
Suitability of Bronchoscopic Biopsy Tissue Samples for Next-Generation Sequencing

 ,
,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients and Study Design
2.2. Pathological Diagnosis and Evaluation of Pathological Factors
2.3. Biomarker Analysis
2.4. ODxTT in Patients with NSCLC
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
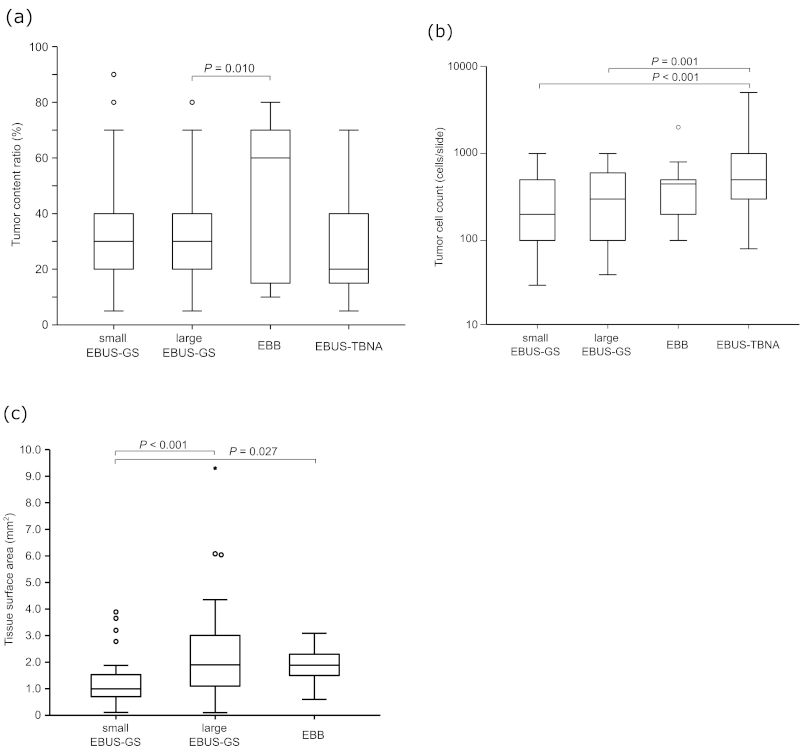
3.2. Tumor Content Determined in Biopsy Samples
3.3. Success Rate of ODxTT Using Different Bronchoscopic Devices
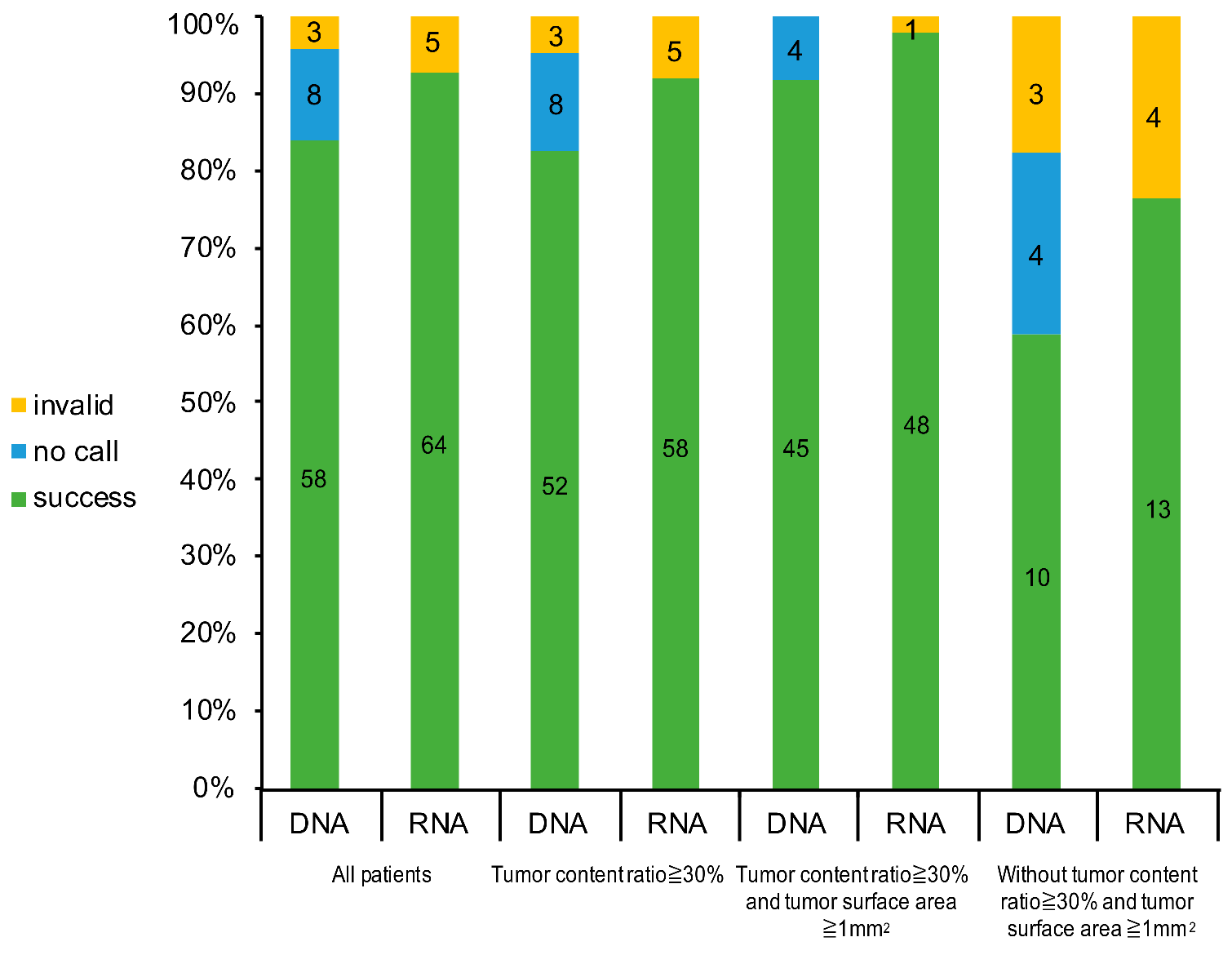
3.4. Success Rate of ODxTT by Criteria
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| EBB | endobronchial biopsy |
| EBUS-GS | endobronchial ultrasonography with a guide sheath |
| EBUS-TBNA | endobronchial ultrasound-guided transbronchial needle aspiration |
| EGFR | epidermal growth factor receptor |
| EML4–ALK | echinoderm microtubule-associated protein-like 4 and anaplastic lymphoma kinase |
| NGS | next-generation sequencing |
| NSCLC | non-small-cell lung cancer |
| ODxTT | Oncomine Dx Target Test |
| OS | overall survival |
| PCR | polymerase chain reaction |
| QC | quality control |
| ROS1 | ROS proto-oncogene 1 |
| SD | standard deviation |
| TBB | transbronchial biopsy |
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Ohe, Y.; Ohashi, Y.; Kubota, K.; Tamura, T.; Nakagawa, K.; Negoro, S.; Nishiwaki, Y.; Saijo, N.; Ariyoshi, Y.; Fukuoka, M. Randomized phase III study of cisplatin plus irinotecan versus carboplatin plus paclitaxel, cisplatin plus gemcitabine, and cisplatin plus vinorelbine for advanced non-small-cell lung cancer: Four-Arm Cooperative Study in Japan. Ann. Oncol. 2007, 18, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Schiller, J.H.; Harrington, D.; Belani, C.P.; Langer, C.; Sandler, A.; Krook, J.; Zhu, J.; Johnson, D.H. Comparison of four chemotherapy regimens for advanced non-small-cell lung cancer. N. Engl. J. Med. 2002, 346, 92–98. [Google Scholar] [CrossRef]
