1. Introduction
The morphology of the adult knee joint is complex [
1,
2,
3,
4]. Therefore, an exact reconstruction of the physiological knee morphology by implants for knee joint replacement is difficult [
5,
6,
7,
8]. One approach is to use individually designed implants based on computed tomographic images [
9,
10]. Furthermore, the necessity of gender-specific implants is a discussed topic in the current literature [
11,
12,
13].
In particular, the morphology of the distal femur is difficult to reconstruct [
5,
7]. Regarding the age of individualised arthroplasty, the question arises whether currently available standard implants adequately represent femoral condylar morphology (FCM) [
7,
11]. The anterior (ACO) and posterior (PCO) condylar femoral offset have an influence on postoperative knee joint function and patients’ satisfaction after knee arthroplasty [
5,
14,
15,
16,
17,
18]. In this context, Zheng et al. analysed the phenomenon wherein patients describe the feeling of an increase in the size of their own knee after primary implantation of a total knee arthroplasty [
5]. The authors called this “patient-perceived enlargement of knee” (PPEK). The authors demonstrated that patients with PPEK have worse postoperative functional scores and satisfaction levels, while radiological analysis showed a significantly higher ACO and smaller PCO postoperatively in PPEK. In addition, increased ACO is associated with the occurrence of anterior knee pain [
5,
15]. An increase in patellofemoral contact pressure is assumed to be the causative factor [
5,
19]. There is ambiguity in the literature regarding the influence of PCO on postoperative outcome after total knee arthroplasty [
16,
17,
18,
20]. Some studies suggest that a reduction in PCO leads to bony impingement and flexion inhibition [
18,
20]. Other studies have failed to find associations between an increase or decrease in PCO with postoperative range of motion/occurrence of knee pain [
16,
17].
It can be concluded that FCM has a significant influence on postoperative outcome and patient satisfaction after total knee arthroplasty. There are findings which indicate that the current standard implants do not sufficiently reconstruct physiological FCM, which can lead to complaints in the form of knee pain and reduced mobility [
7,
11].
However, to the authors’ knowledge, no study exists in the current literature that provides reference values for physiological FCM based on a radiological examination of patients without manifest osteoarthritis.
