
Role of Dietary and Environmental Factors on Thyroid Cancer in Romania: A Brief Review

Abstract
:1. Introduction
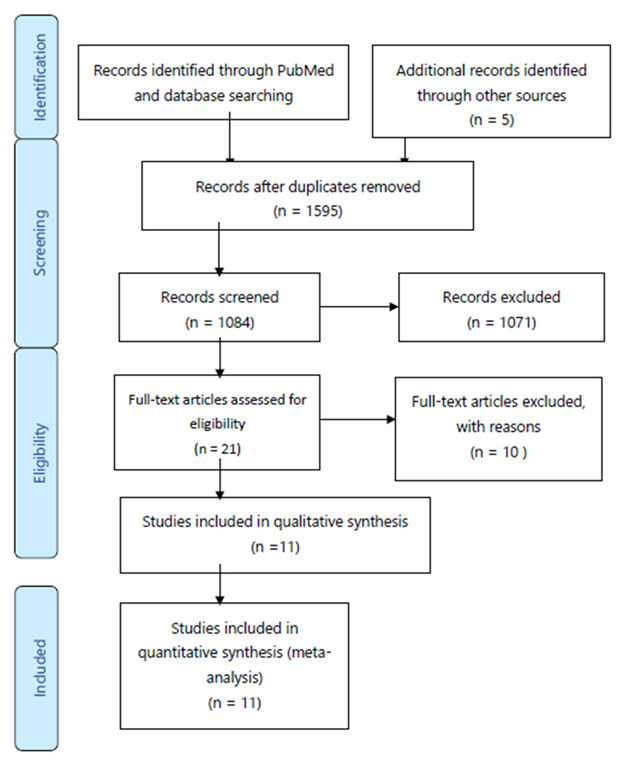
2. Materials and Methods
3. Results
4. Discussion
4.1. Iodine Deficiency
4.2. Dietary Pattern
4.3. Vitamin D Deficiency
4.4. Effects of the Chernobyl Fallout Radiation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Prete, A.; Borges De Souza, P.; Censi, S.; Muzza, M.; Nucci, N.; Sponziello, M. Update on Fundamental Mechanisms of Thyroid Cancer. Front. Endocrinol. 2020, 11, 102. [Google Scholar] [CrossRef] [PubMed]
- Ye, L.; Zhou, X.; Huang, F.; Wang, W.; Qi, Y.; Xu, H.; Shu, Y.; Shen, L.; Fei, X.; Xie, J.; et al. The genetic landscape of benign thyroid nodules revealed by whole exome and transcriptome sequencing. Nat. Commun. 2017, 8, 15533. [Google Scholar] [CrossRef] [PubMed]
- Piciu, D. Thyroid cancer incidence 25 years after Chernobyl, in a Romanian cancer center: Is it a public health problem? Curr. Radiopharm. 2013, 6, 249–252. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Photosynthesis of vitamin D in the skin: Effect of environmental and life-style variables. Fed. Proc. 1987, 46, 1876–1882. [Google Scholar] [PubMed]
- Gimm, O. Thyroid cancer. Cancer Lett. 2001, 163, 143–156. [Google Scholar] [CrossRef]
- Nettore, I.C.; Colao, A.; Macchia, P.E. Nutritional and Environmental Factors in Thyroid Carcinogenesis. Int. J. Environ. Res. Public Health 2018, 15, 1735. [Google Scholar] [CrossRef] [PubMed]
- Buzduga, C.; Mogoş, V.; Găleşanu, C.; Vulpoi, C.; Ungureanu, M.; Cristea, C.; Preda, C.; Ciobanu, D.; Ferariu, D.; Florea, N.; et al. Epidemiology and histology of malignant thyroid nodules in North East Region of Romania (Moldavia) before and after alimentary salt universal iodination. Rev. Med. Chir. Soc. Med. Nat. 2011, 115, 45–48. [Google Scholar]
- Szántó, Z.; Kun, I.Z.; Borda, A.; Jung, J. Thyroid cancer in two representative medical centers in Mures County between 1984–2007. Acta Endocrinol. 2009, 5, 199–211. [Google Scholar]
- Cătană, R.; Boilă, A.; Borda, A. Thyroid cancer profile in Mures County (Romania): A 20 years study. Rom. J. Morphol. Embryol. 2012, 53, 1007–1012. [Google Scholar]
