
Follow-Up Infarct Volume Prediction by CTP-Based Hypoperfusion Index, and the Discrepancy between Small Follow-Up Infarct Volume and Poor Functional Outcome—A Multicenter Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
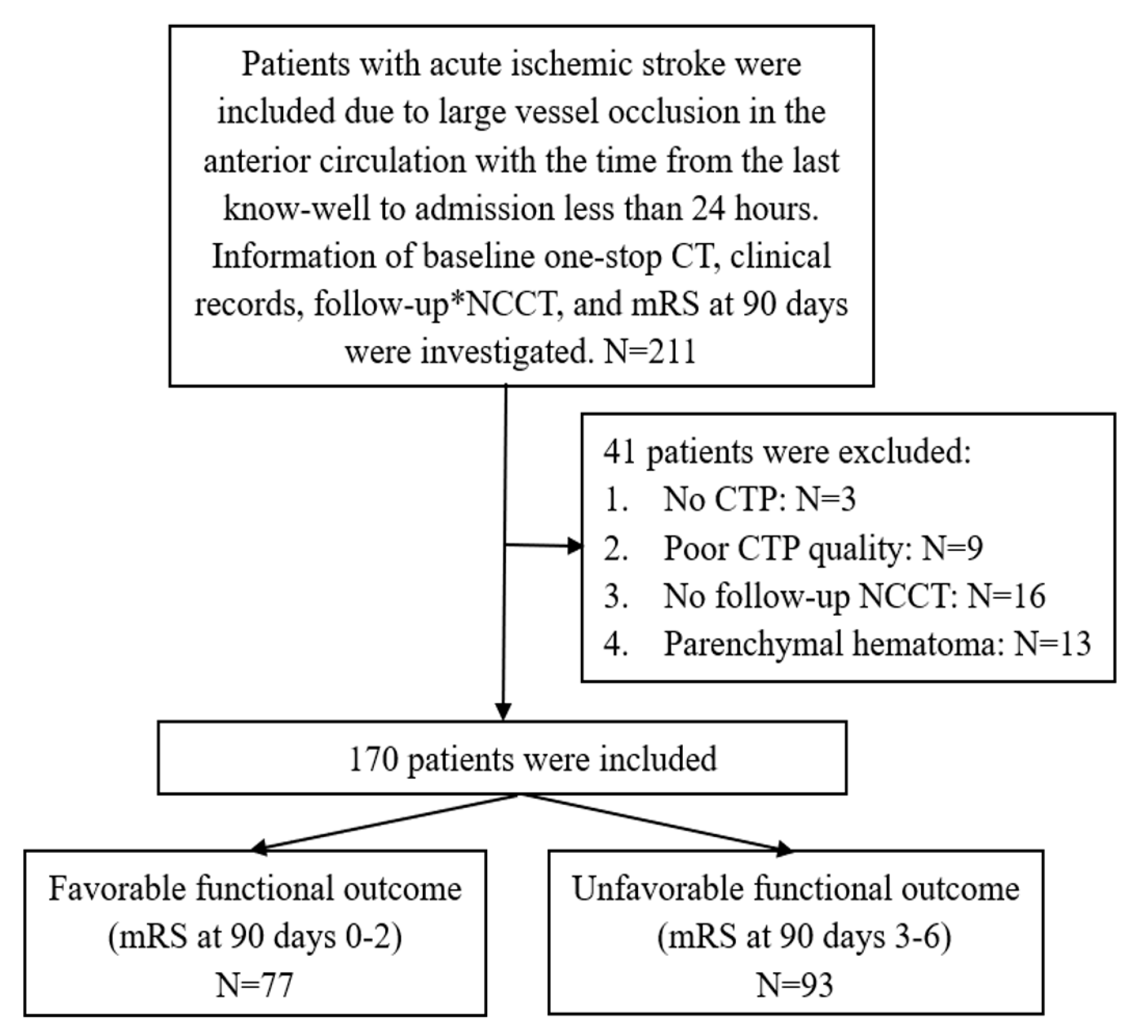
2.1. Study Design and Patients
2.2. Demographics and Clinical Risk Factors
2.3. Image Processing and Analysis
2.4. Statistics
3. Results
3.1. Predictive Model Construction
3.2. The Discrepancy Associated with Poor Functional Outcomes in Small FIV
4. Discussion
4.1. Predictive Models for FIV
4.2. The Discrepancy Associated with Poor Functional Outcomes in Small FIV
4.3. NSK Software
4.4. Future Directions
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Berkhemer, O.A.; Fransen, P.S.S.; Beumer, D.; Berg, L.A.V.D.; Lingsma, H.F.; Yoo, A.J.; Schonewille, W.J.; Vos, J.A.; Nederkoorn, P.J.; Wermer, M.J.H.; et al. A Randomized Trial of Intraarterial Treatment for Acute Ischemic Stroke. N. Engl. J. Med. 2015, 372, 11–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jovin, T.G.; Chamorro, A.; Cobo, E.; De Miquel, M.A.; Molina, C.A.; Rovira, A.; Román, L.S.; Serena, J.; Abilleira, S.; Ribo, M.; et al. Thrombectomy within 8 Hours after Symptom Onset in Ischemic Stroke. N. Engl. J. Med. 2015, 372, 2296–2306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Broocks, G.; Jafarov, H.; McDonough, R.; Austein, F.; Meyer, L.; Bechstein, M.; van Horn, N.; Nawka, M.T.; Schön, G.; Fiehler, J.; et al. Relationship between the degree of recanalization and functional outcome in acute ischemic stroke is mediated by penumbra salvage volume. J. Neurol. 2021, 268, 2213–2222. [Google Scholar] [CrossRef] [PubMed]
- Meng, X.; Ji, J. Infarct volume and outcome of cerebral ischaemia, a systematic review and meta-analysis. Int. J. Clin. Pract. 2021, 75, e14773. [Google Scholar] [CrossRef] [PubMed]
- Farzin, B.; Fahed, R.; Guilbert, F.; Poppe, A.Y.; Daneault, N.; Durocher, A.P.; Lanthier, S.; Boudjani, H.; Khoury, N.N.; Roy, D.; et al. Early CT changes in patients admitted for thrombectomy: Intrarater and interrater agreement. Neurology 2016, 87, 249–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McTaggart, R.A.; Jovin, T.G.; Lansberg, M.G.; Mlynash, M.; Jayaraman, M.V.; Choudhri, O.A.; Inoue, M.; Marks, M.P.; Albers, G.W. Alberta stroke program early computed tomographic scoring performance in a series of patients undergoing computed tomography and MRI: Reader agreement, modality agreement, and outcome prediction. Stroke 2015, 46, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Xing, H.; Li, Y.; Wang, S.; Liu, L.; Li, F.; Jing, H. Deep learning-based automated segmentation of eight brain anatomical regions using head CT images in PET/CT. BMC Med. Imaging 2022, 22, 99. