1. Introduction
Since the establishment of artificial respiration, the technique of lung isolation began to develop around the early 1900s, mainly to prevent infected secretions from one side of the lung cross contaminating the other lung [
1]. Nowadays, in thoracic surgery, lung isolation has become an essential or standard procedure for most patients. Lung isolation has not only facilitated the protective purpose but has also made one lung ventilation possible. The one lung ventilation technique allows the controlled collapse of the operative lung facilitating surgical access into the thoracic and mediastinal area [
2]. Specially designed equipment, such as single lumen endotracheal tubes (SLTs), bronchial blockers (BBs), or double lumen endotracheal tubes (DLTs), can all be used to achieve lung isolation, however DLTs eventually became the most popular choice among anesthesiologists, primarily because they are easier and quicker to place [
3].
The concept of a DLT first appeared in 1889 and has been continuously modified over the last century [
1]. Modern day DLT designs are based on the design published by Carlens in 1949 [
4], which was later refined by Robertshaw [
5], and have since been popular in practice until now [
6]. DLTs today are single-use, disposable equipment made of polyvinyl chloride (PVC), instead of rubber due to sterilization concerns [
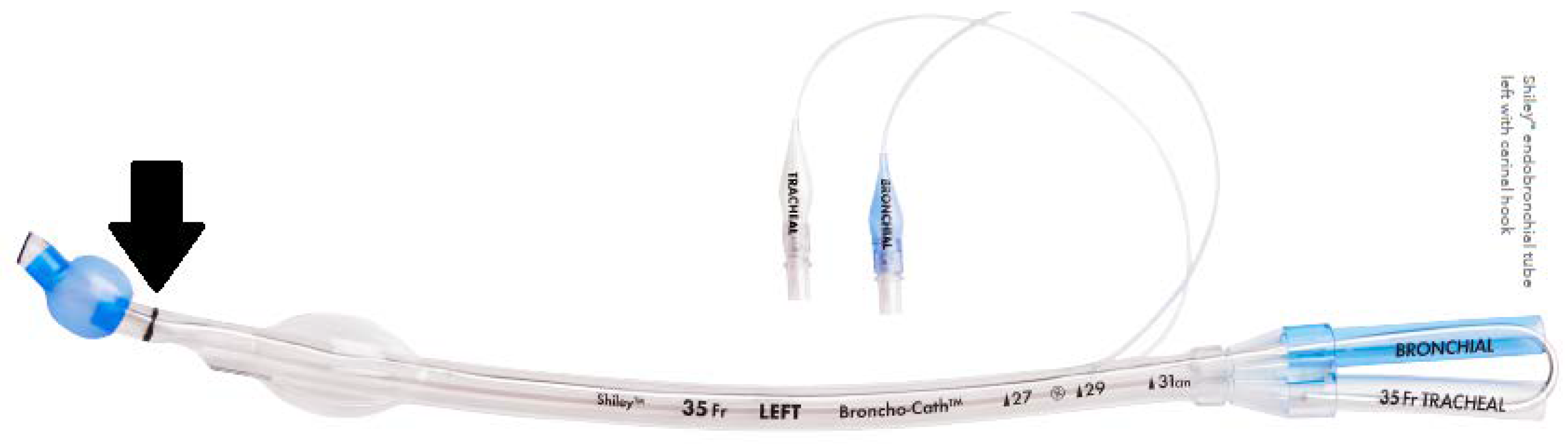
2]. They are composed of two endotracheal tubes bonded together: the shorter tracheal lumen ends in the distal trachea when placed correctly, and the longer, angled bronchial lumen enters either the left or right main bronchus based on its sidedness. In addition, they also possess balloon-like tracheal and bronchial cuffs, which can block the according position when inflated, further allowing the anesthesiologist to control which lung they choose to ventilate.
In most clinical situations, left-sided DLTs are preferred over right-sided DLTs, while both designs allow individual ventilation for either lung. Although the angle of the right main bronchus (RMB) is generally more aligned with the trachea, there is also a greater risk of obstructing the ventilation of the right upper lobe when using a right-sided DLT, especially in some patients whose right upper lobar bronchus originated near the carina or even from the trachea [
7,
8]. Therefore, right-sided DLTs are usually used as a last approach in situations such as when there is an obstruction of the LMB, or when there is a surgical procedure involving the proximal LMB [
9]. Since the bifurcation of the left main bronchus (LMB) usually occurs more distal than the RMB, it is considered to have a wider safety margin, which is defined as the length that a DLT may be moved or positioned without obstructing a conducting airway [
10].
Incorrect placement of the DLT during surgery can cause many problems, such as airway trauma or rupture; incidents such as accidental blockage of the left upper lobe by the bronchial cuff leading to hypoxemia during one lung ventilation can also occur [
11]. The correct placement of a DLT depends a lot on choosing the best fitting DLT size for the patient. Using an undersized DLT can cause airway injuries because of the need to use higher pressures in the bronchial cuff to completely seal off the space between the outer border of the DLT and the airway; the smaller internal diameter of the DLT can also increase airway resistance during mechanical ventilation, which could lead to auto positive end-expiratory pressure (PEEP). DLTs that are too small also have higher chances of dislodgment, which can lead to the failure of lung isolation and an inability to suction secretions [
8]. On the other hand, the use of oversized DLTs have been observed to correlate with postoperative sequelae, such as a sore throat and hoarseness. Because larger sized DLTs are more difficult to intubate, this could also lead to forceful insertions and repeated attempts of intubation, causing airway and teeth injury during the process, and the extra wasting of time and equipment [
12].
