
NGAL as Biomarker of Clinical and Subclinical Damage of Kidney Function after Coronary Angiography
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Populations
2.2. Laboratory Measures
2.3. Study Endpoints and Definitions
2.4. Statistical Methods (Statistical Analysis)
3. Results
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Morcos, S.K.; Thomsen, H.S.; Webb, J.A.W. Contrast-media-induced nephrotoxicity: A consensus report. Contrast Media Safety Committee, European Society of Urogenital Radiology (ESUR). Eur. Radiol. 1999, 9, 1602–1613. [Google Scholar] [CrossRef] [PubMed]
- Khwaja, A. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney International Supplements. Nephron Clin. Pract. 2012, 2 (Suppl. S1), c184. [Google Scholar]
- American College of Radiology Committee on Drugs and Contrast Media. ACR Manual on Contrast Media, Version 10.3. 2018. Available online: https://www.acr.org/-/media/ACR/Files/Clinical-Resources/Contrast_Media.pdf8 (accessed on 14 June 2019).
- van der Molen, A.J.; Reimer, P.; Dekkers, I.A.; Bongartz, G.; Bellin, M.F.; Bertolotto, M.; Clement, O.; Heinz-Peer, G.; Stacul, F.; Webb, J.A.; et al. Post-contrast acute kidney injury—Part 1: Definition, clinical features, incidence, role of contrast medium and risk factors. Recommendations for updated ESUR Contrast Medium Safety Committee guidelines. Eur. Radiol. 2018, 28, 2845–2855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.; Duan, N.; Zhao, J.; Li, Z.; Dong, P.; Wang, S.; Zhao, Y.; Wang, L. Furosemide with Saline Hydration for Prevention of Contrast-Induced Nephropathy in Patients undergoing Coronary Angiography: A Meta-Analysis of Randomized Controlled Trials. Experiment 2015, 21, 292–297. [Google Scholar] [CrossRef] [Green Version]
- Tsai, T.T.; Patel, U.D.; Chang, T.I.; Kennedy, K.F.; Masoudi, F.A.; Matheny, M.E.; Kosiborod, M.; Amin, A.P.; Messenger, J.C.; Rumsfeld, J.S.; et al. Contemporary Incidence, Predictors, and Outcomes of Acute Kidney Injury in Patients Undergoing Percutaneous Coronary Interventions. Insights From the NCDR Cath-PCI Registry. JACC Cardiovasc. Interv. 2014, 7, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Gargiulo, G.; Sannino, A.; Capodanno, D.; Barbanti, M.; Buccheri, S.; Perrino, C.; Capranzano, P.; Indolfi, C.; Trimarco, B.; Tamburino, C.; et al. Transcatheter aortic valve implantation versus surgical aortic valve replacement: A systematic review and meta-analysis. Ann. Intern. Med. 2016, 165, 334–344. [Google Scholar] [CrossRef]
- Gargiulo, G.; Sannino, A.; Capodanno, D.; Perrino, C.; Capranzano, P.; Barbanti, M.; Stabile, E.; Trimarco, B.; Tamburino, C.; Esposito, G. Impact of postoperative acute kidney injury on clinical outcomes after transcatheter aortic valve implantation: A meta-analysis of 5971 patients. Catheter. Cardiovasc. Interv. 2015, 86, 518–527. [Google Scholar] [CrossRef]
- Zlatanovic, P.; Koncar, I.; Dragas, M.; Ilic, N.; Sladojevic, M.; Mutavdzic, P.; Tomic, I.; Kostic, D.; Davidovic, L. Combined Impact of Chronic Kidney Disease and Contrast Induced Acute Kidney Injury on Long-term Outcomes in Patients with Acute Lower Limb Ischaemia. Eur. J. Vasc. Endovasc. Surg. 2018, 56, 78–86. [Google Scholar] [CrossRef] [Green Version]
