
Performance of Clinical and Biochemical Parameters in Identifying Renal Histopathology and Predictors of One-Year Renal Outcome in Lupus Nephritis—A Single Centre Study from India
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
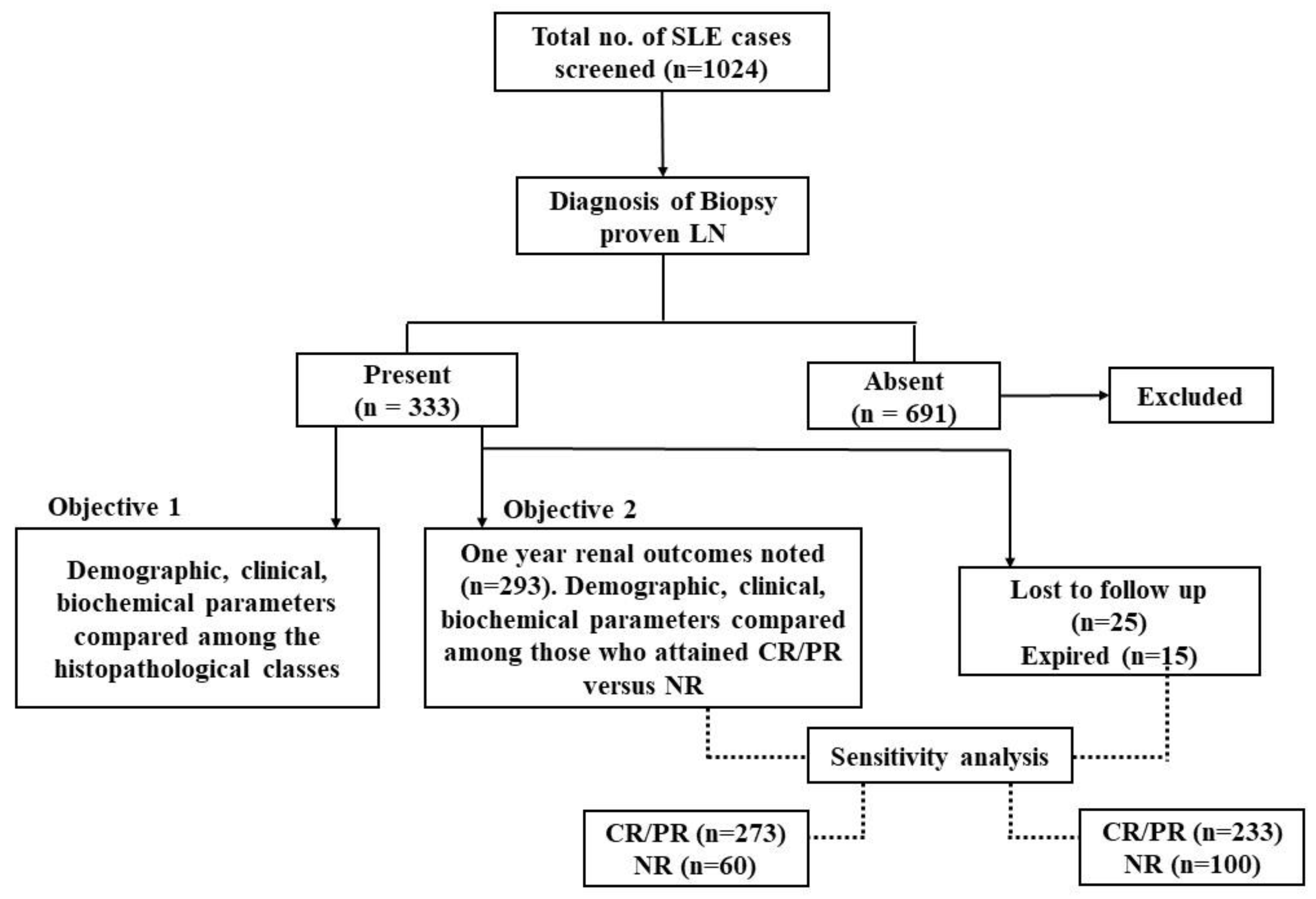
3. Results
3.1. Patient Characteristics
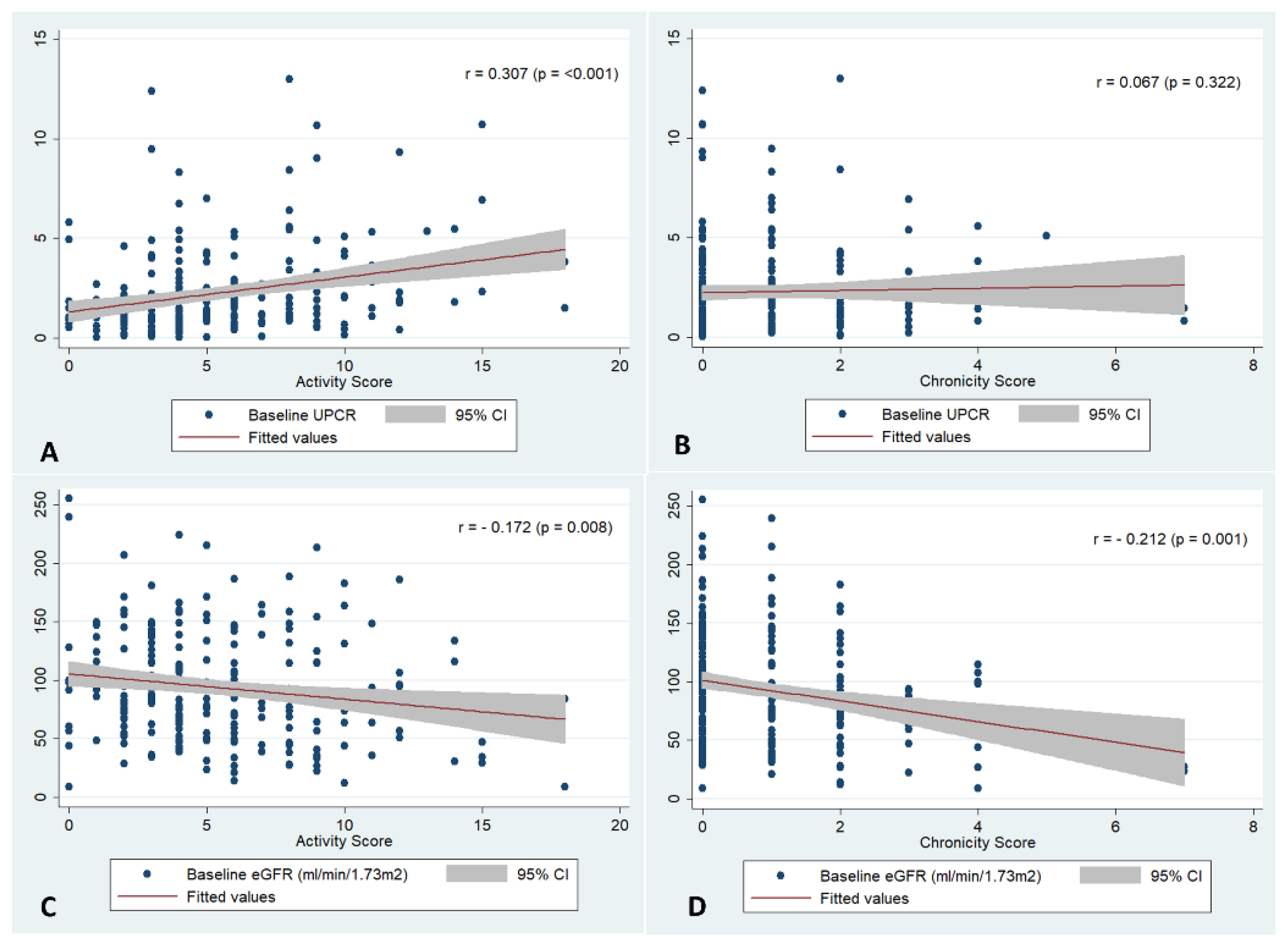
3.2. Correlation and Performance of Clinical Parameters with the Renal Histopathology at Baseline
3.3. Performance of the Clinical and Biochemical Parameters in Identifying the Renal Histopathology
3.4. Renal Outcomes at One Year
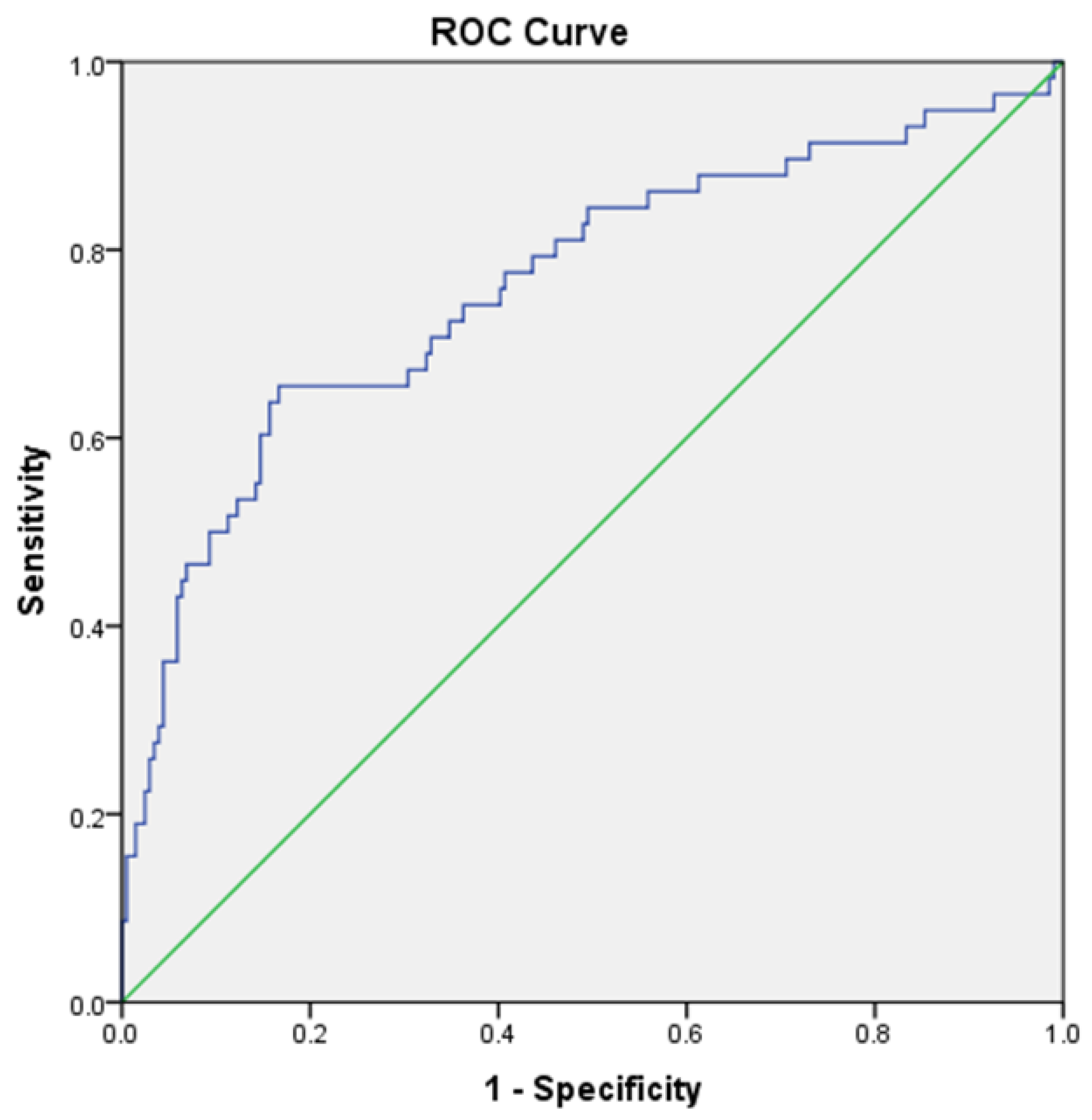
3.5. Model to Predict Non-Response at One Year
3.6. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Almaani, S.; Meara, A.; Rovin, B.H. Update on Lupus Nephritis. Clin. J. Am. Soc. Nephrol. 2017, 12, 825–835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wenderfer, S.E.; Lane, J.C.; Shatat, I.F.; von Scheven, E.; Ruth, N.M. Practice patterns and approach to kidney biopsy in lupus: A collaboration of the Midwest pediatric nephrology consortium and the childhood arthritis and rheumatology research alliance. Pediatr. Rheumatol. Online J. 2015, 13, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiorentino, M.; Bolignano, D.; Tesar, V.; Pisano, A.; Van Biesen, W.; D’Arrigo, G.; Tripepi, G.; Gesualdo, L. Renal Biopsy in 2015—From Epidemiology to Evidence-Based Indications. Am. J Nephrol. 2016, 43, 1–19. [Google Scholar] [CrossRef]
- Liu, C.C.; Kao, A.H.; Manzi, S.; Ahearn, J.M. Biomarkers in systemic lupus erythematosus: Challenges and prospects for the future. Ther. Adv. Musculoskelet. Dis. 2013, 5, 210–233. [Google Scholar] [PubMed]
- Appel, G.B.; Contreras, G.; Dooley, M.A.; Ginzler, E.M.; Isenberg, D.; Jayne, D.; Li, L.E.; Mysler, E.; Sánchez-Guerrero, J.; Solomons, N.; et al. Mycophenolate Mofetil versus Cyclophosphamide for Induction Treatment of Lupus Nephritis. J. Am. Soc. Nephrol. 2009, 20, 1103–1112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehra, S.; Usdadiya, J.B.; Jain, V.K.; Misra, D.P.; Negi, V.S. Comparing the efficacy of low-dose vs high-dose cyclophosphamide regimen as induction therapy in the treatment of proliferative lupus nephritis: A single center study. Rheumatol. Int. 2018, 38, 557–568. [Google Scholar] [CrossRef]
