
Outcome of Newborns with Confirmed or Possible SARS-CoV-2 Vertical Infection—A Scoping Review

 , , , and
, , , and
Abstract
:1. Introduction
2. General Aspects of the SARS-CoV-2
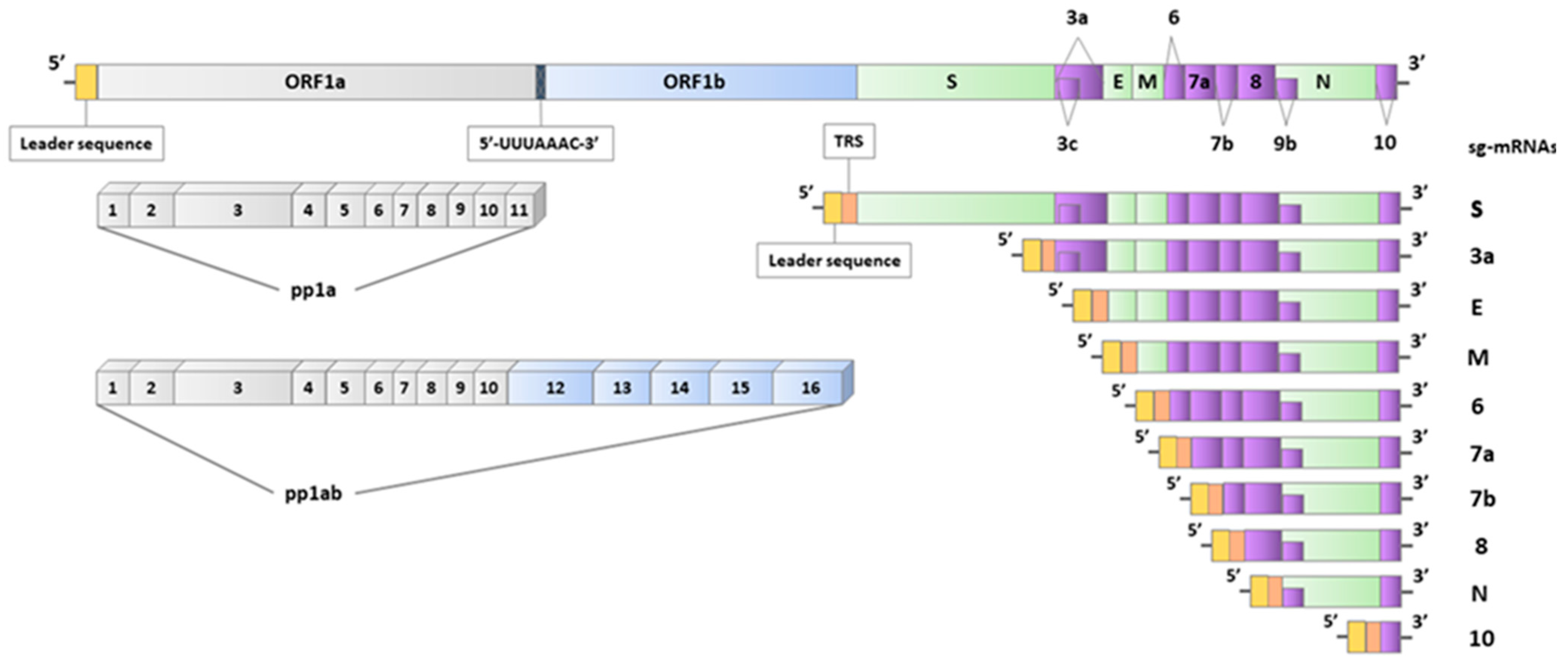
2.1. Genomics of SARS-CoV-2
2.2. Diagnostic Approaches Used to Detect SARS-CoV-2 Infection
2.2.1. Viral Isolation Methods
2.2.2. Protein-Based Detection Methods
2.2.3. Methods Based on the Reverse Transcription Polymerase Chain Reaction
2.2.4. Serology-Based Tests
2.2.5. Diagnostic Tools and Their Role in Demonstrating SARS-CoV-2 Vertical Transmission
3. Maternal-Fetal-Neonatal SARS-CoV-2 Transmission
3.1. Vertical vs. Congenital Transmission of SARS-CoV-2
3.2. Proposed Criteria for Diagnosing Vertical Transmission
3.2.1. Classification Criteria Defined by World Health Organization
3.2.2. Classification System Proposed by the Nordic Federation of Societies of Obstetrics and Gynecology
3.3. Rates and Statistics Concerning the Vertical Transmission
3.4. Intrauterine Fetal Exposure to SARS-CoV-2
3.4.1. Placental Infection with SARS-CoV-2
3.4.2. Fetal Infection with SARS-CoV-2
3.4.3. Intrapartum Fetal Exposure to SARS-CoV-2
4. Review of Available Evidence on Neonatal Outcome in Case of Vertical Transmission
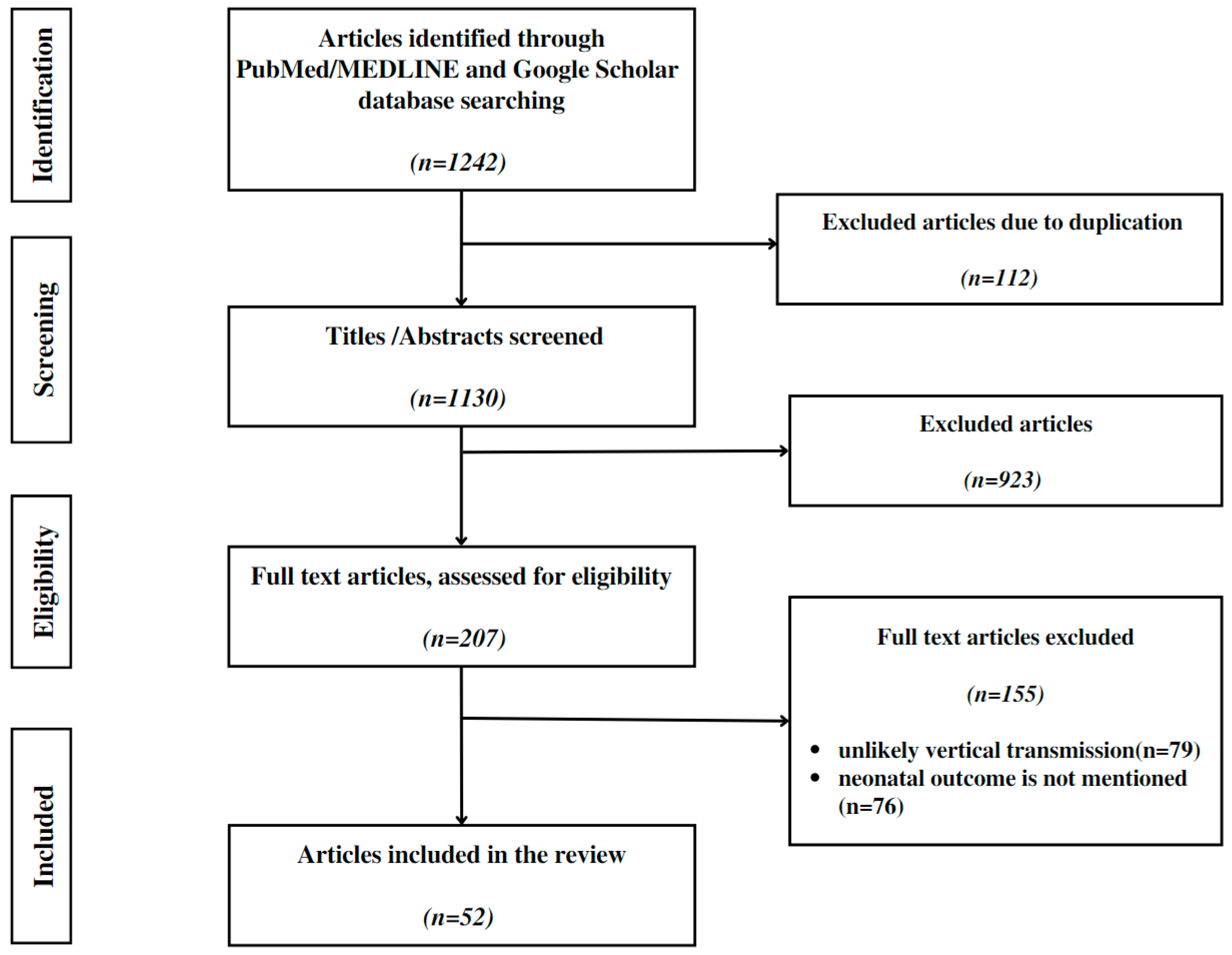
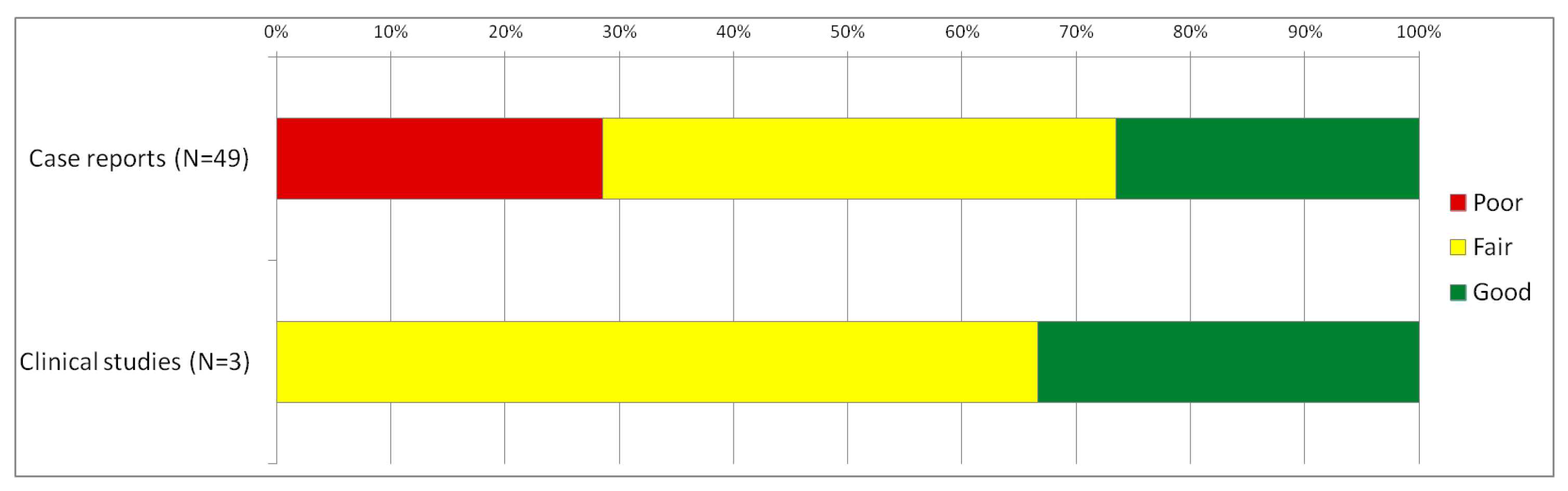
4.1. Review Approach and Methods
- Application of the standard criteria (the WHO or NFSOG criteria) in the attempt to diagnose vertical transmission;
- Delivery after 20 weeks of gestation;
- Delivery using strict infection control and prevention practices;
- Mother–neonate separation at least for 24 h after birth.
4.2. Review Results
4.2.1. Possible Association between Vertical Transmission and Adverse Neonatal Outcome
4.2.2. Livebirths Characteristics
4.2.3. Symptoms of SARS-CoV-2 in Neonates Classified as Confirmed/Possible Vertical Transmission
5. Discussions
5.1. Vertical Transmission, Still an Under-Researched Subject
5.2. Detecting Vertical Transmission, a Multistep-Time Framed Process
5.3. Proposed Algorithm for Diagnosing Vertical Transmission
5.4. Vertical Transmission, from the Mechanism of Action to Clinical Aspects
5.5. Is Screening for Vertical Transmission Necessary?
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zaki, A.M.; Van Boheemen, S.; Bestebroer, T.M.; Osterhaus, A.D.M.E.; Fouchier, R.A.M. Isolation of a Novel Coronavirus from a Man with Pneumonia in Saudi Arabia. N. Engl. J. Med. 2012, 367, 1814–1820. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Lee, J.Y.; Yang, J.S.; Kim, J.W.; Kim, V.N.; Chang, H. The Architecture of SARS-CoV-2 Transcriptome. Cell 2020, 181, 914–921. [Google Scholar] [CrossRef] [PubMed]
- Zhong, N.S.; Zheng, B.J.; Li, Y.M.; Poon, L.L.M.; Xie, Z.H.; Chan, K.H.; Li, P.H.; Tan, S.Y.; Chang, Q.; Xie, J.P.; et al. Epidemiology and cause of severe acute respiratory syndrome (SARS) in Guangdong, People’s Republic of China, in February, 2003. Lancet 2003, 362, 1353–1358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cui, J.; Li, F.; Shi, Z.-L. Origin and evolution of pathogenic coronaviruses. Nat. Rev. Microbiol. 2019, 17, 181–192. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Wu, D.; Yu, Y.; Li, T.; Li, K.; Xiao, M.-M.; Li, Y.; Zhang, Z.-Y.; Zhang, G.-J. Rapid and unamplified identification of COVID-19 with morpholino-modified graphene field-effect transistor nanosensor. Biosens. Bioelectron. 2021, 183, 113206. [Google Scholar] [CrossRef]
- Wong, Y.; Khong, T.; Tan, G. The Effects of COVID-19 on Placenta and Pregnancy: What Do We Know So Far? Diagnostics 2021, 11, 94. [Google Scholar] [CrossRef]
- Moore, K.M.; Suthar, M.S. Comprehensive analysis of COVID-19 during pregnancy. Biochem. Biophys. Res. Commun. 2020, 538, 180–186. [Google Scholar] [CrossRef]
- Zaim, S.; Chong, J.H.; Sankaranarayanan, V.; Harky, A. COVID-19 and Multiorgan Response. Curr. Probl. Cardiol. 2020, 45, 100618. [Google Scholar] [CrossRef]
- Jeganathan, K.; Paul, A.B. Vertical transmission of SARS-CoV-2: A systematic review. Obstet. Med. 2022, 15, 91–98. [Google Scholar] [CrossRef]
