
Patient Population and Test Utilization for Thyroid Function in Local Clinics and Hospitals in Korea


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Baseline Characteristics of the Study Subjects
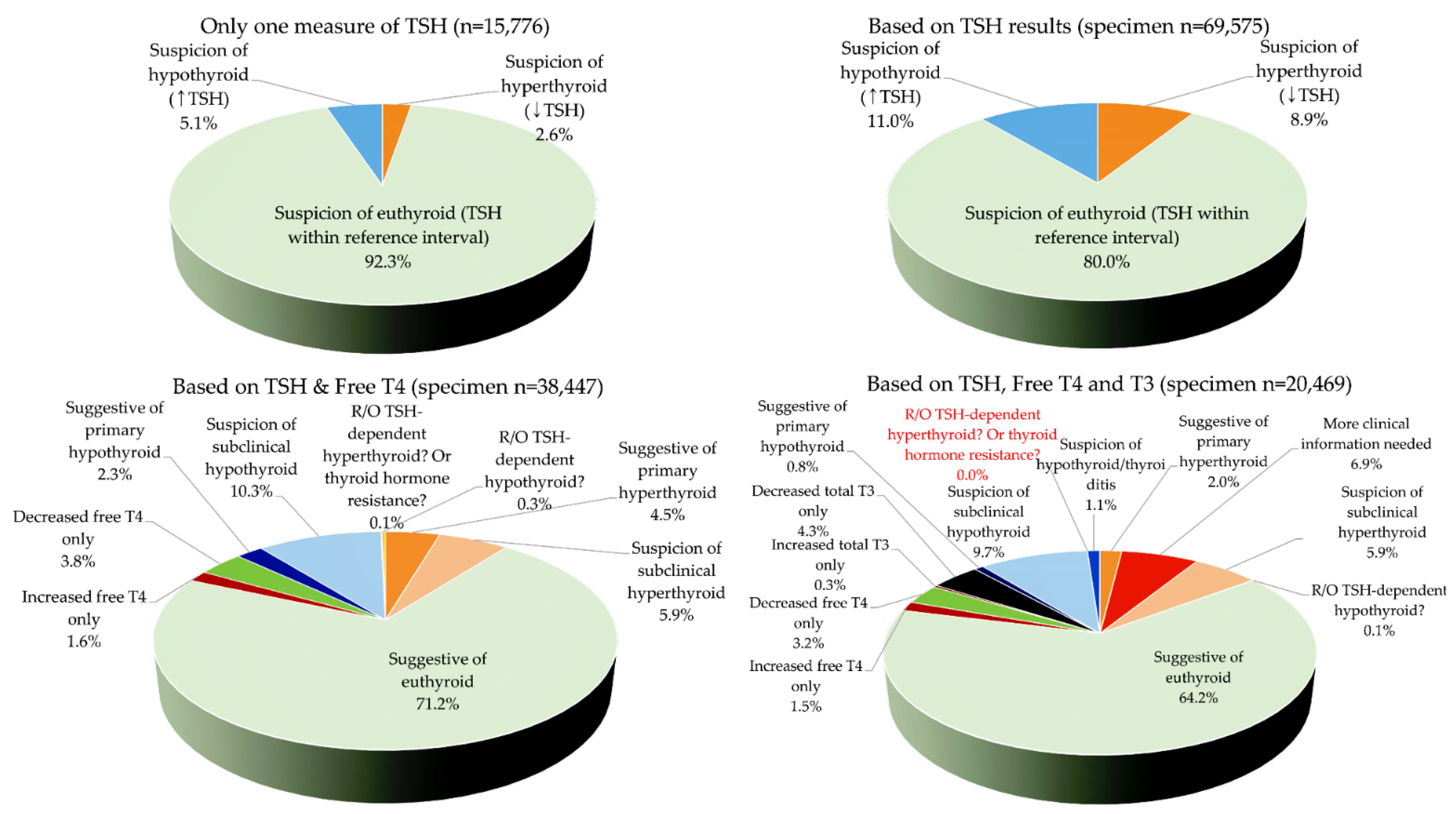
3.2. Thyroid Function Test Results and Possible Interpretation
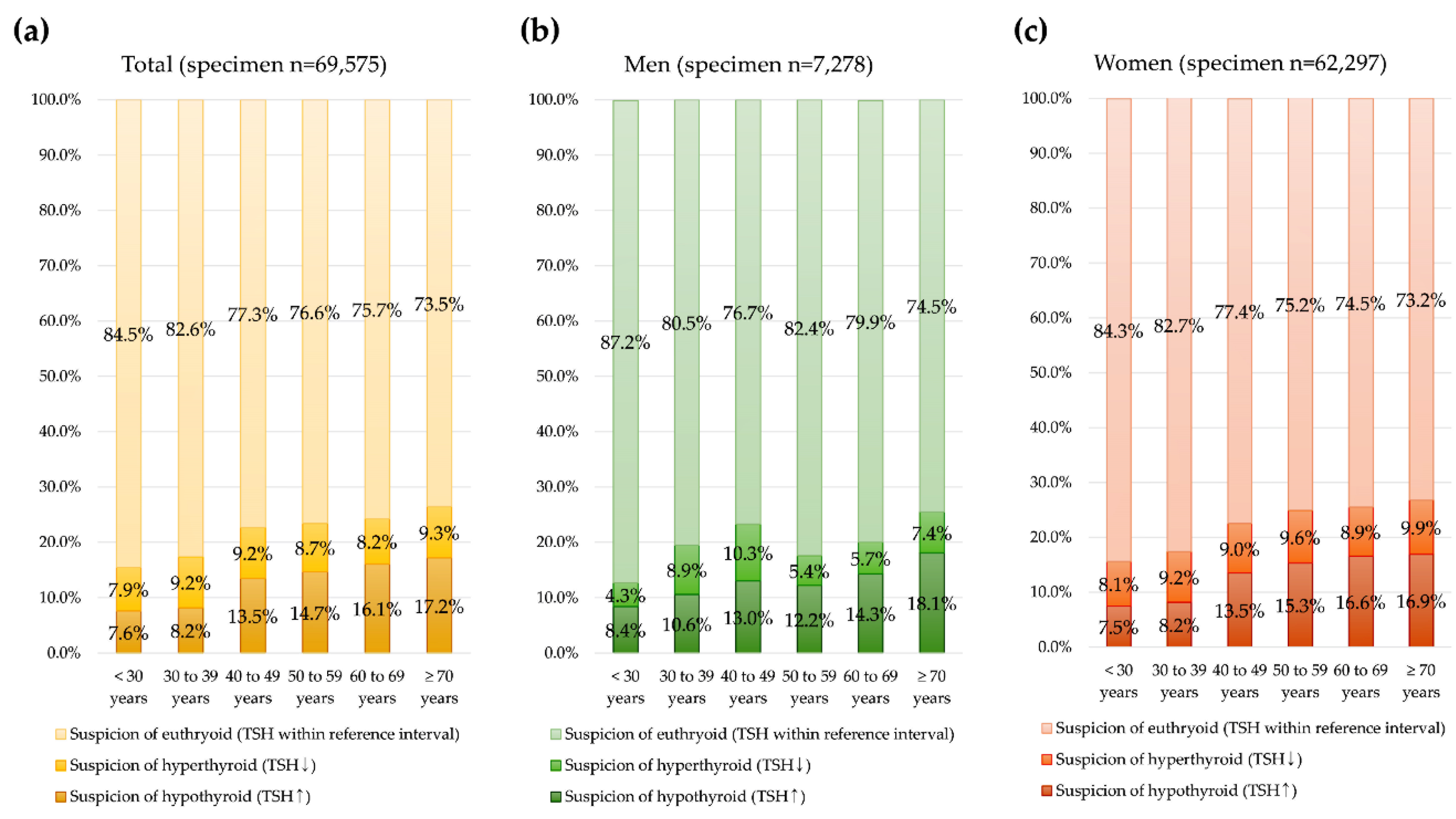
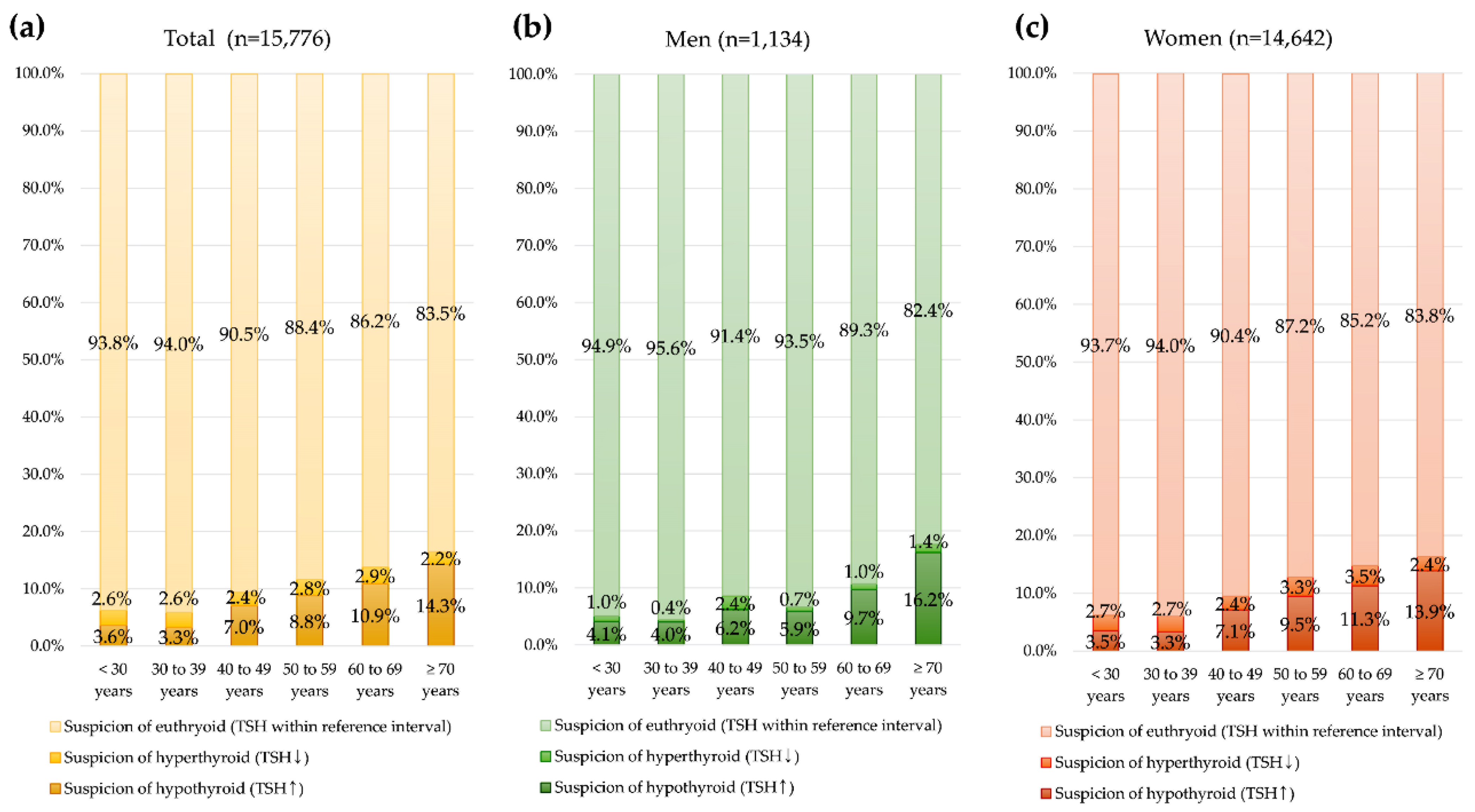
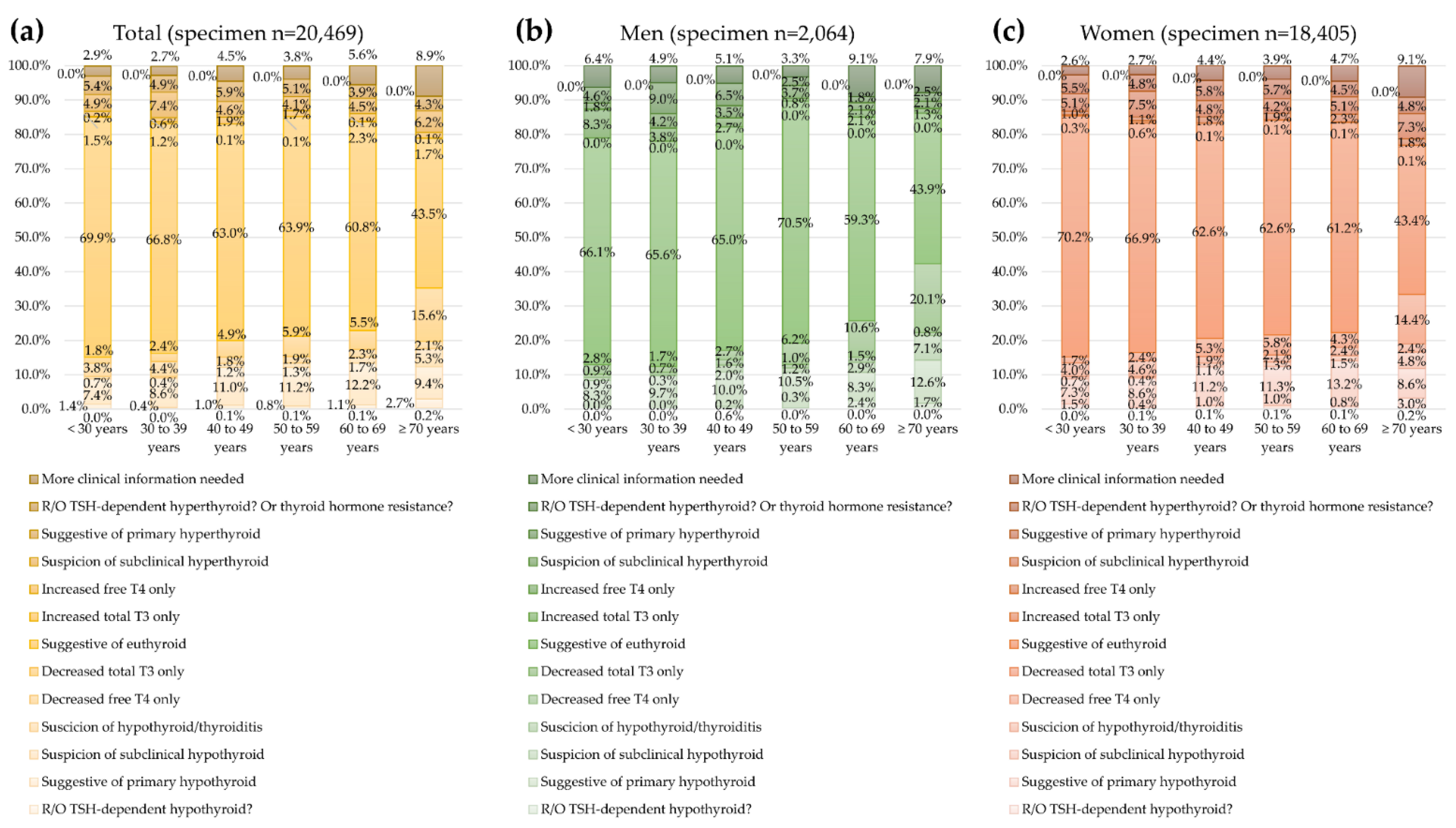
3.3. Thyroid Function Test Results and Possible Interpretation by Sex and Age
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jonklaas, J.; Razvi, S. Reference intervals in the diagnosis of thyroid dysfunction: Treating patients not numbers. Lancet Diabetes Endocrinol. 2019, 7, 473–483. [Google Scholar] [CrossRef]
- Burch, H.B. Drug Effects on the Thyroid. N. Engl. J. Med. 2019, 381, 749–761. [Google Scholar] [CrossRef] [PubMed]
- Köhrle, J. The Colorful Diversity of Thyroid Hormone Metabolites. Eur. Thyroid J. 2019, 8, 115–129. [Google Scholar] [CrossRef] [PubMed]
- Moon, J.H.; Yi, K.H. The diagnosis and management of hyperthyroidism in Korea: Consensus report of the Korean thyroid association. Endocrinol. Metab. 