
Hyaline Vascular Type of Unicentric Castleman Disease in a Kidney with End-Stage Renal Disease: A Case Report of a Rare Entity at an Unusual Location and a Special Clinical Setting

Abstract
:1. Introduction
2. Case Description
3. Discussion

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case No. | Age/Sex | Symptom | Comorbidities | Side | Size | Imaging | Type | Treatment | Follow-Up | Reference |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 56/M | None Detected in a health checkup | HTN and diabetes | Right upper-middle | 4 × 3.5 cm | CT: Iso-density lesion | HV | Partial nephrectomy | Free of disease 6 months after surgery | [5] |
| 2 | 61/M | None Detected in a health checkup | None | Right upper | 2 × 1.8 cm | MRI: Lesion detected CT: Enhancement at the early phase and washed out at the late phase, suspecting RCC | HV | Laparoscopic partial nephrectomy | NA | [28] |
| 3 | 59/F | None Incidentally found | Pneumonia | Left posterior midportion | 1.5 cm | CT and MRI: Enhancing mass, suspecting RCC | HV | Open partial nephrectomy | NA | [27] |
| 4 | NA/F | Low-grade fever, sweating, malaise and polyarthralgia | NA | Right | NA | Renal mass | HV | Nephrectomy | Free of disease 12 months after surgery | [26] |
| 5 | 69/F | NA | None | Right inferior pole | 2.0 cm | CT: Renal mass, suspecting RCC, leiomyoma or angiomyolipoma | HV | NA | NA | [7] |
| 6 | 38/M | None Incidentally found | Renal stones and degenerative disk disease | Left anterior mid-region | 1.8 cm | CT: Enhancing renal mass | HV | Open partial nephrectomy | Free of disease 10 months after surgery | [6] |
| 7 | 70/M | None Incidentally found | Chronic diverticulitis | Left | 2.0 cm | CT: Enhancement at the early phase and washed out at the late phase, suspecting RCC and other malignant tumors MRI: Iso-intensity in the T1-weighted image and low-intensity in the T2-weighted image | HV | Partial nephrectomy | Free of disease 8 months after surgery | [29] |