- Rathi, M.; Goyal, A.; Jaryal, A.; Sharma, A.; Gupta, P.K.; Ramachandran, R.; Kumar, V.; Kohli, H.S.; Sakhuja, V.; Jha, V.; et al. Comparison of low-dose intravenous cyclophosphamide with oral mycophenolate mofetil in the treatment of lupus nephritis. Kidney Int. 2016, 89, 235–242. [Google Scholar] [CrossRef] [Green Version]
- Fanouriakis, A.; Kostopoulou, M.; Cheema, K.; Anders, H.J.; Aringer, M.; Bajema, I.; Berden, J.H.M.; Boletis, J.; Cervera, R.; Dörneret, T.; et al. 2019 Update of the Joint European League Against Rheumatism and European Renal Association-European Dialysis and Transplant Association (EULAR/ERA-EDTA) recommendations for the management of lupus nephritis. Ann. Rheum. Dis. 2020, 79, 713–723. [Google Scholar]
- Parikh, S.V.; Rovin, B.H. Current and Emerging Therapies for Lupus Nephritis. J. Am. Soc. Nephrol. 2016, 27, 2929–2939. [Google Scholar] [CrossRef] [Green Version]
- Dall’Era, M.; Cisternas, M.G.; Smilek, D.E.; Straub, L.; Houssiau, F.A.; Cervera, R.; Rovin, B.H.; Mackay, M. Predictors of Long-Term Renal Outcome in Lupus Nephritis Trials: Lessons Learned from the Euro-Lupus Nephritis Cohort: Predictors of Renal Outcome in Lupus Nephritis Trials. Arthritis Rheumatol. 2015, 67, 1305–1313. [Google Scholar] [CrossRef]
- Najafi, C.C.; Korbet, S.M.; Lewis, E.J.; Schwartz, M.M.; Reichlin, M.; Evans, J. Significance of histologic patterns of glomerular injury upon long-term prognosis in severe lupus glomerulonephritis. Kidney Int. 2001, 59, 2156–2163. [Google Scholar] [CrossRef] [PubMed]
- Moroni, G.; Porata, G.; Raffiotta, F.; Quaglini, S.; Frontini, G.; Sacchi, L.; Binda, V.; Calatroni, M.; Reggiani, F.; Banfi, G.; et al. Beyond ISN/RPS Lupus Nephritis Classification: Adding Chronicity Index to Clinical Variables Predicts Kidney Survival. Kidney360 2021, 3, 122–132. [Google Scholar] [CrossRef] [PubMed]
- Moroni, G.; Gatto, M.; Tamborini, F.; Quaglini, S.; Radice, F.; Saccon, F.; Frontini, G.; Alberici, F.; Sacchi, L.; Binda, V.; et al. Lack of EULAR/ERA-EDTA response at 1 year predicts poor long-term renal outcome in patients with lupus nephritis. Ann. Rheum. Dis. 2020, 79, 1077–1083. [Google Scholar] [CrossRef]
- Mok, M.; Li, W. Do Asian patients have worse lupus? Lupus 2010, 19, 1384–1390. [Google Scholar] [CrossRef] [PubMed]