- Fenizia, C.; Biasin, M.; Cetin, I.; Vergani, P.; Mileto, D.; Spinillo, A.; Gismondo, M.R.; Perotti, F.; Callegari, C.; Mancon, A.; et al. Analysis of SARS-CoV-2 vertical transmission during pregnancy. Nat. Commun. 2020, 11, 5128. [Google Scholar] [CrossRef]
- Rebutini, P.Z.; Zanchettin, A.C.; Stonoga, E.T.S.; Prá, D.M.M.; de Oliveira, A.L.P.; Dezidério, F.D.S.; Fonseca, A.S.; Dagostini, J.C.H.; Hlatchuk, E.C.; Furuie, I.N.; et al. Association between COVID-19 Pregnant Women Symptoms Severity and Placental Morphologic Features. Front. Immunol. 2021, 12, 685919. [Google Scholar] [CrossRef] [PubMed]
- Tolu, L.B.; Ezeh, A.; Feyissa, G.T. Vertical transmission of Severe Acute Respiratory Syndrome Coronavirus 2: A scoping review. PLoS ONE 2021, 16, e0250196. [Google Scholar] [CrossRef] [PubMed]
- Morotti, D.; Cadamuro, M.; Rigoli, E.; Sonzogni, A.; Gianatti, A.; Parolin, C.; Patanè, L.; Schwartz, D. Molecular Pathology Analysis of SARS-CoV-2 in Syncytiotrophoblast and Hofbauer Cells in Placenta from a Pregnant Woman and Fetus with COVID-19. Pathogens 2021, 10, 479. [Google Scholar] [CrossRef] [PubMed]
- Coronaviridae Study Group of the International Committee on Taxonomy of Viruses. The species Severe acute respiratory syndrome-related coronavirus: Classifying 2019-nCoV and naming it SARS-CoV-2. Nat. Microbiol. 2020, 5, 536–544. [Google Scholar] [CrossRef] [Green Version]
- Storch, G.A. Diagnostic Virology. Clin. Infect. Dis. 2000, 31, 739–751. [Google Scholar] [CrossRef] [Green Version]
- Chen, Q.; He, Z.; Mao, F.; Pei, H.; Cao, H.; Liu, X. Diagnostic technologies for COVID-19: A review. RSC Adv. 2020, 10, 35257–35264. [Google Scholar] [CrossRef]
- LaSala, P.R.; Bufton, K.K.; Ismail, N.; Smith, M.B. Prospective comparison of R-mix™ shell vial system with direct antigen tests and conventional cell culture for respiratory virus detection. J. Clin. Virol. 2007, 38, 210–216. [Google Scholar] [CrossRef]
- Cassedy, A.; Parle-McDermott, A.; O’Kennedy, R. Virus Detection: A Review of the Current and Emerging Molecular and Immunological Methods. Front. Mol. Biosci. 2021, 8, 637559. [Google Scholar] [CrossRef]
- Sciuto, E.L.; Leonardi, A.A.; Calabrese, G.; De Luca, G.; Coniglio, M.A.; Irrera, A.; Conoci, S. Nucleic Acids Analytical Methods for Viral Infection Diagnosis: State-of-the-Art and Future Perspectives. Biomolecules 2021, 11, 1585. [Google Scholar] [CrossRef]
- Louten, J. Detection and Diagnosis of Viral Infections. Essent. Hum. Virol. 2016, 32, 111–132. [Google Scholar] [CrossRef]
- Lino, A.; Cardoso, M.A.; Gonçalves, H.M.R.; Martins-Lopes, P. SARS-CoV-2 Detection Methods. Chemosensors 2022, 10, 221. [Google Scholar] [CrossRef]
- Mardian, Y.; Kosasih, H.; Karyana, M.; Neal, A.; Lau, C.-Y. Review of Current COVID-19 Diagnostics and Opportunities for Further Development. Front. Med. 2021, 8, 615099. [Google Scholar] [CrossRef] [PubMed]
- Metcalf, T.G.; Melnick, J.L.; Estes, M.K. ENVIRONMENTAL VIROLOGY: From Detection of Virus in Sewage and Water by Isolation to Identification by Molecular Biology—A Trip of Over 50 Years. Annu. Rev. Microbiol. 1995, 49, 461–487. [Google Scholar] [CrossRef]
- Liu, F.G.; Chen, G.F.; Zhang, C.Y.; Wang, Y.Y.; Zhou, J. Exponential rolling circle amplification coupled with lateral flow dipstick strips as a rapid and sensitive method for the field detection of Karlodinium veneficum. J. Appl. Phycol. 2019, 31, 2423–2436. [Google Scholar] [CrossRef]
- Lin, C.-Y.; Hwang, D.; Chiu, N.-C.; Weng, L.-C.; Liu, H.-F.; Mu, J.-J.; Liu, C.-P.; Chi, H. Increased Detection of Viruses in Children with Respiratory Tract Infection Using PCR. Int. J. Environ. Res. Public Health 2020, 17, 564. [Google Scholar] [CrossRef] [Green Version]
- Definition and Categorization of the Timing of Mother-To-Child Transmission of SARS-CoV-2. Available online: https://www.who.int/publications-detail-redirect/WHO-2019-nCoV-mother-to-child-transmission-2021.1 (accessed on 3 November 2022).
