
Review of Recent Prevalence of Urogenital Schistosomiasis in Sub-Saharan Africa and Diagnostic Challenges in the Field Setting

Abstract
:1. Introduction
2. Recent Status of UGS in Sub-Saharan Africa
2.1. Overall Reports on Prevalence
2.2. Mapping Reports
2.3. Local Prevalence Reports
3. Diagnosis of UGS
3.1. Urine Microscopy
3.1.1. UM by Filtration
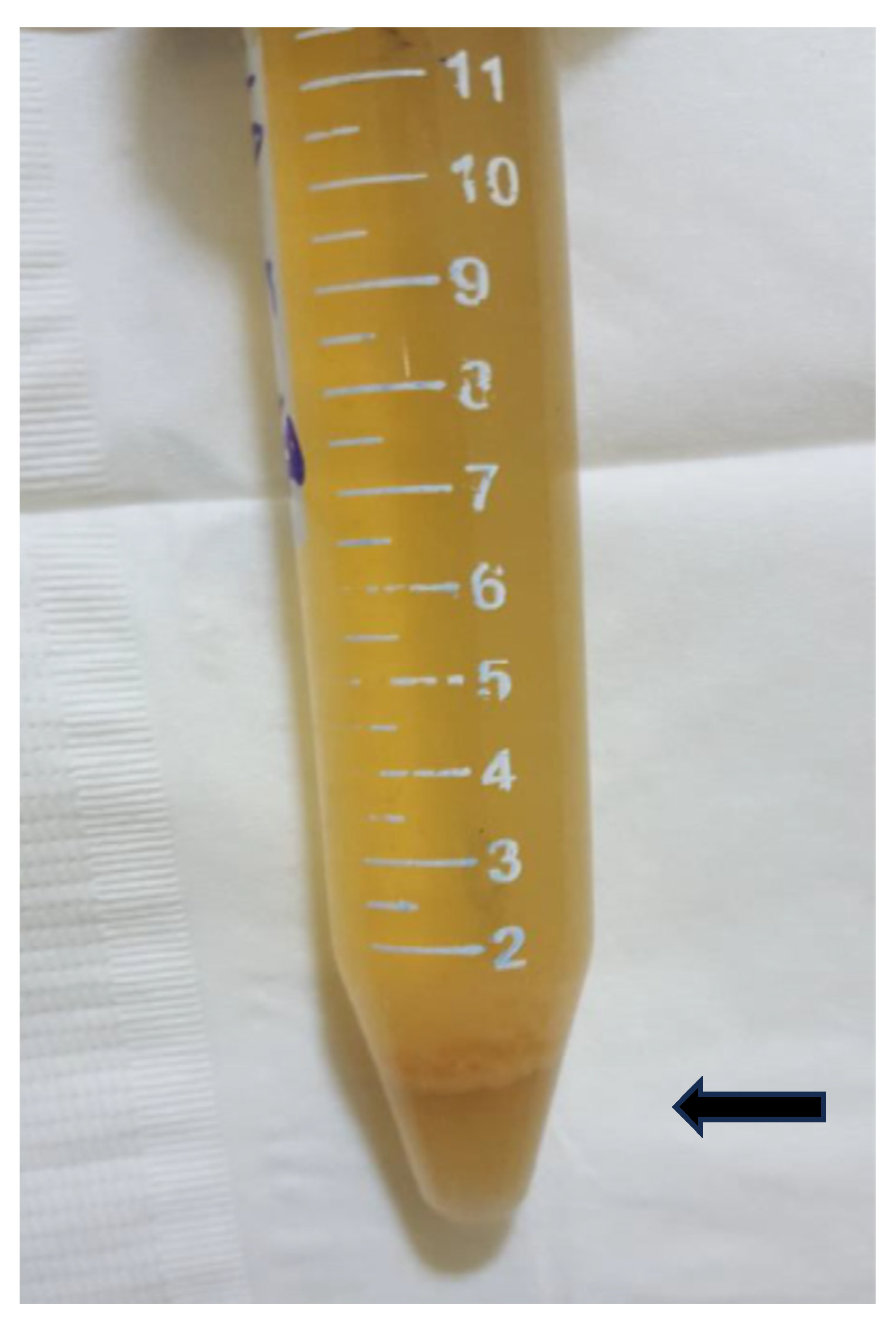
3.1.2. UM by Centrifugation
3.1.3. UM by or Mobile Phone Microscopy or SchistoScope
3.2. Detection of Hematuria
3.2.1. Detection of Microhematuria by Urine Reagent Strips
3.2.2. Macrohematuria
3.3. Serodiagnosis and Molecular Diagnosis of UGS
3.3.1. Serology
3.3.2. Molecular Diagnosis

{kind=link}
{kind=link}
{kind=link}
| Country | Urine Strip Test for Microhematuria | Gold-Standard (%) | References | ||||
|---|---|---|---|---|---|---|---|
| Positive Rate (%) | Sensitivity (%) | Specificity (%) | Positive Predictive Value | Negative Predictive Value | |||
| Angola | 65.7 | 96.0 | 61.3 | 88.8 | UM 61.2 | [7] | |
| Cameroon | 24.9 | 70.3 | 87.9 | UM 31.5 | [12] | ||
| Ethiopia | 22.5 | 99.3 | 88.1 | 53.8 | 99.8 | UM 12.2 | [19] |
| Ethiopia | 2.35 | 100 | 97.4 | UM 0.2 | [22] | ||
| Tanzania | 9.3 | 78 | 99.8 | 97.8 | 97.8 | UM 7.4 | [62] |
| 0 | |||||||
| 48.0 | 96.6 | 82.6 | 77.8 | 97.4 | UM 38.7 | ||
| Zimbabwe | 81 | 96.9 | 87.2 | 95.2 | Early SI | [78] | |
| Zambia DDIA | 60 | UM 61% | [75] | ||||
| IHA | 74 | ||||||
| Meta-analysis | 81 | 89 | [89] | ||||
| Tanzania | 26.6 | 75.0 | 75.7 | 18.4 | 97.6 | UM 6.8 | [90] |
| Senegal | 23.1 | UM 20.3 qPCR 34.6 | [98] | ||||
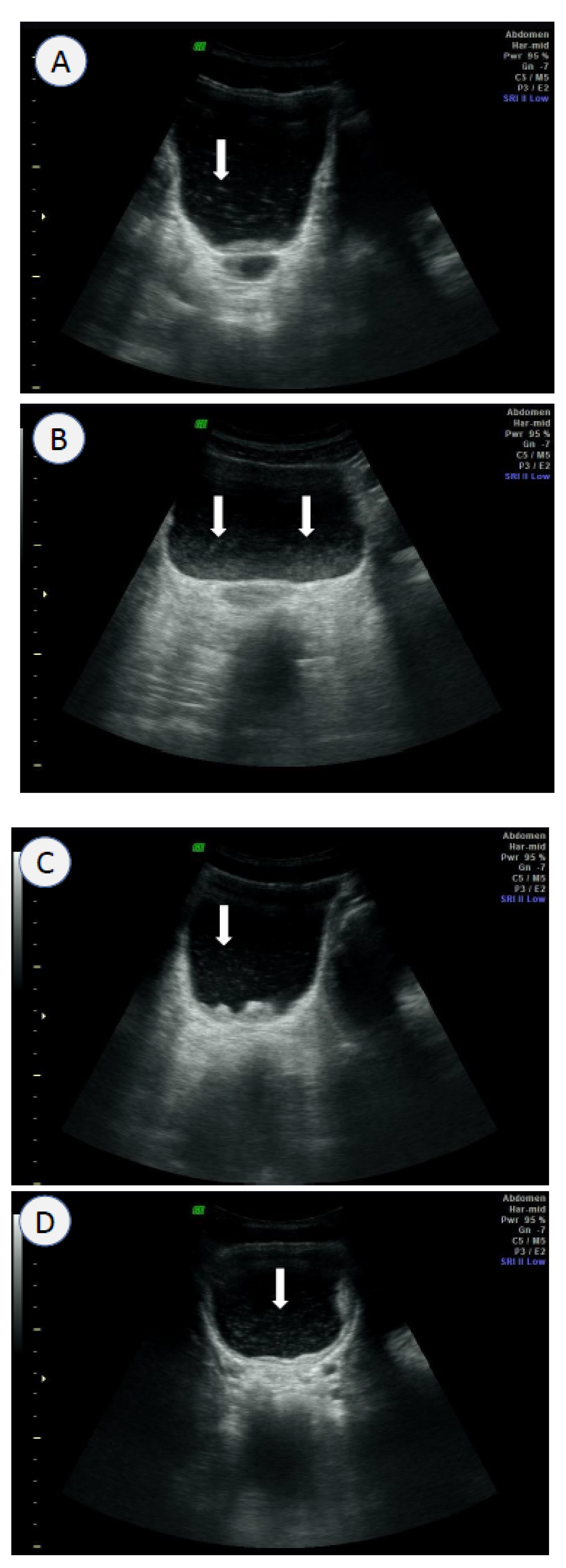
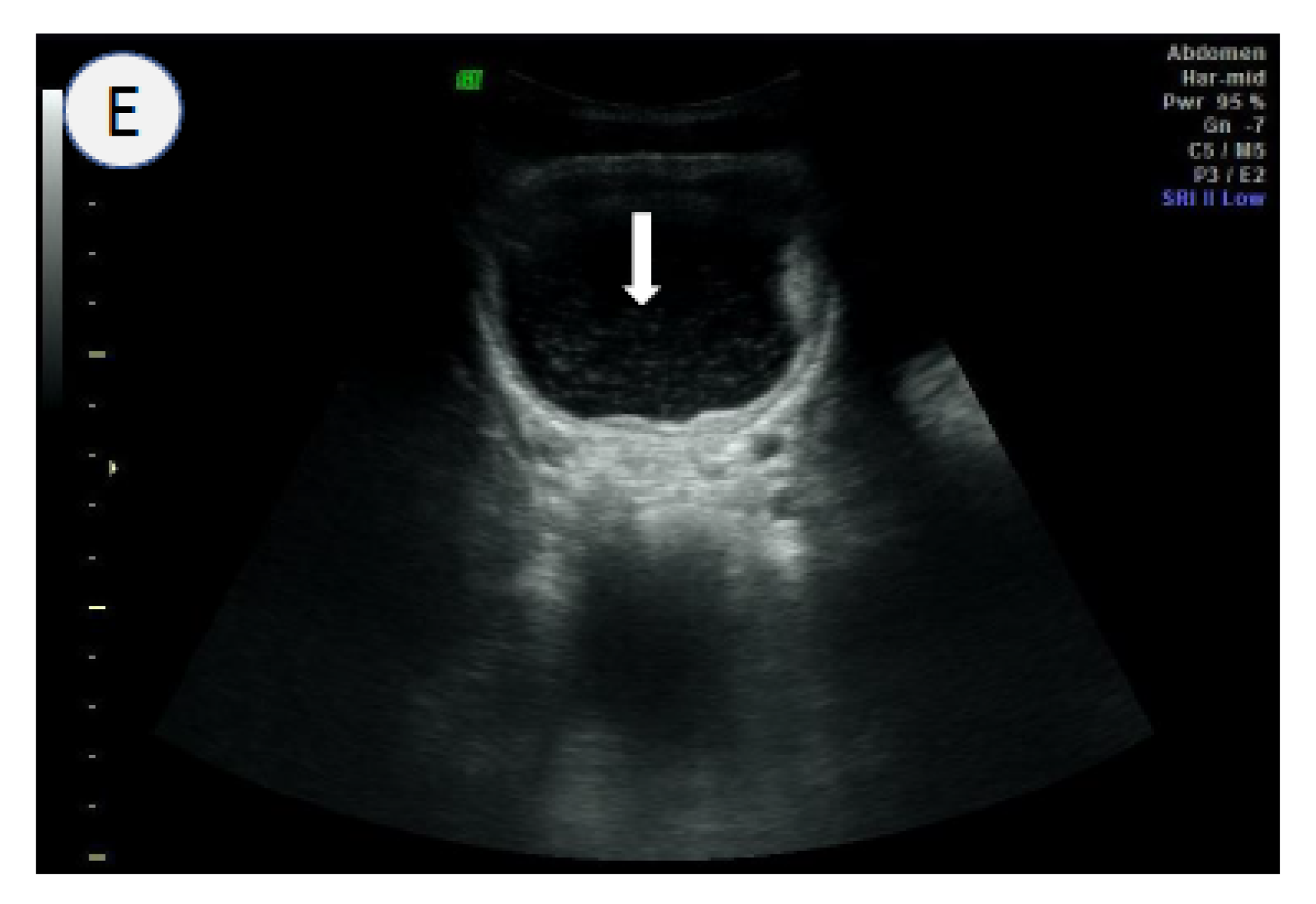
3.4. Ultrasound Scanning
4. Conclusions
Funding
Conflicts of Interest
Abbreviations
| CAA | circulating anodic antigen |
| CCA | circulating cathodic antigen |
| ELISA | enzyme-linked immunosorbent assay |
| IS | intestinal schistosomiasis |
| KK | Kato–Katz |
| LAMP | loop-mediated isothermal amplification |
| MacH | macrohematuria |
| M&E | monitoring and evaluation |
| MDA | mass drug administration |
| MDGs | millennium development goals |
| MicH | microhematuria |
| NGO | non-governmental organization |
| NTDs | neglected tropical diseases |
| PC | preventive chemotherapy |
| PCR | polymerase chain reaction |
| qPCR | quantitative polymerase chain reaction |
| RPA | recombinase polymerase amplification |
| SAC | school-aged children |
| SCI | schistosomiasis control initiative |
| SDGs | sustainable developmental goals |
| SEA | soluble egg antigen |
| SSA | sub-Saharan Africa |
| UGS | urogenital schistosomiasis |
| UM | urine microscopy |
| UN | United Nations |
| WHO | World Health Organization |
References
- WHO. Schistosomiasis. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/schistosomiasis (accessed on 24 January 2023).
- United Nations. The 17 Goals. 2019. Available online: https://sdgs.un.org/goals (accessed on 2 February 2023).
- MERCK. Merck Provides 1.5 Billionth Tablet of Praziquantel for Treatment of Schistosomiasis. Available online: https://www.merckgroup.com/en/news/praziquantel-tablet-donation-24-01-2022.html (accessed on 25 February 2023).
- WHO. Control of Neglected Tropical Diseases. PCT Databank—Schistosomiasis. Available online: https://www.who.int/teams/control-of-neglected-tropical-diseases/data-platforms/pct-databank/schistosomiasis (accessed on 24 January 2023).
- Mendes, E.P.; Okhai, H.; Cristóvão, R.E.; Almeida, M.C.; Katondi, N.; Thompson, R.; Mupoyi, S.; Mwinzi, P.; Ndayishimiye, O.; Djerandouba, F.; et al. Mapping of schistosomiasis and soil-transmitted helminthiases across 15 provinces of Angola. PLoS Negl. Trop. Dis. 2022, 16, e0010458. [Google Scholar] [CrossRef]
- Bartlett, A.W.; Sousa-Figueiredo, J.C.; van Goor, R.C.; Monaghan, P.; Lancaster, W.; Mugizi, R.; Mendes, E.P.; Nery, S.V.; Lopes, S. Burden and factors associated with schistosomiasis and soil-transmitted helminth infections among school-age children in Huambo, Uige and Zaire provinces, Angola. Infect. Dis. Poverty 2022, 11, 73. [Google Scholar] [CrossRef]
- Bocanegra, C.; Gallego, S.; Mendioroz, J.; Moreno, M.; Sulleiro, E.; Salvador, F.; Sikaleta, N.; Nindia, A.; Tchipita, D.; Joromba, M.; et al. Epidemiology of schistosomiasis and usefulness of indirect diagnostic tests in school-age children in Cubal, Central Angola. PLoS Negl. Trop. Dis. 2015, 9, e0004055. [Google Scholar] [CrossRef]
- Onzo-Aboki, A.; Ibikounlé, M.; Boko, P.M.; Savassi, B.S.; Doritchamou, J.; Siko, E.J.; Daré, A.; Batcho, W.; Massougbodji, A.; Tougoue, J.J.; et al. Human schistosomiasis in Benin: Countrywide evidence of Schistosoma haematobium predominance. Acta Trop. 2019, 191, 185–197. [Google Scholar] [CrossRef]
- Cisse, M.; Sangare, I.; Djibougou, A.D.; Tahita, M.C.; Gnissi, S.; Bassinga, J.K.W.; Konda, S.; Diallo, A.H. Prevalence and risk factors of Schistosoma mansoni infection among preschool-aged children from Panamasso village, Burkina Faso. Parasites Vectors 2021, 14, 185. [Google Scholar] [CrossRef]
- Jatsa, H.B.; Femoe, U.M.; Dongmo, C.N.; Kamwa, R.I.N.; Fesuh, B.N.; Tchuente, L.-A.T.; Kamtchouing, P. Reduction of testosterone levels in Schistosoma haematobium- or Schistosoma mansoni-infected men: A cross-sectional study in two schistosomiasis-endemic areas of the Adamawa region of Cameroon. BMC Infect. Dis. 2022, 22, 230. [Google Scholar] [CrossRef]
- Sumbele, I.U.N.; Tabi, D.B.; Teh, R.N.; Njunda, A.L. Urogenital schistosomiasis burden in school-aged children in Tiko, Cameroon: A cross-sectional study on prevalence, intensity, knowledge and risk factors. Trop. Med. Health 2021, 49, 75. [Google Scholar] [CrossRef]
