
How the COVID-19 Pandemic Affected Attendance at a Tertiary Orthopedic Center Emergency Department: A Comparison between the First and Second Waves
 , ,
, ,
Abstract
:1. Introduction
- The comparison of first-wave data with the immediate period before the COVID-19 outbreak and the same timeframe of the first wave in 2019.
- The comparison between the first and second waves of the pandemic.
2. Materials and Methods
2.1. Study Population
- Period A: 21 February 2020–31 May 2020 (first wave of the pandemic)
- Period B: 1 October 2020–31 December 2020 (second wave of the pandemic)
- Period C: 1 December 2019–20 February 2020 (three months immediately before the COVID-19 outbreak)
- Period D: 21 February 2019–31 May 2019 (same timeframe of first wave of the pandemic spread but in 2019)
- Age and sex
- Reason for admission (traumatic versus non-traumatic)
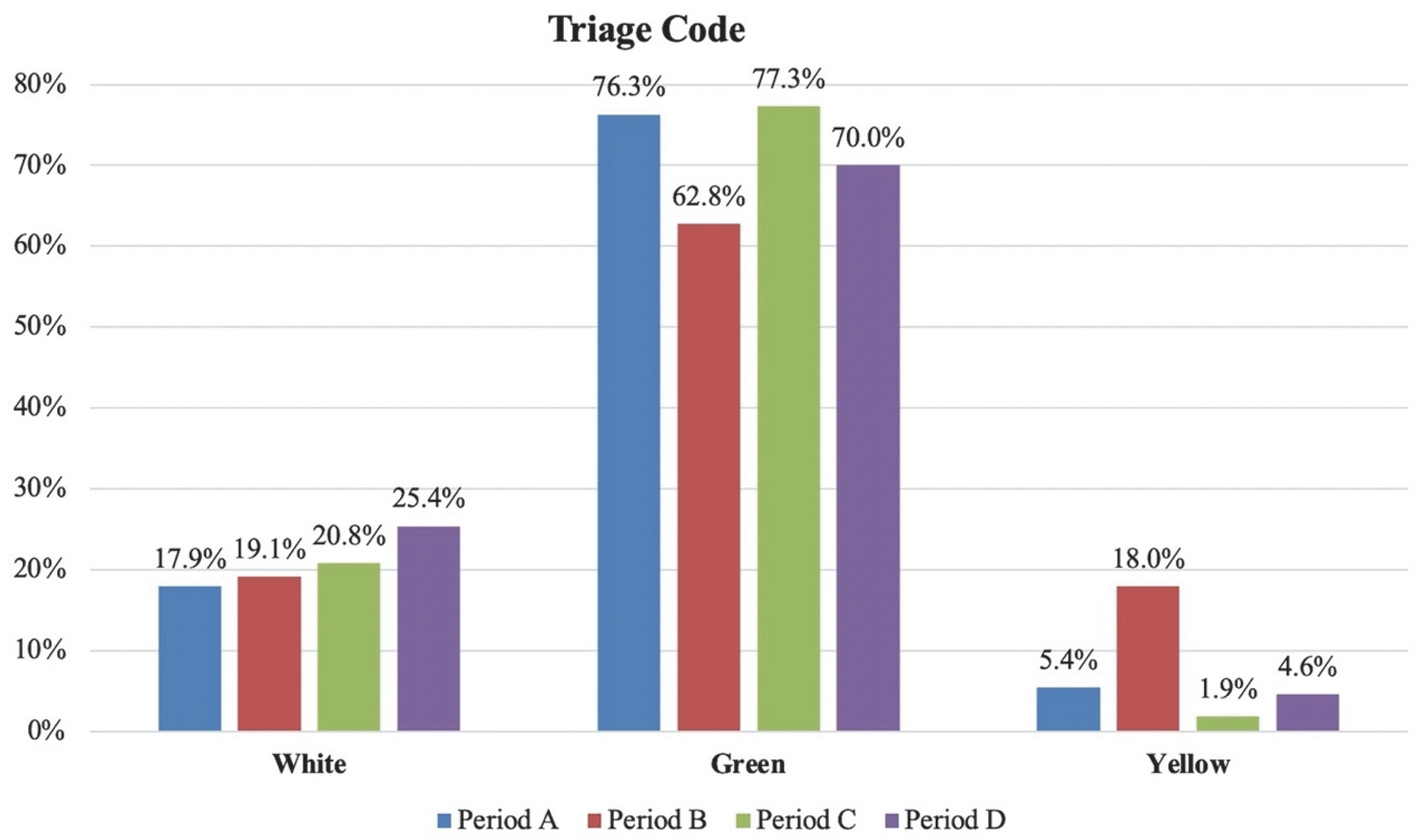
- Triage code at discharge: clinical severity according to four-degree urgency scale: white codes (non-urgent cases), green codes (urgent cases, not critical), yellow codes (moderately critical cases), red codes (highly urgent cases, risk of death). Admission triage code is assigned by paramedic staff according to a patient’s history and symptoms, whereas discharge triage code is assigned by the orthopedic surgeon at the end of the consultation (after the imaging study is performed, if needed).
