
Treating COVID-19: Targeting the Host Response, Not the Virus
Independent Researcher, 57 Chemin du Lavoir, 01630 Sergy, France
Life 2023, 13(3), 712; https://doi.org/10.3390/life13030712
Submission received: 20 December 2022
/
Revised: 19 January 2023
/
Accepted: 31 January 2023
/
Published: 6 March 2023
(This article belongs to the Special Issue COVID-19 and Long-COVID-19: Pathogenesis, Clinical Manifestation, and Therapeutic Options: 2nd Edition)
Abstract
:In low- and middle-income countries (LMICs), inexpensive generic drugs like statins, ACE inhibitors, and ARBs, especially if used in combination, might be the only practical way to save the lives of patients with severe COVID-19. These drugs will already be available in all countries on the first pandemic day. Because they target the host response to infection instead of the virus, they could be used to save lives during any pandemic. Observational studies show that inpatient statin treatment reduces 28–30-day mortality but randomized controlled trials have failed to show this benefit. Combination treatment has been tested for antivirals and dexamethasone but, with the exception of one observational study in Belgium, not for inexpensive generic drugs. Future pandemic research must include testing combination generic drug treatments that could be used in LMICs.
1. Introduction
The COVID-19 pandemic has had a devastating impact on global health. As of January 2022, estimates of excess deaths exceeded 20 million worldwide [1]. The pandemic’s impact on social and economic life throughout the world has been enormous [2,3]. Remarkably, the one bright spot has been the rapid development of COVID vaccines [4]. They are estimated to have saved tens of millions of lives [5]. Despite a call for vaccine equity from the World Health Organization (WHO) [6], vaccine nationalism has been the dominant theme of global vaccination. Low-and middle-income countries (LMICs) have encountered great difficulty in obtaining supplies of COVID vaccines [7]. The same problems apply to treatments [8,9,10].
Most efforts to develop COVID-19 treatments have focused on antivirals [10,11]; for the most part, these are monoclonal antibody preparations. There have been appeals for a coordinated system for organizing and financing global pandemic research and development [12], but no one has suggested a practical way to create such a system and make it accountable. In the meantime, important public health issues (e.g., masking) have become deeply polarizing and have led to highly politicized debate [13].
For more than a decade I have argued that the only practical response to a global pandemic would be to target the host response to infection using inexpensive generic drugs [14,15,16,17,18,19,20,21,22,23,24,25,26,27,28]. People who live in any country with basic healthcare would already have these repurposed drugs on the first pandemic day. I recently wrote, “If we already knew that these drugs could save lives, they could be used in every country that is still affected by COVID-19” [25]. Host response treatment could be especially important for LMICs, which have experienced great difficulty in obtaining meaningful and affordable supplies of vaccines and antivirals.
This article will discuss several issues related to the use of generic drugs (including but not limited to statins, ACE inhibitors (ACEis), and angiotensin receptor blockers (ARBs)) to treat patients with COVID-19. It will focus on their ability to reduce 28–30-day mortality (not that reducing hospitalization rates and ICU admissions is unimportant). I reviewed the rationale for this idea in many articles written during periods when an influenza pandemic was anticipated (especially Refs. [15,17,19,22]). The principles outlined in these earlier articles apply equally well to COVID-19 and, in fact, to any pandemic, regardless of cause. They might also improve the host response to critical illness caused by any pathogen.
2. The COVID-19 Pandemic
The pathophysiology of COVID-19 has been extensively reviewed [29,30,31,32,33,34,35,36,37,38,39,40], especially in relation to endothelial dysfunction [41,42,43,44,45,46,47,48,49,50,51,52,53,54]. The acute disease is also characterized by extensive modification of innate and adaptive immunity, increased inflammatory cytokines, abnormal interferon responses and immunothrombosis (Figure 1). This article will not review the pathophysiology of acute COVID-19 in any detail, but three points deserve emphasis. First, the many manifestations of acute COVID-19 (and probably other acute virus infections) reflect underlying differences in subphenotypes [55]. Host response treatment might affect only one of these many subphenotypes [56]. Second, the low mortality of COVID-19 in children and the much higher mortality in older adults must lie in their different evolutionary heritages [23,57,58,59]. The mechanisms underlying this difference remain to be determined. Third, findings for the pathophysiology and treatment of COVID-19 may apply to long COVID as well as the acute disease, even for those who initially had mild illness [60,61,62,63,64,65].
