
Has COVID-19 Modified the Weight of Known Systemic Inflammation Indexes and the New Ones (MCVL and IIC) in the Assessment as Predictive Factors of Complications and Mortality in Acute Pancreatitis?

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
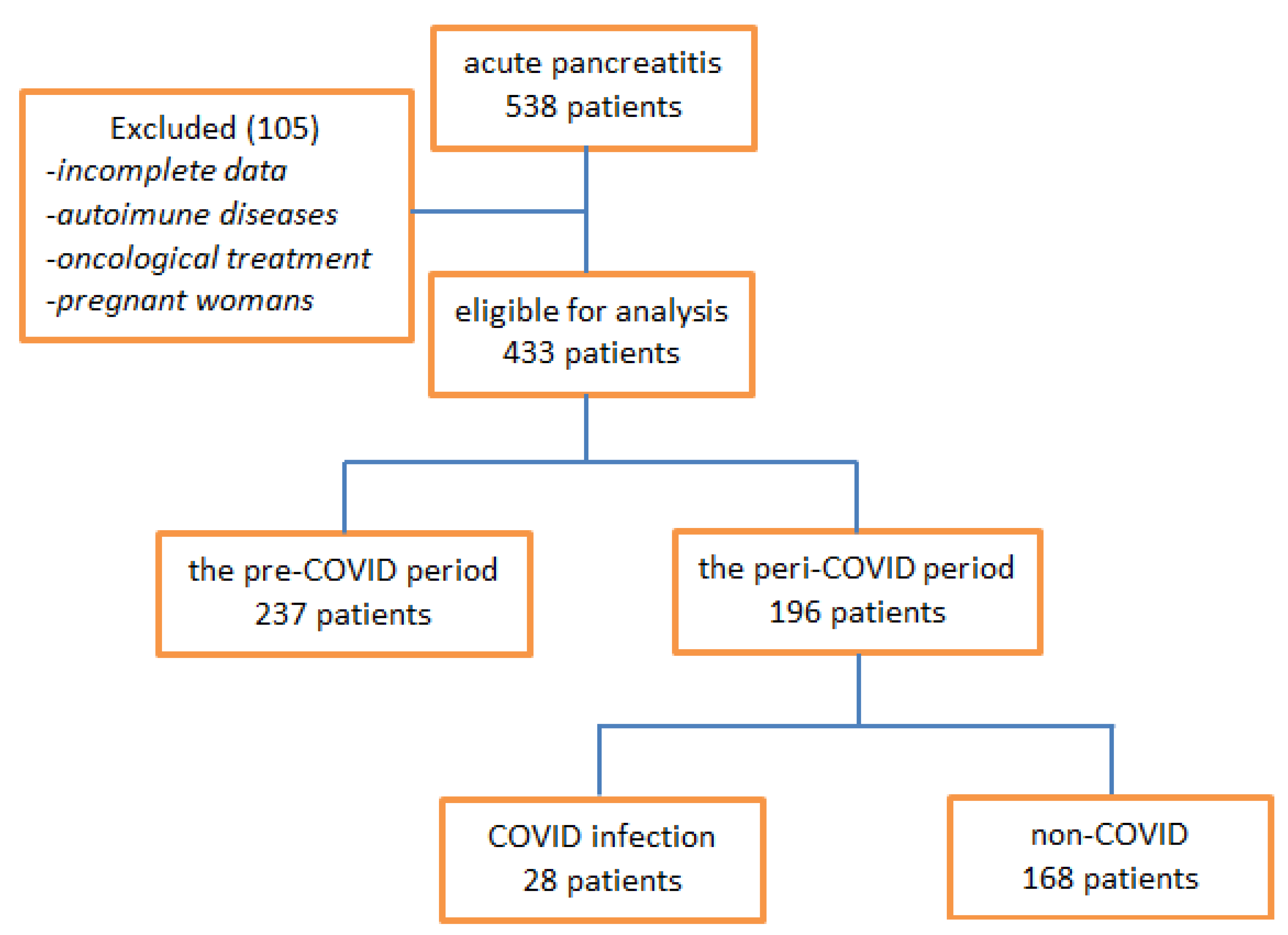
2.1. Study Design
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Patients
3.2. Biological Parameters at Admission
3.3. Levels of Inflammatory Indices Calculated at Admission
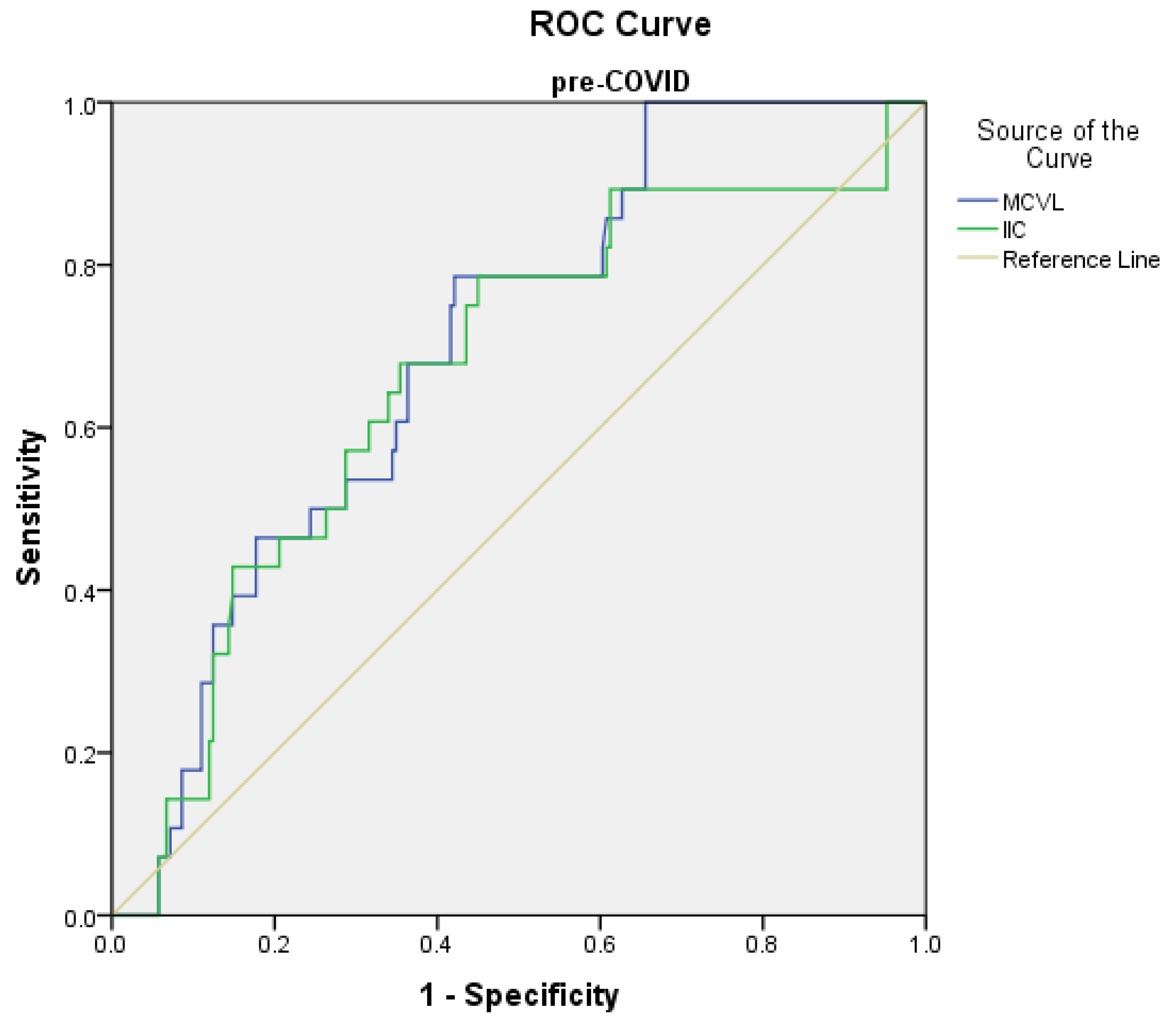
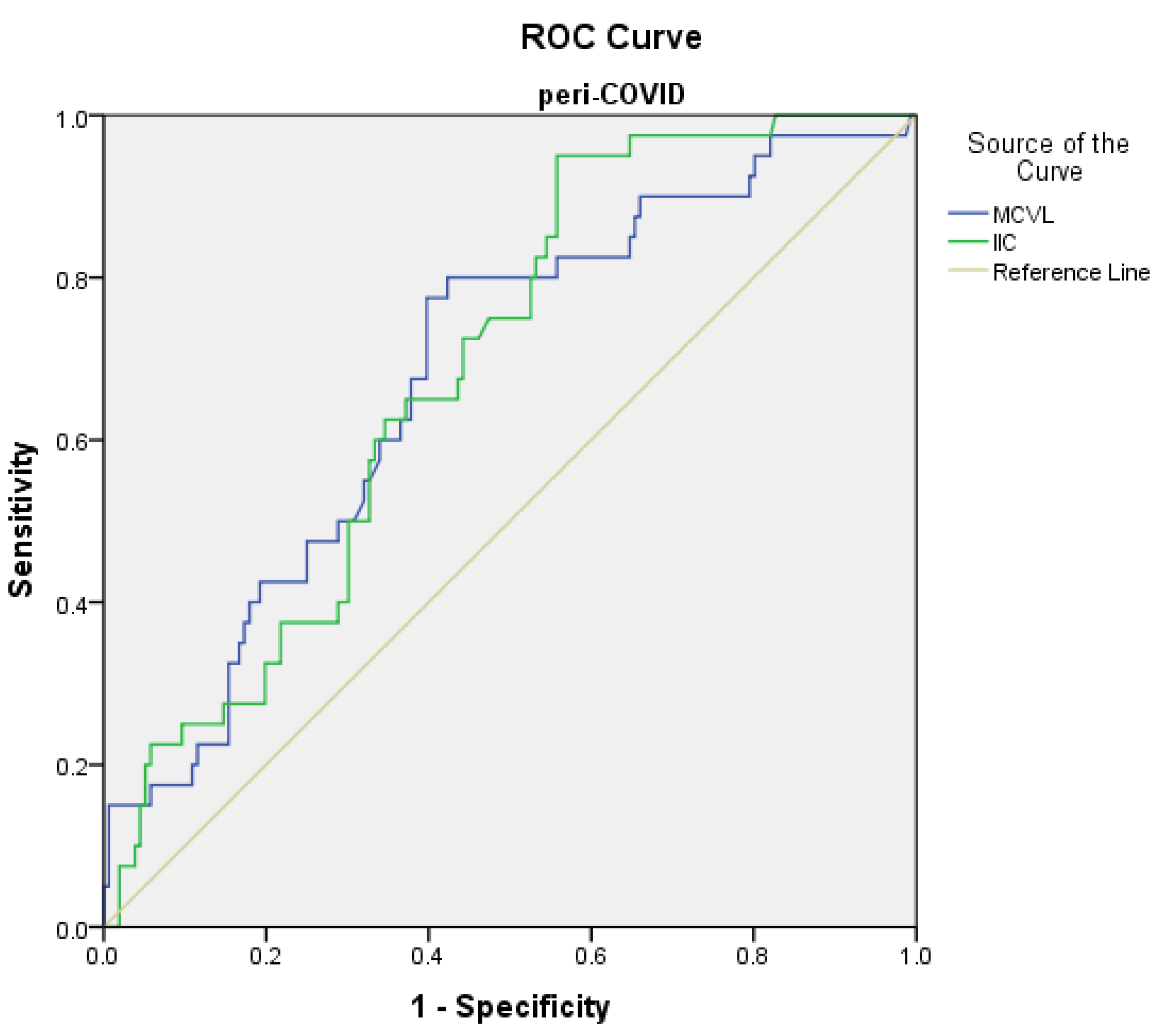
3.4. The Predictive Values of Inflammatory Indices in Terms of Complications with Surgical Risk
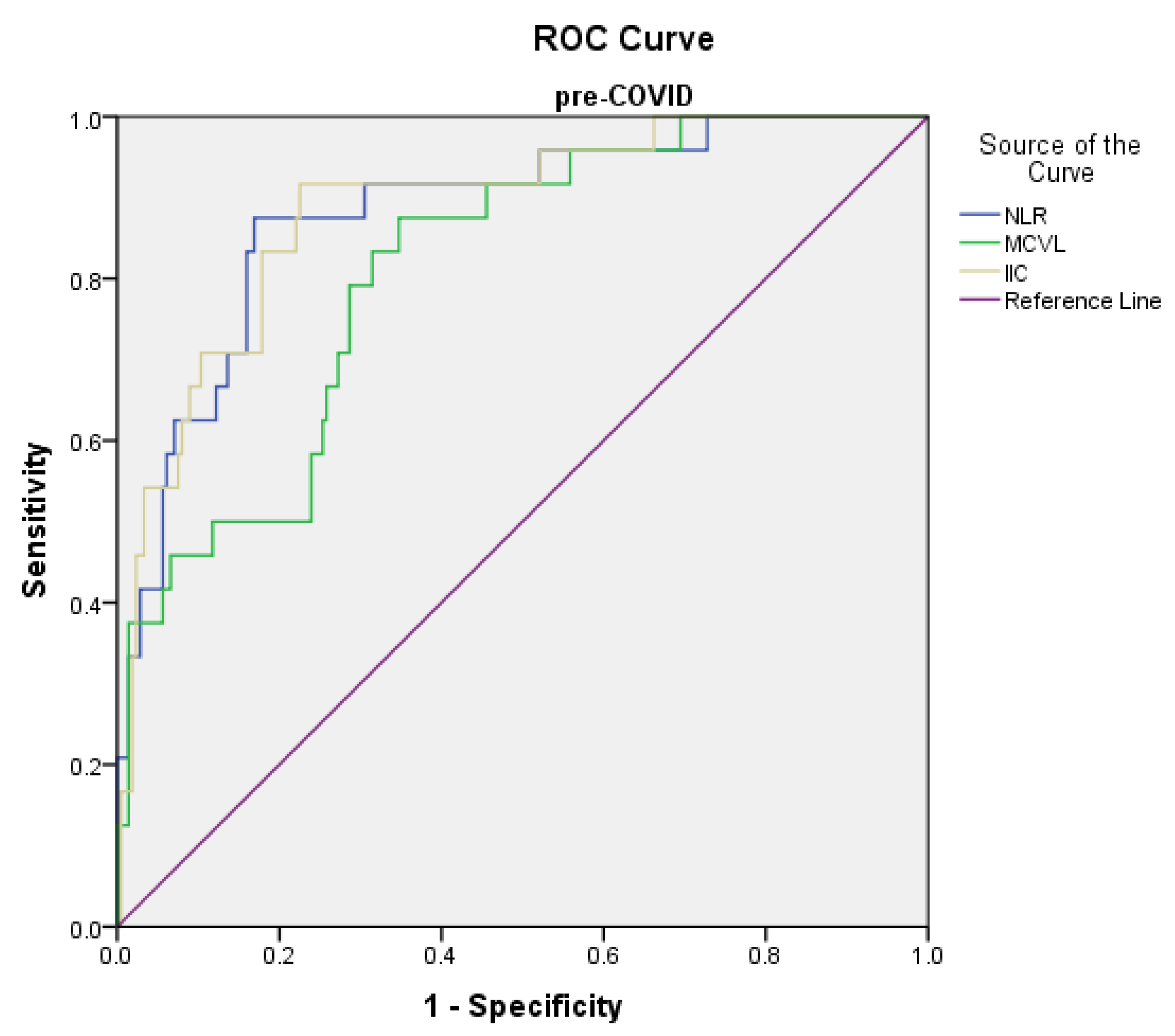
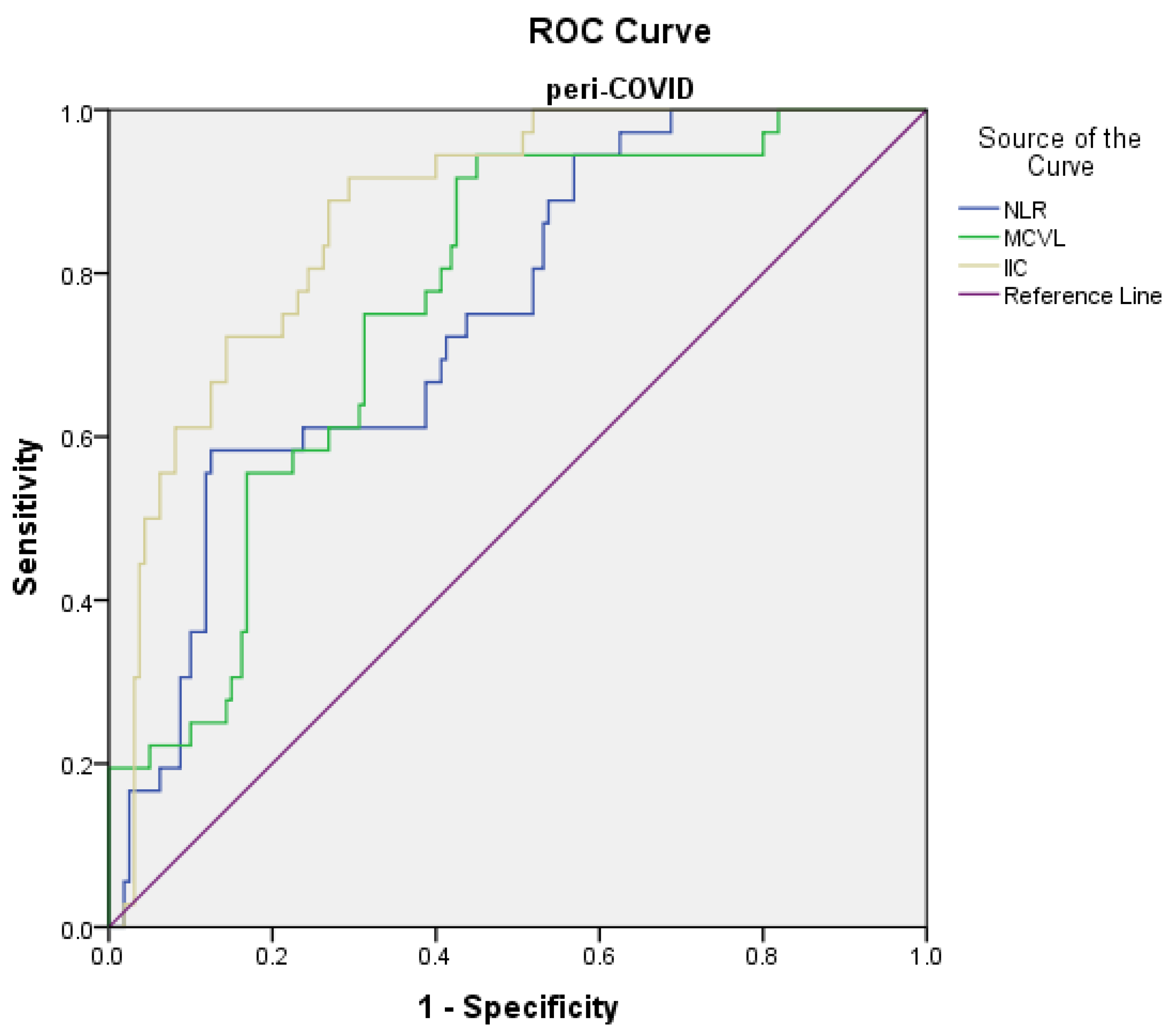
3.5. The Predictive Values of Inflammatory Indices in Mortality
3.6. Univariate and Multivariate Analysis of Predictive Factors for Complications
3.7. Univariate and Multivariate Analysis of Predictive Factors for Mortality
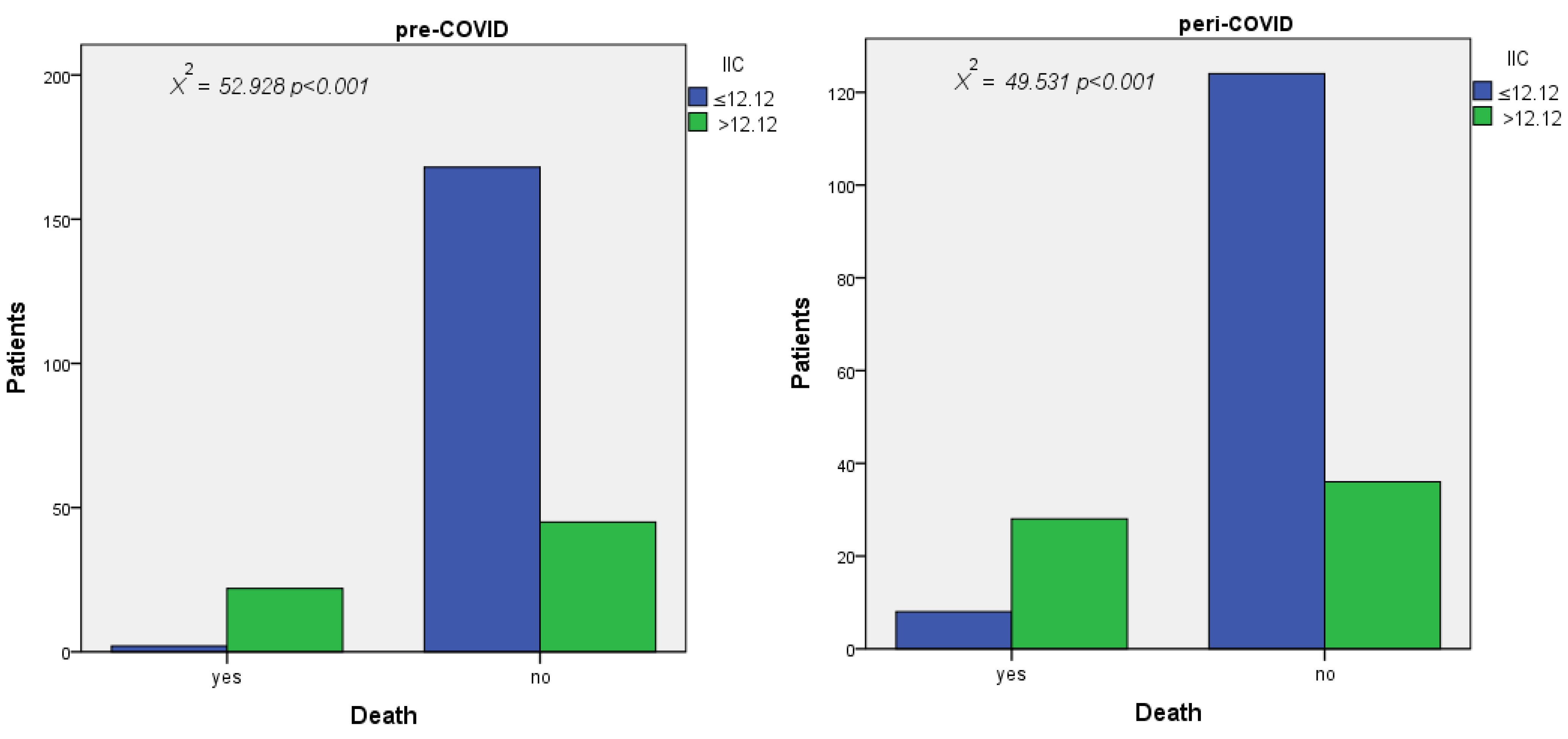
3.8. Results of Pearson Chi-Square Test
4. Discussions
Limitations of the study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sternby, H.; Bolado, F.; Canaval-Zuleta, H.J.; Marra-Lopez, C.; Hernando-Alonso, A.I.; DelVal-Antonana, A.; Adolfo, M.D.; García-Rayado, G.; Rivera-Irigoin, R.; Grau-García, F.J.; et al. Determinants of severity in acute pancreatitis: A nationwide multicenter prospective cohort study. Ann. Surg. 2019, 270, 348–355. [Google Scholar] [CrossRef]
- Stephen, E.R.; Sian, M.R.; Ann, J.; John, G.W.; Tim, H.B.; David, G.S. The incidence andaetiology of acute pancreatitis across Europe. Pancreatology 2017, 17, 155–165. [Google Scholar]
- Khan, J.; Nordback, I.; Sand, J. Serum lipid levels are associated with the severityof acute pancreatitis. Digestion 2013, 87, 223–228. [Google Scholar] [CrossRef]
- Căluianu, E.I.; Alexandru, D.O.; Târtea, E.A.; Georgescu, M.; Mercuţ, D.; Traşcă, E.T.; Iancău, M. Assessment of T- and B-lymphocytes and VEGF-A in acute pancreatitis. Rom. J. Morphol. Embryol. 2017, 58, 481–486. [Google Scholar]
- Ksi, D. Drug-induced acute pancreatitisrelated to medications commonly used in gastroenterology. Eur. J. Intern. Med. 2011, 22, 20–25. [Google Scholar]
- Tinto, A.; Lloyd, D.A.J.; Kang, J.-Y.; Majeed, A.; Ellis, C.; Williamson, R.C.N.; Maxwell, J.D. Acute and chronic pancreatitisdiseases on the rise: A study of hospital admissions in England1989/90–1999/2000. Aliment. Pharmacol. Therapeut. 2002, 16, 2097–2105. [Google Scholar] [CrossRef]
- Petrov, M.S.; Windsor, J.A. Classification of the severity of acutepancreatitis: How many categories make sense? Am. J. Gastroenterol. 2010, 105, 74–76. [Google Scholar] [CrossRef]
- Jaber, S.; Garnier, M.; Asehnoune, K.; Bounes, F.; Buscail, L.; Chevaux, J.B.; Dahyot-Fizelier, C.; Darrivere, L.; Jabaudon, M.; Joannes-Boyau, O.; et al. Guidelines for the management of patients with severe acute pancreatitis, 2021. Anaesth. Crit. Care Pain Med. 2022, 41, 101060. [Google Scholar] [CrossRef]
