
Prognostic Value of Bladder Involvement in the Outcome of Upper Tract Urothelial Carcinoma
 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Tumor Specimens
2.2. Outcomes and Statistical Analysis
3. Results
3.1. Baseline Clinicopathologic Characteristics
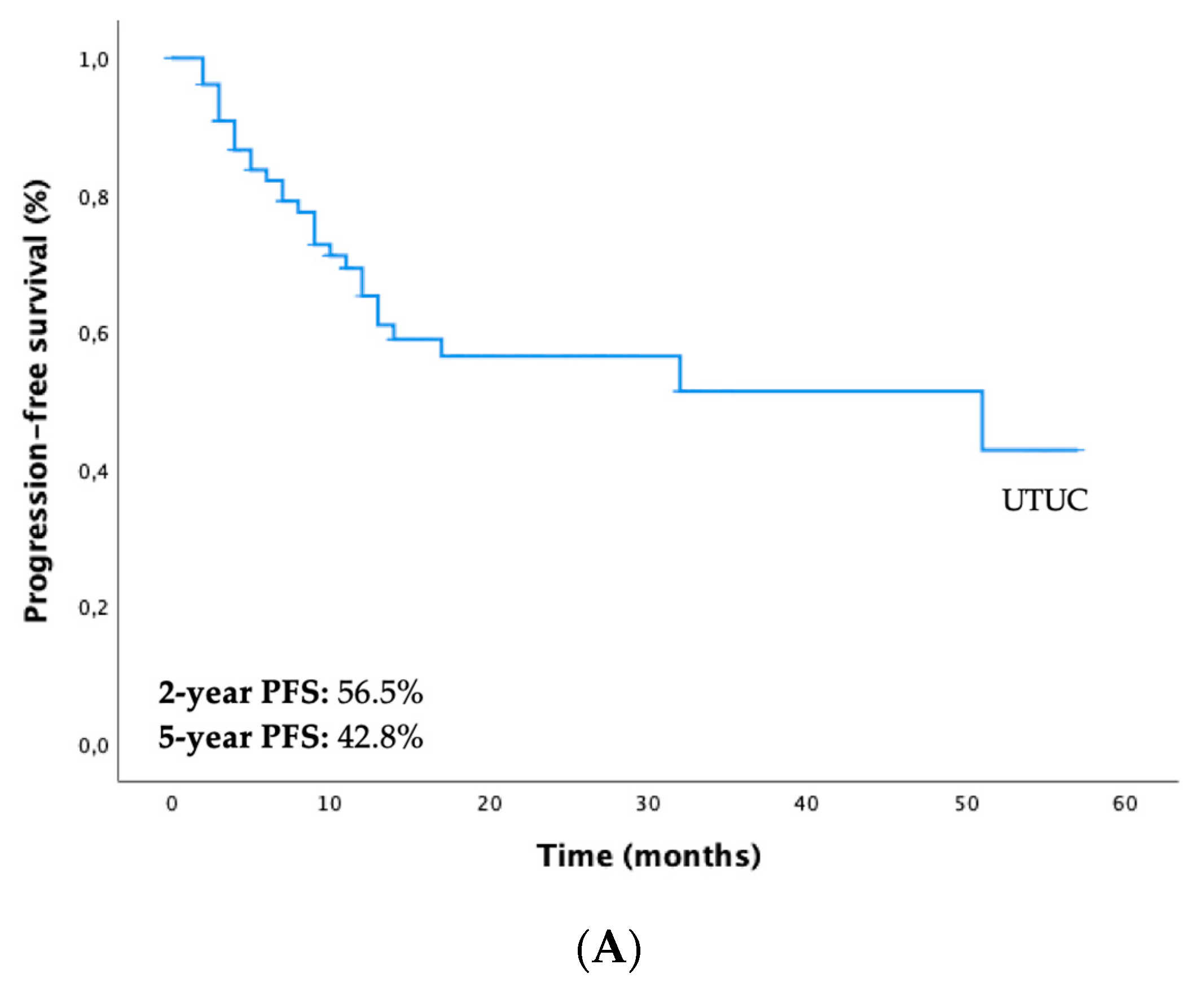
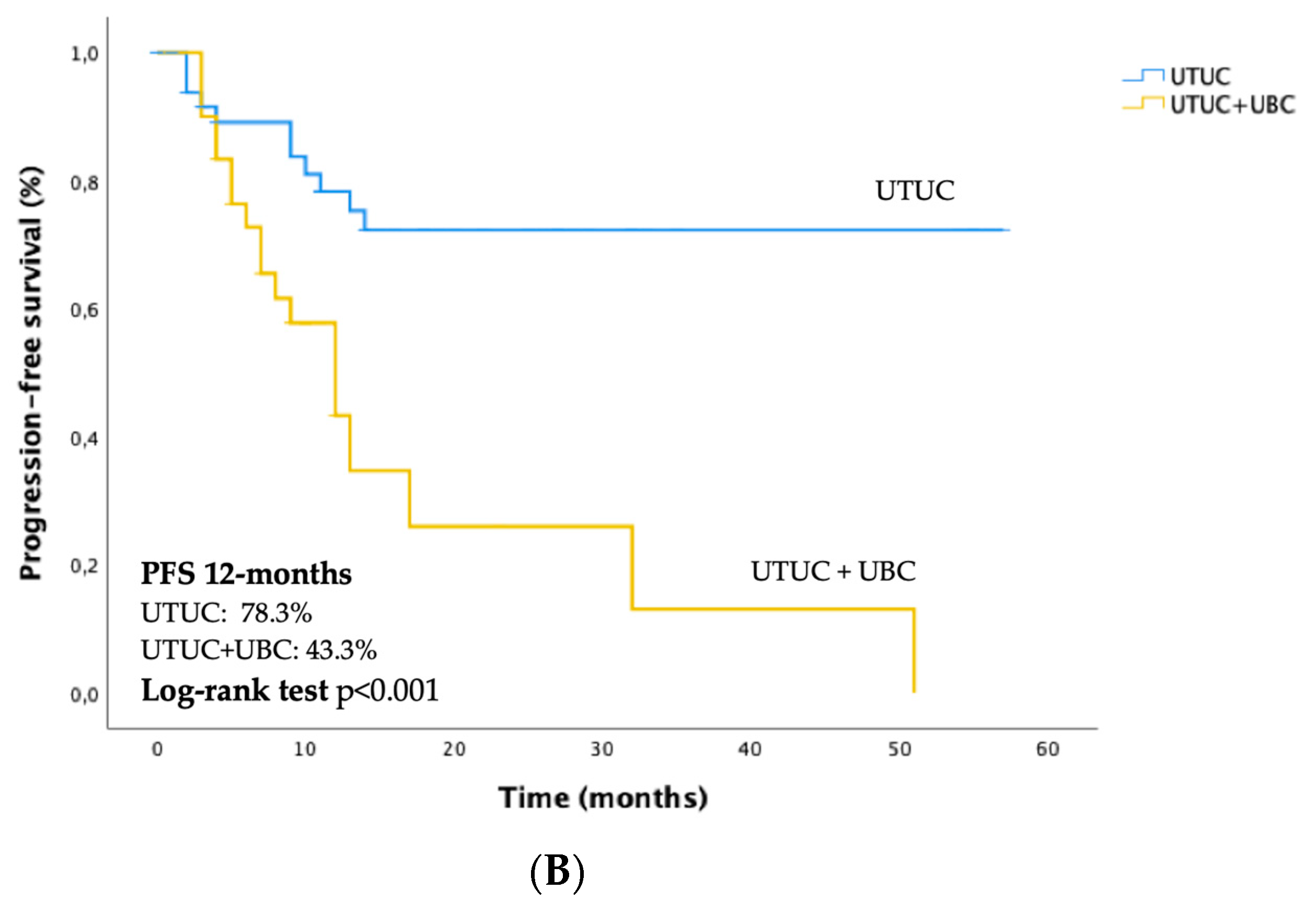
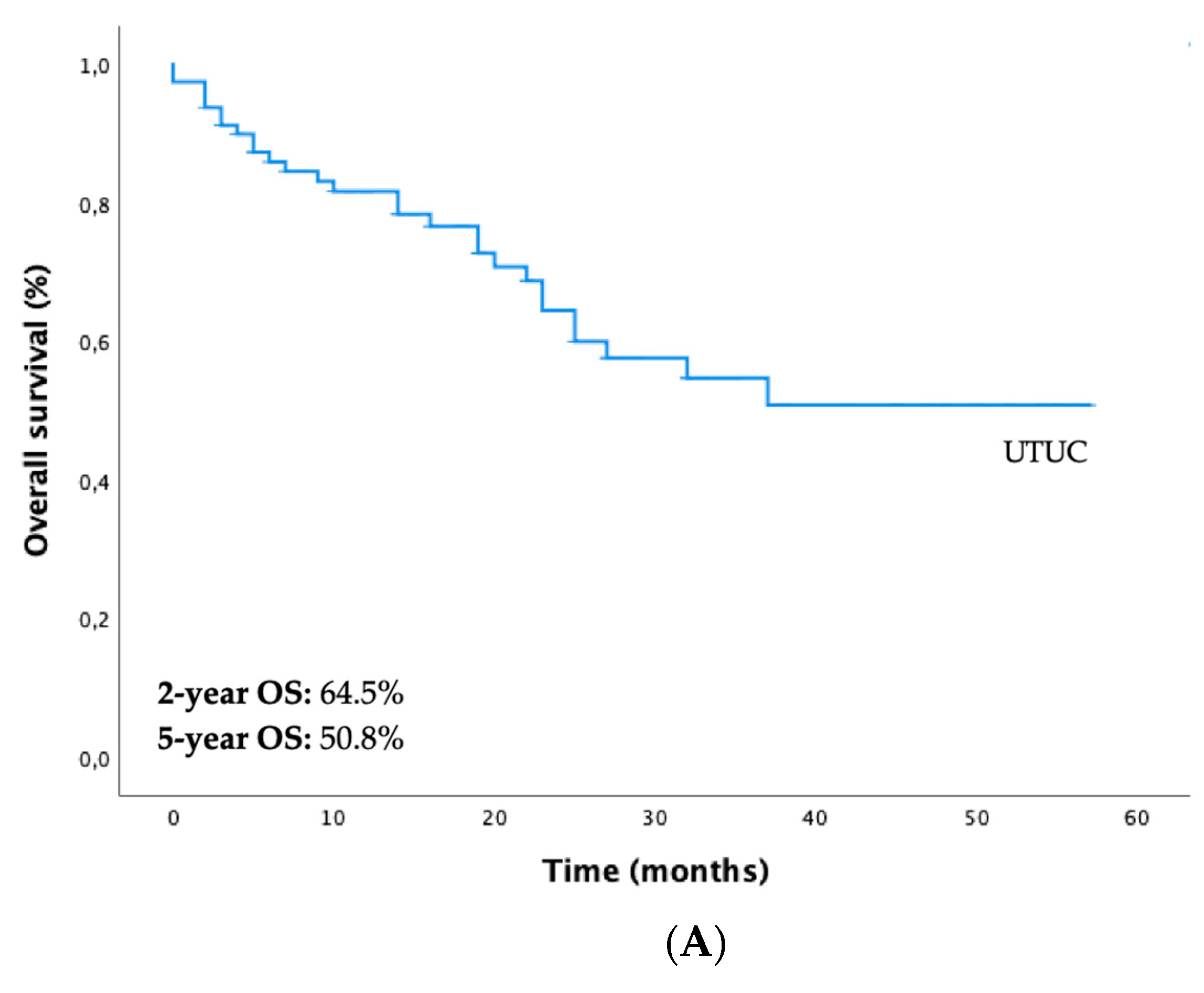
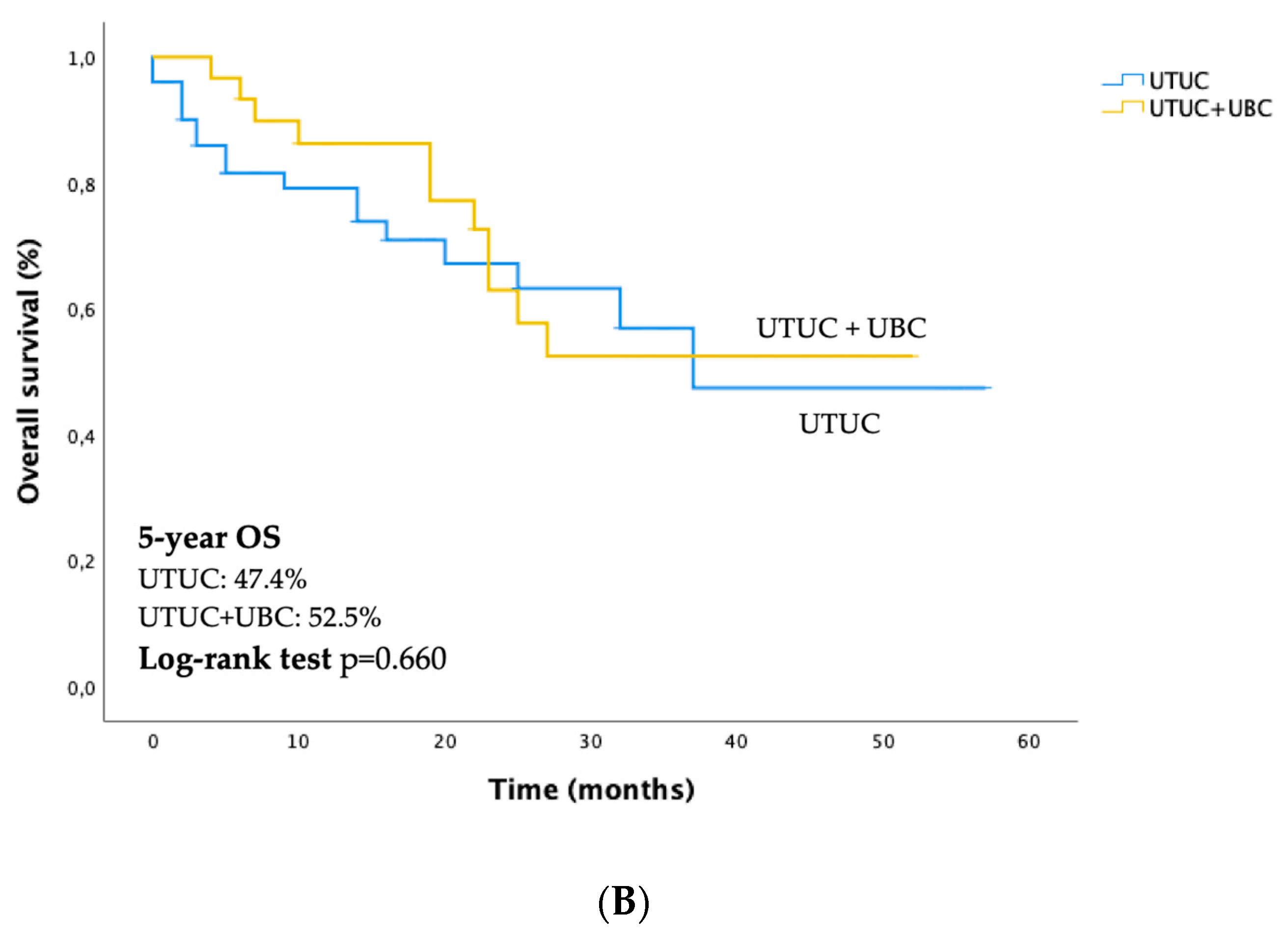
3.2. Survival Outcomes of UTUC and Differences between Both Subgroups (only UTUC vs. UTUC + UBC)