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Zhen, Y.; Liu, H.; Zeng, W.; Li, Y.; Liu, L.; Yang, R. Automated ASPECTS in acute ischemic stroke: Comparison of the overall scores and Hounsfield unit values of two software packages and radiologists with different levels of experience. Acta Radiol. 2022, 64, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Conrad, J.; Ertl, M.; Oltmanns, M.H.; zu Eulenburg, P. Prediction contribution of the cranial collateral circulation to the clinical and radiological outcome of ischemic stroke. J. Neurol. 2020, 267, 2013–2021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonetti, D.A.; Gross, B.; Desai, S.; Jadhav, A.; Jankowitz, B.; Jovin, T. Final Infarct Volume of <10 cm(3) is a Strong Predictor of Return to Home in Nonagenarians Un-dergoing Mechanical Thrombectomy. World Neurosurg. 2018, 119, e941–e946. [Google Scholar]
- Bouslama, M.; Barreira, C.M.; Haussen, D.C.; Rodrigues, G.M.; Pisani, L.; Frankel, M.R.; Nogueira, R.G. Endovascular reperfusion outcomes in patients with a stroke and low ASPECTS is highly dependent on baseline infarct volumes. J. NeuroInterventional Surg. 2021, 14, 117–121. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association Professional Practice Committee. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2022. Diabetes Care 2022, 45 (Suppl. S1), S17–S38. [Google Scholar] [CrossRef]
- Zaidat, O.O.; Yoo, A.; Khatri, P.; Tomsick, T.; von Kummer, R.; Saver, J.; Marks, M.; Prabhakaran, S.; Kallmes, D.; Fitzsimmons, B.-F.; et al. Recommendations on angiographic revascularization grading standards for acute ischemic stroke: A consensus statement. Stroke 2013, 44, 2650–2663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sims, J.R.; Gharai, L.R.; Schaefer, P.W.; Vangel, M.; Rosenthal, E.S.; Lev, M.H.; Schwamm, L. ABC/2 for rapid clinical estimate of infarct, perfusion, and mismatch volumes. Neurology 2009, 72, 2104–2110. [Google Scholar] [CrossRef] [PubMed]
- Albers, G.W.; Goyal, M.; Jahan, R.; Bonafe, A.; Diener, H.-C.; Levy, E.I.; Pereira, V.M.; Cognard, C.; Cohen, D.J.; Hacke, W.; et al. Ischemic core and hypoperfusion volumes predict infarct size in SWIFT PRIME. Ann. Neurol. 2015, 79, 76–89. [Google Scholar] [CrossRef]
- Hopf-Jensen, S.; Anraths, M.; Lehrke, S.; Szymczak, S.; Hasler, M.; Müller-Hülsbeck, S. Early prediction of final infarct volume with material decomposition images of dual-energy CT after mechanical thrombectomy. Neuroradiology 2020, 63, 695–704. [Google Scholar] [CrossRef]
