
Morphological Parameters of the Hip Joint and Its Relation to Gender, Joint Side and Age—A CT-Based Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
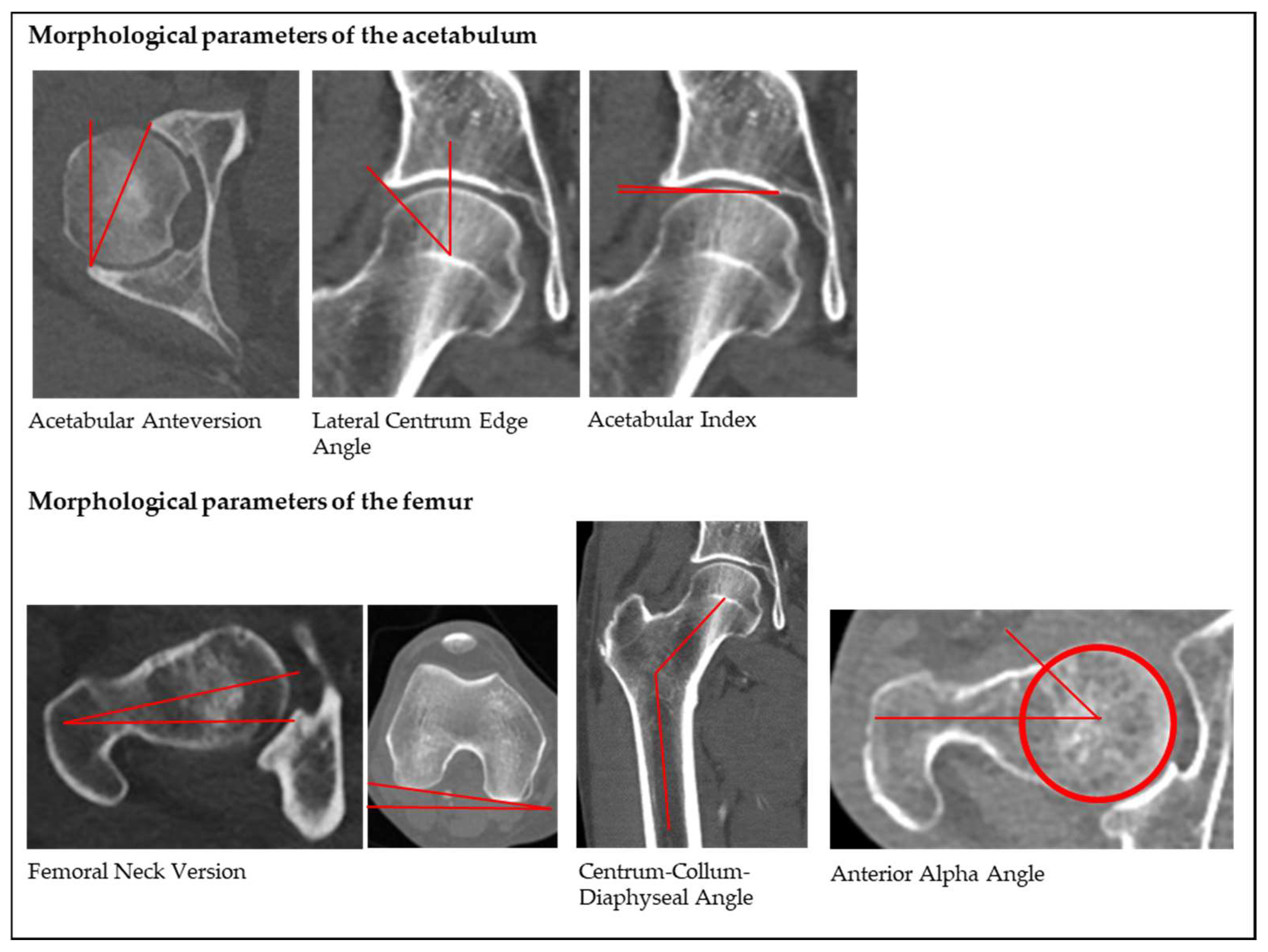
2.2. Radiological Assessment and Parameters
2.3. Age Groups
2.4. Statistical Analysis
3. Results
3.1. Morphological Parameters of the Hip Joint and OA Grade
3.1.1. Acetabular Anteversion (AcetAV)
3.1.2. Lateral Centrum Edge Angle (LCE)
3.1.3. Acetabular Index (AI)
3.1.4. Femoral Neck Version (FNV)
3.1.5. Centrum-Collum-Diaphyseal Angle (CCD)
3.1.6. Anterior Alpha Angle (AαA)
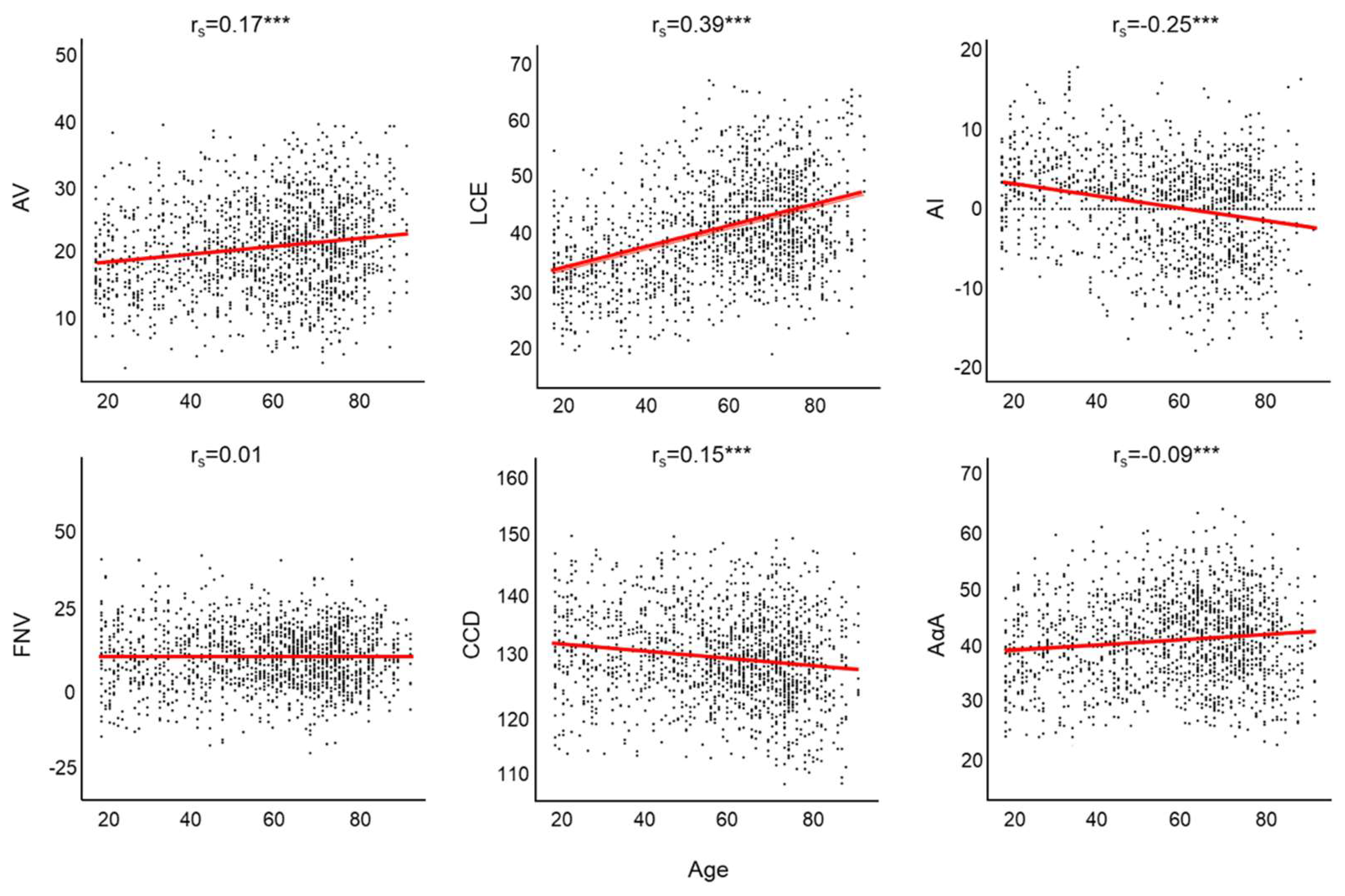
3.2. Association between Age and Alterations of Morphological Parameters of the Hip Joint
3.3. Incidence for Pathological Morphological Parameters of the Hip Joint According to Reference Values of the Literature
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lerch, T.D.; Todorski, I.A.S.; Steppacher, S.D.; Schmaranzer, F.; Werlen, S.F.; Siebenrock, K.A.; Tannast, M. Prevalence of Femoral and Acetabular Version Abnormalities in Patients with Symptomatic Hip Disease: A Controlled Study of 538 Hips. Am. J. Sports Med. 2018, 46, 122–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tschauner, C.; Fock, C.M.; Hofmann, S.; Raith, J. Rotationsfehler des Hüftgelenks [Rotational abnormalities of the hip joint]. Radiologe 2002, 42, 457–466. (In Germany) [Google Scholar] [CrossRef]
- Tönnis, D.; Heinecke, A. Acetabular and femoral anteversion: Relationship with osteoarthritis of the hip. J. Bone Joint Surg Am. 1999, 81, 1747–1770. [Google Scholar] [CrossRef]
- Lee, C.B.; Kim, Y.J. Imaging hip dysplasia in the skeletally mature. Orthop. Clin. N. Am. 2012, 43, 329–342. [Google Scholar] [CrossRef] [PubMed]
- Sankar, W.N.; Matheney, T.H.; Zaltz, I. Femoroacetabular impingement: Current concepts and controversies. Orthop. Clin. N. Am. 2013, 44, 575–589. [Google Scholar] [CrossRef] [PubMed]
- Hetsroni, I.; Dela, T.K.; Duke, G.; Lyman, S.; Kelly, B.T. Sex differences of hip morphology in young adults with hip pain and labral tears. Arthroscopy 2013, 29, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Siebenrock, K.A.; Steppacher, S.D.; Haefeli, P.C.; Schwab, J.M.; Tannast, M. Valgus hip with high antetorsion causes pain through posterior extraarticular FAI. Clin. Orthop. Relat. Res. 2013, 471, 3774–3780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nötzli, H.P.; Wyss, T.F.; Stoecklin, C.H.; Schmid, M.R.; Treiber, K.; Hodler, J. The contour of the femoral head-neck junction as a predictor for the risk of anterior impingement. J. Bone Joint Surg Br. 2002, 84, 556–560. [Google Scholar] [CrossRef]
