
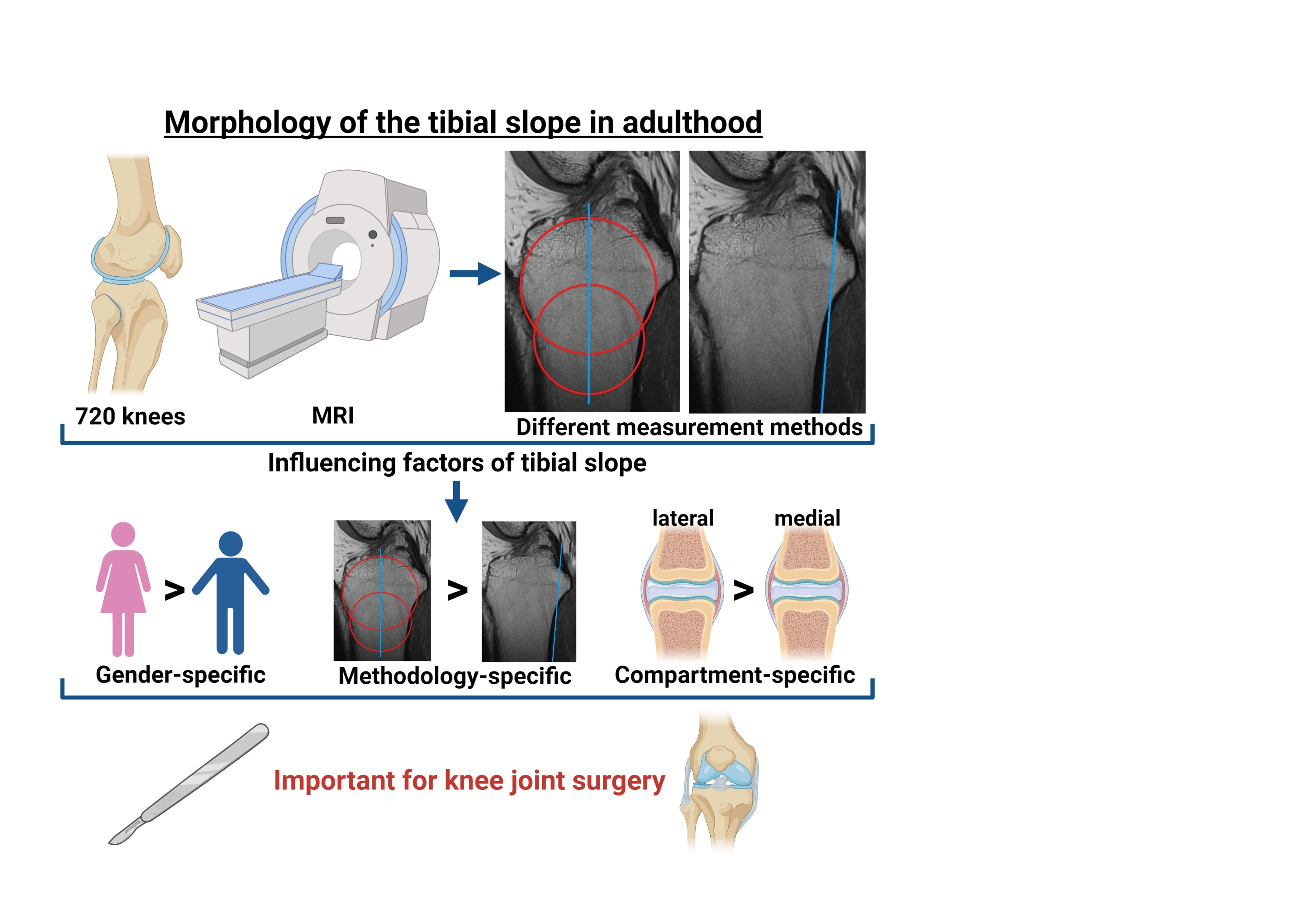
Morphological Analysis of the Tibial Slope in 720 Adult Knee Joints

 , ,
, ,  ,
,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Inclusion Criteria
2.3. Exclusion Criteria
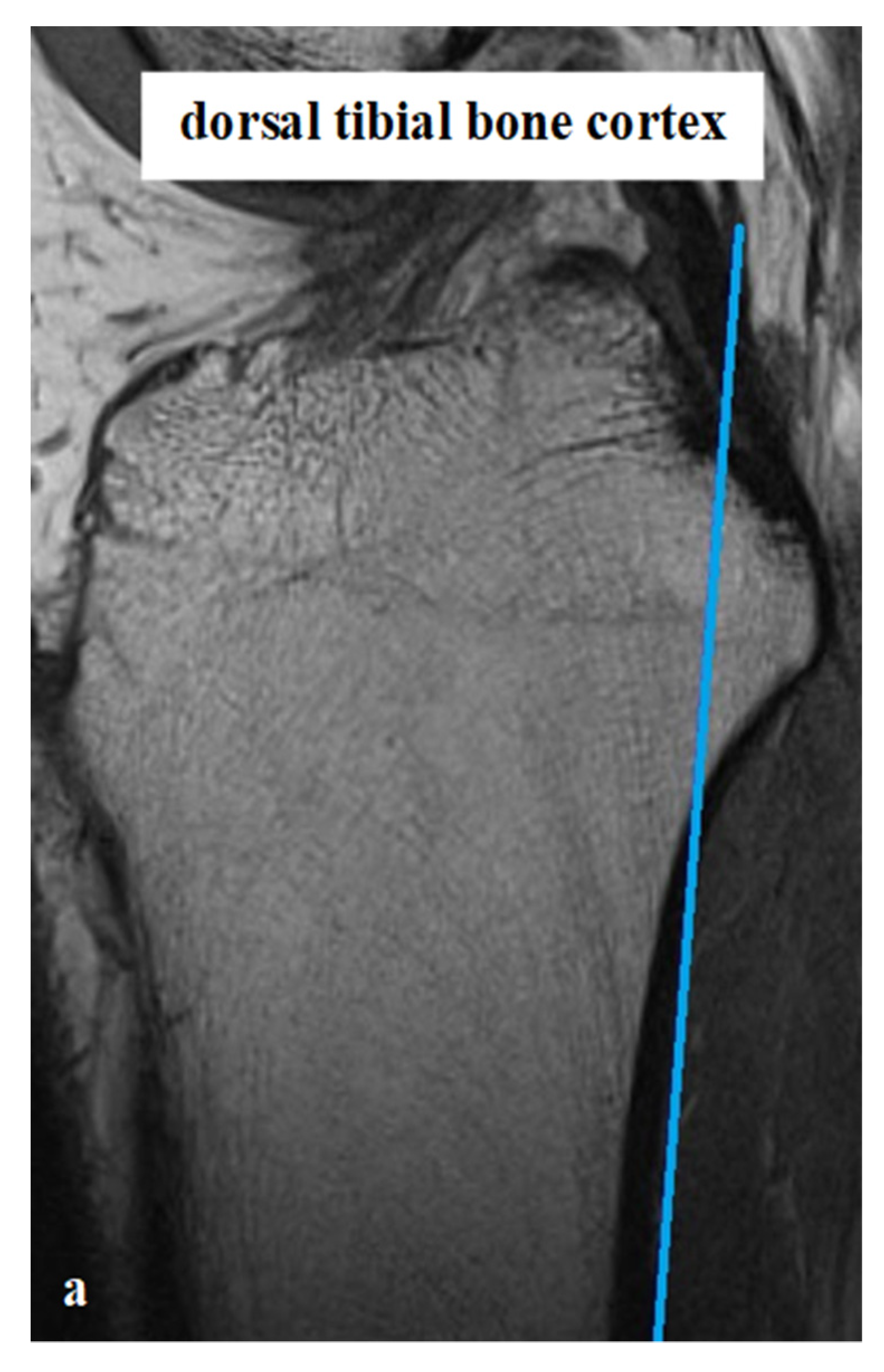
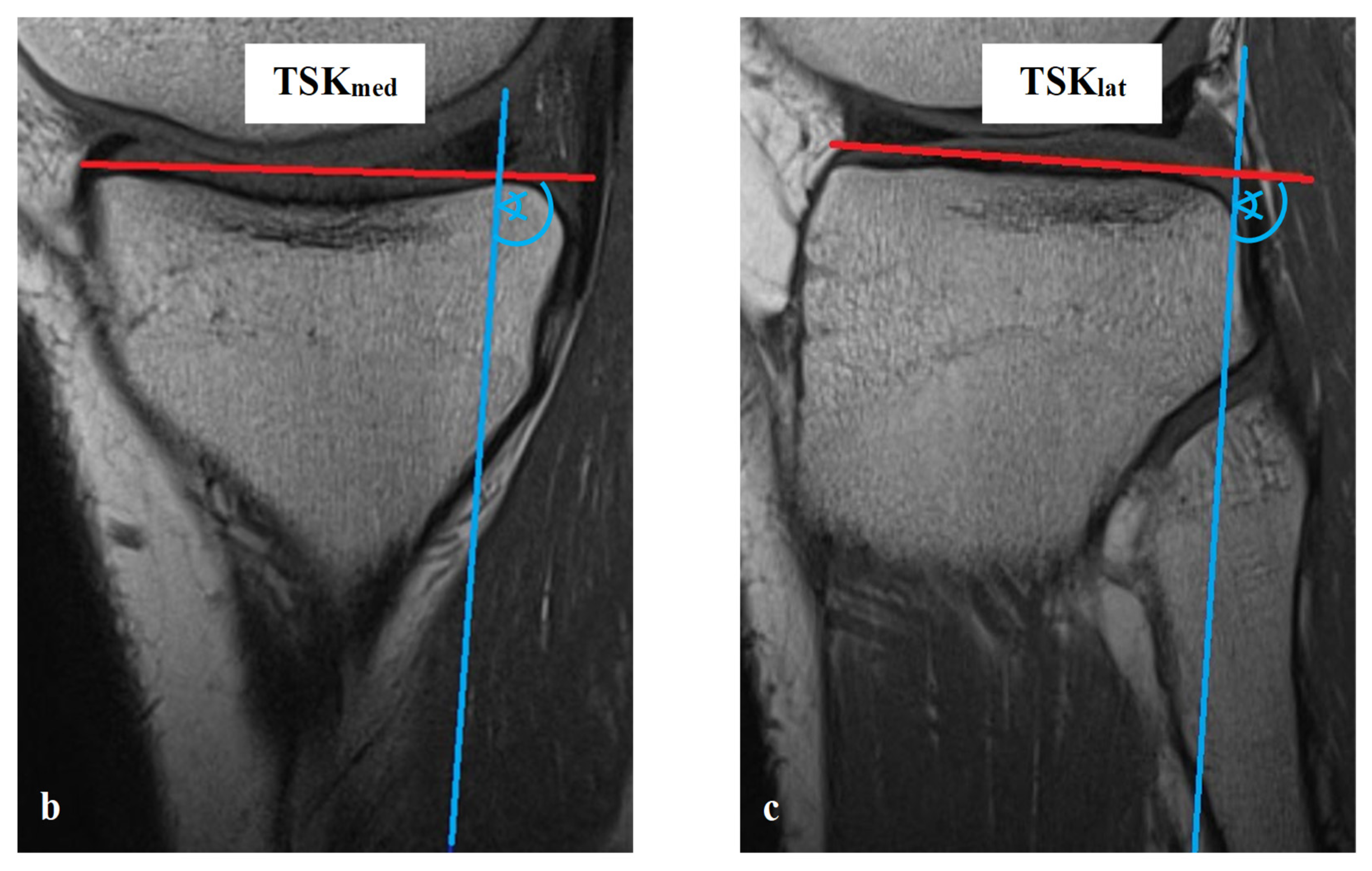
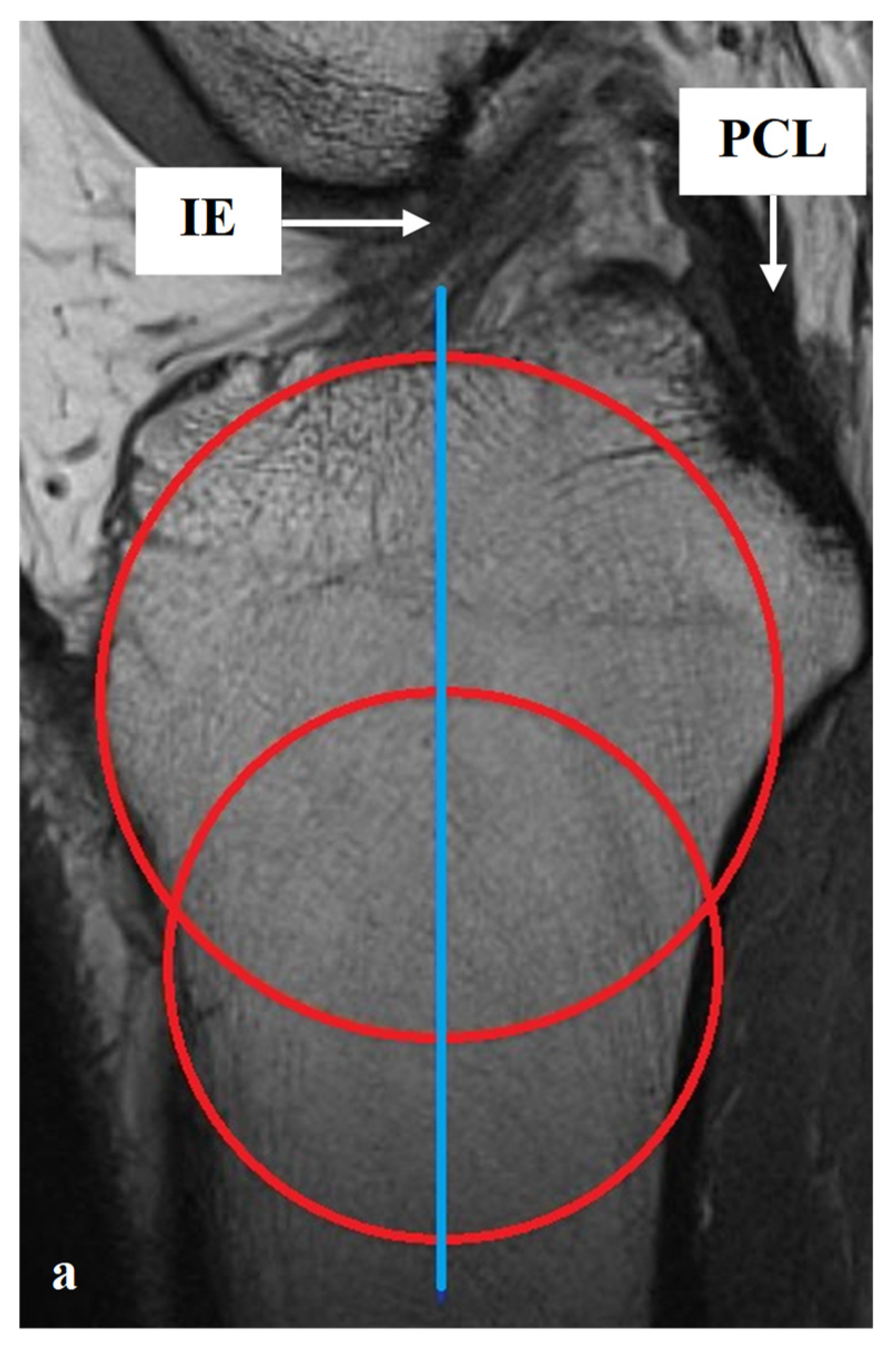
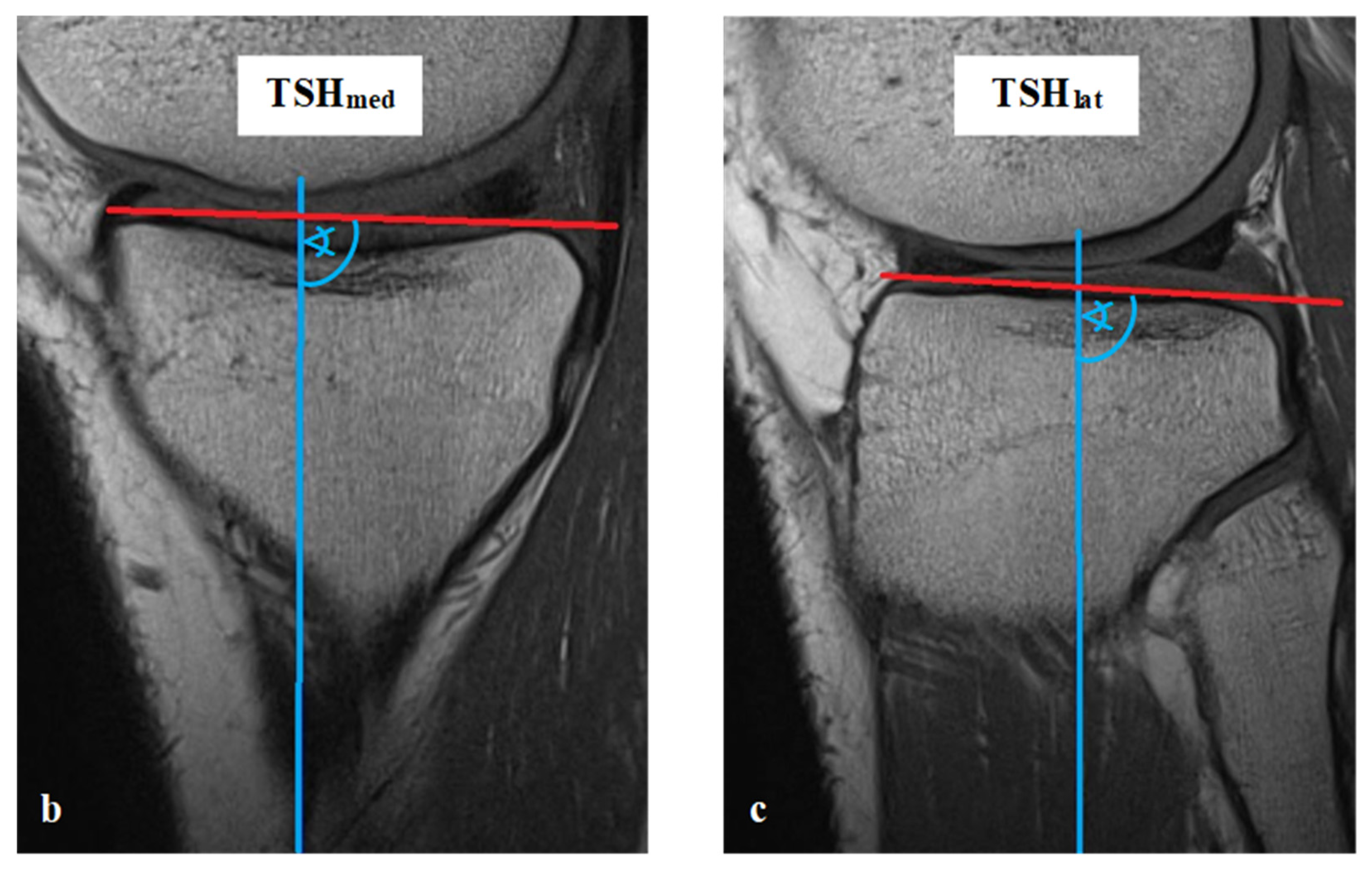
2.4. MRI Analysis, Parameters and Methods of Measurement
2.5. Statistics
3. Results
3.1. Characteristics of the Study Population
3.2. Differences between TSK and TSH
3.3. Differences between Medial and Lateral Knee-Joint Surface
3.4. Analysis of Gender Specific Differences
3.5. Analysis of Side Specific Differences
3.6. Comparison of HKJ and PKJ
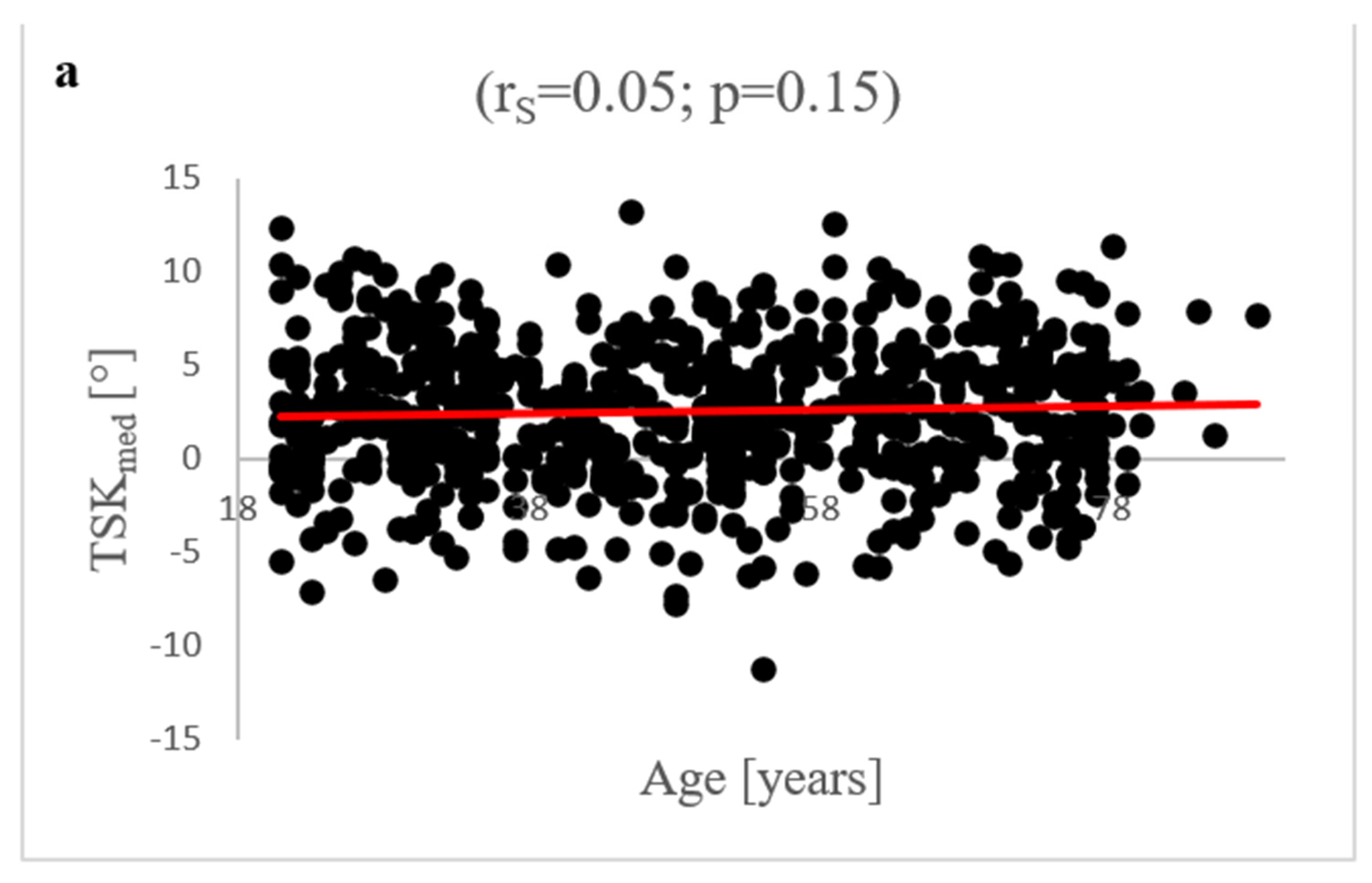
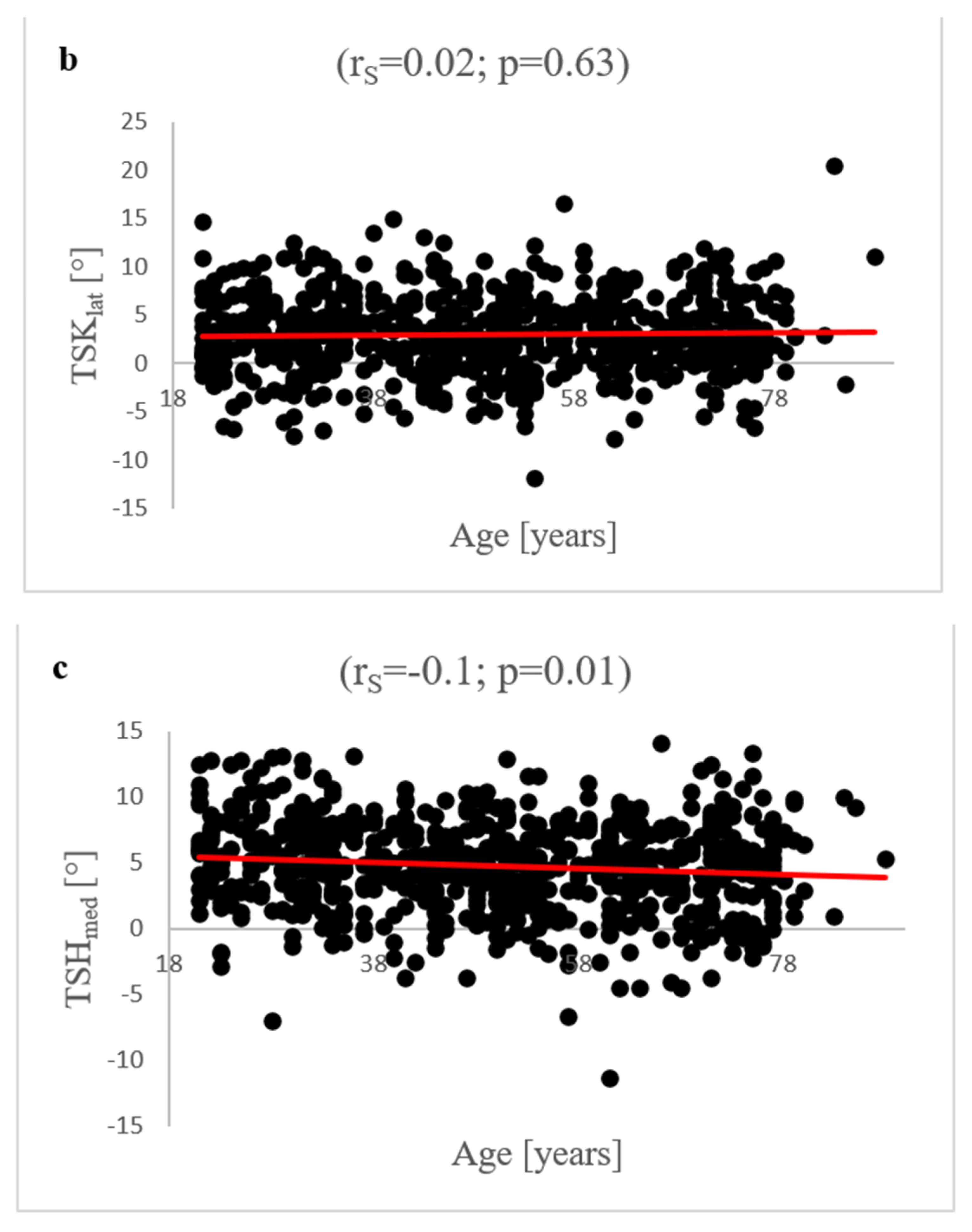
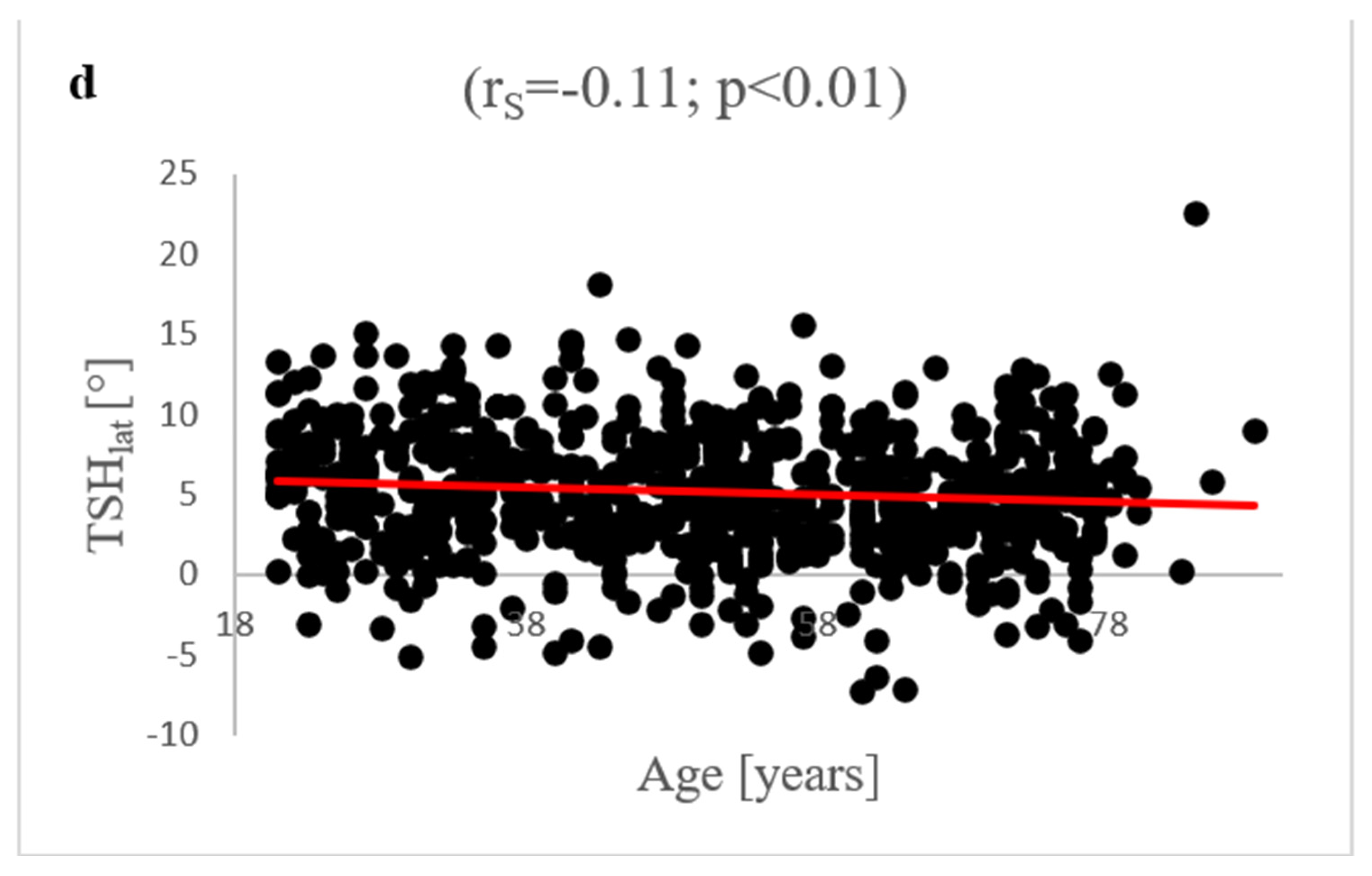
3.7. Age-Dependent Correlation Analysis of TS Parameters
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cerveri, P.; Belfatto, A.; Manzotti, A. Representative 3D shape of the distal femur, modes of variation and relationship with abnormality of the trochlear region. J. Biomech. 2019, 94, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Macri, E.M.; Neogi, T.; Tolstykh, I.; Widjajahakim, R.; Lewis, C.E.; Torner, J.C.; Nevitt, M.C.; Roux, M.; Stefanik, J.J. Relation of Patellofemoral Joint Alignment, Morphology, and Radiographic Osteoarthritis to Frequent Anterior Knee Pain: Data from the Multicenter Osteoarthritis Study. Arthritis Care Res. 2020, 72, 1066–1073. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.K.; Phillips, M.; Bhandari, M.; Watson, J.; Malhotra, R. What Differences in Morphologic Features of the Knee Exist Among Patients of Various Races? A Systematic Review. Clin. Orthop. Relat. Res. 2017, 475, 170–182. [Google Scholar] [CrossRef] [Green Version]
