2 | 10.2 | 10.2 | 10.2 | 10.2 |
| 5.6 | 10.2 | 10.2 | 10.2 | 10.2 | 10.2 | 10.2 | 10.2 | 10.2 | 10.2 | 10.2 | 10.2 | 10.2 |
| 5.8 | 10.2 | 10.2 | 10.2 | 10.2 | 10.2 | 10.2 | 10.2 | 10.2 | 10.2 | 10.2 | 10.2 | 10.2 |
| 6 | 10.2 | 10.2 | 10.2 | 10.2 | 10.2 | 10.2 | 10.2 | 10.3 | 10.2 | 10.2 | 10.2 | 10.2 |
| 6.2 | 10.2 | 10.3 | 10.3 | 10.3 | 10.2 | 10.3 | 10.3 | 10.3 | 10.3 | 10.3 | 10.3 | 10.3 |
| 6.4 | 10.3 | 10.3 | 10.3 | 10.3 | 10.3 | 10.3 | 10.3 | 10.3 | 10.3 | 10.3 | 10.3 | 10.3 |
| 6.6 | 10.3 | 10.3 | 10.3 | 10.3 | 10.3 | 10.3 | 10.3 | 10.3 | 10.3 | 10.3 | 10.3 | 10.3 |
| 6.8 | 10.3 | 10.3 | 10.3 | 10.4 | 10.4 | 10.4 | 10.4 | 10.4 | 10.4 | 10.3 | 10.4 | 10.3 |
| 7 | 10.4 | 10.4 | 10.4 | 10.4 | 10.4 | 10.4 | 10.4 | 10.4 | 10.4 | 10.4 | 10.4 | 10.4 |
| x | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 7.2 | 10.4 | 10.4 | 10.4 | 10.4 | 10.4 | 10.4 | 10.4 | 10.4 | 10.4 | 10.4 | 10.4 | 10.4 |
| 7.4 | 10.3 | 10.3 | 10.3 | 10.4 | 10.4 | 10.4 | 10.4 | 10.4 | 10.4 | 10.3 | 10.4 | 10.3 |
| 7.6 | 10.3 | 10.3 | 10.3 | 10.3 | 10.3 | 10.4 | 10.3 | 10.3 | 10.3 | 10.3 | 10.4 | 10.3 |
| 7.8 | 10.3 | 10.3 | 10.3 | 10.3 | 10.3 | 10.3 | 10.3 | 10.3 | 10.3 | 10.3 | 10.3 | 10.3 |
| 8 | 10.3 | 10.33 | 10.32 | 10.34 | 10.33 | 10.36 | 10.35 | 10.34 | 10.33 | 10.31 | 10.35 | 10.33 |
| 8.2 | 10.2 | 10.31 | 10.3 | 10.3 | 10.31 | 10.34 | 10.34 | 10.3 | 10.32 | 10.29 | 10.3 | 10.32 |
| 8.4 | 10.2 | 10.3 | 10.29 | 10.28 | 10.3 | 10.32 | 10.31 | 10.28 | 10.3 | 10.28 | 10.29 | 10.31 |
| 8.6 | 10.1 | 10.18 | 10.17 | 10.16 | 10.21 | 10.22 | 10.2 | 10.16 | 10.17 | 10.15 | 10.16 | 10.16 |
| 8.8 | 10.0 | 10.04 | 10.03 | 10.02 | 10.06 | 10.06 | 10.03 | 10.02 | 10.02 | 10.01 | 10.04 | 10.05 |
| 9 | 9.88 | 9.92 | 9.91 | 9.89 | 9.93 | 9.92 | 9.88 | 9.87 | 9.89 | 9.86 | 9.88 | 9.91 |
| 9.2 | 9.73 | 9.75 | 9.74 | 9.74 | 9.76 | 9.77 | 9.75 | 9.74 | 9.79 | 9.78 | 9.75 | 9.77 |
| 9.4 | 9.58 | 9.62 | 9.65 | 9.63 | 9.64 | 9.65 | 9.65 | 9.64 | 9.65 | 9.63 | 9.62 | 9.63 |
| 9.6 | 9.47 | 9.49 | 9.5 | 9.51 | 9.49 | 9.53 | 9.51 | 9.48 | 9.49 | 9.51 | 9.5 | 9.51 |
| 9.8 | 9.34 | 9.35 | 9.35 | 9.36 | 9.37 | 9.38 | 9.37 | 9.33 | 9.34 | 9.35 | 9.38 | 9.34 |
| 10 | 9.34 | 9.35 | 9.35 | 9.36 | 9.37 | 9.38 | 9.37 | 9.33 | 9.34 | 9.35 | 9.38 | 9.34 |
| 10.2 | 9.12 | 9.14 | 9.15 | 9.16 | 9.14 | 9.18 | 9.13 | 9.12 | 9.14 | 9.13 | 9.16 | 9.15 |
| 10.4 | 8.9 | 8.91 | 8.91 | 8.93 | 8.92 | 8.95 | 8.93 | 8.91 | 8.93 | 8.9 | 8.94 | 8.92 |
| 10.6 | 8.68 | 8.7 | 8.71 | 8.69 | 8.69 | 8.71 | 8.73 | 8.68 | 8.72 | 8.69 | 8.73 | 8.68 |
| 10.8 | 8.52 | 8.53 | 8.53 | 8.55 | 8.57 | 8.58 | 8.6 | 8.57 | 8.54 | 8.52 | 8.57 | 8.55 |
| 11 | 8.44 | 8.48 | 8.46 | 8.47 | 8.5 | 8.49 | 8.51 | 8.46 | 8.47 | 8.47 | 8.49 | 8.5 |
| 11.2 | 8.33 | 8.34 | 8.36 | 8.35 | 8.37 | 8.36 | 8.38 | 8.34 | 8.36 | 8.37 | 8.36 | 8.38 |
| 11.4 | 8.2 | 8.24 | 8.27 | 8.25 | 8.26 | 8.24 | 8.25 | 8.23 | 8.24 | 8.26 | 8.24 | 8.25 |
| 11.6 | 8.08 | 8.1 | 8.14 | 8.13 | 8.15 | 8.11 | 8.14 | 8.1 | 8.12 | 8.1 | 8.12 | 8.13 |
| 11.8 | 7.9 | 7.93 | 8.19 | 8 | 7.93 | 7.98 | 8.1 | 7.99 | 8.01 | 7.95 | 8.02 | 7.96 |
| 12 | 7.82 | 7.85 | 7.89 | 7.92 | 7.87 | 7.88 | 7.86 | 7.87 | 7.95 | 7.86 | 7.9 | 7.89 |
| 12.2 | 7.78 | 7.8 | 7.81 | 7.81 | 7.83 | 7.78 | 7.78 | 7.81 | 7.81 | 7.8 | 7.81 | 7.82 |
| 12.4 | 7.72 | 7.74 | 7.73 | 7.76 | 7.74 | 7.73 | 7.76 | 7.77 | 7.74 | 7.74 | 7.75 | 7.73 |
| 12.6 | 7.48 | 7.47 | 7.5 | 7.51 | 7.48 | 7.46 | 7.52 | 7.51 | 7.53 | 7.5 | 7.49 | 7.48 |
| 12.8 | 7.23 | 7.25 | 7.26 | 7.26 | 7.24 | 7.23 | 7.25 | 7.24 | 7.26 | 7.23 | 7.24 | 7.24 |
| 13 | 6.96 | 6.97 | 6.99 | 6.99 | 6.98 | 6.96 | 6.98 | 6.97 | 6.98 | 6.96 | 6.98 | 6.98 |
| 13.2 | 6.72 | 6.75 | 6.76 | 6.74 | 6.75 | 6.72 | 6.73 | 6.71 | 6.74 | 6.72 | 6.73 | 6.74 |
| 13.4 | 6.49 | 6.52 | 6.54 | 6.5 | 6.55 | 6.51 | 6.53 | 6.52 | 6.56 | 6.51 | 6.54 | 6.53 |