- Thompson, D.; Lei, Y. Mini review: Recent progress in RT-LAMP enabled COVID-19 detection. Sens. Actuators Rep. 2020, 2, 100017. [Google Scholar] [CrossRef] [PubMed]
- Heijnen, L.; Elsinga, G.; de Graaf, M.; Molenkamp, R.; Koopmans, M.P.; Medema, G. Droplet digital RT-PCR to detect SARS-CoV-2 signature mutations of variants of concern in wastewater. Sci. Total. Environ. 2021, 799, 149456. [Google Scholar] [CrossRef]
- Broughton, J.P.; Deng, X.; Yu, G.; Fasching, C.L.; Servellita, V.; Singh, J.; Miao, X.; Streithorst, J.A.; Granados, A.; Sotomayor-Gonzalez, A.; et al. CRISPR–Cas12-based detection of SARS-CoV-2. Nat. Biotechnol. 2020, 38, 870–874. [Google Scholar] [CrossRef] [Green Version]
- Misra, R.; Acharya, S.; Sushmitha, N. Nanobiosensor-based diagnostic tools in viral infections: Special emphasis on COVID-19. Rev. Med. Virol. 2021, 32, e2267. [Google Scholar] [CrossRef]
- Ibrahim, N.; Jamaluddin, N.; Tan, L.; Yusof, N.M. A Review on the Development of Gold and Silver Nanoparticles-Based Biosensor as a Detection Strategy of Emerging and Pathogenic RNA Virus. Sensors 2021, 21, 5114. [Google Scholar] [CrossRef]
- Du, Y.; Dong, S. Nucleic Acid Biosensors: Recent Advances and Perspectives. Anal. Chem. 2016, 89, 189–215. [Google Scholar] [CrossRef] [PubMed]
- Qiu, G.; Gai, Z.; Tao, Y.; Schmitt, J.; Kullak-Ublick, G.A.; Wang, J. Dual-Functional Plasmonic Photothermal Biosensors for Highly Accurate Severe Acute Respiratory Syndrome Coronavirus 2 Detection. ACS Nano 2020, 14, 5268–5277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Zhang, Z.; Yang, L.; Lian, X.; Xie, Y.; Li, S.; Xin, S.; Cao, P.; Lu, J. The MERS-CoV Receptor DPP4 as a Candidate Binding Target of the SARS-CoV-2 Spike. Iscience 2020, 23, 101160. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.-L.; Kuo, S.-C.; Wang, P.-H. Pregnant women with COVID-19. Taiwan. J. Obstet. Gynecol. 2022, 61, 197–198. [Google Scholar] [CrossRef]
- Wang, P.-H.; Lee, W.-L.; Yang, S.-T.; Tsui, K.-H.; Chang, C.-C.; Lee, F.-K. The impact of COVID-19 in pregnancy: Part I. Clinical presentations and untoward outcomes of pregnant women with COVID-19. J. Chin. Med. Assoc. 2021, 84, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Afzal, A. Molecular diagnostic technologies for COVID-19: Limitations and challenges. J. Adv. Res. 2020, 26, 149–159. [Google Scholar] [CrossRef] [PubMed]
- Bukasov, R.; Dossym, D.; Filchakova, O. Detection of RNA viruses from influenza and HIV to Ebola and SARS-CoV-2: A review. Anal. Methods 2020, 13, 34–55. [Google Scholar] [CrossRef]
- Baek, Y.H.; Um, J.; Antigua, K.J.C.; Park, J.-H.; Kim, Y.; Oh, S.; Kim, Y.-I.; Choi, W.-S.; Kim, S.G.; Jeong, J.H.; et al. Development of a reverse transcription-loop-mediated isothermal amplification as a rapid early-detection method for novel SARS-CoV-2. Emerg. Microbes Infect. 2020, 9, 998–1007. [Google Scholar] [CrossRef] [Green Version]
- Shah, P.S.; Diambomba, Y.; Acharya, G.; Morris, S.K.; Bitnun, A. Classification system and case definition for SARS-CoV-2 infection in pregnant women, fetuses, and neonates. Acta Obstet. Et Gynecol. Scand. 2020, 99, 565–568. [Google Scholar] [CrossRef] [Green Version]
- Peng, Z.; Wang, J.; Mo, Y.; Duan, W.; Xiang, G.; Yi, M.; Bao, L.; Shi, Y. Unlikely SARS-CoV-2 vertical transmission from mother to child: A case report. J. Infect. Public Health 2020, 13, 818–820. [Google Scholar] [CrossRef]
- Pierce-Williams, R.A.; Burd, J.; Felder, L.; Khoury, R.; Bernstein, P.S.; Avila, K.; Penfield, C.A.; Roman, A.S.; DeBolt, C.A.; Stone, J.L.; et al. Clinical course of severe and critical coronavirus disease 2019 in hospitalized pregnancies: A United States cohort study. Am. J. Obstet. Gynecol. MFM 2020, 2, 100134. [Google Scholar] [CrossRef] [PubMed]
- Xiong, X.; Wei, H.; Zhang, Z.; Chang, J.; Ma, X.; Gao, X.; Chen, Q.; Pang, Q. Vaginal delivery report of a healthy neonate born to a convalescent mother with COVID-19. J. Med. Virol. 2020, 92, 1657–1659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.; Guo, J.; Wang, C.; Luo, F.; Yu, X.; Zhang, W.; Li, J.; Zhao, D.; Xu, D.; Gong, Q.; et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: A retrospective review of medical records. Lancet 2020, 395, 809–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breslin, N.; Baptiste, C.; Miller, R.; Fuchs, K.; Goffman, D.; Gyamfi-Bannerman, C.; D’Alton, M. Coronavirus disease 2019 in pregnancy: Early lessons. Am. J. Obstet. Gynecol. MFM 2020, 2, 100111. [Google Scholar] [CrossRef]
- Ferrazzi, E.; Frigerio, L.; Savasi, V.M.; Vergani, P.; Prefumo, F.; Barresi, S.; Bianchi, S.; Ciriello, E.; Facchinetti, F.; Gervasi, M.T.; et al. Vaginal delivery in SARS-CoV-2-infected pregnant women in Northern Italy: A retrospective analysis. BJOG Int. J. Obstet. Gynaecol. 2020, 127, 1116–1121. [Google Scholar] [CrossRef]
- Massoth, L.R.; Desai, N.; Szabolcs, A.; Harris, C.K.; Neyaz, A.; Crotty, R.; Chebib, I.; Rivera, M.N.; Sholl, L.M.; Stone, J.R.; et al. Comparison of RNA In Situ Hybridization and Immunohistochemistry Techniques for the Detection and Locali-zation of SARS-CoV-2 in Human Tissues. Am. J. Surg. Pathol. 2021, 45, 14–24. [Google Scholar] [CrossRef]
- Hosier, H.; Farhadian, S.F.; Morotti, R.A.; Deshmukh, U.; Lu-Culligan, A.; Campbell, K.H.; Yasumoto, Y.; Vogels, C.B.; Casanovas-Massana, A.; Vijayakumar, P.; et al. SARS–CoV-2 infection of the placenta. J. Clin. Investig. 2020, 130, 4947–4953. [Google Scholar] [CrossRef]
- Blumberg, D.A.; Underwood, M.A.; Hedriana, H.L.; Lakshminrusimha, S. Vertical Transmission of SARS-CoV-2: What is the Optimal Definition? Am. J. Perinatol. 2020, 37, 769–772. [Google Scholar] [CrossRef]
- Kotlyar, A.M.; Grechukhina, O.; Chen, A.; Popkhadze, S.; Grimshaw, A.; Tal, O.; Taylor, H.S.; Tal, R. Vertical transmission of coronavirus disease 2019: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2020, 224, 35–53.e3. [Google Scholar] [CrossRef]
- Allotey, J.; Stallings, E.; Bonet, M.; Yap, M.; Chatterjee, S.; Kew, T.; Debenham, L.; Llavall, A.C.; Dixit, A.; Zhou, D.; et al. Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: Living systematic review and meta-analysis. BMJ 2020, 370, m3320. [Google Scholar] [CrossRef]