- Mederos, M.A.; Reber, H.A.; Girgis, M.D. Acute Pancreatitis: A review: A review. JAMA 2021, 325, 382–390. [Google Scholar] [CrossRef]
- Wang, C.; Wang, Z.; Wang, G.; Lau, J.Y.-N.; Zhang, K.; Li, W. COVID-19 in early 2021: Current status and looking forward. Signal Transduct. Target. Ther. 2021, 6, 114. [Google Scholar] [CrossRef]
- Kissler, S.M.; Tedijanto, C.; Goldstein, E.; Grad, Y.H.; Lipsitch, M. Projecting thetransmission dynamics of SARS-CoV-2 through the postpandemic period. Science 2020, 368, 860–868. [Google Scholar] [CrossRef]
- Liu, F.; Long, X.; Zhang, B.; Zhang, W.; Chen, X.; Zhang, Z. Ace2expression in pancreas may cause pancreatic damage after SARSCoV-2 infection. Clin. Gastroenterol. Hepatol. 2020, 18, 2128–2130.e2. [Google Scholar] [CrossRef]
- Suppiah, A.; Malde, D.; Arab, T.; Hamed, M.; Allgar, V.; Smith, A.M.; Morris-Stiff, G. The prognostic value of the neutrophil-lymphocyte ratio (NLR) in acute pancreatitis: Identification of an optimal NLR. J. Gastrointest. Surg. 2013, 17, 675–681. [Google Scholar] [CrossRef]
- Wang, B.; Tang, R.; Wu, S.; Liu, M.; Kanwal, F.; Rehman, M.F.u.; Wu, F.; Zhu, J. Clinical Value of Neutrophil CD64 Index, PCT, and CRP in Acute Pancreatitis Complicated with Abdominal Infection. Diagnostics 2022, 12, 2409. [Google Scholar] [CrossRef]
- García-Núñez, A.; Jiménez-Gómez, G.; Hidalgo-Molina, A.; Córdoba-Doña, J.A.; León-Jiménez, A.; Campos-Caro, A. Inflammatory indices obtained from routine blood tests show an inflammatory state associated with disease progression in engineered stone silicosis patients. Sci. Rep. 2022, 12, 8211. [Google Scholar] [CrossRef]
- Efros, O.; Beit Halevi, T.; Meisel, E.; Soffer, S.; Barda, N.; Cohen, O.; Kenet, G.; Lubetsky, A. The Prognostic Role of Neutrophil-to-Lymphocyte Ratio in Patients Hospitalized with Acute Pulmonary Embolism. J. Clin. Med. 2021, 10, 4058. [Google Scholar] [CrossRef]
- Gasparyan, A.Y.; Ayvazyan, L.; Mukanova, U.; Yessirkepov, M.; Kitas, G.D. The Platelet-to-Lymphocyte Ratio as an Inflammatory Marker in Rheumatic Diseases. Ann. Lab. Med. 2019, 39, 345–357. [Google Scholar] [CrossRef] [Green Version]
- Ghobadi, H.; Mohammadshahi, J.; Javaheri, N.; Fouladi, N.; Mirzazadeh, Y.; Aslani, M.R. Role of leukocytes and systemic inflammation indexes (NLR, PLR, MLP, dNLR, NLPR, AISI, SIR-I, and SII) on admission predicts in-hospital mortality in non-elderly and elderly COVID-19 patients. Front. Med. 2022, 18, 916453. [Google Scholar] [CrossRef]
- Radulescu, D.; Baleanu, V.D.; Padureanu, V.; Radulescu, P.M.; Bordu, S.; Patrascu, S.; Socea, B.; Bacalbasa, N.; Surlin, M.V.; Georgescu, I.; et al. Neutrophil/Lymphocyte Ratio as Predictor of Anastomotic Leak after Gastric Cancer Surgery. Diagnostics 2020, 10, 799. [Google Scholar] [CrossRef]
- Liu, X.; Guan, G.; Cui, X.; Liu, Y.; Liu, Y.; Luo, F. Systemic Immune-Inflammation Index (SII) Can Be an Early Indicator for Predicting the Severity of Acute Pancreatitis: A Retrospective Study. Int. J. Gen. Med. 2021, 14, 9483–9489. [Google Scholar] [CrossRef]
