
Development of an In-House EphA2 ELISA for Human Serum and Measurement of Circulating Levels of EphA2 in Hypertensive Patients with Renal Dysfunction
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Monoclonal Antibodies to Human EphA2
2.2. Novel ELISA for Detecting of Human EphA2
2.3. Validation Procedures
2.3.1. Specificity
2.3.2. Accuracy
2.3.3. Lower Limit of Detection and Quantitation Limit
2.3.4. Precision
2.3.5. Measurement with a Commercially Available EphA2 ELISA
2.4. Patients and Sample Collection
2.5. Patients and Sample Collection
3. Results
3.1. Validation of the Novel In-House EphA2 ELISA
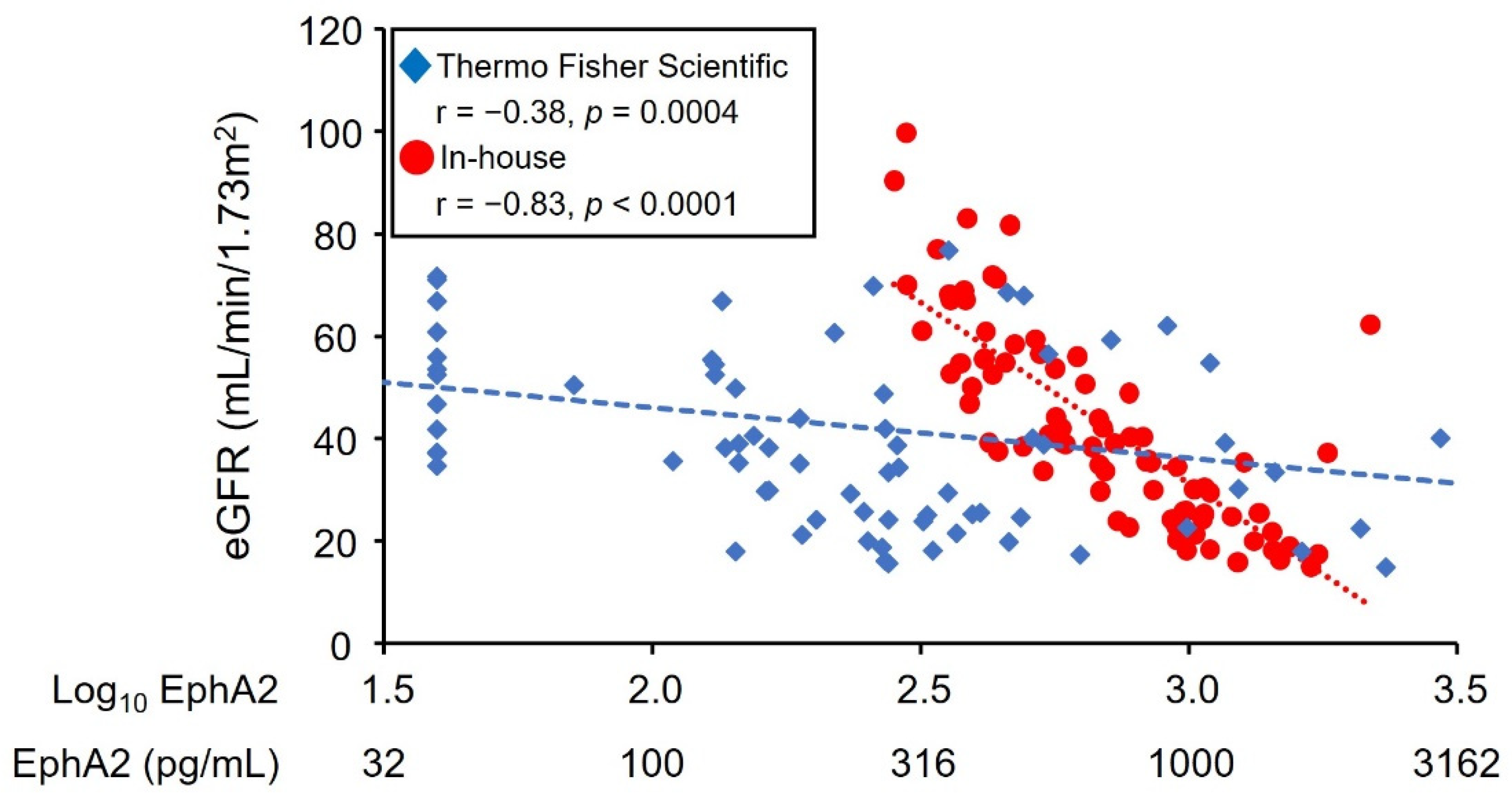
3.2. Comparison with the EphA2 ELISA Kit from Thermo Fisher Scientific
3.3. Circulating EphA2 Levels in Patients with Hypertension
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bikbov, B.; Purcell, C.A.; Levey, A.S.; Smith, M.; Abdoli, A.; Abebe, M.; Adebayo, O.M.; Afarideh, M.; Agarwal, S.K.; Agudelo-Botero, M.; et al. Global, regional, and national burden of chronic kidney disease, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murakoshi, M.; Gohda, T.; Sakuma, H.; Shibata, T.; Adachi, E.; Kishida, C.; Ichikawa, S.; Koshida, T.; Kamei, N.; Suzuki, Y. Progranulin and Its Receptor Predict Kidney Function Decline in Patients with Type 2 Diabetes. Front. Endocrinol. (Lausanne) 2022, 13, 849457. [Google Scholar] [CrossRef] [PubMed]
- Gohda, T.; Yanagisawa, N.; Murakoshi, M.; Ueda, S.; Nishizaki, Y.; Nojiri, S.; Ohashi, Y.; Ohno, I.; Shibagaki, Y.; Imai, N.; et al. Association between Kidney Function Decline and Baseline TNFR Levels or Change Ratio in TNFR by Febuxostat Chiefly in Non-diabetic CKD Patients with Asymptomatic Hyperuricemia. Front. Med. (Lausanne) 2021, 8, 634932. [Google Scholar] [CrossRef]
- Gohda, T.; Niewczas, M.A.; Ficociello, L.H.; Walker, W.H.; Skupien, J.; Rosetti, F.; Cullere, X.; Johnson, A.C.; Crabtree, G.; Smiles, A.M.; et al. Circulating TNF receptors 1 and 2 predict stage 3 CKD in type 1 diabetes. J. Am. Soc. Nephrol. 2012, 23, 516–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niewczas, M.A.; Gohda, T.; Skupien, J.; Smiles, A.M.; Walker, W.H.; Rosetti, F.; Cullere, X.; Eckfeldt, J.H.; Doria, A.; Mayadas, T.N.; et al. Circulating TNF receptors 1 and 2 predict ESRD in type 2 diabetes. J. Am. Soc. Nephrol. 2012, 23, 507–515. [Google Scholar] [CrossRef] [Green Version]
- Kamei, N.; Yamashita, M.; Nishizaki, Y.; Yanagisawa, N.; Nojiri, S.; Tanaka, K.; Yamashita, Y.; Shibata, T.; Murakoshi, M.; Suzuki, Y.; et al. Association between circulating tumor necrosis factor-related biomarkers and estimated glomerular filtration rate in type 2 diabetes. Sci. Rep. 2018, 8, 15302. [Google Scholar] [CrossRef] [Green Version]
