
Soluble ST2 as a Useful Biomarker for Predicting Clinical Outcomes in Hospitalized COVID-19 Patients
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
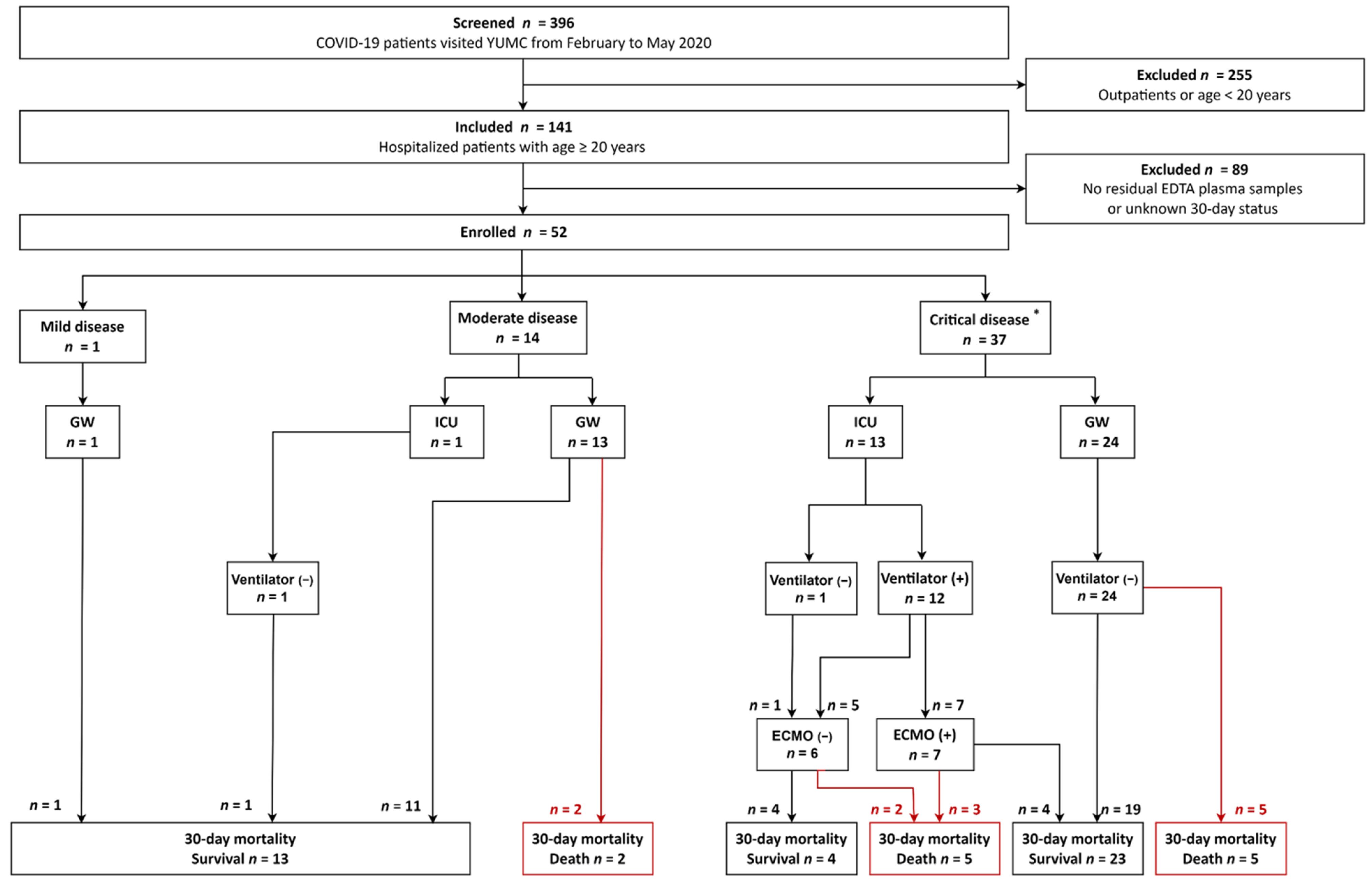
2.1. Study Population
2.2. sST2 Assay
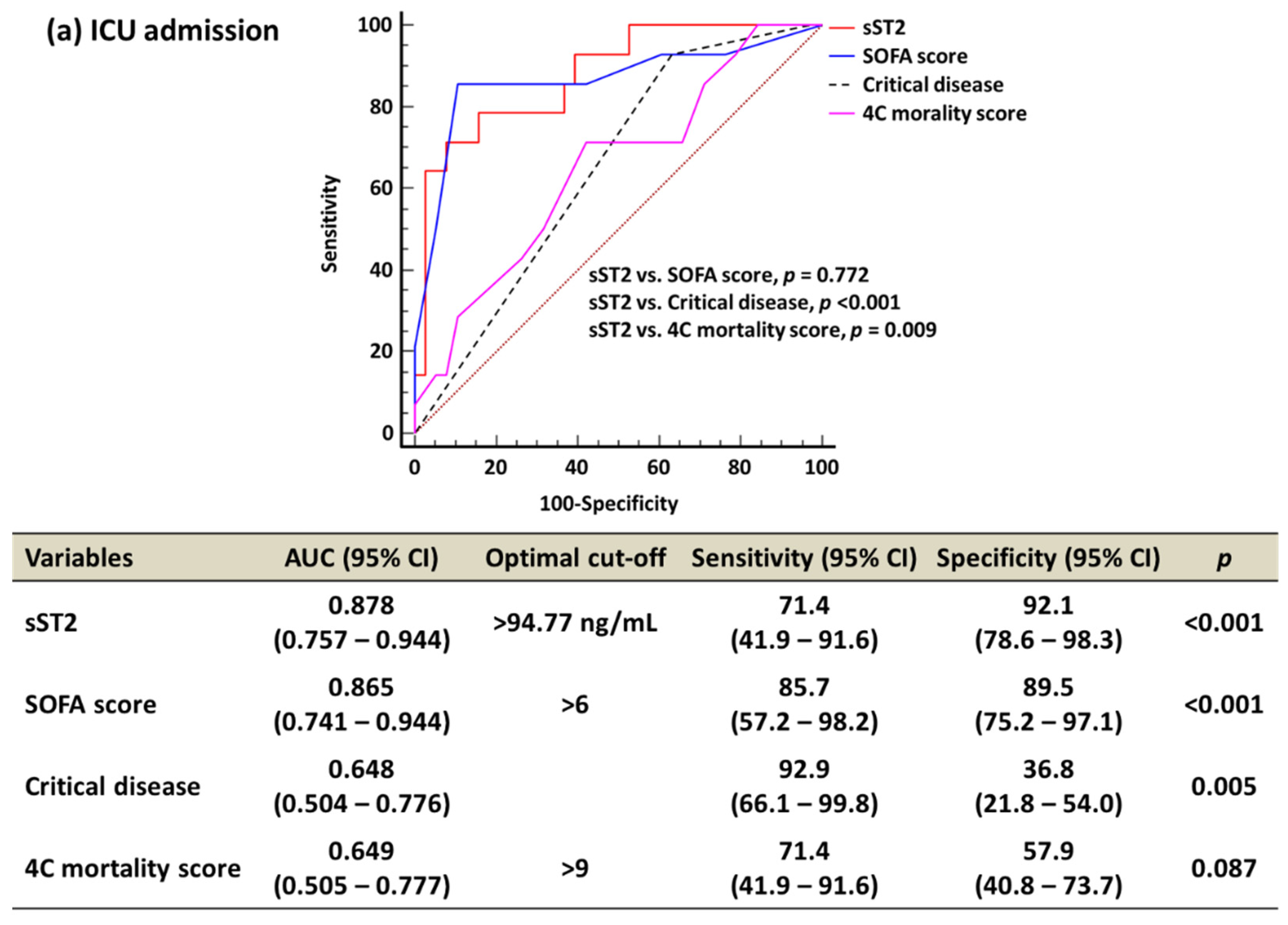
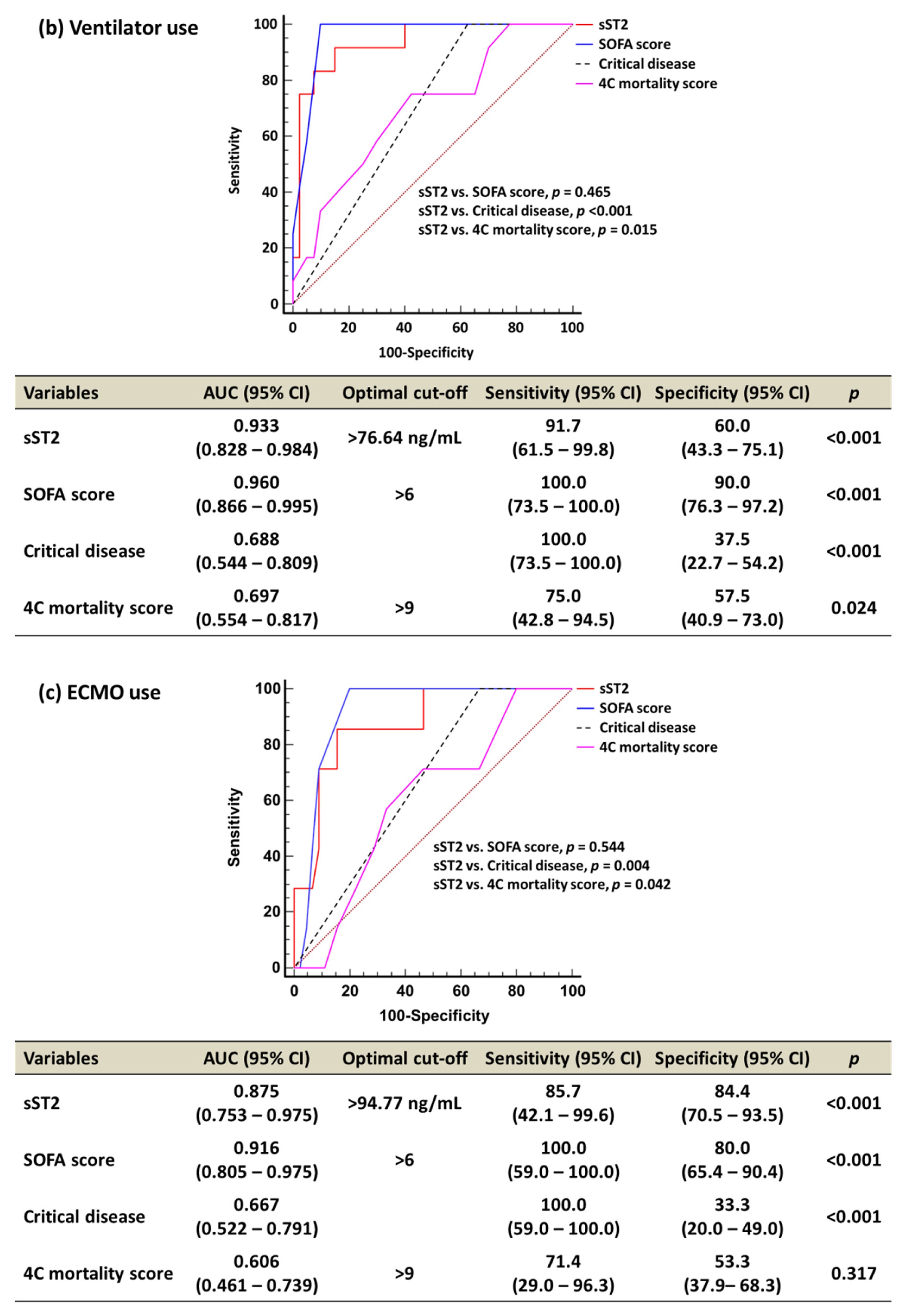
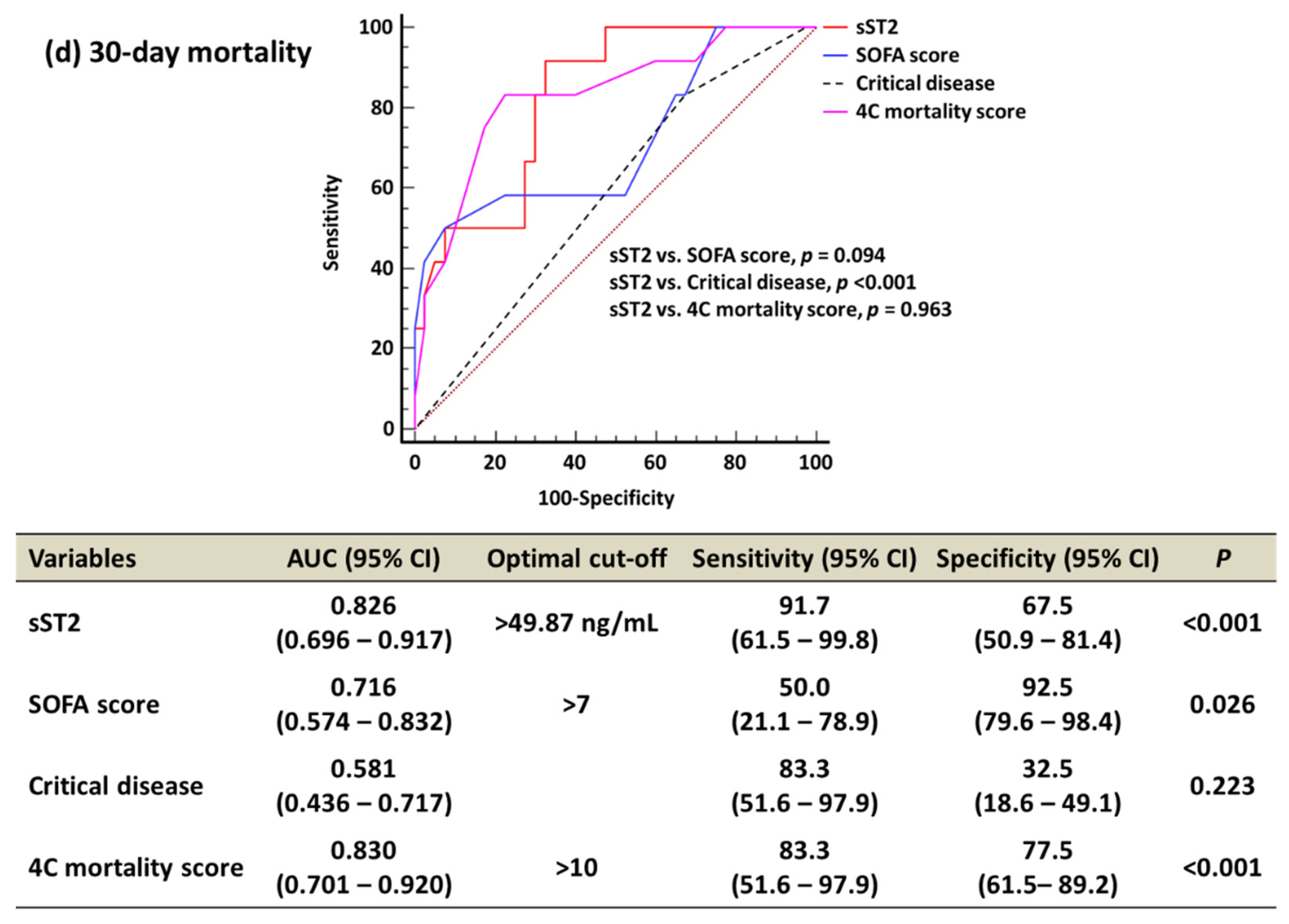
2.3. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hong, K.H.; Lee, S.W.; Kim, T.S.; Huh, H.J.; Lee, J.; Kim, S.Y.; Park, J.S.; Kim, G.J.; Sung, H.; Roh, K.H.; et al. Guidelines for Laboratory Diagnosis of Coronavirus Disease 2019 (COVID-19) in Korea. Ann. Lab. Med. 2020, 40, 351–360. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/table (accessed on 8 November 2022).
- Word Health Organization: Living Guidance for Clinical Management of COVID-19. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-clinical-2021-2 (accessed on 8 November 2022).
- Mokhtari, T.; Hassani, F.; Ghaffari, N.; Ebrahimi, B.; Yarahmadi, A.; Hassanzadeh, G. COVID-19 and Multiorgan Failure: A Narrative Review on Potential Mechanisms. J. Mol. Histol. 2020, 51, 613–628. [Google Scholar] [CrossRef] [PubMed]
- Park, M.; Hur, M.; Kim, H.; Lee, C.H.; Lee, J.H.; Kim, H.W.; Nam, M. Prognostic Utility of Procalcitonin, Presepsin, and the VACO Index for Predicting 30-day Mortality in Hospitalized COVID-19 Patients. Ann. Lab. Med. 2022, 42, 406–414. [Google Scholar] [CrossRef] [PubMed]
- Knight, S.R.; Ho, A.; Pius, R.; Buchan, I.; Carson, G.; Drake, T.M.; Dunning, J.; Fairfield, C.J.; Gamble, C.; Green, C.A.; et al. Risk Stratification of Patients Admitted to Hospital with COVID-19 Using the ISARIC WHO Clinical Characterisation Protocol: Development and Validation of the 4C Mortality Score. BMJ 2020, 370, m3339. [Google Scholar] [CrossRef] [PubMed]
- Morgan, P.; Arnold, S.J.; Hsiao, N.W.; Shu, C.W. A Closer Look at Dexamethasone and the SARS-CoV-2-Induced Cytokine Storm: In Silico Insights of the First Life-Saving COVID-19 Drug. Antibiotics 2021, 10, 1507. [Google Scholar] [CrossRef]