3. Randomized Controlled Trials vs. Observational Studies
Controversies over study methods—randomized controlled trials (RCTs) versus observational studies—continue to plague the literature on COVID-19. Most existing studies of treatments (antivirals and some of the drugs targeting the host response) are based on the results of RCTs, whereas much of the information on generic treatment is based on observational studies. The advantages and disadvantages of both study methods are summarized in Table 1.
Strong arguments have been made for the validity of observational studies for establishing the causal effects of treatments [67,68,69]. These reports and others [70,71,72,73] have criticized a sole reliance on RCTs for demonstrating treatment efficacy. Observational studies that use propensity scores have been shown to reliably mimic the results of RCTs [74]. Effectively managing the complex pathophysiology of COVID-19 probably requires using more than one drug; i.e., combination treatments are required [75]. A “pragmatic pluralism” is probably more suitable than a single method for establishing an effective approach to COVID-19 treatment [76].
4. Treatments for COVID-19
Treatments for COVID-19 can be divided into those that target the virus (antiviral agents) and those that target the host response to infection (often called immunomodulators). There may be some overlap between the two; drugs that modify the host response might also have antiviral effects. Comprehensive treatment guidelines have been issued for the U.S. by the National Institutes of Health [77] which offer extensive advice (448 pages) on treating non-hospitalized as well as hospitalized patients. For Europe, the European Respiratory Society (ERS) guidelines are much more succinct [78,79]. Treatment guidelines have also been issued by The World Health Organization (WHO) [80]. Table 2 summarizes both sets of guidelines.
5. Treatments Targeting the Virus
Soon after the emergence of SARS-CoV-2, there was initial enthusiasm for treatment with either chloroquine or hydroxychloroquine (CQ/HCQ). Although in vitro evidence indicated these drugs might work, clinical trials and observational studies suggested they would be ineffective [81], a finding that recalled earlier clinical trials showing that CQ/HCQ did not work against other virus diseases (influenza and dengue) [82]. For remdesivir, clinical trials initially showed that intravenous treatment had no effect on 28-day mortality, although it appeared to shorten the length of hospital stay [83,84]. Two more recent RCTs [85,86] and an observational study [87] suggest that remdesivir treatment may actually reduce mortality by about 30–40% and prevent hospitalization but also may prolong the hospital length-of-stay. Studies of favipiravir have shown it offers no advantages over other ineffective antiviral agents [88,89]. The same lack of effect has been shown for ivermectin, an anti-schistosomal drug that has attracted a great deal of controversy [90,91,92,93]. In large studies, two other drugs that target the virus—colchicine [94,95] and convalescent plasma [96,97,98]—have also been shown not to reduce COVID-19 mortality. One hallmark of COVID 19 pathophysiology is disruption of normal interferon signaling [99,100]. Nonetheless, the WHO Solidarity trial [101] and studies of interferon-β [102] and pegylated interferon lambda [103] have shown interferon treatment does not reduce COVID-19 mortality.
Several monoclonal antibodies (mAbs) targeting SARS-CoV-2 have been developed [104] and tested to determine whether they reduce the severity of COVID-19 illness and its consequences [105]. A detailed Cochrane analysis of four RCTs included 9749 seropositive but unvaccinated, pre-omicron COVID-19 patients. It showed that pre-exposure prophylaxis with tixagevimab/ciligavimab probably reduced the number of symptoms and hospital admissions but had no effect on mortality [105]. A smaller study of casirivimab and imdevimab showed that treatment with these mAbs might have reduced symptomatic infections, but had uncertain effects on more severe symptoms and deaths. Two RCTs of post-exposure prophylaxis showed that the same two mAbs probably reduced the number of people infected but had little or no effect on mortality. A more recent study of Regdanvimab has shown a modest reduction in mortality [106]. After the Food and Drug Administration decided to deauthorize casirivimab and imdevimab (they were ineffective against omicron subvariants of SARS-CoV-2), there was a slow decline in their use [107]. Although most monoclonal antibodies are less effective against omicron subvariants, bebtelovimab appeared to be the most effective mAb against these subvariants [108] but it has since been withdrawn, because it is not effective. In addition, mAbs require parenteral administration, a feature that mostly limits their use to hospitalized patients.
Among antiviral agents shown to be effective against COVID-19 in unvaccinated adults, Paxlovid (nirmatrelvir/ritonavir) and molnupiravir have been shown to reduce symptomatic infections and hospital admissions [109,110]. During the recent omicron surge, Paxlovid reduced mortality in patients over 65 years of age, but not in younger individuals [111]. A small proportion of patients have tested positive for SARS-CoV-2 soon after completing a five-day course of Paxlovid treatment [112,113]. This “rebound” appears to be a general phenomenon and is not unique to Paxlovid [114].