- DeQuattro, K.; Trupin, L.; Murphy, L.B.; Rush, S.; Criswell, L.A.; Lanata, C.M.; Dall’Era, M.; Katz, P.; Yazdany, J. High Disease Severity Among Asian Patients in a US Multiethnic Cohort of Individuals with Systemic Lupus Erythematosus. Arthritis Care Res. 2022, 74, 896–903. [Google Scholar] [CrossRef]
- Weening, J.J.; D’Agati, V.D.; Schwartz, M.M.; Seshan, S.V.; Alpers, C.E.; Appel, G.B.; Balow, J.E.; Bruijn, J.A.N.A.; Cook, T.; Ferrario, F.; et al. The classification of glomerulonephritis in systemic lupus erythematosus revisited. J. Am. Soc. Nephrol. 2004, 15, 241–250. [Google Scholar] [CrossRef]
- Bajema, I.M.; Wilhelmus, S.; Alpers, C.E.; Bruijn, J.A.; Colvin, R.B.; Cook, H.T.; D’Agati, V.D.; Ferrario, F.; Haas, M.; Jennette, J.C.; et al. Revision of the International Society of Nephrology/Renal Pathology Society classification for lupus nephritis: Clarification of definitions, and modified National Institutes of Health activity and chronicity indices. Kidney Int. 2018, 93, 789–796. [Google Scholar] [CrossRef]
- Yee, C.S.; Cresswell, L.; Farewell, V.; Rahman, A.; Teh, L.S.; Griffiths, B.; Bruce, I.N.; Ahmad, Y.; Prabu, A.; Akil, M.; et al. Numerical scoring for the BILAG-2004 index. Rheumatol. Oxf. Engl. 2010, 49, 1665–1669. [Google Scholar] [CrossRef] [Green Version]
- Gladman, D.D.; Ibañez, D.; Urowitz, M.B. Systemic lupus erythematosus disease activity index 2000. J. Rheumatol. 2002, 29, 288–291. [Google Scholar]
- Wakasugi, D.; Gono, T.; Kawaguchi, Y.; Hara, M.; Koseki, Y.; Katsumata, Y.; Hanaoka, M.; Yamanaka, H. Frequency of class III and IV nephritis in systemic lupus erythematosus without clinical renal involvement: An analysis of predictive measures. J. Rheumatol. 2012, 39, 79–85. [Google Scholar] [CrossRef]
- Nasri, H.; Ahmadi, A.; Baradaran, A.; Momeni, A.; Nasri, P.; Mardani, S.; Rafieian-Kopaei, M.; Mubarak, M. Clinicopathological correlations in lupus nephritis; a single center experience. J. Nephropathol. 2014, 3, 115–120. [Google Scholar] [PubMed]
- Yu, F.; Tan, Y.; Liu, G.; Wang, S.X.; Zou, W.Z.; Zhao, M.H. Clinicopathological characteristics and outcomes of patients with crescentic lupus nephritis. Kidney Int. 2009, 76, 307–317. [Google Scholar] [CrossRef] [PubMed]