A fundamental problem for choosing an adequately sized DLT for individual patients is the lack of evidence-based guidelines. It is traditionally recommended to select DLT size based on the patient’s gender and height, however this method is not very accurate, especially in females, persons with smaller statures, and Asian populations [
2,
8]. Using patients’ airway measurements acquired from various imaging techniques, such as chest X-rays (CXR), computed tomography (CT), magnetic resonance imaging (MRI) or ultrasound (UR), to facilitate the choosing of DLT sizes appears to be a more accurate approach [
12,
13,
14,
15,
16]. However, this method still has its shortcomings, for example, this is not applicable for emergency trauma patients who may not have time to perform chest CT.
In this study, our goal is to analyze tracheobronchial tree measurements from the clinical imaging records of adult patients who received DLT intubation in Tainan Municipal An-Nan Hospital-China Medical University. From the dataset, we have analyzed the correlation between patients’ demographic data (such as age, sex and body sizes), in the hope of developing a formula via machine learning that can be used to predict the best fit DLT size for the local population. The results would allow us to expand the analysis to a larger dataset and develop a mobile formula-based application, which can provide clinicians with easy and actual application in real life.
3. Data Processing and Statistical Analysis
The first step was performing a correlational ranking of all the parameters: for all 231 subjects, each of their 17 body parameters were linearly correlated with either ‘size’ or ’depth’ values. Their correlation coefficient, or r values, were then ordered from high-to-low, for ‘depth’ and ‘size’, respectively. The easily available parameters with r values > 0.5 for ‘depth’ and ‘size’ separately were identified. A Support Vector Machine (SVM) was then adopted to model the clinical data of ‘size’ or ‘depth’ based on the four or five body parameters identified. A detailed description of SVM is given separately in
Supplementary Materials S1. In brief, it is a machine learning model using a supervised learning model with associated algorithms, typically applied for classification and regression analyses. Support Vector Machine (SVM) is a supervised algorithm based on statistical learning that separates two distinct sets by a hyperplane. The classification is to find the dividing line between different classes of data. In general, the dividing line is complex with multiple possibilities. SVM is to find the best solution among these possibilities. The spirit of the SVM algorithm is to find a separation line (or hyperplane) so that all points on the boundary are separated as far as possible, to better resist noise in data. It has advantages over the robust linear regression model (details shown in
Supplementary Materials S2) when data distribution is not normal, as in our present study. For comparison purposes, we also tested a linear regression model at a later stage. For example, a cell-phone with a dedicated software would allow clinicians to obtain values on ‘depth’ and ‘size’ almost instantly after entering the five parameters.
The computer language used for modeling was Python [
17], which is a general-purpose language with a wide array of modules and tool packages that can be used for statistical analysis. In this study, statistical analyses were conducted in Jupyter Notebook (Version 6.3.0) using Python packages Pandas, NumPy, Mlxtend, Matplotlib and scikit-learn.
5. Discussion
The principal finding of this study is that the DLT both ‘size’ and ‘depth’ were modeled rather satisfactorily, using the SVM approach. Inputs to the model were four or five body parameters, including one measured from chest X-ray images. All of these parameters are easily available from the medical records of patients. Chest X-ray images are also routinely available. Results fulfilled our primary aim in finding body parameters that could be conveniently used to predict ‘size’ and ‘depth’ settings in the DLT procedure, especially for patients in emergent situations.
Since we had measured other parameters such as those from CT images, and calculated their r values, we performed an alternative modeling based on the top five parameters with r values >0.65. Despite their higher r values, only slightly better results were found (
Supplementary Table S1). The reason for such minimal improvements is likely due to the high correlation among those new parameters themselves (r values: 0.72 to 0.79, results not shown).
The fact that body parameters are able to predict chest-related metric, is first consistent with our report predicting the tidal volume of the lung based on similar body parameters. For tidal volume, the six parameters used were, in descending order of importance: weight, height, chest circumference, sex, BMI and age. The first four parameters overlap with those in our present study. In the tidal volume study, we applied only linear regression analysis. There, data were more evenly distributed (giving rise to higher values of r) compared with our present study. Given the relatively low values of r of the four or five parameters against ‘depths’ or ‘sizes’, the hyperplane classifier as provided by SVM, is likely more appropriate than linear regression for modeling. Since hyperplane can better handle the characteristics of our data, such as the small number of model targets, and uneven distribution. These, and other data characteristics, might well lead to the discrepancy in model performance between ‘depth’ and ‘size’.
The pre-processing step of rejecting statistical outliers in the dataset was used in the present study. The rationale was to produce a more homogeneous dataset for modeling. Without outlier rejection, model performance was expectedly poorer (
Supplementary Table S2).
There were similar studies focusing on using airway parameters to predict the best fit DLT size for individual patients [
12,
14,
15,
16]. Most of these studies used CT imaging and multiplanar reconstruction (MPR) to measure the cricoid and LMB for subjective determination of the DLT size. These parameters were also found to have high values of r in our present study. While MPR has the advantage of creating a 3D model of the airway for more precise measurements, it is not practical for emergency patients.
In contrast, the measurements used in our method were easy to acquire; weight, height and chest circumference can be directly measured from the patient, and TD-trachea can be obtained from chest X-ray images. Moreover, a predictive machine learning model trained with local population data could be more tailored to the local population’s average bodily features. The formula derived from machine learning could be easily developed into assisting tools such as mobile device applications. For example, a cell-phone with a dedicated software would allow clinicians to obtain values on ‘depth’ and ‘size’ almost instantly after entering the five parameters.
Some imitations of our study are as follows. First, it had a relatively small sample size. Second, ‘depth’ and ‘size’ were separately modeled instead of using the same model, making the development of future software applications more complicated. Third, we did not test exhaustively all models, and therefore cannot rule out the possibility of other better models than SVM outside linear regression.

 ,
, 









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}