2013, 28, 275–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- LeFevre, M.L. Screening for thyroid dysfunction: U.S. Preventive Services Task Force recommendation statement. Ann. Intern. Med. 2015, 162, 641–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, T.E.; Wong, W.B.; Janowiak, D.; Hilborne, L.H. Strategies for laboratory professionals to drive laboratory stewardship. Pract. Lab. Med. 2021, 26, e00249. [Google Scholar] [CrossRef] [PubMed]
- Ross, D.S.; Burch, H.B.; Cooper, D.S.; Greenlee, M.C.; Laurber, P.; Maia, A.L.; Rivkees, S.A.; Samuels, M.; Sosa, J.A.; Stan, M.N.; et al. 2016 American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of Thyrotoxicosis. Thyroid 2016, 26, 1343–1421. [Google Scholar] [CrossRef] [PubMed]
- Biondi, B.; Bartalena, L.; Cooper, D.S.; Hegedüs, L.; Laurberg, P.; Kahaly, G.J. The 2015 European Thyroid Association Guidelines on Diagnosis and Treatment of Endogenous Subclinical Hyperthyroidism. Eur. Thyroid J. 2015, 4, 149–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gill, J.; Barakauskas, V.E.; Thomas, D.; Rodriguez-Capote, K.; Higgins, T.; Zhang, D.; VanSpronsen, A.; Babenko, O.; Martindale, R.; Estey, M.P. Evaluation of thyroid test utilization through analysis of population-level data. Clin. Chem. Lab. Med. 2017, 55, 1898–1906. [Google Scholar] [CrossRef] [PubMed]
- Bahn, C.R.S.; Burch, H.B.; Cooper, D.S.; Garber, J.R.; Greenlee, M.C.; Klein, I.; Laurberg, P.; McDougall, I.R.; Montori, V.M.; Rivkees, S.A.; et al. American Thyroid Association; American Association