- Chitramuthu, B.P.; Bennett, H.P.J.; Bateman, A. Progranulin: A new avenue towards the understanding and treatment of neurodegenerative disease. Brain 2017, 140, 3081–3104. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, Y.; Chambers, J.K.; Matsuwaki, T.; Yamanouchi, K.; Nishihara, M. Possible involvement of lysosomal dysfunction in pathological changes of the brain in aged progranulin-deficient mice. Acta Neuropathol. Commun. 2014, 2, 78. [Google Scholar] [CrossRef]
- Neill, T.; Buraschi, S.; Goyal, A.; Sharpe, C.; Natkanski, E.; Schaefer, L.; Morrione, A.; Iozzo, R.V. EphA2 is a functional receptor for the growth factor progranulin. J. Cell Biol. 2016, 215, 687–703. [Google Scholar] [CrossRef] [Green Version]
- Miao, B.; Ji, Z.; Tan, L.; Taylor, M.; Zhang, J.; Choi, H.G.; Frederick, D.T.; Kumar, R.; Wargo, J.A.; Flaherty, K.T.; et al. EPHA2 is a mediator of vemurafenib resistance and a novel therapeutic target in melanoma. Cancer Discov. 2015, 5, 274–287. [Google Scholar] [CrossRef]
- Zhao, P.; Jiang, D.; Huang, Y.; Chen, C. EphA2: A promising therapeutic target in breast cancer. J. Genet. Genom. 2021, 48, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.; Shahzad, M.M.; Wang, H.; Landen, C.N.; Kim, S.W.; Allen, J.; Nick, A.M.; Jennings, N.; Kinch, M.S.; Bar-Eli, M.; et al. EphA2 overexpression promotes ovarian cancer growth. Cancer Biol. Ther. 2008, 7, 1098–1103. [Google Scholar] [CrossRef] [Green Version]
- Hirai, H.; Maru, Y.; Hagiwara, K.; Nishida, J.; Takaku, F. A novel putative tyrosine kinase receptor encoded by the eph gene. Science 1987, 238, 1717–1720. [Google Scholar] [CrossRef] [PubMed]
- Park, J.E.; Son, A.I.; Zhou, R. Roles of EphA2 in Development and Disease. Genes 2013, 4, 334–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruiz, J.C.; Robertson, E.J. The expression of the receptor-protein tyrosine kinase gene, eck, is highly restricted during early mouse development. Mech. Dev. 1994, 46, 87–100. [Google Scholar] [CrossRef] [PubMed]
- Cooper, M.A.; Son, A.I.; Komlos, D.; Sun, Y.; Kleiman, N.J.; Zhou, R. Loss of ephrin-A5 function disrupts lens fiber cell packing and leads to cataract. Proc. Natl. Acad. Sci. USA 2008, 105, 16620–16625. [Google Scholar] [CrossRef] [Green Version]
- Noberini, R.; Koolpe, M.; Peddibhotla, S.; Dahl, R.; Su, Y.; Cosford, N.D.; Roth, G.P.; Pasquale, E.B. Small molecules can selectively inhibit ephrin binding to the EphA4 and EphA2 receptors. J. Biol. Chem. 2008, 283, 29461–29472. [Google Scholar] [CrossRef] [Green Version]
- Finney, A.C.; Funk, S.D.; Green, J.M.; Yurdagul, A., Jr.; Rana, M.A.; Pistorius, R.; Henry, M.; Yurochko, A.; Pattillo, C.B.; Traylor, J.G.; et al. EphA2 Expression Regulates Inflammation and Fibroproliferative Remodeling in Atherosclerosis. Circulation 2017, 136, 566–582. [Google Scholar] [CrossRef]