- Lum, C.; Ahmed, M.E.; Patro, S.; Thornhill, R.; Hogan, M.; Iancu, D.; Lesiuk, H.; dos Santos, M.; Dowlatshahi, D. Computed Tomographic Angiography and Cerebral Blood Volume Can Predict Final Infarct Volume and Outcome After Recanalization. Stroke 2014, 45, 2683–2688. [Google Scholar] [CrossRef] [Green Version]
- Mokin, M.; Levy, E.I.; Saver, J.L.; Siddiqui, A.H.; Goyal, M.; Bonafé, A.; Cognard, C.; Jahan, R.; Albers, G.W. Predictive Value of RAPID Assessed Perfusion Thresholds on Final Infarct Volume in SWIFT PRIME (Solitaire with the Intention for Thrombectomy as Primary Endovascular Treatment). Stroke 2017, 48, 932–938. [Google Scholar] [CrossRef]
- Olive-Gadea, M.; Martins, N.; Boned, S.; Carvajal, J.; Moreno, M.J.; Muchada, M.; Molina, C.A.; Tomasello, A.; Ribo, M.; Rubiera, M. Baseline ASPECTS and e-ASPECTS Correlation with Infarct Volume and Functional Outcome in Patients Undergoing Mechanical Thrombectomy. J. Neuroimaging 2018, 29, 198–202. [Google Scholar] [CrossRef]
- Robben, D.; Boers, A.M.; Marquering, H.A.; Langezaal, L.L.; Roos, Y.B.; van Oostenbrugge, R.J.; van Zwam, W.H.; Dippel, D.W.; Majoie, C.B.; van der Lugt, A.; et al. Prediction of final infarct volume from native CT perfusion and treatment parameters using deep learning. Med. Image Anal. 2019, 59, 101589. [Google Scholar] [CrossRef]
- Albers, G.W.; Goyal, M.; Jahan, R.; Bonafe, A.; Diener, H.-C.; Levy, E.I.; Pereira, V.M.; Cognard, C.; Yavagal, D.R.; Saver, J.L.; et al. Relationships Between Imaging Assessments and Outcomes in Solitaire with the Intention for Thrombectomy as Primary Endovascular Treatment for Acute Ischemic Stroke. Stroke 2015, 46, 2786–2794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boers, A.M.M.; Jansen, I.G.H.; Beenen, L.F.M.; Devlin, T.G.; Roman, L.S.; Heo, J.H.; Ribó, M.; Brown, S.; Almekhlafi, M.A.; Liebeskind, D.S.; et al. Association of follow-up infarct volume with functional outcome in acute ischemic stroke: A pooled analysis of seven randomized trials. J. NeuroInterventional Surg. 2018, 10, 1137–1142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bucker, A.; Boers, A.M.; Bot, J.C.; Berkhemer, O.A.; Lingsma, H.F.; Yoo, A.J.; van Zwam, W.H.; van Oostenbrugge, R.J.; van der Lugt, A.; Dippel, D.W.; et al. Associations of Ischemic Lesion Volume with Functional Outcome in Patients with Acute Ischemic Stroke: 24-Hour Versus 1-Week Imaging. Stroke 2017, 48, 1233–1240. [Google Scholar] [CrossRef] [PubMed]
- Federau, C.; Mlynash, M.; Christensen, S.; Zaharchuk, G.; Michael, M.; Lansberg, M.; Wintermark, M.; Albers, G.W. Evolution of Volume and Signal Intensity on Fluid-attenuated Inversion Recovery MR Images after Endovascular Stroke Therapy. Radiology 2016, 280, 184–192. [Google Scholar] [CrossRef]
