
A Pilot Study on the Reliability of Ultrasound-Based Assessment of Patella Diameter and Sulcus Angle
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Examiners
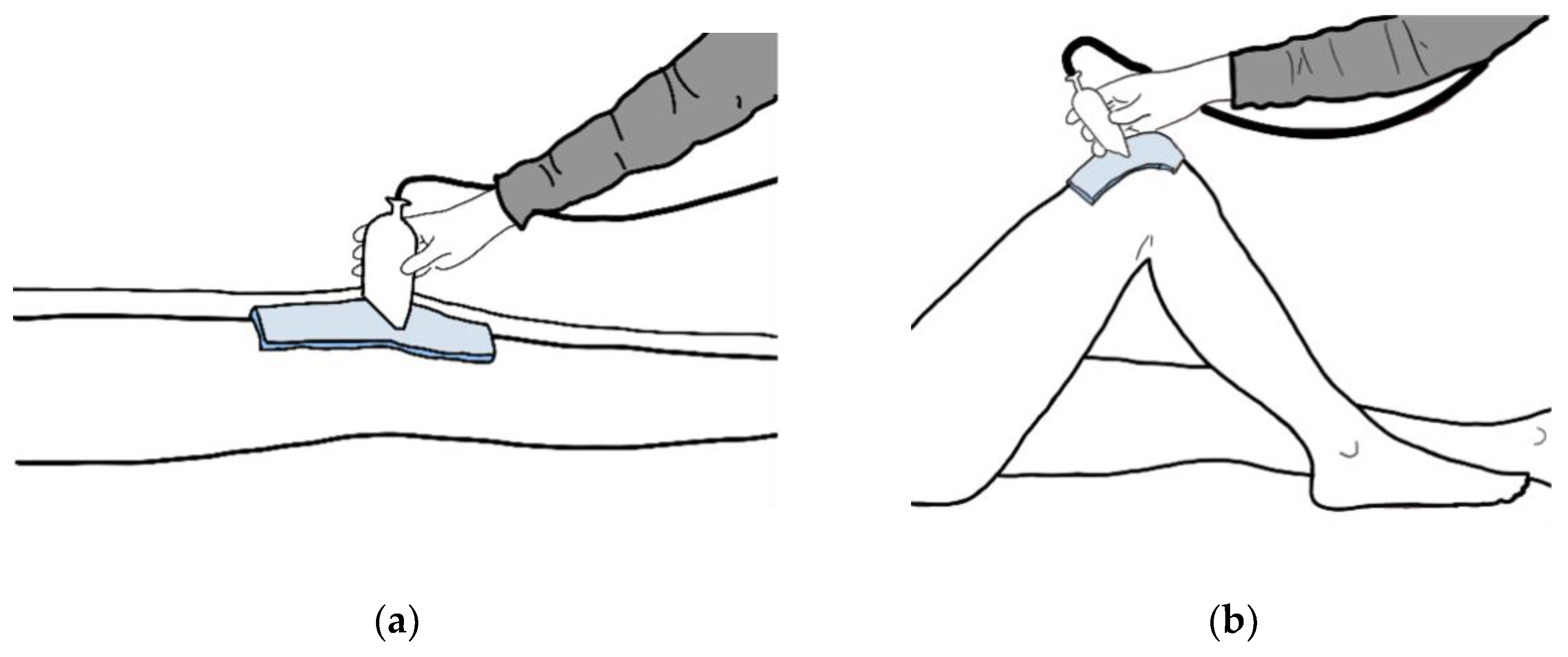
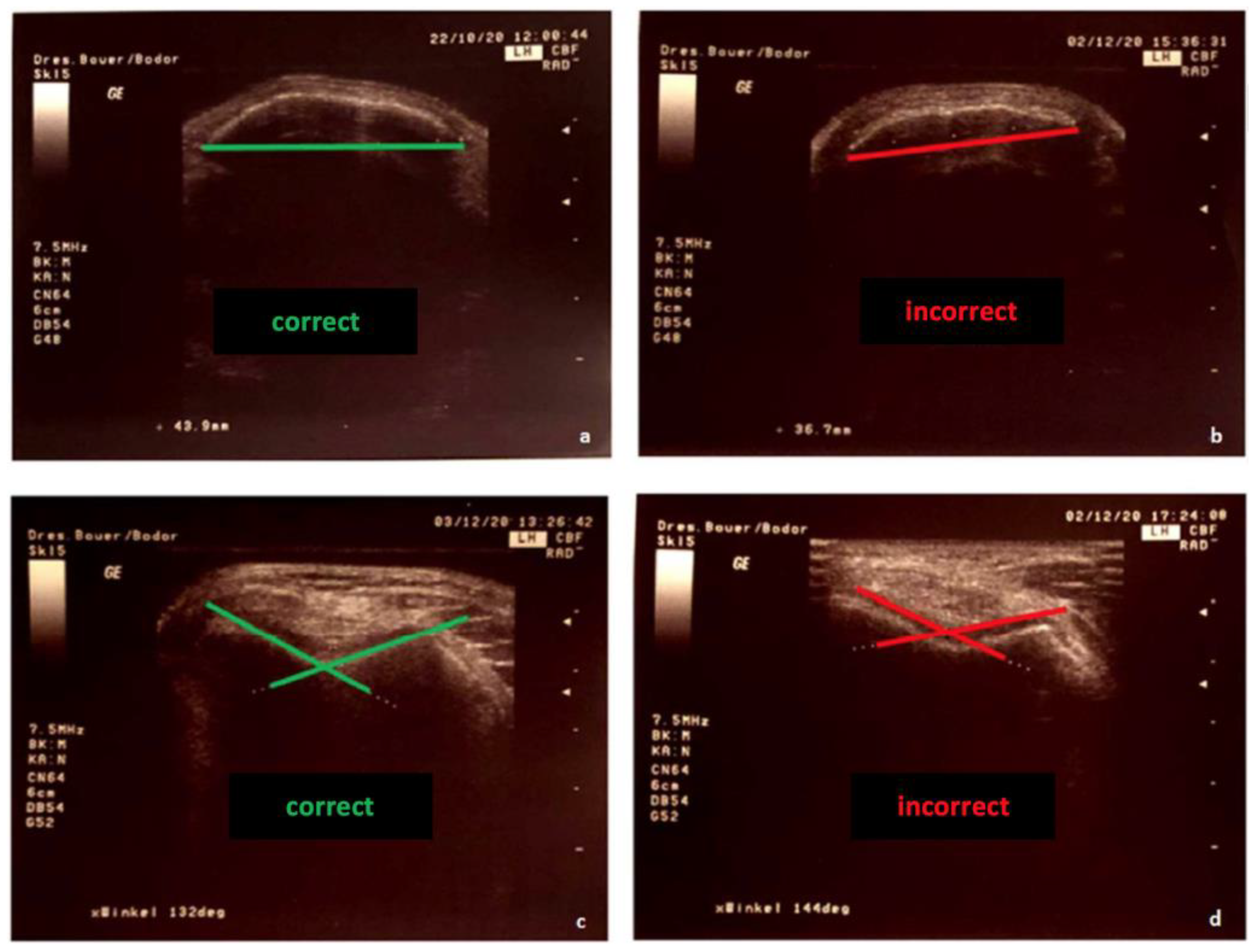
2.2. Measuring Procedure
2.3. Statistical Analysis
3. Results
Intra-Rater Reliability
4. Discussion
4.1. Main Findings of the Study
4.2. Limitations of the Study
4.3. Potential Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Strich, R. Gutachterliche Bewertung der Patellaluxation. Med. Sach. 2017, 113, 24–34. [Google Scholar]
- Wolfe, S.; Varacallo, M.; Thomas, J.D.; Carroll, J.J.; Kahwaji, C.I. Patellar Instability. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Schmeling, A. Aktuelle Aspekte der patellofemoralen Instabilität. In Jahresausgabe der SFA Aktuell; Stifung zur Förderung der Arthroskopie: Tuttlingen, Germany, 2010; Volume 23. [Google Scholar]
- Dejour, H.; Walch, G.; Nove-Josserand, L.; Guier, C. Factors of patellar instability: An anatomic radiographic study. Knee Surg. Sports Traumatol. Arthrosc. 1994, 2, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Jagodzinski, M.; Niemeyer, P.; Zeichen, J.; Balcarek, P. S1 Leitlinie Patella-Luxation. 2014. Available online: https://docplayer.org/93005476-Patella-luxation-leitlinienreport.html (accessed on 14 September 2022).
