Uterine leiomyoma is the most common tumor of the female pelvic organs, mostly occurring during reproductive age. The prevalence ranges from 4% in women 20–30 years of age to 11–18% in women 30–40 years of age and 33% in women 40–60 years of age [
1]. In general, the diagnosis is based on ultrasound examination, which exhibits recurrent refractory shadowing pattern or multiple discrete shadows originating from within the mass [
2]. However, it may be difficult to make the diagnosis in unusual cases of atypical findings. Subserous leiomyoma can simulate the adnexal mass, possibly mistaken for the ovarian tumor/malignancy, and exhibit different degenerative changes such as hyaline degeneration, cystic degeneration, fatty degeneration, red degeneration, and calcified degeneration. Uterine leiomyoma with calcified degeneration is rather uncommon, but severely calcified degeneration all over the mass is extremely rare and has been reported in a very limited number of cases [
3,
4,
5,
6]. Here, we describe a severely calcified leiomyoma forming a scattered popcorn pattern in a postmenopausal woman. It can lead to some diagnostic confusion with ovarian teratoma/malignancy or large bladder calculus in the imaging investigation. Sonographically, different from typical uterine leiomyomas, our case showed heavy homogeneous acoustic shadow obscuring all structures beneath the mass surface, resulting in a suboptimal ultrasound examination. Accordingly, CT scans, which are usually not a primary tool for the diagnosis of uterine leiomyomas, are helpful to characterize the mass and identify their organ of origin. The case presented here was treated with a hysterectomy with bilateral oophorectomy and was post-operatively confirmed for severely calcified leiomyomas. The objective of this report is to describe the unusual appearance of leiomyoma which might be mistaken for adnexal mass and focus on the limitation of ultrasound examination as well as the usefulness of CT scans.
Calcification tends to develop in uterine leiomyomas in the absence of vascular supply, especially in postmenopausal women. Calcification of leiomyomas may present in various patterns such as a mottled or popcorn appearance with no well-defined curvilinear outline, totally calcified as a solid stony mass or a well-defined outer part, or the high-attenuation border with less calcification of the inner part. The presence of calcification in the uterus is a reliable sign of uterine leiomyoma [
7]. Nevertheless, calcified leiomyoma is rather uncommon. The prevalence of calcified uterine leiomyomas is reported to be 3–10% of cases [
3]. However, in a majority of cases, calcifications are confined to only a small part of leiomyomas. Extensive calcification involving all of the mass as seen in our case is extremely rare.
Though uterine leiomyomas can be recognized with confidence by ultrasound in most cases, large leiomyoma with various types of degeneration can be a diagnostic challenge. Moreover, they can be mistaken for ovarian tumors or malignancy, especially in postmenopausal women [
8]. An ultrasound examination of severely calcified mass is less informative. Generally, a diagnosis of a pedunculated subserous leiomyoma can be made by sonographic visualization of a vascular pedicle connecting to the uterus. Nevertheless, such a finding may not always be demonstrated by ultrasound [
2], and it is very difficult or impossible in cases with severe calcifications as seen in our cases because of heavy acoustic shadow. Accordingly, in these cases, a CT scan is helpful to characterize pelvic calcified masses and identify their organ of origin [
9], though CT scans are usually not the primary tool for the diagnosis of leiomyomas.
Typical leiomyomas are associated with the presence of three or more well-defined shadows originating from within a mass, defined as the recurrent refractory shadowing pattern [
2,
10], not originating from echogenic lead points which are presumed to arise from calcifications. Pathologically, these discrete recurrent shadows originate from transitional zones between the margins of smooth muscle whorls and the margins of fibrous connective tissue within the leiomyoma [
10]. The ultrasound beam is refracted and distorted when it passes through the different tissues or curved surfaces. This pattern is typically expressed by uterine leiomyomas and is used as a diagnostic sonographic sign. The heavy shadowing in our case was not a recurrent refractory shadow pattern of leiomyoma but an acoustic shadow, which occurred because no ultrasound beams passed through the multiple layers of calcifications.