- Discharge diagnosis (performed by the orthopedic surgeon).
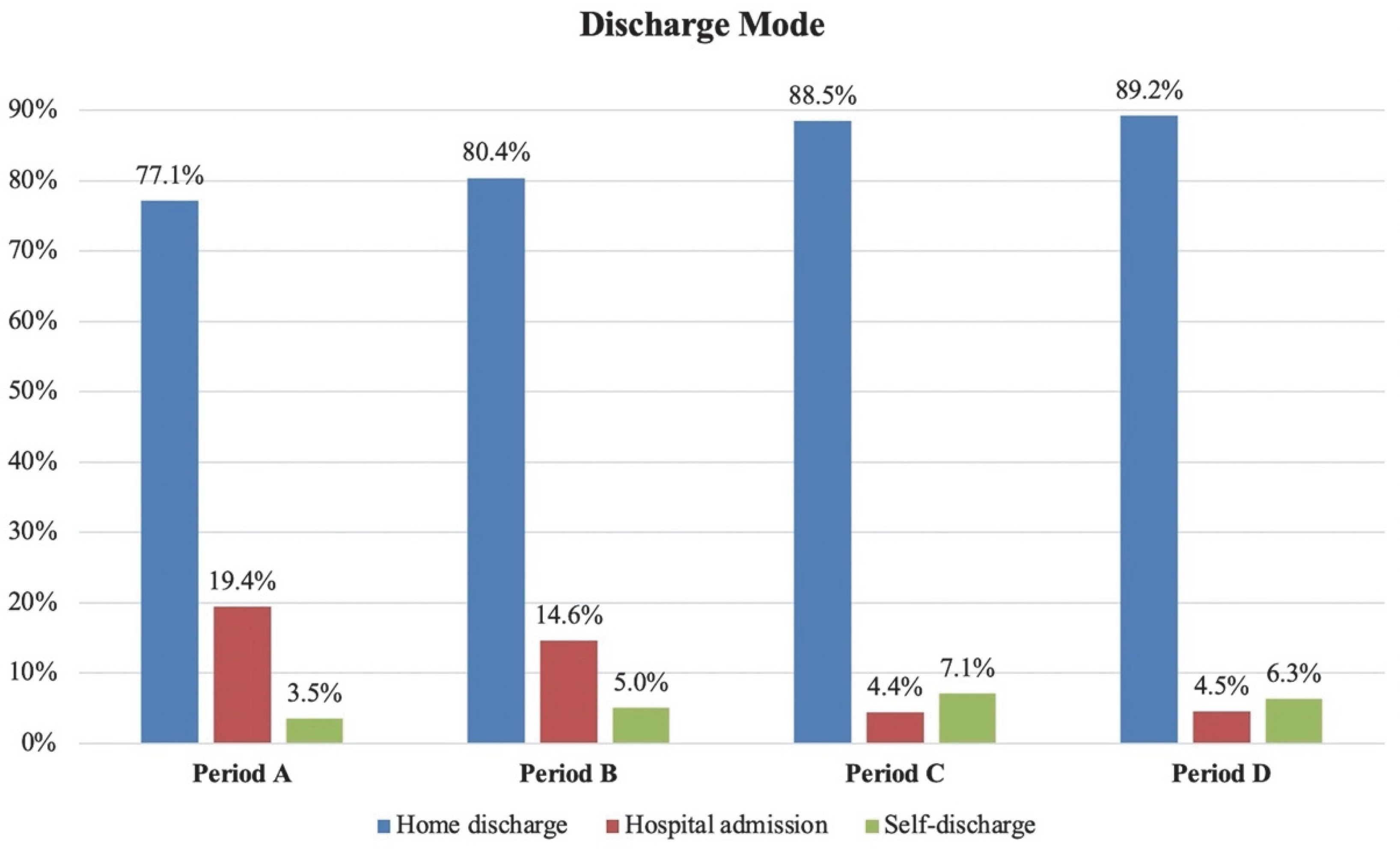
- Discharge destination (home discharge, hospital admission, or voluntary discharge)
2.2. Hospital Setting
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lombardi, A.F.; Afsahi, A.M.; Gupta, A.; Gholamrezanezhad, A. Severe Acute Respiratory Syndrome (SARS), Middle East Respiratory Syndrome (MERS), Influenza, and COVID-19, beyond the Lungs: A Review Article. Radiol. Med. 2021, 126, 561–569. [Google Scholar] [CrossRef]
- Briguglio, M.; Giorgino, R.; Dell’Osso, B.; Cesari, M.; Porta, M.; Lattanzio, F.; Banfi, G.; Peretti, G.M. Consequences for the Elderly After COVID-19 Isolation: FEaR (Frail Elderly amid Restrictions). Front. Psychol. 2020, 11, 565052. [Google Scholar] [CrossRef]
- Messina, C.; Buzzoni, A.C.; Gitto, S.; Almolla, J.; Albano, D.; Sconfienza, L.M. Disruption of Bone Densitometry Practice in a Northern Italy Orthopedic Hospital during the COVID-19 Pandemic. Osteoporos. Int. 2021, 32, 199–203. [Google Scholar] [CrossRef]
- Remuzzi, A.; Remuzzi, G. COVID-19 and Italy: What Next? Lancet 2020, 395, 1225–1228. [Google Scholar] [CrossRef]
- Castaldi, S.; Perrone, P.M.; Luconi, E.; Marano, G.; Auxilia, F.; Maraschini, A.; Bono, P.; Alagna, L.; Palomba, E.; Bandera, A.; et al. Hospital Acquired Infections in COVID-19 Patients in Sub Intensive Care Unit: Analysis of Two Waves of Admissions. Acta Biomed. 2022, 93, e2022313. [Google Scholar] [CrossRef]
- Bandirali, M.; Sconfienza, L.M.; Serra, R.; Brembilla, R.; Albano, D.; Pregliasco, F.E.; Messina, C. Chest Radiograph Findings in Asymptomatic and Minimally Symptomatic Quarantined Patients in Codogno, Italy during COVID-19 Pandemic. Radiology 2020, 295, 201102. [Google Scholar] [CrossRef] [Green Version]
- Vinceti, M.; Filippini, T.; Rothman, K.J.; Di Federico, S.; Orsini, N. SARS-CoV-2 Infection Incidence during the First and Second COVID-19 Waves in Italy. Environ. Res. 2021, 197, 111097. [Google Scholar] [CrossRef]