- Alzamora, M.C.; Paredes, T.; Caceres, D.; Webb, C.M.; Valdez, L.M.; La Rosa, M. Severe COVID-19 during Pregnancy and Possible Vertical Transmission. Am. J. Perinatol. 2020, 37, 861–865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, M.; Wang, Q.; Song, Y.; Zou, M.; Li, Y.; Xu, G.; Yan, T.; Bai, Y. A critical assessment of the potential vertical transmission hypotheses: Implications for research on the early-life infection with COVID-19. Placenta 2021, 115, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.; Fadila, A.P.; Akhtar, A.; Chaudhary, B.K.; Tiwari, L.K.; Chaudhry, N. Vertical transmission and clinical outcome of the neonates born to SARS-CoV-2-positive mothers: A tertiary care hospital-based observational study. BMJ Paediatr. Open 2021, 5, e001193. [Google Scholar] [CrossRef] [PubMed]
- Vivanti, A.J.; Vauloup-Fellous, C.; Prevot, S.; Zupan, V.; Suffee, C.; Do Cao, J.; Benachi, A.; De Luca, D. Transplacental transmission of SARS-CoV-2 infection. Nat. Commun. 2020, 11, 3572. [Google Scholar] [CrossRef]
- Al-Kuraishy, H.M.; Al-Gareeb, A.I.; Albezrah, N.K.A.; Bahaa, H.A.; El-Bouseary, M.M.; Alexiou, A.; Al-Ziyadi, S.H.; Batiha, G.E.-S. Pregnancy and COVID-19: High or low risk of vertical transmission. Clin. Exp. Med. 2022, 17, 1–11. [Google Scholar] [CrossRef]
- Sevilla-Montoya, R.; Hidalgo-Bravo, A.; Estrada-Gutiérrez, G.; Villavicencio-Carrisoza, O.; Leon-Juarez, M.; Villegas-Mota, I.; Espino-Y-Sosa, S.; Monroy-Muñoz, I.E.; Martinez-Portilla, R.J.; Poon, L.C.; et al. Evidence of possible SARS-CoV-2 vertical transmission according to World Health Organization criteria in asymptomatic pregnant women. Ultrasound Obstet. Gynecol. 2021, 58, 900–908. [Google Scholar] [CrossRef]
- Fornari, F. Vertical Transmission of COVID-19-A Systematic Review. J. Pediatr. Perinatol. Child Health 2020, 4, 007–013. [Google Scholar] [CrossRef]
- Massalha, M.; Yefet, E.; Rozenberg, O.; Soltsman, S.; Hasanein, J.; Smolkin, T.; Alter, A.; Perlitz, Y.; Nachum, Z. Vertical transmission and humoral immune response following maternal infection with SARS-CoV-2: A prospective multicenter cohort study. Clin. Microbiol. Infect. 2022, 28, 1258–1262. [Google Scholar] [CrossRef]
- Garcia-Ruiz, I.; Sulleiro, E.; Serrano, B.; Fernandez-Buhigas, I.; Rodriguez-Gomez, L.; Fernandez, D.S.-N.; Anton-Pagarolas, A.; Esperalba-Esquerra, J.; Frick, M.A.; Camba, F.; et al. Congenital infection of SARS-CoV-2 in live-born neonates: A population-based descriptive study. Clin. Microbiol. Infect. 2021, 27, 1521.e1–1521.e5. [Google Scholar] [CrossRef]
- Egloff, C.; Vauloup-Fellous, C.; Picone, O.; Mandelbrot, L.; Roques, P. Evidence and possible mechanisms of rare maternal-fetal transmission of SARS-CoV-2. J. Clin. Virol. 2020, 128, 104447. [Google Scholar] [CrossRef]
- Oncel, M.Y.; Akın, I.M.; Kanburoglu, M.K.; Tayman, C.; Coskun, S.; Narter, F.; Er, I.; Oncan, T.G.; Memisoglu, A.; Cetinkaya, M.; et al. A multicenter study on epidemiological and clinical characteristics of 125 newborns born to women infected with COVID-19 by Turkish Neonatal Society. Eur. J. Pediatr. 2020, 180, 733–742. [Google Scholar] [CrossRef] [PubMed]
- Demirjian, A.; Singh, C.; Tebruegge, M.; Herbert, R.; Draz, N.; Mirfenderesky, M.; Jones, V.; Hinstridge, P.; Seneviratne, R.; Myers, R.; et al. Probable Vertical Transmission of SARS-CoV-2 Infection. Pediatr. Infect. Dis. J. 2020, 39, e257–e260. [Google Scholar] [CrossRef]
- Valdés, G.; Neves, L.; Anton, L.; Corthorn, J.; Chacón, C.; Germain, A.; Merrill, D.; Ferrario, C.; Sarao, R.; Penninger, J.; et al. Distribution of Angiotensin-(1-7) and ACE2 in Human Placentas of Normal and Pathological Pregnancies. Placenta 2006, 27, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Zhao, Z.; Wang, Y.; Zhou, Y.; Ma, Y.; Zuo, W. Single-Cell RNA Expression Profiling of ACE2, the Receptor of SARS-CoV-2. Am. J. Respir. Crit. Care Med. 2020, 202, 756–759. [Google Scholar] [CrossRef] [PubMed]
- Van Der Made, C.I.; Simons, A.; Schuurs-Hoeijmakers, J.; Heuvel, G.V.D.; Mantere, T.; Kersten, S.; Van Deuren, R.C.; Steehouwer, M.; Van Reijmersdal, S.V.; Jaeger, M.; et al. Presence of Genetic Variants among Young Men with Severe COVID-19. JAMA 2020, 324, 663. [Google Scholar] [CrossRef] [PubMed]
- Mourad, M.; Jacob, T.; Sadovsky, E.; Bejerano, S.; Simone, G.S.-D.; Bagalkot, T.R.; Zucker, J.; Yin, M.T.; Chang, J.Y.; Liu, L.; et al. Placental response to maternal SARS-CoV-2 infection. Sci. Rep. 2021, 11, 14390. [Google Scholar] [CrossRef]
- Zhang, Y.; Qin, L.; Zhao, Y.; Zhang, P.; Xu, B.; Li, K.; Liang, L.; Zhang, C.; Dai, Y.; Feng, Y.; et al. Interferon-Induced Transmembrane Protein 3 Genetic Variant rs12252-C Associated with Disease Severity in Coronavirus Disease 2019. J. Infect. Dis. 2020, 222, 34–37. [Google Scholar] [CrossRef]
- Marton, T.; Hargitai, B.; Hunter, K.; Pugh, M.; Murray, P. Massive Perivillous Fibrin Deposition and Chronic Histiocytic Intervillositis a Complication of SARS-CoV-2 Infection. Pediatr. Dev. Pathol. 2021, 24, 450–454. [Google Scholar] [CrossRef]
- Li, M.; Chen, L.; Zhang, J.; Xiong, C.; Li, X. The SARS-CoV-2 receptor ACE2 expression of maternal-fetal interface and fetal organs by single-cell transcriptome study. PLoS ONE 2020, 15, e0230295. [Google Scholar] [CrossRef] [Green Version]
- Piras, M.; Cau, F.; Manchia, M.; Paribello, P.; Saba, L.; Suri, J.S.; Faa, G.; Pichiri, G.; Cerrone, G.; Scano, A.; et al. Strong ACE-2 expression in the choroidal vessels: Do high choroid plexuses serve as a gateway for SARS-CoV-2 infection on the human brain? Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 3025–3029. [Google Scholar] [CrossRef]
- Atarod, Z.; Zamaniyan, M.; Moosazadeh, M.; Valadan, R.; Soleimanirad, S.M.; Gordani, N. Investigation of vaginal and rectal swabs of women infected with COVID-19 in two hospitals covered by Mazandaran University of Medical Sciences, 2020. J. Obstet. Gynaecol. 2022, 42, 2225–2229. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Perez, O.; Vouga, M.; Melguizo, S.C.; Acebal, L.F.; Panchaud, A.; Muñoz-Chápuli, M.; Baud, D. Association Between Mode of Delivery among Pregnant Women with COVID-19 and Maternal and Neonatal Outcomes in Spain. JAMA 2020, 324, 296–299. [Google Scholar] [CrossRef] [PubMed]