- Fois, A.G.; Paliogiannis, P.; Scano, V.; Cau, S.; Babudieri, S.; Perra, R.; Ruzzittu, G.; Zinellu, E.; Pirina, P.; Carru, C.; et al. The systemic inflammation index on admission predicts in-hospital mortality in COVID-19 patients. Molecules 2020, 25, 5725. [Google Scholar] [CrossRef]
- Moss, P. The T cell immune response against SARS-CoV-2. Nat. Immunol. 2022, 23, 186–193. [Google Scholar] [CrossRef]
- Bollen, T.L.; Singh, V.K.; Maurer, R.; Repas, K.; van Es, H.W.; A Banks, P.; Mortele, K.J. A comparative evaluation of radiologic and clinical scoring systems in the early prediction of severity in acute pancreatitis. Am. J. Gastroenterol. 2011, 107, 612–619. [Google Scholar] [CrossRef]
- Colvin, S.D.; Smith, E.N.; Morgan, D.E.; Porter, K.K. Acute pancreatitis: An update on the revised Atlanta classification. Abdom. Radiol. 2020, 45, 1222–1231. [Google Scholar] [CrossRef]
- David, N.; Zumbo, B. A Cautionary Tale About Levene’s Tests for Equal Variances. J. Educ. Res. Policy Stud. 2007, 7, 1–14. [Google Scholar]
- Wang, F.; Wang, H.; Fan, J.; Zhang, Y.; Wang, H.; Zhao, Q. Pancreatic Injury Patterns in Patients With Coronavirus Disease 19 Pneumonia. Gastroenterology 2020, 159, 367–370. [Google Scholar] [CrossRef]
- Hayati, F.; Lah, N.A.S.N.; Zakaria, A.D.; Rahim, S.S.S.A.; Azizan, N. Issuesand impact of COVID-19 on surgical services in Northern Borneo, Sabah. BJMS 2022, 16, 1–4. [Google Scholar]
- Mărcău, F.-C.; Purec, S.; Niculescu, G. Study on the refusal of vaccination against covid-19 in Romania. Vaccines 2022, 10, 261. [Google Scholar] [CrossRef]
- Mărcău, F.C.; Peptan, C.; Nedelcuță, R.M.; Băleanu, V.D.; Băleanu, A.R.; Niculescu, B. Parental COVID-19 Vaccine Hesitancy for Children in Romania: National Survey. Vaccines 2022, 10, 547. [Google Scholar] [CrossRef]
- O’Brien, C.M.; Jung, K.; Dang, W.; Jang, H.J.; Kielar, A.Z. Collateral damage: The impact of the covid-19 pandemic on acute abdominal emergency presentations. J. Am. Coll. Radiol. 2020, 17, 1443–1449. [Google Scholar] [CrossRef]
- Nodora, J.N.; Gupta, S.; Howard, N.; Motadel, K.; Propst, T.; Rodriguez, J.; Schultz, J.; Velasquez, S.; Castañeda, S.F.; Rabin, B.; et al. The COVID-19 pandemic: Identifying adaptive solutions for colorectal cancer screening in underserved communities. J. Natl. Cancer Inst. 2021, 113, 962–968. [Google Scholar] [CrossRef]
- Galanopoulos, M.; Gkeros, F.; Doukatas, A.; Karianakis, G.; Pontas, C.; Tsoukalas, N.; Viazis, N.; Liatsos, C.; Mantzaris, G.J. COVID-19 pandemic: Pathophysiology and manifestations from the gastrointestinal tract. World J. Gastroenterol. 2020, 26, 4579–4588. [Google Scholar] [CrossRef]
- Hoilat, G.J.; Katta, S. Pancreatic Abscess [Updated 14 August 2022]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022; Available online: https://www.ncbi.nlm.nih.gov/books/NBK560555/ (accessed on 18 October 2022).