- Andreis, A.; Budano, C.; Levis, M.; Garrone, P.; Usmiani, T.; D’Ascenzo, F.; De Filippo, O.; D’Amico, M.; Bergamasco, L.; Biancone, L.; et al. Contrast-induced kidney injury: How does it affect long-term cardiac mortality? J. Cardiovasc. Med. 2017, 18, 908–915. [Google Scholar] [CrossRef] [PubMed]
- James, M.T.; Ghali, W.A.; Tonelli, M.; Faris, P.; Knudtson, M.L.; Pannu, N.; Klarenbach, S.W.; Manns, B.J.; Hemmelgarn, B.R. Acute kidney injury following coronary angiography is associated with a long-term decline in kidney function. Kidney Int. 2010, 78, 803–809. [Google Scholar] [CrossRef] [Green Version]
- Desanti De Oliveira, B.; Xu, K.; Shen, T.H.; Callahan, M.; Kiryluk, K.; D’Agati, V.D.; Tatonetti, N.P.; Barasch, J.; Devarajan, P. Molecular nephrology: Types of acute tubular injury. Nat. Rev. Nephrol. 2019, 15, 599–612. [Google Scholar] [CrossRef]
- Moledina, D.; Parikh, C.R. Phenotyping of Acute Kidney Injury: Beyond Serum Creatinine. Semin. Nephrol. 2018, 38, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Brooks, C.R.; Xiao, S.; Sabbisetti, V.; Yeung, M.Y.; Hsiao, L.-L.; Ichimura, T.; Kuchroo, V.; Bonventre, J.V. KIM-1–mediated phagocytosis reduces acute injury to the kidney. J. Clin. Investig. 2015, 125, 1620–1636. [Google Scholar] [CrossRef]
- Mori, K.; Lee, H.T.; Rapoport, D.; Drexler, I.R.; Foster, K.; Yang, J.; Schmidt-Ott, K.M.; Chen, X.; Li, J.Y.; Weiss, S.; et al. Endocytic delivery of lipocalin-siderophore-iron complex rescues the kidney from ischemia-reperfusion injury. J. Clin. Investig. 2005, 115, 610–621. [Google Scholar] [CrossRef] [PubMed]
- Koyner, J.L.; Parikh, C.R. Clinical utility of biomarkers of AKI in cardiac surgery and critical illness. Clin. J. Am. Soc. Nephrol. 2013, 8, 1034–1042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liao, B.; Nian, W.; Xi, A.; Zheng, M. Evaluation of a Diagnostic Test of Serum Neutrophil Gelatinase-Associated Lipocalin (NGAL) and Urine KIM-1 in Contrast-Induced Nephropathy (CIN). Experiment 2019, 25, 565–570. [Google Scholar] [CrossRef]
- Murray, P.T.; Mehta, R.L.; Shaw, A.; Ronco, C.; Endre, Z.H.; Kellum, J.A.; Chawla, L.S.; Cruz, D.N.; Ince, C.; Okusa, M.D. ADQI 10 workgroup Potential use of biomarkers in acute kidney injury: Report and summary of recommendations from the 10th Acute Dialysis Quality Initiative consensus conference. Kidney Int. 2014, 85, 513–521. [Google Scholar] [CrossRef] [Green Version]
- Endre, Z.H.; Kellum, J.A.; Di Somma, S.; Doi, K.; Goldstein, S.L.; Koyner, J.L.; Macedo, E.; Mehta, R.L.; Murray, P.T. Differential Diagnosis of AKI in Clinical Practice by Functional and Damage Biomarkers: Workgroup Statements from the Tenth Acute Dialysis Quality Initiative Consensus Conference. ADQI Consens. AKI Biomark. Cardiorenal Syndr. 2013, 182, 30–44. [Google Scholar] [CrossRef] [Green Version]