- Nagashima, S.; Dutra, A.A.; Arantes, M.P.; Zeni, R.C.; Klein, C.K.; de Oliveira, F.C.; Piper, G.W.; Brenny, I.D.; Pereira, M.R.C.; Stocco, R.B.; et al. COVID-19 and Lung Mast Cells: The Kallikrein–Kinin Activation Pathway. Int. J. Mol. Sci. 2022, 23, 1714. [Google Scholar] [CrossRef]
- Bader, F.; Manla, Y.; Atallah, B.; Starling, R.C. Heart Failure and COVID-19. Heart Fail Rev. 2021, 26, 1–10. [Google Scholar] [CrossRef]
- Tajbakhsh, A.; Gheibi Hayat, S.M.; Taghizadeh, H.; Akbari, A.; Inabadi, M.; Savardashtaki, A.; Johnston, T.P.; Sahebkar, A. COVID-19 and Cardiac injury: Clinical Manifestations, Biomarkers, Mechanisms, Diagnosis, Treatment, and Follow up. Expert Rev. Anti. Infect. Ther. 2021, 19, 345–357. [Google Scholar] [CrossRef]
- Sokolski, M.; Trenson, S.; Sokolska, J.M.; D’Amario, D.; Meyer, P.; Poku, N.K.; Biering-Sørensen, T.; Højbjerg Lassen, M.C.; Skaarup, K.G.; Barge-Caballero, E.; et al. Heart Failure in COVID-19: The Multicentre, Multinational PCHF-COVICAV Registry. ESC Heart Fail. 2021, 8, 4955–4967. [Google Scholar] [CrossRef]
- Aleksova, A.; Sinagra, G.; Beltrami, A.P.; Pierri, A.; Ferro, F.; Janjusevic, M.; Gagno, G. Biomarkers in the Management of Acute Heart Failure: State of the Art and Role in COVID-19 era. ESC Heart Fail. 2021, 8, 4465–4483. [Google Scholar] [CrossRef]
- Aimo, A.; Januzzi, J.L.; Bayes-Genis, A.; Vergaro, G.; Sciarrone, P.; Passino, C.; Emdin, M. Clinical and Prognostic Significance of sST2 in Heart Failure: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2019, 74, 2193–2203. [Google Scholar] [CrossRef]
- Yang, H.S.; Kim, H.J.; Shim, H.J.; Kim, S.J.; Hur, M.; Di Somma, S. Soluble ST2 and Troponin I Combination: Useful Biomarker for Predicting Development of Stress Cardiomyopathy in Patients Admitted to the Medical Intensive Care Unit. Heart Lung 2015, 44, 282–288. [Google Scholar] [CrossRef]