of Clinical Endocrinologists. Hyperthyroidism and other causes of thyrotoxicosis: Management guidelines of the American Thyroid Association and American Association of Clinical Endocrinologists. Thyroid 2011, 21, 593–646. [Google Scholar]
- Persani, L.; Brabant, G.; Dattani, M.; Bonomi, M.; Feldt-Rasmussen, U.; Fliers, E.; Gruters, A.; Maiter, D.; Schoenmakers, N.; van Trotsenburg, A.S.P. 2018 European Thyroid Association (ETA) Guidelines on the Diagnosis and Management of Central Hypothyroidism. Eur. Thyroid J. 2018, 7, 225–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, R.; Lee, S.; Lee, S.G.; Lee, E.H. Utilization of Anti-Thyroid Peroxidase Antibody in Local Clinics and Hospitals and Intraindividual Changes in Korean Patients. Clin. Lab. 2021, 67, 2152–2156. [Google Scholar] [CrossRef] [PubMed]
- McPherson, R.; Pincus, R. Chapter 25. Evaluation of Endocrine Function, Table 25.6. Characterization of thyroid disorders according to results of thyroid function tests. In Henry’s Clinical Diagnosis and Management by Laboratory Methods, 24th ed.; Elsevier: Philadelphia, PA, USA, 2022. [Google Scholar]
- Taylor, P.N.; Albrecht, D.; Scholz, A.; Gutierrez-Buey, G.; Lazarus, J.H.; Dayan, C.M.; Okosieme, O.E. Global epidemiology of hyperthyroidism and hypothyroidism. Nat. Rev. Endocrinol. 2018, 14, 301–316. [Google Scholar] [CrossRef] [PubMed]