- Torregrosa, I.; Montoliu, C.; Urios, A.; Andrés-Costa, M.J.; Giménez-Garzó, C.; Juan, I.; Puchades, M.J.; Blasco, M.L.; Carratalá, A.; Sanjuán, R.; et al. Urinary KIM-1, NGAL and L-FABP for the diagnosis of AKI in patients with acute coronary syndrome or heart failure undergoing coronary angiography. Heart Vessel. 2014, 30, 703–711. [Google Scholar] [CrossRef]
- Vijayasimha, M.; Padma, V.; Mujumdar, S.K.; Satyanarayana, P.V.V.; Yadav, A. Kidney injury molecule-1: A urinary biomarker for contrast-induced acute kidney injury. Med. J. Dr. D.Y. Patil Univ. 2014, 7, 321. [Google Scholar] [CrossRef]
- Malyszko, J.; Bachorzewska-Gajewska, H.; Koc-Zorawska, E.; Malyszko, J.S.; Kobus, G.; Dobrzycki, S. Midkine: A Novel and Early Biomarker of Contrast-Induced Acute Kidney Injury in Patients Undergoing Percutaneous Coronary Interventions. BioMed Res. Int. 2015, 2015, 879509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gutiérrez-Escolano, A.; Santacruz-Vázquez, E.; Gómez-Pérez, F. Dysregulated microRNAs involved in contrast-induced acute kidney injury in rat and human. Ren. Fail. 2015, 37, 1498–1506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Briguori, C.; Visconti, G.; Rivera, N.V.; Focaccio, A.; Golia, B.; Giannone, R.; Castaldo, D.; De Micco, F.; Ricciardelli, B.; Colombo, A. Cystatin C and Contrast-Induced Acute Kidney Injury. Circulation 2010, 121, 2117–2122. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Zhang, L.; Yue, R.; You, G.; Zeng, R. Significance of Cystatin C for Early Diagnosis of Contrast-Induced Nephropathy in Patients Undergoing Coronary Angiography. Experiment 2016, 22, 2956–2961. [Google Scholar] [CrossRef] [Green Version]
- Bachorzewska-Gajewska, H.; Poniatowski, B.; Dobrzycki, S. NGAL (neutrophil gelatinase-associated lipocalin) and L-FABP after percutaneous coronary interventions due to unstable angina in patients with normal serum creatinine. Adv. Med. Sci. 2009, 54, 221–224. [Google Scholar] [CrossRef] [Green Version]
- Ling, W.; Zhaohui, N.; Ben, H.; Leyi, G.; Jianping, L.; Huili, D.; Jiaqi, Q. Urinary IL-18 and NGAL as Early Predictive Biomarkers in Contrast-Induced Nephropathy after Coronary Angiography. Nephron Clin. Prac. 2008, 108, c176–c181. [Google Scholar] [CrossRef]
- He, H.; Li, W.; Qian, W.; Zhao, X.; Wang, L.; Yu, Y.; Liu, J.; Cheng, J. Urinary interleukin-18 as an early indicator to predict contrast-induced nephropathy in patients undergoing percutaneous coronary intervention. Exp. Ther. Med. 2014, 8, 1263–1266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wybraniec, M.T.; Chudek, J.; Bożentowicz-Wikarek, M.; Mizia-Stec, K. Prediction of contrast-induced acute kidney injury by early post-procedural analysis of urinary biomarkers and intra-renal Doppler flow indices in patients undergoing coronary angiography. J. Interv. Cardiol. 2017, 30, 465–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gul, C.B.; Gullulu, M.; Oral, B.; Aydinlar, A.; Oz, O.; Budak, F.; Yilmaz, Y.; Yurtkuran, M. Urinary IL-18: A marker of contrast-induced nephropathy following percutaneous coronary intervention? Clin. Biochem. 2008, 41, 544–547. [Google Scholar]