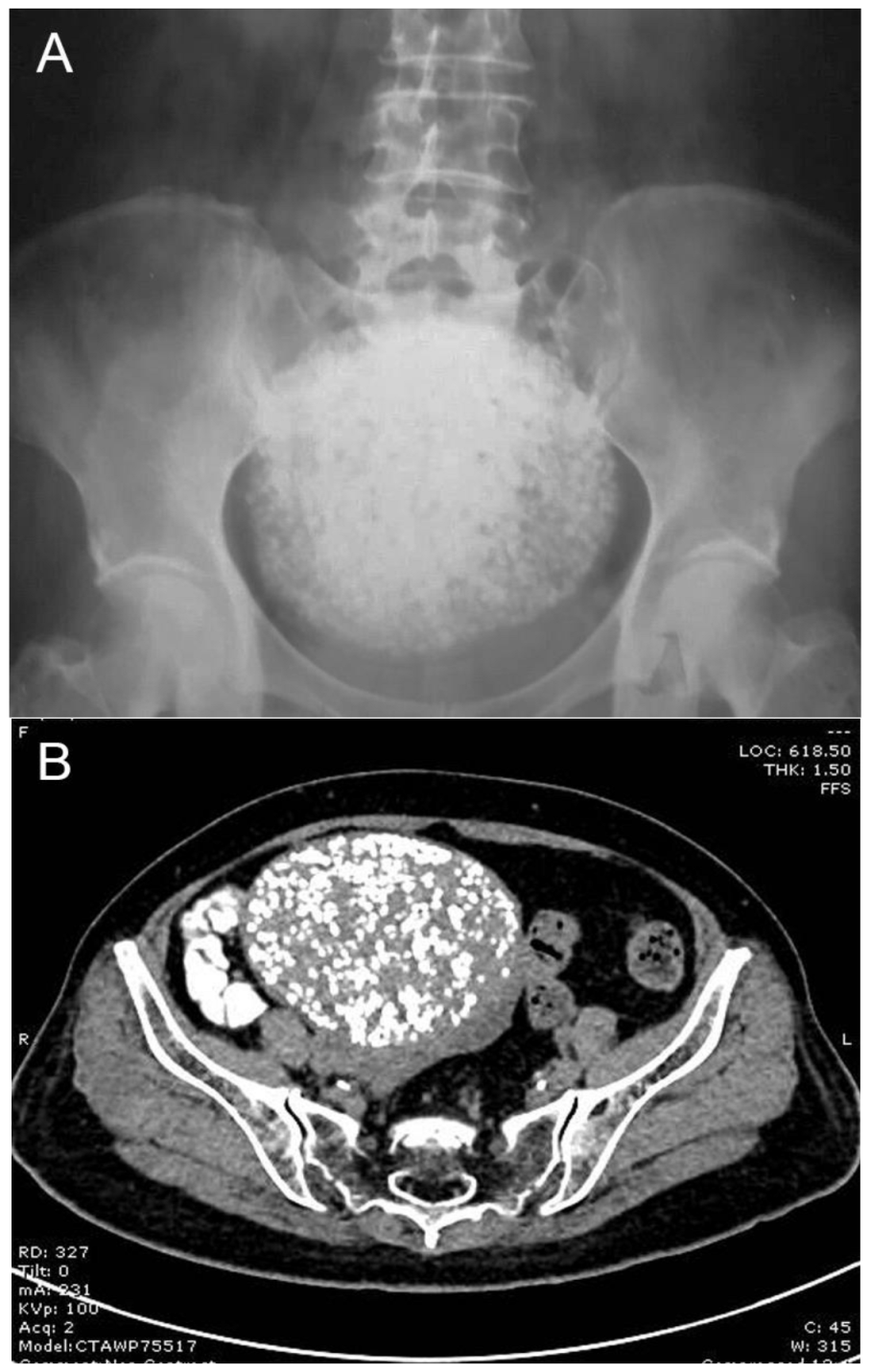
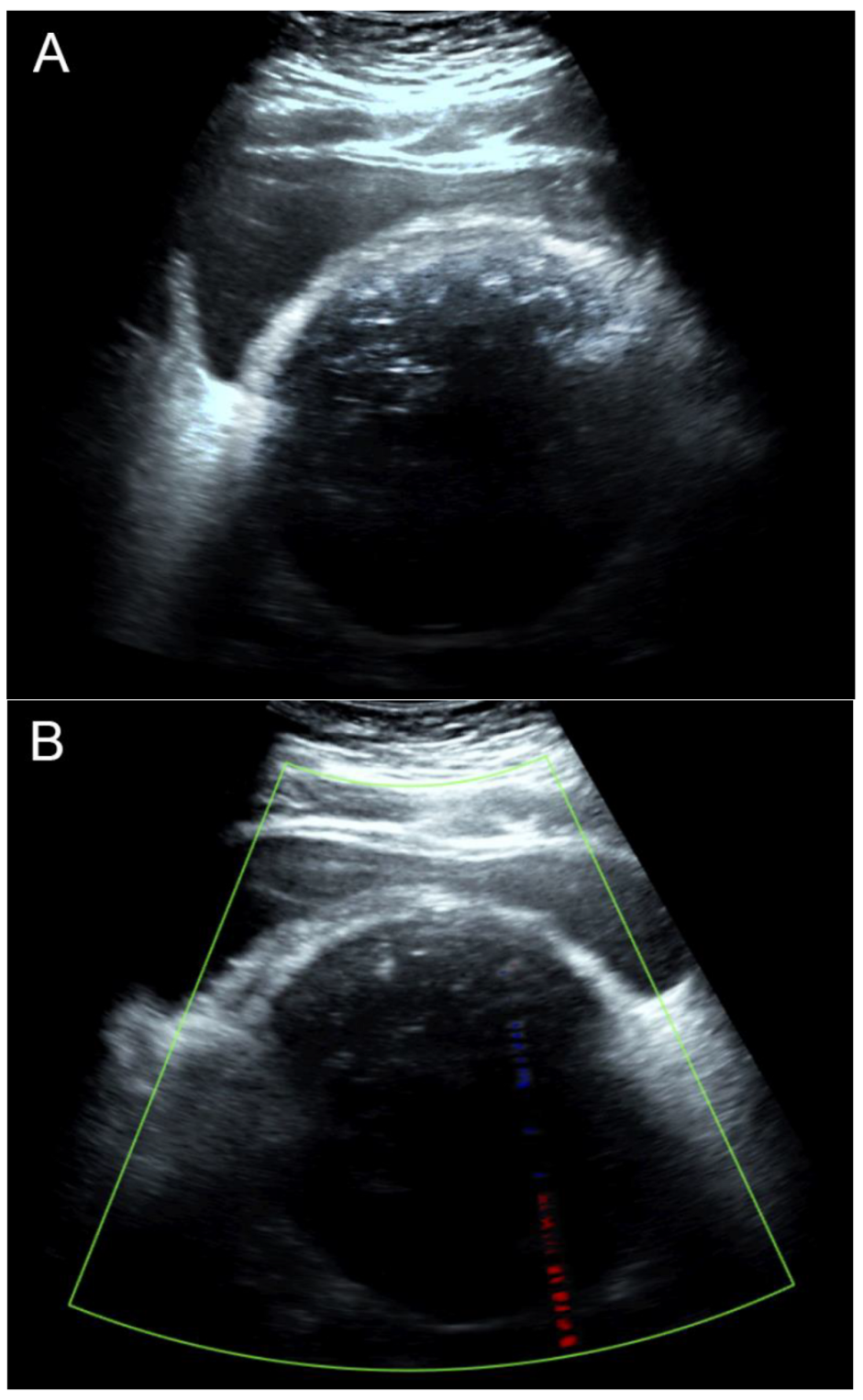
Figure 1 and
Figure 2 illustrate the discrepancy in image quality between the two modalities. The stacked calcific pellets in numerous layers produced stacked shadows on conventional ultrasound to completely obscure the underlying structures. The numerous calcific pellets, proven by pathological examination in
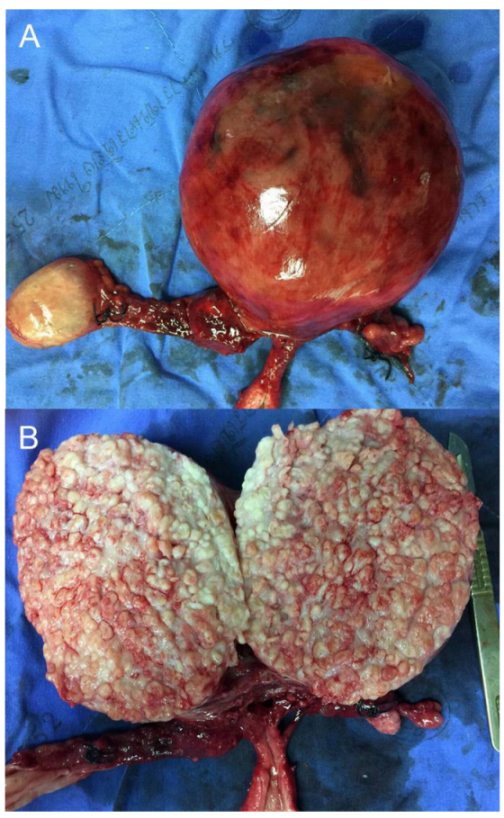
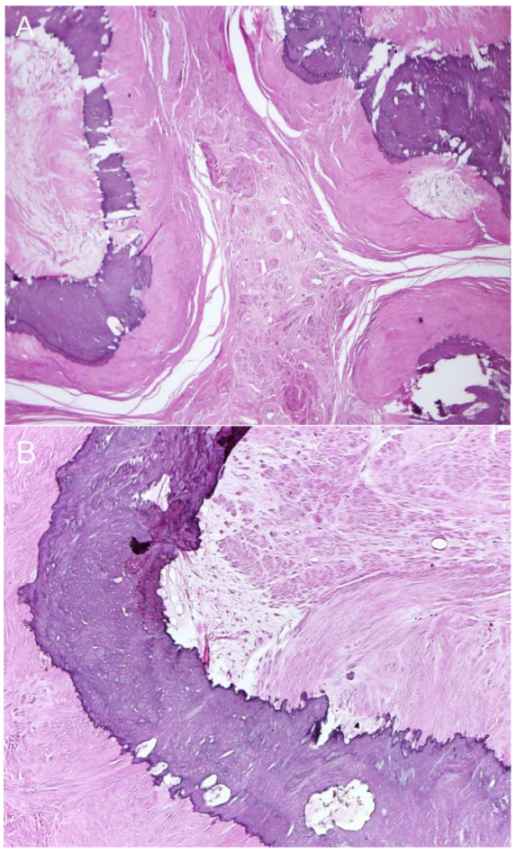
Figure 3 and
Figure 4, corresponded to the numerous popcorn spots on the pre-operative CT scan image (
Figure 1), whereas they could not be correlated with the ultrasound findings (
Figure 2). In conclusion, our findings emphasize that, though leiomyoma can usually be diagnosed with conventional ultrasound without difficulty, in cases of severe calcifications, it is difficult to make a diagnosis by ultrasound because of severe acoustic shadows leading to a non-informative examination. In this circumstance, a CT scan is superior, as it illustrates a clear and typical popcorn appearance of heavy calcifications. Accordingly, in cases of non-informative ultrasound, which is used as a primary tool of pelvic imaging, a CT scan should be performed to make the diagnosis.
