
Transcatheter Arterial Embolization for Alleviating Chronic Musculoskeletal Pain and Improving Physical Function: A Narrative Review

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Mechanisms Underlying Chronic Musculoskeletal Pain Associated with OA
3. Osteoarthritis
3.1. Knee Osteoarthritis
3.2. Trapeziometacarpal Osteoarthritis
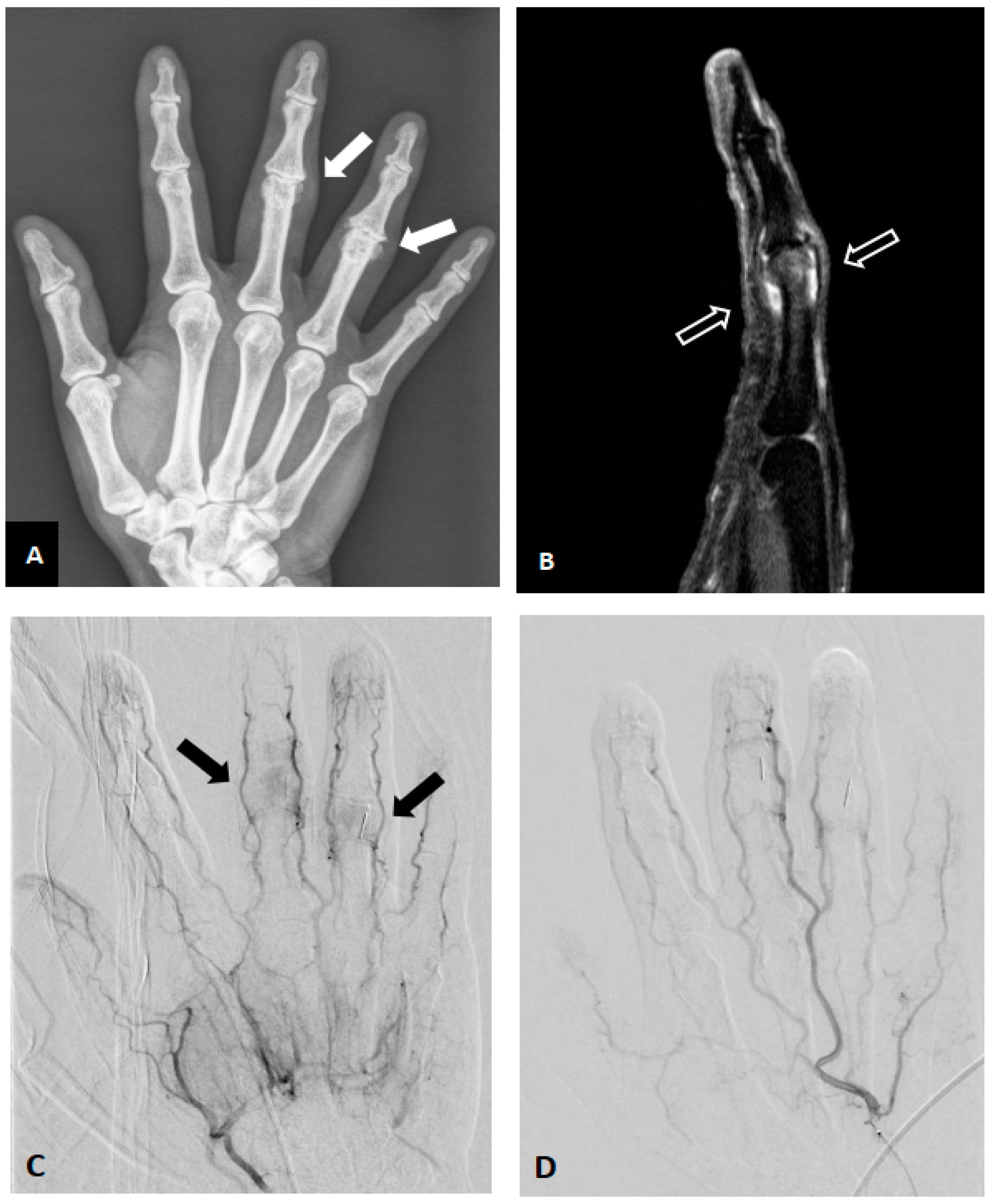
3.3. Finger Osteoarthritis
3.4. Facet Joints and Sacroiliac Joints Osteoarthritis
3.5. Shoulder Osteoarthritis
3.6. Osteoarthritis-Related synovitis
3.7. Osteoarthritis-Related Bone Marrow Lesion
4. Non-Osteoarthritic Synovitis
4.1. Adhesive Capsulitis (Synovium)
4.2. Secondary Adhesive Capsulitis (Post-Operation)
4.3. Hip Synovitis
5. Tendon and Enthesopathy
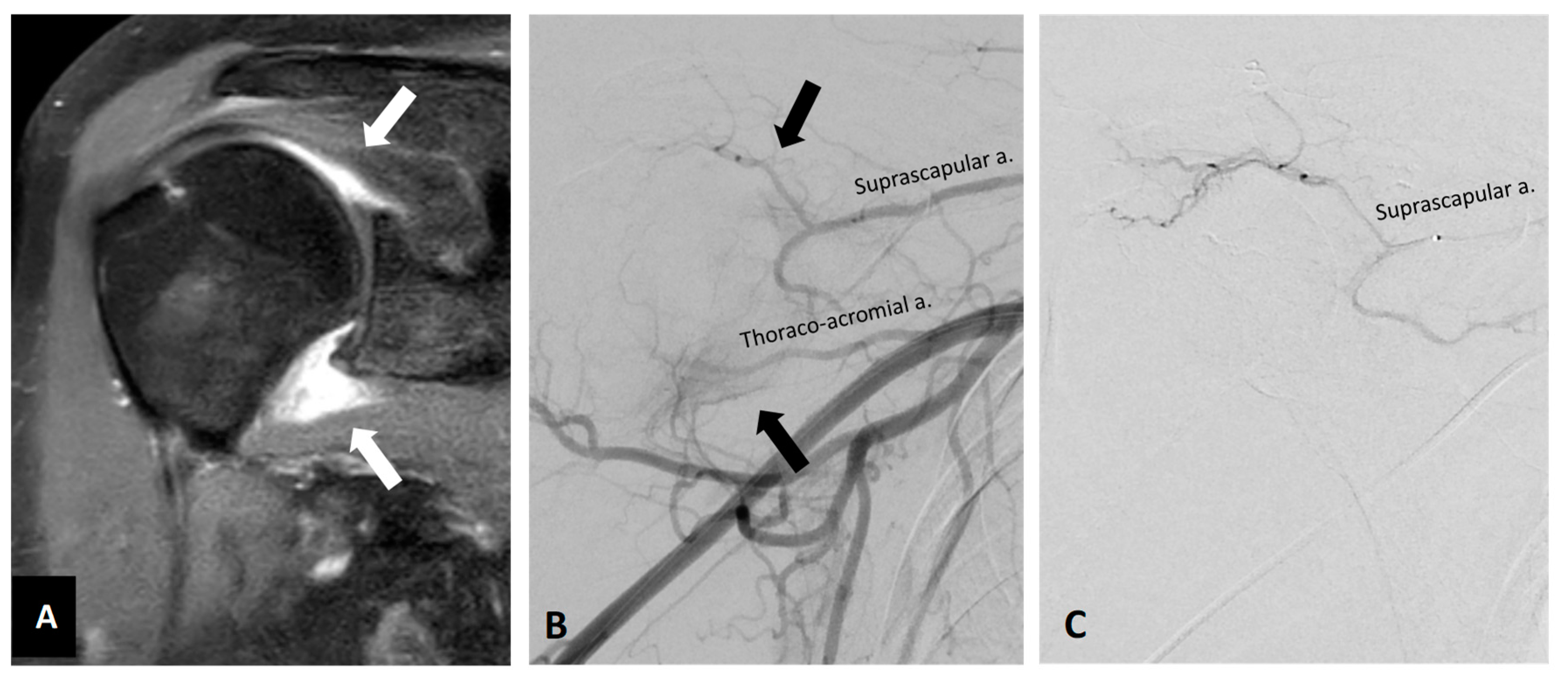
5.1. Shoulder Tendinopathy
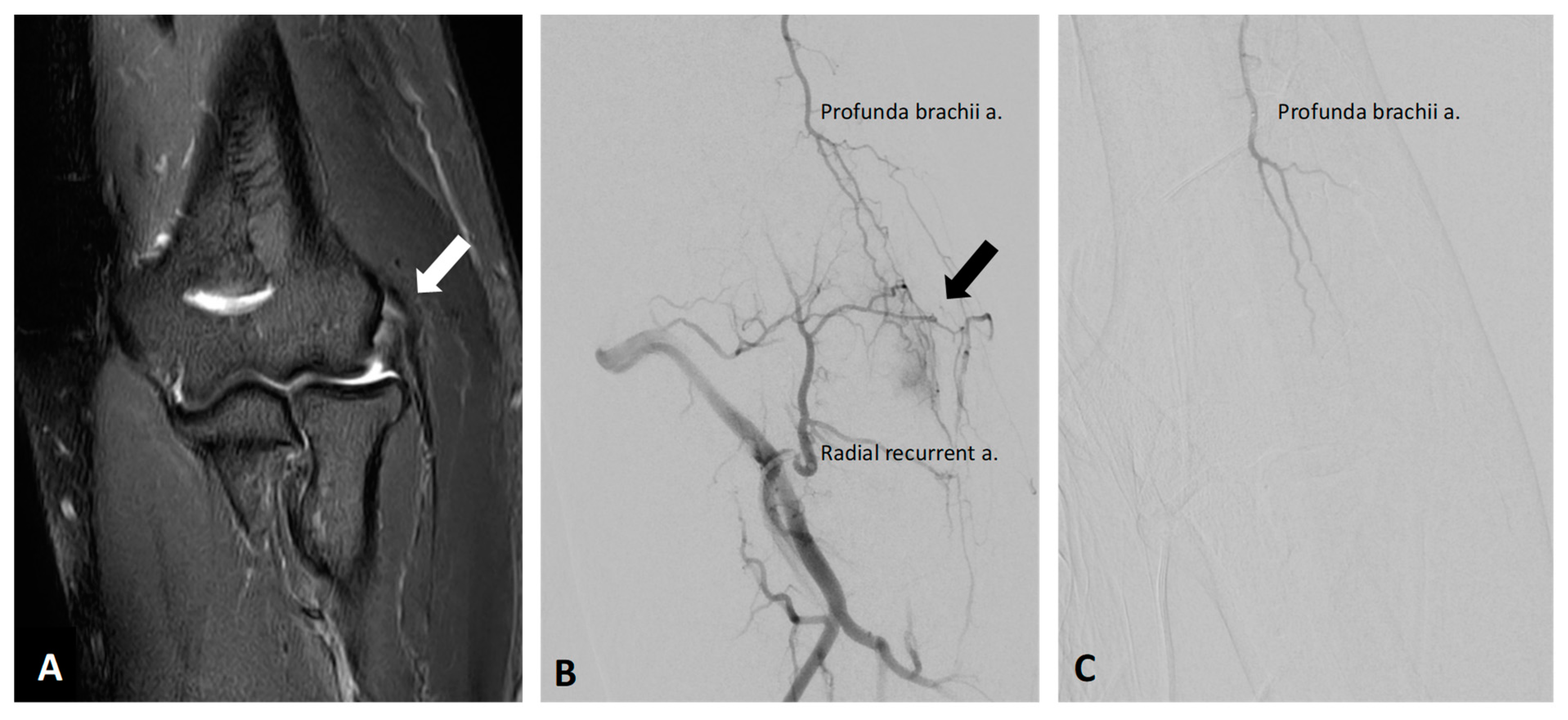
5.2. Lateral Epicondylitis
5.3. Medial Epicondylitis
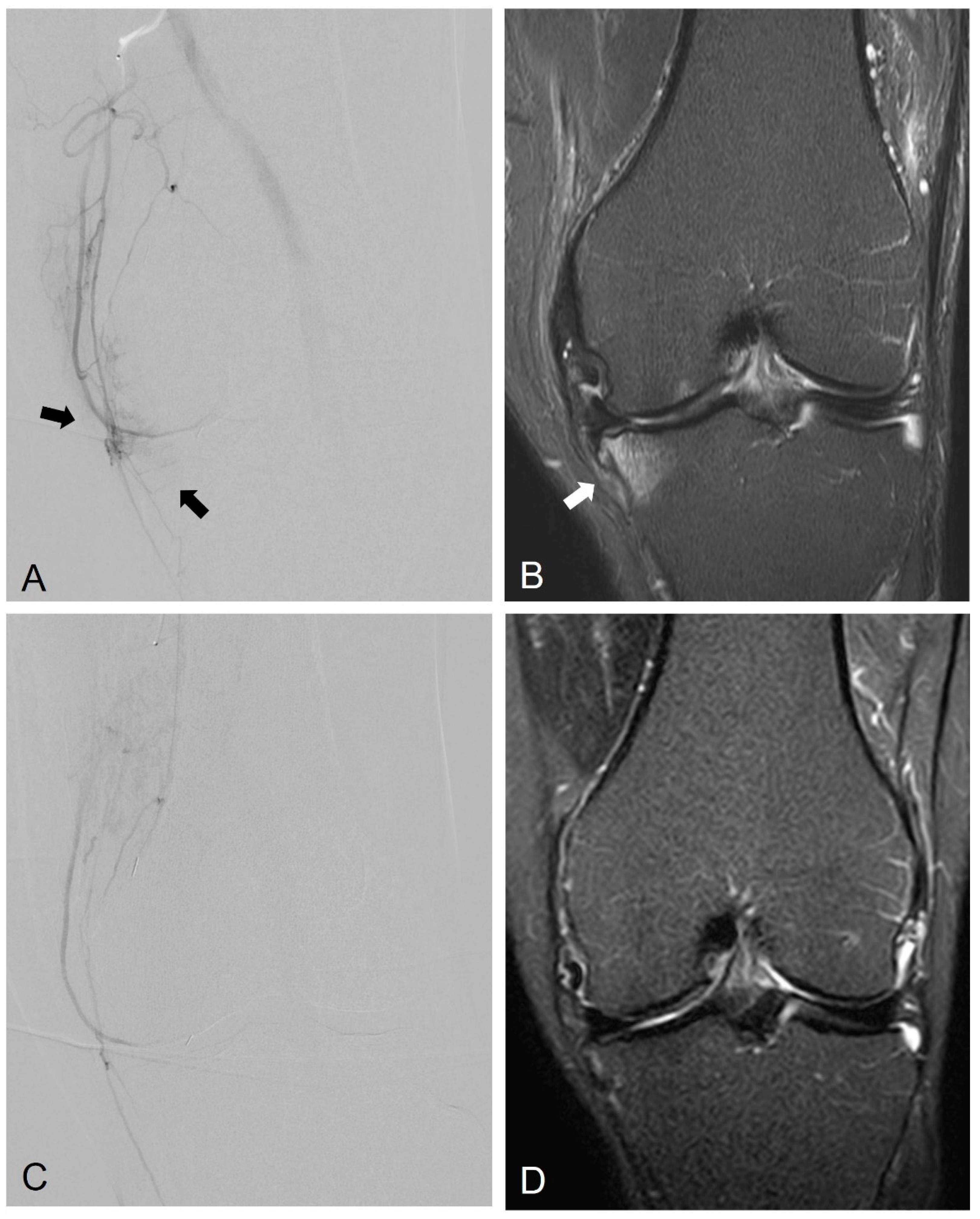
5.4. Patellar Tendinitis
5.5. Plantar Fasciitis
5.6. Insertional Achilles Tendinopathy
6. Others
Trapezius Myalgia
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Crofford, L.J. Chronic Pain: Where the Body Meets the Brain. Trans. Am. Clin. Climatol. Assoc. 2015, 126, 167–183. [Google Scholar] [PubMed]
- El-Tallawy, S.N.; Nalamasu, R.; Salem, G.I.; LeQuang, J.A.K.; Pergolizzi, J.V.; Christo, P.J. Management of Musculoskeletal Pain: An Update with Emphasis on Chronic Musculoskeletal Pain. Pain Ther. 2021, 10, 181–209. [Google Scholar] [CrossRef] [PubMed]
- Dieppe, P. Chronic musculoskeletal pain. BMJ 2013, 346, f3146. [Google Scholar] [CrossRef] [PubMed]
- Katz, J.N.; Arant, K.R.; Loeser, R.F. Diagnosis and Treatment of Hip and Knee Osteoarthritis: A Review. JAMA 2021, 325, 568–578. [Google Scholar] [CrossRef]
- Yu, Q.; Funaki, B.; Navuluri, R.; Zangan, S.; Zhang, A.; Cao, D.; Leef, J.; Ahmed, O. Empiric Transcatheter Embolization for Acute Arterial Upper Gastrointestinal Bleeding: A Meta-Analysis. AJR Am. J. Roentgenol. 2021, 216, 880–893. [Google Scholar] [CrossRef]
- Kishore, S.; Friedman, T.; Madoff, D.C. Update on Embolization Therapies for Hepatocellular Carcinoma. Curr. Oncol. Rep. 2017, 19, 40. [Google Scholar] [CrossRef]
- Malling, B.; Lonn, L.; Jensen, R.J.; Lindh, M.; Frevert, S.; Brasso, K.; Roder, M.A. Prostate Artery Embolization for Lower Urinary Tract Symptoms in Men Unfit for Surgery. Diagnostics 2019, 9, 46. [Google Scholar] [CrossRef] [Green Version]
- Manyonda, I.; Belli, A.M.; Lumsden, M.A.; Moss, J.; McKinnon, W.; Middleton, L.J.; Cheed, V.; Wu, O.; Sirkeci, F.; Daniels, J.P.; et al. Uterine-Artery Embolization or Myomectomy for Uterine Fibroids. N. Engl. J. Med. 2020, 383, 440–451. [Google Scholar] [CrossRef]