- Hur, M.; Kim, H.; Kim, H.J.; Yang, H.S.; Magrini, L.; Marino, R.; Cardelli, P.; Somma, S.D.; GREAT Network. Soluble ST2 Has a Prognostic Role in Patients With Suspected Sepsis. Ann. Lab. Med. 2015, 35, 570–577. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Hur, M.; Moon, H.-W.; Yun, Y.-M.; Di Somma, S. Multi-Marker Approach Using Procalcitonin, Presepsin, Galectin-3, and Soluble Suppression of Tumorigenicity 2 for the Prediction of Mortality in Sepsis. Ann. Intensive Care 2017, 7, 27. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Chen, Z.; Ma, M.; He, Y. Soluble ST2 in Coronary Artery Disease: Clinical Biomarkers and Treatment Guidance. Front. Cardiovasc. Med. 2022, 9, 924461. [Google Scholar] [CrossRef]
- Marino, L.; Concistrè, A.; Suppa, M.; Galardo, G.; Rosa, A.; Bertazzoni, G.; Pugliese, F.; Letizia, C.; Petramala, L. Prognostic Role of sST2 in Acute Heart Failure and COVID-19 Infection—A Narrative Review on Pathophysiology and Clinical Prospective. Int. J. Mol. Sci. 2022, 23, 8230. [Google Scholar] [CrossRef]
- Khan, S.; Rasool, S.T.; Ahmed, S.I. Role of Cardiac Biomarkers in COVID-19: What Recent Investigations Tell Us? Curr. Probl. Cardiol. 2021, 46, 100842. [Google Scholar] [CrossRef]
- Ragusa, R.; Basta, G.; Del Turco, S.; Caselli, C. A Possible Role for ST2 as Prognostic Biomarker for COVID-19. Vascul. Pharmacol. 2021, 138, 106857. [Google Scholar] [CrossRef]
- Miftode, R.S.; Petriș, A.O.; Onofrei Aursulesei, V.; Cianga, C.; Costache, I.I.; Mitu, O.; Miftode, I.L.; Șerban, I.L. The Novel Perspectives Opened by ST2 in the Pandemic: A Review of Its Role in the Diagnosis and Prognosis of Patients with Heart Failure and COVID-19. Diagnostics 2021, 11, 175. [Google Scholar] [CrossRef]
- Wendt, R.; Lingitz, M.T.; Laggner, M.; Mildner, M.; Traxler, D.; Graf, A.; Krotka, P.; Moser, B.; Hoetzenecker, K.; Kalbitz, S.; et al. Clinical Relevance of Elevated Soluble ST2, HSP27 and 20S Proteasome at Hospital Admission in Patients with COVID-19. Biology 2021, 10, 1186. [Google Scholar] [CrossRef]