- Cai, J.; Tang, M.; Gao, Y.; Zhang, H.; Yang, Y.; Zhang, D.; Wang, H.; Liang, H.; Zhang, R.; Wu, B. Cesarean Section or Vaginal Delivery to Prevent Possible Vertical Transmission from a Pregnant Mother Confirmed with COVID-19 to a Neonate: A Systematic Review. Front. Med. 2021, 8, 634949. [Google Scholar] [CrossRef]
- Craina, M.; Iacob, D.; Dima, M.; Bernad, S.; Silaghi, C.; Moza, A.; Pantea, M.; Gluhovschi, A.; Bernad, E. Clinical, Laboratory, and Imaging Findings of Pregnant Women with Possible Vertical Transmission of SARS-CoV-2—Case Series. Int. J. Environ. Res. Public Health 2022, 19, 10916. [Google Scholar] [CrossRef]
- Chi, H.; Chiu, N.-C.; Tai, Y.-L.; Chang, H.-Y.; Lin, C.-H.; Sung, Y.-H.; Tseng, C.-Y.; Liu, L.Y.-M.; Lin, C.-Y. Clinical features of neonates born to mothers with coronavirus disease-2019: A systematic review of 105 neonates. J. Microbiol. Immunol. Infect. 2020, 54, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Al-Lawama, M.; Badran, E.; Ghanim, N.; Irsheid, A.; Qtaishat, H.; Al-Ammouri, I.; Al-Zyadneh, E.; Al-Iede, M.; Daher, A.H.; Bakri, F.G.; et al. Perinatal Transmission and Clinical Outcomes of Neonates Born to SARS-CoV-2-Positive Mothers. J. Clin. Med. Res. 2021, 13, 420–424. [Google Scholar] [CrossRef] [PubMed]
- Ishqeir, A.; Nir, A.; Aptowitzer, I.; Godfrey, M.; Pediatric Cardiology Unit, Shaare Zedek Medical Center, Jerusalem, Israel. Increased incidence of Persistent Pulmonary Hypertension of the Newborn following third trimester maternal COVID-19 infection. Eur. Heart J. 2021, 42, ehab724.1843. [Google Scholar] [CrossRef]
- Pawar, R.; Gavade, V.; Patil, N.; Mali, V.; Girwalkar, A.; Tarkasband, V.; Loya, S.; Chavan, A.; Nanivadekar, N.; Shinde, R.; et al. Neonatal Multisystem Inflammatory Syndrome (MIS-N) Associated with Prenatal Maternal SARS-CoV-2: A Case Series. Children 2021, 8, 572. [Google Scholar] [CrossRef]
- Khalil, A.; Blakeway, H.; Samara, A.; O’Brien, P. COVID-19 and stillbirth: Direct vs indirect effect of the pandemic. Ultrasound Obstet. Gynecol. 2022, 59, 288–295. [Google Scholar] [CrossRef]
- Halici-Ozturk, F.; Ocal, F.D.; Aydin, S.; Tanacan, A.; Ayhan, S.G.; Altinboga, O.; Dinc, B.; Moraloglu, T.; Sahin, D. Investigating the risk of maternal-fetal transmission of SARS-CoV-2 in early pregnancy. Placenta 2021, 106, 25–29. [Google Scholar] [CrossRef]
- Edlow, A.G.; Li, J.Z.; Collier, A.-R.Y.; Atyeo, C.; James, K.E.; Boatin, A.A.; Gray, K.J.; Bordt, E.A.; Shook, L.L.; Yonker, L.M.; et al. Assessment of Maternal and Neonatal SARS-CoV-2 Viral Load, Transplacental Antibody Transfer, and Placental Pathology in Pregnancies During the COVID-19 Pandemic. JAMA Netw. Open 2020, 3, e2030455. [Google Scholar] [CrossRef] [PubMed]
- Deniz, M.; Tezer, H. Vertical transmission of SARS CoV-2: A systematic review. J. Matern. Neonatal Med. 2020, 35, 2655–2662. [Google Scholar] [CrossRef]
- Iacob, D.; Enatescu, I.; Dima, M.; Bernad, E.; Pantea, M.; Bozgan, D.; Bernad, S.; Craina, M. First Neonates with Vertical Transmission of SARS-CoV-2 Infection in Late Pregnancy in West Part of Romania: Case Series. Diagnostics 2022, 12, 1668. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, M.D.J.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for conducting systematic scoping reviews. Int. J. Evid. Based Healthc. 2015, 13, 141–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inplasy Protocol 4294, INPLASY, 23 December 2022. Available online: https://inplasy.com/inplasy-2022-12-0093/ (accessed on 24 December 2022).
- Murad, M.H.; Sultan, S.; Haffar, S.; Bazerbachi, F. Methodological quality and synthesis of case series and case reports. BMJ Evid. Based Med. 2018, 23, 60–63. [Google Scholar] [CrossRef] [Green Version]
- Lo, C.K.-L.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef] [Green Version]
- Metodiev, D.; Ruseva, M.; Parvanov, D.; Ganeva, R.; Handzhiyska, M.; Vidolova, N.; Stamenov, G. Vertical Transmission of SARS-CoV-2 Infection and Miscarriage in the Second Trimester: Report of an Immunohistochemically Proven Case. Clin. Pract. 2022, 14, 579–590. [Google Scholar] [CrossRef]
- Kato, M.; Yamaguchi, K.; Maegawa, Y.; Komine-Aizawa, S.; Kondo, E.; Ikeda, T. Intrauterine fetal death during COVID-19 pregnancy: Typical fetal heart rate changes, coagulopathy, and placentitis. J. Obstet. Gynaecol. Res. 2022, 48, 1978–1982. [Google Scholar] [CrossRef]
- Borges Charepe, N.; Queirós, A.; Alves, M.J.; Serrano, F.; Ferreira, C.; Gamito, M.; Smet, C.; Silva, V.; Féria, B.; Laranjo, M.; et al. One Year of COVID-19 in Pregnancy: A National Wide Collaborative Study. Acta Med. Port. 2022, 35, 357–366. [Google Scholar] [CrossRef] [PubMed]
- Patanè, L.; Cadamuro, M.; Massazza, G.; Pirola, S.; Stagnati, V.; Comerio, C.; Carnelli, M.; Arosio, M.; Callegaro, A.P.; Tebaldi, P.; et al. Evidence of vertical transmission of SARS-CoV-2 and interstitial pneumonia in second-trimester twin stillbirth in asymp-tomatic woman. Case report and review of the literature. Am. J. Obstet. Gynecol. MFM 2022, 4, 100589. [Google Scholar] [CrossRef] [PubMed]
- Zaigham, M.; Gisselsson, D.; Sand, A.; Wikström, A.; von Wowern, E.; Schwartz, D.A.; Iorizzo, L.; Nelander, M.; Blomberg, M.; Papadogiannakis, N.; et al. Clinical-pathological features in placentas of pregnancies with SARS-CoV-2 infection and adverse outcome: Case series with and without congenital transmission. BJOG Int. J. Obstet. Gynaecol. 2022, 129, 1361–1374. [Google Scholar] [CrossRef] [PubMed]
- Lesieur, E.; Torrents, J.; Fina, F.; Zandotti, C.; Blanc, J.; Collardeau-Frachon, S.; Gazin, C.; Sirgant, D.; Mezouar, S.; Otmani Idrissi, M.; et al. Congenital Infection of Severe Acute Respiratory Syndrome Coronavirus 2 with Intrauterine Fetal Death: A Clinicopathological Study with Molecular Analysis. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2022, 75, e1092–e1100. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, B.; O’Donoghue, K.; McEntagart, N.; Gillan, J.E.; Kelehan, P.; O’Leary, J.; Downey, P.; Dean, J.; De Gascun, C.F. Fetal Deaths in Ireland Due to SARS-CoV-2 Placentitis Caused by SARS-CoV-2 Alpha. Arch. Pathol. Lab. Med. 2022, 146, 529–537. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, M.D.F.C.; Pavon, J.A.R.; Napoleão, A.C.B.; Figueiredo, G.M.D.P.; Florêncio, P.C.B.; Arantes, R.B.d.S.; Rizzo, P.S.; Carmo, M.A.M.V.; Nakazato, L.; Dutra, V.; et al. Clinical and genomic data of SARS-CoV-2 detected in maternal–fetal interface during the first wave of infection in Brazil. Microbes Infect. 2022, 24, 104949. [Google Scholar] [CrossRef] [PubMed]
