
PD-L1 Expression Is an Independent Marker for Lymph Node Metastasis in Middle Eastern Endometrial Cancer

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Selection
2.2. Tissue Microarray Construction and Immunohistochemistry
2.3. POLE Mutation Analysis
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
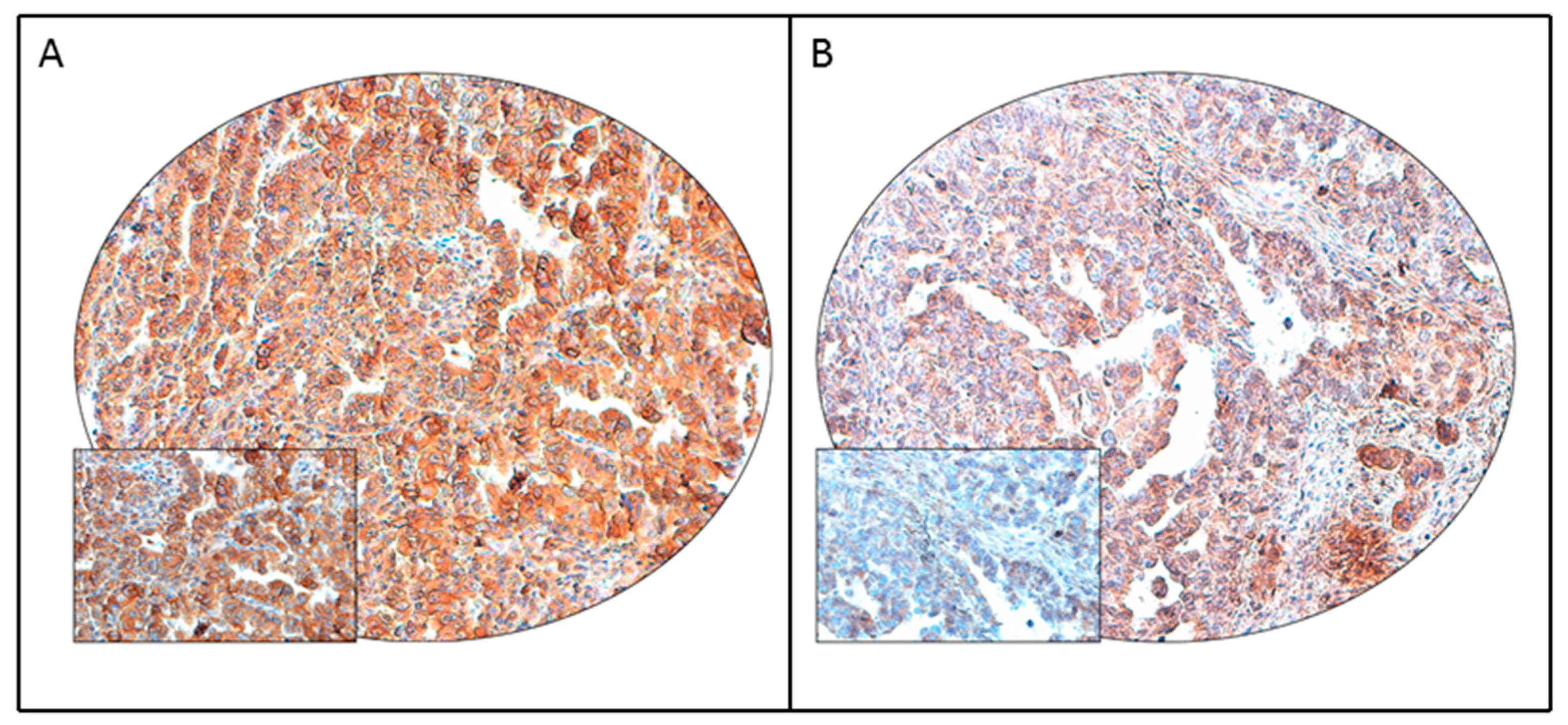
3.2. PD-L1 Protein Expression in Endometrial Cancer and Its Clinico-Pathological Associations
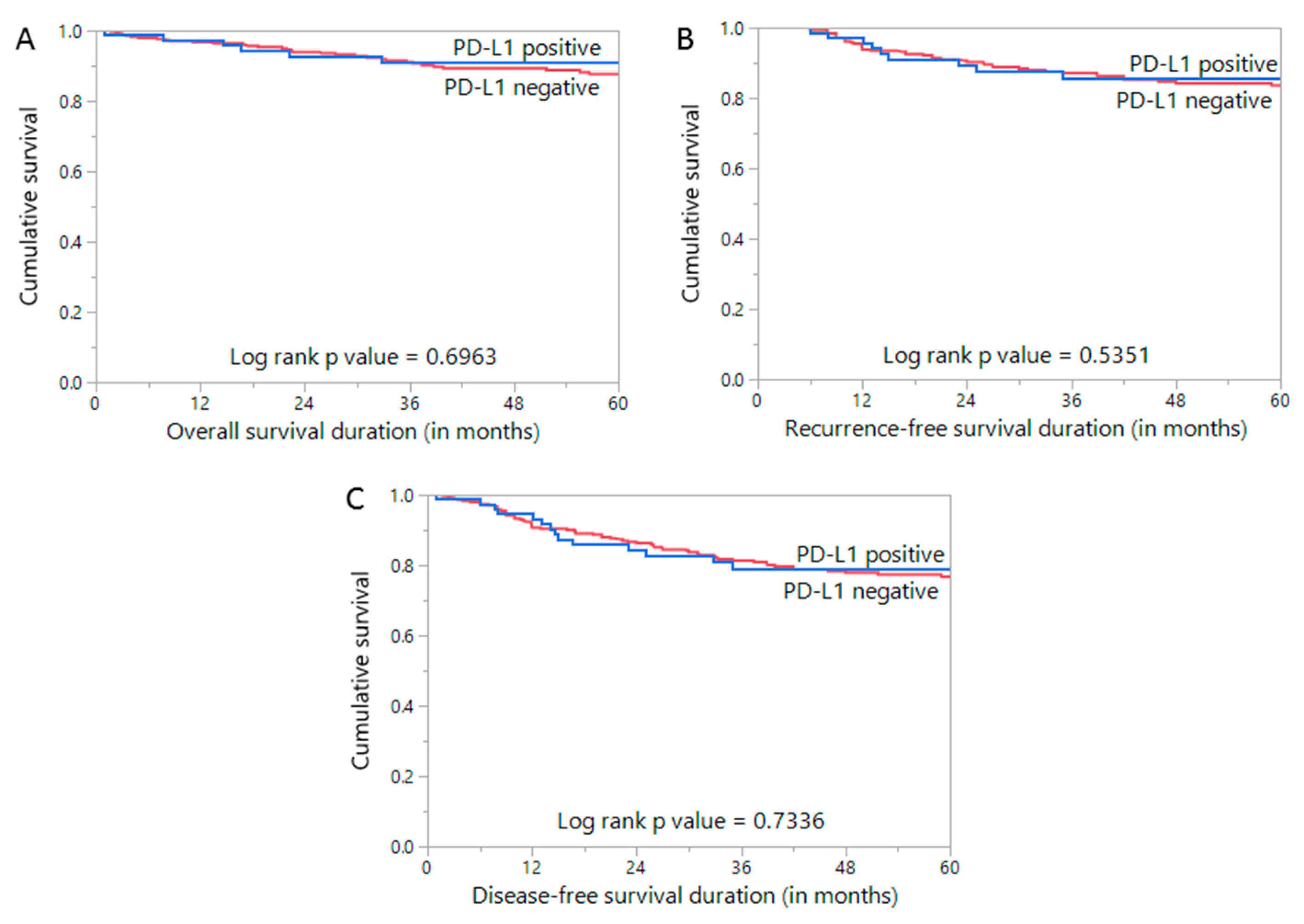
3.3. Prognostic Impact of PD-L1 Expression in Endometrial Cancer
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Howlader, N.; Krapcho, M.; Miller, D.; Bishop, K.; Kosary, C.; Yu, M.; Cronin, K.A. (Eds.) SEER Cancer Statistics Review, 1975–2014; National Cancer Institute: Bethesda, MD, USA, 2017. [Google Scholar]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA A Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- Alrawaji, A.; Alshahrani, Z.; Alzahrani, W.; Alomran, F.; Almadouj, A.; Alshehri, S.; Alzahrani, A.; Bazarbashi, S.; Alhashmi, H.; Almutlaq, H.; et al. Cancer Incidence Report Saudi Arabia 2015. In Saudi Cancer Registry; Saudi Health Council 2015: Riyadh, Saudi Arabia, 2018. [Google Scholar]
- Althubiti, M.A.; Eldein, M.M.N. Trends in the incidence and mortality of cancer in Saudi Arabia. Saudi Med. J. 2018, 39, 1259. [Google Scholar] [CrossRef]
- World Health Organization; Global Health Observatory (GHO) Data. Overweight and Obesity, Adults Aged 18+. World Health Organization [updated 16 June 2015]. Available online: http://www.who.int/gho/ncd/risk_factors/overweight_text/en (accessed on 22 December 2020).
- Colombo, N.; Creutzberg, C.; Amant, F.; Bosse, T.; González-Martín, A.; Ledermann, J.; Marth, C.; Nout, R.; Querleu, D.; Mirza, M.R. ESMO-ESGO-ESTRO consensus conference on endometrial cancer: Diagnosis, treatment and follow-up. Int. J. Gynecol. Cancer 2016, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Remmerie, M.; Janssens, V. Targeted therapies in type II endometrial cancers: Too little, but not too late. Int. J. Mol. Sci. 2018, 19, 2380. [Google Scholar] [CrossRef] [Green Version]