| 13.6 | 6.47 | 6.49 | 6.5 | 6.48 | 6.48 | 6.46 | 6.47 | 6.46 | 6.49 | 6.46 | 6.48 | 6.47 |
| 13.8 | 5.83 | 5.82 | 5.83 | 5.8 | 5.82 | 5.78 | 5.83 | 5.81 | 5.83 | 5.82 | 5.82 | 5.8 |
| 14 | 5.17 | 5.15 | 5.15 | 5.16 | 5.16 | 5.14 | 5.17 | 5.17 | 5.18 | 5.17 | 5.19 | 5.16 |
| 14.2 | 4.88 | 4.87 | 4.9 | 4.89 | 4.91 | 4.87 | 4.9 | 4.92 | 4.9 | 4.88 | 4.91 | 4.9 |
| 14.4 | 4.49 | 4.48 | 4.51 | 4.51 | 4.47 | 4.5 | 4.51 | 4.49 | 4.48 | 4.52 | 4.48 | 4.49 |
| 14.6 | 4.1 | 4 | 4.08 | 4.09 | 4.09 | 4.08 | 4.1 | 4.07 | 4.12 | 4.11 | 4.09 | 4.08 |
| 14.8 | 3.68 | 3.67 | 3.71 | 3.7 | 3.7 | 3.7 | 3.68 | 3.69 | 3.73 | 3.7 | 3.68 | 3.69 |
| 15 | 3.49 | 3.47 | 3.51 | 3.48 | 3.5 | 3.52 | 3.49 | 3.49 | 3.52 | 3.51 | 3.5 | 3.51 |
| 15.2 | 3.29 | 3.3 | 3.34 | 3.39 | 3.39 | 3.32 | 3.34 | 3.61 | 3.34 | 3.26 | 3.22 | 3.38 |
| 15.4 | 2.49 | 2.52 | 2.51 | 2.47 | 2.53 | 2.48 | 2.5 | 2.51 | 2.51 | 2.5 | 2.52 | 2.48 |
| 15.6 | 1.59 | 1.57 | 1.62 | 1.6 | 1.61 | 1.61 | 1.58 | 1.63 | 1.59 | 1.6 | 1.61 | 1.61 |
| 15.8 | 1.09 | 1.11 | 1.12 | 1.08 | 1.13 | 1.11 | 1.12 | 1.09 | 1.08 | 1.12 | 1.13 | 1.07 |
| 16 | 1.03 | 1.05 | 1.04 | 1.06 | 1.04 | 1.07 | 1.06 | 1.06 | 1.05 | 1.04 | 1.05 | 1.06 |
| 16.2 | 0.9 | 0.99 | 1.02 | 1.04 | 1.01 | 1.02 | 1.02 | 1.03 | 0.99 | 1.02 | 1.03 | 1.01 |
| 16.4 | 0.9 | 0.97 | 0.99 | 0.96 | 0.98 | 0.99 | 0.98 | 0.97 | 0.97 | 0.95 | 0.98 | 0.97 |
| 16.6 | 0.89 | 0.88 | 0.88 | 0.85 | 0.87 | 0.86 | 0.9 | 0.89 | 0.87 | 0.88 | 0.87 | 0.89 |
| 16.8 | 0.64 | 0.61 | 0.66 | 0.6 | 0.59 | 0.58 | 0.62 | 0.64 | 0.58 | 0.6 | 0.57 | 0.53 |
| 17.0 | 0.11 | 0.09 | 0.08 | 0.08 | 0.07 | 0.12 | 0.13 | 0.15 | 0.09 | 0.12 | 0.07 | 0.07 |
| 17 | −0.1 | −0.09 | −0.07 | −0.12 | −0.08 | −0.01 | −0.13 | −0.14 | −0.09 | −0.13 | −0.09 | −0.08 |
| 16.8 | −0.6 | −0.61 | −0.6 | −0.58 | −0.59 | −0.58 | −0.6 | −0.62 | −0.59 | −0.59 | −0.6 | −0.51 |
| 16.6 | −0.89 | −0.87 | −0.87 | −0.86 | −0.88 | −0.86 | −0.89 | −0.89 | −0.88 | −0.87 | −0.86 | −0.89 |
| 16.4 | −0.91 | −0.98 | −0.92 | −0.97 | −0.98 | −0.98 | −0.96 | −0.94 | −0.99 | −0.98 | −0.97 | −0.96 |
| 16.2 | −0.9 | −0.97 | −1.03 | −1.04 | −0.99 | −1.04 | −1.02 | −1.03 | −1.01 | −1.01 | −1.03 | −0.99 |
| 16 | −1.02 | −1.06 | −1.03 | −1.06 | −1.02 | −1.05 | −1.07 | −1.07 | −1.04 | −1.05 | −1.04 | −1.06 |
| 15.8 | −1.09 | −1.12 | −1.09 | −1.1 | −1.12 | −1.13 | −1.09 | −1.08 | −1.09 | −1.1 | −1.14 | −1.14 |
| x | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 15.6 | −1.58 | −1.59 | −1.6 | −1.58 | −1.58 | −1.62 | −1.63 | −1.6 | −1.59 | −1.61 | −1.62 | −1.6 |
| 15.4 | −2.51 | −2.48 | −2.5 | −2.52 | −2.49 | −2.49 | −2.5 | −2.51 | −2.5 | −2.49 | −2.52 | −2.5 |
| 15.2 | −3.28 | −3.32 | −3.3 | −3.2 | −3.29 | −3.34 | −3.29 | −3.31 | −3.33 | −3.28 | −3.4 | −3.3 |
| 15 | −3.48 | −3.47 | −3.49 | −3.5 | −3.51 | −3.5 | −3.52 | −3.49 | −3.53 | −3.5 | −3.52 | −3.5 |
| 14.8 | −3.69 | −3.67 | −3.7 | −3.71 | −3.67 | −3.7 | −3.69 | −3.68 | −3.72 | −3.7 | −3.68 | −3.69 |
| 14.6 | −4.2 | −4.1 | −4 | −4.07 | −4.08 | −4.08 | −4.1 | −4.08 | −4.11 | −4.12 | −4.08 | −4.07 |
| 14.4 | −4.47 | −4.48 | −4.45 | −4.5 | −4.51 | −4.49 | −4.51 | −4.48 | −4.52 | −4.51 | −4.49 | −4.5 |
| 14.2 | −4.9 | −4.89 | −4.93 | −4.92 | −4.89 | −4.88 | −4.87 | −4.93 | −4.94 | −4.8 | −4.92 | −4.91 |
| 14 | −5.17 | −5.16 | −5.15 | −5.14 | −5.17 | −5.16 | −5.18 | −5.14 | −5.19 | −5.17 | −5.17 | −5.18 |
| 13.8 | −5.8 | −5.81 | −5.82 | −5.86 | −5.8 | −5.84 | −5.87 | −5.87 | −5.89 | −5.88 | −5.87 | −5.87 |
| 13.6 | −6.48 | −6.47 | −6.48 | −6.49 | −6.5 | −6.48 | −6.48 | −6.47 | −6.49 | −6.5 | −6.51 | −6.48 |
| 13.4 | −6.51 | −6.52 | −6.49 | −6.54 | −6.51 | −6.5 | −6.53 | −6.53 | −6.52 | −6.5 | −6.48 | −6.5 |
| 13.2 | −6.75 | −6.72 | −6.72 | −6.73 | −6.75 | −6.72 | −6.71 | −6.71 | −6.75 | −6.73 | −6.72 | −6.75 |