- Mirzaei, R.; Goodarzi, P.; Asadi, M.; Soltani, A.; Aljanabi, H.A.A.; Jeda, A.S.; Dashtbin, S.; Jalalifar, S.; Mohammadzadeh, R.; Teimoori, A.; et al. Bacterial co-infections with SARS-CoV-2. IUBMB Life 2020, 72, 2097–2111. [Google Scholar] [CrossRef] [PubMed]
- Lansbury, L.; Lim, B.; Baskaran, V.; Lim, W.S. Co-infections in people with COVID19: A systematic review and meta-analysis. J. Inf. Secur. 2020, 11, 266–275. [Google Scholar]
- Rashid, M.U.; Hussain, I.; Jehanzeb, S.; Ullah, W.; Ali, S.; Jain, A.G.; Khetpal, N.; Ahmad, S. Pancreatic necrosis: Complications and changing trend of treatment. World J. Gastrointest. Surg. 2019, 27, 198–217. [Google Scholar] [CrossRef]
- Petrov, M.S.; Shanbhag, S.; Chakraborty, M.; Phillips, A.R.; Windsor, J.A. Organ failure and infection of pancreatic necrosis as determinants of mortality in patients with acute pancreatitis. Gastroenterology 2010, 139, 813–820. [Google Scholar] [CrossRef]
- Bradley, E.L., III. A clinically based classification system for acute pancreatitis. Summary of the International Symposium on Acute Pancreatitis, Atlanta, Ga, September 11 through 13, 1992. Arch. Surg. 1993, 128, 586–590. [Google Scholar] [CrossRef]
- Tan, J.H.; Chin, W.; Shaikh, A.L.; Zheng, S. Pancreatic pseudocyst: Dilemma of its recent management (Review). Exp. Ther. Med. 2021, 21, 159. [Google Scholar] [CrossRef]
- Farias, G.F.A.; Bernardo, W.M.; De Moura, D.T.H.; Guedes, H.G.; Brunaldi, V.O.; Visconti, T.A.C.; Gonçalves, C.V.T.; Sakai, C.M.; Matuguma, S.E.; Santos, M.E.L.D.; et al. Endoscopic versus surgical treatment for pancreatic pseudocysts: Systematic review and meta-analysis. Medicine 2019, 98, e14255. [Google Scholar] [CrossRef]
- Heider, R.; Meyer, A.A.; Galanko, J.A.; Behrns, K.E. Percutaneous drainage of pancreatic pseudocysts is associated with a higher failure rate than surgical treatment in unselected patients. Ann. Surg. 1999, 229, 781–789. [Google Scholar] [CrossRef]
- Wang, X.; Cui, Z.; Zhang, J.; Li, H.; Zhang, D.; Miao, B.; Cui, Y.; Zhao, E.; Li, Z.; Cui, N. Early Predictive Factors of in Hospital Mortality in Patients with Severe Acute Pancreatitis. Pancreas 2010, 39, 114–115. [Google Scholar] [CrossRef] [PubMed]
- Huguet, E.; Maccallini, G.; Pardini, P.; Hidalgo, M.; Obregon, S.; Botto, F.; Koretzky, M.; Nilsson, P.M.; Ferdinand, K.; Kotliar, C. Reference Values for Neutrophil to Lymphocyte Ratio (NLR), a Biomarker of Cardiovascular Risk, According to Age and Sex in a Latin American Population. Curr. Probl. Cardiol. 2021, 46, 100422. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Z.-Y.; Feng, S.-D.; Chen, G.-P.; Wu, J.-N. Predictive Value of the Neutrophil to Lymphocyte Ratio for Disease Deterioration and Serious Adverse Outcomes in Patients with COVID-19: A Prospective Cohort Study. BMC Infect. Dis. 2021, 21, 80. [Google Scholar] [CrossRef] [PubMed]
- Cupp, M.A.; Cariolou, M.; Tzoulaki, I.; Aune, D.; Evangelou, E.; Berlanga-Taylor, A.J. Neutrophil to lymphocyte ratio and cancer prognosis: An umbrella review of systematic reviews and meta-analyses of observational studies. BMC Med. 2020, 18, 360. [Google Scholar] [CrossRef]
- Forget, P.; Khalifa, C.; Defour, J.P.; Latinne, D.; Van Pel, M.C.; De Kock, M. What is the normal value of the neutrophil-to-lymphocyte ratio? BMC. Res. Notes 2017, 10, 12. [Google Scholar] [CrossRef] [Green Version]
- Yao, J.; Lv, G. Association between red cell distribution width and acute pancreatitis: A cross-sectional study. BMJ Open 2014, 4, e004721. [Google Scholar] [CrossRef]
- Jeon, T.J.; Park, J.Y. Clinical significance of the neutrophil-lymphocyte ratio as an early predictive marker foradverse outcomes in patients with acute pancreatitis. World J. Gastroenterol. 2017, 23, 3883–3889. [Google Scholar] [CrossRef]
- Azab, B.; Jaglall, N.; Atallah, J.P.; Lamet, A.; Raja-Surya, V.; Farah, B.; Lesser, M.; Widmann, W.D. Neutrophillymphocyte ratio as a predictor of adverse outcomes of acute pancreatitis. Pancreatology 2011, 11, 445–452. [Google Scholar] [CrossRef]
- Kutlucan, L.; Kutlucan, A.; Basaran, B.; Dagli, M.; Basturk, A.; Kozanhan, B.; Gur, M.; Senocak, E.; Kos, M. The predictive effect of initial complete blood count of intensive care unit patients on mortality, length of hospitalization, and nosocomial infections. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 1467–1473. [Google Scholar]
- Afdhal, N.; McHutchison, J.; Brown, R.; Jacobson, I.; Manns, M.; Poordad, F.; Weksler, B.; Esteban, R. Thrombocytopenia associated with chronic liver disease. J. Hepatol. 2008, 48, 1000–1007. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.; Liu, A.; Liang, L.; Jiang, J.; Luo, H.; Deng, W.; Lin, G.; Wu, M.; Li, T.; Jiang, Y. Diagnostic value of blood parameters for community-acquired pneumonia. Int. Immunopharmacol. 2018, 64, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.C.; Chan, D.L.; Diakos, C.I.; Engel, A.; Pavlakis, N.; Gill, A.; Clarke, S.J. The Lymphocyte-to-Monocyte Ratio is a Superior Predictor of Overall Survival in Comparison to Established Biomarkers of Resectable Colorectal Cancer. Ann. Surg. 2017, 265, 539–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, D.; Fu, Y.; Tong, W.; Li, F. Prognostic significance of lymphocyte to monocyte ratio in colorectal cancer: A meta-analysis. Int. J. Surg. 2018, 55, 128–138. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Deng, Q.; Zhang, L.; He, S.; Rong, J.; Zheng, F. The pretreatment lymphocyte to monocyte ratio predicts clinical outcome for patients with urological cancers: A meta-analysis. Pathol. Res. Pract. 2019, 215, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Takada, K.; Takamori, S.; Yoneshima, Y.; Tanaka, K.; Okamoto, I.; Shimokawa, M.; Oba, T.; Osoegawa, A.; Tagawa, T.; Takenoyama, M.; et al. Serum markers associated with treatment response and survival in non-small cell lung cancer patients treated with anti-PD-1 therapy. Lung Cancer 2020, 145, 18–26. [Google Scholar] [CrossRef]
- Zhang, Y.; Xing, Z.; Zhou, K.; Jiang, S. The predictive role of systemic inflammation response index (Siri) in the prognosis of stroke patients. Clin. Interv. Aging. 2021, 16, 1997–2007. [Google Scholar] [CrossRef]