- Zeng, Z.; Hong, X.-Y.; Li, Y.; Chen, W.; Ye, G.; Li, Y.; Luo, Y. Serum-soluble ST2 as a Novel Biomarker Reflecting Inflammatory Status and Illness Severity in Patients With COVID-19. Biomark. Med. 2020, 14, 1619–1629. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Marteles, M.; Rubio-Gracia, J.; Peña-Fresneda, N.; Garcés-Horna, V.; Gracia-Tello, B.; Martínez-Lostao, L.; Crespo-Aznárez, S.; Pérez-Calvo, J.I.; Giménez-López, I. Early Measurement of Blood sST2 Is a Good Predictor of Death and Poor Outcomes in Patients Admitted for COVID-19 Infection. J. Clin. Med. 2021, 10, 3534. [Google Scholar] [CrossRef]
- Abers, M.S.; Delmonte, O.M.; Ricotta, E.E.; Fintzi, J.; Fink, D.L.; de Jesus, A.A.A.; Zarember, K.A.; Alehashemi, S.; Oikonomou, V.; Desai, J.V.; et al. An Immune-based Biomarker Signature is Associated With Mortality in COVID-19 patients. JCI Insight 2021, 6, e144455. [Google Scholar] [CrossRef] [PubMed]
- Umesh, M.; Singaravelu, V.; Daulatabad, V.; Kamble, P.; Singhal, A.; John, N.A.; John, J. An Overview of Prognostic Value of Neurologic and Cardiac Biomarkers in Patients With COVID-19 Sequelae. Horm. Mol. Biol. Clin. Investig. 2022, in press. [Google Scholar] [CrossRef] [PubMed]
- Motloch, L.J.; Jirak, P.; Gareeva, D.; Davtyan, P.; Gumerov, R.; Lakman, I.; Tataurov, A.; Zulkarneev, R.; Kabirov, I.; Cai, B.; et al. Cardiovascular Biomarkers for Prediction of In-hospital and 1-Year Post-discharge Mortality in Patients with COVID-19 Pneumonia. Front Med. 2022, 9, 906665. [Google Scholar] [CrossRef]
- Omland, T.; Prebensen, C.; Jonassen, C.; Svensson, M.; Berdal, J.E.; Seljeflot, I.; Myhre, P.L. Soluble ST2 Concentrations Associate With In-hospital Mortality and Need for Mechanical Ventilation in Unselected Patients With COVID-19. Open Heart 2021, 8, e001884. [Google Scholar] [CrossRef]
- Rubio-Gracia, J.; Sánchez-Marteles, M.; Garcés-Horna, V.; Martínez-Lostao, L.; Ruiz-Laiglesia, F.; Crespo-Aznarez, S.; Peña-Fresneda, N.; Gracia-Tello, B.; Cebollada, A.; Carrera-Lasfuentes, P.; et al. Multiple Approaches at Admission Based on Lung Ultrasound and Biomarkers Improves Risk Identification in COVID-19 Patients. J. Clin. Med. 2021, 10, 5478. [Google Scholar] [CrossRef]