- Ganz, R.; Leunig, M.; Leunig-Ganz, K.; Harris, W.H. The etiology of osteoarthritis of the hip: An integrated mechanical concept. Clin. Orthop. Relat. Res. 2008, 466, 264–272. [Google Scholar] [CrossRef] [Green Version]
- Clohisy, J.C.; Carlisle, J.C.; Trousdale, R.; Kim, Y.J.; Beaule, P.E.; Morgan, P.; Steger-May, K.; Schoenecker, P.L.; Millis, M. Radiographic evaluation of the hip has limited reliability. Clin. Orthop. Relat. Res. 2009, 467, 666–675. [Google Scholar] [CrossRef] [Green Version]
- Register, B.; Pennock, A.T.; Ho, C.P.; Strickland, C.D.; Lawand, A.; Philippon, M.J. Prevalence of abnormal hip findings in asymptomatic participants: A prospective, blinded study. Am. J. Sports Med. 2012, 40, 2720–2724. [Google Scholar] [CrossRef] [PubMed]
- Blankenstein, T.; Grainger, A.; Dube, B.; Evans, R.; Robinson, P. MRI hip findings in asymptomatic professional rugby players, ballet dancers, and age-matched controls. Clin. Radiol. 2020, 75, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Frank, J.M.; Harris, J.D.; Erickson, B.J.; Slikker, W., 3rd; Bush-Joseph, C.A.; Salata, M.J.; Nho, S.J. Prevalence of Femoroacetabular Impingement Imaging Findings in Asymptomatic Volunteers: A Systematic Review. Arthroscopy 2015, 31, 1199–1204. [Google Scholar] [CrossRef]
- Thier, S.; Gerisch, D.; Weiss, C.; Fickert, S.; Brunner, A. Prevalence of Cam and Pincer Deformities in the X-rays of Asymptomatic Individuals. Biomed. Res. Int. 2017, 2017, 8562329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toogood, P.A.; Skalak, A.; Cooperman, D.R. Proximal femoral anatomy in the normal human population. Clin. Orthop. Relat. Res. 2009, 467, 876–885. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braten, M.; Terjesen, T.; Rossvoll, I. Femoral anteversion in normal adults: Ultrasound measurements in 50 men and 50 women. Acta Orthop. Scand. 1992, 63, 29–32. [Google Scholar] [CrossRef] [Green Version]