- Green, A.E.; Anchang-Kimbi, J.K.; Wepnje, G.B.; Ndassi, V.D.; Kimbi, H.K. Distribution and factors associated with urogenital schistosomiasis in the Tiko Health District, a semi-urban setting, South West Region, Cameroon. Infect. Dis. Poverty 2021, 10, 49. [Google Scholar] [CrossRef]
- Ndassi, V.D.; Anchang-Kimbi, J.K.; Sumbele, I.U.N.; Ngufor, L.A.; Nadege, K.; Kimbi, H.K. The epidemiological status of urogenital schistosomiasis among reproductive aged individuals in the Tiko Health Area—A semi-urban setting in the Mount Cameroon area. PLoS Negl. Trop. Dis. 2021, 15, e0008978. [Google Scholar] [CrossRef]
- Visclosky, T.; Hashikawa, A.; Kroner, E. Discovery of a hidden schistosomiasis endemic in the Salamat Region of Chad, Africa. Glob. Health Sci. Pract. 2022, 10, e2000703. [Google Scholar] [CrossRef]
- Moser, W.; Batil, A.A.; Ott, R.; Abderamane, M.; Clements, R.; Wampfler, R.; Poppert, S.; Steinmann, P.; Allan, F.; Greter, H. High prevalence of urinary schistosomiasis in a desert population: Results from an exploratory study around the Ounianga lakes in Chad. Infect. Dis. Poverty 2022, 11, 5. [Google Scholar] [CrossRef] [PubMed]
- Coulibaly, J.T.; Silue, K.D.; Armstrong, M.; Derby, M.D.d.L.; D’ambrosio, M.V.; Fletcher, D.A.; Keiser, J.; Fisher, K.; Andrews, J.R.; Bogoch, I.I. High Sensitivity of mobile phone microscopy screening for Schistosoma haematobium in Azaguié, Côte d’Ivoire. Am. J. Trop. Med. Hyg. 2023, 108, 41–43. [Google Scholar] [CrossRef]
- Ouattara, M.; Bassa, F.K.; Diakité, N.R.; Hattendorf, J.; Coulibaly, J.T.; Yao, P.K.; Tian-Bi, Y.-N.T.; Konan, C.K.; Assaré, R.K.; Koné, N.; et al. Effectiveness of four different interventions against Schistosoma haematobium in a seasonal transmission setting of Côte d’Ivoire: A cluster randomized trial. Clin. Infect. Dis. 2021, 74, 2181–2190. [Google Scholar] [CrossRef] [PubMed]
- Bassa, F.K.; Eze, I.C.; Assaré, R.K.; Essé, C.; Koné, S.; Acka, F.; Laubhouet-Koffi, V.; Kouassi, D.; Bonfoh, B.; Utzinger, J.; et al. Prevalence of Schistosoma mono- and co-infections with multiple common parasites and associated risk factors and morbidity profile among adults in the Taabo health and demographic surveillance system, South-Central Côte d’Ivoire. Infect. Dis. Poverty 2022, 11, 3. [Google Scholar] [CrossRef] [PubMed]
- Deribew, K.; Yewhalaw, D.; Erko, B.; Mekonnen, Z. Urogenital schistosomiasis prevalence and diagnostic performance of urine filtration and urinalysis reagent strip in schoolchildren, Ethiopia. PLoS ONE 2022, 17, e0271569. [Google Scholar] [CrossRef]
- Degarege, A.; Animut, A.; Negash, Y.; Erko, B. Performance of urine reagent strips in detecting the presence and estimating the prevalence and intensity of Schistosoma haematobium infection. Microorganisms 2022, 10, 2062. [Google Scholar] [CrossRef]
- Phillips, A.E.; Ower, A.K.; Mekete, K.; Liyew, E.F.; Maddren, R.; Belay, H.; Chernet, M.; Anjulo, U.; Mengistu, B.; Salasibew, M.; et al. Association between water, sanitation, and hygiene access and the prevalence of soil-transmitted helminth and schistosome infections in Wolayita, Ethiopia. Parasites Vectors 2022, 15, 410. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, H.; Landeryou, T.; Chernet, M.; Liyew, E.F.; Wulataw, Y.; Getachew, B.; Difabachew, H.; Phillips, A.; Maddren, R.; Ower, A.; et al. Comparing the accuracy of two diagnostic methods for detection of light Schistosoma haematobium infection in an elimination setting in Wolaita Zone, South Western Ethiopia. PLoS ONE 2022, 17, e0267378. [Google Scholar] [CrossRef]
- Dejon-Agobé, J.C.; Adegnika, A.A.; Grobusch, M.P. Haematological changes in Schistosoma haematobium infections in school children in Gabon. Infection 2021, 49, 645–651. [Google Scholar] [CrossRef]
- Dejon-Agobé, J.C.; Edoa, J.R.; Honkpehedji, Y.J.; Zinsou, J.F.; Adégbitè, B.R.; Ngwese, M.M.; Mangaboula, A.; Lell, B.; Woldearegai, T.G.; Grobusch, M.P.; et al. Schistosoma haematobium infection morbidity, praziquantel effectiveness and reinfection rate among children and young adults in Gabon. Parasites Vectors 2019, 12, 577. [Google Scholar] [CrossRef]
- Dejon-Agobé, J.C.; Zinsou, J.F.; Honkpehedji, Y.J.; Ateba-Ngoa, U.; Edoa, J.-R.; Adegbite, B.R.; Mombo-Ngoma, G.; Agnandji, S.T.; Ramharter, M.; Kremsner, P.G.; et al. Schistosoma haematobium effects on Plasmodium falciparum infection modified by soil-transmitted helminths in school-age children living in rural areas of Gabon. PLoS Negl. Trop. Dis. 2018, 12, e0006663. [Google Scholar] [CrossRef]
- Joof, E.; Sanyang, A.M.; Camara, Y.; Sey, A.P.; Baldeh, I.; Jah, S.L.; Ceesay, S.J.; Sambou, S.M.; Sanyang, S.; Wade, C.M.; et al. Prevalence and risk factors of schistosomiasis among primary school children in four selected regions of The Gambia. PLoS Negl. Trop. Dis. 2021, 15, e0009380. [Google Scholar] [CrossRef]
- Camara, Y.; Sanneh, B.; Joof, E.; Sanyang, A.M.; Sambou, S.M.; Sey, A.P.; Sowe, F.O.; Jallow, A.W.; Jatta, B.; Lareef-Jah, S.; et al. Mapping survey of schistosomiasis and soil-transmitted helminthiases towards mass drug administration in The Gambia. PLoS Negl. Trop. Dis. 2021, 15, e0009462. [Google Scholar] [CrossRef] [PubMed]
- Dassah, S.; Asiamah, G.K.; Harun, V.; Appiah-Kubi, K.; Oduro, A.; Asoala, V.; Amenga-Etego, L. Urogenital schistosomiasis transmission, malaria and anemia among school-age children in Northern Ghana. Heliyon 2022, 8, e10440. [Google Scholar] [CrossRef]
- Tetteh-Quarcoo, P.B.; Forson, P.O.; Amponsah, S.K.; Ahenkorah, J.; Opintan, J.A.; Ocloo, J.E.Y.; Okine, E.N.; Aryee, R.; Afutu, E.; Anang, A.K.; et al. Persistent urogenital schistosomiasis and its associated morbidity in endemic communities within Southern Ghana: Suspected praziquantel resistance or reinfection? Med. Sci. 2020, 8, 10. [Google Scholar] [CrossRef] [PubMed]