- Cabrera-Garcia, D.; Miltiades, A.; Yim, P.; Parsons, S.; Elisman, K.; Mansouri, M.T.; Wagener, G.; Harrison, N.L. Plasma Biomarkers Associated With Survival and Thrombosis in Hospitalized COVID-19 Patients. Int. J. Hematol. 2022, 116, 937–946. [Google Scholar] [CrossRef]
- Park, M.; Hur, M.; Kim, H.; Lee, C.H.; Lee, J.H.; Nam, M. Usefulness of KL-6 for Predicting Clinical Outcomes in Hospitalized COVID-19 Patients. Medicina 2022, 58, 1317. [Google Scholar] [CrossRef]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the Areas under Two or More Correlated Receiver Operating Characteristic Curves: A Nonparametric Approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Feng, D.; Cortese, G.; Baumgartner, R. A Comparison of Confidence/Credible Interval Methods for the Area Under the ROC Curve for Continuous Diagnostic Tests With Small Sample Size. Stat. Methods Med. Res. 2017, 26, 2603–2621. [Google Scholar] [CrossRef]
- Nagashima, K.; Noma, H.; Sato, Y.; Gosho, M. Sample Size Calculations for Single-Arm Survival Studies Using Transformations of the Kaplan–Meier Estimator. Pharm. Stat. 2020, 20, 499–511. [Google Scholar] [CrossRef]
- Zizzo, G.; Cohen, P.L. Imperfect Storm: Is Interleukin-33 The Achilles Geel of COVID-19? Lancet Rheumatol. 2020, 2, e779–e790. [Google Scholar] [CrossRef]
- Pascual-Figal, D.A.; Pérez-Martínez, M.T.; Asensio-Lopez, M.C.; Sanchez-Más, J.; García-García, M.E.; Martinez, C.M.; Lencina, M.; Jara, R.; Januzzi, J.L.; Lax, A. Pulmonary Production of Soluble ST2 in Heart Failure. Circ. Heart Fail. 2018, 11, e005488. [Google Scholar] [CrossRef]
- Jones, A.; Pitre, T.; Junek, M.; Kapralik, J.; Patel, R.; Feng, E.; Dawson, L.; Tsang, J.L.Y.; Duong, M.; Ho, T.; et al. External Validation of the 4C Mortality Score among COVID-19 Patients Admitted to Hospital in Ontario, Canada: A Retrospective Study. Sci. Rep. 2021, 11, 18638. [Google Scholar] [CrossRef]
- Sarlo, F.; De Luca, C.; Moretti, G.; Urbani, A.; Baroni, S. Analytical Performance Evaluation of the New sST2 Turbidimetric Assay Implemented in Laboratory Automation Systems. Clin. Chem. Lab. Med. 2021, 60, e54–e56. [Google Scholar] [CrossRef]