- Soh, S.-B.; Aw, T.-C. Laboratory Testing in Thyroid Conditions-Pitfalls and Clinical Utility. Ann. Lab. Med. 2019, 39, 3–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Favresse, J.; Burlacu, M.-C.; Maiter, D.; Gruson, D. Interferences With Thyroid Function Immunoassays: Clinical Implications and Detection Algorithm. Endocr. Rev. 2018, 39, 830–850. [Google Scholar] [CrossRef] [PubMed]
- Vasikaran, S.; Logh, T.P. Interpretative commenting in clinical chemistry with worked examples for thyroid function test reports. Pract. Lab. Med. 2021, 26, e00243. [Google Scholar] [CrossRef] [PubMed]
- CLSI. User Protocol for Evaluation of Qualitative Test Performance, 2nd ed.; Approved Guideline; CLSI Document EP12A2; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2008. [Google Scholar]
- CLSI. Evaluation of Total Analytical Error for Quantitative Medical Laboratory Measurement Procedures, 2nd ed.; CLSI Guideline EP21; Clinical and Laboratory Institute: Wayne, PA, USA, 2016. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total Subjects (n = 47,685) | Men (n = 4878) | Women (n = 42,807) |
|---|---|---|---|
| Age, years (median, IQR) | 37.8 (33.0 to 51.8) | 52.7 (41.3 to 60.8) | 36.9 (32.7 to 49.6) |
| Age group (n, %) | |||
| <30 years | 4755 (10.0%) | 326 (6.7%) | 4429 (10.3%) |
| 30–39 years | 22,483 (47.1%) | 788 (16.2%) | 21,695 (50.7%) |