- Romano, V.; Ancillotti, M.; Mascalzoni, D.; Biasiotto, R. Italians Locked down: People’s Responses to Early COVID-19 Pandemic Public Health Measures. Humanit. Soc. Sci. Commun. 2022, 9, 342. [Google Scholar] [CrossRef]
- Grasselli, G.; Pesenti, A.; Cecconi, M. Critical Care Utilization for the COVID-19 Outbreak in Lombardy, Italy. JAMA 2020, 323, 1545–1546. [Google Scholar] [CrossRef] [Green Version]
- Brayda-Bruno, M.; Giorgino, R.; Gallazzi, E.; Morelli, I.; Manfroni, F.; Briguglio, M.; Accetta, R.; Mangiavini, L.; Peretti, G.M. How SARS-CoV-2 Pandemic Changed Traumatology and Hospital Setting: An Analysis of 498 Fractured Patients. J. Clin. Med. 2021, 10, 2585. [Google Scholar] [CrossRef]
- Luceri, F.; Morelli, I.; Accetta, R.; Mangiavini, L.; Maffulli, N.; Peretti, G.M. Italy and COVID-19: The Changing Patient Flow in an Orthopedic Trauma Center Emergency Department. J. Orthop. Surg. Res. 2020, 15, 323. [Google Scholar] [CrossRef]
- Giorgino, R.; Maggioni, D.M.; Viganò, M.; Verdoni, F.; Pandini, E.; Balbino, C.; Manta, N.; D’anchise, R.; Mangiavini, L. Knee Pathology before and after SARS-CoV-2 Pandemic: An Analysis of 1139 Patients. Healthcare 2021, 9, 1311. [Google Scholar] [CrossRef]
- Tagliafico, A.S.; Albano, D.; Torri, L.; Messina, C.; Gitto, S.; Bruno, F.; Barile, A.; Giovagnoni, A.; Miele, V.; Grassi, R.; et al. Impact of Coronavirus Disease 2019 (COVID-19) Outbreak on Radiology Research: An Italian Survey. Clin. Imaging 2021, 76, 144–148. [Google Scholar] [CrossRef]
- Stramare, R.; Carretta, G.; Capizzi, A.; Boemo, D.G.; Contessa, C.; Motta, R.; De Conti, G.; Causin, F.; Giraudo, C.; Donato, D. Radiological Management of COVID-19: Structure Your Diagnostic Path to Guarantee a Safe Path. Radiol. Med. 2020, 125, 691–694. [Google Scholar] [CrossRef]
- Colombini, A.; Lombardo, M.D.M.; de Girolamo, L.; De Vecchi, E.; Giorgino, R.; Peretti, G.M.; Banfi, G.; Mangiavini, L. COVID-19 in Elderly Patients Surgically Treated for Lower Limbs Fracture. J. Clin. Med. 2022, 11, 168. [Google Scholar] [CrossRef]