- Duren, D.L.; Sherwood, R.J.; Czerwinski, S.A.; Chumlea, W.C.; Lee, M.; Demerath, E.W.; Sun, S.S.; Siervogel, R.M.; Towne, B. Genetic Architecture of Knee Radiographic Joint Space in Healthy Young Adults. Hum. Biol. 2008, 80, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Gwinner, C.; Weiler, A.; Plachel, F. Normalwerte—Wie bestimme ich den tibialen Slope richtig? Arthroskopie 2021, 34, 10–13. [Google Scholar] [CrossRef]
- Hinterwimmer, S.; Feucht, M. Biomechanik der Sagittalebene des Kniegelenks. Arthroskopie 2021, 34, 2–9. [Google Scholar] [CrossRef]
- Pangaud, C.; Laumonerie, P.; Dagneaux, L.; LiArno, S.; Wellings, P.; Faizan, A.; Sharma, A.; Ollivier, M. Measurement of the Posterior Tibial Slope Depends on Ethnicity, Sex, and Lower Limb Alignment: A Computed Tomography Analysis of 378 Healthy Participants. Orthop. J. Sports Med. 2020, 8, 2325967119895258. [Google Scholar] [CrossRef] [Green Version]
- Plachel, F.; Kirschbaum, S.; Perka, C.F.; Gwinner, C. Stellenwert des tibialen Slopes in der primären Knietotalendoprothetik. Arthroskopie 2021, 34, 54–58. [Google Scholar] [CrossRef]
- De Boer, J.J.; Blankevoort, L.; Kingma, I.; Vorster, W. In vitro study of inter-individual variation in posterior slope in the knee joint. Clin. Biomech. 2009, 24, 488–492. [Google Scholar] [CrossRef]
- Dejour, H.; Bonnin, M. Tibial translation after anterior cruciate ligament rupture. Two radiological tests compared. J. Bone Jt. Surg. Br. Vol. 1994, 76, 745–749. [Google Scholar] [CrossRef]
- Marriott, K.; Birmingham, T.B.; Kean, C.O.; Hui, C.; Jenkyn, T.R.; Giffin, J.R. Five-year changes in gait biomechanics after concomitant high tibial osteotomy and ACL reconstruction in patients with medial knee osteoarthritis. Am. J. Sports Med. 2015, 43, 2277–2285. [Google Scholar] [CrossRef] [PubMed]