- Padhy, M.; Kaushik, S.; Girish, M.; Mohapatra, S.; Shah, S.; Koner, B.C. Serum neutrophil gelatinase associated lipocalin (NGAL) and cystatin C as early predictors of contrast-induced acute kidney injury in patients undergoing percutaneous coronary intervention. Clin. Chim. Acta 2014, 435, 48–52. [Google Scholar] [CrossRef]
- Bachorzewska-Gajewska, H.; Malyszko, J.; Sitniewska, E.; Malyszko, J.S.; Pawlak, K.; Mysliwiec, M.; Lawnicki, S.; Szmitkowski, M.; Dobrzycki, S. Could Neutrophil-Gelatinase-Associated Lipocalin and Cystatin C Predict the Development of Contrast-Induced Nephropathy after Percutaneous Coronary Interventions in Patients with Stable Angina and Normal Serum Creatinine Values? Kidney Blood Press. Res. 2007, 30, 408–415. [Google Scholar] [CrossRef]
- Shaker, O.G.; El-Shehaby, A.; El-Khatib, M. Early Diagnostic Markers for Contrast Nephropathy in Patients Undergoing Coronary Angiography. Angiology 2010, 61, 731–736. [Google Scholar] [CrossRef]
- Haase, M.; Bellomo, R.; Devarajan, P.; Schlattmann, P.; Haase-Fielitz, A.; NGAL Meta-Analysis Investigator Group. Accuracy of Neutrophil Gelatinase-Associated Lipocalin (NGAL) in Diagnosis and Prognosis in Acute Kidney Injury: A Systematic Review and Meta-analysis. Am. J. Kidney Dis. 2009, 54, 1012–1024. [Google Scholar] [CrossRef] [Green Version]
- Tong, J.; Li, H.; Zhang, H.; Luo, Z.; Huang, Y.; Huang, J.; He, F.; Fu, J. Neutrophil Gelatinase-associated Lipocalin in the Prediction of Contrast-induced Nephropathy. J. Cardiovasc. Pharmacol. 2015, 66, 239–245. [Google Scholar] [CrossRef]
- Wang, K.; Duan, C.-Y.; Wu, J.; Liu, Y.; Bei, W.-J.; Chen, J.-Y.; He, P.C.; Liu, Y.-H.; Tan, N. Predictive Value of Neutrophil Gelatinase-Associated Lipocalin for Contrast-Induced Acute Kidney Injury After Cardiac Catheterization: A Meta-analysis. Can. J. Cardiol. 2015, 32, 1033.e19–1033.e29. [Google Scholar] [CrossRef] [PubMed]
- Paraboschi, I.; Mantica, G.; Dalton, N.R.; Turner, C.; Garriboli, M. Urinary biomarkers in pelvic-ureteric junction obstruction: A systematic review. Transl. Androl. Urol. 2020, 9, 722–742. [Google Scholar] [CrossRef] [PubMed]
- Ebru, A.; Kılıç, A.; Korkmaz, F.; Seker, R.; Sasmaz, H.; Demirtas, S.; Biyikli, Z. Is Cystatin-C superior to creatinine in the early diagnosis of contrast-induced nephropathy?: A potential new biomarker for an old complication. J. Postgrad. Med. 2014, 60, 135–140. [Google Scholar] [CrossRef]
- Haase, M.; Devarajan, P.; Haase-Fielitz, A.; Bellomo, R.; Cruz, D.N.; Wagener, G.; Krawczeski, C.D.; Koyner, J.L.; Murray, P.; Zappitelli, M.; et al. The Outcome of Neutrophil Gelatinase-Associated Lipocalin-Positive Subclinical Acute Kidney Injury: A Multicenter Pooled Analysis of Prospective Studies. J. Am. Coll. Cardiol. 2011, 57, 1752–1761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nash, K.; Hafeez, A.; Hou, S. Hospital-acquired renal insufficiency. Am. J. Kidney Dis. 2002, 39, 930–936. [Google Scholar] [CrossRef]
- Jorgensen, A.L. Contrast-Induced Nephropathy: Pathophysiology and Preventive Strategies. Crit. Care Nurse 2013, 33, 37–46. [Google Scholar] [CrossRef] [Green Version]