- Takeuchi, S.; Goto, H.; Iguchi, H.; Watanabe, N.; Osaga, S.; Murakami, H.; Yoshida, M. Ultrasonographic Assessment of Femoral Torsion Angle Based on Tilting Angles of Femoral Neck and Condylar Axis. Ultrasound Med. Biol. 2019, 45, 1970–1976. [Google Scholar] [CrossRef]
- Nardo, L.; Parimi, N.; Liu, F.; Lee, S.; Jungmann, P.M.; Nevitt, M.C.; Link, T.M.; Lane, N.E. Osteoporotic Fractures in Men (MrOS) Research Group. Femoroacetabular Impingement: Prevalent and Often Asymptomatic in Older Men: The Osteoporotic Fractures in Men Study. Clin. Orthop. Relat. Res. 2015, 473, 2578–2586. [Google Scholar] [CrossRef] [Green Version]
- Wells, J.; Nepple, J.J.; Crook, K.; Ross, J.R.; Bedi, A.; Schoenecker, P.; Clohisy, J.C. Femoral Morphology in the Dysplastic Hip: Three-dimensional Characterizations With CT. Clin. Orthop. Relat. Res. 2017, 475, 1045–1054. [Google Scholar] [CrossRef] [Green Version]
- Fischer, C.S.; Kühn, J.P.; Völzke, H.; Ittermann, T.; Gümbel, D.; Kasch, R.; Haralambiev, L.; Laqua, R.; Hinz, P.; Lange, J. The neck-shaft angle: An update on reference values and associated factors. Acta Orthop. 2020, 91, 53–57. [Google Scholar] [CrossRef] [Green Version]
- Larson, C.M.; Moreau-Gaudry, A.; Kelly, B.T.; Byrd, J.W.; Tonetti, J.; Lavallee, S.; Chabanas, L.; Barrier, G.; Bedi, A. Are normal hips being labeled as pathologic? A CT-based method for defining normal acetabular coverage. Clin. Orthop. Relat. Res. 2015, 473, 1247–1254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stem, E.S.; O’Connor, M.I.; Kransdorf, M.J.; Crook, J. Computed tomography analysis of acetabular anteversion and abduction. Skeletal Radiol. 2006, 35, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Tallroth, K.; Lepistö, J. Computed tomography measurement of acetabular dimensions: Normal values for correction of dysplasia. Acta Orthop. 2006, 77, 598–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dimitriou, D.; Tsai, T.Y.; Yue, B.; Rubash, H.E.; Kwon, Y.M.; Li, G. Side-to-side variation in normal femoral morphology: 3D CT analysis of 122 femurs. Orthop. Traumatol. Surg. Res. 2016, 102, 91–97. [Google Scholar] [CrossRef]
- Croom, W.P.; Lorenzana, D.J.; Auran, R.L.; Cavallero, M.J.; Heckmann, N.; Lee, J.; White, E.A. Is contralateral templating reliable for establishing rotational alignment during intramedullary stabilization of femoral shaft fractures? A study of individual bilateral differences in femoral version. J. Orthop. Trauma 2018, 32, 61–66. [Google Scholar] [CrossRef]