- Albano, D.; Bruno, A.; Bruno, F.; Calandri, M.; Caruso, D.; Clemente, A.; Coppolino, P.; Cozzi, D.; De Robertis, R.; Gentili, F.; et al. Impact of Coronavirus Disease 2019 (COVID-19) Emergency on Italian Radiologists: A National Survey. Eur. Radiol. 2020, 30, 6635–6644. [Google Scholar] [CrossRef]
- Borghesi, A.; Maroldi, R. COVID-19 Outbreak in Italy: Experimental Chest X-Ray Scoring System for Quantifying and Monitoring Disease Progression. Radiol. Med. 2020, 125, 509–513. [Google Scholar] [CrossRef]
- Vitale, J.A.; Bonato, M.; Borghi, S.; Messina, C.; Albano, D.; Corbetta, S.; Sconfienza, L.M.; Banfi, G. Home-Based Resistance Training for Older Subjects during the COVID-19 Outbreak in Italy: Preliminary Results of a Six-Months RCT. Int. J. Environ. Res. Public Health 2020, 17, 9533. [Google Scholar] [CrossRef]
- Druel, T.; Andeol, Q.; Rongieras, F.; Bertani, A.; Bordes, M.; Alvernhe, A. Evaluation of Containment Measures’ Effect on Orthopaedic Trauma Surgery during the COVID-19 Pandemic: A Retrospective Comparison between 2019 and 2020. Int. Orthop. 2020, 44, 2229–2234. [Google Scholar] [CrossRef]
- Borghesi, A.; Sverzellati, N.; Polverosi, R.; Balbi, M.; Baratella, E.; Busso, M.; Calandriello, L.; Cortese, G.; Farchione, A.; Iezzi, R.; et al. Impact of the COVID-19 Pandemic on the Selection of Chest Imaging Modalities and Reporting Systems: A Survey of Italian Radiologists. Radiol. Med. 2021, 126, 1258–1272. [Google Scholar] [CrossRef]
- Schiaffino, S.; Codari, M.; Cozzi, A.; Albano, D.; Alì, M.; Arioli, R.; Avola, E.; Bnà, C.; Cariati, M.; Carriero, S.; et al. Machine Learning to Predict In-Hospital Mortality in COVID-19 Patients Using Computed Tomography-Derived Pulmonary and Vascular Features. J. Pers. Med. 2021, 11, 501. [Google Scholar] [CrossRef]
- Giovagnoni, A. Facing the COVID-19 Emergency: We Can and We Do. Radiol. Med. 2020, 125, 337–338. [Google Scholar] [CrossRef] [Green Version]
- Francolini, G.; Desideri, I.; Stocchi, G.; Ciccone, L.P.; Salvestrini, V.; Garlatti, P.; Aquilano, M.; Greto, D.; Bonomo, P.; Meattini, I.; et al. Impact of COVID-19 on Workload Burden of a Complex Radiotherapy Facility. Radiol. Med. 2021, 126, 717–721. [Google Scholar] [CrossRef]