- Richtmann, R.; Torloni, M.R.; Oyamada Otani, A.R.; Levi, J.E.; Crema Tobara, M.; de Almeida Silva, C.; Dias, L.; Miglioli-Galvão, L.; Martins Silva, P.; Macoto Kondo, M. Fetal deaths in pregnancies with SARS-CoV-2 infection in Brazil: A case series. Case Rep. Womens Health 2020, 27, e00243. [Google Scholar] [CrossRef] [PubMed]
- Pulinx, B.; Kieffer, D.; Michiels, I.; Petermans, S.; Strybol, D.; Delvaux, S.; Baldewijns, M.; Raymaekers, M.; Cartuyvels, R.; Maurissen, W. Vertical transmission of SARS-CoV-2 infection and preterm birth. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 2441–2445. [Google Scholar] [CrossRef]
- Stonoga, E.T.S.; Lanzoni, L.D.A.; Rebutini, P.Z.; de Oliveira, A.L.P.; Chiste, J.A.; Fugaça, C.A.; Prá, D.M.M.; Percicote, A.P.; Rossoni, A.; Nogueira, M.B.; et al. Intrauterine Transmission of SARS-CoV-2. Emerg. Infect. Dis. 2021, 27, 638–641. [Google Scholar] [CrossRef]
- di Gioia, C.; Zullo, F.; Bruno Vecchio, R.C.; Pajno, C.; Perrone, G.; Galoppi, P.; Pecorini, F.; Di Mascio, D.; Carletti, R.; Prezioso, C.; et al. Stillbirth and fetal capillary infection by SARS-CoV-2. Am. J. Obstet. Gynecol. 2022, 4, 100523. [Google Scholar] [CrossRef]
- Enache, A.; Ciocan, V.; Muresan, C.O.; Cut, T.G.; Novacescu, D.; Paul, C.; Andreescu, N.; Mihailescu, A.; Raica, M.; Dumache, R. Postmortem Documentation of SARS-CoV-2 in Utero and Postpartum Transmission, through Amniotic Fluid, Placental, and Pulmonary Tissue RT-PCR. Appl. Sci. 2021, 11, 9505. [Google Scholar] [CrossRef]
- Popescu, D.E.; Cioca, A.; Muresan, C.; Navolan, D.; Gui, A.; Pop, O.; Marcovici, T.; Ilie, C.; Craina, M.; Boia, M.A. A Case of COVID-19 Pregnancy Complicated with Hydrops Fetalis and Intrauterine Death. Med. Kaunas Lith. 2021, 57, 667. [Google Scholar] [CrossRef] [PubMed]
- Marinho, P.S.; da Cunha, A.J.L.A.; Chimelli, L.; Avvad-Portari, E.; Andreiuolo, F.D.M.; de Oliveira-Szejnfeld, P.S.; Mendes, M.A.; Gomes, I.C.; Souza, L.R.Q.; Guimarães, M.Z.; et al. Case Report: SARS-CoV-2 Mother-to-Child Transmission and Fetal Death Associated with Severe Placental Thromboem-bolism. Front. Med. 2021, 8, 677001. [Google Scholar] [CrossRef]
- Gant, T.F.; Villegas, T.P.; Summerall-Smith, J.; Watkins, B. Intrauterine fetal demise as a result of maternal COVID-19 infection in the third trimester of pregnancy: A case report. Int. J. Surg. Case Rep. 2022, 98, 107492. [Google Scholar] [CrossRef] [PubMed]
- Babal, P.; Krivosikova, L.; Sarvaicova, L.; Deckov, I.; Szemes, T.; Sedlackova, T.; Palkovic, M.; Kalinakova, A.; Janega, P. Intrau-terine Fetal Demise After Uncomplicated COVID-19: What Can We Learn from the Case? Viruses 2021, 13, 2545. [Google Scholar] [CrossRef]
- Zinserling, V.A.; Bornstein, S.R.; Narkevich, T.A.; Sukhanova, Y.V.; Semenova, N.Y.; Vashukova, M.A.; Steenblock, C. Stillborn child with diffuse SARS-CoV-2 viral infection of multiple organs. Idcases 2021, 26, e01328. [Google Scholar] [CrossRef]
- Rodrigues, M.L.; Gasparinho, G.; Sepúlveda, F.; Matos, T. Signs suggestive of congenital SARS-CoV-2 infection with in-trauterine fetal death: A case report. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 256, 508–509. [Google Scholar] [CrossRef]
- Sessa, R.; Masciullo, L.; Filardo, S.; Di Pietro, M.; Brandolino, G.; Brunelli, R.; Galoppi, P.; Terrin, G.; Viscardi, M.F.; Anastasi, E.; et al. SARS-CoV-2 vertical transmission in a twin-pregnant woman: A case report. Int. J. Infect. Dis. 2022, 125, 192–194. [Google Scholar] [CrossRef]
- Fusco, M.A.; Mantini, V.; de Souza Salmont Júnior, J.; de Carvalho Gomes, R.G.; de Oliveira Lima, A.R.; de Oliveira Clarim, H.L.; Ferreira, E.C.; de Abreu Almeida, S.S.; Salmont, C.G.; de Sousa Rizzo-Valente, V.; et al. Assessment of SARS-CoV-2 Vertical Transmission through Nested RT-PCR Testing of Neonatal Samples: Three Case Reports. J. Pediatr. Perinatol. Child Health 2022, 6, 370–376. [Google Scholar]
- Shen, W.-B.; Turan, S.; Wang, B.; Cojocaru, L.; Harman, C.; Logue, J.; Reece, E.A.; Frieman, M.B.; Yang, P. A SARS-CoV-2 Delta Variant Case Manifesting as Extensive Placental Infection and Fetal Transmission. Gynecol. Obstet. Investig. 2022, 87, 165–172. [Google Scholar] [CrossRef]
- Von Kohorn, I.; Stein, S.R.; Shikani, B.T.; Ramos-Benitez, M.J.; Vannella, K.M.; Hewitt, S.M.; E Kleiner, D.; Alejo, J.C.; Burbelo, P.; I Cohen, J.; et al. In Utero Severe Acute Respiratory Syndrome Coronavirus 2 Infection. J. Pediatr. Infect. Dis. Soc. 2020, 9, 769–771. [Google Scholar] [CrossRef] [PubMed]
- Zamaniyan, M.; Ebadi, A.; Aghajanpoor, S.; Rahmani, Z.; Haghshenas, M.; Azizi, S. Preterm delivery, maternal death, and vertical transmission in a pregnant woman with COVID-19 infection. Prenat. Diagn. 2020, 40, 1759–1761. [Google Scholar] [CrossRef] [PubMed]
- Vivanti, A.J.; Vauloup-Fellous, C.; Escourrou, G.; Rosenblatt, J.; Jouannic, J.-M.; Laurent-Bellue, A.; De Luca, D. Factors associated with SARS-CoV-2 transplacental transmission. Am. J. Obstet. Gynecol. 2022, 227, 541–543.e11. [Google Scholar] [CrossRef] [PubMed]
- Buonsenso, D.; Costa, S.; Sanguinetti, M.; Cattani, P.; Posteraro, B.; Marchetti, S.; Carducci, B.; Lanzone, A.; Tamburrini, E.; Vento, G. Neonatal Late Onset Infection with Severe Acute Respiratory Syndrome Coronavirus 2. Am. J. Perinatol. 2020, 37, 869–872. [Google Scholar] [CrossRef]
- Abadía-Cuchí, N.; Ruiz-Martínez, S.; Fabre, M.; Mateo, P.; Remacha Sienes, M.; Ventura Faci, P.; Bueno Sancho, J.; Paules, C. SARS-CoV-2 congenital infection and pre-eclampsia-like syndrome in dichorionic twins: A case report and review of the literature. Int. J. Gynaecol. Obstet. Off. Organ Int. Fed. Gynaecol. Obstet. 2021, 154, 370–372. [Google Scholar] [CrossRef]