| 40–49 years | 7268 (15.2%) | 981 (20.1%) | 6287 (14.7%) |
| 50–59 years | 7209 (15.1%) | 1448 (29.7%) | 5761 (13.5%) |
| 60–69 years | 3904 (8.2%) | 875 (17.9%) | 3029 (7.1%) |
| 70 years | 2066 (4.3%) | 460 (9.4%) | 1606 (3.8%) |
| Follow-up, number (median, IQR) | 1 (1 to 1) | 1 (1 to 1) | 1 (1 to 1) |
| Baseline thyroid function test result | |||
| TSH, μIU/mL (median, IQR) | 1.78 (1.08 to 2.78) | 1.79 (1.15 to 2.79) | 1.77 (1.07 to 2.78) |
| Free T4, ng/dL (median, IQR) | 1.25 (1.12 to 1.39) | 1.30 (1.17 to 1.45) | 1.24 (1.11 to 1.38) |
| Total T3, ng/mL (median, IQR) | 1.00 (0.90 to 1.20) | 1.10 (0.90 to 1.20) | 1.00 (0.90 to 1.20) |
| TFT | TSH | Free T4 | Total T3 | Possible Interpretation | n | % |
|---|---|---|---|---|---|---|
| TSH only (n = 69,575) | ↓ | N/A | N/A | Suspicion of hyperthyroid | 6207 | 8.9 |
| - | N/A | N/A | Suspicion of euthyroid | 55,686 | 80.0 | |
| ↑ | N/A | N/A | Suspicion of hypothyroid | 7682 | 11.0 | |
| TSH & Free T4 (n = 38,447) | ↓ | ↑ | N/A | Suggestive of primary hyperthyroid | 1745 | 4.5 |
| ↓ | - | N/A | Suspicion of subclinical hyperthyroid | 2252 | 5.9 | |
| - | - | N/A | Suggestive of euthyroid | 27,387 | 71.2 | |
| - | ↑ | N/A | Increased free T4 only | 630 | 1.6 | |
| - | ↓ | N/A | Decreased free T4 only | 1443 | 3.8 | |
| ↑ | ↓ | N/A | Suggestive of primary hypothyroid | 870 | 2.3 | |