- Poggetti, A.; Del Chiaro, A.; Nucci, A.M.; Suardi, C.; Pfanner, S. How Hand and Wrist Trauma Has Changed during COVID-19 Emergency in Italy: Incidence and Distribution of Acute Injuries. What to Learn? J. Clin. Orthop. Trauma 2021, 12, 22–26. [Google Scholar] [CrossRef]
- Schiaffino, S.; Albano, D.; Cozzi, A.; Messina, C.; Arioli, R.; Bnà, C.; Bruno, A.; Carbonaro, L.A.; Carriero, A.; Carriero, S.; et al. CT-Derived Chest Muscle Metrics for Outcome Prediction in Patients with COVID-19. Radiology 2021, 300, E328–E336. [Google Scholar] [CrossRef]
- Man, C.Y.; Yeung, R.S.D.; Chung, J.Y.M.; Cameron, P.A. Impact of SARS on an Emergency Department in Hong Kong. Emerg. Med. 2003, 15, 418–422. [Google Scholar] [CrossRef]
- Hahn, A.; Brown, T.; Chapman, B.; Marr, A.; Stuke, L.; Greiffenstein, P.; Schoen, J.; Hunt, J.P.; Smith, A. How Did the COVID-19 Pandemic Affect Trauma Volume at an Urban Level I Trauma Center? Am. Surg. 2022, 88, 000313482110540. [Google Scholar] [CrossRef]
- Runtz, A.; Sleiman, L.; Dabert, A.; Obert, L.; Garbuio, P.; Pluvy, I.; Loisel, F. Has the COVID Lockdown Altered the Incidence and Management of Fragility Fractures in Older Adults? Case-Control Study at a French University Hospital. Orthop. Traumatol. Surg. Res. 2022, 103419. [Google Scholar] [CrossRef]
- Moroni, C.; Cozzi, D.; Albanesi, M.; Cavigli, E.; Bindi, A.; Luvarà, S.; Busoni, S.; Mazzoni, L.N.; Grifoni, S.; Nazerian, P.; et al. Chest X-Ray in the Emergency Department during COVID-19 Pandemic Descending Phase in Italy: Correlation with Patients’ Outcome. Radiol. Med. 2021, 126, 661–668. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Period A (1st Wave) 21 February 2020–31 May 2020 | Period B (2nd Wave) 1 October 2020–31 December 2020 | Period C 1 December 2019–20 February 2020 | Period D 21 February 2019–31 May 2019 | |||||
|---|---|---|---|---|---|---|---|---|
| n= | % | n= | % | n= | % | n= | % | |