- Ioannidis, J.P.; Boki, K.A.; Katsorida, M.E.; Drosos, A.A.; Skopouli, F.N.; Boletis, J.N.; Moutsopoulos, H.M. Remission, relapse, and re-remission of proliferative lupus nephritis treated with cyclophosphamide. Kidney Int. 2000, 57, 258–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rijnink, E.C.; Teng, Y.K.O.; Wilhelmus, S.; Almekinders, M.; Wolterbeek, R.; Cransberg, K.; Bruijn, J.A.; Bajema, I.M. Clinical and Histopathologic Characteristics Associated with Renal Outcomes in Lupus Nephritis. Clin. J. Am. Soc. Nephrol. 2017, 12, 734–743. [Google Scholar] [CrossRef] [Green Version]
- Yadav, S.; Balakrishnan, C.; Kothari, J. Long-term outcome and predictors of long-term outcome in patients with lupus nephritis managed at a tertiary hospital in Mumbai. Lupus 2022, 31, 1191–1201. [Google Scholar] [CrossRef]
- Tesar, V.; Hruskova, Z. Understanding Histolopathologic Characteristics to Predict Renal Outcomes in Lupus Nephritis. Clin. J. Am. Soc. Nephrol. 2017, 12, 711–712. [Google Scholar] [CrossRef] [Green Version]
- Ichinose, K.; Kitamura, M.; Sato, S.; Eguchi, M.; Okamoto, M.; Endo, Y.; Tsuji, S.; Takatani, A.; Shimizu, T.; Umeda, M.; et al. Complete renal response at 12 months after induction therapy is associated with renal relapse-free rate in lupus nephritis: A single-center, retrospective cohort study. Lupus 2019, 28, 501–509. [Google Scholar] [CrossRef]
- Hsu, C.Y.; Chiu, W.C.; Yang, T.S.; Chen, C.J.; Chen, Y.C.; Lai, H.M.; Yu, S.-F.; Su, Y.-J.; Cheng, T.-T. Age- and gender-related long-term renal outcome in patients with lupus nephritis. Lupus 2011, 20, 1135–1141. [Google Scholar] [CrossRef]
- de Carvalho, J.F.; do Nascimento, A.P.; Testagrossa, L.A.; Barros, R.T.; Bonfá, E. Male gender results in more severe lupus nephritis. Rheumatol. Int. 2010, 30, 1311–1315. [Google Scholar] [CrossRef]
- Park, D.J.; Kang, J.H.; Lee, J.W.; Lee, K.E.; Kim, T.J.; Park, Y.W.; Choi, Y.D.; Lee, S.S. Risk factors to predict the development of chronic kidney disease in patients with lupus nephritis. Lupus 2017, 26, 1139–1148. [Google Scholar] [CrossRef]
- Clemmer, J.S.; Hillegass, W.B.; Taylor, E.B. Antihypertensive effects of immunosuppressive therapy in autoimmune disease. J. Hum. Hypertens. 2022. [Google Scholar] [CrossRef] [PubMed]
- Gomez Mendez, L.M.; Cascino, M.D.; Katsumoto, T.R.; Brakeman, P.; Brunetta, P.; Jayne, D.; Dall’Era, M.; Rovin, B.; Garg, J. Outcome of participants with nephrotic syndrome in combined clinical trials of lupus nephritis. Lupus Sci. Med. 2019, 6, e000308. [Google Scholar] [CrossRef] [PubMed]