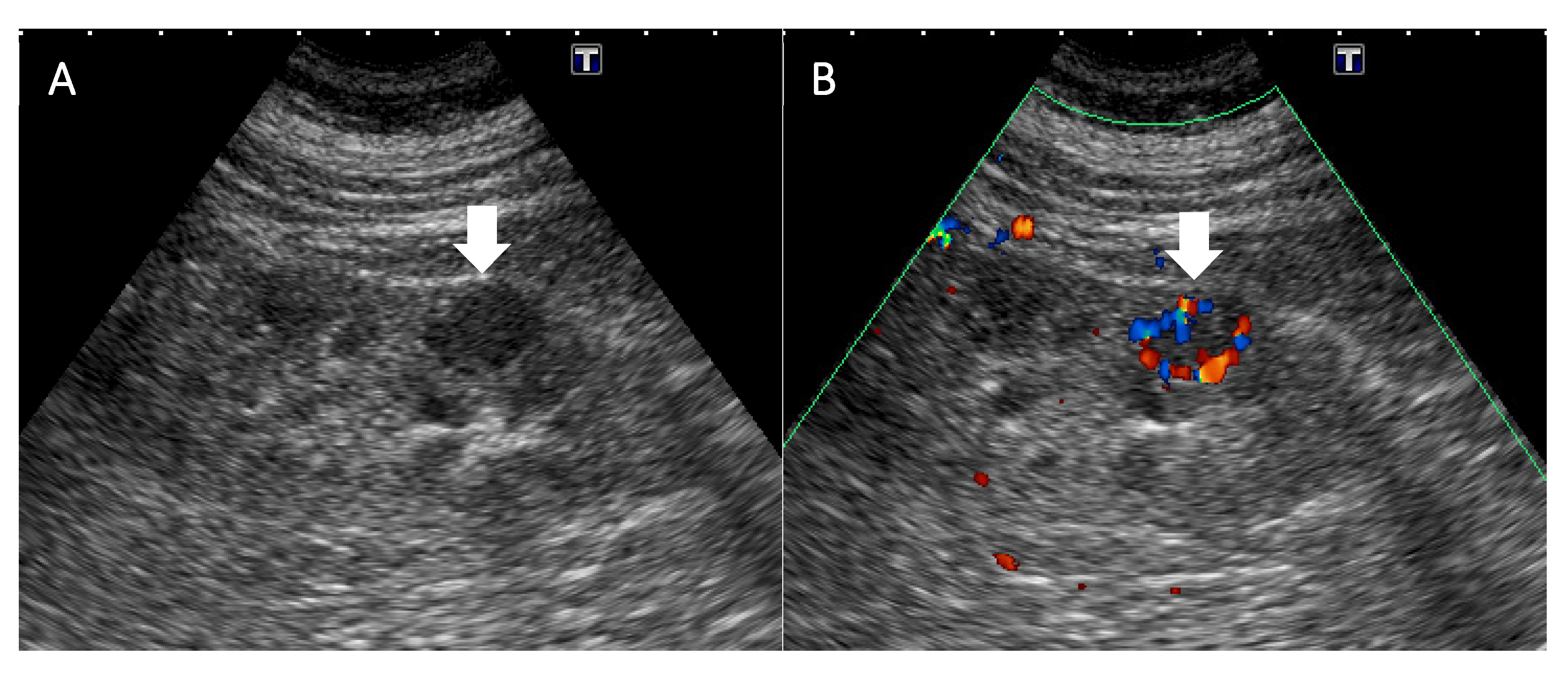
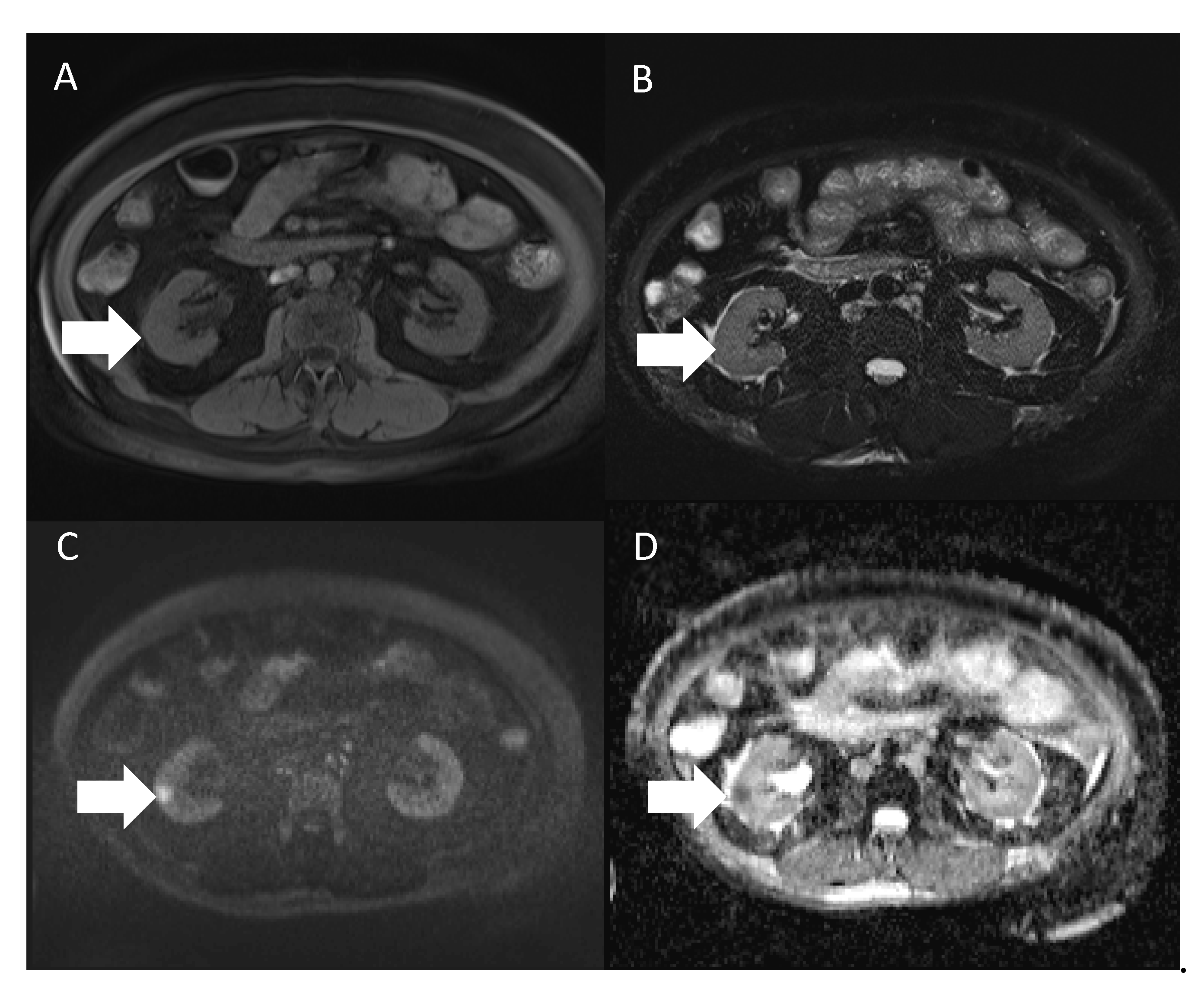
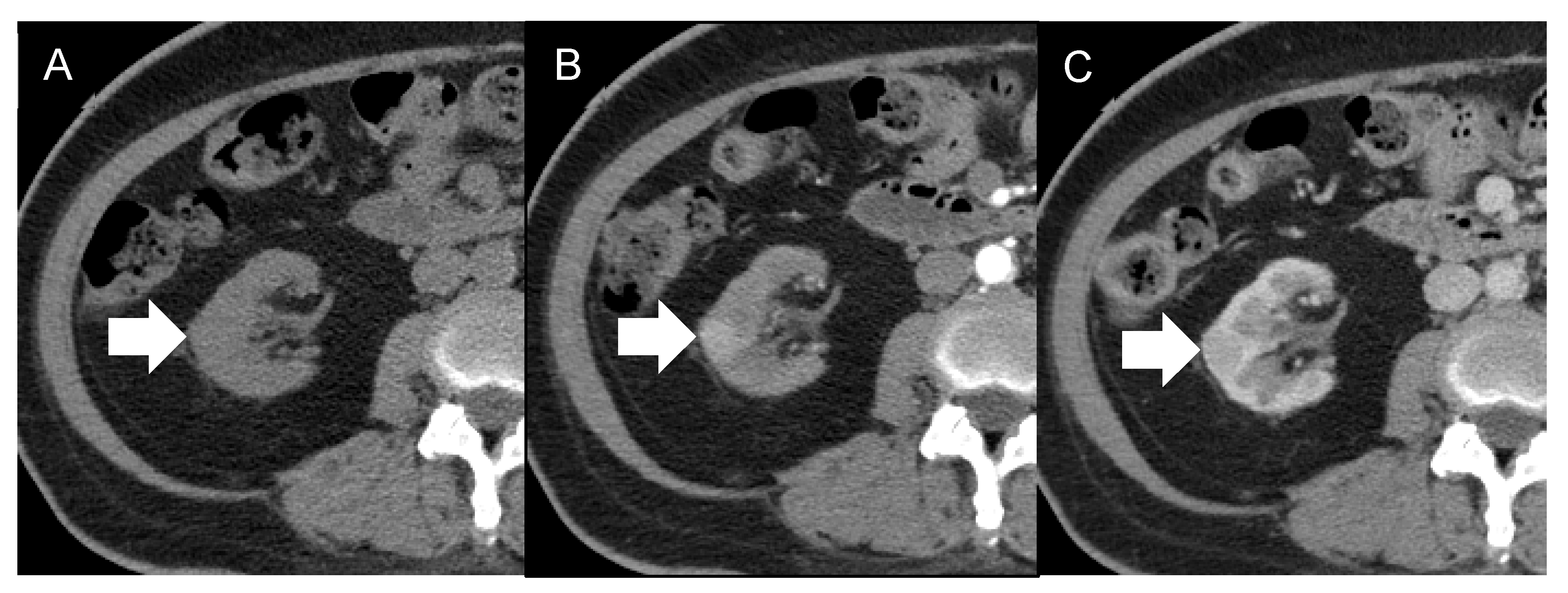
| 8 | 56/F | None Incidentally found | ESRD, HTN, diabetes, hyperlipidemia | Right lateroposterior cortex of the lower pole | 1.3 cm | US: Lesion detected MRI: Iso-intensity in the T1- and T2-weighted images and low ADC value CT: Early enhancement, suspecting RCC | HV | Laparoscopic nephroureterectomy | Free of disease 17 months after surgery | Our case |
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Carbone, A.; Borok, M.; Damania, B.; Gloghini, A.; Polizzotto, M.N.; Jayanthan, R.K.; Fajgenbaum, D.C.; Bower, M. Castleman disease. Nat. Rev. Dis. Primers 2021, 7, 84. [Google Scholar] [CrossRef] [PubMed]
- Van Rhee, F.; Stone, K.; Szmania, S.; Barlogie, B.; Singh, Z. Castleman disease in the 21st century: An update on diagnosis, assessment, and therapy. Clin. Adv. Hematol. Oncol. 2010, 8, 486–498. [Google Scholar] [PubMed]
- Van Rhee, F.; Oksenhendler, E.; Srkalovic, G.; Voorhees, P.; Lim, M.; Dispenzieri, A.; Ide, M.; Parente, S.; Schey, S.; Streetly, M.; et al. International evidence-based consensus diagnostic and treatment guidelines for unicentric Castleman disease. Blood Adv. 2020, 4, 6039–6050. [Google Scholar] [CrossRef] [PubMed]
- Dispenzieri, A.; Fajgenbaum, D.C. Overview of Castleman disease. Blood 2020, 135, 1353–1364. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhao, H.; Su, B.; Yang, C.; Li, S.; Fu, W. Primary hyaline vascular Castleman disease of the kidney: Case report and literature review. Diagn. Pathol. 2019, 14, 94. [Google Scholar] [CrossRef] [Green Version]