Therefore, the aim of the present study was to investigate the physiological FCM retrospectively using magnetic resonance imaging (MRI), and to analyse the presence of side-, age-, gender- and joint degeneration-specific differences.
2. Materials and Methods
2.1. Patients
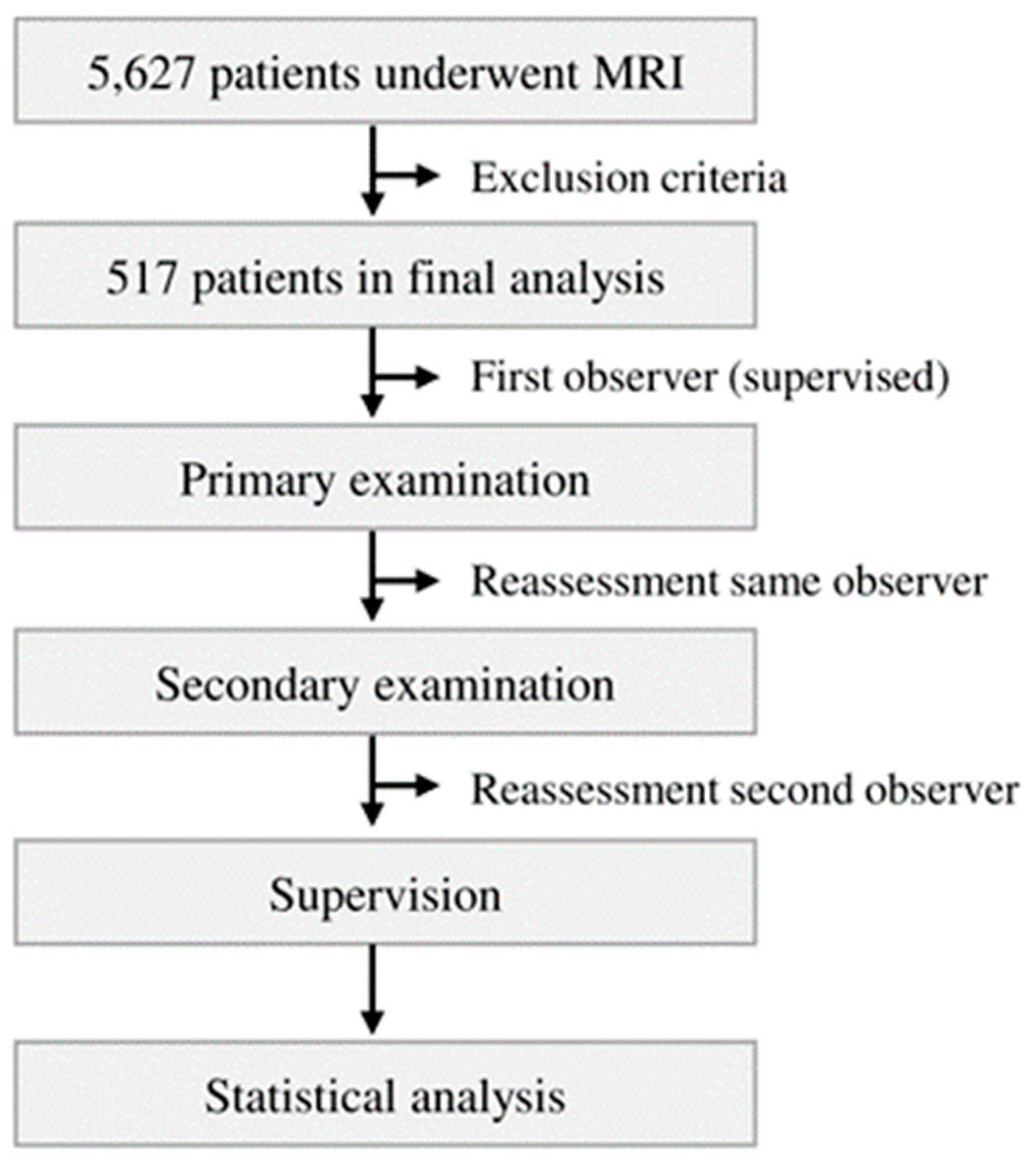
Between 2007 and 2020, a total of n = 5627 patients underwent magnetic resonance imaging of the knee joint in the Department for Diagnostic and Interventional Radiology of the University Medical Center Goettingen. These MRIs were reviewed retrospectively. After applying inclusion and exclusion criteria, 517 patients were included in the final analysis. The study collective was divided into two age groups (20–50 and >50 years). The study was approved by the local ethics committee (IRB number: 35/7/20) and performed in accordance with the principles expressed in the Declaration of Helsinki. Without exception, the evaluated MRIs were taken as part of routine diagnostics because of clinical symptoms. All MRIs were assessed by a senior radiologist and Y.H., M.-P.M., A.S.A.H. and T.H. to exclude extended structural injuries or heavy joint degeneration.
2.2. Inclusion Criteria
All examinations accessible via the PACS system (Picture Archiving and Communication System) between 1 January 2007 and 31 December 2020 were initially included in the study. Out of these, all patients with an age of 20 years or more were included. All MRI scans were performed on patients to assess knee joint pathologies. A Kellgren/Lawrence score [
21] ≥3 was classified as manifest osteoarthritis. The study collective was divided up in two groups (without and with radiological osteoarthritis). All MRIs were examined by the internal radiology department as part of the clinical diagnostic procedure. Every report was re-evaluated by Y.H., M.-P.M., A.S.A.H. and T.H. in a blinded fashion.
2.3. Exclusion Criteria
All patients with fractures, osteonecrosis, dysplasia, ligament damage or tumours were excluded. Patients who had undergone osteosynthesis or arthroplasty were likewise excluded. Similarly, the data did not include patients who had any other implants after knee joint preservation surgery. Low-quality MRIs (based on only a few gates), were excluded. In addition, all MRIs with imaging artefacts were ruled out.