| Total ED Admissions | 2516 | 4595 | 6278 | 7906 | ||||
| Gender | ||||||||
| Males | 1197 | 47.6% | 2222 | 48.4% | 3251 | 51.8% | 4080 | 51.6% |
| Females | 1319 | 52.4% | 2373 | 51.6% | 3027 | 48.2% | 3826 | 48.4% |
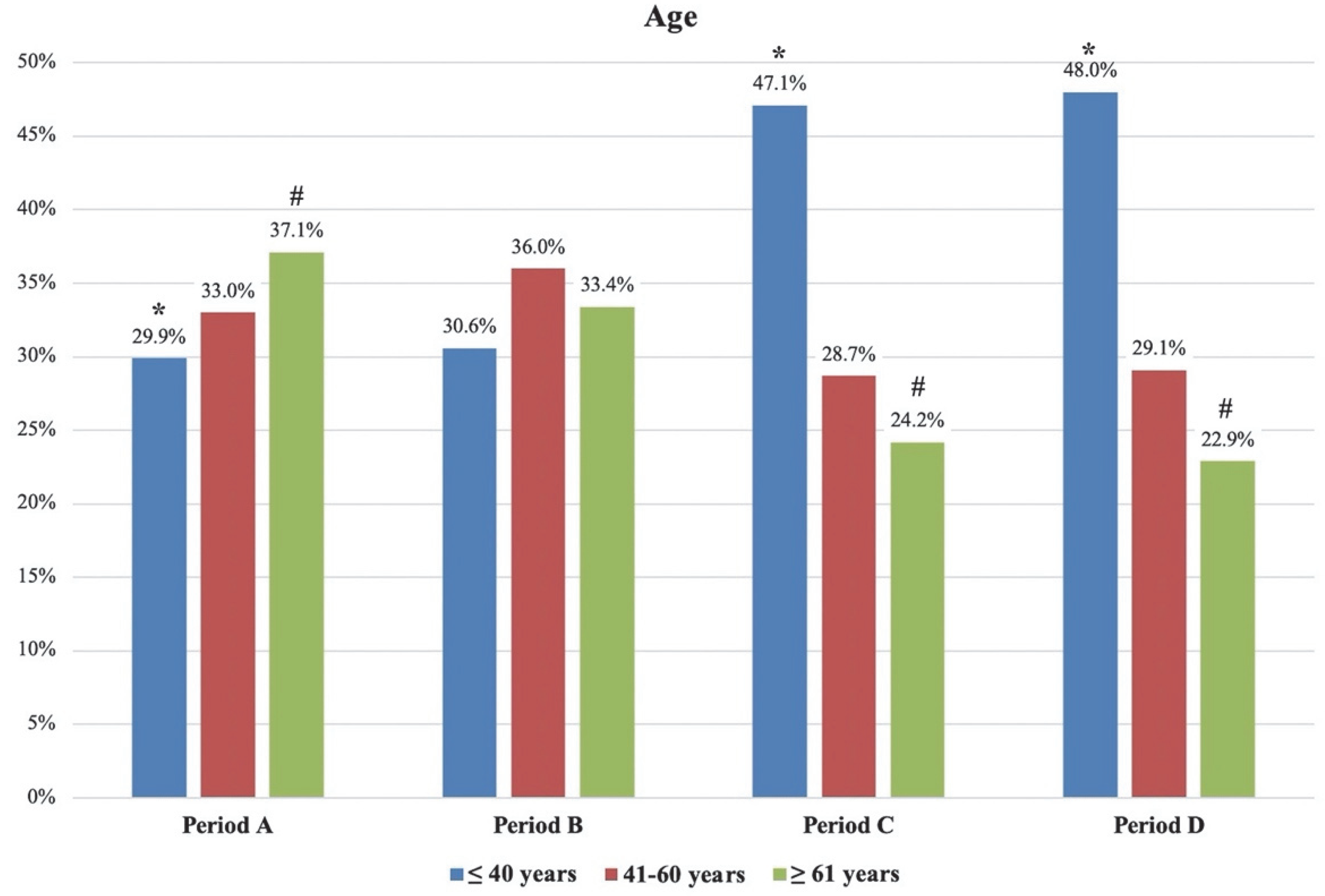
| Age | ||||||||
| ≤40 years | 751 | 29.9% | 1406 | 30.6% | 2958 | 47.1% | 3800 | 48.0% |
| 41–60 years | 831 | 33.0% | 1655 | 36.0% | 1801 | 28.7% | 2299 | 29.1% |
| ≥61 years | 934 | 37.1% | 1534 | 33.4% | 1519 | 24.2% | 1807 | 22.9% |
| Triage Code | ||||||||
| White | 450 | 17.9% | 877 | 19.1% | 1304 | 20.8% | 2007 | 25.4% |
| Green | 1921 | 76.3% | 2884 | 62.8% | 4855 | 77.3% | 5536 | 70.0% |
| Yellow | 136 | 5.4% | 827 | 18.0% | 118 | 1.9% | 362 | 4.6% |
| Red | 9 | 0.4% | 7 | 0.2% | 1 | 0.02% | 1 | 0.01% |
| Discharge | ||||||||
| Home discharge | 1939 | 77.1% | 3694 | 80.4% | 5558 | 88.5% | 7053 | 89.2% |
| Hospital admission | 489 | 19.4% | 673 | 14.6% | 276 | 4.4% | 357 | 4.5% |
| Self-discharge | 88 | 3.5% | 228 | 5.0% | 444 | 7.1% | 496 | 6.3% |
| Comparison between Periods A and B | Comparison between Periods A and C | Comparison between Periods A and D | ||||
|---|---|---|---|---|---|---|
| Absolute Variation | Relative Variation | Absolute Variation | Relative Variation | Absolute Variation | Relative Variation | |
| Total ED Admissions | −45.2% (*) | −59.9% (*) | −68.2% (*) | |||
| Gender | ||||||
| Males | −46.1% (*) | −0.8% | −63.2% (*) | −4.2% | −70.7% (*) | −4.0% |
| Females | −44.4% (*) | +0.8% | −56.4% (*) | +4.2% | −65.5% (*) | +4.0% |
| Age | ||||||
| ≤40 years | −46.6% (*) | −0.7% | −74.6% (*) | −17.2% (*) | −80.2% (*) | −18.2% (*) |
| 41–60 years | −49.8% (*) | −3.0% | −53.9% (*) | +4.3% | −63.9% (*) | +3.9% |
| ≥61 years | −39.1% (*) | +3.7% | −38.5% (*) | +12.9% (*) | −48.3% (*) | +14.2% (*) |
| Triage Code | ||||||
| White | −48.7% (*) | −1.2% | −65.5% (*) | −2.9% | −77.6% (*) | −7.5% (*) |
| Green | −33.4% (*) | +13.5% (*) | −60.4% (*) | −1.0% | −65.3% (*) | +6.3% |
| Yellow | −83.6% (*) | −12.6% (*) | −15.3% (*) | +3.5% | −62.4% (*) | +0.8% |