- Dong, L.; Tian, J.; He, S.; Zhu, C.; Wang, J.; Liu, C.; Yang, J. Possible Vertical Transmission of SARS-CoV-2 from an Infected Moth-er to Her Newborn. JAMA 2020, 323, 1846–1848. [Google Scholar] [CrossRef] [Green Version]
- Karade, S.; Vishal, A.K.; Sen, S.; Bewal, N.; Gupta, R.M. Probable vertical transmission of severe acute respiratory syn-drome coronavirus 2 infection from mother to neonate. Med. J. Armed Forces India 2021, 77, S490–S493. [Google Scholar] [CrossRef]
- Zhang, P.; Salafia, C.; Heyman, T.; Salafia, C.; Lederman, S.; Dygulska, B. Detection of severe acute respiratory syndrome coronavirus 2 in placentas with pathology and vertical transmission. Am. J. Obstet. Gynecol. MFM 2020, 2, 100197. [Google Scholar] [CrossRef]
- Correia, C.R.; Marçal, M.; Vieira, F.; Santos, E.; Novais, C.; Maria, A.T.; Malveiro, D.; Prior, A.R.; Aguiar, M.; Salazar, A.; et al. Congenital SARS-CoV-2 Infection in a Neonate with Severe Acute Respiratory Syndrome. Pediatr. Infect. Dis. J. 2020, 39, e439–e443. [Google Scholar] [CrossRef]
- Reagan-Steiner, S.; Bhatnagar, J.; Martines, R.B.; Milligan, N.S.; Gisondo, C.; Williams, F.B.; Lee, E.; Estetter, L.; Bullock, H.; Goldsmith, C.S.; et al. Detection of SARS-CoV-2 in Neonatal Autopsy Tissues and Placenta. Emerg. Infect. Dis. 2022, 28, 510–517. [Google Scholar] [CrossRef]
- Lorenz, N.; Treptow, A.; Schmidt, S.; Hofmann, R.; Raumer-Engler, M.; Heubner, G.; Gröber, K. Neonatal Early-Onset Infection with SARS-CoV-2 in a Newborn Presenting with Encephalitic Symptoms. Pediatr. Infect. Dis. J. 2020, 39, e212. [Google Scholar] [CrossRef] [PubMed]
- Kirtsman, M.; Diambomba, Y.; Poutanen, S.M.; Malinowski, A.K.; Vlachodimitropoulou, E.; Parks, W.T.; Erdman, L.; Morris, S.K.; Shah, P.S. Probable congenital SARS-CoV-2 infection in a neonate born to a woman with active SARS-CoV-2 infection. Can. Med. Assoc. J. 2020, 192, E647–E650. [Google Scholar] [CrossRef] [PubMed]
- Parsa, Y.; Shokri, N.; Jahedbozorgan, T.; Naeiji, Z.; Zadehmodares, S.; Moridi, A. Possible Vertical Transmission of COVID-19 to the Newborn; a Case Report. Arch. Acad. Emerg. Med. 2021, 9, e5. [Google Scholar] [CrossRef] [PubMed]
- Marzollo, R.; Aversa, S.; Prefumo, F.; Saccani, B.; Perez, C.R.; Sartori, E.; Motta, M. Possible Coronavirus Disease 2019 Pandemic and Pregnancy: Vertical Transmission Is Not Excluded. Pediatr. Infect. Dis. J. 2020, 39, e261–e262. [Google Scholar] [CrossRef] [PubMed]
- Facchetti, F.; Bugatti, M.; Drera, E.; Tripodo, C.; Sartori, E.; Cancila, V.; Papaccio, M.; Castellani, R.; Casola, S.; Boniotti, M.B.; et al. SARS-CoV2 vertical transmission with adverse effects on the newborn revealed through integrated immunohistochemical, electron microscopy and molecular analyses of Placenta. Ebiomedicine 2020, 59, 102951. [Google Scholar] [CrossRef]
- Sukhikh, G.; Petrova, U.; Prikhodko, A.; Starodubtseva, N.; Chingin, K.; Chen, H.; Bugrova, A.; Kononikhin, A.; Bourmenskaya, O.; Brzhozovskiy, A.; et al. Vertical Transmission of SARS-CoV-2 in Second Trimester Associated with Severe Neonatal Pathology. Viruses 2021, 13, 447. [Google Scholar] [CrossRef]
- Boncompagni, A.; De Agostini, M.; Lugli, L.; Ternelli, G.; Colonna, V.; Biagioni, E.; Bonasoni, M.P.; Salviato, T.; Gabrielli, L.; Falconi, M.; et al. Unexpected Vertical Transmission of SARS-CoV-2: Discordant Clinical Course and Transmission from Mother to Newborn. Microorganisms 2022, 10, 1718. [Google Scholar] [CrossRef]
- Farhadi, R.; Mehrpisheh, S.; Ghaffari, V.; Haghshenas, M.; Ebadi, A. Clinical course, radiological findings and late outcome in preterm infant with suspected vertical transmission born to a mother with severe COVID-19 pneumonia: A case report. J. Med. Case Rep. 2021, 15, 213. [Google Scholar] [CrossRef]
- Rebello, C.M.; Fascina, L.P.; Annicchino, G.; Pinho, J.R.R.; Yoshida, R.D.A.M.; Zacharias, R.S.B. Vertical transmission of SARS-CoV-2 from infected pregnant mother to the neonate detected by cord blood real-time polymerase chain reaction (RT-PCR). Pediatr. Res. 2020, 89, 1592–1593. [Google Scholar] [CrossRef]
- Disse, S.C.; Manuylova, T.; Adam, K.; Lechler, A.; Zant, R.; Klingel, K.; Aepinus, C.; Finkenzeller, T.; Wellmann, S.; Schneble, F. COVID-19 in 28-Week Triplets Caused by Intrauterine Transmission of SARS-CoV-2—Case Report. Front. Pediatr. 2021, 9, 812057. [Google Scholar] [CrossRef]
- Shaiba, L.A.; Hadid, A.; Altirkawi, K.A.; Bakheet, H.M.; Alherz, A.M.; Hussain, S.A.; Sobaih, B.H.; Alnemri, A.M.; Almaghrabi, R.; Ahmed, M.; et al. Case Report: Neonatal Multi-System Inflammatory Syndrome Associated with SARS-CoV-2 Exposure in Two Cases from Saudi Arabia. Front. Pediatr. 2021, 9, 652857. [Google Scholar] [CrossRef] [PubMed]
- Choobdar, F.A.; Ghassemzadeh, M.; Attarian, M.; Abbariki, E.; Nateghian, A.; Ghanbari, B.; Hamzehi, S.S.; Hashemi, M.R.; Azarbin, Z. Transplacental Transmission of SARS-CoV-2 Infection: A Case Report from Iran. Arch. Pediatr. Infect. Dis. 2021, 9, e108582. [Google Scholar] [CrossRef]
- Ng, D.C.; Chin, L.; Choo, P.P.L.; Paramasivam, U. COVID-19 in a premature infant. BMJ Case Rep. 2021, 14, e243783. [Google Scholar] [CrossRef] [PubMed]
- Ergon, E.Y.; Akbay, S.; Aytemiz, G.; Çelik, E.C.A.; Çalıskan Polat, A.; Umit, Z.; Paytoncu, S. A novel case of neonatal acute respiratory distress syndrome with SARS-CoV-2 infection: Potential perinatal transmission. Arch. Argent. De Pediatr. 2021, 119, e531–e535. [Google Scholar] [CrossRef]
- Favre, G.; Mazzetti, S.; Gengler, C.; Bertelli, C.; Schneider, J.; Laubscher, B.; Capoccia, R.; Pakniyat, F.; Ben Jazia, I.; Eggel-Hort, B.; et al. Decreased Fetal Movements: A Sign of Placental SARS-CoV-2 Infection with Perinatal Brain Injury. Viruses 2021, 13, 2517. [Google Scholar] [CrossRef]
- Gesaka, S.R.; Obimbo, M.M.; Wanyoro, A. Coronavirus disease 2019 and the placenta: A literature review. Placenta 2022, 126, 209–223. [Google Scholar] [CrossRef]
- Zimmermann, P.; Curtis, N. COVID-19 in Children, Pregnancy and Neonates: A Review of Epidemiologic and Clinical Features. Pediatr. Infect. Dis. J. 2020, 39, 469–477. [Google Scholar] [CrossRef]
- Carosso, A.; Cosma, S.; Borella, F.; Marozio, L.; Coscia, A.; Ghisetti, V.; Di Perri, G.; Benedetto, C. Pre-labor anorectal swab for SARS-CoV-2 in COVID-19 pregnant patients: Is it time to think about it? Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 249, 98–99. [Google Scholar] [CrossRef]