3.3. Prognostic Factors for PFS and OS and the Impact of Synchronous and Metachronous UBC Diagnosis in Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7. [Google Scholar] [CrossRef] [PubMed]
- van Doeveren, T.; van de Werken, H.J.G.; van Riet, J.; Aben, K.K.H.; van Leeuwen, P.J.; Zwarthoff, E.C.; Boormans, J.L. Synchronous and metachronous urothelial carcinoma of the upper urinary tract and the bladder: Are they clonally related? A systematic review. Urol. Oncol. 2020, 8, 590–598. [Google Scholar] [CrossRef] [PubMed]
- Soria, F.; Shariat, S.F.; Lerner, S.P.; Fritsche, H.M.; Rink, M.; Kassouf, W.; Spiess, P.E.; Lotan, Y.; Ye, D.; Fernández, M.I.; et al. Epidemiology, diagnosis, preoperative evaluation, and prognostic assessment of upper tract urothelial carcinoma (UTUC). World J. Urol. 2017, 35, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Ploussard, G.; Xylinas, E.; Lotan, Y.; Novara, G.; Margulis, V.; Rouprêt, M.; Matsumoto, K.; Karakiewicz, P.I.; Montorsi, F.; Remzi, M.; et al. Conditional survival after radical nephroureterectomy for upper tract carcinoma. Eur. Urol. 2015, 67, 803–812. [Google Scholar] [CrossRef]
- Rouprêt, M.; Babjuk, M.; Burger, M.; Compérat, E.; Gontero, P.; Liedberg, F.; Masson-Lecomte, A.; Mostadif, A.H.; Palou, J.; van Rhijn, B.W.G.; et al. European Association of Urology Guidelines on Upper Urinary Tract Urothelial Carcinoma: 2022 Update. Available online: https://uroweb.org/guidelines/upper-urinary-tract-urothelial-cell-carcinoma (accessed on 22 December 2022).