- Dickschas, J. Korrekturosteotomie bei posttraumatischen Slope-Veränderungen. Arthroskopie 2021, 34, 33–44. [Google Scholar] [CrossRef]
- Webb, J.M.; Salmon, L.J.; Leclerc, E.; Pinczewski, L.A.; Roe, J.P. Posterior tibial slope and further anterior cruciate ligament injuries in the anterior cruciate ligament-reconstructed patient. Am. J. Sports Med. 2013, 41, 2800–2804. [Google Scholar] [CrossRef] [PubMed]
- El-Azab, H.; Glabgly, P.; Paul, J.; Imhoff, A.B.; Hinterwimmer, S. Patellar height and posterior tibial slope after open- and closed-wedge high tibial osteotomy: A radiological study on 100 patients. Am. J. Sports Med. 2010, 38, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Veizi, E.; Firat, A.; Tecimel, O.; Cepni, S.; Subasi, I.Ö.; Kilcarslan, K. The Change in Posterior Tibial Slope after Cementless Unicondylar Knee Arthroplasty. J. Arthroplast. 2021, 36, 1784–1791. [Google Scholar] [CrossRef] [PubMed]
- Barrett, W.P.; Mason, J.B.; Moskal, J.T.; Dalury, D.F.; Oliashirazi, A.; Fisher, D.A. Comparison of radiographic alignment of imageless computer-assisted surgery vs conventional instrumentation in primary total knee arthroplasty. J. Arthroplast. 2011, 26, 1273–1284. [Google Scholar] [CrossRef] [PubMed]
- Todd, M.M.S.; Lalliss, M.S.; Garcia, E.S.; DeBerardino, T.; Cameron, K.L. The relationship between posterior tibial slope and anterior cruciate ligament injuries. Am. J. Sports Med. 2010, 38, 63–67. [Google Scholar] [CrossRef]
- Brandon, M.L.; Haynes, P.T.; Bonamo, J.R.; Flynn, M.I.; Barrett, G.R.; Sherman, M.F. The association between posterior-inferior tibial slope and anterior cruciate ligament insufficiency. Arthroscopy 2006, 22, 894–899. [Google Scholar] [CrossRef]