- Hafner, C.; Schmitz, G.; Meyer, S.; Bataille, F.; Hau, P.; Langmann, T.; Dietmaier, W.; Landthaler, M.; Vogt, T. Differential gene expression of Eph receptors and ephrins in benign human tissues and cancers. Clin. Chem. 2004, 50, 490–499. [Google Scholar] [CrossRef] [Green Version]
- Satake, E.; Saulnier, P.J.; Kobayashi, H.; Gupta, M.K.; Looker, H.C.; Wilson, J.M.; Md Dom, Z.I.; Ihara, K.; O’Neil, K.; Krolewski, B.; et al. Comprehensive Search for Novel Circulating miRNAs and Axon Guidance Pathway Proteins Associated with Risk of ESKD in Diabetes. J. Am. Soc. Nephrol. 2021, 32, 2331–2351. [Google Scholar] [CrossRef]
- Kouros-Mehr, H.; Werb, Z. Candidate regulators of mammary branching morphogenesis identified by genome-wide transcript analysis. Dev. Dyn. 2006, 235, 3404–3412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nahm, O.; Woo, S.K.; Handler, J.S.; Kwon, H.M. Involvement of multiple kinase pathways in stimulation of gene transcription by hypertonicity. Am. J. Physiol. Cell Physiol. 2002, 282, C49–C58. [Google Scholar] [CrossRef] [Green Version]
- Baldwin, C.; Chen, Z.W.; Bedirian, A.; Yokota, N.; Nasr, S.H.; Rabb, H.; Lemay, S. Upregulation of EphA2 during in vivo and in vitro renal ischemia-reperfusion injury: Role of Src kinases. Am. J. Physiol. Renal Physiol. 2006, 291, F960–F971. [Google Scholar] [CrossRef]
- Costantino, V.V.; Gil Lorenzo, A.F.; Bocanegra, V.; Vallés, P.G. Molecular Mechanisms of Hypertensive Nephropathy: Renoprotective Effect of Losartan through Hsp70. Cells 2021, 10, 3146. [Google Scholar] [CrossRef] [PubMed]
- Xiao, T.; Xiao, Y.; Wang, W.; Tang, Y.Y.; Xiao, Z.; Su, M. Targeting EphA2 in cancer. J. Hematol. Oncol. 2020, 13, 114. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Total (n = 80) | eGFR (mL/min/1.73 m2) | p | |
|---|---|---|---|---|
| <60 (n = 64) | ≥60 (n = 16) | (<60 vs. ≥60) | ||
| eGFR, mL/min/1.73 m2 | 39 (26, 56) | 35 (24, 43) | 71 (67, 79) | By design |
| eGFR categories, no | ||||
| G1+2 (≥60 mL/min/1.73 m2) | 16 | |||
| G3a (45–59 mL/min/1.73 m2) | 14 | |||
| G3b (30–44 mL/min/1.73 m2) | 26 | |||
| G4 (15–29 mL/min/1.73 m2) | 24 | |||
| Age, year | 72 ± 11 | 73 ± 11 | 68 ± 6 | 0.13 |
| Male, no (%) | 52 (65.0) | 43 (67.2) | 9 (56.3) | 0.42 |
| SBP, mmHg | 128 ± 13 | 128 ± 13 | 125 ± 11 | 0.42 |
| DBP, mmHg | 73 ± 10 | 72 ± 10 | 78 ± 8 | 0.03 |
| RAS blockers Tx, no (%) | 54 (67.5) | 43 (67.2) | 11 (68.8) | 0.91 |
| UPCR, g/gCr | 0.38 (0.10, 1.00) | 0.50 (0.19, 1.46) | 0.09 (0.06, 0.26) | <0.0001 |
| EphA2, pg/mL | 682 (434, 1006) | 775 (564, 1061) | 382 (329, 430) | <0.0001 |
| Vendor | In-House | Thermo Fisher Scientific | ||