- Laumonerie, P.; Ollivier, M.; LiArno, S.; Faizan, A.; Cavaignac, E.; Argenson, J.N. Which factors influence proximal femoral asymmetry?: A 3D CT analysis of 345 femoral pairs. Bone Joint J. 2018, 100, 839–844. [Google Scholar] [CrossRef]
- Tannast, M.; Hanke, M.S.; Zheng, G.; Steppacher, S.D.; Siebenrock, K.A. What are the radiographic reference values for acetabular under- and overcoverage? Clin. Orthop. Relat. Res. 2015, 473, 1234–1246. [Google Scholar] [CrossRef] [Green Version]
- Sharp, I.K. Acetabular dysplasia, the acetabular angle. J. Bone Joint Surg. Br. 1961, 43, 268–272. [Google Scholar] [CrossRef]
- Murphy, S.B.; Simon, S.R.; Kijewski, P.K.; Wilkinson, R.H.; Griscom, N.T. Femoral anteversion. J. Bone Joint Surg. Am. 1987, 69, 1169–1176. [Google Scholar] [CrossRef]
- Kellgren, J.H.; Lawrence, J.S. Radiological assessment of osteo-arthrosis. Ann. Rheum. Dis. 1957, 16, 494–502. [Google Scholar] [CrossRef] [Green Version]
- Tannenbaum, E.P.; Zhang, P.; Maratt, J.D.; Gombera, M.M.; Holcombe, S.A.; Wang, S.C.; Bedi, A.; Goulet, J.A. A Computed Tomography Study of Gender Differences in Acetabular Version and Morphology: Implications for Femoroacetabular Impingement. Arthroscopy 2015, 31, 1247–1254. [Google Scholar] [CrossRef] [PubMed]
- Buller, L.T.; Rosneck, J.; Monaco, F.M.; Butler, R.; Smith, T.; Barsoum, W.K. Relationship between proximal femoral and acetabular alignment in normal hip joints using 3-dimensional computed tomography. Am. J. Sports Med. 2012, 40, 367–375. [Google Scholar] [CrossRef] [PubMed]
- Miyasaka, D.; Sakai, Y.; Ibuchi, S.; Suzuki, H.; Imai, N.; Endo, N. Sex- and age-specific differences in femoral head coverage and acetabular morphology among healthy subjects-derivation of normal ranges and thresholds for abnormality. Skeletal Radiol. 2017, 46, 523–531. [Google Scholar] [CrossRef] [PubMed]
- Tannast, M.; Siebenrock, K.A.; Anderson, S.E. Femoroacetabular impingement: Radiographic diagnosis—What the radiologist should know. AJR Am. J. Roentgenol. 2007, 188, 1540–1552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartel, M.J.; Petersik, A.; Schmidt, A.; Kendoff, D.; Nüchtern, J.; Rueger, J.M.; Lehmann, W.; Grossterlinden, L.G. Determination of Femoral Neck Angle and Torsion Angle Utilizing a Novel Three-Dimensional Modeling and Analytical Technology Based on CT Datasets. PLoS ONE 2016, 11, e0149480. [Google Scholar] [CrossRef]