| 13 | −6.96 | −6.97 | −6.99 | −7 | −6.98 | −6.96 | −6.99 | −6.97 | −6.98 | −7 | −6.98 | −6.98 |
| 12.8 | −7.2 | −7.24 | −7.25 | −7.25 | −7.23 | −7.26 | −7.2 | −7.28 | −7.26 | −7.27 | −7.25 | −7.24 |
| 12.6 | −7.48 | −7.46 | −7.51 | −7.52 | −7.49 | −7.46 | −7.5 | −7.53 | −7.55 | −7.52 | −7.48 | −7.52 |
| 12.4 | −7.73 | −7.72 | −7.73 | −7.72 | −7.72 | −7.74 | −7.78 | −7.71 | −7.74 | −7.75 | −7.74 | −7.73 |
| 12.2 | −7.79 | −7.78 | −7.78 | −7.8 | −7.82 | −7.79 | −7.79 | −7.79 | −7.82 | −7.74 | −7.78 | −7.76 |
| 12 | −7.82 | −7.85 | −7.9 | −7.92 | −7.8 | −7.9 | −7.92 | −7.87 | −7.96 | −7.86 | −7.92 | −7.88 |
| 11.8 | −7.99 | −8.03 | −7.98 | −7.96 | −7.99 | −7.92 | −7.96 | −8.05 | −8.03 | −7.95 | −8.03 | −8.02 |
| 11.6 | −8.06 | −8.04 | −8.16 | −8.12 | −8.13 | −8.11 | −8.16 | −8.14 | −8.12 | −8.1 | −8.12 | −8.14 |
| 11.4 | −8.21 | −8.23 | −8.24 | −8.24 | −8.25 | −8.23 | −8.2 | −8.26 | −8.26 | −8.24 | −8.23 | −8.26 |
| 11.2 | −8.31 | −8.32 | −8.3 | −8.34 | −8.4 | −8.38 | −8.36 | −8.34 | −8.35 | −8.37 | −8.36 | −8.38 |
| 11 | −8.44 | −8.4 | −8.48 | −8.5 | −8.46 | −8.47 | −8.5 | −8.47 | −8.47 | −8.48 | −8.48 | −8.49 |
| 10.8 | −8.51 | −8.51 | −8.54 | −8.56 | −8.52 | −8.56 | −8.59 | −8.57 | −8.57 | −8.54 | −8.57 | −8.58 |
| 10.6 | −8.68 | −8.72 | −8.7 | −8.7 | −8.69 | −8.7 | −8.74 | −8.75 | −8.72 | −8.69 | −8.68 | −8.69 |
| 10.4 | −8.8 | −8.9 | −8.94 | −8.92 | −8.91 | −8.92 | −8.91 | −8.92 | −8.93 | −8.94 | −8.9 | −8.92 |
| 10.2 | −9.12 | −9.11 | −9.13 | −9.11 | −9.12 | −9.16 | −9.17 | −9.15 | −9.14 | −9.18 | −9.16 | −9.17 |
| 10 | −9.35 | −9.36 | −9.34 | −9.33 | −9.37 | −9.4 | −9.38 | −9.32 | −9.38 | −9.36 | −9.37 | −9.38 |
| 9.8 | −9.34 | −9.36 | −9.37 | −9.36 | −9.35 | −9.37 | −9.36 | −9.33 | −9.34 | −9.35 | −9.37 | −9.34 |
| 9.6 | −9.49 | −9.46 | −9.48 | −9.46 | −9.47 | −9.5 | −9.51 | −9.48 | −9.51 | −9.49 | −9.51 | −9.48 |
| 9.4 | −9.58 | −9.69 | −9.7 | −9.63 | −9.69 | −9.65 | −9.64 | −9.71 | −9.65 | −9.64 | −9.63 | −9.62 |
| 9.2 | −9.71 | −9.74 | −9.73 | −9.75 | −9.76 | −9.78 | −9.76 | −9.74 | −9.78 | −9.77 | −9.76 | −9.78 |
| 9 | −9.87 | −9.89 | −9.91 | −9.89 | −9.94 | −9.9 | −9.91 | −9.88 | −9.91 | −9.9 | −9.87 | −9.87 |
| 8.8 | −10.0 | −10.0 | −10.0 | −10.0 | −10.0 | −10.0 | −10.0 | −10.0 | −10.0 | −10.0 | −10.0 | −10.0 |
| 8.6 | −10.1 | −10.1 | −10.1 | −10.1 | −10.1 | −10.1 | −10.1 | −10.1 | −10.1 | −10.1 | −10.1 | −10.1 |
| 8.4 | −10.2 | −10.2 | −10.2 | −10.2 | −10.2 | −10.2 | −10.3 | −10.3 | −10.3 | −10.2 | −10.2 | −10.3 |
| 8.2 | −10.3 | −10.3 | −10.3 | −10.2 | −10.2 | −10.3 | −10.3 | −10.3 | −10.2 | −10.2 | −10.2 | −10.3 |
| 8 | −10.3 | −10.3 | −10.3 | −10.3 | −10.3 | −10.3 | −10.3 | −10.3 | −10.3 | −10.3 | −10.3 | −10.3 |
| 7.8 | −10.3 | −10.3 | −10.3 | −10.3 | −10.4 | −10.3 | −10.3 | −10.3 | −10.3 | −10.3 | −10.3 | −10.3 |
| 7.6 | −10.3 | −10.3 | −10.3 | −10.4 | −10.3 | −10.3 | −10.3 | −10.3 | −10.3 | −10.4 | −10.3 | −10.3 |
| 7.4 | −10.3 | −10.3 | −10.3 | −10.4 | −10.4 | −10.4 | −10.4 | −10.4 | −10.4 | −10.3 | −10.3 | −10.4 |
| 7.2 | −10.4 | −10.4 | −10.4 | −10.4 | −10.4 | −10.4 | −10.4 | −10.4 | −10.4 | −10.4 | −10.4 | −10.4 |
| 7 | −10.4 | −10.4 | −10.4 | −10.4 | −10.4 | −10.4 | −10.4 | −10.4 | −10.4 | −10.4 | −10.4 | −10.4 |
| 6.8 | −10.3 | −10.3 | −10.3 | −10.3 | −10.4 | −10.4 | −10.4 | −10.4 | −10.4 | −10.3 | −10.4 | −10.3 |
| 6.6 | −10.3 | −10.3 | −10.3 | −10.3 | −10.3 | −10.3 | −10.3 | −10.4 | −10.3 | −10.3 | −10.3 | −10.3 |
| 6.4 | −10.3 | −10.3 | −10.3 | −10.3 | −10.3 | −10.3 | −10.3 | −10.3 | −10.3 | −10.3 | −10.3 | −10.3 |
| 6.2 | −10.2 | −10.2 | −10.3 | −10.3 | −10.2 | −10.2 | −10.2 | −10.3 | −10.3 | −10.2 | −10.3 | −10.3 |
| 6 | −10.2 | −10.2 | −10.2 | −10.2 | −10.2 | −10.2 | −10.2 | −10.3 | −10.3 | −10.3 | −10.2 | −10.2 |
| 5.8 | −10.2 | −10.2 | −10.2 | −10.2 | −10.2 | −10.2 | −10.2 | −10.2 | −10.2 | −10.2 | −10.2 | −10.2 |