| ↑ | - | N/A | Suspicion of subclinical hypothyroid | 3979 | 10.3 | |
| ↑ | ↑ | N/A | R/O TSH dependent hyperthyroid? Or thyroid hormone resistance? | 38 | 0.1 | |
| ↓ | ↓ | N/A | R/O TSH-dependent hypothyroid? | 103 | 0.3 | |
| TSH, Free T4 & Total T3 (n = 20,469) | ↓ | ↑ | ↑ | Suggestive of primary hyperthyroid | 400 | 2.0 |
| ↓ | ↑ | - | Suggestive of primary hyperthyroid | 628 | 3.1 | |
| ↓ | ↑ | ↓ | More clinical information needed a | 15 | 0.1 | |
| ↓ | - | - | Suspicion of subclinical hyperthyroid | 1202 | 5.9 | |
| ↓ | - | ↑ | More clinical information needed a | 65 | 0.3 | |
| ↓ | - | ↓ | More clinical information needed a | 74 | 0.4 | |
| ↓ | ↓ | ↓ | R/O TSH-dependent hypothyroid? | 14 | 0.1 | |
| ↓ | ↓ | - | More clinical information needed a | 58 | 0.3 | |
| ↓ | ↓ | ↑ | More clinical information needed a | 2 | <0.1 | |
| - | - | - | Suggestive of euthyroid | 13,131 | 64.2 | |
| - | ↓ | - | Increased free T4 only | 314 | 1.5 | |
| - | ↑ | - | Decreased free T4 only | 660 | 3.2 | |
| - | - | ↑ | Increased total T3 only | 65 | 0.3 | |
| - | - | ↓ | Decreased total T3 only | 889 | 4.3 | |
| - | ↓ | ↓ | More clinical information needed a | 111 | 0.5 | |
| - | ↑ | ↑ | More clinical information needed a | 3 | 0.0 | |
| - | ↑ | ↓ | More clinical information needed a | 47 | 0.2 | |