| Red | +28.6% (*) | +0.2% | +800.0% (*) | +0.3% | +800.0% (*) | +0.3% |
| Discharge | ||||||
| Home discharge | −47.5% (*) | −3.3% | −65.1% (*) | −11.4% (*) | −72.5% (*) | −12.1% (*) |
| Hospital admission | −27.3% (*) | +4.8% | +77.2% (*) | +15.0% (*) | +37.0% (*) | +14.9% (*) |
| Self-discharge | −61.4% (*) | −1.5% | −80.2% (*) | −3.6% | −82.3% (*) | −2.8% |
| Period A (1st Wave) 21 February 2020–31 May 2020 | Period B (2nd Wave) 1 October 2020–31 December 2020 | Period C 1 December 2019–20 February 2020 | Period D 21 February 2019–31 May 2019 | |||||
|---|---|---|---|---|---|---|---|---|
| Total ED Admissions | 2516 | 4595 | 6278 | 7906 | ||||
| Total fractures | 907 | 36.0% | 1571 | 34.2% | 1422 | 22.7% | 1666 | 21.1% |
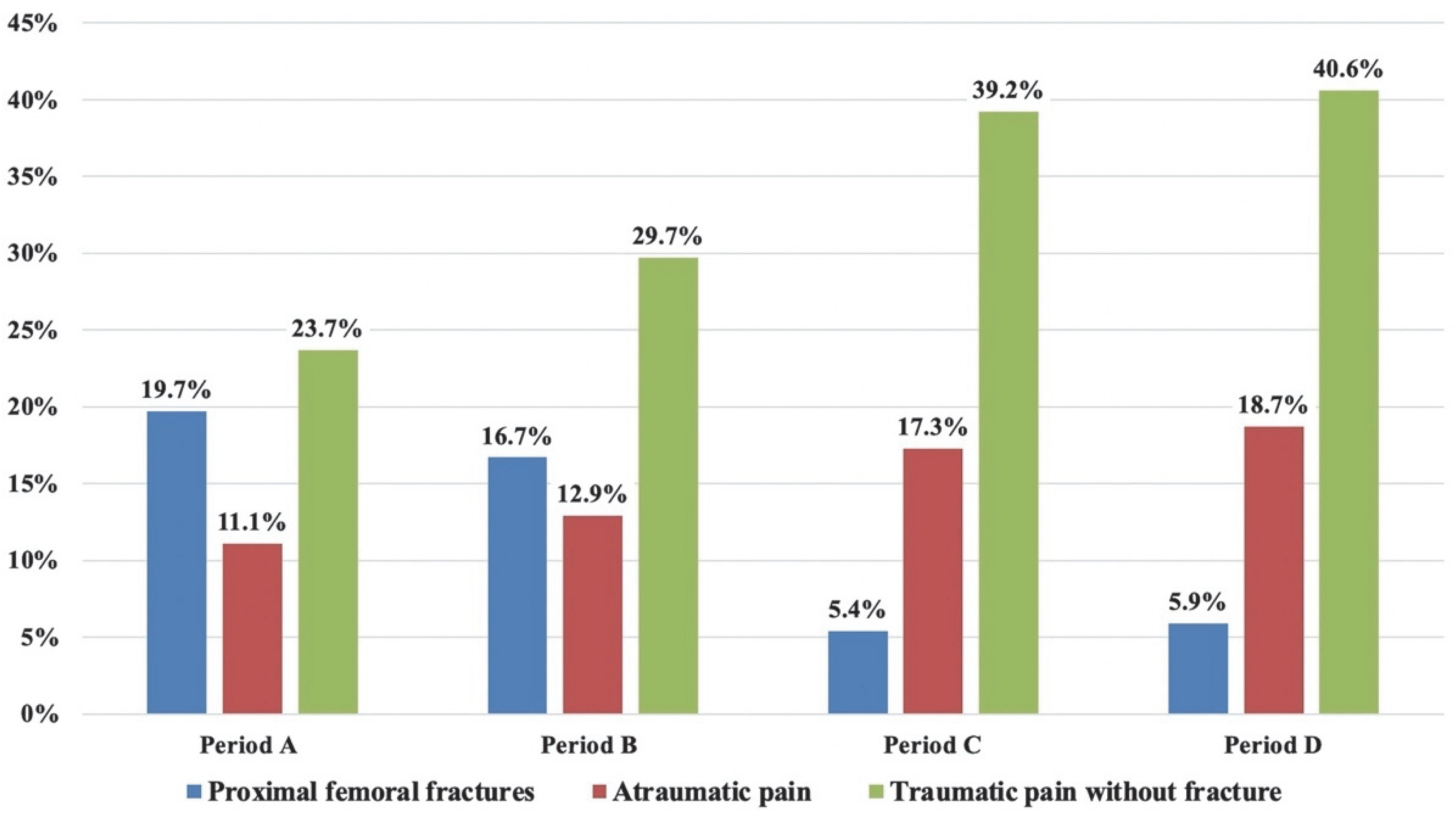
| Proximal femoral fractures | 179 | 19.7% | 262 | 16.7% | 77 | 5.4% | 99 | 5.9% |
| Atraumatic pain | ||||||||
| Lower back pain | 70 | 2.8% | 171 | 3.7% | 303 | 4.8% | 384 | 4.9% |
| Sciatica | 36 | 1.4% | 96 | 2.1% | 142 | 2.3% | 242 | 3.1% |
| Joint pain | 109 | 4.3% | 226 | 4.9% | 421 | 6.7% | 600 | 7.6% |
| Malaise | 33 | 1.3% | 38 | 0.8% | 104 | 1.7% | 127 | 1.6% |
| Osteoarthritis | 22 | 0.9% | 40 | 0.9% | 80 | 1.3% | 91 | 1.2% |
| Tendinitis | 10 | 0.4% | 22 | 0.5% | 35 | 0.6% | 31 | 0.4% |
| Total | 280 | 11.1% | 593 | 12.9% | 1085 | 17.3% | 1456 | 18.7% |
| Traumatic pain without fracture | ||||||||
| Bone contusion | 253 | 10.1% | 655 | 14.3% | 898 | 14.3% | 1087 | 13.7% |
| Joint sprain | 343 | 13.6% | 712 | 15.5% | 1561 | 24.9% | 2123 | 26.9% |
| Total | 596 | 23.7% | 1367 | 29.7% | 2459 | 39.2% | 3210 | 40.6% |
| Comparison between Periods A and B | Comparison between Periods A and C | Comparison between Periods A and D | ||||
|---|---|---|---|---|---|---|
| Absolute Variation | Relative Variation | Absolute Variation | Relative Variation | Absolute Variation | Relative Variation | |
| Total ED Admissions | −45.2% (*) | −59.9% (*) | −68.2% (*) | |||
| Total fractures | −42.3% (*) | +1.8% | −36.2% (*) | +13.3% (*) | −45.6% (*) | +14.9% (*) |