- Touma, Z.; Urowitz, M.B.; Ibañez, D.; Gladman, D.D. Time to Recovery from Proteinuria in Patients with Lupus Nephritis Receiving Standard Treatment. J. Rheumatol. 2014, 41, 688–697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Austin, H.A.; Muenz, L.R.; Joyce, K.M.; Antonovych, T.T.; Balow, J.E. Diffuse proliferative lupus nephritis: Identification of specific pathologic features affecting renal outcome. Kidney Int. 1984, 25, 689–695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Broder, A.; Mowrey, W.B.; Khan, H.N.; Jovanovic, B.; Londono-Jimenez, A.; Izmirly, P.; Putterman, C. Tubulointerstitial damage predicts end stage renal disease in lupus nephritis with preserved to moderately impaired renal function: A retrospective cohort study. Semin. Arthritis Rheum. 2018, 47, 545–551. [Google Scholar] [CrossRef] [Green Version]
- Clark, M.R.; Trotter, K.; Chang, A. The Pathogenesis and Therapeutic Implications of Tubulointerstitial Inflammation in Human Lupus Nephritis. Semin. Nephrol. 2015, 35, 455–464. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, C.; Chang, A.; Brandt, D.; Guttikonda, R.; Utset, T.O.; Clark, M.R. Predicting outcomes of lupus nephritis with tubulointerstitial inflammation and scarring. Arthritis Care Res. 2011, 63, 865–874. [Google Scholar] [CrossRef] [Green Version]
- Pattanashetti, N.; Anakutti, H.; Ramachandran, R.; Rathi, M.; Sharma, A.; Nada, R.; Gupta, K. Effect of Thrombotic Microangiopathy on Clinical Outcomes in Indian Patients with Lupus Nephritis. Kidney Int. Rep. 2017, 2, 844–849. [Google Scholar] [CrossRef] [Green Version]
- Bolognesi, M.M.; Capitoli, G.; Galimberti, S.; Cattoretti, G.; Bajema, I.; Bruijn, J.A.; Cook, H.T.; Noel, L.-H.; Pagni, F.; Ferrario, F.; et al. Dissecting the histological features of lupus nephritis highlights new common patterns of injury in class III/IV. Ann. Rheum. Dis. 2022, 81, 1704–1711. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Class I/II (n = 52) | Class III/IV (n = 240) | Class V (n = 28) | Combined (III/IV+V) (n = 13) | p-Value |
|---|---|---|---|---|---|
| Demography | |||||
| Female, n (%) | 46(88.5) | 221(92.1) | 26(92.9) | 14(100) | 0.372 |
| Age at SLE onset (median, range) | 29(10–57) | 25(8–67) | 32(11–44) | 28(13–47) | 0.707 |
| Age at nephritis onset (median, range) | 30(11–57) | 27(9–67) | 33(17–45) | 32(13–48) | 0.350 |