- Vaidya, R.; Waldron, J.; Scott, A.; Nasr, K. Angiography and Embolization in the Management of Bleeding Pelvic Fractures. J. Am. Acad. Orthop. Surg. 2018, 26, e68–e76. [Google Scholar] [CrossRef]
- Sajan, A.; Bagla, S.; Isaacson, A. A Review of Musculoskeletal Embolization to Treat Pain Outside of the Knee. Semin. Interv. Radiol. 2021, 38, 515–517. [Google Scholar] [CrossRef]
- Digge, V.K.; Kumar, V.; Kar, S.; Sai Krishna, M.L.V.; Chaudhury, B.; Jain, V.K.; Desai, J. Is there evidence to recommend transcatheter arterial embolisation in adhesive capsulitis: A review of literature. J. Orthop. 2022, 30, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Kishore, S.; Sheira, D.; Malin, M.L.; Trost, D.W.; Mandl, L.A. Transarterial Embolization for the Treatment of Chronic Musculoskeletal Pain: A Systematic Review of Indications, Safety, and Efficacy. ACR Open Rheumatol. 2022, 4, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.H.; Shin, J.H.; Nam, I.C.; Chu, H.H.; Kim, J.H.; Yoon, H.K. Transcatheter Arterial Embolization for Benign Chronic Inflammatory Joint Pain: A Systematic Review and Meta-Analysis. J. Vasc. Interv. Radiol. 2022, 33, 538–545.e3. [Google Scholar] [CrossRef] [PubMed]
- Casadaban, L.C.; Mandell, J.C.; Epelboym, Y. Genicular Artery Embolization for Osteoarthritis Related Knee Pain: A Systematic Review and Qualitative Analysis of Clinical Outcomes. Cardiovasc. Interv. Radiol. 2021, 44, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Okuno, Y.; Matsumura, N.; Oguro, S. Transcatheter arterial embolization using imipenem/cilastatin sodium for tendinopathy and enthesopathy refractory to nonsurgical management. J. Vasc. Interv. Radiol. 2013, 24, 787–792. [Google Scholar] [CrossRef] [PubMed]
- Mapp, P.I.; Walsh, D.A. Mechanisms and targets of angiogenesis and nerve growth in osteoarthritis. Nat. Rev. Rheumatol. 2012, 8, 390–398. [Google Scholar] [CrossRef]
- Walsh, D.A.; Bonnet, C.S.; Turner, E.L.; Wilson, D.; Situ, M.; McWilliams, D.F. Angiogenesis in the synovium and at the osteochondral junction in osteoarthritis. Osteoarthr. Cartil. 2007, 15, 743–751. [Google Scholar] [CrossRef] [Green Version]
- MacDonald, I.J.; Liu, S.C.; Su, C.M.; Wang, Y.H.; Tsai, C.H.; Tang, C.H. Implications of Angiogenesis Involvement in Arthritis. Int. J. Mol. Sci. 2018, 19, 2012. [Google Scholar] [CrossRef] [Green Version]
- Walsh, D.A.; McWilliams, D.F.; Turley, M.J.; Dixon, M.R.; Franses, R.E.; Mapp, P.I.; Wilson, D. Angiogenesis and nerve growth factor at the osteochondral junction in rheumatoid arthritis and osteoarthritis. Rheumatology 2010, 49, 1852–1861. [Google Scholar] [CrossRef] [Green Version]
- Day, B.; Mackenzie, W.G.; Shim, S.S.; Leung, G. The vascular and nerve supply of the human meniscus. Arthroscopy 1985, 1, 58–62. [Google Scholar] [CrossRef]