- Habuchi, T.; Takahashi, R.; Yamada, H.; Kakehi, Y.; Sugiyama, T.; Yoshida, O. Metachronous multifocal development of urothelial cancers by intraluminal seeding. Lancet 1993, 342, 1087–1088. [Google Scholar] [CrossRef]
- Harris, A.L.; Neal, D.E. Bladder cancer--field versus clonal origin. N. Engl. J. Med. 1992, 326, 759–761. [Google Scholar] [CrossRef]
- Hafner, C.; Knuechel, R.; Zanardo, L.; Dietmaier, W.; Blaszyk, H.; Cheville, J.; Hofstaedter, F.; Hartmann, A. Evidence for oligoclonality and tumor spread by intraluminal seeding in multifocal urothelial carcinomas of the upper and lower urinary tract. Oncogene 2001, 20, 4910–4915. [Google Scholar] [CrossRef] [Green Version]
- Hafner, C.; Knuechel, R.; Stoehr, R.; Hartmann, A. Clonality of multifocal urothelial carcinomas: 10 years of molecular genetic studies. Int. J. Cancer. 2002, 101, 1–6. [Google Scholar] [CrossRef]
- Miyake, H.; Hara, I.; Kamidono, S.; Eto, H. Multifocal transitional cell carcinoma of the bladder and upper urinary tract: Molecular screening of clonal origin by characterizing CD44 alternative splicing patterns. J. Urol. 2004, 172, 1127–1129. [Google Scholar] [CrossRef]
- Wang, Y.; Lang, M.R.; Pin, C.L.; Izawa, J.I. Comparison of the clonality of urothelial carcinoma developing in the upper urinary tract and those developing in the bladder. Springerplus 2013, 2, 412. [Google Scholar] [CrossRef]
- Leow, J.J.; Chong, Y.L.; Chanh, S.L.; Valderrame, B.P.; Powles, T.; Bellmunt, J. Neoadjuvant and Adjuvant Chemotherapy for Upper Tract Urothelial Carcinoma: A 2020 Systematic Review and Meta-analysis, and Future Perspectives on Systemic Therapy. Eur. Urol. 2021, 79, 635–654. [Google Scholar] [CrossRef]
- Duquesne, I.; Ouzaid, I.; Loriot, Y.; Moschini, M.; Xylinas, E. Lymphadenectomy for Upper Tract Urothelial Carcinoma: A Systematic Review. J. Clin. Med. 2019, 8, 1190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xylinas, E.; Rink, M.; Margulis, V.; Karakiewicz, P.; Novara, G.; Shariat, S.F. Upper Tract Urothelial Carcinoma Collaboration. Multifocal carcinoma in situ of the upper tract is associated with high risk of bladder cancer recurrence. Eur. Urol. 2012, 61, 1069–1070. [Google Scholar] [CrossRef] [PubMed]
- Azemar, M.D.; Comperat, E.; Richard, F.; Cussenot, O.; Rouprêt, M. Bladder recurrence after surgery for upper urinary tract urothelial cell carcinoma: Frequency, risk factors, and surveillance. Urol. Oncol. 2011, 29, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Shigeta, K.; Kikuchi, E.; Hagiwara, M.; Ando, T.; Mizuno, R.; Abe, T.; Mikami, S.; Miyajima, A.; Nakagawa, K.; Oya, M. The Conditional Survival with Time of Intravesical Recurrence of Upper Tract Urothelial Carcinoma. J. Urol. 2017, 198, 1278–1285. [Google Scholar] [CrossRef]
- Millán-Rodríguez, F.; Chéchile-Toniolo, G.; Salvador-Bayarri, J.; Huguet-Pérez, J.; Vicente-Rodríguez, J. Upper urinary tract tumors after primary superficial bladder tumors: Prognostic factors and risk groups. J. Urol. 2000, 164, 1183–1187. [Google Scholar] [CrossRef] [PubMed]
- Cosentino, M.; Palou, J.; Gaya, J.M.; Breda, A.; Rodriguez-Faba, O.; Villavicencio-Mavrich, H. Upper urinary tract urothelial cell carcinoma: Location as a predictive factor for concomitant bladder carcinoma. World J. Urol. 2013, 31, 141–145. [Google Scholar] [CrossRef]
- Lughezzani, G.; Burger, M.; Margulis, V.; Matin, S.F.; Novara, G.; Roupret, M.; Shariat, S.F.; Wood, C.G.; Zigeuner, R. Prognostic factors in upper urinary tract urothelial carcinomas: A comprehensive review of the current literature. Eur. Urol. 2012, 62, 100–114. [Google Scholar] [CrossRef]