- Herbst, R.S.; Morgensztern, D.; Boshoff, C. The biology and management of non-small cell lung cancer. Nature 2018, 553, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Maemondo, M.; Inoue, A.; Kobayashi, K.; Sugawara, S.; Oizumi, S.; Isobe, H.; Gemma, A.; Harada, M.; Yoshizawa, H.; Kinoshita, I.; et al. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N. Engl. J. Med. 2010, 362, 2380–2388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inoue, A.; Kobayashi, K.; Usui, K.; Maemondo, M.; Okinaga, S.; Mikami, I.; Ando, M.; Yamazaki, K.; Saijo, Y.; Gemma, A.; et al. First-line gefitinib for patients with advanced non-small-cell lung cancer harboring epidermal growth factor receptor mutations without indication for chemotherapy. J. Clin. Oncol. 2009, 27, 1394–1400. [Google Scholar] [CrossRef]
- Mok, T.S.; Wu, Y.L.; Thongprasert, S.; Yang, C.H.; Chu, D.T.; Saijo, N.; Sunpaweravong, P.; Han, B.; Margono, B.; Ichinose, Y.; et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N. Engl. J. Med. 2009, 361, 947–957. [Google Scholar] [CrossRef]
- Solomon, B.J.; Mok, T.; Kim, D.W.; Wu, Y.L.; Nakagawa, K.; Mekhail, T.; Felip, E.; Cappuzzo, F.; Paolini, J.; Usari, T.; et al. First-line crizotinib versus chemotherapy in ALK-positive lung cancer. N. Engl. J. Med. 2014, 371, 2167–2177. [Google Scholar] [CrossRef] [Green Version]
- Shaw, A.T.; Ou, S.H.; Bang, Y.J.; Camidge, D.R.; Solomon, B.J.; Salgia, R.; Riely, G.J.; Varella-Garcia, M.; Shapiro, G.I.; Costa, D.B.; et al. Crizotinib in ROS1-rearranged non-small-cell lung cancer. N. Engl. J. Med. 2014, 371, 1963–1971. [Google Scholar] [CrossRef] [Green Version]
- Planchard, D.; Besse, B.; Groen, H.J.M.; Souquet, P.J.; Quoix, E.; Baik, C.S.; Barlesi, F.; Kim, T.M.; Mazieres, J.; Novello, S.; et al. Dabrafenib plus trametinib in patients with previously treated BRAF(V600E)-mutant metastatic non-small cell lung cancer: An open-label, multicentre phase 2 trial. Lancet Oncol. 2016, 17, 984–993. [Google Scholar] [CrossRef] [Green Version]