- Okuno, Y.; Korchi, A.M.; Shinjo, T.; Kato, S. Transcatheter arterial embolization as a treatment for medial knee pain in patients with mild to moderate osteoarthritis. Cardiovasc. Interv. Radiol. 2015, 38, 336–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heller, D.B.; Beggin, A.E.; Lam, A.H.; Kohi, M.P.; Heller, M.B. Geniculate Artery Embolization: Role in Knee Hemarthrosis and Osteoarthritis. Radiographics 2022, 42, 289–301. [Google Scholar] [CrossRef] [PubMed]
- Landers, S.; Hely, R.; Page, R.; Maister, N.; Hely, A.; Harrison, B.; Gill, S. Genicular Artery Embolization to Improve Pain and Function in Early-Stage Knee Osteoarthritis-24-Month Pilot Study Results. J. Vasc. Interv. Radiol. 2020, 31, 1453–1458. [Google Scholar] [CrossRef] [PubMed]
- Torkian, P.; Golzarian, J.; Chalian, M.; Clayton, A.; Rahimi-Dehgolan, S.; Tabibian, E.; Talaie, R. Osteoarthritis-Related Knee Pain Treated With Genicular Artery Embolization: A Systematic Review and Meta-analysis. Orthop. J. Sports Med. 2021, 9, 23259671211021356. [Google Scholar] [CrossRef]
- Lee, S.H.; Hwang, J.H.; Kim, D.H.; So, Y.H.; Park, J.; Cho, S.B.; Kim, J.E.; Kim, Y.J.; Hur, S.; Jae, H.J. Clinical Outcomes of Transcatheter Arterial Embolisation for Chronic Knee Pain: Mild-to-Moderate Versus Severe Knee Osteoarthritis. Cardiovasc. Interv. Radiol. 2019, 42, 1530–1536. [Google Scholar] [CrossRef]
- Okuno, Y.; Korchi, A.M.; Shinjo, T.; Kato, S.; Kaneko, T. Midterm Clinical Outcomes and MR Imaging Changes after Transcatheter Arterial Embolization as a Treatment for Mild to Moderate Radiographic Knee Osteoarthritis Resistant to Conservative Treatment. J. Vasc. Interv. Radiol. 2017, 28, 995–1002. [Google Scholar] [CrossRef]
- Bagla, S.; Piechowiak, R.; Hartman, T.; Orlando, J.; Del Gaizo, D.; Isaacson, A. Genicular Artery Embolization for the Treatment of Knee Pain Secondary to Osteoarthritis. J. Vasc. Interv. Radiol. 2020, 31, 1096–1102. [Google Scholar] [CrossRef]
- Padia, S.A.; Genshaft, S.; Blumstein, G.; Plotnik, A.; Kim, G.H.J.; Gilbert, S.J.; Lauko, K.; Stavrakis, A.I. Genicular Artery Embolization for the Treatment of Symptomatic Knee Osteoarthritis. JBJS Open Access 2021, 6, e21.00085. [Google Scholar] [CrossRef]
- Bagla, S.; Piechowiak, R.; Sajan, A.; Orlando, J.; Hartman, T.; Isaacson, A. Multicenter Randomized Sham Controlled Study of Genicular Artery Embolization for Knee Pain Secondary to Osteoarthritis. J. Vasc. Interv. Radiol. 2022, 33, 2–10.e2. [Google Scholar] [CrossRef]
- Choi, J.W.; Ro, D.H.; Chae, H.D.; Kim, D.H.; Lee, M.; Hur, S.; Kim, H.C.; Jae, H.J.; Chung, J.W. The Value of Preprocedural MR Imaging in Genicular Artery Embolization for Patients with Osteoarthritic Knee Pain. J. Vasc. Interv. Radiol. 2020, 31, 2043–2050. [Google Scholar] [CrossRef]