- Valdespino-Vázquez, M.Y.; Helguera-Repetto, C.A.; León-Juárez, M.; Villavicencio-Carrisoza, O.; Flores-Pliego, A.; Moreno-Verduzco, E.R.; Díaz-Pérez, D.L.; Villegas-Mota, I.; Carrasco-Ramírez, E.; López-Martínez, I.E.; et al. Fetal and placental infection with SARS-CoV-2 in early pregnancy. J. Med. Virol. 2021, 93, 4480–4487. [Google Scholar] [CrossRef] [PubMed]
- Figueiro-Filho, E.A.; Hobson, S.R.; Farine, D.; Yudin, M.H. Highly expressed ACE-2 receptors during pregnancy: A protective factor for SARS-CoV-2 infection? Med. Hypotheses 2021, 153, 110641. [Google Scholar] [CrossRef]
- Maeda, M.D.F.Y.; Brizot, M.D.L.; Gibelli, M.A.B.C.; Ibidi, S.M.; de Carvalho, W.B.; Hoshida, M.S.; Machado, C.M.; Sabino, E.C.; Silva, L.C.D.O.D.; Jaenisch, T.; et al. Vertical transmission of SARS-CoV2 during pregnancy: A high-risk cohort. Prenat. Diagn. 2021, 41, 998–1008. [Google Scholar] [CrossRef] [PubMed]
- Yılmaz, Y.Z.; Tüten, A.; Çakan, D.; Kara, E.; Akşahin, E.; Gülmez, Z.D.; Batıoğlu-Karaaltın, A. The Relationship Between the Presence of Severe Acute Respiratory Syndrome-Coronavirus-2 during Pregnancy and Neonatal Hearing Loss. Istanb. Med. J. 2022, 23, 144–148. [Google Scholar] [CrossRef]
- Buonsenso, D.; Costa, S.; Giordano, L.; Priolo, F.; Colonna, A.T.; Morini, S.; Sbarbati, M.; Pata, D.; Acampora, A.; Conti, G.; et al. Short- and mid-term multidisciplinary outcomes of newborns exposed to SARS-CoV-2 in utero or during the perinatal period: Preliminary findings. Eur. J. Pediatr. 2022, 181, 1507–1520. [Google Scholar] [CrossRef]
- Di Guardo, F.; Di Grazia, F.M.; Di Gregorio, L.M.; Zambrotta, E.; Carrara, G.; Gulino, F.A.; Tuscano, A.; Palumbo, M. Poor maternal–neonatal outcomes in pregnant patients with confirmed SARS-CoV-2 infection: Analysis of 145 cases. Arch. Gynecol. Obstet. 2021, 303, 1483–1488. [Google Scholar] [CrossRef]
- Resta, L.; Vimercati, A.; Cazzato, G.; Fanelli, M.; Scarcella, S.V.; Ingravallo, G.; Colagrande, A.; Sablone, S.; Stolfa, M.; Arezzo, F.; et al. SARS-CoV-2, Placental Histopathology, Gravity of Infection and Immunopathology: Is There an Association? Viruses 2022, 14, 1330. [Google Scholar] [CrossRef]
- Mahyuddin, A.P.; Kanneganti, A.; Wong, J.J.L.; Dimri, P.S.; Su, L.L.; Biswas, A.; Illanes, S.E.; Mattar, C.N.Z.; Huang, R.Y.; Choolani, M. Mechanisms and evidence of vertical transmission of infections in pregnancy including SARS-CoV-2s. Prenat Diagn. 2020, 40, 1655–1670. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Livebirths | Stillbirths | ||
|---|---|---|---|
| Asymptomatic | Symptomatic | ||
| Total | 19 | 24 | 32 |
| C-IUE | 15 | 8 | 31 |
| P-IUE | 4 | 14 | 1 |
| C-IPE | - | 2 | - |
| Symptomatic N = 24 | Asymptomatic N = 19 | |
|---|---|---|
| Gestational age at the moment of maternal infection, in weeks (median) | 32 | 32 |
| The interval between the moment of maternal infection and birth, in weeks (median) | 7 | 8 |
| Gestational age at delivery, in weeks (median) | 34 | 34 |
| 5-min APGAR SCORE (median) | 9 | 9 |
| Birth weight, in grams (median) | 2109.5 | 2109 |
| Caesarian section (c-section) | 19 (79%) | 18 (94.73%) |
| Emergency c-section for non-reassuring CTG | 8 (33.3%) | 6 (18.75%) |
| Emergency c-section for severe maternal COVID disease | 3 (12.5%) | 0 |
| Neonatal death | 3 (12.5%) | 0 |
| Persistence of COVID-19 sequelae after neonatal discharge | 2 (8.3%) | 0 |
| Author | Type of Vertical Transmission | Gestational Age at Delivery (Weeks) | Neonatal Clinical Outcome | Neonatal Evolution | Case Particularities |
|---|---|---|---|---|---|
| Alzamora [52] | C-IPE b | 33 |
| good evolution |
|
| Boncompagni [129] | C-IUE a | 35 |
| good evolution |
|
| Choobdar [134] | P-IUE a | 31 |
| good evolution |
|
| Disse [132] | P-IUE a | 28 |
| good evolution |
|
| P-IUEa | 28 |
| good evolution |
| |
| Ergon [136] | P-IUE a | 34 |
| neonatal death in DOL 17 |
|
| Facchetti [127] | P-IUE a | 37 |
| good evolution |
|
| Farhadi [130] | C-IUE b | 32 |
| good evolution |
|
| Rebello [131] | P-IUE a | 34 |
| good evolution |
|
| Favre [137] | C-IUE b | 29 |
| abnormal neurological examination DOL 54 |
|
| Kirtsman [124] | P-IUE a | 35 |
| good evolution |
|
| Lorenz [123] | C-IPE b | 40 |
| good evolution | |
| Marzollo [126] | P-IUE a | 38 |
| good evolution |
|
| D. C. Ng [135] | P-IUE a | 29 |
| good evolution |
|
| Parsa [125] | C-IUE b | 37 |
| good evolution |
|
| Reagan-Steiner [122] | P-IUE a | 25 |
| neonatal death in DOL 4 |
|
| Shaiba [133] | C-IPE a | 32 |
| good evolution |
|
| Sukhikh [128] | C-IUE b | 26 |
| neonatal death in DOL 1 | |
| Vivanti [55] | C-IUE b | 35 |
| good evolution |
|
| Vivanti [115] | P-IUE a | 40 |
| good evolution | |
| Zaigham [95] | P-IUE b | 34 |
| good evolution |
|
| P-IUE a | 34 |
| good evolution |
| |
| P-IUE a | 29 |
| good evolution |
|
| qRT-PCR at Birth Nasopharyngeal | qRT-PCR at 24–48 h | ||
|---|---|---|---|
| Neonatal Blood | NPS | ||
| Positive | positive | C-IUE a | |
| Positive | positive | C-IPE b | |
| Negative | positive | C-IPE a | |
| Negative | positive | C-IPE a,* | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moza, A.; Duica, F.; Antoniadis, P.; Bernad, E.S.; Lungeanu, D.; Craina, M.; Bernad, B.C.; Paul, C.; Muresan, C.; Nitu, R.; et al. Outcome of Newborns with Confirmed or Possible SARS-CoV-2 Vertical Infection—A Scoping Review. Diagnostics 2023, 13, 245. https://doi.org/10.3390/diagnostics13020245
Moza A, Duica F, Antoniadis P, Bernad ES, Lungeanu D, Craina M, Bernad BC, Paul C, Muresan C, Nitu R, et al. Outcome of Newborns with Confirmed or Possible SARS-CoV-2 Vertical Infection—A Scoping Review. Diagnostics. 2023; 13(2):245. https://doi.org/10.3390/diagnostics13020245
Chicago/Turabian StyleMoza, Andreea, Florentina Duica, Panagiotis Antoniadis, Elena S. Bernad, Diana Lungeanu, Marius Craina, Brenda C. Bernad, Corina Paul, Cezara Muresan, Razvan Nitu, and et al. 2023. "Outcome of Newborns with Confirmed or Possible SARS-CoV-2 Vertical Infection—A Scoping Review" Diagnostics 13, no. 2: 245. https://doi.org/10.3390/diagnostics13020245