- Mbeutcha, A.; Rouprêt, M.; Kamat, A.M.; Karakiewicz, P.I.; Lawrentschuk, N.; Novara, G.; Raman, J.D.; Seitz, C.; Xylinas, E.; Shariat, S.F. Prognostic factors and predictive tools for upper tract urothelial carcinoma: A systematic review. World J. Urol. 2017, 35, 337–353. [Google Scholar] [CrossRef]
- Petrelli, F.; Yasser Hussein, M.I.; Vavassori, I.; Barni, S. Prognostic Factors of Overall Survival in Upper Urinary Tract Carcinoma: A Systematic Review and Meta-analysis. Urology 2017, 100, 9–15. [Google Scholar] [CrossRef]
- Raman, J.D.; Messer, J.; Sielatycki, J.A.; Hollenbeak, C.S. Incidence and survival of patients with carcinoma of the ureter and renal pelvis in the USA, 1973-2005. BJU Int. 2011, 107, 1059–1064. [Google Scholar] [CrossRef]
- Mullerad, M.; Russo, P.; Golijanin, D.; Chen, H.N.; Tsai, H.H.; Donat, S.M.; Bochner, B.H.; Herr, H.W.; Sheinfeld, J.; Sogani, P.C.; et al. Bladder cancer as a prognostic factor for upper tract transitional cell carcinoma. J. Urol. 2004, 172, 2177–2181. [Google Scholar] [CrossRef] [PubMed]
- Novara, G.; De Marco, V.; Gottardo, F.; Dalpiaz, O.; Bouygues, V.; Galfano, A.; Martignoni, G.; Patard, J.J.; Artibani, W.; Ficarra, V. Independent predictors of cancer-specific survival in transitional cell carcinoma of the upper urinary tract: Multi-institutional dataset from 3 European centers. Cancer 2007, 110, 1715–1722. [Google Scholar] [CrossRef] [PubMed]
- Li, W.M.; Li, C.C.; Ke, H.L.; Wu, W.J.; Huang, C.N.; Huang, C.H. The prognostic predictors of primary ureteral transitional cell carcinoma after radical nephroureterectomy. J. Urol. 2009, 182, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Tran, W.; Serio, A.M.; Raj, G.V.; Dalbagni, G.; Vickers, A.J.; Bochner, B.H.; Herr, H.; Donat, S.M. Longitudinal risk of upper tract recurrence following radical cystectomy for urothelial cancer and the potential implications for long-term surveillance. J. Urol. 2008, 179, 96–100. [Google Scholar] [CrossRef]
- Wu, J.; Xu, P.H.; Luo, W.J.; Dai, B.; Shen, Y.J.; Ye, D.W.; Wang, Y.C.; Zhu, Y.P. Intravesical Recurrence After Radical Nephroureterectomy of Upper Urinary Tract Urothelial Carcinoma: A Large Population-Based Investigation of Clinicopathologic Characteristics and Survival Outcomes. Front. Surg. 2021, 8, 590448:1–590448:11. [Google Scholar] [CrossRef]
- Kang, H.W.; Jung, H.D.; Ha, Y.S.; Kim, T.H.; Kwon, T.G.; Byun, S.S.; Yun, S.J.; Kim, W.J.; Choi, Y.D. Preoperative Underweight Patients with Upper Tract Urothelial Carcinoma Survive Less after Radical Nephroureterectomy. J. Korean Med. Sci. 2015, 30, 1483–1489. [Google Scholar] [CrossRef] [Green Version]
- Novara, G.; Matsumoto, K.; Kassouf, W.; Walton, T.J.; Fritsche, H.M.; Bastian, P.J.; Martínez-Salamanca, J.I.; Seitz, C.; Lemberger, R.J.; Burger, M.; et al. Prognostic role of lymphovascular invasion in patients with urothelial carcinoma of the upper urinary tract: An international validation study. Eur. Urol. 2010, 57, 1064–1071. [Google Scholar] [CrossRef]
- Kikuchi, E.; Margulis, V.; Karakiewicz, P.I.; Roscigno, M.; Mikami, S.; Lotan, Y.; Remzi, M.; Bolenz, C.; Langner, C.; Weizer, A.; et al. Lymphovascular invasion predicts clinical outcomes in patients with node-negative upper tract urothelial carcinoma. J. Clin. Oncol. 2009, 27, 612–618. [Google Scholar] [CrossRef] [Green Version]
- Emamekhoo, H.; Dhillon, P.; Gopalakrishnan, D.; Elson, P.; Stephenson, A.; Magi-Galluzzi, C.; McKenney, J.; Harper, H.; Haber, G.P.; Kaouk, J.; et al. Prognostic Factors and Risk Stratification in Invasive Upper Tract Urothelial Carcinoma. Clin. Genitourin. Cancer 2018, 16, 751–760. [Google Scholar] [CrossRef]