- Haara, M.M.; Heliovaara, M.; Kroger, H.; Arokoski, J.P.; Manninen, P.; Karkkainen, A.; Knekt, P.; Impivaara, O.; Aromaa, A. Osteoarthritis in the carpometacarpal joint of the thumb. Prevalence and associations with disability and mortality. J. Bone Jt. Surg. Am. 2004, 86, 1452–1457. [Google Scholar] [CrossRef] [PubMed]
- Fowler, A.; Swindells, M.G.; Burke, F.D. Intra-articular corticosteroid injections to manage trapeziometacarpal osteoarthritis-a systematic review. Hand 2015, 10, 583–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inui, S.; Yoshizawa, S.; Shintaku, T.; Kaneko, T.; Ikegami, H.; Okuno, Y. Intra-Arterial Infusion of Imipenem/Cilastatin Sodium through a Needle Inserted into the Radial Artery as a New Treatment for Refractory Trapeziometacarpal Osteoarthritis. J. Vasc. Interv. Radiol. 2021, 32, 1341–1347. [Google Scholar] [CrossRef] [PubMed]
- Kalichman, L.; Hernandez-Molina, G. Hand osteoarthritis: An epidemiological perspective. Semin. Arthritis Rheum. 2010, 39, 465–476. [Google Scholar] [CrossRef]
- Kroon, F.P.; Rubio, R.; Schoones, J.W.; Kloppenburg, M. Intra-Articular Therapies in the Treatment of Hand Osteoarthritis: A Systematic Literature Review. Drugs Aging 2016, 33, 119–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kung, S.-C.; Chou, M.-Y.; Yang, K.-W.; Hsu, Y. Intra-arterial Infusion of Temporary Embolic Agent as a New Treatment in a Patient with Osteoarthritis of the Fingers. Asia Pac. J. Pain 2022, 32, 10–15. [Google Scholar] [CrossRef]
- Maher, C.; Underwood, M.; Buchbinder, R. Non-specific low back pain. Lancet 2017, 389, 736–747. [Google Scholar] [CrossRef] [Green Version]
- Russo, M.; Deckers, K.; Eldabe, S.; Kiesel, K.; Gilligan, C.; Vieceli, J.; Crosby, P. Muscle Control and Non-specific Chronic Low Back Pain. Neuromodulation 2018, 21, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Fujiwara, K.; Inui, S.; Shibuya, M.; Sugihara, E.; Miyazaki, K.; Sakugawa, T.; Okuno, Y. Transcatheter Arterial Embolization Using Imipenem/Cilastatin Sodium for Chronic Low Back Pain Resistant to Conservative Treatment: A Pilot Study with 2-Year Follow-Up. Cardiovasc. Interv. Radiol. 2021, 44, 1964–1970. [Google Scholar] [CrossRef]
- Suzuki, H.; Kanchiku, T.; Imajo, Y.; Yoshida, Y.; Nishida, N.; Taguchi, T. Diagnosis and Characters of Non-Specific Low Back Pain in Japan: The Yamaguchi Low Back Pain Study. PLoS ONE 2016, 11, e0160454. [Google Scholar] [CrossRef]
- Katoh, M.; Schott, P.; Freyhardt, P.; Feyen, L.; Ziegler, H.R.; Kraft, C. Transarterial Periarticular Embolization (TAPE): Indications and Initial Experience in Germany. Rofo 2020, 192, 1046–1052. [Google Scholar] [CrossRef] [PubMed]