- Mah, N.A.; Peretsman, S.J.; Teigland, C.M.; Banks, P.M. Castleman disease of the hyaline-vascular type confined to the kidney. Am. J. Clin. Pathol. 2007, 127, 465–468. [Google Scholar] [CrossRef]
- Nishimura, M.F.; Nishimura, Y.; Nishikori, A.; Maekawa, Y.; Maehama, K.; Yoshino, T.; Sato, Y. Clinical and Pathological Characteristics of Hyaline-Vascular Type Unicentric Castleman Disease: A 20-Year Retrospective Analysis. Diagnostics 2021, 11, 2008. [Google Scholar] [CrossRef]
- El-Zaatari, Z.M.; Truong, L.D. Renal Cell Carcinoma in End-Stage Renal Disease: A Review and Update. Biomedicines 2022, 10, 657. [Google Scholar] [CrossRef]
- Tsuzuki, T.; Iwata, H.; Murase, Y.; Takahara, T.; Ohashi, A. Renal tumors in end-stage renal disease: A comprehensive review. Int. J. Urol. 2018, 25, 780–786. [Google Scholar] [CrossRef] [Green Version]
- Castleman, B.; Towne, V.W. Case records of the Massachusetts General Hospital: Case No. 40231. N. Engl. J. Med. 1954, 250, 1001–1005. [Google Scholar] [CrossRef]
- Zhou, T.; Wang, H.W.; Pittaluga, S.; Jaffe, E.S. Multicentric Castleman disease and the evolution of the concept. Pathologica 2021, 113, 339–353. [Google Scholar] [CrossRef]
- Cronin, D.M.; Warnke, R.A. Castleman disease: An update on classification and the spectrum of associated lesions. Adv. Anat. Pathol. 2009, 16, 236–246. [Google Scholar] [CrossRef]
- Keller, A.R.; Hochholzer, L.; Castleman, B. Hyaline-vascular and plasma-cell types of giant lymph node hyperplasia of the mediastinum and other locations. Cancer 1972, 29, 670–683. [Google Scholar] [CrossRef]
- Yu, L.; Tu, M.; Cortes, J.; Xu-Monette, Z.Y.; Miranda, R.N.; Zhang, J.; Orlowski, R.Z.; Neelapu, S.; Boddu, P.C.; Akosile, M.A.; et al. Clinical and pathological characteristics of HIV- and HHV-8-negative Castleman disease. Blood 2017, 129, 1658–1668. [Google Scholar] [CrossRef] [Green Version]