2.4. MRI Analysis, Parameters and Methods of Measurement
All measurements were taken via the PACS system (Picture Archiving and Communication System). Software from GE Healthcare, called Centricity
TM Universal Viewer, was used (RA1000, edition 2019, Buckinghamshire, UK). The osteoarthritis score of each knee joint was classified according to Kellgren/Lawrence (KL, [
21]).
Table 1 shows the characteristics of the study population.
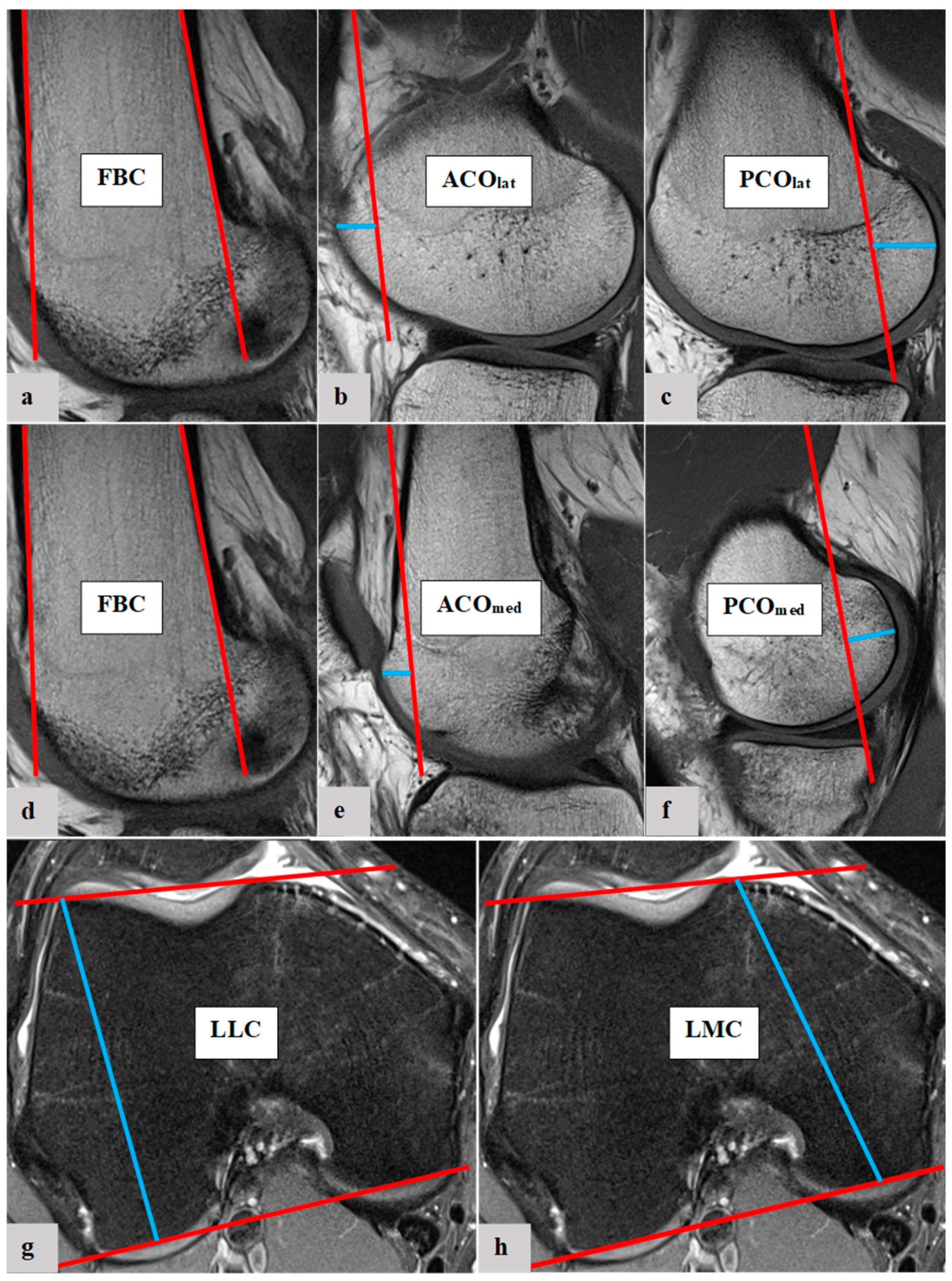
The femoral condylar offset parameters and length of femoral condyles were measured with established methods. The ACO
med, ACO
lat, PCO
med, PCO
lat, LMC and LLC were determined [
5,
7,
22]. To measure the femoral condylar offset parameters, the anterior and posterior femoral shaft bone cortex have to be determined in the sagittal view. Using measurement software, the position of each anterior and posterior femoral shaft axis was projected in the image, which best represented the anterior/posterior femoral condyle. The distance between the cortical bone of the anterior femoral condyle and the anterior cortex axis defines the ACO. According to the same principle, the PCO was defined in the posterior compartment, considering the posterior cortex axis and posterior cortical condylar bone. ACO and PCO were measured in the medial and lateral knee joint compartments. LMC and LLC were measured in axial view.