- Mathiessen, A.; Conaghan, P.G. Synovitis in osteoarthritis: Current understanding with therapeutic implications. Arthritis Res. Ther. 2017, 19, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guermazi, A.; Hayashi, D.; Roemer, F.W.; Zhu, Y.; Niu, J.; Crema, M.D.; Javaid, M.K.; Marra, M.D.; Lynch, J.A.; El-Khoury, G.Y.; et al. Synovitis in knee osteoarthritis assessed by contrast-enhanced magnetic resonance imaging (MRI) is associated with radiographic tibiofemoral osteoarthritis and MRI-detected widespread cartilage damage: The MOST study. J. Rheumatol. 2014, 41, 501–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathiessen, A.; Slatkowsky-Christensen, B.; Kvien, T.K.; Hammer, H.B.; Haugen, I.K. Ultrasound-detected inflammation predicts radiographic progression in hand osteoarthritis after 5 years. Ann. Rheum. Dis. 2016, 75, 825–830. [Google Scholar] [CrossRef] [PubMed]
- Kortekaas, M.C.; Kwok, W.Y.; Reijnierse, M.; Watt, I.; Huizinga, T.W.; Kloppenburg, M. Pain in hand osteoarthritis is associated with inflammation: The value of ultrasound. Ann. Rheum. Dis. 2010, 69, 1367–1369. [Google Scholar] [CrossRef]
- Kon, E.; Ronga, M.; Filardo, G.; Farr, J.; Madry, H.; Milano, G.; Andriolo, L.; Shabshin, N. Bone marrow lesions and subchondral bone pathology of the knee. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 1797–1814. [Google Scholar] [CrossRef]
- Aso, K.; Shahtaheri, S.M.; McWilliams, D.F.; Walsh, D.A. Association of subchondral bone marrow lesion localization with weight-bearing pain in people with knee osteoarthritis: Data from the Osteoarthritis Initiative. Arthritis Res. Ther. 2021, 23, 35. [Google Scholar] [CrossRef]
- Driban, J.B.; Price, L.; Lo, G.H.; Pang, J.; Hunter, D.J.; Miller, E.; Ward, R.J.; Eaton, C.B.; Lynch, J.A.; McAlindon, T.E. Evaluation of bone marrow lesion volume as a knee osteoarthritis biomarker--longitudinal relationships with pain and structural changes: Data from the Osteoarthritis Initiative. Arthritis Res. Ther. 2013, 15, R112. [Google Scholar] [CrossRef] [Green Version]
- van Zadelhoff, T.A.; Okuno, Y.; Bos, P.K.; Bierma-Zeinstra, S.M.A.; Krestin, G.P.; Moelker, A.; Oei, E.H.G. Association between Baseline Osteoarthritic Features on MR Imaging and Clinical Outcome after Genicular Artery Embolization for Knee Osteoarthritis. J. Vasc. Interv. Radiol. 2021, 32, 497–503. [Google Scholar] [CrossRef]
- Wang, B.; Tai, T.-W.; Liang, K.-W.; Wang, C.-K.; Liu, Y.-S.; Huang, M.-T.; Chang, C.-W. Short-term effects of genicular artery embolization on bone marrow lesions in patients with refractory knee osteoarthritis. 2022; unpublished. [Google Scholar]
- Alliston, T.; Hernandez, C.J.; Findlay, D.M.; Felson, D.T.; Kennedy, O.D. Bone marrow lesions in osteoarthritis: What lies beneath. J. Orthop. Res. 2018, 36, 1818–1825. [Google Scholar] [CrossRef]