- Talat, N.; Belgaumkar, A.P.; Schulte, K.M. Surgery in Castleman’s disease: A systematic review of 404 published cases. Ann. Surg. 2012, 255, 677–684. [Google Scholar] [CrossRef] [PubMed]
- Goel, R.; Raut, A.; Agarwal, A.; Raghav, S.; Kumar, S.; Chaudhary, S.; Golhait, P.; Kumar, S.; Saran, R. A Rare Presentation of Orbital Castleman’s Disease. Case Rep. Ophthalmol. Med. 2020, 2020, 1012759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, D.; Lee, J.; Lee, H.; Baek, S. Unicentric Castleman’s disease in the orbit: A case report. Indian J. Ophthalmol. 2015, 63, 555–557. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Liu, H.; Li, H.; Li, A.; Yu, G.; Yin, W. Hyaline vascular variant of unicentric Castleman disease of the tonsil: A case report. Diagn. Pathol. 2019, 14, 70. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Chen, G.; Qiu, X.; Xu, S.; Wu, Y.; Liu, R.; Zhou, Q.; Chen, J. Intrapulmonary unicentric Castleman disease mimicking peripheral pulmonary malignancy. Thorac. Cancer 2014, 5, 576–580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lv, K.; Zhang, C.L.; Xu, M.S. Primary Castleman’s disease.e in the liver: A case report and literature review. Mol. Clin. Oncol. 2018, 8, 575–578. [Google Scholar] [CrossRef]
- Maruyama, S.; Hao, N.; Cheng, J.; Horino, K.; Ohnishi, M.; Fukushi, M.; Fujii, M.; Saku, T. Castleman’s disease of the buccal mucosa: Report of a case and review of the literature of head and neck cases. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2002, 93, 305–310. [Google Scholar] [CrossRef] [PubMed]