- Campbell, J.D.; Alexandrov, A.; Kim, J.; Wala, J.; Berger, A.H.; Pedamallu, C.S.; Shukla, S.A.; Guo, G.; Brooks, A.N.; Murray, B.A.; et al. Distinct patterns of somatic genome alterations in lung adenocarcinomas and squamous cell carcinomas. Nat. Genet. 2016, 48, 607–616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- FDA, U. Summary of Safety and Effectiveness Data for Oncomine Dx Target Test; 2017. Available online: https://www.accessdata.fda.gov/cdrh_docs/pdf16/P160045B.pdf (accessed on 23 February 2021).
- Liam, C.K.; Lee, P.; Yu, C.J.; Bai, C.; Yasufuku, K. The diagnosis of lung cancer in the era of interventional pulmonology. Int. J. Tuberc. Lung Dis. 2021, 25, 6–15. [Google Scholar] [CrossRef]
- Yu, T.M.; Morrison, C.; Gold, E.J.; Tradonsky, A.; Layton, A.J. Multiple Biomarker Testing Tissue Consumption and Completion Rates With Single-gene Tests and Investigational Use of Oncomine Dx Target Test for Advanced Non-Small-cell Lung Cancer: A Single-center Analysis. Clin. Lung Cancer 2019, 20, 20–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nemoto, D.; Yokose, T.; Katayama, K.; Murakami, S.; Kato, T.; Saito, H.; Suzuki, M.; Eriguchi, D.; Samejima, J.; Nagashima, T.; et al. Tissue surface area and tumor cell count affect the success rate of the Oncomine Dx Target Test in the analysis of biopsy tissue samples. Thorac. Cancer 2020, 12, 194–200. [Google Scholar] [CrossRef]
- Katsurada, N.; Tachihara, M.; Jimbo, N.; Yamamoto, M.; Yoshioka, J.; Mimura, C.; Satoh, H.; Furukawa, K.; Otoshi, T.; Kiriu, T. Yield of Tumor Samples with a Large Guide-sheath in Endobronchial Ultrasound Transbronchial Biopsy for Non-Small Cell Lung Cancer: A Prospective Study, 2020. Available online: https://assets.researchsquare.com/files/rs-69225/v1/5c999452-8779-469f-9502-44f8c998f226.pdf (accessed on 23 February 2021).