Figure 1 shows the experimental process of the presented study.
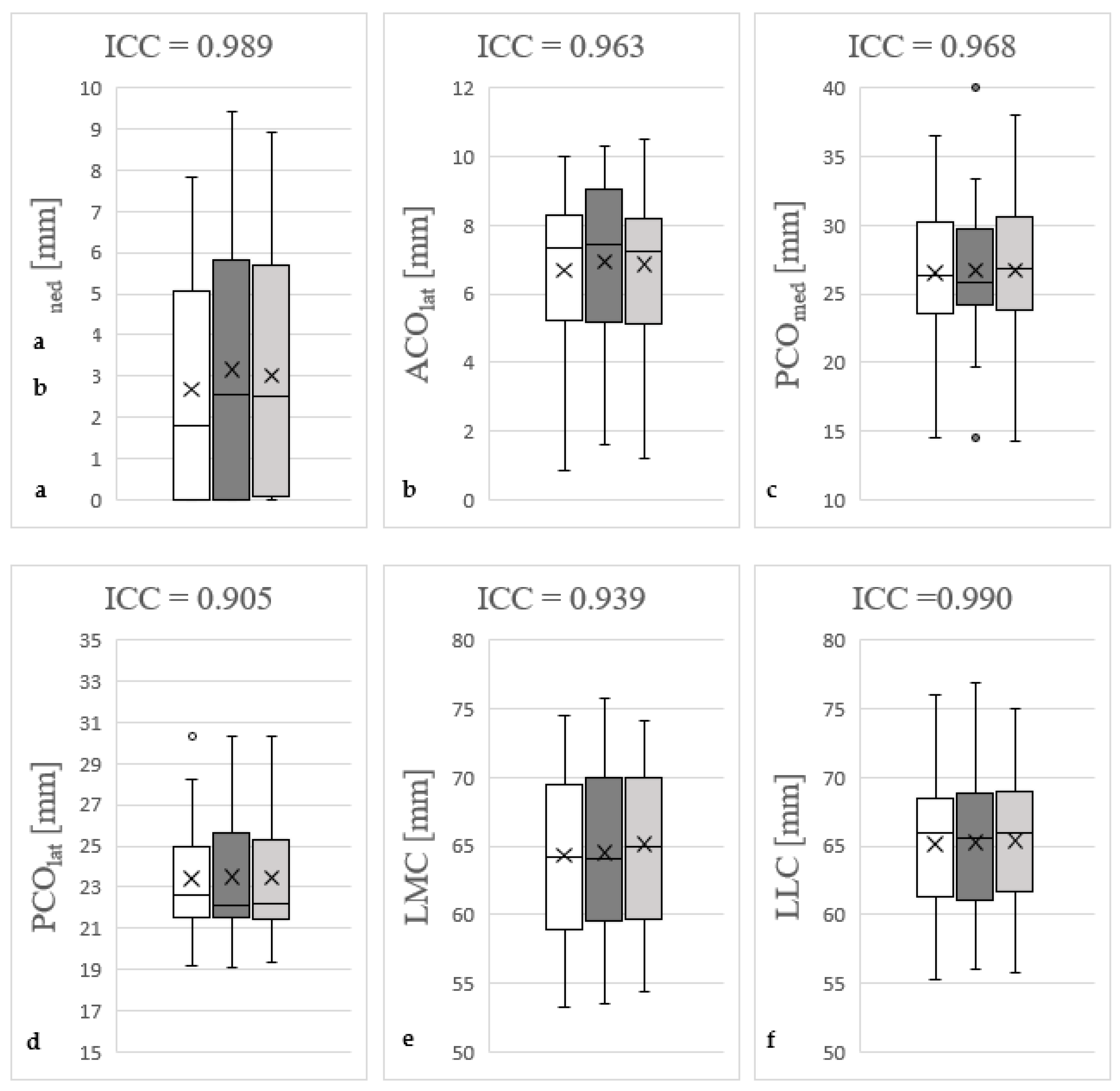
Figure 2 shows the measurement methodology in principle. Furthermore, the quotient of LMC/LLC was determined. All radiographic parameters in this MRI study were manually measured separately in a standardized manner by the same observer (Y.H.) under supervision of an experienced senior radiologist (A.S.A.H.). Intraobserver reliability of the measurements of all parameters was assessed for a subset of 50 subjects by blinded re-evaluation at 2 weeks after the first measurement and using the same technique. Interobserver reliability was assessed by two observers (Y.H. and M.-P.M.) independently for 50 subjects.
2.5. Statistics
For side-, age- and gender-specific analyses of ACOmed, ACOlat, PCOmed, PCOlat, LMC, LLC and LMC/LLC, a Mann–Whitney U test was used because data were not parametric. Likewise, a Mann–Whitney U test was implemented for the comparison of patients without and with osteoarthritis for all assessed parameters. Intra- and interobserver reliabilities were evaluated using intraclass correlation coefficients (ICC). Overall, mean ± standard deviation is stated. Statistical analysis was performed with GraphPad Prism 9.00 (GraphPad Software, San Diego, CA, USA), SPSS Statistics software version 27.0 (IBM SPSS Inc., Chicago, IL, USA) and Microsoft Excel (Microsoft Office 2016, Redmond, WA, USA). Significant differences are marked with asterisks (*** p < 0.001, ** p < 0.01, * p < 0.05).
4. Discussion
The morphology of the distal femur is complex [
1,
2,
3,
4]. Various studies showed that medial and lateral femoral condyle morphology differ in ACO, PCO and length [
23,
24,
25,
26]. In this context, the current literature raises the question of whether the existing standard implants for arthroplasty of the knee joint adequately consider the physiological morphology of femoral condyles [
11,
12,
13]. Knowledge of the exact physiological FCM is the prerequisite for clarifying the question of whether side-, age- and gender-specific implants are necessary in order to be able to take into account possible morphological differences in the FCM. In the present study, MRI scans of 517 knee joints were examined to establish reference values of FCM parameters for future diagnostic, preoperative planning and therapeutic applicability.
Kuo et al. retrospectively studied 199 patients who underwent total knee arthroplasty to determine whether the femoral arthroplasty component adequately represented the bony resection height of the anterior and posterior condyles. The authors demonstrated that current standard implants do not appropriately reconstruct ACO and PCO [
7].