- McDonnell, O.; Morris, M.; Khaleel, Z. Isolated nasopharyngeal castleman disease: An uncommon diagnosis in an unusual location. Case Rep. Radiol. 2014, 2014, 475690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rawashdeh, B.; Meyer, M.; Yimin, D.; Anthony, C.; Nguyn, D.; Moslemi, M.; Golestani, S.; Richard, S.; Kim, S. Unicentric Castleman’s disease presenting as a pulmonary mass: A diagnostic dilemma. Am. J. Case Rep. 2015, 16, 259–261. [Google Scholar] [CrossRef] [Green Version]
- Tsai, M.H.; Pai, H.H.; Yen, P.T.; Huang, T.S. Unusual localization of Castleman’s disease: Report of the first case in the nasopharynx. Ear Nose Throat J. 1997, 76, 731–735, 739. [Google Scholar] [CrossRef]
- Akram, W.; Degliuomini, J.; Wallack, M.K.; Huang, S.; Okechukwu, E.; Eric, T. Unicentric Castleman’s Disease Masquerading as a Carcinoid Tumor of the Small Intestine. Am. Surg. 2016, 82, e287–e289. [Google Scholar] [CrossRef]
- De Feudis, L.; Carota, G.; Sargiacomo, R.; Traisci, G. Castleman’s disease with isolated renal location: Clinical case. Ann. Ital. Med. Int. 1998, 13, 117–120. [Google Scholar] [PubMed]
- Kaneko, T.; Ogushi, T.; Asakage, Y.; Kitamura, T. Hyaline vascular type of Castleman’s disease confined to the kidney. Nihon Hinyokika Gakkai Zasshi 2008, 99, 597–600. [Google Scholar] [CrossRef] [Green Version]
- Koh, Y.; Kinjo, T.; Nonomura, D.; Yamamoto, Y.; Yoneda, S.; Nomura, H.; Tei, N.; Takada, S.; Matsumiya, K.; Jokoji, R.; et al. Castleman’s disease of the kidney: A case report. Hinyokika Kiyo 2014, 60, 129–132. [Google Scholar]
- Hatano, K.; Fujita, S.; Tsujimoto, Y.; Takada, T.; Honda, M.; Tsujimoto, M.; Matsumiya, K.; Fujioka, H. Rare case of the hyaline vascular type of Castleman’s disease of the kidney. Int. J. Urol. 2007, 14, 1098–1100. [Google Scholar] [CrossRef]