- Fuller, C.B.; Farnsworth, C.L.; Bomar, J.D.; Jeffords, M.E.; Murphy, J.S.; Edmonds, E.W.; Pennock, A.T.; Wenger, D.R.; Upasani, V.V. Femoral version: Comparison among advanced imaging methods. J. Orthop. Res. 2018, 36, 1536–1542. [Google Scholar] [CrossRef] [Green Version]
- Sutter, R.; Dietrich, T.J.; Zingg, P.O.; Pfirrmann, C.W. Assessment of Femoral Antetorsion With MRI: Comparison of Oblique Measurements to Standard Transverse Measurements. AJR Am. J. Roentgenol. 2015, 205, 130–135. [Google Scholar] [CrossRef]
- Schmaranzer, F.; Lerch, T.D.; Siebenrock, K.A.; Tannast, M.; Steppacher, S.D. Differences in Femoral Torsion Among Various Measurement Methods Increase in Hips With Excessive Femoral Torsion. Clin. Orthop. Relat. Res. 2019, 477, 1073–1083. [Google Scholar] [CrossRef]
- Sutter, R.; Dietrich, T.J.; Zingg, P.O.; Pfirrmann, C.W. Femoral antetorsion: Comparing asymptomatic volunteers and patients with femoroacetabular impingement. Radiology 2012, 263, 475–483. [Google Scholar] [CrossRef] [Green Version]
- Jiang, N.; Peng, L.; Al-Qwbani, M.; Xie, G.P.; Yang, Q.M.; Chai, Y.; Zhang, Q.; Yu, B. Femoral version, neck-shaft angle, and acetabular anteversion in Chinese Han population: A retrospective analysis of 466 healthy adults. Medicine (Baltim.) 2015, 94, e891. [Google Scholar] [CrossRef]
- Boese, C.K.; Dargel, J.; Oppermann, J.; Eysel, P.; Scheyerer, M.J.; Bredow, J.; Lechler, P. The femoral neck-shaft angle on plain radiographs: A systematic review. Skeletal Radiol. 2016, 45, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Boese, C.K.; Frink, M.; Jostmeier, J.; Haneder, S.; Dargel, J.; Eysel, P.; Lechler, P. The Modified Femoral Neck-Shaft Angle: Age- and Sex-Dependent Reference Values and Reliability Analysis. Biomed. Res. Int. 2016, 2016, 8645027. [Google Scholar] [CrossRef] [PubMed]
- Gilligan, I.; Chandraphak, S.; Mahakkanukrauh, P. Femoral neck-shaft angle in humans: Variation relating to climate, clothing, lifestyle, sex, age and side. J. Anat. 2013, 223, 133–151. [Google Scholar] [CrossRef] [PubMed]
- Hack, K.; Di Primio, G.; Rakhra, K.; Beaulé, P.E. Prevalence of cam-type femoroacetabular impingement morphology in asymptomatic volunteers. J. Bone Joint Surg. Am. 2010, 92, 2436–2444. [Google Scholar] [CrossRef]