- Jenny, J.Y. The stability of the cemented tibial component of total knee arthroplasty: Posterior cruciate-retaining versus posterior-stabilized design. J. Arthroplast. 2005, 20, 406. [Google Scholar] [CrossRef]
- Singh, G.; Tan, J.H.; Sng, B.Y.; Awiszus, F.; Lohmann, C.H.; Nathan, S.S. Restoring the anatomical tibial slope and limb axis may maximise post-operative flexion in posterior-stabilised total knee replacements. Bone Jt. J. 2013, 95, 1354–1358. [Google Scholar] [CrossRef]
- Kim, K.-H.; Bin, S.-I.; Kim, J.-M. The Correlation between Posterior Tibial Slope and Maximal Angle of Flexion after Total Knee Arthroplasty. Knee Surg. Relat. Res. 2012, 24, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Utzschneider, S.; Goettinger, M.; Weber, P.; Horng, A.; Glaser, C.; Jansson, V.; Müller, P.E. Development and validation of a new method for the radiologic measurement of the tibial slope. Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 1643–1648. [Google Scholar] [CrossRef] [PubMed]
- Koh, Y.-G.; Nam, J.-H.; Chung, H.-S.; Kim, H.-J.; Chun, H.-J.; Kang, K.-T. Gender differences in morphology exist in posterior condylar offsets of the knee in Korean population. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 1628–1634. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Cavaignac, E.; Xu, W.; Cheng, Q.; Telmon, N.; Huang, W. Morphometric evaluation of the knee in Chinese population reveals sexual dimorphism and age-related differences. Int. Orthop. 2018, 42, 2349–2356. [Google Scholar] [CrossRef]
- Pinskerova, V.; Nemec, K.; Landor, I. Gender differences in the morphology of the trochlea and the distal femur. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 2342–2349. [Google Scholar] [CrossRef]