- Munsch, M.A.; Safran, M.R.; Mai, M.C.; Vasileff, W.K. Bone marrow lesions: Etiology and pathogenesis at the hip. J. Hip Preserv. Surg. 2020, 7, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Cai, G.; Aitken, D.; Laslett, L.L.; Pelletier, J.P.; Martel-Pelletier, J.; Hill, C.; March, L.; Wluka, A.E.; Wang, Y.; Antony, B.; et al. Effect of Intravenous Zoledronic Acid on Tibiofemoral Cartilage Volume among Patients With Knee Osteoarthritis with Bone Marrow Lesions: A Randomized Clinical Trial. JAMA 2020, 323, 1456–1466. [Google Scholar] [CrossRef] [PubMed]
- Laslett, L.L.; Dore, D.A.; Quinn, S.J.; Boon, P.; Ryan, E.; Winzenberg, T.M.; Jones, G. Zoledronic acid reduces knee pain and bone marrow lesions over 1 year: A randomised controlled trial. Ann. Rheum. Dis. 2012, 71, 1322–1328. [Google Scholar] [CrossRef] [PubMed]
- Muratovic, D.; Findlay, D.M.; Cicuttini, F.M.; Wluka, A.E.; Lee, Y.R.; Edwards, S.; Kuliwaba, J.S. Bone marrow lesions in knee osteoarthritis: Regional differences in tibial subchondral bone microstructure and their association with cartilage degeneration. Osteoarthr. Cartil. 2019, 27, 1653–1662. [Google Scholar] [CrossRef] [PubMed]
- Klement, M.R.; Sharkey, P.F. The Significance of Osteoarthritis-associated Bone Marrow Lesions in the Knee. J. Am. Acad. Orthop. Surg. 2019, 27, 752–759. [Google Scholar] [CrossRef]
- Fernandez Martinez, A.M.; Baldi, S.; Alonso-Burgos, A.; Lopez, R.; Vallejo-Pascual, M.E.; Cuesta Marcos, M.T.; Romero Alonso, D.; Rodriguez Prieto, J.; Mauriz, J.L. Mid-Term Results of Transcatheter Arterial Embolization for Adhesive Capsulitis Resistant to Conservative Treatment. Cardiovasc. Interv. Radiol. 2021, 44, 443–451. [Google Scholar] [CrossRef]
- Okuno, Y.; Oguro, S.; Iwamoto, W.; Miyamoto, T.; Ikegami, H.; Matsumura, N. Short-term results of transcatheter arterial embolization for abnormal neovessels in patients with adhesive capsulitis: A pilot study. J. Shoulder Elb. Surg. 2014, 23, e199–e206. [Google Scholar] [CrossRef]
- Taguchi, H.; Tanaka, T.; Nishiofuku, H.; Fukuoka, Y.; Minamiguchi, K.; Taiji, R.; Takayama, K.; Takeda, M.; Hatakeyama, K.; Inoue, T.; et al. A Rat Model of Frozen Shoulder Demonstrating the Effect of Transcatheter Arterial Embolization on Angiography, Histopathology, and Physical Activity. J. Vasc. Interv. Radiol. 2021, 32, 376–383. [Google Scholar] [CrossRef]
- Okuno, Y.; Iwamoto, W.; Matsumura, N.; Oguro, S.; Yasumoto, T.; Kaneko, T.; Ikegami, H. Clinical Outcomes of Transcatheter Arterial Embolization for Adhesive Capsulitis Resistant to Conservative Treatment. J. Vasc. Interv. Radiol. 2017, 28, 161–167.e1. [Google Scholar] [CrossRef]