- Asuming-Brempong, E.K.; Ayi, I.; van der Puije, W.; Gyan, B.A.; Larbi, I.A.; Ashong, Y.; Frempong, N.A.; Quartey, J.K.; Otchere, J.; Jones, F.M.; et al. Increased ShTAL1 IgE responses post-praziquantel treatment may be associated with a reduced risk to re-infection in a Ghanaian S. haematobium-endemic community. PLoS Negl. Trop. Dis. 2022, 16, e0010115. [Google Scholar] [CrossRef]
- Duah, E.; Kenu, E.; Adela, E.M.; Halm, H.A.; Agoni, C.; Kumi, R.O. Assessment of urogenital schistosomiasis among basic school children in selected communities along major rivers in the central region of Ghana. Pan Afr. Med. J. 2021, 40, 96. [Google Scholar]
- Sarpong-Baidoo, M.; Ofori, M.F.; Asuming-Brempong, E.K.; Kyei-Baafour, E.; Idun, B.K.; Owusu-Frimpong, I.; Amonoo, N.A.; Quarshie, Q.D.; Tettevi, E.J.; Osei-Atweneboana, M.Y. Associations of IL13 gene polymorphisms and immune factors with Schistosoma haematobium infection in schoolchildren in four schistosomiasis-endemic communities in Ghana. PLoS Negl. Trop. Dis. 2021, 15, e0009455. [Google Scholar] [CrossRef]
- Akosah-Brempong, G.; Attah, S.K.; Hinne, I.A.; Abdulai, A.; Addo-Osafo, K.; Appiah, E.L.; Osei, M.-M.; Afrane, Y.A. Infection of Plasmodium falciparum and helminths among school children in communities in Southern and Northern Ghana. BMC Infect. Dis. 2021, 21, 1259. [Google Scholar] [CrossRef] [PubMed]
- Jeza, V.T.; Mutuku, F.; Kaduka, L.; Mwandawiro, C.; Masaku, J.; Okoyo, C.; Kanyi, H.; Kamau, J.; Ng’ang’a, Z.; Kihara, J.H. Schistosomiasis, soil transmitted helminthiasis, and malaria co-infections among women of reproductive age in rural communities of Kwale County, coastal Kenya. BMC Public Health 2022, 22, 136. [Google Scholar] [CrossRef]
- Njenga, S.M.; Kanyi, H.M.; Mwatele, C.M.; Mukoko, D.A.; Bockarie, M.J.; Kelly-Hope, L.A. Integrated survey of helminthic neglected tropical diseases and comparison of two mosquito sampling methods for lymphatic filariasis molecular xenomonitoring in the River Galana area, Kilifi County, coastal Kenya. PLoS ONE 2022, 17, e0278655. [Google Scholar] [CrossRef]
- Kaiglová, A.; Changoma, M.J.S.; Špajdelová, J.; Jakubcová, D.; Bírová, K. Urinary schistosomosis in patients of rural medical health centers in Kwale county, Kenya. Helminthologia 2020, 57, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Rasoamanamihaja, C.F.; Rahetilahy, A.M.; Ranjatoarivony, B.; Dhanani, N.; Andriamaro, L.; Andrianarisoa, S.H.; Jourdan, P.M. Baseline prevalence and intensity of schistosomiasis at sentinel sites in Madagascar: Informing a national control strategy. Parasites Vectors 2016, 9, 50. [Google Scholar] [CrossRef] [PubMed]
- Kayuni, S.A.; Al-Harbi, M.H.; Makaula, P.; Injesi, B.; Mainga, B.; Lampiao, F.; Juziwelo, L.; LaCourse, E.J.; Stothard, J.R. Pathological abnormalities observed on ultrasonography among fishermen associated with male genital schistosomiasis (MGS) along the South Lake Malawi Shoreline in Mangochi District, Malawi. Trop. Med. Infect. Dis. 2022, 7, 169. [Google Scholar] [CrossRef]
- Kayuni, S.A.; O’ferrall, A.M.; Baxter, H.; Hesketh, J.; Mainga, B.; Lally, D.; Al-Harbi, M.H.; LaCourse, E.J.; Juziwelo, L.; Musaya, J.; et al. An outbreak of intestinal schistosomiasis, alongside increasing urogenital schistosomiasis prevalence, in primary school children on the shoreline of Lake Malawi, Mangochi District, Malawi. Infect. Dis. Poverty 2020, 9, 121. [Google Scholar] [CrossRef]
- Phillips, A.E.; Gazzinelli-Guimarães, P.H.; Aurelio, H.O.; Dhanani, N.; Ferro, J.; Nala, R.; Deol, A.; Fenwick, A. Urogenital schistosomiasis in Cabo Delgado, northern Mozambique: Baseline findings from the SCORE study. Parasites Vectors 2018, 11, 30. [Google Scholar] [CrossRef] [PubMed]
- Phillips, A.E.; Tohon, Z.; Dhanani, N.A.; Sofo, B.; Gnandou, I.; Sidikou, B.; Noma, A.G.; Madougou, B.; Alto, O.; Sebangou, H.; et al. Evaluating the impact of biannual school-based and community-wide treatment on urogenital schistosomiasis in Niger. Parasites Vectors 2020, 13, 557. [Google Scholar] [CrossRef]
- Alade, T.; Ta-Tang, T.-H.; Nassar, S.A.; Akindele, A.A.; Capote-Morales, R.; Omobami, T.B.; Berzosa, P. Prevalence of Schistosoma haematobium and intestinal helminth infections among Nigerian school children. Diagnostics 2023, 13, 759. [Google Scholar] [CrossRef]
- Onyekwere, A.; Rey, O.; Nwanchor, M.; Alo, M.; Angora, E.; Allienne, J.; Boissier, J. Prevalence and risk factors associated with urogenital schistosomiasis among primary school pupils in Nigeria. Parasite Epidemiol. Control 2022, 18, e00255. [Google Scholar] [CrossRef]
- Ajakaye, O.G.; Dagona, A.G.; Haladu, A.G.; Ombugadu, A.; Lapang, M.P.; Enabulele, E.E. Contrasting epidemiology of urogenital schistosomiasis among pastoral communities surrounding three Ramsar wetland in Nigeria. J. Parasit. Dis. 2022, 46, 637–642. [Google Scholar] [CrossRef] [PubMed]
- Balogun, J.B.; Adewale, B.; Balogun, S.U.; Lawan, A.; Haladu, I.S.; Dogara, M.M.; Aminu, A.U.; Caffrey, C.R.; De Koning, H.P.; Watanabe, Y.; et al. Prevalence and associated risk factors of urinary schistosomiasis among primary school pupils in the Jidawa and Zobiya Communities of Jigawa State, Nigeria. Ann. Glob. Health 2022, 88, 71. [Google Scholar] [CrossRef] [PubMed]
- Esiere, R.K.; Ibeneme, E.O.; Imalele, E.E.; Effanga, E.O.; Esiere, M.K.; Inyang-Etoh, P.C.; Alaribe, A.A.A. Morbidity indicators of urogenital schistosomosis and risk factors in school children in three Senatorial Districts of Cross River State, Nigeria. Ann. Parasitol. 2022, 68, 61–70. [Google Scholar]