- Kim, J.W.; Jung, J.Y.; Suh, C.H.; Kim, H.A. Systemic immune-inflammation index combined with ferritin can serve as a reliable assessment score for adult-onset Still’s disease. Clin. Rheumatol. 2021, 40, 661–668. [Google Scholar] [CrossRef]
- Hu, B.; Yang, X.-R.; Xu, Y.; Sun, Y.-F.; Sun, C.; Guo, W.; Zhang, X.; Wang, W.-M.; Qiu, S.-J.; Zhou, J.; et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin. Cancer Res. 2014, 20, 6212–6222. [Google Scholar] [CrossRef] [Green Version]
- Kleinbongard, P.; Schulz, R.; Rassaf, T.; Lauer, T.; Dejam, A.; Jax, T.; Kumara, I.; Gharini, P.; Kabanova, S.; Özüyaman, B.; et al. Red blood cells express a functional endothelial nitric oxide synthase. Blood 2006, 107, 2943–2951. [Google Scholar] [CrossRef] [Green Version]
- Solak, Y.; Yilmaz, M.I.; Saglam, M.; Demirbas, S.; Verim, S.; Unal, H.U.; Gaipov, A.; Oguz, Y.; Kayrak, M.; Caglar, K.; et al. Mean corpuscular volume is associated with endothelial dysfunction and predicts composite cardiovascular events in patients with chronic kidney disease. Nephrology 2013, 18, 728–735. [Google Scholar] [CrossRef]
- Huang, Y.-L.; Hu, Z.-D.; Liu, S.-J.; Sun, Y.; Qin, Q.; Qin, B.-D.; Zhang, W.-W.; Zhang, J.-R.; Zhong, R.-Q.; Deng, A.-M. Prognostic value of red blood cell distribution width for patients with heart failure: A systematic review and meta-analysis of cohort studies. PLoS ONE 2014, 9, e104861. [Google Scholar] [CrossRef] [Green Version]
- Maruyama, S.; Hirayama, C.; Yamamoto, S.; Koda, M.; Udagawa, A.; Kadowaki, Y.; Inoue, M.; Sagayama, A.; Umeki, K. Red blood cell status in alcoholic and non-alcoholic liver disease. J. Lab. Clin. Med. 2001, 138, 332–337. [Google Scholar] [CrossRef] [PubMed]
- Sloop, G.D.; De Mast, Q.; Pop, G.; Weidman, J.J.; St Cyr, J.A. The Role of Blood Viscosity in Infectious Diseases. Cureus 2020, 24, e7090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Güneş, H.; Kirişci, M.; Turkiye Klinikleri, J. The relationship between whole blood viscosity and deep vein thrombosis. Cardiovasc. Sci. 2018, 30, 6–12. [Google Scholar] [CrossRef] [Green Version]
- Katayama, Y.; Horigome, H.; Takahashi, H.; Tanaka, K.; Yoshinaga, M. Determinants of blood rheology in healthy adults and children using the microchannel array flow analyzer. Clin. Appl. Thromb. Hemost. 2010, 16, 414–421. [Google Scholar] [CrossRef] [PubMed]
- Tavakolpour, S.; Rakhshandehroo, T.; Wei, E.X.; Rashidian, M. Lymphopenia during the COVID-19 infection: What it shows and what can be learned. Immunol. Lett. 2020, 225, 31–32. [Google Scholar] [CrossRef]
- Jie Chee, Y.; Seneviratna, A.; Joo Lim, C.; Chiong, C.X.; Peh, D.S.; Hawkins, R.; Chew, D.E.; Dalan, R. Red cell distribution width is associated with mortality and cardiovascular complications in diabetes mellitus in Singapore. Eur. J. Prev. Cardiol. 2020, 27, 216–219. [Google Scholar] [CrossRef]
- Sadaka, F.; O’Brien, J.; Prakash, S. Red cell distribution width and outcome in patients with septic shock. J. Intensive Care Med. 2013, 28, 307–313. [Google Scholar] [CrossRef]
- Kim, C.H.; Park, J.T.; Kim, E.J.; Han, J.H.; Han, J.S.; Choi, J.Y.; Han, S.H.; Yoo, T.H.; Kim, Y.S.; Kang, S.W.; et al. An increase in red blood cell distribution width from baseline predicts mortality in patients with severe sepsis or septic shock. Crit. Care 2013, 17, R282. [Google Scholar] [CrossRef] [Green Version]
- Xue, J.; Sharma, V.; Habtezion, A. Immune cells and immune-based therapy in pancreatitis. Immunol. Res. 2014, 58, 378–386. [Google Scholar] [CrossRef]
- Takeyama, Y.; Takas, K.; Ueda, T.; Hori, Y.; Goshima, M.; Kuroda, Y. Peripheral lymphocyte reduction in severe acute pancreatitis is caused by apoptotic cell death. J. Gastrointest. Surg 2000, 4, 379–387. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Research Questions |
|---|
| Did the number of patients diagnosed with AP decrease during the COVID-19 pandemic, and what would the explanation for this be? Did the mean values of the already known inflammatory markers NLR, PLR, MLR, dNLR, AISI, SIRI, and SII and the newly introduced MCVL and IIC change during the COVID-19 period? Were there any differences in terms of the number of complications with surgical risk and their degree of operability during the COVID-19 period? Among the already known inflammatory markers NLR, PLR, MLR, dNLR, AISI, SIRI, and SII and the newly introduced MCVL and IIC, which of them can effectively predict the complications with the surgical risk (abscess, necrosis, and pseudocyst) and mortality in the pre-COVID and peri-COVID periods? |
| Variable | Category | Total n = 433 | Pre-COVID n = 237 | Peri-COVID n = 196 | p |
|---|---|---|---|---|---|
| Gender | Men | 225 (51.9%) | 134 (56.5%) | 91 (46.4%) | 0.036 * |
| Women | 208 (48.03) | 103 (43.5%) | 105 (53.6%) | ||
| Age | Men | ||||
| mean ± SD Women | 59.44 ± 15.21 | 57.57 ± 13.43 | 62.19 ± 17.21 | 0.596 | |
| mean ± SD | 62.2 ± 18.07 | 58.78 ± 19.89 | 65.55 ± 15.45 | 0.151 | |
| Total | |||||
| mean ± SD | 60.76 ± 16.68 | 58.09 ± 19.52 | 63.99 ± 16.34 | <0.001 * | |
| Etiology | Biliary | 357 (82.4%) | 195 (82.2%) | 162 (82.6%) | 0.830 |
| Alcohol | 53 (12.2%) | 31 (13%) | 22 (11.2%) | ||
| Unknown | 23 (5.3%) | 11 (4.6%) | 12 (6.1%) | ||
| Form | Mild | 120 (27.7%) | 81 (34.1%) | 39 (19.8%) | 0.072 |
| Moderate | 184 (42.4%) | 86 (36.2%) | 98 (50.0%) | ||
| Severe | 129 (29.7%) | 70 (29.5%) | 59 (30.1%) | ||
| Hours_onset | 35.28 ± 26.4 | 32.99 ± 26.27 | 38.04 ± 26.34 | 0.047 * | |
| Hosp_days | 12.81 ± 13.31 | 14 ± 16.55 | 11.37 ± 7.58 | 0.030 * | |
| Complications | Abscess | 24 (5.5%) | 9 (3.8%) | 15(7.7%) | 0.006 * |
| Necrosis | 29 (6.7%) | 9 (3.8%) | 20 (10.2%) | ||
| Pseudocyst | 15 (3.5%) | 10 (4.2%) | 5 (2.6%) | ||
| Without | 364 (84.1%) | 208 (87.8%) | 156 (79.6%) | ||
| Treatment | Surgical | 25 (5.8%) | 16 (6.8%) | 9 (4.6%) | 0.339 |
| Medical | 408 (94.2%) | 221 (93.2%) | 187 (95.4%) | ||
| Mortality | Discharged | 60 (13.9%) | 24 (10.1%) | 36 (18.4%) | 0.016 * |
| Alive | 373 (86.1%) | 213 (89.9%) | 160 (81.6%) |
| Variable | Category | Peri-COVID n = 196 | COVID-19 n = 28 | Non-COVID-19 n = 168 | p |
|---|---|---|---|---|---|