- Bagla, S.; Nagda, S.; Piechowiak, R.; Orlando, J.; Sajan, A.; Isaacson, A. Results from a United States Investigational Device Study of Adhesive Capsulitis Embolization in the Treatment of Shoulder Pain: The Adhesive Capsulitis Embolization Study. J. Vasc. Interv. Radiol. 2022, 33, 177–182. [Google Scholar] [CrossRef]
- Ahn, K.S.; Kang, C.H.; Kim, Y.; Jeong, W.K. Diagnosis of adhesive capsulitis: Comparison of contrast-enhanced MRI with noncontrast-enhanced MRI. Clin. Imaging 2015, 39, 1061–1067. [Google Scholar] [CrossRef] [PubMed]
- Suh, C.H.; Yun, S.J.; Jin, W.; Lee, S.H.; Park, S.Y.; Park, J.S.; Ryu, K.N. Systematic review and meta-analysis of magnetic resonance imaging features for diagnosis of adhesive capsulitis of the shoulder. Eur. Radiol. 2019, 29, 566–577. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Martinez, A.M.; Alonso-Burgos, A.; Lopez, R.; Cuesta Marcos, M.T.; Baldi, S. Clinical Outcomes of Transcatheter Arterial Embolization for Secondary Stiff Shoulder. J. Vasc. Interv. Radiol. 2021, 32, 489–496. [Google Scholar] [CrossRef]
- Correa, M.P.; Puton, R.C.; Saleh, J.N.; Noel, R.S.; da Silva, L.H.P.; de Castro, D.M.; de Mello Bajesrki, J.C. Short-term follow-up of embolization of hip synovitis. CVIR Endovasc. 2020, 3, 35. [Google Scholar] [CrossRef]
- Bass, E. Tendinopathy: Why the difference between tendinitis and tendinosis matters. Int. J. Ther. Massag. Bodyw. 2012, 5, 14–17. [Google Scholar] [CrossRef]
- Scott, A.; Danielson, P. An Emerging Role for Angiogenesis in Tendinopathy. Eur. Musculoskelet. Rev. 2009, 4, 75–76. [Google Scholar]
- Hwang, J.H.; Park, S.W.; Kim, K.H.; Lee, S.J.; Oh, K.S.; Chung, S.W.; Moon, S.G. Early Results of Transcatheter Arterial Embolization for Relief of Chronic Shoulder or Elbow Pain Associated with Tendinopathy Refractory to Conservative Treatment. J. Vasc. Interv. Radiol. 2018, 29, 510–517. [Google Scholar] [CrossRef]
- Gremen, E.; Frandon, J.; Lateur, G.; Finas, M.; Rodiere, M.; Horteur, C.; Benassayag, M.; Thony, F.; Pailhe, R.; Ghelfi, J. Safety and Efficacy of Embolization with Microspheres in Chronic Refractory Inflammatory Shoulder Pain: A Pilot Monocentric Study on 15 Patients. Biomedicines 2022, 10, 744. [Google Scholar] [CrossRef]
- Iwamoto, W.; Okuno, Y.; Matsumura, N.; Kaneko, T.; Ikegami, H. Transcatheter arterial embolization of abnormal vessels as a treatment for lateral epicondylitis refractory to conservative treatment: A pilot study with a 2-year follow-up. J. Shoulder Elb. Surg. 2017, 26, 1335–1341. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, D.H.; Lee, S.H.; Hwang, J.H.; Cho, S.B.; Kim, M.; So, Y.H.; Kim, Y.J.; Choi, W.S.; Yoon, C.J. Short-term Results of Transcatheter Arterial Embolization for Chronic Medial Epicondylitis Refractory to Conservative Treatment: A Single-Center Retrospective Cohort Study. Cardiovasc. Interv. Radiol. 2022, 45, 197–204. [Google Scholar] [CrossRef]