- Olamiju, F.; Nebe, O.J.; Mogaji, H.; Marcus, A.; Amodu–Agbi, P.; Urude, R.O.; Apake, E.; Olamiju, O.; Okoronkwo, C.; Achu, I.; et al. Schistosomiasis outbreak during COVID-19 pandemic in Takum, Northeast Nigeria: Analysis of infection status and associated risk factors. PLoS ONE 2022, 17, e0262524. [Google Scholar] [CrossRef]
- Meulah, B.; Oyibo, P.; Bengtson, M.; Agbana, T.; Lontchi, R.A.L.; Adegnika, A.A.; Oyibo, W.; Hokke, C.H.; Diehl, J.C.; van Lieshout, L. Performance evaluation of the Schistoscope 5.0 for (Semi-)automated digital detection and quantification of Schistosoma haematobium eggs in urine: A field-based study in Nigeria. Am. J. Trop. Med. Hyg. 2022, 107, 1047–1054. [Google Scholar] [CrossRef]
- Opara, K.; Akomalafe, R.; Udoidung, N.; Afia, U.; Yaro, C.; Bassey, B. Urogenital schistosomiasis among primary school children in rural communities in Obudu, Southern Nigeria. Int. J. Matern. Child Health AIDS (IJMA) 2020, 10, 70–80. [Google Scholar] [CrossRef] [PubMed]
- Enabulele, E.E.; Platt, R.N.; Adeyemi, E.; Agbosua, E.; Aisien, M.S.; Ajakaye, O.G.; Ali, M.U.; Amaechi, E.C.; Atalabi, T.E.; Auta, T.; et al. Urogenital schistosomiasis in Nigeria post receipt of the largest single praziquantel donation in Africa. Acta Trop. 2021, 219, 105916. [Google Scholar] [CrossRef]
- Ojo, J.A.; Adedokun, S.A.; Akindele, A.A.; Olorunfemi, A.B.; Otutu, O.A.; Ojurongbe, T.A.; Thomas, B.N.; Velavan, T.P.; Ojurongbe, O. Prevalence of urogenital and intestinal schistosomiasis among school children in South-west Nigeria. PLoS Negl. Trop. Dis. 2021, 15, e0009628. [Google Scholar] [CrossRef]
- Gambo, S.; Ibrahim, M.; A Oyelami, O.; Raymond, B. A comparative study on the prevalence and intensity of urinary schistosomiasis among primary (formal) and almajiri (informal) school pupils in kura local government area of Kano State, Nigeria. Niger. Postgrad. Med. J. 2021, 28, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Igetei, J.; Boih, L.; Okaka, C. A survey of urinary schistosomiasis among school aged children of ten communities in South-South, Nigeria. J. Vector Borne Dis. 2021, 58, 63. [Google Scholar] [CrossRef]
- Noriode, R.M.; Idowu, E.T.; Otubanjo, O.A.; Mafe, M.A. Urinary schistosomiasis in school aged children of two rural endemic communities in Edo State, Nigeria. J. Infect. Public Health 2018, 11, 384–388. [Google Scholar] [CrossRef] [PubMed]
- Lund, A.J.; Sokolow, S.H.; Jones, I.J.; Wood, C.L.; Ali, S.; Chamberlin, A.; Sy, A.B.; Sam, M.M.; Jouanard, N.; Schacht, A.-M.; et al. Exposure, hazard, and vulnerability all contribute to Schistosoma haematobium re-infection in northern Senegal. PLoS Negl. Trop. Dis. 2021, 15, e0009806. [Google Scholar] [CrossRef]
- Léger, E.; Borlase, A.; Fall, C.B.; Diouf, N.D.; Diop, S.D.; Yasenev, L.; Catalano, S.; Thiam, C.T.; Ndiaye, A.; Emery, A.; et al. Prevalence and distribution of schistosomiasis in human, livestock, and snail populations in northern Senegal: A One Health epidemiological study of a multi-host system. Lancet Planet. Health 2020, 4, e330–e342. [Google Scholar] [CrossRef]
- Mogeni, P.; Vandormael, A.; Cuadros, D.; Appleton, C.; Tanser, F. Impact of community piped water coverage on re-infection with urogenital schistosomiasis in rural South Africa. Elife 2020, 9. [Google Scholar] [CrossRef]
- Zulu, S.G.; Kjetland, E.F.; Gundersen, S.G.; Taylor, M. Prevalence and intensity of neglected tropical diseases (schistosomiasis and soil-transmitted helminths) amongst rural female pupils in Ugu district, KwaZulu-Natal, South Africa. S. Afr. J. Infect. Dis. 2020, 35, 1–7. [Google Scholar] [CrossRef]
- Senkwe, M.N.; Berta, K.K.; Yibi, S.M.; Sube, J.; Bidali, A.; Abe, A.; Onyeze, A.; Ajo, J.P.H.; Pascale, J.R.; Ndenzako, F.; et al. Prevalence and factors associated with transmission of schistosomiasis in school-aged children in South Sudan: A cross-sectional study. Pan Afr. Med. J. 2022, 42, 2. [Google Scholar]
- Cha, S.; Hong, S.T.; Lee, J.S.; Jeong, H.G.; Kwon, I.S.; Saed, A.A.W.; Elhag, M.S.; Ismail, H.A.H.A.; Amin, M.; Lee, Y.H. Comparison of the changes in the prevalence and intensity of Schistosoma haematobium infection between high and low prevalence areas of White Nile State, Sudan. Korean J. Parasitol. 2020, 58, 421–430. [Google Scholar] [CrossRef]
- Cha, S.; Elhag, M.S.; Lee, Y.-H.; Cho, D.-S.; Ismail, H.A.H.A.; Hong, S.-T. Epidemiological findings and policy implications from the nationwide schistosomiasis and intestinal helminthiasis survey in Sudan. Parasites Vectors 2019, 12, 429. [Google Scholar] [CrossRef]
- Mazigo, H.D.; Mwingira, U.J.; Zinga, M.M.; Uisso, C.; Kazyoba, P.E.; Kinung’hi, S.M.; Mutapi, F. Urogenital schistosomiasis among pre-school and school aged children in four districts of north western Tanzania after 15 years of mass drug administration: Geographical prevalence, risk factors and performance of haematuria reagent strips. PLoS Negl. Trop. Dis. 2022, 16, e0010834. [Google Scholar] [CrossRef]
- Ngassa, N.; Zacharia, A.; Lupenza, E.T.; Mushi, V.; Ngasala, B. Urogenital schistosomiasis: Prevalence, knowledge and practices among women of reproductive age in Northern Tanzania. IJID Reg. 2023, 6, 15–23. [Google Scholar] [CrossRef]
- Kajembe, V.R.; Gasarasi, D.B.; Tarimo, D.S.; Lushina, M.; Sylvester, B. Prevalence and factors associated with persistent transmission of Schistosoma haematobium among primary school children after five rounds of mass drug administration using praziquantel: A cross sectional study in Mkuranga district, Tanzania. Trop. Dr. 2022, 52, 526–531. [Google Scholar] [CrossRef]
- Mushi, V.; Zacharia, A.; Shao, M.; Mubi, M.; Tarimo, D. Persistence of Schistosoma haematobium transmission among school children and its implication for the control of urogenital schistosomiasis in Lindi, Tanzania. PLoS ONE 2022, 17, e0263929. [Google Scholar] [CrossRef]