- Kelly, A.M.; Dwamena, B.; Cronin, P.; Bernstein, S.J.; Carlos, R.C. Meta-analysis: Effectiveness of Drugs for Preventing Contrast-Induced Nephropathy. Ann. Intern. Med. 2008, 148, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Solomon, R. Contrast-Induced Acute Kidney Injury: Is There a Risk after Intravenous Contrast? Clin. J. Am. Soc. Nephrol. 2008, 3, 1242–1243. [Google Scholar] [CrossRef] [Green Version]
- Dong, M.; Jiao, Z.; Liu, T.; Guo, F.; Li, G. Effect of administration route on the renal safety of contrast agents: A meta-analysis of randomized controlled trials. J. Nephrol. 2012, 25, 290–301. [Google Scholar] [CrossRef]
- Bitla, A.; Ashalatha, V.; Kumar, V.; Rajasekhar, D.; Suchitra, M.; Lakshmi, A.; Rao, P. Biomarker response to contrast administration in diabetic and nondiabetic patients following coronary angiography. Indian J. Nephrol. 2017, 27, 20–27. [Google Scholar] [CrossRef]
- Singer, E.; Markó, L.; Paragas, N.; Barasch, J.; Dragun, D.; Müller, D.N.; Budde, K.; Schmidt-Ott, K.M. Neutrophil gelatinase-associated lipocalin: Pathophysiology and clinical applications. Acta Physiol. 2013, 207, 663–672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mishra, J.; Ma, Q.; Prada, A.; Mitsnefes, M.; Zahedi, K.; Yang, J.; Barasch, J.; Devarajan, P. Identification of neutrophil gelatinase-associated lipocalin as a novel early urinary biomarker for ischemic renal injury. J. Am. Soc. Nephrol. 2003, 14, 2534–2543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mishra, J.; Ma, Q.; Kelly, C.; Mitsnefes, M.; Mori, K.; Barasch, J.; Devarajan, P. Kidney NGAL is a novel early marker of acute injury following transplantation. Pediatr. Nephrol. 2006, 21, 856–863. [Google Scholar] [CrossRef]
- Grigoryev, D.N.; Liu, M.; Hassoun, H.T.; Cheadle, C.; Barnes, K.C.; Rabb, H. The local and systemic inflammatory transcriptome after acute kidney injury. J. Am. Soc. Nephrol. 2008, 19, 547–558. [Google Scholar] [CrossRef] [Green Version]
- Tasanarong, A.; Hutayanon, P.; Piyayotai, D. Urinary Neutrophil Gelatinase-Associated Lipocalin predicts the severity of contrast-induced acute kidney injury in chronic kidney disease patients undergoing elective coronary procedures. BMC Nephrol. 2013, 14, 270. [Google Scholar] [CrossRef] [Green Version]
- Alharazy, S.M.; Kong, N.; Saidin, R.; Gafor, A.H.A.; Maskon, O.; Mohd, M.; Zakaria, S.Z.S. Neutrophil Gelatinase-Associated Lipocalin as an Early Marker of Contrast-Induced Nephropathy After Coronary Angiography. Angiology 2014, 65, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Akrawinthawong, K.; Ricci, J.; Cannon, L.; Dixon, S.; Kupfer, K.; Stivers, D.; Alexander, P.; David, S.; McCullough, P.A. Subclinical and clinical contrast-induced acute kidney injury: Data from a novel blood marker for determining the risk of developing contrastinduced nephropathy (ENCINO), a prospective study. Ren. Fail. 2015, 37, 187–191. [Google Scholar] [CrossRef] [Green Version]