| Proximal femoral fractures | −31.7% (*) | +3.0% | +132.5% (*) | +14.3% (*) | +80.8% (*) | +13.8% (*) |
| Atraumatic pain | ||||||
| Lower back pain | −59.1% (*) | −0.9% | −76.9% (*) | −2.0% | −81.8% (*) | −2.1% |
| Sciatica | −62.5% (*) | −0.7% | −74.6% (*) | −0.9% | −85.1% (*) | −1.7% |
| Joint pain | −51.8% (*) | −0.6% | −74.1% (*) | −2.4% | −81.8% (*) | −3.3% |
| Malaise | −13.2% (*) | +0.5% | −68.3% (*) | −0.4% | −74.0% (*) | −0.3% |
| Osteoarthritis | −45.0% (*) | 0% | −72.5% (*) | −0.4% | −75.8% (*) | −0.3% |
| Tendinitis | −54.5% (*) | −0.1% | −71.4% (*) | −0.2% | −67.7% (*) | 0% |
| Total | −52.8% (*) | −1.8% | −74.2% (*) | −6.2% | −80.8% (*) | −7.6% (*) |
| Traumatic pain without fracture | ||||||
| Bone contusion | −61.4% | −4.2% | −71.8% | −4.2% | −76.7% | −3.6% |
| Joint sprain | −51.8% | −1.9% | −78.0% | −11.3% (*) | −83.8% | −13.3% (*) |
| Total | −56.4% | −6.0% | −75.8% | −15.5% (*) | −81.4% | −16.9% (*) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carlicchi, E.; Di Sabato, M.E.; Cincotta, A.; Accetta, R.; Aliprandi, A.; Albano, D.; Sconfienza, L.M.; Messina, C. How the COVID-19 Pandemic Affected Attendance at a Tertiary Orthopedic Center Emergency Department: A Comparison between the First and Second Waves. Diagnostics 2022, 12, 2855. https://doi.org/10.3390/diagnostics12112855
Carlicchi E, Di Sabato ME, Cincotta A, Accetta R, Aliprandi A, Albano D, Sconfienza LM, Messina C. How the COVID-19 Pandemic Affected Attendance at a Tertiary Orthopedic Center Emergency Department: A Comparison between the First and Second Waves. Diagnostics. 2022; 12(11):2855. https://doi.org/10.3390/diagnostics12112855
Chicago/Turabian StyleCarlicchi, Eleonora, Maria Eugenia Di Sabato, Antonino Cincotta, Riccardo Accetta, Alberto Aliprandi, Domenico Albano, Luca Maria Sconfienza, and Carmelo Messina. 2022. "How the COVID-19 Pandemic Affected Attendance at a Tertiary Orthopedic Center Emergency Department: A Comparison between the First and Second Waves" Diagnostics 12, no. 11: 2855. https://doi.org/10.3390/diagnostics12112855