- Pardoll, D.M. The blockade of immune checkpoints in cancer immunotherapy. Nat. Rev. Cancer 2012, 12, 252–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zou, W.; Wolchok, J.D.; Chen, L. PD-L1 (B7-H1) and PD-1 pathway blockade for cancer therapy: Mechanisms, response biomarkers, and combinations. Sci. Transl. Med. 2016, 8, rv324–rv328. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Jiang, C.; Jin, L.; Zhang, X. Regulation of PD-L1: A novel role of pro-survival signalling in cancer. Ann. Oncol. 2016, 27, 409–416. [Google Scholar] [CrossRef]
- Topalian, S.L.; Taube, J.M.; Anders, R.A.; Pardoll, D.M. Mechanism-driven biomarkers to guide immune checkpoint blockade in cancer therapy. Nat. Rev. Cancer 2016, 16, 275–287. [Google Scholar] [CrossRef]
- Sheng, X.; Yan, X.; Chi, Z.; Si, L.; Cui, C.; Tang, B.; Li, S.; Mao, L.; Lian, B.; Wang, X. Axitinib in combination with toripalimab, a humanized immunoglobulin G4 monoclonal antibody against programmed cell death-1, in patients with metastatic mucosal melanoma: An open-label phase IB trial. J. Clin. Oncol. 2019, 37, 2987–2999. [Google Scholar] [CrossRef] [PubMed]
- Dang, T.O.; Ogunniyi, A.; Barbee, M.S.; Drilon, A. Pembrolizumab for the treatment of PD-L1 positive advanced or metastatic non-small cell lung cancer. Expert Rev. Anticancer Ther. 2016, 16, 13–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antill, Y.C.; Kok, P.S.; Robledo, K.; Barnes, E.; Friedlander, M.; Baron-Hay, S.E.; Shannon, C.M.; Coward, J.; Beale, P.J.; Goss, G. Activity of durvalumab in advanced endometrial cancer (AEC) according to mismatch repair (MMR) status: The phase II PHAEDRA trial (ANZGOG1601). J. Clin. Oncol. 2019, 37, 5501. [Google Scholar] [CrossRef]
- Balar, A.V.; Galsky, M.D.; Rosenberg, J.E.; Powles, T.; Petrylak, D.P.; Bellmunt, J.; Loriot, Y.; Necchi, A.; Hoffman-Censits, J.; Perez-Gracia, J.L. Atezolizumab as first-line treatment in cisplatin-ineligible patients with locally advanced and metastatic urothelial carcinoma: A single-arm, multicentre, phase 2 trial. Lancet 2017, 389, 67–76. [Google Scholar] [CrossRef] [Green Version]
- McDermott, D.F.; Sosman, J.A.; Sznol, M.; Massard, C.; Gordon, M.S.; Hamid, O.; Powderly, J.D.; Infante, J.R.; Fassò, M.; Wang, Y.V. Atezolizumab, an anti-programmed death-ligand 1 antibody, in metastatic renal cell carcinoma: Long-term safety, clinical activity, and immune correlates from a phase Ia study. J. Clin. Oncol. 2016, 34, 833–842. [Google Scholar] [CrossRef] [PubMed]