- Seisen, T.; Shariat, S.F.; Cussenot, O.; Peyronnet, B.; Renard-Penna, R.; Colin, P.; Rouprêt, M. Contemporary role of lymph node dissection at the time of radical nephroureterectomy for upper tract urothelial carcinoma. World J. Urol. 2017, 35, 535–548. [Google Scholar] [CrossRef] [PubMed]
- Mason, R.J.; Kassouf, W.; Bell, D.G.; Lacombe, L.; Kapoor, A.; Jacobsen, N.; Fairey, A.; Izawa, J.; Black, P.; Tanguay, S.; et al. The contemporary role of lymph node dissection during nephroureterectomy in the management of upper urinary tract urothelial carcinoma: The Canadian experience. Urology 2012, 79, 840–845. [Google Scholar] [CrossRef] [PubMed]
- Ouzzane, A.; Colin, P.; Ghoneim, T.P.; Zerbib, M.; De La Taille, A.; Audenet, F.; Saint, F.; Hoarau, N.; Adam, E.; Azemar, M.D.; et al. The impact of lymph node status and features on oncological outcomes in urothelial carcinoma of the upper urinary tract (UTUC) treated by nephroureterectomy. World J. Urol. 2013, 31, 189–197. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinicopathologic Variables | Overall, n (%) |
|---|---|
| Number of patients (n/%) | 115 (100) |
| Age (median, years) | 75 (41–94) |
| Gender Male Female | 80 (69.6) 35 (30.4) |
| Risk factors Smoking Occupational exposure | 49 (55) 13 (25) |
| ECOG PS 0–1 ≥2 | 83 (72.2) 32 (27.8) |
| Clinical presentation Gross hematuria Hydronephrosis | 67 (59.8) 56 (50) |
| Laterality Left Right | 59 (51.3) 56 (48.7) |
| Primary tumor location Renal pelvis Ureter Both | 66 (57.4) 33 (28.7) 16 (13.9) |
| Surgical procedure Nephroureterectomy Kidney-sparing approach | 106 (92.2) 9 (7.8) |
| Histological subtype Pure UC Non-pure UC | 103 (89.6) 12 (10.4) |
| Lymphadenectomy Yes No | 32 (28.1) 82 (71.9) |
| Tumor size, cm ≤2 >2 | 16 (14) 98 (86) |
| Multifocality Yes No | 11 (9.6) 104 (90.4) |
| Tumor grade Low-grade High-grade | 7 (6.2) 106 (93.8) |
| Lymphovascular invasion Yes No | 38 (33.9) 74 (66.1) |
| Concomitant carcinoma in situ Yes No | 20 (17.4) 95 (82.6) |
| Tumor necrosis Yes No | 16 (14.2) 97 (85.8) |
| AJCC staging a 0is 0a I II III IV | 2 (2) 7 (7.1) 25 (25.5) 20 (20.4) 40 (40.8) 4 (4.1) |
| Lymph node involvement Yes No | 7 (22.6) 24 (77.4) |
| Metastasis at diagnosis Yes No | 14 (12.2) 101 (87.8) |
| Synchronous or metachronous UBC Yes No | 43 (37.4) 72 (62.6) |
| Variables | Univariate Analysis | Multivariate Cox Regression Model | ||||
|---|---|---|---|---|---|---|
| HR | CI 95% | p-Value | HRª | CI 95% | p-Value | |
| Gender (male vs. female) | 1.578 | 0.694–3.587 | 0.276 | - | - | - |
| ECOG PS (0–1 vs. ≥2) | 2.067 | 0.973–4.560 | 0.072 | - | - | - |
| Smoking status (never vs former/current) | 1.049 | 0.465–2.363 | 0.908 | - | - | - |
| Occupational exposure (yes/no) | 1.289 | 0.434–3.833 | 0.648 | - | - | - |
| Laterality (left vs. right) | 2.004 | 0.928–4.327 | 0.077 | - | - | - |
| Location of tumor | 0.945 | - | - | - | ||
| Renal pelvis | 0.983 | 0.286–3.382 | 0.979 | - | - | - |
| Ureter | 0.869 | 0.292–2.584 | 0.801 | - | - | - |
| Both | 1 (ref.) | - | - | - | ||
| Hydronephrosis (yes/no) | 1.077 | 0.520–2.233 | 0.842 | 1.042 | 0.485–2.239 | 0.917 |
| Histological subtype (pure UC vs. non-pure UC) | 4.292 | 1.806–10.196 | <0.001 b | 1.553 | 0.585–4.125 | 0.377 |
| Multifocality (single vs. multiple) | 1.909 | 0.725–5.025 | 0.190 | - | - | - |
| Tumor size (≤2 vs. > 2) | 3.005 | 0.711–12.692 | 0.134 | - | - | - |
| Tumor grade (low-grade vs high-grade) | 3.210 | 0.436–23.650 | 0.252 | - | - | - |