Although antiviral drugs are sometimes useful against COVID-19 [115], they have several disadvantages. First, not all of these drugs are available as oral preparations; some (e.g., mAbs) require intravenous or subcutaneous administration, which may require hospital care. Second, supplies of many antiviral drugs are limited. The company that manufactures molnupiravir—an expensive antiviral—has negotiated agreements for supplying it to resource-poor countries at low prices [116]. However, molnupiravir is less attractive as an antiviral than Paxlovid because it appears to be less effective. Third, cost is still a barrier to widespread antiviral use, especially in resource-poor countries, because many of these drugs are still under patent.
As yet there are no descriptive data that document the global use of any antiviral agent for COVID-19 treatment. It is doubtful that any of these drugs have been or will be widely used in LMICs. Moreover, in patients who die of COVID-19, virus loads in the last days of life are far lower than they were when patients first tested positive (Figure 1) [117]. Because a dysregulated host response is largely responsible for disease severity at the end of life, treatments that target the host response to infection instead of the virus are more likely to improve patient survival.
6. Treatments Targeting the Host Response to Infection
Dexamethasone was the first drug shown to improve survival in hospitalized COVID-19 patients. In the RECOVERY RCT, dexamethasone reduced 28-day mortality in patients receiving mechanical ventilation (MV; rate ratio = 0.64) and in those requiring oxygen treatment without MV (rate ratio = 0.82), but not in those who received no respiratory support (rate ratio = 1.19) [118]. These results were not surprising: steroid treatment had been tested previously (with mixed results) in patients with sepsis and ARDS [119,120,121]. In. another RCT, intravenous dexamethasone decreased the need for MV but did not reduce 28-day all-cause mortality [122]. A WHO-sponsored meta-analysis of seven RCTs showed that dexamethasone and hydrocortisone decreased mortality (ORs = 0.64 and 0.69, respectively) [123].
Dexamethasone may work through its effects on endothelial dysfunction [124], but treatment is not without its hazards (e.g., hyperglycemia and opportunistic infections) [125]. Unfortunately, its use in non-hospitalized adults (for which there is no evidence of efficacy) has been considerable [126]. A recent observational study compared the results of steroid treatment with those from RCTs. The investigators argued that both methods could obtain similar results as long as the observational study methods were rigorous [127].
In spite of the encouraging results from RCTs, questions still remain about the role of steroid treatment in patients with COVID-19 [128]. Are currently recommended doses of dexamethasone immunomodulatory? Can responders and non-responders be identified before treatment starts? Who benefits most from steroid treatment? Do patients infected with only certain SARS-CoV-2 subphenotypes benefit from treatment? These and other questions will require ongoing attention from clinical and laboratory-based investigators.
A small retrospective cohort study showed that anakinra, an IL-1 receptor antagonist, reduced 21-day mortality but an RCT with 116 patients showed it failed to improve outcomes [129].
IL-6 is a prominent component of the “cytokine storm” seen in many seriously ill COVID-19 patients. Two RCTs have shown that tocilizumab (an mAb) reduces COVID-19 mortality [130,131]. In a WHO-sponsored meta-analysis [132], tocilizumab was associated with a reduction in 28-day all-cause mortality. The absolute mortality reduction (22%) was slightly less than that seen in patients who received dexamethasone instead of other corticosteroid preparations. In spite of the appearance of many subvariants of SARS-CoV-2, there have been no reports of tocilizumab’s reduced efficacy, probably because it targets IL-6, not the virus itself.
Fluvoxamine and fluvoxatine are selective serotonin uptake inhibitors (SSRIs) known to suppress cytokine levels and reduce COVID-19 mortality [133]. In a retrospective cohort study, both drugs reduced mortality (RR = 0.74; p = 0.04) [134]. Subsequent RCTs showed that fluvoxamine reduced hospitalization among outpatients [135,136], but did not reduce mortality [137].