- Gaengler, S.; Andrianou, X.D.; Piciu, A.; Charisiadis, P.; Zira, C.; Aristidou, K.; Piciu, D.; Makris, K.C. Iodine status and thyroid nodules in females: A comparison of Cyprus and Romania. Public Health 2017, 143, 37–43. [Google Scholar] [CrossRef]
- Ștefan, A.-I.; Piciu, A.; Căinap, S.S.; Gabora, K.; Piciu, D. Differentiated Thyroid Cancer in Children in the Last 20 Years: A Regional Study in Romania. J. Clin. Med. 2020, 9, 3617. [Google Scholar] [CrossRef]
- Diop, O.; Peştean, C.; Bathily, E.; Bãrbuş, E.; Mbodj, M.; Piciu, D. Thyroid cancer in pediatric population in Romania: 30-year aft Chernobyl accident at Institute of Oncology, Cluj-Napoca, “Prof. Dr. Ion Chiricut”. Méd. Nucl. 2019, 43, 196–197. [Google Scholar] [CrossRef]
- Piciu, D.; Irimie, A.; Piciu, A. Thyroid cancer in children: A 20-year study at a Romanian oncology institute. Endocr. J. 2019, 59, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Teodoriu, L.; Ungureanu, M.C.; Leustean, L.; Preda, C.; Ciobanu, D.; Grierosu, I.; Matei, M.; Iacob, R.; Stefanescu, C. Updated Incidence of Thyroid Cancer in the North East Region of Romania after 35 Years of Chernobyl Fallout. Is There a Link between? Diagnostics 2021, 11, 907. [Google Scholar] [CrossRef]
- Stanciu, M.; Racz, I.-C.; Bera, L.; Rotaru, M.; Popa, F. Thyroid Cancer Incidence in Sibiu County. Acta Med. Transilv. 2015, 20, 16–18. [Google Scholar]
- Leung, A.M.; Pearce, E.N.; Braverman, L.E. Iodine nutrition in pregnancy and lactation. Endocrinol. Metab. Clin. N. Am. 2011, 40, 765–777. [Google Scholar] [CrossRef] [PubMed]
- Andersson, M.; Karumbunathan, V.; Zimmermann, M.B. Global iodine status in 2011 and trends over the past decade. J. Nutr. 2012, 142, 744–750. [Google Scholar] [CrossRef]
- Popa, A.; Gălușcă, D. The Implications of Alimentation in Thyroid Disorders. Annals of the University of Oradea, Fascicle: Ecotoxicology, Animal Husbandry and Food Science and Technology, Vol. XVII/B 2018; pp. 165–169. Available online: https://www.google.com.hk/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&ved=2ahUKEwjOo5SqpsP5AhUQqFYBHaI5BVUQFnoECAkQAQ&url=https%3A%2F%2Fprotmed.uoradea.ro%2Ffacultate%2Fpublicatii%2Fecotox_zooteh_ind_alim%2F2018A%2FVaria%2FPopa%2520Anca.pdf&usg=AOvVaw3H-kUdmf3kCFxmKDzbY7RD (accessed on 6 June 2022).