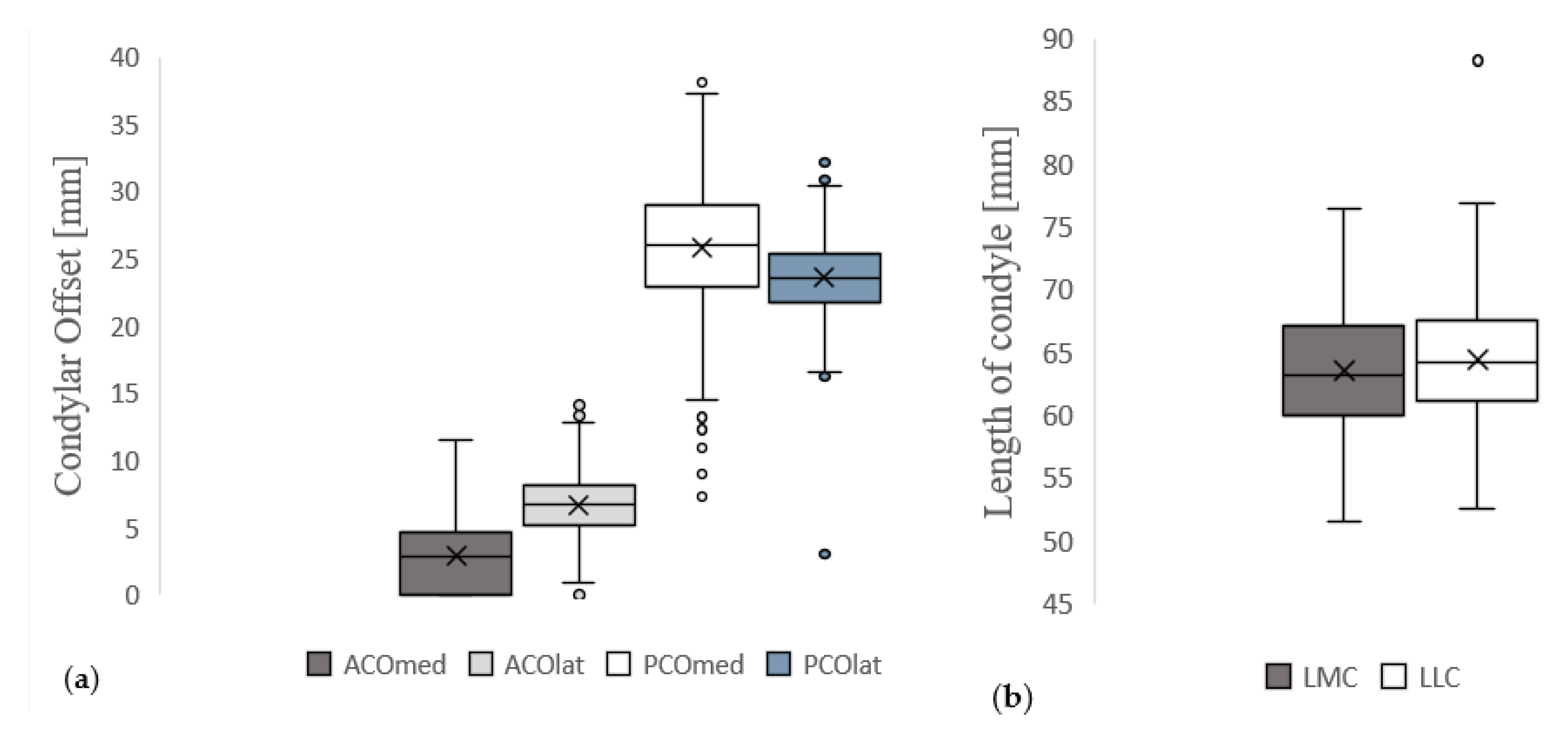
In our analysis, significantly higher mean values for ACO
med were found on the left compared to the right joint side. In contrast to that, the mean values for PCO
med and LMC/LLC were higher on the right joint side. To the authors’ knowledge, there is currently no other study that describes a side dependence of ACO
med, PCO
med and LMC/LLC in radiologically healthy knee joints. An explanation for these side-specific differences could be that 70–90% of the population use the right leg predominantly [
27]. However, due to the retrospective nature of the present study and not using intraindividual analysis, this assumption can only be made hypothetically. In order to finally clarify this question, additional studies are necessary that specifically examine the ACO
med, PCO
med and LMC/LLC between patients with left-leg and right-leg dominance and compare FCM intraindividually. If the assumption is confirmed in this type of study design, implants with side-specific configuration of the ACO and PCO would have to be used.