| 5.6 | −10.2 | −10.2 | −10.2 | −10.2 | −10.2 | −10.2 | −10.2 | −10.2 | −10.2 | −10.2 | −10.2 | −10.2 |
| 5.4 | −10.1 | −10.2 | −10.2 | −10.2 | −10.1 | −10.2 | −10.2 | −10.2 | −10.2 | −10.2 | −10.2 | −10.2 |
| 5.2 | −10.1 | −10.1 | −10.2 | −10.2 | −10.1 | −10.2 | −10.2 | −10.2 | −10.2 | −10.2 | −10.2 | −10.2 |
| 5 | −10.2 | −10.1 | −10.1 | −10.1 | −10.1 | −10.1 | −10.2 | −10.1 | −10.2 | −10.1 | −10.2 | −10.2 |
| 4.8 | −10.0 | −10.0 | −10.0 | −10.0 | −10.0 | −10.0 | −10.0 | −10.0 | −10.0 | −10.0 | −10.0 | −10.0 |
| 4.6 | −9.87 | −9.97 | −9.9 | −9.86 | −9.94 | −9.98 | −9.99 | −9.92 | −9.96 | −9.97 | −9.94 | −9.96 |
| 4.4 | −9.74 | −9.8 | −9.86 | −9.85 | −9.87 | −9.88 | −9.88 | −9.87 | −9.87 | −9.87 | −9.82 | −9.84 |
| x | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 4.2 | −9.75 | −9.76 | −9.69 | −9.69 | −9.71 | −9.72 | −9.69 | −9.7 | −9.69 | −9.68 | −9.75 | −9.75 |
| 4 | −9.6 | −9.58 | −9.59 | −9.57 | −9.62 | −9.63 | −9.59 | −9.67 | −9.64 | −9.63 | −9.63 | −9.69 |
| 3.8 | −9.52 | −9.48 | −9.47 | −9.53 | −9.5 | −9.51 | −9.49 | −9.54 | −9.52 | −9.52 | −9.51 | |
| 3.6 | −9.46 | −9.44 | −9.45 | −9.5 | −9.52 | −9.48 | −9.46 | −9.47 | −9.51 | −9.48 | −9.51 | −9.53 |
| 3.4 | −9.42 | −9.38 | −9.44 | −9.46 | −9.45 | −9.42 | −9.47 | −9.44 | −9.45 | −9.46 | −9.47 | −9.48 |
| 3.2 | −9.37 | −9.35 | −9.36 | −9.42 | −9.41 | −9.38 | −9.42 | −9.4 | −9.39 | −9.41 | −9.42 | −9.38 |
| 3 | −9.28 | −9.32 | −9.36 | −9.29 | −9.37 | −9.35 | −9.29 | −9.28 | −9.28 | −9.38 | −9.4 | −9.38 |
| 2.8 | −9.25 | −9.26 | −9.31 | −9.32 | −9.3 | −9.27 | −9.28 | −9.32 | −9.25 | −9.36 | −9.29 | −9.34 |
| 2.6 | −9.17 | −9.19 | −9.21 | −9.2 | −9.18 | −9.17 | −9.23 | −9.21 | −9.18 | −9.22 | −9.25 | −9.26 |
| 2.4 | −8.93 | −8.89 | −8.99 | −9.28 | −9.21 | −9.16 | −9.08 | −9.18 | −9.21 | −9.18 | −9.18 | −9.17 |
| 2.2 | −8.87 | −8.96 | −8.74 | −8.93 | −8.88 | −8.91 | −8.94 | −8.92 | −8.87 | −8.84 | −8.79 | −8.88 |
| 2 | −8.4 | −8.55 | −8.56 | −8.47 | −8.56 | −8.49 | −8.6 | −8.62 | −8.48 | −8.63 | −8.6 | −8.54 |
| 1.8 | −8.29 | −8.02 | −8.21 | −8.19 | −8.17 | −8.09 | −8.08 | −8.16 | −8.24 | −8.27 | −8.22 | −8.3 |
| 1.6 | −7.89 | −7.94 | −7.99 | −7.86 | −7.89 | −7.97 | −7.93 | −7.97 | −7.93 | −7.99 | −7.6 | −7.95 |
| 1.4 | −7.74 | −7.79 | −7.78 | −7.8 | −7.83 | −7.89 | −7.9 | −7.89 | −7.79 | −7.89 | −7.89 | −7.87 |
| 1.2 | −7.65 | −7.72 | −7.73 | −7.69 | −7.74 | −7.68 | −7.64 | −7.78 | −7.69 | −7.76 | −7.74 | −7.71 |
| 1 | −7.63 | −7.61 | −7.61 | −7.58 | −7.59 | −7.54 | −7.64 | −7.62 | −7.6 | −7.58 | −7.57 | −7.68 |
| 0.8 | −7.32 | −7.58 | −7.39 | −7.52 | −7.38 | −7.52 | −7.49 | −7.39 | −7.55 | −7.48 | −7.53 | −7.55 |
| 0.6 | −7.29 | −7.32 | −7.4 | −7.39 | −7.38 | −7.39 | −7.35 | −7.38 | −7.37 | −7.4 | −7.3 | −7.34 |
| 0.4 | −7.21 | −7.2 | −7.25 | −7.29 | −7.21 | −7.28 | −7.24 | −7.25 | −7.19 | −7.18 | −7.26 | −7.22 |
| 0.2 | −7.05 | −7.12 | −7.08 | −7.22 | −7.09 | −7.12 | −7.11 | −7.14 | −7.03 | −7.12 | −7.13 | −7.13 |
| 0 | −6.95 | −6.97 | −6.94 | −7.2 | −6.96 | −6.98 | −6.91 | −6.95 | −6.93 | −7.09 | −6.98 | −6.99 |
| −0.2 | −6.88 | −6.92 | −6.87 | −6.84 | −6.88 | −6.84 | −6.84 | −6.86 | −6.87 | −6.89 | −6.89 | −6.88 |
| −0.4 | −6.82 | −6.78 | −6.76 | −6.74 | −6.81 | −6.79 | −6.48 | −6.82 | −6.81 | −6.76 | −6.73 | −6.78 |
| −0.6 | −6.64 | −6.68 | −6.8 | −6.84 | −6.73 | −6.74 | −6.72 | −6.48 | −6.44 | −6.58 | −6.57 | −6.53 |
| −0.8 | −6.58 | −6.48 | −6.59 | −6.52 | −6.49 | −6.6 | −6.46 | −6.48 | −6.51 | −6.5 | −6.47 | −6.42 |
| −1 | −6.49 | −6.41 | −6.42 | −6.43 | −6.48 | −6.49 | −6.52 | −6.51 | −6.47 | −6.44 | −6.45 | −6.34 |
| −1.2 | −6.39 | −6.32 | −6.34 | −6.38 | −6.35 | −6.27 | −6.42 | −6.29 | −6.36 | −6.32 | −6.39 | −6.42 |
| −1.4 | −6.1 | −6.19 | −6.01 | −6.25 | −6.02 | −5.95 | −5.89 | −6.01 | −5.98 | −5.91 | −5.97 | −5.87 |