- Laborie, L.B.; Lehmann, T.G.; Engesæter, I.Ø.; Sera, F.; Engesæter, L.B.; Rosendahl, K. The alpha angle in cam-type femoroacetabular impingement: New reference intervals based on 2038 healthy young adults. Bone Joint J. 2014, 96, 449–454. [Google Scholar] [CrossRef] [Green Version]
- Gollwitzer, H.; Suren, C.; Strüwind, C.; Gottschling, H.; Schröder, M.; Gerdesmeyer, L.; Prodinger, P.M.; Burgkart, R. The natural alpha angle of the femoral head-neck junction: A cross-sectional CT study in 1312 femurs. Bone Joint J. 2018, 100, 570–578. [Google Scholar] [CrossRef]
- Gosvig, K.K.; Jacobsen, S.; Sonne-Holm, S.; Gebuhr, P. The prevalence of cam-type deformity of the hip joint: A survey of 4151 subjects of the Copenhagen Osteoarthritis Study. Acta Radiol. 2008, 49, 436–441. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Joint Side | Pathology | Parameter | Study |
|---|---|---|---|
| Acetabular | Acetabular retroversion | AcetAV < 10° | Tönnis D.; Heinecke A. 1999 [3] |
| Acetabular dysplasia | LCE < 20° | Tschauner et al., 2002 [2] | |
| Borderline dysplasia | LCE 20–25° | Lee et al., 2012 [4] | |
| Acetabular overcoverage | LCE > 40°; AI < 0° | Lee et al., 2012 [4] | |
| Femoral | Femoral CAM deformity | AαA > 55° | Nötzli et al., 2002 [8] |
| Coxa vara | CCD < 125° | Tönnis D.; Heinecke A. 1999 [3] | |
| Coxa retrotorta | FNV < 0° | Hetsroni et al., 2013 [6] | |
| Coxa valga et antetorta | CCD > 135° + FNV > 25° | Siebenrock et al., 2013 [7] |
| Total (n = 1.576) | Left (n = 788) | Right (n = 788) | p-Value | Female (n = 514) | Male (n = 1062) | p-Value | |
|---|---|---|---|---|---|---|---|
| AcetAV | 20.5° (±6.9) | 19.9° (±6.5) | 21.1° (±7.2) | 0.001 | 23.3° (±6.8) | 19.2° (±6.5) | <0.0001 |
| LCE | 40.8° (±8.8) | 42.6° (±8.6) | 38.9° (±8.6) | <0.001 | 41.8° (±9.4) | 40.3° (±8.4) | 0.003 |
| AI | 0.3° (±5.6) | 0.5° (±5.4) | 0.1° (±5.8) | 0.58 | 0.4° (±6.1) | 0.2° (±5.3) | 0.37 |
| FNV | 11.0° (±9.8) | 11.4° (±9.5) | 10.6° (±10.0) | 0.14 | 13.7° (±10.1) | 9.7° (±9.3) | <0.0001 |
| CCD | 129.9° (±7.4) | 131.5° (±7.2) | 128.2° (±7.2) | <0.001 | 129.1° (±7.8) | 130.3° (±7.2) | 0.006 |
| AαA | 41.2° (±7.7) | 39.2° (±7.4) | 43.1° (±7.5) | <0.001 | 39.5° (±7.3) | 42.0° (±7.8) | <0.0001 |