- Mushi, V.; Zacharia, A.; Shao, M.; Mubi, M.; Tarimo, D. Prevalence and risk factors of urogenital schistosomiasis among under-fives in Mtama District in the Lindi region of Tanzania. PLoS Negl. Trop. Dis. 2022, 16, e0010381. [Google Scholar] [CrossRef]
- Maseke, L.S.; Mushi, V.; Tarimo, D.; Kwesigabo, G.; Mazigo, H. Adolescents and young adults excluded from preventive chemotherapy for schistosomiasis control in Northern Tanzania: Are they at risk and reservoirs of infection? Prevalence and determinants of transmission in Northern Tanzania. IJID Reg. 2022, 4, 111–119. [Google Scholar] [CrossRef]
- Nazareth, L.C.; Lupenza, E.T.; Zacharia, A.; Ngasala, B.E. Urogenital schistosomiasis prevalence, knowledge, practices and compliance to MDA among school-age children in an endemic district, southern East Tanzania. Parasite Epidemiol. Control 2022, 18, e00257. [Google Scholar] [CrossRef]
- Mazigo, H.D.; Zinga, M.M.; Kepha, S.; Yard, E.; McRee-Mckee, K.; Kabona, G.; Ngoma, D.D.; Nshala, A. Precision and geographical prevalence mapping of schistosomiasis and soil-transmitted helminthiasis among school-aged children in selected districts of north-western Tanzania. Parasites Vectors 2022, 15, 492. [Google Scholar] [CrossRef]
- Rite, E.E.; Kapalata, S.N.; Munisi, D.Z. Prevalence, intensity, and factors associated with urogenital schistosomiasis among women of reproductive age in Mbogwe District Council, Geita Region, Tanzania. BioMed Res. Int. 2020, 2020, 5923025. [Google Scholar] [CrossRef]
- Manz, K.M.; Kroidl, I.; Clowes, P.; Gerhardt, M.; Nyembe, W.; Maganga, L.; Assisya, W.; Ntinginya, N.E.; Berger, U.; Hoelscher, M.; et al. Schistosoma haematobium infection and environmental factors in Southwestern Tanzania: A cross-sectional, population-based study. PLoS Negl. Trop. Dis. 2020, 14, e0008508. [Google Scholar] [CrossRef]
- Knopp, S.; Ame, S.M.; Hattendorf, J.; Ali, S.M.; Khamis, I.S.; Bakar, F.; Khamis, M.A.; Person, B.; Kabole, F.; Rollinson, D. Urogenital schistosomiasis elimination in Zanzibar: Accuracy of urine filtration and haematuria reagent strips for diagnosing light intensity Schistosoma haematobium infections. Parasites Vectors 2018, 11, 552. [Google Scholar] [CrossRef]
- Kapanga, S.; Mulemena, J.A.; Kamvuma, K.; Phiri, C.N.; Chanda, W. Prevalence and correlates of urogenital schistosomiasis in school-going children at Maramba Primary School in Livingstone District, Zambia. Infect. Dis. Now 2022, 52, 456–458. [Google Scholar] [CrossRef]
- Tembo, R.; Muleya, W.; Yabe, J.; Kainga, H.; Nalubamba, K.S.; Zulu, M.; Mwaba, F.; Saad, S.A.; Kamwela, M.; Mukubesa, A.N.; et al. Prevalence and molecular identification of Schistosoma haematobium among children in Lusaka and Siavonga Districts, Zambia. Trop. Med. Infect. Dis. 2022, 7, 239. [Google Scholar] [CrossRef]
- Zhang, L.-J.; Mwanakasale, V.; Xu, J.; Sun, L.-P.; Yin, X.-M.; Zhang, J.-F.; Hu, M.-C.; Si, W.-M.; Zhou, X.-N. Diagnostic performance of two specific Schistosoma japonicum immunological tests for screening Schistosoma haematobium in school children in Zambia. Acta Trop. 2019, 202, 105285. [Google Scholar] [CrossRef]
- Kasambala, M.; Mduluza, T.; Vengesai, A.; Mduluza-Jokonya, T.; Jokonya, L.; Midzi, H.; Makota, R.B.; Mutemeri, A.; Maziti, E.; Dube-Marimbe, B.; et al. Effect of Schistosoma haematobium infection on the cognitive functions of preschool age children and benefits of treatment from an endemic area in Zimbabwe. BMC Infect. Dis. 2022, 22, 809. [Google Scholar] [CrossRef]
- Murenjekwa, W.; Makasi, R.; Ntozini, R.; Chasekwa, B.; Mutasa, K.; Moulton, L.H.; Tielsch, J.M.; Humphrey, J.H.; Smith, L.E.; Prendergast, A.; et al. Determinants of urogenital schistosomiasis among pregnant women and its association with pregnancy outcomes, neonatal deaths, and child growth. J. Infect. Dis. 2019, 223, 1433–1444. [Google Scholar] [CrossRef]
- Mduluza-Jokonya, T.L.; Vengesai, A.; Midzi, H.; Kasambala, M.; Jokonya, L.; Naicker, T.; Mduluza, T. Algorithm for diagnosis of early Schistosoma haematobium using prodromal signs and symptoms in pre-school age children in an endemic district in Zimbabwe. PLoS Negl. Trop. Dis. 2021, 15, e0009599. [Google Scholar] [CrossRef]
- Marume, A.; Vengesai, A.; Mann, J.; Mduluza, T. Interleukin-10 and tumour necrosis factor alpha promoter region polymorphisms and susceptibility to urogenital schistosomiasis in young Zimbabwean children living in Schistosoma haematobium endemic regions. S. Afr. J. Infect. Dis. 2020, 35, 8. [Google Scholar] [CrossRef]
- Midzi, N.; Bärenbold, O.; Manangazira, P.; Phiri, I.; Mutsaka-Makuvaza, M.J.; Mhlanga, G.; Utzinger, J.; Vounatsou, P. Accuracy of different diagnostic techniques for Schistosoma haematobium to estimate treatment needs in Zimbabwe: Application of a hierarchical Bayesian egg count model. PLoS Negl. Trop. Dis. 2020, 14, e0008451. [Google Scholar] [CrossRef]
- Mduluza-Jokonya, T.L.; Naicker, T.; Kasambala, M.; Jokonya, L.; Vengesai, A.; Midzi, H.; Choto, E.; Musonza, K.; Rusankaniko, S.; Sibanda, E.; et al. Clinical morbidity associated with Schistosoma haematobium infection in pre-school age children from an endemic district in Zimbabwe. Trop. Med. Int. Health 2020, 25, 1110–1121. [Google Scholar] [CrossRef]
- Aula, O.P.; McManus, D.P.; Jones, M.K.; Gordon, C.A. Schistosomiasis with a focus on Africa. Trop. Med. Infect. Dis. 2021, 6, 109. [Google Scholar] [CrossRef]
- Kalinda, C.; Mindu, T.; Chimbari, M.J. A systematic review and meta-analysis quantifying schistosomiasis infection burden in pre-school aged children (PreSAC) in sub-Saharan Africa for the period 2000–2020. PLoS ONE 2020, 15, e0244695. [Google Scholar] [CrossRef]