- Government of Romania. National Strategy on the Elimination of Iodine Deficiency Disorders by Universal Iodization of Salt Intended for Direct Human Use and for Bread Baking; MarLink: Bucharest, Romania, 2005; ISBN 973-8411-40-8. [Google Scholar]
- Sehestedt, T.; Knudsen, N.; Perrild, H.; Johansen, C. Iodine intake and incidence of thyroid cancer in Denmark. Clin. Endocrinol. 2006, 65, 229–233. [Google Scholar] [CrossRef]
- Horn-Ross, P.L.; Hoggatt, K.J.; Lee, M.M. Phytoestrogens and thyroid cancer risk: The San Francisco Bay Area thyroid cancer study. Cancer Epidemiol. Biomark. Prev. 2002, 11, 43–49. [Google Scholar]
- Dijkstra, B.; Prichard, R.S.; Lee, A.; Kelly, L.M.; Smyth, P.P.A.; Crotty, T.; McDermott, E.W.; Hill, A.D.K.; O’Higgins, N. Changing patterns of thyroid carcinoma. Ir. J. Med. Sci. 2007, 176, 87–90. [Google Scholar] [CrossRef]
- Wang, F.; Wang, Y.; Wang, L.; Wang, X.; Sun, C.; Xing, M.; Zhao, W. Strong association of high urinary iodine with thyroid nodule and papillary thyroid cancer. Tumor Biol. 2014, 35, 11375–11379. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Park, H.K.; Byun, D.W.; Suh, K.; Yoo, M.H.; Min, Y.-K.; Kim, S.W.; Chung, J.H. Iodine intake as a risk factor for BRAF mutations in papillary thyroid cancer patients from an iodine-replete area. Eur. J. Nutr. 2018, 57, 809–815. [Google Scholar] [CrossRef] [PubMed]
- Knobel, M.; Medeiros-Neto, G. Relevance of iodine intake as a reputed predisposing factor for thyroid cancer. Arq. Bras. Endocrinol. Metabol. 2007, 51, 701–712. [Google Scholar] [CrossRef] [PubMed]
- Zamora-Ros, R.; Castañeda, J.; Rinaldi, S.; Cayssials, V.; Slimani, N.; Weiderpass, E.; Tsilidis, K.K.; Boutron-Ruault, M.-C.; Overvad, K.; Eriksen, A.K.; et al. Consumption of Fish Is Not Associated with Risk of Differentiated Thyroid Carcinoma in the European Prospective Investigation into Cancer and Nutrition (EPIC) Study. J. Nutr. 2017, 147, 1366–1373. [Google Scholar] [CrossRef] [PubMed]
- European Parliament. Available online: https://www.europarl.europa.eu/doceo/document/E-9-2019-003731_EN.html (accessed on 23 April 2022).
- Zamora-Ros, R.; Béraud, V.; Franceschi, S.; Cayssials, V.; Tsilidis, K.K.; Boutron-Ruault, M.-C.; Weiderpass, E.; Overvad, K.; Tjonneland, A.; Eriksen, A.K.; et al. Consumption of fruits, vegetables and fruit juices and differentiated thyroid carcinoma risk in the European Prospective Investigation into Cancer and Nutrition (EPIC) study. Int. J. Cancer 2018, 142, 449–459. [Google Scholar] [CrossRef] [PubMed]
- Eurostat. Available online: https://ec.europa.eu/eurostat/fr/ (accessed on 23 April 2022).