| Disease duration at enrolment (months) (median, range) | 15(0–232) | 12(0–228) | 24(0–144) | 40(0–96) | 0.499 |
| Clinical and biochemical parameters | |||||
| Hypertension, n (%) | 8(15.4) | 125(52.1) | 7(25.0) | 8(61.5) | 0.001 |
| Median Serum Creatinine (mg/dL), Median (IQR) | 0.7(0.5–0.86) | 0.84(0.68–1.1) | 0.65(0.5–0.83) | 0.70(0.54–0.79) | <0.001 |
| Serum Creatinine > 1.3 g/dL, n (%) | 4(7.7) | 39(16.3) | 2(7.1) | 13(100) | 0.044 |
| eGFR (ml/min/1.73 m2), Median (IQR) | 115.8(79.4–152.7) | 87.6(62.75–118.8) | 130.8(105.7–164.9) | 99.5(87.2–126.2) | <0.001 |
| eGFR categories, n (%) >90 61–90 30–60 <30 | 34(65.4) 22(21.2) 5(9.6) 1(1.9) | 116(48.3) 67(27.9) 42(17.5) 14(5.8) | 23(82.1) 3(10.7) 2(7.1) 0 | 11(84.6) 2(15.4) 0 0 | 0.002 |
| Serum albumin(g/dL), Median (IQR) | 3.2(2.75–3.60) | 2.9(2.4–3.3) | 2.8(2.48–3.40) | 3.0(2.30–3.55) | 0.069 |
| Active urinary sediments, n (%) | 24(46.2) | 154(64.2) | 10(35.7) | 8(61.5) | 0.006 |
| UPCR (mg/mg), Median (IQR) | 1.2(0.69–1.70) | 1.6(0.88–2.79) | 1.9(1.5–3.49) | 3.2(1.17–6.0) | <0.001 |
| UPCR category, n (%) >3 g 2–3 g <2 g | 6(11.5) 4(7.7) 41(78.8) | 52(21.7) 39(16.3) 144(60.0) | 9(32.1) 3(10.7) 15(53.6) | 6(46.2) 1(7.7) 6(46.2) | 0.004 |
| Disease activity measures | |||||
| Renal SLEDAI, Median (IQR) | 4(4–12) | 12(8–12) | 8(4–8) | 8(4–12) | <0.001 |
| SLEDAI, Median (IQR) | 14(9.5–20.5) | 18(14–24) | 14(8–18) | 14(10.75–16.75) | 0.032 |
| Extrarenal SLEDAI, Median (IQR) | 7 (2–12) | 7 (3–13) | 4.5 (2–10) | 4 (2–10) | 0.243 |
| Serological parameters | |||||
| * Anti-dsDNA high titre positivity, n (%) | 23(44.2) | 145(60.4) | 11(39.3) | 7(53.8) | 0.849 |
| Low C3/C4, n (%) | 34(65.4) | 181(75.4) | 20(71.4) | 10(76.9) | 0.838 |
| ACLA/Anti-B2gpI/LAC positivity (any one positive), n (%) | 16(30.8) | 68(28.3) | 7(25.0) | 1(7.7) | 0.279 |
| Proliferative LN | Crescents | Interstitial Inflammation | Chronicity | |||||
|---|---|---|---|---|---|---|---|---|
| Baseline Parameter | Sensitivity (%) | Specificity (%) | Sensitivity (%) | Specificity (%) | Sensitivity (%) | Specificity (%) | Sensitivity (%) | Specificity (%) |
| Any one parameter present | 96.4 | 8.7 | 98.4 | 4.5 | 94.5 | 3.16 | 95.8 | 3.85 |
| All four parameters present | 7.5 | 98.7 | 16.9 | 95.4 | 8.8 | 95.5 | 11.6 | 95.6 |
| >1 or <4 parameters present | 53.7 | 81.2 | 49.2 | 64.4 | 41.9 | 63.9 | 48.8 | 67.7 |