Author Contributions
C.T.: Clinical diagnosis, investigation, manuscript writing, final approval; S.K.: Pathological diagnosis, manuscript editing, final approval; S.S.: Clinical management, manuscript editing, final approval; T.T.: Conceptualization, investigation, manuscript revising, final approval. All authors have read and agreed to the published version of the manuscript.
Funding
The Chiang Mai University Research Fund (CMU-2566).
Informed Consent Statement
Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
The data of this report are available from the corresponding authors upon request.
Acknowledgments
We would like to express our gratitude to the MFM team who helped us in collecting data.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lurie, S.; Piper, I.; Woliovitch, I.; Glezerman, M. Age-related prevalence of sonographicaly confirmed uterine myomas. J. Obstet. Gynaecol. 2005, 25, 42–44. [Google Scholar] [CrossRef] [PubMed]
- Caoili, E.M.; Hertzberg, B.S.; Kliewer, M.A.; DeLong, D.; Bowie, J.D. Refractory shadowing from pelvic masses on sonography: A useful diagnostic sign for uterine leiomyomas. AJR Am. J. Roentgenol. 2000, 174, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Casillas, J.; Joseph, R.C.; Guerra, J.J., Jr. CT appearance of uterine leiomyomas. Radiographics 1990, 10, 999–1007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ueda, H.; Togashi, K.; Konishi, I.; Kataoka, M.L.; Koyama, T.; Fujiwara, T.; Kobayashi, H.; Fujii, S.; Konishi, J. Unusual appearances of uterine leiomyomas: MR imaging findings and their histopathologic backgrounds. Radiographics 1999, 19, S131–S145. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.H.; Modi, G.V.; Jeong Oh, M.; Lee, N.W.; Hur, J.Y.; Lee, K.W.; Lee, J.K. An unusual presentation of a severely calcified parasitic leiomyoma in a postmenopausal woman. JSLS 2010, 14, 299–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iliyas, M. Calcified leiomyoma of the uterus following brachytherapy. Postgrad. Med. J. 2019, 95, 219. [Google Scholar] [CrossRef] [PubMed]
- Walsh, J.W.; Rosenfield, A.T.; Jaffe, C.C.; Schwartz, P.E.; Simeone, J.; Dembner, A.G.; Taylor, K.J. Prospective comparison of ultrasound and computed tomography in the evaluation of gynecologic pelvic masses. AJR Am. J. Roentgenol. 1978, 131, 955–960. [Google Scholar] [CrossRef] [PubMed]
- Ciarmela, P.; Ciavattini, A.; Giannubilo, S.R.; Lamanna, P.; Fiorini, R.; Tranquilli, A.L.; Christman, G.M.; Castellucci, M. Management of leiomyomas in perimenopausal women. Maturitas 2014, 78, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Rajanna, D.K.; Pandey, V.; Janardhan, S.; Datti, S.N. Broad ligament fibroid mimicking as ovarian tumor on ultrasonography and computed tomography scan. J. Clin. Imaging Sci. 2013, 3, 8. [Google Scholar] [CrossRef] [PubMed]
- Kliewer, M.A.; Hertzberg, B.S.; George, P.Y.; McDonald, J.W.; Bowie, J.D.; Carroll, B.A. Acoustic shadowing from uterine leiomyomas: Sonographic-pathologic correlation. Radiology 1995, 196, 99–102. [Google Scholar] [CrossRef] [PubMed]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).



{kind=link}
{kind=link}
{kind=link}
{kind=link}