- Pasanen, A.; Ahvenainen, T.; Pellinen, T.; Vahteristo, P.; Loukovaara, M.; Bützow, R. PD-L1 expression in endometrial carcinoma cells and intratumoral immune cells: Differences across histologic and TCGA-based molecular subgroups. Am. J. Surg. Pathol. 2020, 44, 174–181. [Google Scholar] [CrossRef]
- Asaka, S.; Yen, T.-T.; Wang, T.-L.; Shih, I.-M.; Gaillard, S. T cell-inflamed phenotype and increased Foxp3 expression in infiltrating T-cells of mismatch-repair deficient endometrial cancers. Mod. Pathol. 2019, 32, 576–584. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kim, S.; Lee, H.S.; Yang, W.; Cho, H.; Chay, D.B.; Cho, S.J.; Hong, S.; Kim, J.-H. Prognostic implication of programmed cell death 1 protein and its ligand expressions in endometrial cancer. Gynecol. Oncol. 2018, 149, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Joehlin-Price, A.S.; Rhoades, J.; Ayoola-Adeola, M.; Miller, K.; Parwani, A.V.; Backes, F.J.; Felix, A.S.; Suarez, A.A. Programmed death ligand 1 expression among 700 consecutive endometrial cancers: Strong association with mismatch repair protein deficiency. Int. J. Gynecol. Cancer 2018, 28, 59–68. [Google Scholar] [CrossRef]
- Bregar, A.; Deshpande, A.; Grange, C.; Zi, T.; Stall, J.; Hirsch, H.; Reeves, J.; Sathyanarayanan, S.; Growdon, W.B.; Rueda, B.R. Characterization of immune regulatory molecules B7-H4 and PD-L1 in low and high grade endometrial tumors. Gynecol. Oncol. 2017, 145, 446–452. [Google Scholar] [CrossRef] [Green Version]
- Inaguma, S.; Wang, Z.; Lasota, J.; Sarlomo-Rikala, M.; McCue, P.A.; Ikeda, H.; Miettinen, M. Comprehensive immunohistochemical study of programmed cell death ligand 1 (PD-L1). Analysis in 5536 cases revealed consistent expression in trophoblastic tumors. Am. J. Surg. Pathol. 2016, 40, 1133. [Google Scholar] [CrossRef] [Green Version]
- Siraj, A.; Bavi, P.; Abubaker, J.; Jehan, Z.; Sultana, M.; Al-Dayel, F.; Al-Nuaim, A.; Alzahrani, A.; Ahmed, M.; Al-Sanea, O. Genome-wide expression analysis of Middle Eastern papillary thyroid cancer reveals c-MET as a novel target for cancer therapy. J. Pathol. 2007, 213, 190–199. [Google Scholar] [CrossRef]