| Parameter | Responders (CR/PR) (n = 233) | Non-Responders (NR) (n = 60) | p-Value |
|---|---|---|---|
| Demography | |||
| Female/male, n (%) | 221(94.8)/12(5.2) | 48(80)/12(20) | 0.001 |
| Age at SLE onset, Median (range) | 26(10–62) | 23.5(12–67) | 0.067 |
| Age at nephritis onset, Median (range) | 28(11–65) | 25(13–67) | 0.079 |
| Disease duration at enrolment (months), Median (range) | 12(0–232) | 18(0–144) | 0.770 |
| Duration of follow-up, | 37(9–180) | 24(2–86) | 0.001 |
| Clinical and biochemical parameters | |||
| Hypertension, n (%) | 100(42.9) | 34(56.7) | 0.061 |
| Creatinine, Median (IQR) | 0.79(0.6–0.96) | 0.9(0.7–1.33) | 0.009 |
| Creatinine > 1.3 mg/dL, Median (IQR) | 21(9.0) | 15(25) | 0.001 |
| eGFR (ml/min/1.73 m2), Median (IQR) | 97.2(73.6–136.5) | 83.85(50.7–123) | 0.203 |
| eGFR categories, n (%) >90 61–90 30–60 <30 | 137(58.8) 57(24.5) 34(14.6) 4(1.7) | 27(45) 15(25) 9(15) 8(13.3) | 0.003 |
| Serum albumin (mg/dL), Median (IQR) | 3(2.5–3.4) | 2.9(2.2–3.1) | 0.314 |
| Active urinary sediments, n (%) | 132(56.7) | 44(73.3) | 0.019 |
| UPCR (g/day), Median (IQR) | 1.38(0.8–2.67) | 1.95(1.18–4.19) | 0.098 |
| UPCR categories, n (%) >2 2–3 <2 | 51(21.9) 25(11.2) 151(64.8) | 18(30) 12(20) 30(50) | 0.114 |
| Renal SLEDAI, Median (IQR) | 8(4–12) | 12(8–12) | 0.014 |
| Total SLEDAI, Median (IQR) | 17(12–22) | 16.5(13.7–24.2) | 0.852 |
| Serological parameters | |||
| * Anti-dsDNA high titre positivity, n (%) | 129(55.4) | 36(60) | 0.658 |
| $ Low C3/C4, n (%) | 166(71.2) | 45(75) | 0.347 |
| ACLA/Anti-B2gpI/LAC positivity (any one positive), n (%) | 62(26.6) | 21(35) | 0.401 |
| Histological | |||
| Class I/II, n (%) | 42(18.0) | 3(5) | 0.013 |
| Class III/IV, n (%) | 167(71.7) | 49(81.7) | 0.117 |
| Class V, n (%) | 17(7.3) | 5(8.3) | 0.788 |
| Combined class, n (%) | 7(3.0) | 3(5.0) | 0.469 |
| Activity score, Median (IQR) | 3(1–6) | 6(3–9) | 0.001 |
| Chronicity score, Median (IQR) | 0(0–1) | 1(0–2) | 0.001 |
| Chronicity score >3, n (%) | 5(2.1) | 6(10) | 0.013 |
| Presence of crescents, no (%) | 43(18.5) | 17(28.3) | 0.104 |
| Fibrinoid necrosis, n (%) | 28(12.0) | 7(11.7) | 0.791 |
| Interstitial inflammation, n (%) | 86(36.9) | 33(55) | 0.004 |
| Interstitial fibrosis, n (%) | 23(10.7) | 9(15) | 0.273 |
| Tubular injury, n (%) | 44(18.9) | 16(26.7) | 0.130 |
| Tubular atrophy, n (%) | 64(27.5) | 27(45) | 0.003 |