| Gender | Men | 91 (46.4%) | 19 (67.9%) | 72 (32.8%) | 0.017 * |
| Women | 105 (53.5%) | 9 (32.1%) | 96 (67.2%) | ||
| Age | Men | ||||
| mean ± SD Women | 62.19 ± 17.21 | 47 ± 15.61 | 66.19 ± 15.35 | <0.001 * | |
| mean ± SD | 65.55 ± 15.45 | 48.44 ± 20.71 | 67.16 ± 13.96 | <0.001 * | |
| Total | |||||
| mean ± SD | 63.99 ± 16.34 | 47.46 ± 17.03 | 66.74 ± 14.54 | <0.001 * | |
| Etiology | Biliary | 162 (82.6%) | 13 (46.4%) | 149 (88.7%) | <0.001 * |
| Alcohol | 22 (11.22%) | 8 (28.6%) | 14 (8.3%) | ||
| Unknown | 12 (6.12%) | 7 (25%) | 5 (3%) | ||
| Form | Mild | 39 (30.1%) | 3 (10.7%) | 117 (28.9%) | 0.040 * |
| Moderate | 98 (50%) | 13 (46.4%) | 171 (42.2%) | ||
| Severe | 59 (30.1%) | 12 (42.9%) | 117 (28.9%) | ||
| Hours_onset | 38.04 ± 26.34 | 41 ± 32.27 | 37.55 ± 25.30 | 0.594 | |
| Hosp_days | 11.37 ± 7.58 | 12.36 ± 8.89 | 11.21 ± 7.36 | 0.459 | |
| Complications | Abscess | 15 (7.7%) | 3 (10.7%) | 12 (7.1%) | 0.142 |
| Necrosis | 20 (10.2%) | 5 (17.9%) | 15 (8.9%) | ||
| Pseudocyst | 6 (3.1%) | 2 (7.1%) | 4 (2.4%) | ||
| Without | 155 (79.1%) | 18 (64.3%) | 137 (81.5%) | ||
| Treatment | Surgical | 10 (4.6%) | 1 (3.6%) | 9 (5.4%) | 0.693 |
| Medical | 186 (95.4%) | 27 (96.4%) | 159 (94.6%) | ||
| Mortality | Discharged | 36 (18.4%) | 12 (42.9%) | 24 (14.3%) | 0.007 * |
| Alive | 160 (81.6%) | 16 (57.1%) | 144 (85.7%) |
| Laboratory Parameters | Pre-COVID n = 237 | Peri-COVID n = 196 | p | COVID-19 n = 28 | Non-COVID-19 n = 168 | p |
|---|---|---|---|---|---|---|
| WBC (×103/μL) | 13.25 ± 5.84 | 13.64 ± 6.71 | 0.047 * | 16.07 ± 7.94 | 13.24 ± 6.42 | 0.082 |
| NEU (×103/μL) | 10.81 ± 5.86 | 11.17 ± 6.45 | 0.513 | 12.07 ± 7.48 | 11.02 ± 6.27 | 0.427 |
| LYM (×103/μL) | 1.65 ± 0.94 | 1.53 ± 1.26 | 0.545 | 1.99 ± 1.18 | 1.45 ± 1.26 | 0.037 * |
| MON (×103/μL) | 0.86 ± 0.48 | 0.97 ± 1.21 | 0.242 | 1.84 ± 2.83 | 0.82 ± 0.51 | 0.069 |
| PLT (×103/μL) | 217.50 ± 115.79 | 212.97 ± 113.79 | 0.683 | 237.43 ± 143.72 | 208.89 ± 107.99 | 0.220 |
| MCV (fL) | 89.67 ± 8.68 | 93.57 ± 7.56 | <0.001 * | 96.02 ± 7.85 | 93.17 ± 7.46 | 0.065 |
| RDW | 13.24 ± 1.88 | 13.51 ± 1.48 | 0.101 | 14.20 ± 1.36 | 13.39 ± 1.47 | 0.007 * |
| NLR | 8.46 ± 6.01 | 10.24 ± 8.61 | 0.015 * | 7.85 ± 6.17 | 10.64 ± 8.91 | 0.045 * |
| PLR | 160.35 ± 112.62 | 171.72 ± 105.24 | 0.282 | 114.23 ± 112.56 | 176.30 ± 103.62 | 0.136 |
| MLR | 0.61 ± 0.38 | 0.78 ± 0.77 | 0.005 * | 1.04 ± 1.41 | 0.74 ± 0.60 | 0.278 |
| dNLR | 4.66 ± 2.93 | 6.08 ± 6.68 | 0.006 * | 4.40 ± 3.34 | 6.36 ± 7.05 | 0.152 |
| AISI | 1899.28 ± 2994.76 | 2075.22 ± 280372 | 0.531 | 2352.12 ± 2240.83 | 2029.07 ± 2889.99 | 0.574 |
| SIRI | 7.76 ± 8.13 | 9.28 ± 10.98 | 0.109 | 10.63 ± 11.35 | 9.06 ± 10.93 | 0.438 |
| SII | 1870.92 ± 2000.38 | 2072.69 ± 2193.28 | 0.318 | 1689.64 ± 1460.38 | 2136.53 ± 2289.87 | 0.319 |
| MCVL | 70.26 ± 37.17 | 90.65 ± 67.15 | <0.001 * | 65.04 ± 34.33 | 94.91 ± 70.33 | 0.029 * |
| IIC | 10.73 ± 8.71 | 13.03 ± 10.86 | 0.006 * | 11.04 ± 8.99 | 13.36 ± 11.31 | <0.001 * |
| Laboratory Parameters | With Complications | Without Complications | p | Deceased n = 24 | Alive n = 213 | p |
|---|---|---|---|---|---|---|
| Gender (M/F) | 20/8 (71.4%/28.6%) | 106/103 (50.7%/49.3%) | 0.039 *† | 10/14 41.7%/58.3% | 124/89 58.3%/41.8% | 0.121 † |
| Age | 52.4 ± 2.54 | 58.9 ± 1.15 | 0.072 | 63.25 ± 1.67 | 57.51 ± 1.17 | 0.007 * |
| Hours_onset | 42.86 ± 5.43 | 31.67 ± 1.77 | 0.212 | 44.17 ± 6.56 | 31.73 ± 1.73 | 0.078 |
| Area (U/R) | 13/15 (46.4%/53.6%) | 121/88 (57.9%/42.1%) | 0.250 † | 10/14 41.7%/58.3% | 124/89 58.3%/41.8% | 0.121 † |
| Proteins | 6.24 ± 0.10 | 6.37 ± 0.05 | <0.001 * | 5.83 ± 0.14 | 6.42 ± 0.49 | <0.001 * |
| Amylase | 373.76 ± 29.99 | 462.19 ± 42.17 | 0.694 | 492.54 ± 89.89 | 448.06 ± 40.90 | 0.721 |
| AST | 67.36 ± 45.85 | 142.83 ± 237.83 | 0.001 * | 100.13 ± 135.31 | 123.3 ± 208.16 | 0.466 |
| ALT | 57.90 ± 58.53 | 155.91 ± 222.78 | 0.001 * | 92.33 ± 77.44 | 152.00 ± 222.76 | 0.008 * |
| BT | 2.06 ± 4.26 | 1.76 ± 2.23 | 0.573 | 4.19 ± 5.62 | 1.51 ± 1.66 | 0.029 * |
| Urea | 47.95 ± 4.1 | 53.49 ± 3.04 | 0.48 | 92.12 ± 10.91 | 48.23 ± 2.58 | 0.001 * |
| Creatinine | 1.19 ± 0.16 | 1.35 ± 0.09 | <0.001 * | 2.54 ± 0.36 | 1.19 ± 0.08 | 0.001 * |
| Glucose | 159.24 ± 14.30 | 109.55 ± 4.02 | 0.330 | 100.46 ± 6.87 | 117.4 ± 4.49 | 0.186 |
| INR | 2.22 ± 0.56 | 1.23 ± 0.02 | 0.087 | 2.7 ± 0.64 | 1.19 ± 0.08 | 0.028 * |
| Hb (g/dl) | 13.27 ± 0.55 | 13.01 ± 0.17 | 0.213 | 11.41 ± 0.36 | 13.23 ± 0.18 | 0.001 * |
| Ht (%) | 39.28 ± 1.44 | 38.71 ± 0.50 | <0.001 * | 34.47 ± 1.04 | 39.27 ± 0.50 | 0.002 * |
| WBC (×103/μL) | 13.85 ± 6.92 | 13.17 ± 5.70 | 0.564 | 14.52 ± 5.93 | 13.1 ± 5.83 | 0.259 |
| NEU (×103/μL) | 11.58 ± 6.52 | 10.71 ± 5.78 | 0.459 | 14.38 ± 7.48 | 10.41 ± 5.53 | 0.002 * |
| LYM (×103/μL) | 1.16 ± 0.39 | 1.72 ± 0.79 | <0.001 * | 0.91 ± 0.41 | 1.74 ± 0.94 | <0.001 * |
| MON (×103/μL) | 0.99 ± 0.45 | 0.84 ± 0.48 | 0.122 | 0.90 ± 0.51 | 0.85 ± 0.48 | 0.672 |
| PLT (×103/μL) | 245.32 ± 194.70 | 213.77 ± 100.85 | 0.407 | 207.89 ± 26.22 | 218.58 ± 114.55 | 0.669 |
| MCV (fL) | 89.85 ± 8.95 | 89.64 ± 8.67 | 0.908 | 87.83 ± 8.26 | 89.87 ± 8.72 | 0.277 |
| RDW | 13.52 ± 1.54 | 13.20 ± 1.92 | 0.392 | 14.5 ± 1.30 | 13.09 ± 1.88 | <0.001 * |
| NLR | 10.41 ± 4.85 | 8.20 ± 6.10 | 0.067 | 17.609 ± 7.15 | 7.43 ± 4.9 | <0.001 * |
| PLR | 206.73 ± 108.62 | 154.13 ± 111.95 | 0.020 * | 227.36 ± 119 | 152.8 ± 109.63 | 0.002 * |
| MLR | 0.92 ± 0.48 | 5.03 ± 2.04 | 0.001 * | 0.96 ± 0.45 | 0.57 ± 0.35 | <0.001 * |
| dNLR | 5.03 ± 2.04 | 4.61 ± 3.03 | 0.484 | 8.06 ± 4.82 | 4.28 ± 2.36 | 0.001 * |
| AISI | 3676.43 ± 4063.20 | 1661.20 ± 2747.85 | 0.016 * | 3891.86 ± 4342.95 | 1674.77 ± 2727.18 | 0.022 * |
| SIRI | 11.73 ± 8.02 | 7.23 ± 8.01 | 0.006 * | 14.34 ± 9.69 | 7.02 ± 7.61 | 0.001 * |
| SII | 2963.02 ± 2910.07 | 1724.61 ± 1805.22 | 0.036 * | 3542.55 ± 2775.46 | 1682.57 ± 1807.43 | 0.004 * |
| MCVL | 84.69 ± 25.93 | 13.01 ± 6.75 | 0.028 * | 117.88 ± 52.93 | 64.89 ± 30.80 | <0.001 * |
| IIC | 13.01 ± 6.75 | 10.01 ± 8.89 | 0.088 | 22.62 ± 10.55 | 8.99 ± 7.31 | <0.001 * |
| Laboratory Parameters | With Complications | Without Complications | p | Deceased n = 36 | Alive n = 213 | p |
|---|---|---|---|---|---|---|