- Figueroa, D.; Figueroa, F.; Calvo, R. Patellar Tendinopathy: Diagnosis and Treatment. J. Am. Acad. Orthop. Surg. 2016, 24, e184–e192. [Google Scholar] [CrossRef] [PubMed]
- Ghelfi, J.; Soulairol, I.; Stephanov, O.; Bacle, M.; de Forges, H.; Sanchez-Ballester, N.; Ferretti, G.; Beregi, J.P.; Frandon, J. Feasibility of Neovessel Embolization in a Large Animal Model of Tendinopathy: Safety and Efficacy of Various Embolization Agents. J. Pers. Med. 2022, 12, 1530. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, B.K.; Kushner, D. Plantar Fasciitis. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Shibuya, M.; Sugihara, E.; Miyazaki, K.; Fujiwara, K.; Sakugawa, T.; Okuno, Y. Intra-arterial Infusion of Temporary Embolic Material in a Patient with Plantar Fasciitis: A Case Report. Cardiovasc. Interv. Radiol. 2021, 44, 1823–1826. [Google Scholar] [CrossRef]
- Gaston, T.E.; Daniel, J.N. Achilles Insertional Tendinopathy- Is There a Gold Standard? Arch. Bone Jt. Surg. 2021, 9, 5–8. [Google Scholar] [CrossRef]
- De Meulemeester, K.; Calders, P.; De Pauw, R.; Grymonpon, I.; Govaerts, A.; Cagnie, B. Morphological and physiological differences in the upper trapezius muscle in patients with work-related trapezius myalgia compared to healthy controls: A systematic review. Musculoskelet. Sci. Pract. 2017, 29, 43–51. [Google Scholar] [CrossRef]
- Shibuya, M.; Sugihara, E.; Miyazaki, K.; Yamamoto, M.; Fujiwara, K.; Okuno, Y. Effects of Transcatheter Arterial Microembolization on Persistent Trapezius Myalgia Refractory to Conservative Treatment. Cardiovasc. Interv. Radiol. 2021, 44, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Hindso, L.; Riis, R.G.C.; Holmich, P.; Petersen, M.M.; Nielsen, M.B.; Lonn, L.; Taudorf, M. Current Status of Trans-Arterial Embolization in Pain Management of Musculoskeletal Inflammatory Conditions—An Evidence-Based Review. Cardiovasc. Interv. Radiol. 2021, 44, 1699–1708. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, B.; Liang, K.-W.; Chen, C.-H.; Wang, C.-K. Transcatheter Arterial Embolization for Alleviating Chronic Musculoskeletal Pain and Improving Physical Function: A Narrative Review. Diagnostics 2023, 13, 134. https://doi.org/10.3390/diagnostics13010134
Wang B, Liang K-W, Chen C-H, Wang C-K. Transcatheter Arterial Embolization for Alleviating Chronic Musculoskeletal Pain and Improving Physical Function: A Narrative Review. Diagnostics. 2023; 13(1):134. https://doi.org/10.3390/diagnostics13010134
Chicago/Turabian StyleWang, Bow, Keng-Wei Liang, Chia-Hui Chen, and Chien-Kuo Wang. 2023. "Transcatheter Arterial Embolization for Alleviating Chronic Musculoskeletal Pain and Improving Physical Function: A Narrative Review" Diagnostics 13, no. 1: 134. https://doi.org/10.3390/diagnostics13010134