- Malyszko, J.; Bachorzewska-Gajewska, H.; Malyszko, J.; Iaina-Levin, N.; Kobus, G.; Dobrzycki, S. Markers of kidney function in the elderly in relation to the new CKD-EPI formula for estimation of glomerular filtration rate. Arch. Med. Sci. 2011, 7, 658–664. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Yu, Z.; Gan, L.; Peng, L.; Zhou, Q. Serum NGAL and FGF23 may have certain value in early diagnosis of CIN. Ren. Fail. 2018, 40, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.L.; Wang, Z.J.; Yang, Q.; Yu, M.; Shen, H.; Nie, B.; Han, H.Y.; GAd, F.; Zhou, Y.J. Plasma neutrophil-gelatinase-associated lipocalin and cystatin C could early diagnose contrast-induced acute kidney injury in patients with renal insufficiency undergoing an elective percutaneous coronary intervention. Chin. Med. J. 2012, 125, 1051–1056. [Google Scholar] [PubMed]
- Liebetrau, C.; Gaede, L.; Doerr, O.; Blumenstein, J.; Rixe, J.; Teichert, O.; Willmer, M.; Weber, M.; Rolf, A.; Moellmann, H.; et al. Neutrophil gelatinase-associated lipocalin (NGAL) for the early detection of contrast-induced nephropathy after percutaneous coronary intervention. Scand. J. Clin. Lab. Investig. 2014, 74, 81–88. [Google Scholar] [CrossRef]
- Kafkas, N.; Liakos, C.; Zoubouloglou, F.; Dagadaki, O.; Dragasis, S.; Makris, K. Neutrophil Gelatinase–Associated Lipocalin as an Early Marker of Contrast-Induced Nephropathy After Elective Invasive Cardiac Procedures. Clin. Cardiol. 2016, 39, 464–470. [Google Scholar] [CrossRef]
- Ronco, C.; Stacul, F.; McCullough, P.A. Subclinical acute kidney injury (AKI) due to iodine-based contrast media. Eur. Radiol. 2013, 23, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Spasojević-Dimitrijeva, B.; Kotur-Stevuljević, J.; Đukić, M.; Paripović, D.; Miloševski-Lomić, G.; Spasojević-Kalimanovska, V.; Pavićević, P.; Mitrović, J.; Kostić, M. Serum Neutrophil Gelatinase-Associated Lipocalin and Urinary Kidney Injury Molecule-1 as Potential Biomarkers of Subclinical Nephrotoxicity After Gadolinium-Based and Iodinated-Based Contrast Media Exposure in Pediatric Patients with Normal Kidney Function. Med. Sci. Monit. 2017, 23, 4299–4305. [Google Scholar] [CrossRef] [Green Version]
- Seibert, F.S.; Heringhaus, A.; Pagonas, N.; Rudolf, H.; Rohn, B.; Bauer, F.; Timmesfeld, N.; Trappe, H.J.; Babel, N.; Westhoff, T.H. Biomarkers in the prediction of contrast media induced nephropathy—The BITCOIN study. PLoS ONE 2020, 15, e0234921. [Google Scholar] [CrossRef]
- Breglia, A.; Godi, I.; Virzì, G.M.; Guglielmetti, G.; Iannucci, G.; De Cal, M.; Brocca, A.; Carta, M.; Giavarina, D.; Ankawi, G.; et al. Subclinical Contrast-Induced Acute Kidney Injury in Patients Undergoing Cerebral Computed Tomography. Cardiorenal Med. 2020, 10, 125–136. [Google Scholar] [CrossRef]
- Rozenfeld, K.L.; Zahler, D.; Shtark, M.; Goldiner, I.; Keren, G.; Banai, S.; Shacham, Y. Elevated Neutrophil Gelatinase-Associated Lipocalin for the Assessment of Structural versus Functional Renal Damage among ST-Segment Elevation Myocardial Infarction Patients. Blood Purif. 2020, 49, 560–566. [Google Scholar] [CrossRef] [PubMed]