- A Ochodo, E.; Gopalakrishna, G.; Spek, B.; Reitsma, J.B.; Van Lieshout, L.; Polman, K.; Lamberton, P.; Bossuyt, P.M.; Leeflang, M.M. Circulating antigen tests and urine reagent strips for diagnosis of active schistosomiasis in endemic areas. Cochrane Database Syst. Rev. 2015, 1–292. [Google Scholar] [CrossRef]
- Osei, E.; Nkambule, S.J.; Vezi, P.N.; Mashamba-Thompson, T.P. Systematic review and meta-analysis of the diagnostic accuracy of mobile-linked point-of-care diagnostics in Sub-Saharan Africa. Diagnostics 2021, 11, 1081. [Google Scholar] [CrossRef]
- Armstrong, M.; Harris, A.R.; D’ambrosio, M.V.; Coulibaly, J.T.; Essien-Baidoo, S.; Ephraim, R.K.D.; Andrews, J.R.; Bogoch, I.I.; Fletcher, D.A. Point-of-care sample preparation and automated quantitative detection of Schistosoma haematobium using mobile phone microscopy. Am. J. Trop. Med. Hyg. 2022, 106, 1442–1449. [Google Scholar] [CrossRef]
- Oyibo, P.; Jujjavarapu, S.; Meulah, B.; Agbana, T.; Braakman, I.; van Diepen, A.; Bengtson, M.; van Lieshout, L.; Oyibo, W.; Vdovine, G.; et al. Schistoscope: An automated microscope with artificial intelligence for detection of Schistosoma haematobium eggs in resource-limited settings. Micromachines 2022, 13, 643. [Google Scholar] [CrossRef]
- Grolimund, C.M.; Bärenbold, O.; Hatz, C.F.; Vennervald, B.J.; Mayombana, C.; Mshinda, H.; Utzinger, J.; Vounatsou, P. Infection intensity-dependent accuracy of reagent strip for the diagnosis of Schistosoma haematobium and estimation of treatment prevalence thresholds. PLoS Negl. Trop. Dis. 2022, 16, e0010332. [Google Scholar] [CrossRef]
- King, C.H.; Bertsch, D. Meta-analysis of urine heme dipstick diagnosis of Schistosoma haematobium infection, including low-prevalence and previously-treated populations. PLoS Negl. Trop. Dis. 2013, 7, e2431. [Google Scholar] [CrossRef] [PubMed]
- Ngasala, B.; Juma, H.; Mwaiswelo, R.O. The usefulness of indirect diagnostic tests for Schistosoma haematobium infection after repeated rounds of mass treatment with praziquantel in Mpwapwa and Chakechake districts in Tanzania. Int. J. Infect. Dis. 2019, 90, 132–137. [Google Scholar] [CrossRef]
- Gobbi, F.; Tamarozzi, F.; Buonfrate, D.; van Lieshout, L.; Bisoffi, Z.; Bottieau, E. New Insights on acute and chronic schistosomiasis: Do we need a redefinition? Trends Parasitol. 2020, 36, 660–667. [Google Scholar] [CrossRef]
- Silva-Moraes, V.; Shollenberger, L.M.; Siqueira, L.M.V.; Castro-Borges, W.; Harn, D.A.; Grenfell, R.; Rabello, A.L.T.; Coelho, P.M.Z. Diagnosis of Schistosoma mansoni infections: What are the choices in Brazilian low-endemic areas? Memórias Inst. Oswaldo Cruz 2019, 114, e180478. [Google Scholar] [CrossRef]
- Mangano, V.D.; Bianchi, C.; Ouedraogo, M.; Kabore, Y.; Corran, P.; Silva, N.; Sirima, S.B.; Nebie, I.; Bruschi, F.; Modiano, D. Antibody response to Schistosoma haematobium and other helminth species in malaria-exposed populations from Burkina Faso. Acta Trop. 2020, 205, 105381. [Google Scholar] [CrossRef]
- Song, H.B.; Kim, J.; Jin, Y.; Lee, J.S.; Jeoung, H.G.; Lee, Y.H.; Saeed, A.A.W.; Hong, S.-T. Comparison of ELISA and urine Mmicroscopy for diagnosis of Schistosoma haematobium infection. J. Korean Med. Sci. 2018, 33, e238. [Google Scholar] [CrossRef]
- Hinz, R.; Schwarz, N.G.; Hahn, A.; Frickmann, H. Serological approaches for the diagnosis of schistosomiasis—A review. Mol. Cell. Probes 2017, 31, 2–21. [Google Scholar] [CrossRef]
- Sheele, J.M.; Kihara, J.H.; Baddorf, S.; Byrne, J.; Ravi, B. Evaluation of a novel rapid diagnostic test for Schistosoma haematobium based on the detection of human immunoglobulins bound to filtered Schistosoma haematobium eggs. Trop. Med. Int. Health 2013, 18, 477–484. [Google Scholar] [CrossRef]
- Esiere, R.K.; Ibeneme, E.O.; Effanga, E.O.; Imalele, E.E.; Esiere, M.K.; Inyang-Etoh, P.C.; Alaribe, A.A.A. Detecting Schistosoma haematobium infection by microscopy and polymerase chain reaction (PCR) in school children in three senatorial districts of Cross River State, Nigeria. J. Parasit. Dis. 2021, 46, 272–279. [Google Scholar] [CrossRef]
- Sow, D.; Sylla, K.; Dieng, N.M.; Senghor, B.; Gaye, P.M.; Fall, C.B.; Goumballa, N.; Diallo, A.; Ndiaye, J.L.A.; Parola, P.; et al. Molecular diagnosis of urogenital schistosomiasis in pre-school children, school-aged children and women of reproductive age at community level in central Senegal. Parasites Vectors 2023, 16, 43. [Google Scholar] [CrossRef]
- Archer, J.; Barksby, R.; Pennance, T.; Rostron, P.; Bakar, F.; Knopp, S.; Allan, F.; Kabole, F.; Ali, S.M.; Ame, S.M.; et al. Analytical and clinical assessment of a portable, isothermal recombinase polymerase amplification (RPA) assay for the molecular diagnosis of urogenital schistosomiasis. Molecules 2020, 25, 4175. [Google Scholar] [CrossRef]
- Gandasegui, J.; Fernández-Soto, P.; Carranza-Rodríguez, C.; Pérez-Arellano, J.L.; Vicente, B.; López-Abán, J.; Muro, A. The rapid-heat LAMPellet method: A potential diagnostic method for human urogenital schistosomiasis. PLoS Negl. Trop. Dis. 2015, 9, e0003963. [Google Scholar] [CrossRef]
- WHO. Ultrasound in Schistosomiasis: A Practical Guide to the Standard Use of Ultrasonography for Assessment of Schistosomiasis-Related Morbidity: Second International Workshop, Niamey, Niger, 22–26 October 1996; WHO: Geneva, Switzerland, 2000. [Google Scholar]
- Kim, M.J.; Hong, S.-T.; Jin, Y.; Ryu, K.; Kim, S.H.; Saeed, A.A.W.; Jeoung, H.G.; Lee, Y.H. Significance of echogenic snow sign as an ultrasonography finding for diagnosis of urogenital schistosomiasis. Am. J. Trop. Med. Hyg. 2016, 95, 842–848. [Google Scholar] [CrossRef]