| 1.2 | −7.65 | −7.72 | −7.73 | −7.69 | −7.74 | −7.68 | −7.64 | −7.78 | −7.69 | −7.76 | −7.74 | −7.71 |
| 1 | −7.63 | −7.61 | −7.61 | −7.58 | −7.59 | −7.54 | −7.64 | −7.62 | −7.6 | −7.58 | −7.57 | −7.68 |
| 0.8 | −7.32 | −7.58 | −7.39 | −7.52 | −7.38 | −7.52 | −7.49 | −7.39 | −7.55 | −7.48 | −7.53 | −7.55 |
| 0.6 | −7.29 | −7.32 | −7.4 | −7.39 | −7.38 | −7.39 | −7.35 | −7.38 | −7.37 | −7.4 | −7.3 | −7.34 |
| 0.4 | −7.21 | −7.2 | −7.25 | −7.29 | −7.21 | −7.28 | −7.24 | −7.25 | −7.19 | −7.18 | −7.26 | −7.22 |
| 0.2 | −7.05 | −7.12 | −7.08 | −7.22 | −7.09 | −7.12 | −7.11 | −7.14 | −7.03 | −7.12 | −7.13 | −7.13 |
| 0 | −6.95 | −6.97 | −6.94 | −7.2 | −6.96 | −6.98 | −6.91 | −6.95 | −6.93 | −7.09 | −6.98 | −6.99 |
| −0.2 | −6.88 | −6.92 | −6.87 | −6.84 | −6.88 | −6.84 | −6.84 | −6.86 | −6.87 | −6.89 | −6.89 | −6.88 |
| −0.4 | −6.82 | −6.78 | −6.76 | −6.74 | −6.81 | −6.79 | −6.48 | −6.82 | −6.81 | −6.76 | −6.73 | −6.78 |
| −0.6 | −6.64 | −6.68 | −6.8 | −6.84 | −6.73 | −6.74 | −6.72 | −6.48 | −6.44 | −6.58 | −6.57 | −6.53 |
| −0.8 | −6.58 | −6.48 | −6.59 | −6.52 | −6.49 | −6.6 | −6.46 | −6.48 | −6.51 | −6.5 | −6.47 | −6.42 |
| −1 | −6.49 | −6.41 | −6.42 | −6.43 | −6.48 | −6.49 | −6.52 | −6.51 | −6.47 | −6.44 | −6.45 | −6.34 |
| −1.2 | −6.39 | −6.32 | −6.34 | −6.38 | −6.35 | −6.27 | −6.42 | −6.29 | −6.36 | −6.32 | −6.39 | −6.42 |
| −1.4 | −6.1 | −6.19 | −6.01 | −6.25 | −6.02 | −5.95 | −5.89 | −6.01 | −5.98 | −5.91 | −5.97 | −5.87 |
| −1.6 | −6.23 | −6.3 | −6.2 | −6.19 | −6.32 | −6.25 | −6.24 | −6.24 | −6.23 | −6.25 | −6.19 | −6.18 |
| −1.8 | −5.58 | −5.69 | −5.68 | −5.67 | −5.67 | −5.59 | −5.61 | −5.67 | −5.68 | −5.72 | −5.79 | −5.79 |
| −1.6 | −5.31 | −5.39 | −5.24 | −5.57 | −5.9 | −5.69 | −5.42 | −5.42 | −5.36 | −5.72 | −5.53 | −5.67 |
| −1.4 | −5.39 | −5.38 | −5.36 | −5.42 | −5.44 | −5.39 | −5.37 | −5.48 | −5.38 | −5.34 | −5.38 | −5.37 |
| −1.2 | −5.19 | −5.22 | −5.02 | −5.03 | −5.34 | −5.42 | −5.15 | −5.21 | −5.16 | −5.49 | −5.2 | −5.29 |
| −1 | −5.1 | −5.09 | −5.08 | −5.08 | −5.12 | −5.11 | −5.1 | −5.09 | −5.08 | −5.07 | −5.09 | −5.12 |
| −0.8 | −4.6 | −4.89 | −4.64 | −5.19 | −4.97 | −5.2 | −4.89 | −4.97 | −4.98 | −4.98 | −4.9 | −4.97 |
| −0.6 | −3.2 | −3.26 | −3.3 | −3.29 | −3.29 | −3.27 | −3.34 | −3.35 | −3.35 | −3.28 | −3.4 | −3.19 |
| −0.4 | −2.5 | −2.49 | −2.48 | −2.44 | −2.46 | −2.48 | −2.46 | −2.49 | −2.45 | −2.51 | −2.52 | −2.48 |
| −0.2 | −1.62 | −1.64 | −1.61 | −1.63 | −1.64 | −1.62 | −1.62 | −1.61 | −1.65 | −1.64 | −1.68 | −1.66 |
References
- Gilbert, C.E.; Canovas, R.; Hagan, M.; Rao, S.; Foster, A. Causes of childhood blindness: Results from west Africa, south India and Chile. Eye 1993, 77, 184–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinkuller, P.G.; Du, L.; Gilbert, C.; Foster, A.; Collins, M.L.; Coats, D.K. Childhood blindness. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 1993, 3, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, C.; Foster, A. Childhood blindness in the context of VISION 2020: The right to sight. Bull. World Health Organ. 2001, 79, 227–232. [Google Scholar]
- Taylor, H.R.; Keeffe, J.E. World blindness: A 21st century perspective. Br. J. Ophthalmol. 2001, 85, 261–266. [Google Scholar] [CrossRef] [Green Version]
- Yorston, D. Retinal diseases and vision 2020. Community Eye Health 2003, 16, 19–20. [Google Scholar]
- Rahi, J.S. Childhood blindness: A UK epidemiological perspective. Eye 2007, 21, 1249–1253. [Google Scholar] [CrossRef] [Green Version]
- Nazimul, H.; Rohit, K.; Anjli, H. Trend of retinal diseases in developing countries. Expert Rev. Ophthalmol. 2008, 3, 43–50. [Google Scholar] [CrossRef]
- Kong, L.; Fry, M.; Al-Samarraie, M.; Gilbert, C.; Steinkuller, P.G. An update on progress and the changing epidemiology of causes of childhood blindness worldwide. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2012, 16, 501–507. [Google Scholar] [CrossRef]