- Lupu, L.; Abukatash, H.; Banai, A.; Rozenfeld, K.-L.; Lewit, D.; Merdler, I.; Loewenstein, I.; Bornstein, G.; Banai, S.; Shacham, Y. Relation of Baseline Neutrophil Gelatinase-Associated Lipocalin (NGAL) Levels and Contrast-Induced Nephropathy following Percutaneous Coronary Intervention among Chronic Kidney Disease Patients. J. Clin. Med. 2021, 10, 5403. [Google Scholar] [CrossRef]
- Petrova, I.; Bogov, I.; Alexandrov, A.; Vladimirov, G.; Avramov, D.; Mateev, H.; Paskaleva, I.; Georgiev, B.; Gotcheva, N. Neutrophil Gelatinase-Associated Lipocalin (NGAL) predict higher risk of serious renal dysfunction in patients with CI-AKI. Eur. Heart J. 2020, 41 (Suppl. S2), 2556. [Google Scholar] [CrossRef]
- Di Somma, S.; Magrini, L.; De Berardinis, B.; Marino, R.; Ferri, E.; Moscatelli, P.; Ballarino, P.; Carpinteri, G.; Noto, P.; Gliozzo, B.; et al. Additive value of blood neutrophil gelatinase-associated lipocalin to clinical judgement in acute kidney injury diagnosis and mortality prediction in patients hospitalized from the emergency department. Crit. Care 2013, 17, R29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nickolas, T.L.; Schmidt-Ott, K.M.; Canetta, P.; Forster, C.; Singer, E.; Sise, M.; Elger, A.; Maarouf, O.; Sola-Del Valle, D.A.; O’Rourke, M.; et al. Diagnostic and prognostic stratification in the Emergency Department using urinary biomarkers of nephron damage: A multicenter prospective cohort study. J. Am. Coll. Cardiol. 2012, 59, 246–255. [Google Scholar] [CrossRef] [Green Version]
- Byeon, J.; Choi, I.J.; Lee, D.; Ahn, Y.; Kim, M.-J.; Jeon, D.S. Predictive and Prognostic Value of Serum Neutrophil Gelatinase-Associated Lipocalin for Contrast-Induced Acute Kidney Injury and Long-Term Clinical Outcomes after Percutaneous Coronary Intervention. J. Clin. Med. 2022, 11, 5971. [Google Scholar] [CrossRef]
- Scridon, A.; Somkereki, C.; Nicoară, T.R.; Oprica, M.; Demian, L. Neutrophil gelatinase-associated lipocalin monitoring reveals persistent subclinical kidney injury following intraarterial administration of iodinated contrast agents. Sci. Rep. 2022, 12, 19464. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Control Group (n = 18) | CI-AKI Group (n = 12) | Group of Subclinical CI-AKI (n = 15) | p |
|---|---|---|---|---|
| Age (mean ± SD) | 61.72 ± 7.71 | 62.9 ± 11.43 | 60.53 ± 6.73 | 0.012 |
| Male gender (%) | 44.4 | 83.3 | 46.7 | 0.366 |
| Arterial hypertension (%) | 100 | 100 | 100 | 1.000 |
| Diabetus mellitus Type 2 (%) | 88.9 | 100 | 86.7 | 0.837 |
| Stable angina (%) | 77.8 | 91.7 | 93.3 | 0.730 |
| History of myocardial infarction (%) | 50 | 25 | 33.3 | 0.740 |
| Previous PCI (%) | 33.3 | 25 | 40 | 0.504 |
| Previous aortocoronary bypass surgery (%) | 11.1 | 41.7 * | 0 | 0.020 |
| Baseline serum creatinine (μmol/L) [Me(IQR)] | 73.6 (67–95) | 93.5 (88.3–105.9) | 77.0 (74–92) | <0.05 |
| Baseline GFR (mL/min/1.73 m2) [Me(IQR)] | 79.8 (72.4–87.3) | 69.0 (66.0–78.2) | 77.1 (68.8–94.3) | <0.05 |
| LV ejection fraction (%) | 55.32 ± 8.87 | 55.17 ± 8.33 | 53.53 ± 9.73 | 0.640 |