- Bavi, P.; Jehan, Z.; Atizado, V.; Al-Dossari, H.; Al-Dayel, F.; Tulbah, A.; Amr, S.S.; Sheikh, S.S.; Ezzat, A.; El-Solh, H. Prevalence of fragile histidine triad expression in tumors from Saudi Arabia: A tissue microarray analysis. Cancer Epidemiol. Prev. Biomark. 2006, 15, 1708–1718. [Google Scholar] [CrossRef] [Green Version]
- Mesnage, S.; Auguste, A.; Genestie, C.; Dunant, A.; Pain, E.; Drusch, F.; Gouy, S.; Morice, P.; Bentivegna, E.; Lhomme, C. Neoadjuvant chemotherapy (NACT) increases immune infiltration and programmed death-ligand 1 (PD-L1) expression in epithelial ovarian cancer (EOC). Ann. Oncol. 2017, 28, 651–657. [Google Scholar] [CrossRef]
- Siraj, A.K.; Prabhakaran, S.; Bavi, P.; Bu, R.; Beg, S.; Hazmi, M.A.; Al-Rasheed, M.; Al-Assiri, M.; Sairafi, R.; Al-Dayel, F. Prevalence of Lynch syndrome in a Middle Eastern population with colorectal cancer. Cancer 2015, 121, 1762–1771. [Google Scholar] [CrossRef]
- Siraj, A.K.; Parvathareddy, S.K.; Bu, R.; Iqbal, K.; Siraj, S.; Masoodi, T.; Concepcion, R.M.; Ghazwani, L.O.; AlBadawi, I.; Al-Dayel, F. Germline POLE and POLD1 proofreading domain mutations in endometrial carcinoma from Middle Eastern region. Cancer Cell Int. 2019, 19, 334. [Google Scholar] [CrossRef]
- Fehrenbacher, L.; von Pawel, J.; Park, K.; Rittmeyer, A.; Gandara, D.R.; Aix, S.P.; Han, J.-Y.; Gadgeel, S.M.; Hida, T.; Cortinovis, D.L. Updated efficacy analysis including secondary population results for OAK: A randomized phase III study of atezolizumab versus docetaxel in patients with previously treated advanced non–small cell lung cancer. J. Thorac. Oncol. 2018, 13, 1156–1170. [Google Scholar] [CrossRef] [Green Version]
- Emens, L.A.; Cruz, C.; Eder, J.P.; Braiteh, F.; Chung, C.; Tolaney, S.M.; Kuter, I.; Nanda, R.; Cassier, P.A.; Delord, J.-P. Long-term clinical outcomes and biomarker analyses of atezolizumab therapy for patients with metastatic triple-negative breast cancer: A phase 1 study. JAMA Oncol. 2019, 5, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Eng, C.; Kim, T.W.; Bendell, J.; Argilés, G.; Tebbutt, N.C.; Di Bartolomeo, M.; Falcone, A.; Fakih, M.; Kozloff, M.; Segal, N.H. Atezolizumab with or without cobimetinib versus regorafenib in previously treated metastatic colorectal cancer (IMblaze370): A multicentre, open-label, phase 3, randomised, controlled trial. Lancet Oncol. 2019, 20, 849–861. [Google Scholar] [CrossRef]