- Dieplinger, B.; Egger, M.; Gegenhuber, A.; Haltmayer, M.; Mueller, T. Analytical and Clinical Evaluation of A Rapid Quantitative Lateral Flow Immunoassay for Measurement of Soluble ST2 in Human Plasma. Clin. Chim. Acta 2015, 451, 310–315. [Google Scholar] [CrossRef] [Green Version]
- Aurora, L.; Peterson, E.; Gui, H.; Zeld, N.; McCord, J.; Pinto, Y.; Cook, B.; Sabbah, H.N.; Keoki Williams, L.; Snider, J.; et al. Suppression Tumorigenicity 2 (ST2) Turbidimetric Immunoassay Compared to Enzyme-Linked Immunosorbent Assay in Predicting Survival in Heart Failure Patients with Reduced Ejection Fraction. Clin. Chim. Acta 2020, 510, 767–771. [Google Scholar] [CrossRef]
- Hanczar, B.; Hua, J.; Sima, C.; Weinstein, J.; Bittner, M.; Dougherty, E.R. Small-sample precision of ROC-related estimates. Bioinformatics 2010, 26, 822–830. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.W.; Kim, S.M.; Kim, Y.K.; Kim, J.Y.; Lee, Y.M.; Kim, B.O.; Hwangbo, S.; Park, T. Clinical Characteristics and Outcomes of COVID-19 Cohort Patients in Daegu Metropolitan City Outbreak in 2020. J. Korean Med. Sci. 2021, 36, e12. [Google Scholar] [CrossRef]
- Jeon, J.; Han, C.; Kim, T.; Lee, S. Evolution of Responses to COVID-19 and Epidemiological Characteristics in South Korea. Int. J. Environ. Res. Public Health 2022, 19, 4056. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | All Patients (n = 52) |
|---|---|
| Age, years | 71.0 (62.5–79.0) |
| Male | 32 (61.5) |
| BMI, kg/m2 | 24.1 (22.3–25.6) |
| Comorbidities | |
| DM | 18 (34.6) |
| Malignancy | 9 (17.3) |
| Chronic neurological conditions | 7 (13.7) |
| Chronic cardiac disease * | 6 (11.5) |
| Chronic respiratory disease (except asthma) | 5 (9.6) |
| Dementia | 5 (9.6) |
| Chronic kidney disease | 3 (5.8) |
| Connective tissue disease | 3 (5.8) |
| Others † | 3 (5.8) |
| Symptoms | |
| Fever or chilling | 33 (63.5) |
| General weakness | 23 (44.2) |
| Dyspnea | 28 (53.8) |
| Cough | 22 (42.3) |
| Sputum | 14 (26.9) |
| Gastrointestinal ‡ | 7 (13.5) |
| Neurological ∥ | 6 (11.5) |
| Myalgia | 5 (9.6) |
| Others ¶ | 5 (9.6) |
| Symptom duration, days | 4.0 (0.5–7.5) |