- Cléro, É.; Doyon, F.; Chungue, V.; Rachédi, F.; Boissin, J.L.; Sebbag, J.; Shan, L.; Rubino, C.; de Vathaire, F. Dietary patterns, goitrogenic food, and thyroid cancer: A case-control study in French Polynesia. Nutr. Cancer 2012, 64, 929–936. [Google Scholar] [CrossRef] [PubMed]
- Sen, A.; Tsilidis, K.K.; Allen, N.E.; Rinaldi, S.; Appleby, P.N.; Almquist, M.; Schmidt, J.A.; Dahm, C.C.; Overvad, K.; Tjonneland, A.; et al. Baseline and lifetime alcohol consumption and risk of differentiated thyroid carcinoma in the EPIC study. Br. J. Cancer 2015, 113, 840–847. [Google Scholar] [CrossRef] [PubMed]
- Furtunescu, F.; Mincă, D.G.; Vasile, A.; Domnariu, C.D. Alcohol consumption impact on premature mortality in Romania. Rom. J. Leg. Med. 2009, 4, 296–302. [Google Scholar] [CrossRef]
- Marcello, M.A.; Sampaio, A.C.; Geloneze, B.; Vasques, A.C.J.; Assumpção, L.V.M.; Ward, L.S. Obesity and excess protein and carbohydrate consumption are risk factors for thyroid cancer. Nutr. Cancer 2012, 64, 1190–1195. [Google Scholar] [CrossRef]
- Bartholomeusz, C.; Gonzalez-Angulo, A.M. Targeting the PI3K signaling pathway in cancer therapy. Expert Opin. Ther. Targets 2012, 16, 121–130. [Google Scholar] [CrossRef]
- Kilfoy, B.A.; Zhang, Y.; Park, Y.; Holford, T.R.; Schatzkin, A.; Hollenbeck, A.; Ward, M.H. Dietary nitrate and nitrite and the risk of thyroid cancer in the NIH-AARP Diet and Health Study. Int. J. Cancer 2011, 129, 160–172. [Google Scholar] [CrossRef] [PubMed]
- Ward, M.H.; Kilfoy, B.A.; Weyer, P.J.; Anderson, K.E.; Folsom, A.R.; Cerhan, J.R. Nitrate intake and the risk of thyroid cancer and thyroid disease. Epidemiology 2010, 21, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Lijinsky, W. The anomalous biological activity of nitroso-2-oxopropyl compounds. Cancer Lett. 1991, 60, 121–127. [Google Scholar] [CrossRef]
- Socaciu, C.; Stãnilã, A. Nitrates in Food, Health and the Environment. In Case Studies in Food Safety and Environmental Health; Springer: Boston, MA, USA, 2007. [Google Scholar] [CrossRef]
- Nettore, I.C.; Albano, L.; Ungaro, P.; Colao, A.; Macchia, P.E. Sunshine vitamin and thyroid. Rev. Endocr. Metab. Disord. 2017, 18, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Sunlight and vitamin D for bone health and prevention of autoimmune diseases, cancers, and cardiovascular disease. Am. J. Clin. Nutr. 2004, 80, 1678–1688. [Google Scholar] [CrossRef]
- Şahin, M.; Uçan, B.; Giniş, Z.; Topaloğlu, O.; Güngüneş, A.; Bozkurt, N.Ç.; Arslan, M.S.; Ünsal, İ.Ö.; Akkaymak, E.T.; Demirci, T.; et al. Vitamin D3 levels and insulin resistance in papillary thyroid cancer patients. Med. Oncol. 2013, 30, 589. [Google Scholar] [CrossRef]
- Roskies, M.; Dolev, Y.; Caglar, D.; Hier, M.P.; Mlynarek, A.; Majdan, A.; Payne, R.J. Vitamin D deficiency as a potentially modifiable risk factor for thyroid cancer. J. Otolaryngol.—Head Neck Surg. 2012, 41, 160–163. [Google Scholar] [PubMed]
- Kim, J.R.; Kim, B.H.; Kim, S.M.; Oh, M.Y.; Kim, W.J.; Jeon, Y.K.; Lee, B.J.; Kim, Y.K.; Kim, I.J. Low serum 25 hydroxyvitamin D is associated with poor clinicopathologic characteristics in female patients with papillary thyroid cancer. Thyroid 2014, 24, 1618–1624. [Google Scholar] [CrossRef]