- Guenego, A.; Mlynash, M.; Christensen, S.; Bs, S.K.; Heit, J.J.; Lansberg, M.G.; Albers, G.W. Hypoperfusion ratio predicts infarct growth during transfer for thrombectomy. Ann. Neurol. 2018, 84, 616–620. [Google Scholar] [CrossRef] [PubMed]
- Wouters, A.; Robben, D.; Christensen, S.; Marquering, H.A.; Roos, Y.B.; van Oostenbrugge, R.J.; van Zwam, W.H.; Dippel, D.W.; Majoie, C.B.; Schonewille, W.J.; et al. Prediction of Stroke Infarct Growth Rates by Baseline Perfusion Imaging. Stroke 2022, 53, 569–577. [Google Scholar] [CrossRef]
- Olivot, J.M.; Mlynash, M.; Inoue, M.; Marks, M.P.; Wheeler, H.M.; Kemp, S.; Straka, M.; Zaharchuk, G.; Bammer, R.; Lansberg, M.; et al. Hypoperfusion Intensity Ratio Predicts Infarct Progression and Functional Outcome in the DEFUSE 2 Cohort. Stroke 2014, 45, 1018–1023. [Google Scholar] [CrossRef] [Green Version]
- Matsumoto, M.; Sakaguchi, M.; Okazaki, S.; Hashikawa, K.; Takahashi, T.; Matsumoto, M.; Ohtsuki, T.; Shimazu, T.; Yoshimine, T.; Mochizuki, H.; et al. Relationship Between Infarct Volume and Prothrombin Time-International Normalized Ratio in Ischemic Stroke Patients with Nonvalvular Atrial Fibrillation. Circ. J. 2017, 81, 391–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, H.; Chen, Y.; Tang, T.; Ma, G.; Zhou, J.; Zhang, J.; Lu, S.; Wu, F.; Luo, L.; Liu, S.; et al. ISP-Net: Fusing features to predict ischemic stroke infarct core on CT perfusion maps. Comput. Methods Programs Biomed. 2022, 215, 106630. [Google Scholar] [CrossRef]
- Kasasbeh, A.S.; Christensen, S.; Parsons, M.W.; Campbell, B.; Albers, G.W.; Lansberg, M.G. Artificial Neural Network Computer Tomography Perfusion Prediction of Ischemic Core. Stroke 2019, 50, 1578–1581. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, D.; Desai, S.; Hudson, J.; Gross, B.; Jha, R.; Molyneaux, B.; Jankowitz, B.; Jovin, T.; Jadhav, A. Large Infarct Volume Post Thrombectomy: Characteristics, Outcomes, and Predictors. World Neurosurg. 2020, 139, e748–e753. [Google Scholar] [CrossRef] [PubMed]
- Warach, S.J.; Luby, M.; Albers, G.; Bammer, R.; Bivard, A.; Campbell, B.; Derdeyn, C.; Heit, J.; Khatri, P.; Lansberg, M.; et al. Acute Stroke Imaging Research Roadmap III Imaging Selection and Outcomes in Acute Stroke Reperfusion Clinical Trials: Consensus Recommendations and Further Research Priorities. Stroke 2016, 47, 1389–1398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christensen, S.; Mlynash, M.; Kemp, S.; Yennu, A.; Heit, J.J.; Marks, M.P.; Lansberg, M.G.; Albers, G.W. Persistent Target Mismatch Profile >24 Hours After Stroke Onset in DEFUSE 3. Stroke 2019, 50, 754–757. [Google Scholar] [CrossRef]