- Liu, J.F.; Gordon, M.; Veneris, J.; Braiteh, F.; Balmanoukian, A.; Eder, J.P.; Oaknin, A.; Hamilton, E.; Wang, Y.; Sarkar, I. Safety, clinical activity and biomarker assessments of atezolizumab from a Phase I study in advanced/recurrent ovarian and uterine cancers. Gynecol. Oncol. 2019, 154, 314–322. [Google Scholar] [CrossRef] [PubMed]
- Sungu, N.; Yildirim, M.; Desdicioglu, R.; Başaran Aydoğdu, Ö.; Kiliçarslan, A.; Tatli Doğan, H.; Kiliç Yazgan, A.; Akyol, M.; Erdoğan, F. Expression of immunomodulatory molecules PD-1, PD-L1, and PD-L2, and their relationship with clinicopathologic characteristics in endometrial cancer. Int. J. Gynecol. Pathol. 2019, 38, 404–413. [Google Scholar] [CrossRef] [PubMed]
- Al-Hussaini, M.; Lataifeh, I.; Jaradat, I.; Abdeen, G.; Otay, L.; Badran, O.; Abu Sheikha, A.; Dayyat, A.; El Khaldi, M.; Ashi Al-Loh, S. Undifferentiated endometrial carcinoma, an immunohistochemical study including PD-L1 testing of a series of cases from a single cancer center. Int. J. Gynecol. Pathol. 2018, 37, 564–574. [Google Scholar] [CrossRef] [PubMed]
- Engerud, H.; Berg, H.F.; Myrvold, M.; Halle, M.K.; Bjorge, L.; Haldorsen, I.S.; Hoivik, E.A.; Trovik, J.; Krakstad, C. High degree of heterogeneity of PD-L1 and PD-1 from primary to metastatic endometrial cancer. Gynecol. Oncol. 2020, 157, 260–267. [Google Scholar] [CrossRef]
- Mo, Z.; Liu, J.; Zhang, Q.; Chen, Z.; Mei, J.; Liu, L.; Yang, S.; Li, H.; Zhou, L.; You, Z. Expression of PD-1, PD-L1 and PD-L2 is associated with differentiation status and histological type of endometrial cancer. Oncol. Lett. 2016, 12, 944–950. [Google Scholar] [CrossRef] [Green Version]
- Kamiya, S.; Kato, J.; Kamiya, T.; Yamashita, T.; Sumikawa, Y.; Hida, T.; Horimoto, K.; Sato, S.; Takahashi, H.; Sawada, M. Association between PD-L1 expression and lymph node metastasis in cutaneous squamous cell carcinoma. Asia-Pac. J. Clin. Oncol. 2020, 16, e108–e112. [Google Scholar] [CrossRef]