| COVID-19 diagnosis to admission, days | 0.0 (0.0–2.0) |
| COVID-19 diagnosis to blood sampling, days | 3.0 (0.0–11.0) |
| Hospital stays, days | 28.0 (16.5–47.5) |
| Treatment | |
| Oxygen support | 42 (80.8) |
| Antibiotics | 30 (57.7) |
| Antiviral agent (Lopinavir/Ritonavir) | 25 (48.1) |
| Hydroxychloroquine | 3 (5.8) |
| Severity assessment | |
| SOFA score | 4.0 (1.0–7.0) |
| WHO disease severity | |
| Mild disease | 1 (1.9) |
| Moderate disease | 14 (26.9) |
| Severe disease | 0 (0.0) |
| Critical disease | 37 (71.2) |
| Sepsis/septic shock ** | 31 (83.8)/6 (16.2) |
| Prognosis assessment | |
| 4C mortality score | 9.5 (7.5–12.0) |
| Low (0–3) | 2 (3.8) |
| Intermediate (4–8) | 15 (28.8) |
| High (9–14) | 30 (57.7) |
| Very high (≥15) | 5 (9.6) |
| Clinical outcomes | |
| ICU admission | 14 (26.9) |
| Ventilator use | 12 (23.1) |
| ECMO use | 7 (13.5) |
| 30-day mortality | 12 (23.1) |
| Vital signs | |
| SBP, mm Hg | 120.0 (110.0–140.0) |
| DBP, mm Hg | 71.5 (70.0–80.0) |
| HR, beats/min | 82.0 (74.0–93.5) |
| RR, breaths/min | 20.0 (20.0–23.0) |
| BT, ℃ | 37.1 (36.8–37.8) |
| SpO2, % | 96 (94.3–97.0) |
| Laboratory data | |
| WBC, ×109/L | 5.9 (4.8–8.6) |
| Hb, g/L | 120.0 (109.0–130.5) |
| PLT, ×109/L | 199.0 (148.0–268.0) |
| AST, U/L | 30.5 (23.0–44.0) |
| ALT, U/L | 24.5 (14.5–37.5) |
| Total bilirubin, umol/L | 12.7 (9.6–18.3) |
| Cr, umol/L | 76.5 (56.6–96.4) |
| Lactate, mmol/L | 1.8 (1.2–2.2) |
| CRP, mg/L | 36.4 (4.6–132.5) |
| NT-proBNP ††, pg/mL | 230.2 (111.6–852.3) |
| hs-TnI ‡‡, ng/mL | 0.01 (0.00–0.02) |
| sST2, ng/mL | 46.6 (18.8–106.6) |
| Variables | ICU Admission | Ventilator Use | ECMO Use | 30-Day Mortality | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Yes (n = 14) | No (n = 38) | p * | Yes (n = 12) | No (n = 40) | p * | Yes (n = 7) | No (n = 45) | p * | Yes (n = 12) | No (n = 40) | p * | |
| sST2, ng/mL | 242.7 (77.8–378.0) | 28.0 (16.3–59.5) | <0.001 | 295.1 (137.3–412.5) | 28.1 (16.3–59.1) | <0.001 | 252.5 (146.9–667.9) | 30.0 (17.6–76.9) | 0.002 | 154.8 (59.1–426.6) | 28.1 (16.3–79.2) | <0.001 |