In this study, age-dependent differences for FCM parameters were not found. This result is consistent with the study of Wernecke et al. that analysed MRI scans of 287 male and 243 female patients in order to investigate the morphology of the posterior femoral condyles. Likewise, they found no correlation between patient age and PCO [
28]. To the authors’ knowledge, there are no other studies examining age-specific differences in FCM in the current literature. Therefore, there is no evidence that age-specific implants are needed for physiological reconstruction of the FCM.
The analysis revealed significantly higher mean values for ACOmed, ACOlat, PCOlat, LMC and LLC in male patients compared to female patients. This raises the question of whether gender-specific implants are needed for knee arthroplasty [
29]. Voleti et al. examined 100 patients with nonspecific knee pain via MRI to analyse gender-specific differences in PCO, condylar height and cartilage thickness for medial and lateral knee compartments [
24]. The authors were able to detect sex-specific differences in the comparison of the absolute measured values for PCO
med and PCO
lat, but not in the respective relation to condylar height. Therefore, they concluded that gender-specific implants may not be necessary. Our results also showed no significant gender differences for LMC/LCC and PCO
med. However, Voleti et al. did not consider anterior FCM. As demonstrated by Kuo et al., the current standard implants do not adequately represent the anterior FCM in particular [
7]. This is in accordance with the results of our study, as we found significant gender differences for ACO
med and ACO
lat. Taking these results for ACO into account, the statement of Voleti et al. that gender-specific implants are not needed is debatable. Furthermore, the analysed cohort of Voleti et al.—with 100 patients compared to the 517 analysed knee joints in this study—is rather small. The results of Wernecke et al. are consistent with our results for PCO, pointing out a significant larger PCO
lat in male knee joints and no significant gender dependency of PCO
med [
28]. Bao et al. examined CT scans of 80 patients to investigate posterior FCM [
30]. The authors found a significantly larger mean PCO
lat and PCO
med in males in comparison to females. It has to be noted that for radiological imaging of osseous structures, CT is more suitable than MRI. Perhaps because of this, Bao et al. were able to demonstrate a significant gender-specific difference for PCO
med. However, it must be pointed out that we also found slightly higher mean values for PCOmed in male knee joints compared to female joints, but without significant differences.
In summary, the ACO appears to exhibit gender specificity. In contrast to this, the published studies on PCO are inconclusive. The results, rather, speak for the necessity of gender-specific implants to adequately reconstruct the physiological FCM and thereby achieve the best possible postoperative outcome. To verify this hypothesis, future studies should investigate knee joint prostheses regarding their implant design. In general, a gender dependency of FCM should be investigated to confirm or to disprove these considerations. The results of the present study should be considered as a physiological reference for measured values of FCM.
The analysis of osteoarthritis-specific differences for FCM parameters showed only a significant difference for LMC/LLC, which pointed out a higher mean value in patients with radiological osteoarthritis (KL 3–4). The reason for this seems to be the increase in osteophytic rim attachments in higher stages of osteoarthritis. To the authors’ knowledge, no comparative study examining osteoarthritis-specific differences in FCM exists in the current literature. The assumption that the osteoarthritis-specific difference in LMC/LCC is due to osteophytic rim attachments should be considered clinically, as the osteophytic rim attachments can have an influence on the postoperative outcome after knee joint arthroplasty. Thus, Carender et al. showed that trochlear osteophytes are associated with an increased risk of failure of medial unicondylar knee arthroplasty [
31]. In particular, the resection of medial osteophytes is important for optimal balancing of knee joint endoprostheses [
32]. Taking into account the present results, the occurrence of osteophytes on the medial femoral condyle should, therefore, be conscientiously observed during knee joint arthroplasty, both in the preoperative diagnostics and intraoperatively.
These results illustrate the enormous importance of radiological diagnostics both for basic research for the possible optimisation of existing implant designs and for the preoperative planning of knee joint arthroplasty, especially in severely degenerated knee joints.

 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}