- Stepien, T.; Krupinski, R.; Sopinski, J.; Kuzdak, K.; Komorowski, J.; Lawnicka, H.; Stepien, H. Decreased 1-25 dihydroxyvitamin D3 concentration in peripheral blood serum of patients with thyroid cancer. Arch. Med. Res. 2010, 41, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Jonklaas, J.; Danielsen, M.; Wang, H. A pilot study of serum selenium, vitamin D, and thyrotropin concentrations in patients with thyroid cancer. Thyroid 2013, 23, 1079–1086. [Google Scholar] [CrossRef] [PubMed]
- Danilovic, D.L.S.; Ferraz-De-Souza, B.; Fabri, A.W.; Santana, N.O.; Kulcsar, M.A.; Cernea, C.R.; Marui, S.; Hoff, A.O. 25-Hydroxyvitamin D and TSH as Risk Factors or Prognostic Markers in Thyroid Carcinoma. PLoS ONE 2016, 11, e0164550. [Google Scholar] [CrossRef]
- Chirita-Emandi, A.; Socolov, D.; Haivas, C.; Calapiș, A.; Gheorghiu, C.; Puiu, M. Vitamin D Status: A Different Story in the Very Young versus the Very Old Romanian Patients. PLoS ONE 2015, 10, e0128010. [Google Scholar] [CrossRef]
- Niculescu, D.A.; Capatina, C.A.M.; Dusceac, R.; Caragheorgheopol, A.; Ghemigian, A.; Poiana, C. Seasonal variation of serum vitamin D levels in Romania. Arch. Osteoporos. 2017, 12, 113. [Google Scholar] [CrossRef] [PubMed]
- Oncescu, M.; Sonoc, S. Artificial radioactivity in Romania. In Romanian society for radiological protection; Horia Hulubei Publishing House: Bucharest, Romania, 1995; pp. 7–13. [Google Scholar]
- Piciu, D.; Irimie, A.; Piciu, A. Investigation of thyroid carcinoma over 40 years, using the database of the Ion Chiricuta Institute of Oncology Cluj-Napoca. JBUON 2014, 19, 524–529. [Google Scholar]
- Davidescu, D.; Iacob, O. Thyroid cancer incidence after Chernobyl accident in Eastern Romania. Int. J. Radiat. Med. 2004, 6, 30–37. [Google Scholar]
- Leenhardt, L.; Bernier, M.O.; Boin-Pineau, M.H.; Conte Devolx, B.; Maréchaud, R.; Niccoli-Sire, P.; Nocaudie, M.; Orgiazzi, J.; Schlumberger, M.; Wémeau, J.L.; et al. Advances in diagnostic practices affect thyroid cancer incidence in France. Eur. J. Endocrinol. 2004, 150, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Mazzaferri, E.L. An Overview of the Management of Thyroid Cancer. In Practical Management of Thyroid Cancer, A Multidisciplinary Approach; Springer: London, UK, 2006; pp. 1–28. [Google Scholar]


{kind=link}
| Author | Year | Counties |
|---|---|---|
| Buzduga et al. [7] | 2011 | Moldova Romania |
| Szántó et al. [8] | 2009 | Mures County |
| Catana et al. [9] | 2012 | Mures County |
| Gaengler et al. [10] | 2017 | Romania and Cyprus |
| Author | Number of Patients | Main Findings |
|---|---|---|
| Buzduga et al. [7] | 601 | After the introduction of universal iodination: -the number of thyroid cancers has raised. -the number of follicular cancers decreased. |
| Szántó et al. [8] | 288 | The universal iodine prophylaxis might increase the papillary/follicular carcinoma ratio. |
| Catana et al. [9] | 524 | Increasing proportion of papillary thyroid carcinoma after iodine prophylaxis |
| Gaengler et al. [10] | 208 | Participants with inadequate UI (<100 µg/L) had increased risk for thyroid nodules. |
| Author | Year | Counties |
|---|---|---|