- Slater, N.A.; Googe, P.B. PD-L1 expression in cutaneous squamous cell carcinoma correlates with risk of metastasis. J. Cutan. Pathol. 2016, 43, 663–670. [Google Scholar] [CrossRef]
- García-Pedrero, J.M.; Martínez-Camblor, P.; Diaz-Coto, S.; Munguia-Calzada, P.; Vallina-Alvarez, A.; Vazquez-Lopez, F.; Rodrigo, J.P.; Santos-Juanes, J. Tumor programmed cell death ligand 1 expression correlates with nodal metastasis in patients with cutaneous squamous cell carcinoma of the head and neck. J. Am. Acad. Dermatol. 2017, 77, 527–533. [Google Scholar] [CrossRef]
- Le, D.T.; Uram, J.N.; Wang, H.; Bartlett, B.R.; Kemberling, H.; Eyring, A.D.; Skora, A.D.; Luber, B.S.; Azad, N.S.; Laheru, D. PD-1 blockade in tumors with mismatch-repair deficiency. N. Engl. J. Med. 2015, 372, 2509–2520. [Google Scholar] [CrossRef] [Green Version]
- Le, D.T.; Durham, J.N.; Smith, K.N.; Wang, H.; Bartlett, B.R.; Aulakh, L.K.; Lu, S.; Kemberling, H.; Wilt, C.; Luber, B.S. Mismatch repair deficiency predicts response of solid tumors to PD-1 blockade. Science 2017, 357, 409–413. [Google Scholar] [CrossRef] [Green Version]
- Sloan, E.A.; Ring, K.L.; Willis, B.C.; Modesitt, S.C.; Mills, A.M. PD-L1 expression in mismatch repair-deficient endometrial carcinomas, including lynch syndrome-associated and MLH1 promoter hypermethylated tumors. Am. J. Surg. Pathol. 2017, 41, 326–333. [Google Scholar] [CrossRef] [PubMed]
- Bhangoo, M.S.; Boasberg, P.; Mehta, P.; Elvin, J.A.; Ali, S.M.; Wu, W.; Klempner, S.J. Tumor mutational burden guides therapy in a treatment refractory POLE-mutant uterine carcinosarcoma. Oncologist 2018, 23, 518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howitt, B.E.; Shukla, S.A.; Sholl, L.M.; Ritterhouse, L.L.; Watkins, J.C.; Rodig, S.; Stover, E.; Strickland, K.C.; D’Andrea, A.D.; Wu, C.J. Association of polymerase e–mutated and microsatellite-instable endometrial cancers with neoantigen load, number of tumor-infiltrating lymphocytes, and expression of PD-1 and PD-L1. JAMA Oncol. 2015, 1, 1319–1323. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.; Li, Y.; Luo, R.; Xu, J.; Feng, J.; Wang, M. Prognostic and clinicopathological role of PD-L1 in endometrial cancer: A meta-analysis. Front. Oncol. 2020, 10, 632. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Clinico-Pathological Parameter | n (%) |