- Ganesh, A.; Ospel, J.; Menon, B.; Demchuk, A.; McTaggart, R.; Nogueira, R.; Poppe, A.; Almekhlafi, M.; Hanel, R.; Thomalla, G.; et al. Assessment of Discrepancies Between Follow-up Infarct Volume and 90-Day Outcomes Among Pa-tients With Ischemic Stroke Who Received Endovascular Therapy. JAMA Netw. Open 2021, 4, e2132376. [Google Scholar] [CrossRef]
- Soun, J.; Chow, D.; Nagamine, M.; Takhtawala, R.; Filippi, C.; Yu, W.; Chang, P. Artificial Intelligence and Acute Stroke Imaging. Am. J. Neuroradiol. 2020, 42, 2–11. [Google Scholar] [CrossRef]
- Ospel, J.M.; Menon, B.K.; Qiu, W.; Kashani, N.; Mayank, A.; Singh, N.; Cimflova, P.; Marko, M.; Nogueira, R.G.; McTaggart, R.A.; et al. A Detailed Analysis of Infarct Patterns and Volumes at 24-hour Noncontrast CT and Diffu-sion-weighted MRI in Acute Ischemic Stroke Due to Large Vessel Occlusion: Results from the ESCAPE-NA1 Trial. Radiology 2021, 300, 152–159. [Google Scholar] [CrossRef]
- Regenhardt, R.W.; Etherton, M.R.; Das, A.S.; Schirmer, M.D.; Hirsch, J.A.; Stapleton, C.J.; Patel, A.B.; Leslie-Mazwi, T.M.; Rost, N.S. White Matter Acute Infarct Volume After Thrombectomy for Anterior Circulation Large Vessel Occlusion Stroke is Associated with Long Term Outcomes. J. Stroke Cerebrovasc. Dis. 2020, 30, 105567. [Google Scholar] [CrossRef]
- Ernst, M.; Boers, A.M.; Aigner, A.; Berkhemer, O.A.; Yoo, A.J.; Roos, Y.B.; Dippel, D.W.; Van Der Lugt, A.; Van Oostenbrugge, R.J.; Van Zwam, W.H.; et al. Association of Computed Tomography Ischemic Lesion Location with Functional Outcome in Acute Large Vessel Occlusion Ischemic Stroke. Stroke 2017, 48, 2426–2433. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Median (IQR) or Percentage (N) | |
|---|---|
| Age, years | 68 (57–76) |
| Female | 35.3% (60/170) |
| Hypertension | 71.2% (121/170) |
| Diabetes | 29.4% (50/170) |
| History of stroke | 15.9% (27/170) |
| Current tobacco use | 34.7% (59/170) |
| Current alcohol use | 18.2% (31/170) |
| Baseline NIHSS | 11(6–18) |
| The time from the last known-well to the hospital, hours | 5.0 (2.0–9.3) |
| Occlusion locations | |
| ICA | 30.0% (51/170) |
| MCA | 67.1% (114/170) |
| ACA | 2.9% (5/170) |
| Affected hemisphere | |
| Right | 47.1% (80/170) |
| Left | 50.6% (86/170) |
| Bilateral | 2.3% (4/170) |
| Baseline e-ASPECT ● | 7 (5–9) |
| Baseline manual-ASPECT | 7 (5–9) |
| Infarct core volume ○, mL | 11.0 (3.8–43.8) |
| Hypoperfusion volume ◆, mL | 147.5 (76.5–243.3) |
| Ischemic penumbra volume ◇, mL | 92.5 (44.5–193.8) |
| FIV, mL | 54.2 (11.9–134.7) |
| Hypoperfusion index ★ | 0.25 (0.10–0.50) |
| Tmax8/6 ☆ | 0.52 (0.32–0.70) |
| Therapeutic regimens | |
| Thrombectomy | 67.1% (114/170) |
| Thrombolysis | 13.5% (23/170) |
| Conservative treatment | 17.1% (29/170) |
| Balloon stent dilatation | 2.3% (4/170) |
| Successful recanalization # | 65.3% (111/170) |
| Successful recanalization in EVT | 78.1% (107/137) |