| - | ↓ | ↑ | More clinical information needed a | 10 | <0.1 | |
| ↑ | ↓ | ↓ | Suggestive of primary hypothyroid | 171 | 0.8 | |
| ↑ | ↓ | - | More clinical information needed a | 364 | 1.8 | |
| ↑ | ↓ | ↑ | More clinical information needed a | 3 | <0.1 | |
| ↑ | ↑ | ↑ | R/O TSH-dependent hyperthyroid? Or thyroid hormone resistance? | 0 | 0.0 | |
| ↑ | ↑ | - | More clinical information needed a | 15 | 0.1 | |
| ↑ | ↑ | ↓ | More clinical information needed a | 6 | <0.1 | |
| ↑ | - | - | Suspicion of subclinical hypothyroid | 1987 | 9.7 | |
| ↑ | - | ↑ | More clinical information needed a | 7 | <0.1 | |
| ↑ | - | ↓ | Suspicion of hypothyroid/thyroiditis | 228 | 1.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, R.; Lee, S.G.; Lee, E.H. Patient Population and Test Utilization for Thyroid Function in Local Clinics and Hospitals in Korea. Diagnostics 2022, 12, 1638. https://doi.org/10.3390/diagnostics12071638
Choi R, Lee SG, Lee EH. Patient Population and Test Utilization for Thyroid Function in Local Clinics and Hospitals in Korea. Diagnostics. 2022; 12(7):1638. https://doi.org/10.3390/diagnostics12071638
Chicago/Turabian StyleChoi, Rihwa, Sang Gon Lee, and Eun Hee Lee. 2022. "Patient Population and Test Utilization for Thyroid Function in Local Clinics and Hospitals in Korea" Diagnostics 12, no. 7: 1638. https://doi.org/10.3390/diagnostics12071638