- Jerosch, J.; Heisel, J.; Tibesku, C.O. Knieendoprothetik-Indikationen, Operationstechnik, Nachbehandlung, Begutachtung; Springer: Berlin/Heidelberg, Germany, 2015; Volume 2. [Google Scholar]
- Dejour, H.; Walch, G.; Neyret, P.; Adeleine, P. La dysplasie de la trochlée fémorale. Rev. Chir. Orthop. 1990, 76, 45–54. [Google Scholar] [PubMed]
- AGA-Komitee-Knie-Patellofemoral. Untersuchungstechniken/Diagnostik des Patellofemoralgelenks; 2015. Available online: https://www.aga-online.ch/fileadmin/user_upload/Themenhefte/Pat_fem_I_Untersuchung.pdf (accessed on 14 September 2022).
- Fitzpatrick, C.K.; Steensen, R.N.; Tumuluri, A.; Trinh, T.; Bentley, J.; Rullkoetter, P.J. Computational analysis of factors contributing to patellar dislocation. J. Orthop. Res. 2016, 34, 444–453. [Google Scholar] [CrossRef] [PubMed]
- Prill, R.; Michel, S. Bestimmung der sagittalen Kniegelenksbeweglichkeit-Zuverlässigkeit gängiger Messverfahren. Man. Med. 2015, 53, 290–294. [Google Scholar] [CrossRef]
- Shrout, P.E. Intraclass correlations: Uses in assessing rater reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef]
- Koo, T.K. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chriopr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Anjum, Z.I.; Bacha, R.; Manzoor, I.; Gilani, S.A. Reliability of knee joint sonography in the evaluation of gouty arthritis. J. Ultrason. 2021, 21, e300–e305. [Google Scholar] [CrossRef]
- Roberts, H.M.; Moore, J.P.; Thom, J.M. The Reliability of Suprapatellar Transverse Sonographic Assessment of Femoral Trochlear Cartilage Thickness in Healthy Adults. J. Ultrasound Med. 2019, 38, 935–946. [Google Scholar] [CrossRef] [Green Version]
- Mohammad, A.; Hefny, A.F.; Abu-Zidan, F.M. Focused Assessment Sonography for Trauma (FAST) training: A systematic review. World J. Surg. 2014, 38, 1009–1018. [Google Scholar] [CrossRef]
- Koppenhaver, S.L.; Parent, E.C.; Teyhen, D.S.; Hebert, J.J.; Fritz, J.M. The effect of averaging multiple trials on measurement error during ultrasound imaging of transversus abdominis and lumbar multifidus muscles in individuals with low back pain. J. Orthop. Sport. Phys. Ther. 2009, 39, 604–611. [Google Scholar] [CrossRef] [PubMed]
- Rathleff, M.S.; Moelgaard, C.; Lykkegaard Olesen, J. Intra- and interobserver reliability of quantitative ultrasound measurement of the plantar fascia. J. Clin. Ultrasound 2011, 39, 128–134. [Google Scholar] [CrossRef]
- Prill, R.; Królikowska, A.; Becker, R.; Karlsson, J. Why there is a need to improve evaluation standards for clinical studies in orthopaedic and sports medicine. Knee Surg. Sport. Traumatol. Arthrosc. Off. J. ESSKA 2022. ePub ahead of print. [Google Scholar] [CrossRef]
- Schulz, R.; Langen, G.; Prill, R.; Cassel, M.; Weissgerber, T.L. Reporting and transparent research practices in sports medicine and orthopaedic clinical trials: A meta-research study. BMJ Open 2022, 12, e059347. [Google Scholar] [CrossRef]
- Prill, R.; Karlsson, J.; Ayeni, O.R.; Becker, R. Author guidelines for conducting systematic reviews and meta-analyses. Knee Surg. Sport. Traumatol. Arthrosc. 2021, 29, 2739–2744. [Google Scholar] [CrossRef]
- Kleinert, S.; Horton, R. How should medical science change? Lancet 2014, 383, 197–198. [Google Scholar] [CrossRef]
- Ioannidis, J.P.A.; Greenland, S.; Hlatky, M.A.; Khoury, M.J.; Macleod, M.R.; Moher, D.; Schulz, K.F.; Tibshirani, R. Increasing value and reducing waste in research design, conduct, and analysis. Lancet 2014, 383, 166–175. [Google Scholar] [CrossRef] [Green Version]