| Piciu et al. [3] | 2013 | Not specified |
| Szántó et al. [8] | 2009 | Mures County |
| Catana et al. [9] | 2012 | Mures County |
| Stefan et al. [11] | 2020 | Not specified |
| Diop et al. [12] | 2019 | Not specified |
| Piciu et al. [13] | 2013 | Not specified |
| Teodoriu et al. [14] | 2021 | Northeast region of Romania |
| Stanciu et al. [15] | 2015 | Sibiu |
| Author | Number of Patients | Main Findings |
|---|---|---|
| Piciu et al. [3] | 4779 | Rising TC incidence and major increase in the number and aggressiveness of pediatric TC cases |
| Szántó et al. [8] | 288 | Incidence of TC started to increase continuously from 1992 |
| Catana et al. [9] | 524 | Increasing incidence between 1990 and 2009 of 2–5 times, mostly due to papillary thyroid neoplasm |
| Stefan et al. [11] | 62 | The majority of affected children with TC were born mostly after Chernobyl disaster, with many cases recorded among children born in 1996, 1999 and 2000 at 10, 13 and 14 years after the accident |
| Diop et al. [12] | 40 | Children born between 10 and 15 years after the Chernobyl disaster are the most affected by TC |
| Piciu et al. [13] | 72 | Increasing incidence of adult and pediatric TC |
| Teodoriu et al. [14] | 1159 | Constant increase in TC over 30 years after the Chernobyl fallout |
| Stanciu et al. [15] | 61 | Increasing incidence of TC |
| Study | Risk of Bias (QUADAS-2) | Applicability Concerns (QUADAS-2) | |||||
|---|---|---|---|---|---|---|---|
| P | I | R | FT | P | I | R | |
| Piciu et al., 2013 [3] | ✓ | ✓ | ✓ | ? | ✓ | ✓ | ✓ |
| Buzduga et al., 2011 [7] | ✓ | ✓ | ✓ | ? | ✓ | ✓ | ✓ |
| Szántó et al., 2009 [8] | ✓ | ✓ | ✓ | ? | ✓ | ✓ | ✓ |
| Catana et al., 2012 [9] | ✓ | ✗ | ✓ | ? | ✓ | ✓ | ✓ |
| Gaengler et al., 2017 [10] | ✗ | ✓ | ✓ | ? | ✓ | ✓ | ✓ |
| Stefan et al., 2020 [11] | ? | ✓ | ✓ | ? | ✓ | ✓ | ✓ |
| Diop et al., 2019 [12] | ✗ | ✓ | ✓ | ? | ✓ | ✓ | ✓ |
| Piciu et al., 2013 [13] | ✓ | ✓ | ✓ | ? | ✓ | ✓ | ✓ |
| Teodoriu et al., 2021 [14] | ✓ | ✓ | ✓ | ? | ✓ | ✓ | ✓ |
| Stanciu et al., 2015 [15] | ✗ | ✓ | ✓ | ? | ✓ | ✓ | ✓ |
| Median Urinary Iodine (µg/L) | Iodine Intake | Iodine Nutrition |
|---|---|---|
| <20 | Insufficient | Severe iodine deficiency |
| 20–49 | Insufficient | Moderate iodine deficiency |
| 50–99 | Insufficient | Mild iodine deficiency |
| 100–199 | Adequate | Optimal |
| 200–299 | More than adequate | Risk of iodine- induced hyperthyroidism |
| ≥300 | Excessive | Risk of adverse health consequences (Iodine-induced hyperthyroidism, autoimmune thyroid disease) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kermoison, G.; Draganescu, C. Role of Dietary and Environmental Factors on Thyroid Cancer in Romania: A Brief Review. Diagnostics 2022, 12, 1959. https://doi.org/10.3390/diagnostics12081959
Kermoison G, Draganescu C. Role of Dietary and Environmental Factors on Thyroid Cancer in Romania: A Brief Review. Diagnostics. 2022; 12(8):1959. https://doi.org/10.3390/diagnostics12081959
Chicago/Turabian StyleKermoison, Gilles, and Ciprian Draganescu. 2022. "Role of Dietary and Environmental Factors on Thyroid Cancer in Romania: A Brief Review" Diagnostics 12, no. 8: 1959. https://doi.org/10.3390/diagnostics12081959