- Gwinner, C.; Fuchs, M.; Sentuerk, U.; Perka, C.F.; Walter, T.C.; Schatka, I.; Rogasch, J.M.M. Assessment of the tibial slope is highly dependent on the type and accuracy of the preceding acquisition. Arch. Orthop. Trauma. Surg. 2019, 139, 1691–1697. [Google Scholar] [CrossRef]
- Hoch, A.; Jud, L.; Roth, T.; Vlachopoulos, L.; Fürnstahl, P.; Fucentese, S.F. A real 3D measurement technique for the tibial slope: Differentiation between different articular surfaces and comparison to radiographic slope measurement. BMC Musculoskelet. Disord. 2020, 26, 635. [Google Scholar] [CrossRef]
- Faschingbauer, M.; Sgroi, M.; Juchems, M.; Reichel, H.; Kappe, T. Can the tibial slope be measured on lateral knee radiographs? Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 3163–3167. [Google Scholar] [CrossRef]
- Haddad, B.; Konan, S.; Mannan, K.; Scott, G. Evaluation of the posterior tibial slope on MR images in different population groups using the tibial proximal anatomical axis. Acta Orthop. Belg. 2012, 78, 757–763. [Google Scholar]
- Amirtharaj, M.J.; Hardy, B.M.; Kent, R.N.; Nawabi, D.H.; Wickiewicz, T.L.; Pearle, A.D.; Imhauser, C.W. Automated, accurate, and three-dimensional method for calculating sagittal slope of the tibial plateau. J. Biomech. 2018, 79, 212–217. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, Y.; Qiang, M.; Zhang, K.; Li, H.; Jiang, Y.; Jia, X. Comparison between three-dimensional CT and conventional radiography in proximal tibia morphology. Medicine 2018, 97, e11632. [Google Scholar] [CrossRef] [PubMed]
- Ho, J.P.Y.; Merican, A.M.; Hashim, M.S.; Abbas, A.A.; Chan, C.K.; Mohamad, J.A. Three-Dimensional Computed Tomography Analysis of the Posterior Tibial Slope in 100 Knees. J. Arthroplast. 2017, 32, 3176–3183. [Google Scholar] [CrossRef] [PubMed]
- Amerinatanzi, A.; Summers, R.K.; Ahmadi, K.; Goel, V.K.; Hewett, T.E.; Nyman, E. Automated Measurement of Patient-Specific Tibial Slopes from MRI. Bioengineering 2017, 4, 69. [Google Scholar] [CrossRef] [PubMed]