- Gabrielle, P.H.; Nguyen, V.; Wolff, B.; Essex, R.; Young, S.; Hunt, A.; Cheung, C.M.G.; Arnold, J.J.; Barthelmes, D.; Creuzot- Garcher, C.; et al. Intraocular pressure changes and vascular endothelial growth factor inhibitor use in various retinal diseases: Long-term outcomes in routine clinical practice: Data from the Fight Retinal Blindness! Registry. Ophthalmol. Retin. 2020, 4, 861–870. [Google Scholar] [CrossRef]
- Heath Jeffery, R.C.; Mukhtar, S.A.; McAllister, I.L.; Morgan, W.H.; Mackey, D.A.; Chen, F.K. Inherited retinal diseases are the most common cause of blindness in the working-age population in Australia. Ophthalmic Genet. 2021, 42, 431–439. [Google Scholar] [CrossRef]
- Rattner, A.; Sun, H.; Nathans, J. Molecular genetics of human retinal diseases. Annu. Rev. Genet. 1999, 33, 89–131. [Google Scholar] [CrossRef] [PubMed]
- Bok, D. Contributions of genetics to our understanding of inherited monogenic retinal diseases and age-related macular degeneration. Arch. Ophthalmol. 2007, 125, 160–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiser, P.D.; Palczewski, K. Retinoids and retinal diseases. Annu. Rev. Vis. Sci. 2016, 2, 197–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanow, M.A.; Giarmarco, M.M.; Jankowski, C.S.; Tsantilas, K.; Engel, A.L.; Du, J.; Linton, J.D.; Farnsworth, C.C.; Sloat, S.R.; Rountree, A.; et al. Biochemical adaptations of the retina and retinal pigment epithelium support a metabolic ecosystem in the vertebrate eye. elife 2017, 6, e28899. [Google Scholar] [CrossRef]
- Amin, S.V.; Khanna, S.; Parvar, S.P.; Shaw, L.T.; Dao, D.; Hariprasad, S.M.; Skondra, D. Metformin and retinal diseases in preclinical and clinical studies: Insights and review of literature. Exp. Biol. Med. 2022, 247, 317–329. [Google Scholar] [CrossRef] [PubMed]
- Barnstable, C.J. Epigenetics and degenerative retinal diseases: Prospects for new therapeutic approaches. The Asia-Pac. J. Ophthalmol. 2022, 11, 328–334. [Google Scholar] [CrossRef]
- Chen, Y.; Coorey, N.J.; Zhang, M.; Zeng, S.; Madigan, M.C.; Zhang, X.; Gillies, M.C.; Zhu, L.; Zhang, T. Metabolism dysregulation in retinal diseases and related therapies. Antioxidants 2022, 11, 942. [Google Scholar] [CrossRef]
- Platania, C.B.M.; Drago, F.; Bucolo, C. The P2X7 receptor as a new pharmacological target for retinal diseases. Biochem. Pharmacol. 2022, 114942. [Google Scholar] [CrossRef]
- De Fauw, F.; Ledsam, J.R.; Romera-Paredes, B.; Nikolov, S.; Tomasev, N.; Blackwell, S.; Askham, H.; Glorot, X.; O’Donoghue, B.; Visentin, D.; et al. Clinically applicable deep learning for diagnosis and referral in retinal diseases. Nat. Med. 2018, 24, 1342–1350. [Google Scholar] [CrossRef]
- Jin, K.; Yan, Y.; Chen, M.; Wang, J.; Pan, X.; Liu, X.; Liu, M.; Lou, L.; Wang, Y.; Ye, J. Multimodal deep learning with feature level fusion for identification of choroidal neovascularization activity in age-related macular degeneration. Acta Ophthalmol. 2022, 100, e512–e520. [Google Scholar] [CrossRef]
- Al-Zamil, W.N.; Yassin, S.A. Recent developments in age-related macular degeneration: A review. Clin. Interv. Aging 2017, 12, 1313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tadayoni, R.; Sararols, L.; Weissgerber, G.; Verma, R.; Clemens, A.; Holz, F.G. Brolucizumab: A newly developed anti-VEGF molecule for the treatment of neovascular age-related macular degeneration. Ophthalmologica 2021, 244, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Heier, J.S.; Khanani, A.M.; Ruiz, C.Q.; Basu, K.; Ferrone, P.J.; Brittain, C.; Figueroa, M.S.; Lin, H.; Holz, F.G.; BPharm, V.P.; et al. Efficacy, durability, and safety of intravitreal faricimab up to every 16 weeks for neovascular age-related macular degeneration (TENAYA and LUCERNE): Two randomised, double-masked, phase 3, non-inferiority trials. Lancet 2022, 399, 729–740. [Google Scholar] [CrossRef]