| Total (n = 1.576) | Q1: <45 (n = 390) | Q2: 45–62.9 (n = 358) | Q3: 63–72.9 (n = 406) | Q4: >73 (n = 422) | p-Value | |
|---|---|---|---|---|---|---|
| AcetAV | 20.5° (±6.9) | 19.0° (±6.4) | 20.3° (±6.6) | 21.1° (±7.2) | 21.8° (±7.0) | <0.001 |
| LCE | 40.8° (±8.8) | 35.1° (±7.6) | 41.8° (±8.6) | 43.0° (±7.8) | 43.6° (±8.5) | <0.001 |
| AI | 0.3° (±5.6) | 2.6° (±5.4) | 0.0° (±5.6) | −1.2° (±5.5) | −0.5° (±5.2) | <0.001 |
| FNV | 11.0° (±9.8) | 10.8° (±11.6) | 11.5° (±9.3) | 10.5° (±9.1) | 11.1° (±8.7) | 0.48 |
| CCD | 129.9° (±7.4) | 131.4° (±7.4) | 130.4° (±6.9) | 129.8° (±7.0) | 127.9° (±7.8) | <0.001 |
| AαA | 41.2° (±7.7) | 39.2° (±7.5) | 42.8° (±7.3) | 42.0° (±8.1) | 40.7° (±7.6) | <0.001 |
| Acetabular | ||||
|---|---|---|---|---|
| Pathology: | Retroversion [3] | Dysplasia [2] | Borderline [4] | Overcoverage [4] |
| Parameter: | AcetAV < 10° | LCE < 20° | LCE 20–25° | LCE > 40°; AI < 0 |
| Total in %: | 5.5% | 0.3% | 0.3% | 24.2% |
| Age < 45 years in %: | 5.2% | 0.5% | 0.7% | 12.8% |
| Age > 45 years in %: | 5.6% | 0.3% | 0.1% | 28.1% |
| femoral | ||||
| Pathology: | CAM [8] | Coxa vara [3] | Coxa retrotorta [6] | Coxa valga et antetorta [7] |
| Parameter: | AαA > 55° | CCD < 125° | FNV < 0° | CCD > 135° FNV > 25° |
| Total in %: | 3.4% | 24.4% | 11.5% | 1.5% |
| Age < 45 years in %: | 2.2% | 18.7% | 16.5% | 3.2% |
| Age > 45 years in %: | 3.8% | 26.4% | 9.7% | 0.9% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hawellek, T.; Meier, M.-P.; Seitz, M.-T.; Uhlig, J.; Hosseini, A.S.A.; Beil, F.T.; Lehmann, W.; Hubert, J. Morphological Parameters of the Hip Joint and Its Relation to Gender, Joint Side and Age—A CT-Based Study. Diagnostics 2022, 12, 1774. https://doi.org/10.3390/diagnostics12081774
Hawellek T, Meier M-P, Seitz M-T, Uhlig J, Hosseini ASA, Beil FT, Lehmann W, Hubert J. Morphological Parameters of the Hip Joint and Its Relation to Gender, Joint Side and Age—A CT-Based Study. Diagnostics. 2022; 12(8):1774. https://doi.org/10.3390/diagnostics12081774
Chicago/Turabian StyleHawellek, Thelonius, Marc-Pascal Meier, Mark-Tilman Seitz, Johannes Uhlig, Ali Seif Amir Hosseini, Frank Timo Beil, Wolfgang Lehmann, and Jan Hubert. 2022. "Morphological Parameters of the Hip Joint and Its Relation to Gender, Joint Side and Age—A CT-Based Study" Diagnostics 12, no. 8: 1774. https://doi.org/10.3390/diagnostics12081774