| Blood vessel changes, n (%) Fibrinoid necrosis Other changes ** | 2(0.9) 206(88.4) | 1(1.7) 50(83.3) | 0.606 0.339 |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Male | 4.6 | 1.9–10.8 | <0.001 | 3.9 | 1.4–11.0 | 0.008 |
| Age at SLE onset, years | 0.97 | 0.9–1.0 | 0.080 | 0.9 | 0.9–1.0 | 0.053 |
| Hypertension | 0.5 | 0.3–1.0 | 0.063 | 1.1 | 0.5–2.3 | 0.721 |
| Serum Creatinine, mg/dL | 2.7 | 1.6–4.6 | <0.001 | 1.9 | 1.1–3.2 | 0.041 |
| Serum albumin, mg/dL | 0.6 | 0.4–0.9 | 0.048 | |||
| Active urinary sediments | 0.4 | 0.2–0.8 | 0.020 | 0.7 | 0.3–1.6 | 0.479 |
| UPCR g/day | 1.1 | 1.0–1.3 | 0.002 | 1.2 | 1.0–1.3 | 0.002 |
| Anti-dsDNA high positivity * | 1.1 | 0.5–2.3 | 0.658 | |||
| Low C3/C4 $ | 0.7 | 0.3–1.4 | 0.349 | |||
| ACLA/Anti-B2gpI/LAC positivity | 1.3 | 0.7–2.4 | 0.402 | |||
| Activity score | 1.1 | 1.0–1.2 | <0.001 | 1.0 | 0.7–1.1 | 0.145 |
| Chronicity score | 1.6 | 1.2–2.0 | <0.001 | 1.5 | 1.2–2.0 | 0.001 |
| Crescents | 0.5 | 0.3–1.1 | 0.107 | |||
| Fibrinoid necrosis | 1.0 | 0.4–2.5 | 0.906 | |||
| Interstitial inflammation | 0.3 | 0.2–0.7 | 0.004 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gopal, A.; Kavadichanda, C.; Bairwa, D.; Shah, S.; Mehra, S.; Srinivas, B.H.; Mariaselvam, C.M.; Thabah, M.M.; Negi, V.S. Performance of Clinical and Biochemical Parameters in Identifying Renal Histopathology and Predictors of One-Year Renal Outcome in Lupus Nephritis—A Single Centre Study from India. Diagnostics 2022, 12, 3163. https://doi.org/10.3390/diagnostics12123163
Gopal A, Kavadichanda C, Bairwa D, Shah S, Mehra S, Srinivas BH, Mariaselvam CM, Thabah MM, Negi VS. Performance of Clinical and Biochemical Parameters in Identifying Renal Histopathology and Predictors of One-Year Renal Outcome in Lupus Nephritis—A Single Centre Study from India. Diagnostics. 2022; 12(12):3163. https://doi.org/10.3390/diagnostics12123163
Chicago/Turabian StyleGopal, Aishwarya, Chengappa Kavadichanda, Devender Bairwa, Sanket Shah, Sonal Mehra, Bheemanathi Hanuman Srinivas, Christina Mary Mariaselvam, Molly Mary Thabah, and Vir Singh Negi. 2022. "Performance of Clinical and Biochemical Parameters in Identifying Renal Histopathology and Predictors of One-Year Renal Outcome in Lupus Nephritis—A Single Centre Study from India" Diagnostics 12, no. 12: 3163. https://doi.org/10.3390/diagnostics12123163