- Hufendiek, K.; Pielen, A.; Framme, C. Strategies of Intravitreal Injections with Anti-VEGF: “Pro re Nata versus Treat and Extend”. Klin. Monatsblatter Augenheilkd. 2017, 235, 930–939. [Google Scholar]
- Augsburger, M.; Sarra, G.M.; Imesch, P. Treat and extend versus pro re nata regimens of ranibizumab and aflibercept in neovascular age-related macular degeneration: A comparative study. Graefe’s Arch. Clin. Exp. Ophthalmol. 2019, 257, 1889–1895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mantel, I.; Zola, M.; De Massougnes, S.; Dirani, A.; Bergin, C. Factors influencing macular atrophy growth rates in neovascular age-related macular degeneration treated with ranibizumab or aflibercept according to an observe-and-plan regimen. Br. J. Ophthalmol. 2019, 103, 900–905. [Google Scholar] [CrossRef]
- Sarkar, A.; Sodha, S.J.; Junnuthula, V.; Kolimi, P.; Dyawanapelly, S. Novel and investigational therapies for wet and dry age-related macular degeneration. Drug Discov. Today 2022, 27, 2322–2332. [Google Scholar] [CrossRef]
- Herlihy, K.P.; Williams, S.; Owens, G.; Savage, J.; Gardner, L.; Robeson, R.; Maynor, B.; Navratil, T.; Gilger, B.C.; Yerxa, B.R. Extended release of microfabricated protein particles from biodegradable hydrogel implants for the treatment of age related macular degeneration. Investig. Ophthalmol. Vis. Sci. 2014, 55, 1960. [Google Scholar]
- Seah, I.; Zhao, X.; Lin, Q.; Liu, Z.; Su, S.Z.Z.; Yuen, Y.S.; Hunziker, W.; Lingam, G.; Loh, X.J.; Su, X. Use of biomaterials for sustained delivery of anti-VEGF to treat retinal diseases. Eye 2020, 34, 1341–1356. [Google Scholar] [CrossRef] [Green Version]
- Kathawate, J.; Acharya, S. Computational modeling of intravitreal drug delivery in the vitreous chamber with different vitreous substitutes. J. Abbr. 2008, 51, 5598–5609. [Google Scholar] [CrossRef]
- Dörsam, S.; Friedmann, E.; Stein, J. Modeling and Simulations of Drug Distribution in the Human Vitreous. Top. Probl. Fluid Mech. 2017, 95–102. [Google Scholar] [CrossRef] [Green Version]
- Haghjou, N.; Abdekhodaie, M.J.; Cheng, Y.L.; Saadatmand, M. Computer Modeling of Drug Distribution after Intravitreal Administration. World Acad. Sci. Eng. Technol. 2011, 5, 194–204. [Google Scholar]
- Jooybar, E.; Abdekhodaiea, M.J.; Farhadia, F.; Cheng, Y.L. Computational modeling of drug distribution in the posterior segment of the eye: Effects of device variables and positions. Math. Biosci. 2014, 255, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Ansys Fluent. Southpointe 2600 Ansys Drive Canonsburg. Available online: https://www.ansys.com/ (accessed on 28 December 2022).
- Penkova, A.N.; Martinez, J.C.; Humayun, M.; Tadle, A.; Galesic, A.; Calle, A.; Thompson, M.; Pratt, M.; Sadhal, S.S. Bevacizumab diffusion coefficient in vivo measurement of rabbit vitreous humor with flourescein. Investig. Ophthalmol. Vis. Sci.. 2019, 60, 1552–5783. [Google Scholar]
- Friedrich, S.; Cheng, Y.L.; Saville,, B. FE modeling of drug distribution in the vitreous humor of the rabbit eye. Ann. Biomed. Eng. 1997, 25, 303–314. [Google Scholar] [CrossRef]
- Kim, R.Y.; Kwon, S.; Ra, H. Gravity influences bevacizumab distribution in an undisturbed balanced salt solution in vitro. PLoS ONE 2019, 14, e0223418. [Google Scholar] [CrossRef]
- Friedmann, E.; Dörsam, S.; Olkhovskiy, V. Test and optimization of medical treatments for the human eye. european patent application EP3776566, 2018. Available online: https://register.epo.org/espacenet/regviewer?AP=19714667&CY=EP&LG=en&DB=REG (accessed on 12 January 2023).