|---|---|---|---|---|
| EphA2 | r | p | r | p |
| Age | 0.37 | 0.0007 | 0.03 | 0.82 |
| SBP | 0.16 | 0.16 | 0.19 | 0.08 |
| DBP | −0.26 | 0.02 | 0.07 | 0.57 |
| eGFR | −0.83 | <0.0001 | −0.38 | 0.0004 |
| UPCR | 0.61 | <0.0001 | 0.23 | 0.04 |
| Variable | β | F | p |
|---|---|---|---|
| Age | 0.003 | 4.69 | 0.03 |
| eGFR | −0.156 | 76.91 | <0.0001 |
| UPCR | 0.031 | 3.33 | 0.07 |
| DBP | 0.0003 | 0.03 | 0.86 |
| R2 | 0.70 | ||
| Baseline Characteristics (Units of Increase) | Model 1 | Model 2 | Model 3 | |||
|---|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| Sex (female) | 0.96 (0.21, 4.50) | 0.96 | 1.02 (0.21, 4.92) | 0.98 | 0.82 (0.15, 4.50) | 0.82 |
| Age (10 year) | 1.33 (0.50, 3.57) | 0.57 | 1.21 (0.40, 3.66) | 0.74 | 1.35 (0.50, 3.63) | 0.55 |
| UPCR (1 quartile) | 3.79 (1.31, 10.99) | 0.014 | 3.98 (1.32, 12.02) | 0.01 | 3.81 (1.32, 11.00) | 0.01 |
| EphA2 (1 quartile) | 4.74 (1.46, 15.42) | 0.0096 | 4.48 (1.36, 14.72) | 0.01 | 4.84 (1.47, 15.93) | 0.01 |
| DBP (10 mmHg) | 0.74 (0.36, 1.53) | 0.42 | ||||
| BP control (poor) | 1.58 (0.23, 11.06) | 0.64 | ||||
| Baseline Characteristics (Units of Increase) | Model 1 | Model 2 | Model 3 | |||
|---|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| Sex (female) | 0.45 (0.08, 2.43) | 0.35 | 0.39 (0.07, 2.17) | 0.28 | 0.33 (0.06, 1.95) | 0.22 |
| Age (10 year) | 0.74 (0.40, 1.38) | 0.45 | 0.68 (0.36, 1.30) | 0.24 | 0.88 (0.46, 1.66) | 0.68 |
| UPCR (1 quartile) | 2.43 (1.09, 5.43) | 0.03 | 2.45 (1.07, 5.60) | 0.03 | 2.79 (1.16, 6.75) | 0.02 |
| EphA2 (1 quartile) | 8.78 (2.68, 28.78) | 0.0003 | 10.42 (2.71, 40.07) | 0.0006 | 9.56 (2.81, 32.48) | 0.0003 |
| DBP (10 mmHg) | 0.59 (0.24, 1.47) | 0.26 | ||||
| BP control (poor) | 0.25 (0.03, 1.90) | 0.18 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murakoshi, M.; Iwasawa, T.; Koshida, T.; Suzuki, Y.; Gohda, T.; Kato, K. Development of an In-House EphA2 ELISA for Human Serum and Measurement of Circulating Levels of EphA2 in Hypertensive Patients with Renal Dysfunction. Diagnostics 2022, 12, 3023. https://doi.org/10.3390/diagnostics12123023
Murakoshi M, Iwasawa T, Koshida T, Suzuki Y, Gohda T, Kato K. Development of an In-House EphA2 ELISA for Human Serum and Measurement of Circulating Levels of EphA2 in Hypertensive Patients with Renal Dysfunction. Diagnostics. 2022; 12(12):3023. https://doi.org/10.3390/diagnostics12123023
Chicago/Turabian StyleMurakoshi, Maki, Takumi Iwasawa, Takeo Koshida, Yusuke Suzuki, Tomohito Gohda, and Kazunori Kato. 2022. "Development of an In-House EphA2 ELISA for Human Serum and Measurement of Circulating Levels of EphA2 in Hypertensive Patients with Renal Dysfunction" Diagnostics 12, no. 12: 3023. https://doi.org/10.3390/diagnostics12123023