| Gender (M/F) | 21/19 (52.5%/47.5%) | 106/103 (52.5%/47.5%) | 0.388 † | 21/15 58.3%/41.7% | 70/90 43.8%/56.3% | 0.113 † |
| Age | 61.73 ± 2.74 | 64.57 ± 1.28 | 0.561 | 63.08 ± 2.73 | 64.19 ± 1.29 | 0.714 |
| Hours_onset | 46.75 ± 4.96 | 35.81 ± 1.96 | 0.091 | 44.08 ± 4.31 | 36.68 ± 2.08 | 0.128 |
| Area (U/R) | 12/28 30%/70% | 85/71 54.5%/45.5% | 0.006 *† | 15/21 41.7%/58.3% | 82/78 51.2%/48.8% | 0.299 † |
| Proteins | 5.89 ± 0.14 | 6.36 ± 0.07 | <0.001 * | 5.81 ± 0.15 | 6.37 ± 0.06 | 0.001 * |
| Amylase | 598.03 ± 100.13 | 597.99 ± 58.47 | 0.513 | 758.03 ± 105.27 | 561.53 ± 57.18 | 0.132 |
| AST | 142.83 ± 237.83 | 57.90 ± 58.53 | 0.910 | 252.17 ± 343.29 | 97.56 ± 106.92 | 0.023 * |
| ALT | 138.21 ± 197.66 | 163.05 ± 188.02 | <0.001 * | 113.73 ± 149.93 | 151.50 ± 185.64 | 0.022 * |
| BT | 2.86 ± 4.76 | 2.37 ± 3.71 | 0.494 | 5.61 ± 7.13 | 1.75 ± 2.20 | 0.003 * |
| Urea | 76.95 ± 8.85 | 50.94 ± 3.73 | 0.600 | 95.17 ± 13.47 | 47.45 ± 2.66 | 0.001 * |
| Creatinine | 2.67 ± 0.41 | 1.2 ± 0.10 | 0.664 | 3.35 ± 0.48 | 1.08 ± 0.07 | <0.001 * |
| Glucose | 145.93 ± 16.02 | 126.63 ± 5.34 | 0.010 * | 185.39 ± 18.24 | 47.45 ± 2.66 | 0.001 * |
| INR | 1.26 ± 0.04 | 1.21 ± 0.03 | 0.924 | 1.39 ± 0.06 | 1.18 ± 0.02 | 0.001 * |
| COVID-19 | 9/32.1% | 31/18.5% | 0.097† | 12/42.9% | 24/14.3% | <0.001 *† |
| Hb (g/dl) | 12.15 ± 0.45 | 13.10 ± 0.16 | 0.044 | 11.77 ± 0.55 | 13.16 ± 0.15 | 0.019 * |
| Ht (%) | 36 ± 1.23 | 38.5 ± 0.61 | 0.364 | 34.17 ± 1.40 | 38.85 ± 0.57 | 0.003 * |
| WBC (×103/μL) | 13.18 ± 6.75 | 10.01 ± 8.89 | 0.629 | 15.82 ± 9.63 | 13.15 ± 5.78 | 0.118 |
| NEU (×103/μL) | 11.09 ± 6.01 | 11.19 ± 6.57 | 0.927 | 13.86 ± 8.94 | 10.57 ± 5.60 | 0.040 * |
| LYM (×103/μL) | 1.18 ± 0.84 | 1.62 ± 1.34 | 0.050 | 0.99 ± 0.50 | 1.65 ± 1.35 | <0.001 * |
| MON (×103/μL) | 0.84 ± 0.37 | 1 ± 1.34 | 0.458 | 0.85 ± 0.44 | 0.99 ± 1.32 | 0.519 |
| PLT (×103/μL) | 191.69 ± 124.72 | 218.42 ± 110.58 | 0.186 | 168.59 ± 125.62 | 22.95 ± 108.90 | 0.009 * |
| MCV (fL) | 99.63 ± 5.12 | 92.02 ± 7.31 | <0.001 * | 103.46 ± 4.70 | 91.35 ± 6.17 | <0.001 * |
| RDW | 13.83 ± 1.79 | 13.43 ± 1.39 | 0.191 | 14.57 ± 1.9 | 13.27 ± 1.26 | <0.001 * |
| NLR | 11.49 ± 7.15 | 9.92 ± 8.95 | 0.305 | 14.86 ± 7.72 | 9.20 ± 8.49 | <0.001 * |
| PLR | 171.01 ± 74.68 | 171.90 ± 111.94 | 0.962 | 175.99 ± 105.89 | 170.76 ± 105.41 | 0.788 |
| MLR | 0.94 ± 0.66 | 0.74 ± 0.79 | 0.138 | 1.07 ± 0.72 | 0.71 ± 0.77 | 0.011 * |
| dNLR | 8.20 ± 12.50 | 5.53 ± 3.92 | 0.191 | 7.18 ± 4.42 | 5.83 ± 7.08 | 0.275 |
| AISI | 1738.37 ± 1569.47 | 2161.59 ± 3078.57 | 0.226 | 2604.11 ± 2810.62 | 1956.22 ± 2797.18 | 0.211 |
| SIRI | 8.84 ± 4.75 | 9.39 ± 12.07 | 0.654 | 12.98 ± 9.39 | 8.45 ± 11.16 | 0.025 * |
| SII | 1865.62 ± 1255.04 | 2125.78 ± 2375.22 | 0.505 | 2477.51 ± 2015.04 | 1981.60 ± 2227.2 | 0.221 |
| MCVL | 128.53 ± 99.54 | 80.93 ± 52.10 | 0.005 * | 146.64 ± 104.99 | 78.05 ± 47.27 | <0.001 * |
| IIC | 17.20 ± 10.28 | 12.20 ± 10.73 | 0.009 * | 12.12 ± 9.24 | 10.99 ± 9.86 | <0.001 * |
| Variable | AUC (95%) | Lowest Value | Highest Value | Cutoff | p | Sensitivity | Specificity | |
|---|---|---|---|---|---|---|---|---|
| NLR | 1 2 | 0.651 0.616 | 0.545 0.535 | 0.756 0.697 | 5.58 6.41 | 0.010 * 0.023 * | 78.6% 80% | 42.2% 44.9% |
| PLR | 1 2 | 0.657 0.678 | 0.545 0.487 | 0.768 0.668 | 97.3 140.27 | 0.007 * 0.130 | 89.3% 72.5% | 34.5% 50.6% |
| MLR | 1 2 | 0.719 0.639 | 0.602 0.550 | 0.837 0.729 | 0.66 0.53 | <0.001 * 0.007 * | 78.6% 75% | 69.9% 49.4% |
| dNLR | 1 2 | 0.600 0.534 | 0.494 0.448 | 0.706 0.619 | 2.82 3.12 | 0.085 0.518 | 78.6% 80% | 29.1% 32.1% |
| AISI | 1 2 | 0.635 0.532 | 0.497 0.439 | 0.774 0.625 | 228.79 358.98 | 0.020 * 0.533 | 78.6% 92.5% | 9.2% 21.2% |
| SIRI | 1 2 | 0.672 0.619 | 0.548 0.534 | 0.797 0.703 | 3.56 2.49 | 0.003 * 0.021 * | 78.6% 92.5% | 44.2% 25% |
| SII | 1 2 | 0.620 0.537 | 0.490 0.445 | 0.749 0.630 | 507.7 756.8 | 0.040 * 0.468 | 89.3% 92.5% | 17% 26.9% |
| MCVL | 1 2 | 0.697 0.681 | 0.609 0.591 | 0.785 0.771 | 64.89 78 | 0.001 * <0.001 * | 78.6% 80% | 56.8% 60.3% |
| IIC | 1 2 | 0.663 0.686 | 0.554 0.605 | 0.772 0.767 | 8.41 10.51 | 0.005* <0.001 * | 78.6% 72.5% | 55.8% 52.6% |
| Variable | AUC(95%) | Lowest Value | Highest Value | Cutoff | p | Sensitivity | Specificity | |
|---|---|---|---|---|---|---|---|---|
| NLR | 1 2 | 0.833 0.743 | 0.811 0.662 | 0.954 0.824 | 11.01 5.93 | <0.001 * <0.001 * | 91.7% 91.7% | 80.5% 42.5% |
| PLR | 1 2 | 0.692 0.557 | 0.569 0.451 | 0.816 0.663 | 102.88 100.38 | 0.002 * 0.287 | 87.5% 86.1% | 38.1% 25.6% |
| MLR | 1 2 | 0.737 0.680 | 0.618 0.575 | 0.855 0.785 | 0.38 0.36 | <0.001 * 0.001 * | 87.5% 86.1% | 29.5% 28.1% |
| dNLR | 1 2 | 0.782 0.673 | 0.681 0.587 | 0.884 0.759 | 3 3.53 | <0.001 * 0.001 * | 87.5% 91.7% | 35.2% 43.1% |
| AISI | 1 2 | 0.632 0.536 | 0.506 0.417 | 0.758 0.656 | 360.26 433.57 | 0.034 * 0.495 | 87.5% 86.1% | 26.7% 23.1% |
| SIRI | 1 2 | 0.754 0.688 | 0.657 0.589 | 0.851 0.787 | 4.26 2.85 | <0.001 * <0.001 * | 87.5% 86.1% | 49% 26.9% |
| SII | 1 2 | 0.747 0.561 | 0.629 0.44 | 0.864 0.681 | 906.21 756.8 | <0.001 * 0.256 | 87.5% 86.1% | 41% 25% |
| MCVL | 1 2 | 0.817 0.762 | 0.739 0.684 | 0.896 0.84 | 72.14 74.9 | <0.001 * <0.001 * | 91.7% 94.4% | 67.6% 57.5% |
| IIC | 1 2 | 0.887 0.870 | 0.819 0.815 | 0.956 0.926 | 13.29 12.12 | <0.001 * <0.001 * | 91.7% 91.7% | 78.6% 72.5% |
| Variable | Univariate Analysis | p Value | Multivariate Analysis | p Value |
|---|---|---|---|---|
| OR | OR | |||
| Proteins | 1.29 (0.75–2.21) | 0.347 | ||
| Creatinine | 1.12 (0.77–1.62) | 0.547 | ||
| AST | 1.004 (0.998–1.010) | 0.153 | ||
| ALT | 1.005(1.000–1.009) | 0.062 | ||
| Ht | 0.99 (0.94–1.04) | 0.703 | ||
| LYM | 3.33 (1.15–7.32) | 0.003 * | 0.05 (0.004–0.785) | 0.032 * |
| PLR | ||||
| ≤97.3 (Ref) | ||||
| >97.3 | 4.56 (1.33–15.63) | 0.016 * | 2.04 (0.53–7.38) | 0.296 |
| MLR | ||||
| ≤0.66 (Ref) | ||||
| >0.66 | 8.69 (3.36–22.48) | <0.001 * | 0.43 (0.19–0.99) | 0.048 * |
| AISI | ||||
| ≤228.79 (Ref) | ||||
| >228.79 | 0.83 (0.23–3.01) | 0.781 | ||
| SIRI | ||||
| ≤3.56 (Ref) >3.56 | 2.99 (1.16–7.69) | 0.023 * | 2.38 (0.90–6.22) | 0.077 |
| SII | ||||
| ≤507.7 (Ref) | ||||
| >507.7 | 1.67 (0.48–5.85) | 0.418 | ||