- Amerinatanzi, A.; Summers, R.; Ahmadi, K.; Goel, V.K.; Hewett, T.E.; Nyman, E. A novel 3D approach for determination of frontal and coronal plane tibial slopes from MR imaging. Knee 2017, 24, 207–216. [Google Scholar] [CrossRef] [Green Version]
- Saxena, V.; Anari, J.B.; Ruutiainen, A.T.; Voleti, P.B.; Stephenson, J.W.; Lee, G.-C. Tibial component considerations in bicruciate-retaining total knee arthroplasty: A 3D MRI evaluation of proximal tibial anatomy. Knee 2016, 23, 593–599. [Google Scholar] [CrossRef]
- Weinberg, D.S.; Williamson, D.F.K.; Gebhart, J.J.; Knapik, D.M.; Voos, J.E. Differences in Medial and Lateral Posterior Tibial Slope: An Osteological Review of 1090 Tibiae Comparing Age, Sex, and Race. Am. J. Sports Med. 2017, 45, 106–113. [Google Scholar] [CrossRef]
- Karimi, E.; Norouzian, M.; Birjandinejad, A.; Zandi, R.; Makhmalbaf, H. Measurement of Posterior Tibial Slope Using Magnetic Resonance Imaging. Arch. Bone Jt. Surg. 2017, 5, 435–439. [Google Scholar]
- Hudek, R.; Schmutz, S.; Regenfelder, F.; Fuchs, B.; Koch, P.P. Novel measurement technique of the tibial slope on conventional MRI. Clin. Orthop. Relat. Res. 2009, 467, 2066–2072. [Google Scholar] [CrossRef] [Green Version]
- Kellgren, J.H.; Lawrence, J.S. Radiological assessment of osteo-arthrosis. Ann. Rheum. Dis. 1957, 16, 494–502. [Google Scholar] [CrossRef] [Green Version]
- Naendrup, J.-H.; Drouven, S.F.; Shaikh, H.S.; Jaecker, V.; Offerhaus, C.; Shafizadeh, S.T.; Pfeiffer, T.R. High variability of tibial slope measurement methods in daily clinical practice: Comparisons between measurements on lateral radiograph, magnetic resonance imaging, and computed tomography. Knee 2020, 27, 923–929. [Google Scholar] [CrossRef]