- Sun, X.; Chang, K.C.; Abruzzo, L.V.; Lai, R.; Younes, A.; Jones, D. Epidermal growth factor receptor expression in follicular dendritic cells: A shared feature of follicular dendritic cell sarcoma and Castleman’s disease. Hum. Pathol. 2003, 34, 835–840. [Google Scholar] [CrossRef]
- Vermi, W.; Lonardi, S.; Bosisio, D.; Uguccioni, M.; Danelon, G.; Pileri, S.; Fletcher, C.; Sozzani, S.; Zorzi, F.; Arrigoni, G.; et al. Identification of CXCL13 as a new marker for follicular dendritic cell sarcoma. J. Pathol. 2008, 216, 356–364. [Google Scholar] [CrossRef] [PubMed]
- Cokelaere, K.; Debiec-Rychter, M.; De Wolf-Peeters, C.; Hagemeijer, A.; Sciot, R. Hyaline vascular Castleman’s disease with HMGIC rearrangement in follicular dendritic cells: Molecular evidence of mesenchymal tumorigenesis. Am. J. Surg. Pathol. 2002, 26, 662–669. [Google Scholar] [CrossRef] [PubMed]
- Cobo, G.; Lindholm, B.; Stenvinkel, P. Chronic inflammation in end-stage renal disease and dialysis. Nephrol. Dial. Transplant. 2018, 33, iii35–iii40. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.-H.; Li, H.-N. Hyaline Vascular Type of Unicentric Castleman Disease in a Kidney with End-Stage Renal Disease: A Case Report of a Rare Entity at an Unusual Location and a Special Clinical Setting. Diagnostics 2022, 12, 2878. https://doi.org/10.3390/diagnostics12112878
Chen C-H, Li H-N. Hyaline Vascular Type of Unicentric Castleman Disease in a Kidney with End-Stage Renal Disease: A Case Report of a Rare Entity at an Unusual Location and a Special Clinical Setting. Diagnostics. 2022; 12(11):2878. https://doi.org/10.3390/diagnostics12112878
Chicago/Turabian StyleChen, Chuan-Han, and Hsin-Ni Li. 2022. "Hyaline Vascular Type of Unicentric Castleman Disease in a Kidney with End-Stage Renal Disease: A Case Report of a Rare Entity at an Unusual Location and a Special Clinical Setting" Diagnostics 12, no. 11: 2878. https://doi.org/10.3390/diagnostics12112878