| MCVL | ||||
| ≤64.89 (Ref) | ||||
| >64.89 | 4.94 (1.92–12.69) | <0.001 * | 3.52 (1.52–8.13) | 0.003 * |
| IIC | ||||
| ≤8.41 (Ref) | ||||
| >8.41 | 5.56 (2.87–10.95) | <0.001 * | 2.80 (1.00–7.84) | 0.049 * |
| Variable | Univariate Analysis | p Value | Multivariate Analysis | p Value |
|---|---|---|---|---|
| OR | OR | |||
| Area | 0.35 (0.17–0.75) | 0.007 * | 0.36 (0.15–0.89) | 0.027 * |
| Proteins | 1.88 (1.22–2.92) | 0.004 * | 1.25 (0.76–2.06) | 0.360 |
| Glucose | 0.99 (0.992–1.001) | 0.150 | ||
| ALT | 1.011(1.004–1.018) | 0.001 * | 1.008 (1.001–1016) | 0.026 * |
| MCV | 0.84 (0.79–0.90) | <0.001 * | 0.86 (0.80–0.92) | <0.001 * |
| MCVL | ||||
| ≤78 (Ref) | ||||
| >78 | 3.51 (1.52–8.11) | <0.001 * | 4.22 (1.46–12.14) | 0.008 * |
| IIC | ||||
| ≤10.51 (Ref) | ||||
| >10.51 | 3.64 (2.07–6.38) | <0.001 * | 1.60 (0.66–3.88) | 0.295 |
| Variable | Univariate Analysis | p Value | Multivariate Analysis | p Value |
|---|---|---|---|---|
| OR | OR | |||
| Age | 0.97 (0.95–1) | 0.109 | ||
| Proteins | 3.11 (1.66–5.82) | 0.001 * | 0.97 (0.20–4.53) | 0.970 |
| Urea | 0.98 (0.97–0.99) | <0.001 * | 0.96 (0.93–0.99) | 0.013 * |
| Creatinine | 0.63 (0.49–0.811) | <0.001 * | 1.24 (0.64–2.39) | 0.517 |
| ALT | 1.002 (0.999–1.006) | 0.212 | ||
| BT | 0.75 (0.65–0.87) | <0.001 * | 0.75 (0.59–0.92) | 0.009 * |
| INR | 0.13 (0.04–0.41) | 0.001 * | 0.48 (0.21–1.09) | 0.083 |
| Hb | 1.46 (1.18–1.82) | 0.001 * | 2.56 (0.50–13.10) | 0.258 |
| Ht | 1.12 (1.04–1.21) | 0.001 * | 0.75 (0.59–0.92) | 0.980 |
| NEU | 0.90 (0.85–0.96) | 0.003 * | 0.85 (0.74–0.98) | 0.025 * |
| LYM | 19.86 (5.15–76.49) | <0.001 * | 7.46 (1.51–36.77) | 0.013 * |
| RDW | 0.73 (0.59–0.89) | 0.003 * | 0.70 (0.47–1.05) | 0.086 |
| NLR | ||||
| ≤11.01 (Ref) | ||||
| >11.01 | 46.14 (10.43–204.15) | <0.001 * | 20.10 (3.12–129.42) | 0.002 * |
| PLR | ||||
| ≤102.88 (Ref) | ||||
| >102.88 | 4.46 (1.29–15.45) | 0.018 * | 0.50 (0.10–2.45) | 0.399 |
| MLR | ||||
| ≤0.38 (Ref) | ||||
| >0.38 | 2.87 (0.82–9.98) | 0.097 | ||
| dNLR | ||||
| ≤3 (Ref) | ||||
| >3 | 4.21 (1.21–14.56) | 0.023 * | 0.63 (0.12–3.21) | 0.582 |
| AISI | ||||
| ≤360.26 (Ref) | ||||
| >360.26 | 2.55 (0.73–8.90) | 0.140 | ||
| SIRI | ||||
| ≤4.26 (Ref) | ||||
| >4.26 | 6.93 (2.00–23.94) | 0.002 * | 0.83 (0.51–1.35) | 0.458 |
| SII | ||||
| ≤906.21 (Ref) | ||||
| >906.21 | 5.02 (1.45–17.36) | 0.011 * | 7.64 (0.62–94.05) | 0.112 |
| MCVL | ||||
| ≤72.14 (Ref) | ||||
| >72.14 | 23.45 (5.36–102.62) | <0.001 * | 5.28 (0.90–30.73) | 0.064 |
| IIC | ||||
| ≤13.29 (Ref) | ||||
| >13.29 | 41.06 (9.30–181.2) | <0.001 * | 18.71 (2.60–134.52) | 0.004 * |
| Variable | Univariate Analysis | p Value | Multivariate Analysis | p Value |
|---|---|---|---|---|
| OR | OR | |||
| Age | 1 (0.98–1.02) | 0.712 | ||
| Proteins | 2.21 (1.37–3.55) | 0.001 * | 9.16 (1.72–48.75) | 0.009 * |
| Urea | 0.98 (0.97–0.99) | <0.001 * | 1.03 (1.00–1.07) | 0.015 * |
| Creatinine | 0 (0.39–0.67) | <0.001 * | 0.07 (0.01–0.30) | <0.001 * |
| AST | 0.998 (0.996–0.999) | 0.002 * | 1.001 (0.997–1.005) | 0.586 |
| ALT | 1.003 (0.999–1.006) | 0.103 | ||
| BT | 0.81 (0.73–0.90) | <0.001 * | 0.71 (0.57–0.89) | 0.003 * |
| INR | 0.23 (0.09–0.59) | 0.002 * | 12.09 (11.97–12.22) | 0.042 |
| COVID-19 | 4.5 (1.89–10.68) | 0.001 * | 53.75 (4.96–581.85) | 0.001 * |
| Hb | 1.32 (1.11–1.56) | 0.001 * | 0.55 (0.21–1.46) | 0.232 |
| Ht | 1.07 (1.02–1.12) | 0.002 * | 1.2 (0.91–1.56) | 0.181 |
| NEU | 0.93 (0.88–0.98) | 0.007 * | 0.71 (0.57–0.88) | 0.002 * |
| LYM | 3.81 (1.85–7.85) | <0.001 * | 1.86 (0.62–5.53) | 0.261 |
| RDW | 0.58 (0.46–0.75) | <0.001 * | 0.85 (0.45–1.61) | 0.634 |
| NLR | ||||
| ≤5.93 (Ref) | ||||
| >5.93 | 8.13 (2.39–27.61) | 0.001 * | 10.24 (1.29–81.17) | 0.028 * |
| MLR | ||||
| ≤0.36 (Ref) | ||||
| >0.36 | 1.95 (0.76–5.01) | 0.163 | ||
| SIRI | ||||
| ≤2.85 (Ref) | ||||
| >2.85 | 2.27 (0.83–6.23) | 0.109 | ||
| MCVL | ||||
| ≤74.9 (Ref) | ||||
| >74.9 | 23 (5.34–99.04) | <0.001 * | 8.92 (5.21–141.58) | 0.041 * |
| IIC | ||||
| ≤12.12 (Ref) | ||||
| >12.12 | 29 (8.46–99.39) | <0.001 * | 27.94 (3.57–218.58) | 0.002 |
| Pre-COVID | Peri-COVID | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Cutoff | OR | Chi-Square | df | P | Cutoff | OR | Chi-Square | df | p | |
| Death | ||||||||||
| IIC | 41.067 | 52.928 | 1 | <0.001* | 29.000 | 50.729 | 1 | <0.001* | ||
| Cutoff ROC | >13.29 | 4.339 | >12.12 | 3.333 | ||||||
| ≤13.29 | 0.106 | ≤12.12 | 0.115 | |||||||
| IIC Adjusted | >12.12 | 37.813 4.086 | 49.531 | 1 | <0.001* | 1 | <0.001* | |||
| Cutoff | ≤12.12 | 0.108 | ||||||||
| Complications | ||||||||||
| MCVL | 4.944 | 12.843 | 1 | <0.001* | 6.065 | 20.672 | 1 | <0.001* | ||
| Cutoff ROC | >64.89 | 1.845 | >78 | 2.013 | ||||||
| ≤64.89 | 0.373 | ≤78 | 0.332 | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Radulescu, P.M.; Davitoiu, D.V.; Baleanu, V.D.; Padureanu, V.; Ramboiu, D.S.; Surlin, M.V.; Bratiloveanu, T.C.; Georgescu, E.F.; Streba, C.T.; Mercut, R.; et al. Has COVID-19 Modified the Weight of Known Systemic Inflammation Indexes and the New Ones (MCVL and IIC) in the Assessment as Predictive Factors of Complications and Mortality in Acute Pancreatitis? Diagnostics 2022, 12, 3118. https://doi.org/10.3390/diagnostics12123118
Radulescu PM, Davitoiu DV, Baleanu VD, Padureanu V, Ramboiu DS, Surlin MV, Bratiloveanu TC, Georgescu EF, Streba CT, Mercut R, et al. Has COVID-19 Modified the Weight of Known Systemic Inflammation Indexes and the New Ones (MCVL and IIC) in the Assessment as Predictive Factors of Complications and Mortality in Acute Pancreatitis? Diagnostics. 2022; 12(12):3118. https://doi.org/10.3390/diagnostics12123118
Chicago/Turabian StyleRadulescu, Patricia Mihaela, Dragos Virgil Davitoiu, Vlad Dumitru Baleanu, Vlad Padureanu, Dumitru Sandu Ramboiu, Marin Valeriu Surlin, Tudor Constantin Bratiloveanu, Eugen Florin Georgescu, Costin Teodor Streba, Razvan Mercut, and et al. 2022. "Has COVID-19 Modified the Weight of Known Systemic Inflammation Indexes and the New Ones (MCVL and IIC) in the Assessment as Predictive Factors of Complications and Mortality in Acute Pancreatitis?" Diagnostics 12, no. 12: 3118. https://doi.org/10.3390/diagnostics12123118