| SOFA score | 7.5 (7.0–9.0) | 3.0 (1.0–4.0) | <0.001 | 8.0 (7.0–9.5) | 3.0 (0.5–4.0) | <0.001 | 8.0 (7.3–9.0) | 3.0 (1.0–5.0) | <0.001 | 7.5 (3.0–9.5) | 4.0 (0.5–5.5) | 0.023 |
| Critical disease | 13 (92.9) | 24 (63.2) | <0.043 | 12 (100.0) | 25 (62.5) | 0.011 | 7 (100.0) | 30 (66.7) | 0.093 | 10 (83.3) | 27 (67.5) | 0.470 |
| 4C mortality score | 10.5 (8.0–14.0) | 9.0 (7.0–12.0) | 0.099 | 11.5 (9.0–14.0) | 9.0 (7.0–11.5) | 0.039 | 11.0 (8.5–12.8) | 9.0 (7.0–12.0) | 0.367 | 13.0 (11.5–15.5) | 9.0 (7.0–10.0) | <0.001 |
| Low/intermediate | 4 (28.6) | 13 (34.2) | 0.765 | 3 (25.0) | 14 (35.0) | 0.579 | 2 (28.6) | 15 (33.3) | 0.582 | 1 (8.3) | 16 (40.0) | 0.002 |
| High | 8 (57.1) | 22 (57.9) | 7 (58.3) | 23 (57.5) | 5 (71.4) | 25 (55.6) | 7 (58.3) | 23 (57.5) | ||||
| Very high | 2 (14.3) | 3 (7.9) | 2 (16.7) | 3 (7.5) | 0 (0.0) | 5 (11.1) | 4 (33.3) | 1 (2.5) | ||||
| Variables | Low/Intermediate (n = 17) | High (n = 30) | Very High (n = 5) | p * |
|---|---|---|---|---|
| sST2, ng/mL | 19.2 (12.9–58.7) | 51.8 (22.9–118.3) | 76.6 (49.5–347.8) | 0.042 † |
| SOFA score | 3.0 (0.0–6.3) | 4.0 (2.0–7.0) | 8.0 (3.0–10.3) | 0.093 |
| Critical disease | 9 (52.9) | 23 (76.7) | 5 (100.0) | 0.073 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, M.; Hur, M.; Kim, H.; Lee, C.H.; Lee, J.H.; Kim, H.W.; Nam, M.; Lee, S. Soluble ST2 as a Useful Biomarker for Predicting Clinical Outcomes in Hospitalized COVID-19 Patients. Diagnostics 2023, 13, 259. https://doi.org/10.3390/diagnostics13020259
Park M, Hur M, Kim H, Lee CH, Lee JH, Kim HW, Nam M, Lee S. Soluble ST2 as a Useful Biomarker for Predicting Clinical Outcomes in Hospitalized COVID-19 Patients. Diagnostics. 2023; 13(2):259. https://doi.org/10.3390/diagnostics13020259
Chicago/Turabian StylePark, Mikyoung, Mina Hur, Hanah Kim, Chae Hoon Lee, Jong Ho Lee, Hyung Woo Kim, Minjeong Nam, and Seungho Lee. 2023. "Soluble ST2 as a Useful Biomarker for Predicting Clinical Outcomes in Hospitalized COVID-19 Patients" Diagnostics 13, no. 2: 259. https://doi.org/10.3390/diagnostics13020259