| Blood platelet | 200.8 (150.8–235.5) |
| International normalized ratio | 1.01 (0.96–1.07) |
| 90 days mRS 0–2 | 45.3% (77/170) |
| Variable | Intraclass Correlation Coefficient | Spearman’s Rank Correlation Coefficient, p-Value | Wilcoxon Analysis of Statistical Values, p-Value |
|---|---|---|---|
| Manual-ASPECT in two observers | 0.535 | 0.563, p < 0.01 | Z = 4.676, p < 0.001 |
| e-ASPECT ● and manual-ASPECT mean scoring | 0.821 | 0.744, p < 0.01 | Z = 0.521, p = 0.605 |
| FIV in two observers | 0.921 | 0.870, p < 0.01 | Z = 0.356, p = 0.722 |
| FIV | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| Estimate | SD | p-Value | Estimate | SD | p-Value | |
| Constant | - | - | - | 224.347 | 51.577 | 0.000 ** |
| Gender | 20.819 | 16.188 | 0.200 | - | - | - |
| Age | 0.578 | 0.535 | 0.281 | - | - | - |
| Hypertension | 5.862 | 15.673 | 0.709 | - | - | - |
| Diabetes | 30.520 | 18.829 | 0.055 ^ | 21.364 | 14.982 | 0.156 |
| Current tobacco use | −24.046 | 16.916 | 0.157 | |||
| Current alcohol use | −17.137 | 19.248 | 0.375 | |||
| History of stroke | −25.141 | 19.309 | 0.195 | |||
| The time from the last known-well to the hospital | −1.486 | 1.158 | 0.201 | - | - | - |
| Baseline NIHSS | 1.165 | 0.918 | 0.207 | - | - | - |
| Affected hemisphere | −3.809 | 13.143 | 0.772 | |||
| Occlusion locations | 3.664 | 13.940 | 0.793 | - | - | - |
| Therapeutic regimens | −15.917 | 9.710 | 0.103 | - | - | - |
| Successful recanalization # | −68.326 | 17.909 | 0.000 ^ | −51.449 | 14.508 | 0.001 ** |
| Baseline e-ASPECT ● | −9.879 | 3.128 | 0.002 ^ | −11.736 | 2.882 | 0.000 ** |
| Infarct core volume ○, mL | 0.365 | 0.173 | 0.037 ^ | 0.337 | 0.170 | 0.048 * |
| Hypoperfusion volume ◆, mL | 0.166 | 0.061 | 0.007 | 0.174 | 0.058 | 0.003 * |
| Ischemic penumbra volume ◇, mL | - | - | - | - | - | - |
| Blood platelet | 0.082 | 0.111 | 0.460 | - | - | - |
| International normalized ratio | −79.472 | 43.821 | 0.072 ^ | −88.615 | 41.927 | 0.036 * |
| Hypoperfusion index ★ | 172.953 | 66.682 | 0.010 ^ | 89.262 | 33.808 | 0.009 * |
| Tmax8/6 ☆ | −83.681 | 64.991 | 0.200 | - | - | - |
| 90 Days mRS of 0–2 in FIV < 70 mL | 90 Days mRS of 3–6 in FIV < 70 mL | p-Value, OR (95% CI) | |
|---|---|---|---|
| Variable | Median (IQR) or Percentage (N) | Median (IQR) or Percentage (N) | |
| N | 60 | 38 | - |
| Age, years | 66 (56–74) | 67 (57–76) | 0.64 |
| Female | 61.7% (37/60) | 36.8% (14/38) | 0.53 |
| Hypertension | 63.3% (38/60) | 86.8% (33/38) | 0.01 *3.82 (1.30–11.22) |
| Diabetes | 21.7% (13/60) | 28.9% (11/38) | 0.28 |
| History of stroke | 8.3% (5/60) | 28.9% (11/38) | 0.01 *4.48 (1.42–14.20) |
| Current tobacco use | 15.0% (9/60) | 52.6% (20/38) | 0.00 *6.30 (2.43–16.32) |