|---|---|
| Age | |
| Median | 59.3 |
| Range(IQR) ^ | 53.0–66.2 |
| Histologic subtype | |
| Type I | 387 (88.0) |
| Type II | 53 (12.0) |
| Myometrial invasion | |
| High | 221 (50.2) |
| Low | 219 (49.8) |
| Histological grade | |
| Well differentiated | 148 (33.6) |
| Moderately differentiated | 147 (33.4) |
| Poorly differentiated | 130 (29.6) |
| Unknown | 15 (3.4) |
| pT | |
| T1 | 308 (70.0) |
| T2 | 55 (12.5) |
| T3 | 58 (13.2) |
| T4 | 19 (4.3) |
| pN | |
| N0 | 410 (93.2) |
| N1-2 | 30 (6.8) |
| pM | |
| M0 | 417 (94.8) |
| M1 | 23 (5.2) |
| Tumor Stage | |
| I | 285 (64.8) |
| II | 48 (10.9) |
| III | 70 (15.9) |
| IV | 37 (8.4) |
| Primary treatment | |
| Surgery | 440 (100.0) |
| Adjuvant chemotherapy | 84 (19.1) |
| Paclitaxel and Carboplatin | 69 (15.7) |
| Carboplatin only | 15 (3.4) |
| Adjuvant Radiotherapy | 175 (39.8) |
| Total | PD-L1 Positive | PD-L1 Negative | p Value | ||||
|---|---|---|---|---|---|---|---|
| No. | % | No. | % | No. | % | ||
| No. of patients | 440 | 83 | 18.9 | 357 | 81.1 | ||
| Age (years) | |||||||
| ≤60 | 236 | 53.6 | 42 | 17.8 | 194 | 82.2 | 0.5387 |
| >60 | 204 | 46.4 | 41 | 20.1 | 163 | 79.9 | |
| Histologic subtype | |||||||
| Type I | 387 | 87.9 | 63 | 16.3 | 324 | 83.7 | 0.0005 * |
| Type II | 53 | 12.1 | 20 | 37.7 | 33 | 62.3 | |
| Myometrial invasion | |||||||
| High | 221 | 50.2 | 49 | 22.2 | 172 | 77.8 | 0.0741 |
| Low | 219 | 49.8 | 34 | 15.5 | 185 | 84.5 | |
| Grade | |||||||
| Grade 1 | 148 | 34.8 | 22 | 14.9 | 126 | 85.1 | 0.0893 |
| Grade 2 | 147 | 34.6 | 24 | 16.3 | 123 | 83.7 | |
| Grade 3 | 130 | 30.6 | 32 | 24.6 | 98 | 75.4 | |
| pT | |||||||
| T1 | 308 | 70.0 | 53 | 17.2 | 255 | 82.8 | 0.0570 |
| T2 | 55 | 12.5 | 14 | 25.5 | 41 | 74.5 | |
| T3 | 58 | 13.2 | 8 | 13.8 | 50 | 86.2 | |
| T4 | 19 | 4.3 | 8 | 42.1 | 11 | 57.9 | |
| pN | |||||||
| N0 | 410 | 93.2 | 72 | 17.6 | 338 | 82.4 | 0.0172 * |
| N1-N2 | 30 | 6.8 | 11 | 36.7 | 19 | 63.3 | |
| pM | |||||||
| M0 | 417 | 94.8 | 77 | 18.5 | 340 | 81.5 | 0.3822 |
| M1 | 23 | 5.2 | 6 | 26.1 | 17 | 73.9 | |
| Tumor Stage | |||||||
| I | 285 | 64.8 | 47 | 16.5 | 238 | 83.5 | 0.2443 |