- Ngome, O.; Rohacek, M. Point-of-care ultrasound: A useful diagnostic tool in Africa. Praxis 2020, 109, 608–614. [Google Scholar] [CrossRef]
- Bocanegra, C.; Pintar, Z.; Moreno, M.; Aznar, M.L.; Serres, X.; Sikaleta, N.; Salvador, F.; Nindia, A.; Molina, I.; Mendioroz, J.; et al. Ultrasound evolution of pediatric urinary schistosomiasis after treatment with praziquantel in a highly endemic area. Am. J. Trop. Med. Hyg. 2018, 99, 1011–1017. [Google Scholar] [CrossRef]
- Santos, J.; Chaves, J.; Araújo, H.; Vale, N.; Costa, J.M.; Brindley, P.J.; Lopes, C.; Naples, J.; Shiff, C.; Dupret, J.; et al. Comparison of findings using ultrasonography and cystoscopy in urogenital schistosomiasis in a public health centre in rural Angola. S. Afr. Med. J. 2015, 105, 312–315. [Google Scholar] [CrossRef]
- Cozzi, D.; Bertelli, E.; Savi, E.; Verna, S.; Zammarchi, L.; Tilli, M.; Rinaldi, F.; Pradella, S.; Agostini, S.; Miele, V. Ultrasound findings in urogenital schistosomiasis: A pictorial essay. J. Ultrasound 2019, 23, 195–205. [Google Scholar] [CrossRef]



| Countries | No. of Treated People | No. of Treated SAC | SAC Coverage (%) | National Coverage (%) |
|---|---|---|---|---|
| Angola | 2,025,995 | 2,025,995 | 62.6 | 40.0 |
| Benin | 755,772 | 755,772 | 79.5 | 28.6 |
| Botswana | 364,502 | 364,502 | 86.3 | 25.7 |
| Burkina Faso | 1,154,320 | 870,624 | 89.9 | 89.9 |
| Burundi | 1,681,868 | 1,681,868 | 105.5 | 96.5 |
| Cameroon | 2,766,864 | 2,766,864 | 83.7 | 51.1 |
| Central African Republic | 106,940 | 106,940 | 68.4 | 6.5 |
| Chad | 1,887,341 | 1,887,341 | 91.3 | 45.5 |
| Congo | 79,859 | 79,859 | 70.2 | 18.5 |
| Côte d’Ivoire | 2,328,781 | 1,904,844 | 85.4 | 56.7 |
| Democratic Republic of Congo | 11,885,901 | 11,146,568 | 93.4 | 67.8 |
| Egypt (2020) | 2,897,891 | 1,448,102 | 98.9 | 98.8 |
| Eritrea | 374,853 | 168,590 | 95.3 | 82.8 |
| Ethiopia | 3,562,162 | 3,071,245 | 84.2 | 23.0 |
| Gambia | 63,011 | 37,607 | 46.6 | 13.6 |
| Ghana | 2,792,184 | 2,792,184 | 79.5 | 24.1 |
| Guinea | 2,192,543 | 2,192,543 | 91.8 | 45.4 |
| Guinea-Bissau | 83,515 | 83,515 | 99.8 | 50.7 |
| Kenya | 3,165,901 | 1,374,465 | 95.2 | 80.0 |
| Liberia | 489,715 | 489,715 | 84.8 | 35.3 |
| Madagascar (2020) | 2,705,026 | 2,676,453 | 80.4 | 27.3 |
| Malawi | 2,780,558 | 1,431,603 | 82.6 | 30.6 |
| Mali | 3,977,709 | 3,896,892 | 93.9 | 42.3 |
| Mauritania | 141,370 | 141,370 | 86.7 | 15.2 |
| Mozambique | 1,125,297 | 864,811 | 95.6 | 6.5 |
| Namibia (2019) | 143,383 | 143,383 | 70.7 | 57.4 |
| Niger | 6,943,175 | 2,748,014 | 92.8 | 65.2 |
| Nigeria | 1,810,420 | 1,433,132 | 49.0 | 6.6 |
| Rwanda | 2,856,299 | 1,027,010 | 98.4 | 94.8 |
| Sao Tome and Principe | 17,322 | 17,322 | 90.2 | 42.8 |
| Senegal | 1,845,926 | 1,482,743 | 95.6 | 64.1 |
| Sierra Leone (2020) | 1,071,836 | 678,929 | 61.1 | 35.7 |
| Somalia (2020) | 2,549,993 | 2,549,993 | 113.7 | 89.6 |
| South Sudan | 12,461 | 8,067 | 66.1 | 0.4 |
| Sudan (2019) | 3,058,201 | 2,483,677 | 55.0 | 37.9 |
| Togo | 463,782 | 174,469 | 94.6 | 11.3 |
| Uganda (2020) | 5,301,075 | 2,628,166 | 84.1 | 53.0 |
| Tanzania | 9,374,223 | 8,209,186 | 82.2 | 51.6 |
| Zambia | 1,925,614 | 1,925,614 | 80.0 | 43.8 |
| Zimbabwe (2020) | 404,006 | 317,617 | 79.0 | 11.8 |
| Countries | Studies | Subjects | No. of Examined | Positive Rate, % by | Year of Survey | Year of Publish | References | ||
|---|---|---|---|---|---|---|---|---|---|
| UM | MicH | MacH | |||||||
| Angola | Mapping | SAC | 31,938 | 12.6 | 2018-9 | 2022 | [5] | ||
| Cross-sectional | SAC | 17,093 | 5.0 | 13.6 | 2022 | [6] | |||
| Cross-sectional | SAC | 1283 | 61.2 | 65.7 | 17.1 | 2013-4 | 2015 | [7] | |
| Benin | Mapping | SAC | 19,250 | 17.56 | 2013-5 | 2019 | [8] | ||
| Burkina Faso | Cross-sectional | SAC | 228 | 0 | 2021 | [9] | |||
| Cameroon | Cross-sectional | Men | 89 | 31.4 | 2022 | [10] | |||
| Cross-sectional | SAC | 389 | 32.6 | 24.4 | 2018 | 2021 | [11] | ||
| Cross-sectional | Community residents | 778 | 31.5 | 24.9 | 2018 | 2021 | [12] | ||
| Cross-sectional | Adults | 509 | 18.7 | 16.5 | 2019 | 2021 | [13] | ||
| Chad | Cross-sectional | SAC | 11,832 | 100 | 55 | 2015-9 | 2022 | [14] | |
| Cross-sectional | SAC + Ad | 258 | 39.2 | 58.9 | 2019 | 2022 | [15] | ||
| Côte d’Ivoire | Cross-sectional | SAC | 170 | 20.6 | 2023 | [16] | |||
| Cohort/ | SAC + Ad | 12,239 | 13.1 | 2015-9 | 2022 | [17] | |||
| Cross-sectional | Ad | 901 | 1.0 | 2022 | [18] | ||||
| Ethiopia | Cross-sectional | SAC | 1171 | 12.2 | 22.5 | 2022 | [19] | ||
| Cross-sectional | SAC | 1288 | 31.6 | 32.1 | 2021-2 | 2022 | [20] | ||
| Mapping | SAC | 15,133 | 0.13 | 2.8 | 2018-9 | 2022 | [21] | ||
| Cross-sectional | SAC + Ad | 12,102 | 0.2 | 2.4 | 2022 | [22] | |||
| Gabon | Cross-sectional | SAC | 451 | 26.3 | 2021 | [23] | |||
| Longitudinal | SAC | 328 | 43 | 2019 | [24] | ||||
| Longitudinal | SAC | 739 | 30.3 | 2012-4 | 2018 | [25] | |||
| Gambia | Cross-sectional | SAC | 2016 | 10.2 | 18.0 | 0.5 | 2015 | 2021 | [26] |
| Mapping | SAC | 10,434 | 4.2 | 2014 | 2021 | [27] | |||
| Ghana | Cross-sectional | SAC | 336 | 12.8 | 2022 | [28] | |||
| Cross-sectional | SAC | 520 | 6.5 | 2022 | [29] | ||||
| Cross-sectional | SAC + Ad | 114 | 22.8 | 2022 | [30] | ||||
| Cross-sectional | SAC | 309 | 10.4 | 2021 | [31] | ||||
| Cross-sectional | SAC | 469 | 21.1 | 2021 | [32] | ||||
| Cross-sectional | SAC + PSAC | 493 | 1.6 | 2021 | [33] | ||||
| Kenya | Cross-sectional | Women | 534 | 3.8 | 2018 | 2022 | [34] | ||
| Cross-sectional | SAC + Ad | 897 | 3.2 | [35] | |||||
| Cross-sectional | Health center visitors | 451 | 15.1 | 2018 | 2020 | [36] | |||