| Current alcohol use | 11.7% (7/60) | 18.4% (7/38) | 0.26 |
| Baseline NIHSS | 7 (3–11) | 13.5 (7.5–18.0) | 0.00 ** |
| The time from the last known-well to the hospital, hours | 5.0 (2.6–12.4) | 4.5 (2.0–8.0) | 0.35 |
| Occlusion locations | - | - | 0.41 |
| ICA | 23.3% (14/60) | 31.6% (12/38) | - |
| MCA | 71.7% (43/60) | 65.8% (25/38) | - |
| ACA | 5% (3/60) | 2.6% (1/38) | - |
| Affected hemisphere | - | - | 0.46 |
| Right | 46.7% (28/60) | 47.4% (18/38) | - |
| Left | 51.7% (31/60) | 52.6% (20/38) | - |
| Bilateral | 1.7% (1/60) | 0 | - |
| Baseline e-ASPECT ● | 8.5 (7.00–10.00) | 7.50 (5.75–9.00) | 0.09 |
| Infarct core volume ○, mL | 5.0 (1.0–12.8) | 6.00 (1.00–17.25) | 0.82 |
| Hypoperfusion volume ◆, mL | 88.0 (47.0–162.3) | 137.5 (49.5–269.8) | 0.08 |
| Ischemic penumbra volume ◇, mL | 73.0 (40.5–142.8) | 133.5 (31.0–257.0) | 0.10 |
| Hypoperfusion index ★ | 0.19 (0.06–0.33) | 0.20 (0.06–0.40) | 0.55 |
| Tmax8/6 ☆ | 0.44 (0.25–0.59) | 0.44 (0.22–0.66) | 0.62 |
| FIV, mL | 14.69 (3.02–45.18) | 16.76 (2.60–26.10) | 0.80 |
| Therapeutic regimens | - | - | 0.21 |
| Thrombectomy | 70.0% (42/60) | 65.8% (25/38) | - |
| Thrombolysis | 20% (12/60) | 10.5% (4/38) | - |
| Conservative treatment | 6.7% (4/60) | 21.1% (8/38) | - |
| Balloon stent dilatation | 3.3% (2/60) | 2.6% (1/38) | - |
| Successful recanalization # | 83.3% (50/60) | 71.1% (27/38) | 0.37 |
| Blood platelet | 200.8 (151.25–242.25) | 200.94 (139.50–233.25) | 0.67 |
| International normalized ratio | 1.02 (0.96–1.08) | 1.00 (0.95–1.06) | 0.18 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, P.; Li, R.; Liu, S.; Wang, J.; Huang, L.; Song, B.; Tang, X.; Chen, B.; Yang, H.; Zhu, C.; et al. Follow-Up Infarct Volume Prediction by CTP-Based Hypoperfusion Index, and the Discrepancy between Small Follow-Up Infarct Volume and Poor Functional Outcome—A Multicenter Study. Diagnostics 2023, 13, 152. https://doi.org/10.3390/diagnostics13010152
Zhou P, Li R, Liu S, Wang J, Huang L, Song B, Tang X, Chen B, Yang H, Zhu C, et al. Follow-Up Infarct Volume Prediction by CTP-Based Hypoperfusion Index, and the Discrepancy between Small Follow-Up Infarct Volume and Poor Functional Outcome—A Multicenter Study. Diagnostics. 2023; 13(1):152. https://doi.org/10.3390/diagnostics13010152
Chicago/Turabian StyleZhou, Pengyu, Ran Li, Siyun Liu, Jincheng Wang, Lixiang Huang, Bin Song, Xiaoqiang Tang, Boyu Chen, Haiting Yang, Chengcheng Zhu, and et al. 2023. "Follow-Up Infarct Volume Prediction by CTP-Based Hypoperfusion Index, and the Discrepancy between Small Follow-Up Infarct Volume and Poor Functional Outcome—A Multicenter Study" Diagnostics 13, no. 1: 152. https://doi.org/10.3390/diagnostics13010152