| II | 48 | 10.9 | 11 | 22.9 | 37 | 77.1 | |
| III | 70 | 15.9 | 14 | 20.0 | 56 | 80.0 | |
| IV | 37 | 8.4 | 11 | 29.7 | 26 | 70.3 | |
| MMR IHC | |||||||
| dMMR | 53 | 12.1 | 8 | 15.1 | 45 | 84.9 | 0.4435 |
| pMMR | 387 | 87.9 | 75 | 19.4 | 312 | 80.6 | |
| POLE mutation | |||||||
| Present | 2 | 0.5 | 0 | 0.0 | 2 | 100.0 | 0.3576 |
| Absent | 429 | 99.5 | 82 | 19.1 | 347 | 80.9 | |
| 5 year overall survival | 90.9 | 87.0 | 0.6963 | ||||
| 5 year recurrence-free survival | 85.7 | 83.6 | 0.5351 | ||||
| 5 year disease-free survival | 78.9 | 76.8 | 0.7336 | ||||
| Clinico-Pathological Variables | Odds Ratio | 95% CI | p-Value |
|---|---|---|---|
| Age | |||
| Age>60 years (vs. ≤60 years) | 0.65 | 0.29–1.47 | 0.3020 |
| Histologic grade | |||
| Grade 3 (vs. Grade 1–2) | 2.14 | 0.92–4.96 | 0.0755 |
| Myometrial invasion | |||
| High (vs. Low) | 2.84 | 1.01–7.94 | 0.0473 * |
| pT | |||
| T3-4 (vs. T1-2) | 2.42 | 0.90–6.49 | 0.0801 |
| pM | |||
| M1 (VS. M0) | 0.63 | 0.03–11.74 | 0.7548 |
| Tumor Stage | |||
| IV (vs I–III) | 0.28 | 0.03–2.75 | 0.2766 |
| MMR statusd | |||
| MMR (vs. pMMR) | 1.20 | 0.41–3.58 | 0.7376 |
| PD-L1 expression | |||
| Positive (vs. Negative) | 2.94 | 1.26–6.84 | 0.0123 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siraj, A.K.; Parvathareddy, S.K.; Annaiyappanaidu, P.; Siraj, N.; Al-Rasheed, M.; Al-Badawi, I.A.; Al-Dayel, F.; Al-Kuraya, K.S. PD-L1 Expression Is an Independent Marker for Lymph Node Metastasis in Middle Eastern Endometrial Cancer. Diagnostics 2021, 11, 394. https://doi.org/10.3390/diagnostics11030394
Siraj AK, Parvathareddy SK, Annaiyappanaidu P, Siraj N, Al-Rasheed M, Al-Badawi IA, Al-Dayel F, Al-Kuraya KS. PD-L1 Expression Is an Independent Marker for Lymph Node Metastasis in Middle Eastern Endometrial Cancer. Diagnostics. 2021; 11(3):394. https://doi.org/10.3390/diagnostics11030394
Chicago/Turabian StyleSiraj, Abdul K., Sandeep Kumar Parvathareddy, Padmanaban Annaiyappanaidu, Nabil Siraj, Maha Al-Rasheed, Ismail A. Al-Badawi, Fouad Al-Dayel, and Khawla S. Al-Kuraya. 2021. "PD-L1 Expression Is an Independent Marker for Lymph Node Metastasis in Middle Eastern Endometrial Cancer" Diagnostics 11, no. 3: 394. https://doi.org/10.3390/diagnostics11030394