- Lund, H.; Brunnhuber, K.; Juhl, C.; Robinson, K.; Leenaars, M.; Dorch, B.F.; Jamtvedt, G.; Nortvedt, M.W.; Christensen, R.; Chalmers, I. Towards evidence based research. BMJ 2016, 355, i5440. [Google Scholar] [CrossRef] [Green Version]
- Prill, R.; Becker, R.; Schulz, R.; Michel, S.; Hommel, H. No correlation between symmetry-based performance measures and patient-related outcome prior to and after total knee arthroplasty. Knee Surg. Sport. Traumatol. Arthrosc. 2021, 30, 3155–3161. [Google Scholar] [CrossRef]
- Prill, R.; Cruysen, C.; Królikowska, A.; Kopf, S.; Becker, R. Knee Orthotics Do Not Influence Coordinative Skills-A Randomized Controlled Crossover Pilot Trial. J. Pers. Med. 2022, 12, 1509. [Google Scholar] [CrossRef]
- Kohyama, S.; Yoshii, Y.; Okamoto, Y.; Nakajima, T. Advances in Bone Joint Imaging-Metal Artifact Reduction. Diagnostics 2022, 12, 3079. [Google Scholar] [CrossRef]
- Prill, R.; Walter, M.; Królikowska, A.; Becker, R. A Systematic Review of Diagnostic Accuracy and Clinical Applications of Wearable Movement Sensors for Knee Joint Rehabilitation. Sensors 2021, 21, 8221. [Google Scholar] [CrossRef] [PubMed]
- Frings, J.; Dust, T.; Meyer, J.; Krause, M.; Frosch, K.-H.; Adam, G.; Henes, F.O.; Spink, C.; Maas, K.-J. The Influence of Surgical Realignment Procedures on Dynamic Patellar Tracking: A Dynamic Magnetic Resonance Imaging-Controlled Feasibility Study. Diagnostics 2022, 12, 2761. [Google Scholar] [CrossRef] [PubMed]
- Lachowski, K.; Hammermeister, F.; Halenz, B.; Lieckefett, F.; Götze, T.; Prill, R.; Becker, R. The Patellostabilometer: A New Device for Quantification of Mediolateral Patella Displacement. Preprints 2022, 2022120182. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Distribution (n = 12) |
|---|---|
| Female * | 8 (67%) |
| Male * | 4 (33%) |
| Age (years) | 24 ± 2 |
| Body height (cm) | 174.5 ± 8 |
| Body weight (kg) | 67 ± 11 |
| BMI | 19.13 ± 2.67 |
| Participants with patella luxation * | 1 (8,3%) |
| Intra-Rater Reliability; Examiner 1 | ||
|---|---|---|
| Patella Diameter (mm) | Sulcus Angle (°) | |
| Session 1 | x = 40.50 ± 2.81 | x = 131.50 ± 7.03 |
| Session 2 | x = 40.52 ± 2.81 | x = 131.33 ± 7.52 |
| ICC | 0.994 (0.979; 0.998) | 0.976 (0.921; 0.993) |
| Intra-Rater Reliability; Examiner 2 | ||
|---|---|---|
| Patella Diameter (mm) | Sulcus Angle (°) | |
| Session 1 | x = 40.36 ± 2.69 | x = 132.08 ± 7.27 |
| Session 2 | x = 40.54 ± 3.01 | x = 132.58 ± 7.08 |
| ICC | 0.948 (0.836; 0.985) | 0.849 (0.559; 0.954) |
| Reliability between Examiner 1 and Examiner 2 | ||
|---|---|---|
| Patella Diameter (mm) | Sulcus Angle (°) | |
| Session 1 | 0.956 (0.859; 0.987) | 0.856 (0.578; 0.956) |
| Session 2 | 0.989 (0.964; 0.997) | 0.962 (0.805; 0.990) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schlüter, I.-M.; Prill, R.; Królikowska, A.; Cruysen, C.; Becker, R. A Pilot Study on the Reliability of Ultrasound-Based Assessment of Patella Diameter and Sulcus Angle. Diagnostics 2022, 12, 3164. https://doi.org/10.3390/diagnostics12123164
Schlüter I-M, Prill R, Królikowska A, Cruysen C, Becker R. A Pilot Study on the Reliability of Ultrasound-Based Assessment of Patella Diameter and Sulcus Angle. Diagnostics. 2022; 12(12):3164. https://doi.org/10.3390/diagnostics12123164
Chicago/Turabian StyleSchlüter, Isa-Maria, Robert Prill, Aleksandra Królikowska, Caren Cruysen, and Roland Becker. 2022. "A Pilot Study on the Reliability of Ultrasound-Based Assessment of Patella Diameter and Sulcus Angle" Diagnostics 12, no. 12: 3164. https://doi.org/10.3390/diagnostics12123164