- Marouane, H.; Shirazi-Adl, A.; Hashemi, J. Quantification of the role of tibial posterior slope in knee joint mechanics and ACL force in simulated gait. J. Biomech. 2015, 48, 1899–1905. [Google Scholar] [CrossRef] [PubMed]
- Jahn, R.; Cooper, J.D.; Juhan, T.; Kang, H.P.; Bolia, I.K.; Gamradt, S.C.; Hatch, G.F.; Weber, A.E. Reliability of Plain Radiographs Versus Magnetic Resonance Imaging to Measure Tibial Slope in Sports Medicine Patients: Can They Be Used Interchangeably? Orthop. J. Sports Med. 2021, 9, 23259671211033882. [Google Scholar] [CrossRef] [PubMed]
- Ni, Q.-K.; Song, G.-Y.; Zhang, Z.-J.; Zheng, T.; Cao, Y.-W.; Zhang, H. Posterior tibial slope measurements based on the full-length tibial anatomic axis are significantly increased compared to those based on the half-length tibial anatomic axis. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 1362–1368. [Google Scholar] [CrossRef] [PubMed]
- Bao, L.; Rong, S.; Shi, Z.; Wang, J.; Zhang, Y. Measurement of femoral posterior condylar offset and posterior tibial slope in normal knees based on 3D reconstruction. BMC Musculoskelet. Disord. 2021, 22, 486. [Google Scholar] [CrossRef] [PubMed]
- Wittenberg, S.; Sentuerk, U.; Renner, L.; Weynandt, C.; Perka, C.F.; Gwinner, C. Bedeutung des tibialen Slopes in der Knieendoprothetik. Orthopäde 2019, 49, 10–17. [Google Scholar] [CrossRef]
- Bernhardson, A.S.; DePhillipo, N.N.; Daney, B.T.; Kennedy, M.I.; Aman, Z.S.; LaPrade, R.F. Posterior Tibial Slope and Risk of Posterior Cruciate Ligament Injury. Am. J. Sports Med. 2019, 47, 312–317. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TSK (n = 720) | TSH (n = 720) | p-Value | ||
|---|---|---|---|---|
| medial | [°] | 2.6 (±3.7) | 4.8 (±3.5) | <0.001 ***1 |
| lateral | [°] | 3.0 (±4.0) | 5.2 (±3.9) | <0.001 ***1 |