| Coronary artery disease (CAD) type | ||||
| One-vessel disease (%) | 27.8 | 16.7 | 6.7 | 0.133 |
| Two vessel disease (%) | 11.1 | 25 | 33.3 | |
| Multivessel disease (%) | 22.2 | 50 | 26.7 | |
| Diagnostic coronary angiography and one-stage PCI (%) | 44.4 | 66.7 | 46.7 | 0.695 |
| Volume of contrast medium (mL) | 143.0 ± 104.7 | 204.08 ± 165.00 | 164.53 ± 120.44 | 0.432 |
| Drug antidiabetic therapy (%) | 61.1 | 83.3 | 46.7 | 0.142 |
| Metformin intake (%) | 38.9 | 58.3 | 40 | 0.142 |
| Concomitant therapy with ACE inhibitor (%) | 61.1 | 41.7 | 46.7 | 0.546 |
| Control Group (n = 18) | CI-AKI Group (n = 12) | Subclinical CI-AKI Group (n = 15) | Control Group vs. CI-AKI | Control Group vs. Subclinical CI-AKI | CI-AKI vs. Subclinical CI-AKI | |
|---|---|---|---|---|---|---|
| Serum creatinine (μmol/L) | Median (IQR) | Median (IQR) | Median (IQR) | p values | p values | p values |
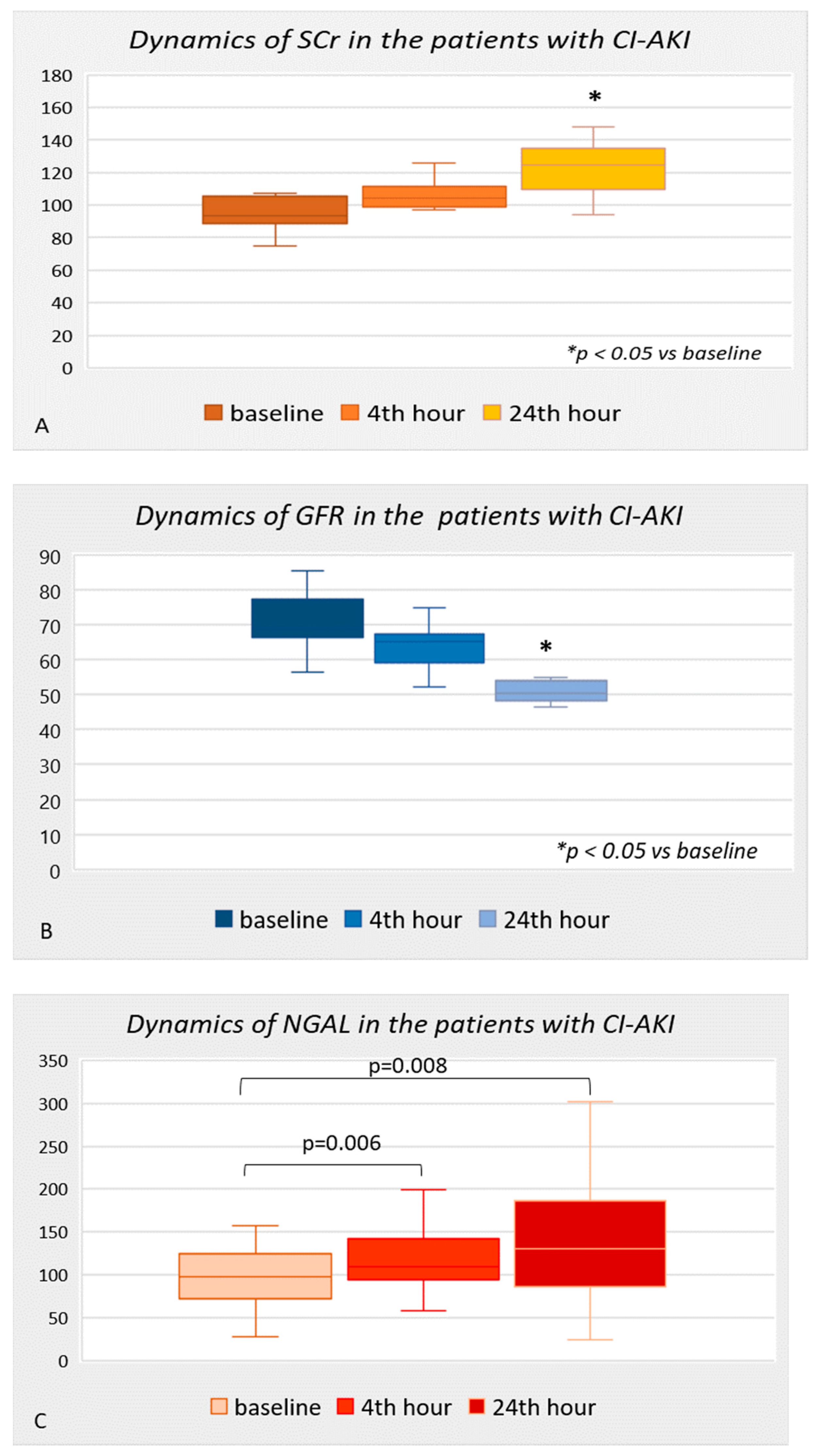
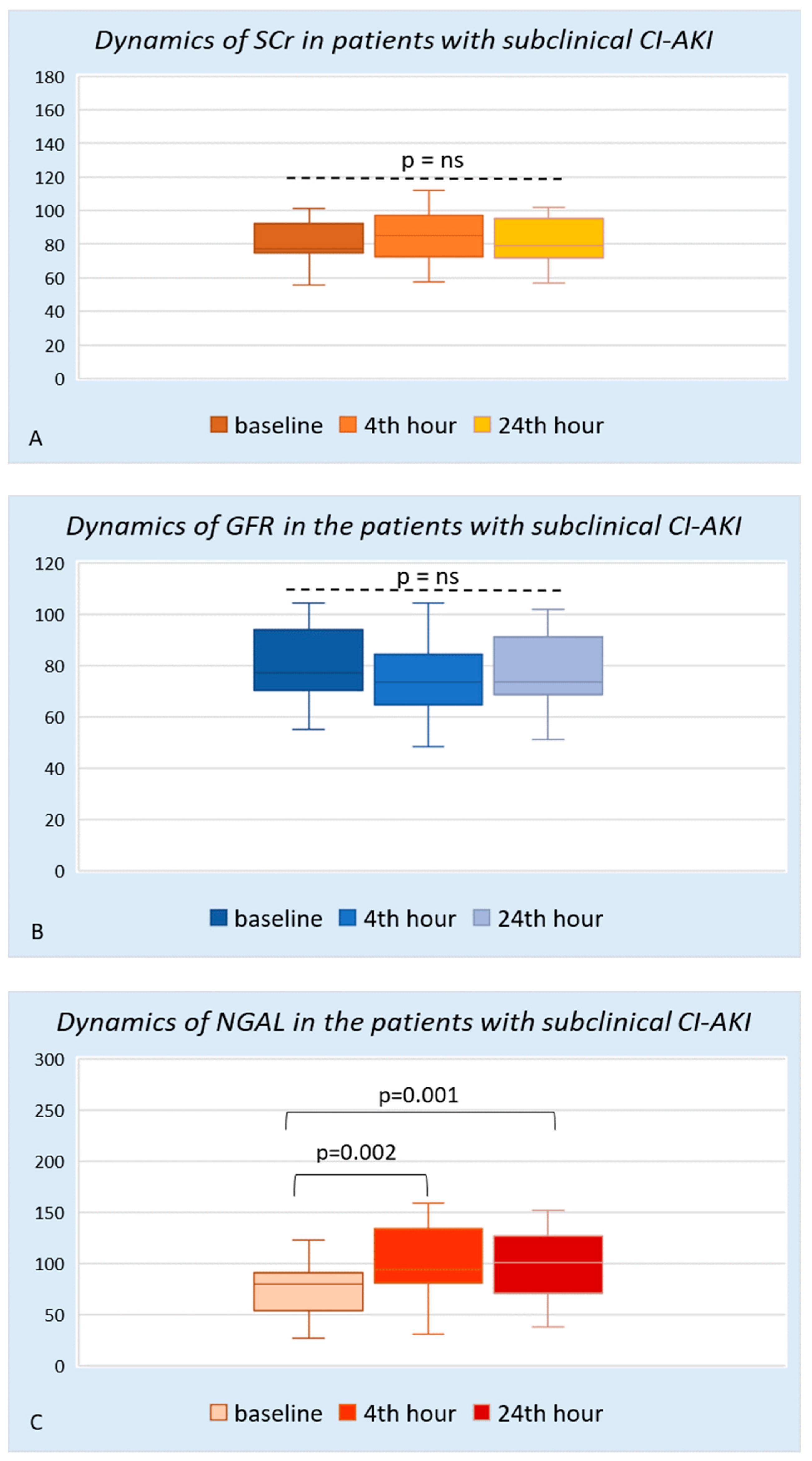
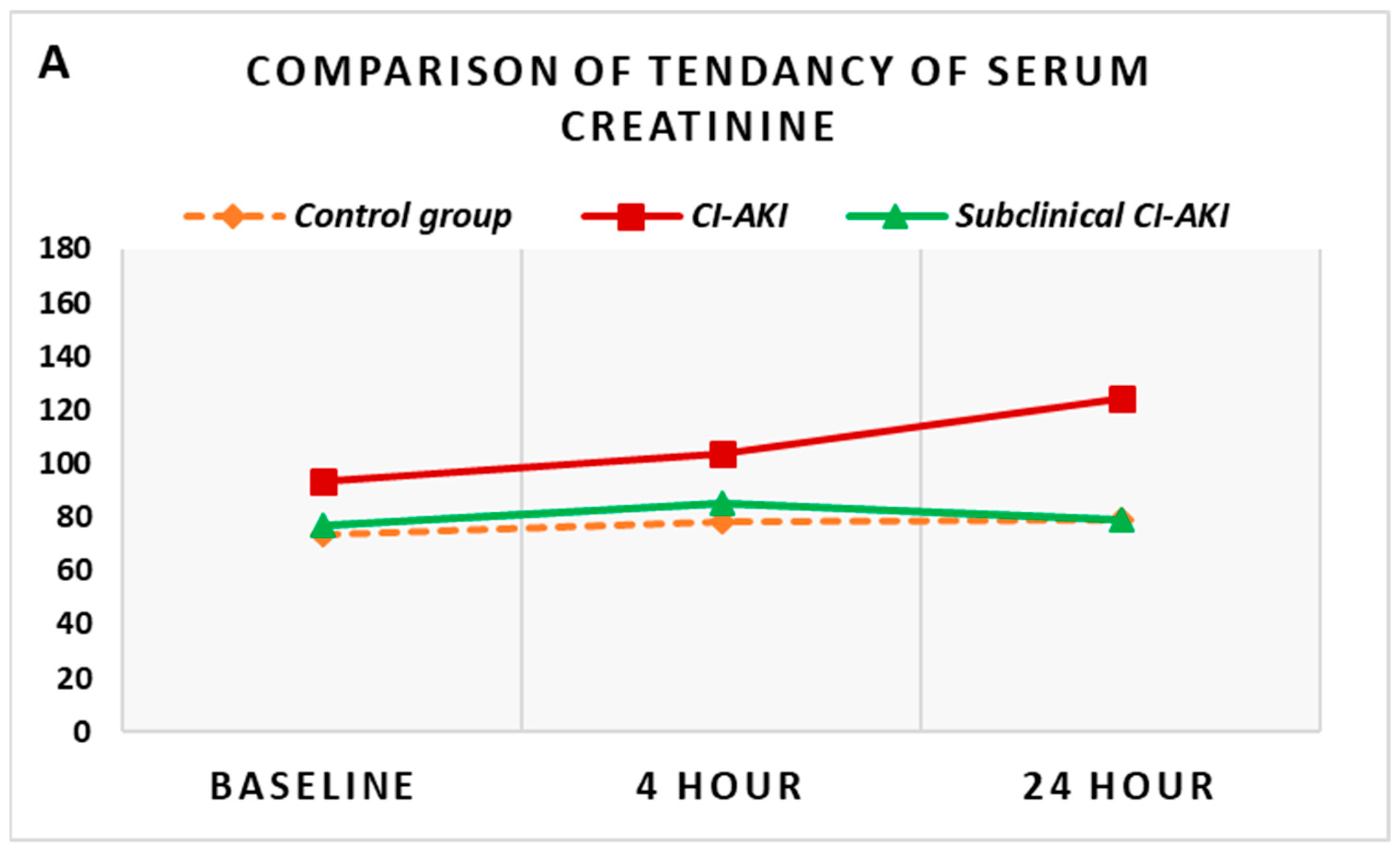
| Baseline | 73.6 (67–95) | 93.5 (88.3–105.9) | 77.0 (74–92) | 0.005 | 0.625 | 0.014 |
| 4th hour | 78.2 (71.5–90.4) | 104.0 (98.7–112.5) | 85.0 (72–100) | <0.001 | 0.458 | 0.004 |
| 24th hour | 79.0 (70.8–92.5) | 124.5 (108.5–136.3) * | 79.0 (71–96) | <0.001 | 0.928 | <0.001 |
| 48th hour | 77.5 (66.7–91) | 106.0 (91.8–119.5) * | 76.5 (69.5–89.5) | 0.002 | 0.884 | 0.005 |
| GFR (mL/min/1.73 m2) | ||||||
| Baseline | 79.8 (72.4–87.3) | 69.0 (66.0–78.2) | 77.1 (68.8–94.3) | 0.020 | 0.971 | 0.130 |
| 4th hour | 76.0 (70.5–85.2) | 65.1 (57.7–68.2) | 73.4 (62.5–87.3) | <0.001 | 0.563 | 0.025 |
| 24th hour | 77.8 (69.1–90.8) | 50.5 (47.7–54.5) * | 73.4 (68–91.9) | <0.001 | 0.914 | <0.001 |
| 48th hour | 77.9 (70.3–94.5) | 62.5 (54.1–71.6) * | 77.9 (63.1–96.2) | 0.010 | 0.861 | 0.016 |
| NGAL (ng/mL) | ||||||
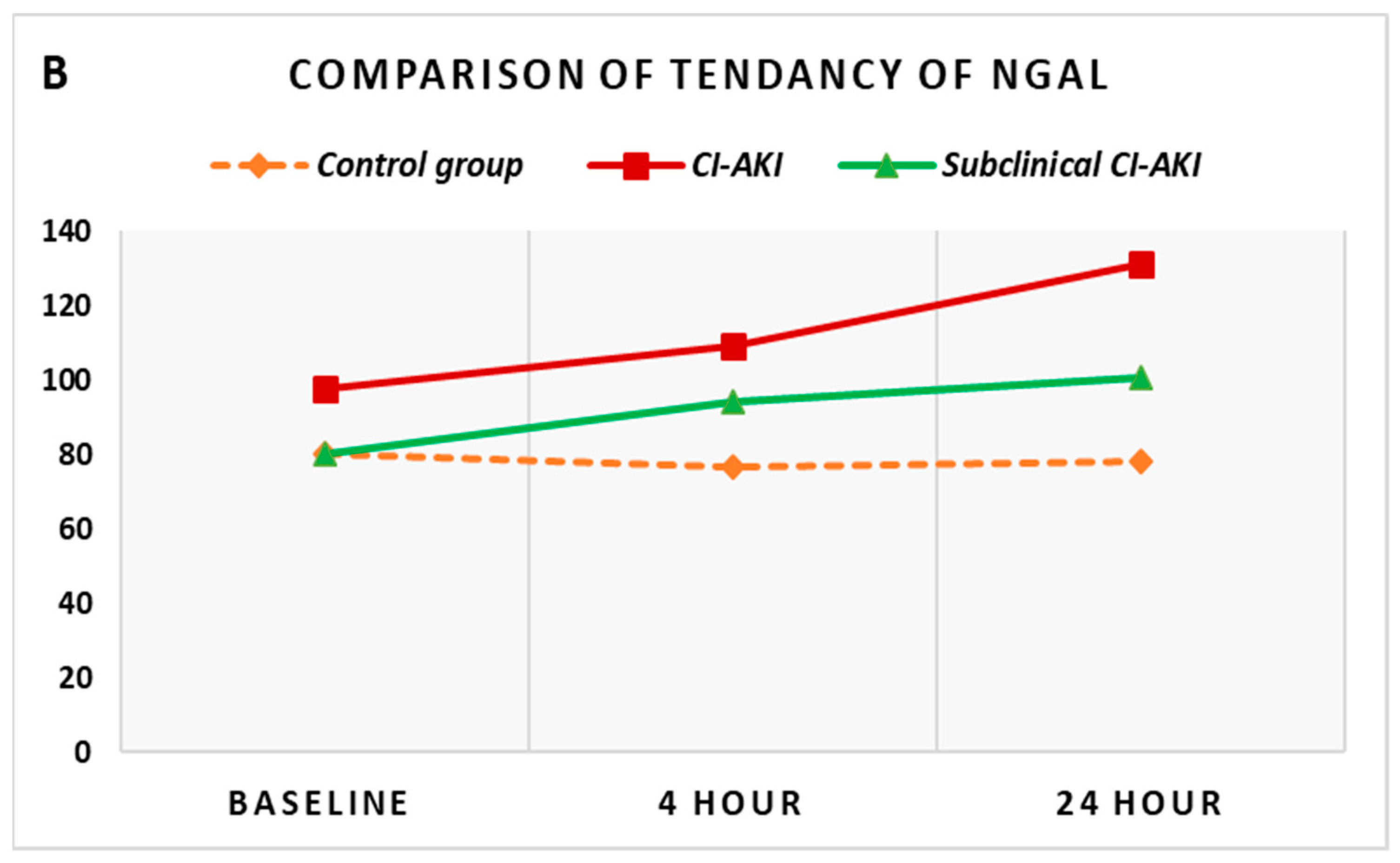
| Baseline | 80.3 (66.9–86.2) | 97.6 (69.4–127.0) | 80.0 (44.4–94.1) | 0.072 | 0.899 | 0.088 |
| 4th hour | 76.6 (65.3–87.6) | 109.3 (92.1–148.7) * | 94.0 (75.5–148.2) * | 0.001 | 0.024 | 0.354 |
| 24th hour | 78.0 (66.4–88.5) | 131.0 (81.1–240.8) * | 100.7 (55–132.2) * | 0.005 | 0.086 | 0.164 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petrova, I.; Alexandrov, A.; Vladimirov, G.; Mateev, H.; Bogov, I.; Paskaleva, I.; Gotcheva, N. NGAL as Biomarker of Clinical and Subclinical Damage of Kidney Function after Coronary Angiography. Diagnostics 2023, 13, 1180. https://doi.org/10.3390/diagnostics13061180
Petrova I, Alexandrov A, Vladimirov G, Mateev H, Bogov I, Paskaleva I, Gotcheva N. NGAL as Biomarker of Clinical and Subclinical Damage of Kidney Function after Coronary Angiography. Diagnostics. 2023; 13(6):1180. https://doi.org/10.3390/diagnostics13061180
Chicago/Turabian StylePetrova, Iliyana, Alexander Alexandrov, Georgi Vladimirov, Hristo Mateev, Ivaylo Bogov, Iva Paskaleva, and Nina Gotcheva. 2023. "NGAL as Biomarker of Clinical and Subclinical Damage of Kidney Function after Coronary Angiography" Diagnostics 13, no. 6: 1180. https://doi.org/10.3390/diagnostics13061180