| Madagascar | Cross-sectional | SAC | 1958 | 30.5 | 2015 | 2016 | [37] | ||
| Malawi | Cross-sectional | Fisherman | 129 | 20.9 | 2022 | [38] | |||
| Cross-sectional | SAC | 240 | 24.0 | 2019 | 2020 | [39] | |||
| Mozambique | Cross-sectional | SAC | 19,039 | 60.4 | 2011 | 2018 | [40] | ||
| Niger | Cross-sectional | SAC + Ad | 48,192 | 15.7 | 2011 | 2020 | [41] | ||
| 54,451 | 8.8 | 2015 | 2020 | [41] | |||||
| Nigeria | Cross-sectional | SAC | 250 | 15.2 | 2023 | [42] | |||
| Cross-sectional | SAC | 5514 | 7.1 | 2019 | 2022 | [43] | |||
| Cross-sectional | Pastoral community | 34.2 | 2.5 | 2022 | [44] | ||||
| Cross-sectional | SAC | 279 | 67.4 | 29.7 | 2022 | [45] | |||
| Cross-sectional | SAC | 777 | 1.7 | 11.6 | 2015-6 | 2022 | [46] | ||
| Cross-sectional | SAC + Ad | 432 | 28.9 | 2020 | 2022 | [47] | |||
| Cross-sectional | SAC | 487 | 34.1 | 2022 | [48] | ||||
| Cross-sectional | SAC | 1113 | 13.7 | 13.7 | 2021 | [49] | |||
| Cross-sectional | SAC | 2023 | 10.4 | 2021 | [50] | ||||
| Cross-sectional | SAC | 466 | 19.1 | 2021 | [51] | ||||
| Cross-sectional | SAC | 400 | 49.2 | 83.0 | 2021 | [52] | |||
| Cross-sectional | SAC | 400 | 17.3 | 22.0 | 2021 | [53] | |||
| Cross-sectional | SAC | 251 | 65.3 | 2018 | [54] | ||||
| Senegal | Cross-sectional | Sac | 821 | 66.7 | 2018 | 2021 | [55] | ||
| Cross-sectional | SAC Ad | 1285 300 | 54.2 32.0 | 2016-8 | 2020 | [56] | |||
| South Africa | Cohort | SAC | 1976 | 16.9 | 2007-8 | 2020 | [57] | ||
| Cross-sectional | SAC | 970 | 32.2 | 2010 | 2020 | [58] | |||
| South Sudan | Cross-sectional | SAC | 13,286 | 3.7 | 2016-9 | 2022 | [59] | ||
| Sudan | Longitudinal | SAC | 9.1/35.2 | 2020 | [60] | ||||
| Mapping | SAC | 100,726 | 5.2 | 2016-7 | 2019 | [61] | |||
| Tanzania | Cross-sectional | SAC + PSAC | 20,389 | 7.4 | 9.3 | 0.3 | 2019 | 2022 | [62] |
| Hospital | Women | 216 | 2.3 | 2021 | 2022 | [63] | |||
| Cross-sectional | SAC | 396 | 5.8 | 2022 | [64] | ||||
| Cross-sectional | SAC | 649 | 52.7 | 46.2 | 13.1 | 2021 | 2022 | [65] | |
| Cross | PSAC | 385 | 16.9 | 17.9 | 6 | 2021 | 2022 | [66] | |
| Cross-sectional | Adolescents | 433 | 15.9 | 3.0 | 2022 | [67] | |||
| Cross-sectional | SAC | 1288 | 31.6 | 32.1 | 2021-2 | 2022 | [68] | ||
| Cross-sectional | SAC | 389 | 6.9 | 9.5 | 1.3 | 2022 | [69] | ||
| Cross-sectional | SAC+ PSAC | 1560 | 0.83 | 0.9 | 2021 | [70] | |||
| Cross-sectional | Women RA | 426 | 4.5 | 2019 | 2020 | [71] | |||
| Mapping | Population-based subjects | 17,280 | 5.3 | 2006-7 | 2020 | [72] | |||
| Cross-sectional | SAC Adult | 39,207 18,155 | 5.4 2.7 | 6.5 | 2013-6 | 2018 | [73] | ||
| Zambia | Cross-sectional | SAC | 173 | 3.5 | 2022 | [74] | |||
| Cross-sectional | SAC | 421 | 9.7 | 2022 | [75] | ||||
| Cross-sectional | SAC | 243,148 | 61 | 2020 | [76] | ||||
| Zimbabwe | Cross-sectional | PSAC | 136 | 22.1 | 2022 | [77] | |||
| Cross-sectional | Pregnant women | 4437 | 10.6 | 24.4 | 2021 | [78] | |||
| Longitudinal | PSAC | 204 | 19.6 | 2019 | 2021 | [79] | |||
| Cross-sectional | SAC | 361 | 26.8 | 2020 | [80] | ||||
| Cross-sectional | SAC | 12,656 | 17.6 | 2010-1 | 2020 | [81] | |||
| Cross-sectional | PSAC | 416 | 35.1 | 2020 | [82] | ||||
| Diagnosis | Advantages | Limitations | Cost–Benefit Analysis |
|---|---|---|---|
| Urine microscopy | Standard method Familiar in most endemic areas High specificity (96.6–100%) | Low sensitivity (25.9–46.4%) Very low sensitivity in ultra-light infections (<10%) | Good Cheap cost Feasible |
| CCA/CAA | High sensitivity (89%) and moderate specificity (55%) for intestinal schistosomiasis Good for field surveys in areas with ultra-light infection | Reliable for S. mansoni infections Not acceptable for diagnosis of UGS Cross reactions with other types of schistosomiasis Limited supply of the kit | Moderate Moderate cost Most feasible in the field setting for IS |
| Urine reagent strips for microhematuria | High sensitivity (71–79%) High specificity (84–90%) Easy to implement | Not standard, supplementary to UM | Good Cheap cost Most feasible in the field setting for UGS |
| Gross screening of macrohematuria | Cheap Easy High specificity Reflects acute infections | Low sensitivity (<10%) with numerous false-negative cases | Most cheap |
| Serology (ELISA) | High sensitivity (87–96%) Optimal in non-endemic areas | Low specificity (31–32%) Not practical in the endemic field setting in SSA | Moderate Moderate cost Lab facilities required |
| Molecular diagnosis (PCR, qPCR, and LAMP) | High sensitivity (>90%) High specificity (>95%) Optimal for setting gold standard Expensive reagents and high technique | Well-established lab support, not practical in the field setting Feasible for small-scale surveys | Poor Expensive method and feasible only in lab |
| Ultrasound | High sensitivity (>80%) High specificity (>80%) Morbidity information of UGS on site Detection of other co-morbidities | Experienced sonographer Expensive sonograph Feasible for small-scale surveys | Poor Expensive method Feasible with a portable sonograph |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hong, S.-T. Review of Recent Prevalence of Urogenital Schistosomiasis in Sub-Saharan Africa and Diagnostic Challenges in the Field Setting. Life 2023, 13, 1670. https://doi.org/10.3390/life13081670
Hong S-T. Review of Recent Prevalence of Urogenital Schistosomiasis in Sub-Saharan Africa and Diagnostic Challenges in the Field Setting. Life. 2023; 13(8):1670. https://doi.org/10.3390/life13081670
Chicago/Turabian StyleHong, Sung-Tae. 2023. "Review of Recent Prevalence of Urogenital Schistosomiasis in Sub-Saharan Africa and Diagnostic Challenges in the Field Setting" Life 13, no. 8: 1670. https://doi.org/10.3390/life13081670