- Travis, W.D.; Brambilla, E.; Nicholson, A.G.; Yatabe, Y.; Austin, J.H.M.; Beasley, M.B.; Chirieac, L.R.; Dacic, S.; Duhig, E.; Flieder, D.B.; et al. The 2015 World Health Organization Classification of Lung Tumors: Impact of Genetic, Clinical and Radiologic Advances Since the 2004 Classification. J. Thorac. Oncol. 2015, 10, 1243–1260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kris, M.G.; Johnson, B.E.; Berry, L.D.; Kwiatkowski, D.J.; Iafrate, A.J.; Wistuba, I.I.; Varella-Garcia, M.; Franklin, W.A.; Aronson, S.L.; Su, P.F.; et al. Using multiplexed assays of oncogenic drivers in lung cancers to select targeted drugs. JAMA 2014, 311, 1998–2006. [Google Scholar] [CrossRef]
- Shimizu, J.; Masago, K.; Saito, H.; Nishino, K.; Kurata, T.; Itoh, Y.; Yoshimura, Y.; Yabuki, Y.; Dosaka-Akita, H. Biomarker testing for personalized, first-line therapy in advanced nonsquamous non-small cell lung cancer patients in the real world setting in Japan: A retrospective, multicenter, observational study (the BRAVE study). Ther. Adv. Med. Oncol. 2020, 12, 1758835920904522. [Google Scholar] [CrossRef]
- Udagawa, H.; Kirita, K.; Naito, T.; Nomura, S.; Ishibashi, M.; Matsuzawa, R.; Hisakane, K.; Usui, Y.; Matsumoto, S.; Yoh, K.; et al. Feasibility and utility of transbronchial cryobiopsy in precision medicine for lung cancer: Prospective single-arm study. Cancer Sci. 2020, 111, 2488–2498. [Google Scholar] [CrossRef]
- Kage, H.; Kohsaka, S.; Shinozaki-Ushiku, A.; Hiraishi, Y.; Sato, J.; Nagayama, K.; Ushiku, T.; Takai, D.; Nakajima, J.; Miyagawa, K.; et al. Small lung tumor biopsy samples are feasible for high quality targeted next generation sequencing. Cancer Sci. 2019, 110, 2652–2657. [Google Scholar] [CrossRef]
- Tone, M.; Inomata, M.; Awano, N.; Kuse, N.; Takada, K.; Minami, J.; Muto, Y.; Fujimoto, K.; Kumasaka, T.; Izumo, T. Comparison of adequacy between transbronchial lung cryobiopsy samples and endobronchial ultrasound-guided transbronchial needle aspiration samples for next-generation sequencing analysis. Thorac. Cancer 2020, 12, 251–258. [Google Scholar] [CrossRef]
- Nakajima, T.; Yasufuku, K.; Takahashi, R.; Shingyoji, M.; Hirata, T.; Itami, M.; Matsui, Y.; Itakura, M.; Iizasa, T.; Kimura, H. Comparison of 21-gauge and 22-gauge aspiration needle during endobronchial ultrasound-guided transbronchial needle aspiration. Respirology 2011, 16, 90–94. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Wu, Y.; Wang, H.; Yu, G.; Xu, B.; Jia, N.; Yao, Z. Slow-pull capillary technique versus suction technique in endobronchial ultrasound-guided transbronchial needle aspiration for diagnosing diseases involving hilar and mediastinal lymph node enlargement. Ther. Adv. Respir. Dis. 2020, 14, 1753466620907037. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | All Patients (n = 184) | Analyzed with ODxTT (n = 69) |
|---|---|---|
| Median age, years (range) | 72 (42–88) | 72 (45–88) |
| Sex (male/female) | 134/50 | 55/14 |
| Tumor stage (I/II/III/IV/r) | 23/17/54/84/6 | 6/9/23/30/1 |
| Histology (SQ/non-SQ) | 51/133 | 27/42 |
| Bronchoscopic device | ||
| Small EBUS-GS | 43 | 14 (32.6%) |
| Large EBUS-GS | 77 | 32 (41.5%) |
| EBB | 14 | 8 (57.1%) |
| EBUS-TBNA | 50 | 15 (30%) |
| Purpose of biopsy (initial/second biopsy) | 165/19 | 66/3 |
| Bronchoscopic Device | Small EBUS-GS | Large EBUS-GS | EBB | EBUS-TBNA |
|---|---|---|---|---|
| n | 43 | 77 | 14 | 50 |
| Tumor content ratio ≥ 30% | 24 (55.8%) | 40 (51.9%) | 9 (64.3%) | 18 (36%) |
| Tissue surface area ≥ 1 mm2 | 21 (48.4%) | 61 (79.2%) | 11 (78.6%) | - |
| Tumor content ratio ≥ 30% and tissue surface area ≥ 1 mm2 | 10 (41.7%) | 33 (42.9%) | 6 (42.9%) | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murakami, S.; Yokose, T.; Nemoto, D.; Suzuki, M.; Usui, R.; Nakahara, Y.; Kondo, T.; Kato, T.; Saito, H. Suitability of Bronchoscopic Biopsy Tissue Samples for Next-Generation Sequencing. Diagnostics 2021, 11, 391. https://doi.org/10.3390/diagnostics11030391
Murakami S, Yokose T, Nemoto D, Suzuki M, Usui R, Nakahara Y, Kondo T, Kato T, Saito H. Suitability of Bronchoscopic Biopsy Tissue Samples for Next-Generation Sequencing. Diagnostics. 2021; 11(3):391. https://doi.org/10.3390/diagnostics11030391
Chicago/Turabian StyleMurakami, Shuji, Tomoyuki Yokose, Daiji Nemoto, Masaki Suzuki, Ryou Usui, Yoshiro Nakahara, Tetsuro Kondo, Terufumi Kato, and Haruhiro Saito. 2021. "Suitability of Bronchoscopic Biopsy Tissue Samples for Next-Generation Sequencing" Diagnostics 11, no. 3: 391. https://doi.org/10.3390/diagnostics11030391