| medial (n = 720) | lateral (n = 720) | p-value | ||
| TSK | [°] | 2.6 (±3.7) | 3.0 (±4.0) | <0.001 ***2 |
| TSH | [°] | 4.8 (±3.5) | 5.2 (±3.9) | 0.002 **2 |
| Males (n = 360) | Females (n = 360) | p-Value | ||
|---|---|---|---|---|
| TSKmed | [°] | 2.0 (±3.9) | 3.2 (±3.4) | <0.001 ***1 |
| TSKlat | [°] | 2.5 (±3.9) | 3.6 (±3.9) | <0.001 ***1 |
| TSHmed | [°] | 4.0 (±3.4) | 5.6 (±3.4) | <0.001 ***1 |
| TSHlat | [°] | 4.4 (±3.8) | 6.0 (±3.8) | <0.001 ***1 |
| left (n = 360) | right (n = 360) | p-value | ||
| TSKmed | [°] | 2.6 (±3.7) | 2.6 (±3.7) | 0.815 1 |
| TSKlat | [°] | 3.0 (±3.8) | 3.0 (±4.1) | 0.920 1 |
| TSHmed | [°] | 4.8 (±3.5) | 4.8 (±3.4) | 0.837 1 |
| TSHlat | [°] | 5.2 (±3.8) | 5.1 (±4.0) | 0.335 1 |
| HKJ (n = 409) | PKJ (n = 311) | p-value | ||
| TSKmed | [°] | 2.6 (±3.7) | 2.6 (±3.7) | 0.693 1 |
| TSKlat | [°] | 2.8 (±3.9) | 3.4 (±4.0) | 0.032 *1 |
| TSHmed | [°] | 4.8 (±3.5) | 4.8 (±3.5) | 0.885 1 |
| TSHlat | [°] | 4.9 (±3.9) | 5.5 (±3.9) | 0.091 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meier, M.-P.; Hochrein, Y.; Saul, D.; Seitz, M.-T.; Klockner, F.S.; Lehmann, W.; Hawellek, T. Morphological Analysis of the Tibial Slope in 720 Adult Knee Joints. Diagnostics 2022, 12, 1346. https://doi.org/10.3390/diagnostics12061346
Meier M-P, Hochrein Y, Saul D, Seitz M-T, Klockner FS, Lehmann W, Hawellek T. Morphological Analysis of the Tibial Slope in 720 Adult Knee Joints. Diagnostics. 2022; 12(6):1346. https://doi.org/10.3390/diagnostics12061346
Chicago/Turabian StyleMeier, Marc-Pascal, Yara Hochrein, Dominik Saul, Mark-Tilmann Seitz, Friederike Sophie Klockner, Wolfgang Lehmann, and Thelonius Hawellek. 2022. "Morphological Analysis of the Tibial Slope in 720 Adult Knee Joints" Diagnostics 12, no. 6: 1346. https://doi.org/10.3390/diagnostics12061346