| Lymphovascular invasion (absent vs. present) | 3.598 | 1.722–7.520 | 0.001 b | 2.687 | 1.172–6.163 | 0.020 b |
| Carcinoma in situ (absent vs. present) | 1.430 | 0.609–3.354 | 0.411 | - | - | - |
| Tumor necrosis (absent vs. present) | 2.185 | 0.886–5.386 | 0.090 | - | - | - |
| AJCC staging system (0is-0a-I vs. II-IV) | 3.670 | 1.391–9.686 | 0.009 b | 2.216 | 0.767–6.403 | 0.142 |
| Lymph node involvement (yes/no) | 2.419 | 0.673–8.692 | 0.176 | - | - | - |
| Subgroups (only UTUC vs. UTUC+UBC) | 3.715 | 1.714–8.051 | 0.001 b | 3.326 | 1.474–7.503 | 0.004 b |
| Variables | Univariate Analysis | Multivariate Cox Regression Model | ||||
|---|---|---|---|---|---|---|
| HR | CI 95% | p-Value | HRa | CI 95% | p-Value | |
| Gender (male vs. female) | 2.439 | 0.926–6.426 | 0.071 | - | - | - |
| ECOG PS (0–1 vs. ≥2) | 3.637 | 1.700–7.783 | <0.001 b | 4.063 | 1.413–11.685 | 0.009 b |
| Smoking status (never vs. former/current) | 3.571 | 1.214–10.506 | 0.021 b | 5.060 | 1.584–16.165 | 0.006 b |
| Occupational exposure (yes/no) | 1.227 | 0.427–3.525 | 0.704 | - | - | - |
| Laterality (left vs. right) | 1.156 | 0.546–2.449 | 0.705 | - | - | - |
| Location of tumor | 0.286 | - | - | - | ||
| Renal pelvis | 0.429 | 0.135–1.356 | 0.149 | |||
| Ureter | 0.507 | 0.196–1.314 | 0.162 | |||
| Both | 1 (ref.) | |||||
| Hydronephrosis (yes/no) | 1.323 | 0.625–2.797 | 0.464 | 1.031 | 0.370–2.874 | 0.954 |
| Histological subtype (pure UC vs. non-pure UC) | 5.012 | 2.070–12.135 | <0.001 b | 1.086 | 0.295–4.002 | 0.901 |
| Multifocality (single vs. multiple) | 1.038 | 0.313–3.442 | 0.952 | - | - | - |
| Tumor size (≤2 vs. >2) | 2.573 | 0.610–10.846 | 0.198 | - | - | - |
| Tumor grade (low-grade vs high-grade) | 1.190 | 0.161–8.808 | 0.865 | - | - | - |
| Lymphovascular invasion (absent vs. present) | 4.454 | 2.079–9.544 | <0.001 b | 4.980 | 1.763–14.064 | <0.002 b |
| Carcinoma in situ (absent vs. present) | 1.867 | 0.782–4.459 | 0.160 | - | - | - |
| Tumor necrosis (absent vs. present) | 1.508 | 0.521–4.364 | 0.448 | - | - | - |
| AJCC staging system (0is-0a-I vs. II-IV) | 3.168 | 1.201–8.360 | 0.020 b | 1.308 | 0.440–3.893 | 0.629 |
| Lymph node involvement (yes/no) | 3.093 | 0.887–10.782 | 0.076 | - | - | - |
| Subgroups (only UTUC vs. UTUC+UBC) | 1.185 | 0.553–2.537 | 0.663 | 1.009 | 0.394–2.586 | 0.985 |
| Recurrencec (absent vs. present) | 2.582 | 1.209–5.518 | 0.014 b | - | - | - |
| Local recurrence (yes/no) | 1.150 | 0.346–3.820 | 0.819 | - | - | - |
| Bladder recurrence (yes/no) | 2.433 | 0.576–10.282 | 0.227 | - | - | - |
| Distant metastasis (yes/no) | 3.920 | 1.842–8.342 | <0.001 b | 2.737 | 1.086–6.901 | 0.033 b |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meireles, S.; Dias, N.; Martins, D.; Dias, C.; Gonçalves, M.; Silva, J.; Silva, C.M.; Oliveira, P.D.; Soares, P.; Lopes, J.M. Prognostic Value of Bladder Involvement in the Outcome of Upper Tract Urothelial Carcinoma. Diagnostics 2023, 13, 153. https://doi.org/10.3390/diagnostics13010153
Meireles S, Dias N, Martins D, Dias C, Gonçalves M, Silva J, Silva CM, Oliveira PD, Soares P, Lopes JM. Prognostic Value of Bladder Involvement in the Outcome of Upper Tract Urothelial Carcinoma. Diagnostics. 2023; 13(1):153. https://doi.org/10.3390/diagnostics13010153
Chicago/Turabian StyleMeireles, Sara, Nuno Dias, Diana Martins, Carolina Dias, Marina Gonçalves, João Silva, Carlos Martins Silva, Paulo Dinis Oliveira, Paula Soares, and José Manuel Lopes. 2023. "Prognostic Value of Bladder Involvement in the Outcome of Upper Tract Urothelial Carcinoma" Diagnostics 13, no. 1: 153. https://doi.org/10.3390/diagnostics13010153