- Dörsam, S. Finite Element Simulations for the Design of Therapeutical Approaches for Retinal Diseases. Ph.D. Thesis, University of Kassel, Kassel, Germany, 2022. [Google Scholar]
- Stein, J. Modeling of Drug Distribution in the Human Vitreous for the Treatment of Retinal Diseases. Ph.D. Thesis, University of Kassel, Kassel, Germany, 2021. Available online: https://kobra.uni-kassel.de/handle/123456789/13993 (accessed on 28 December 2022).
- Drobny, A.; Friedmann, E. Numerical simulation of viscoelastic fluid-structure interaction problems and drug therapy in the eye. Proc. Appl. Math. Mech. 2021, 20, e202000260. [Google Scholar] [CrossRef]
- Bangerth, W.; Heister, T.; Heltai, L.; Kanschat, G.; Kronbichler, M.; Maier, M.; Turcksin, B.; Young, T. The textttdeal.II Library, Version 8.2. In Archive of Numerical Software; University of Heidelberg: Heidelberg, Gemany, 2015; Volume 3, pp. 1–8. [Google Scholar] [CrossRef]
- Bangerth, W.; Hartmann, R.; Kanschat, G. Deal.II—A General Purpose Object Oriented Finite Element Library. ACM Trans. Math. Softw. 2007, 33, 24/1–24/27. [Google Scholar] [CrossRef] [Green Version]
- Großmann, C.; Roos, H.G.; Stynes, M. Numerical Treatment of Partial Differential Equations; Springer: Berlin/Heidelberg, Germany; New York, NY, USA, 2007. [Google Scholar]
- Meidner, D.; Richter, T. Goal-oriented error estimation for the fractional step theta scheme. Comput. Methods Appl. Math. 2014, 288, 45–59. [Google Scholar]
- Benzi, M.; Golub, G.H.; Liesen, J. Numerical solution of saddle point problems. Acta Numer. 2005, 14, 1–137. [Google Scholar] [CrossRef] [Green Version]
- Hestenes, M.R.; Stiefel, E. Methods of conjugate gradients for solving linear systems. J. Res. Natl. Bur. Stand. 1952, 49, 409–436. [Google Scholar] [CrossRef]
- Saad, Y.; Schultz, M.H. A Generalized Minimal Residual Algorithm for Solving Nonsymmetric Linear Systems. SIAM J. Sci. Stat. Comput. 1986, 7, 856–869. [Google Scholar] [CrossRef] [Green Version]
- Heier, J.S.; Bressler, N.M.; Avery, R.L.; Bakri, S.J.; Boyer, D.S.; Brown, D.M.; Dugel, P.U.; Freund, K.B.; Glassman, A.R.; Kim, J.E.; et al. Comparison of Aflibercept, Bevacizumab, and Ranibizumab for Treatment of Diabetic Macular Edema: Extrapolation of Data to Clinical Practice. JAMA Ophthalmol. 2016, 134, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Wells, J.A.; Glassman, A.R.; Ayala, A.R.; Jampol, L.M.; Bressler, N.M.; Bressler, S.B.; Brucker, A.J.; Ferris, F.L.; Hampton, G.R.; Jhaveri, C.; et al. Aflibercept, Bevacizumab, or Ranibizumab for Diabetic Macular Edema: Two-Year Results from a Comparative Effectiveness Randomized Clinical Trial. Ophthalmology 2016, 123, 1351–1359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, S.; Bressler, N.M. Aflibercept, bevacizumab or ranibizumab for diabetic macular oedema. Curr. Opin. Ophthalmol. 2017, 28, 636–643. [Google Scholar] [CrossRef] [PubMed]
- CATT Research Group. Ranibizumab and Bevacizumab for Neovascular Age-Related Macular Degeneration. N. Engl. J. Med. 2011, 364, 1897–1908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarwar, S.; Clearfield, E.; Soliman, M.K.; Sadiq, M.A.; Baldwin, A.J.; Hanout, M.; Agarwal, A.; Sepah, Y.J.; Do, D.V.; Nguyen, Q.D. Aflibercept for neovascular age-related macular degeneration. In Cochrane Database of Systematic Reviews; John Wiley and Sons, Ltd.: Hoboken, NJ, USA, 2016; Volume 2, pp. 1465–1858. [Google Scholar]
- Park, S.C.; Su, D.; Tello, C. Anti-VEGF therapy for the treatment of glaucoma: A focus on ranibizumab and bevacizumab. Expert. Opin. Biol. Ther. 2012, 12, 1641–1647. [Google Scholar] [CrossRef]
- Andreoli, C.M.; Miller, J.W. Anti-vascular endothelial growth factor therapy for ocular neovascular diseaser. Curr. Opin. Ophthalmol. 2007, 18, 502–508. [Google Scholar] [CrossRef]
- Al-Latayfeh, M.; Silva, P.S.; Sun, J.K.; Aiello, L.P. Antiangiogenic therapy for ischemic retinopathies. Cold Spring Harb. Perspect. Med. 2012, 2, a006411. [Google Scholar] [CrossRef] [Green Version]
- Chang, J.H.; Garg, N.K.; Lunde, E.; Han, K.Y.; Jain, S.; Azar, D.T. Corneal neovascularization: An anti-VEGF therapy review. Surv. Ophthalmol. 2012, 57, 415–429. [Google Scholar] [CrossRef] [Green Version]
- Drobny, A. Mathematical Modeling and Adaptive Finite Element Simulation of Viscoelastic Fluid-Structure Interaction Systems and Chemical Processes with Applications to Ophthalmology. Ph.D. Thesis, University of Kassel, Kassel, Germany, 2022. [Google Scholar]
- Pożarowska, D.; Pożarowski, P. The era of anti-vascular endothelial growth factor (VEGF) drugs in ophthalmology, VEGF and anti-VEGF therapy. Cent. Eur. J. Immunol. 2016, 41, 311–316. [Google Scholar] [CrossRef] [PubMed]










Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Friedmann, E.; Dörsam, S.; Auffarth, G.U. Models and Algorithms for the Refinement of Therapeutic Approaches for Retinal Diseases. Diagnostics 2023, 13, 975. https://doi.org/10.3390/diagnostics13050975
Friedmann E, Dörsam S, Auffarth GU. Models and Algorithms for the Refinement of Therapeutic Approaches for Retinal Diseases. Diagnostics. 2023; 13(5):975. https://doi.org/10.3390/diagnostics13050975
Chicago/Turabian StyleFriedmann, Elfriede, Simon Dörsam, and Gerd U. Auffarth. 2023. "Models and Algorithms for the Refinement of Therapeutic Approaches for Retinal Diseases" Diagnostics 13, no. 5: 975. https://doi.org/10.3390/diagnostics13050975