Janus kinase inhibitors and tyrosine kinase inhibitors have also been tested for their effects on host response. In an early study, the Janus kinase inhibitor barcitinib was shown to dramatically reduce inflammatory cytokine levels and the need for oxygen therapy [138]. A later RCT showed that treating hospitalized adults with COVID-19 pneumonia with another Janus kinase inhibitor (tofacitinib) reduced 28-day and 60-day mortality and 28-day all-cause mortality (HR = 0.49) [139]. A meta-analysis of four RCTs and 11 observational studies showed even greater mortality reduction (OR = 0.12, p < 0.001) [140]. These results were confirmed in a critically ill group of mechanically ventilated patients (mortality reduction HR = 0.54; p = 0.03) [141]. In addition, an RCT of imatinib, a tyrosine kinase inhibitor that attenuates endothelial vascular leak, was shown to reduce 28-day and 90-day COVID-19 mortality and improve ventilation [142,143]. A clinical trial is underway to determine whether this improvement is due to attenuation of endothelial dysfunction [143].
Severe COVID-19 is often accompanied by severe coagulopathy, venous thrombosis and occasional pulmonary embolization [144,145]. Several RCTs and observational studies have sought to determine the role of anticoagulant treatment in improving patient survival [144,145]. Some RCTs have shown that therapeutic anticoagulation reduces patient mortality [146,147], while others have been stopped for reasons of futility [148]. Observational studies have shown mixed results: some show therapeutic anticoagulation improves mortality [149] while others do not. In ICU patients, an intermediate dose of low molecular weight heparin offers no increase in benefits over a standard dose [150]. Anticoagulation of COVID-19 inpatients with venous thrombosis is recommended but prophylactic anticoagulation of all inpatients is not. Long-term outpatient anticoagulation of discharged patients is not protective. The use of direct acting oral anticoagulants is not recommended; they have not been shown to be effective in reducing mortality. In patients who have experienced venous thrombosis, the duration of anticoagulant treatment after hospital discharge is uncertain.
7. Treating the Host Response with Inexpensive Generic Drugs
Severe COVID-19 is associated with dysregulated energy metabolism [40]. Several observational studies have shown that metformin, which acts through AMP-activated protein kinase (AMPK) and PGC-1α to increase mitochondrial biogenesis and improve energy metabolism, reduces COVID-19 mortality in outpatients with Type 2 diabetes mellitus [151]. An RCT of outpatient metformin treatment, however, failed to show this benefit [137].
Fenofibrate is a peroxisome proliferator activated receptor alpha (PPAR-α) agonist that may help minimize the inflammatory and thrombotic consequences associated with SARSCoV-2 infection [152]. It attenuates the interaction between SARS-CoV-2 and ACE2, which could directly reduce infection-related inflammation. Unfortunately, an RCT has shown that fenofibrate has no effect on COVID-19 outcomes [153]. Pioglitazone and rosiglitazone are peroxisome proliferator activated receptor gamma (PPAR-γ,) agonists (thiazolidinediones) that also have anti-inflammatory activities in COVID-19 patients and have been suggested for treatment [154,155]. They too have been shown not to affect outcomes in COVID-19 patients.
8. Treating the Host Response to COVID-19 with Inexpensive Generic Statins, ACE Inhibitors (ACEis), and Angiotensin Receptor Blockers (ARBs)
Soon after the onset of the COVID-19 pandemic, an observational study from China reported that inpatient statin treatment was associated with a reduction in mortality [156]. This was thought to be due to the pleiotropic effects of statin treatment on the host response.
I have reviewed the putative mechanisms for these statin effects many times [17,19,22]. and will not repeat them here. Many observational studies have reported that outpatient statins reduce COVID-19 hospitalizations and mortality [157]. These findings also apply to patients with coagulopathies and immunothrombosis [158] and risk conditions such as diabetes [159].
Observational studies have also shown that chronic treatment with ACE inhibitors or ARBs is not harmful and can be beneficial in COVID-19 patients [160,161]. A clinical trial of telmisartan (an ARB) has yielded similar results [162]. Moreover, continuation of ACE inhibitor/ARB outpatient treatment after hospitalization has beneficial effects on COVID-19 outcomes [163], whereas discontinuing treatment can be harmful [164,165,166,167,168]. Similarly, an increase in COVID-19 mortality has been observed following withdrawal of statin treatment [169,170]. Withdrawal of treatment with these drugs is discussed in greater detail below.
Although the complexities of COVID-19 have been extensively reviewed, there is no single consensus on its pathophysiology. Nonetheless, many of the biomarkers associated with COVID-19 hyperinflammation, endothelial dysfunction and immunothrombosis are beneficially affected by both statins and ACEis/ARBs. The effects of these drugs on several important COVID-19 biomarkers are shown in Table 3.
Cardiologists have known for many years that combination treatment with a statin and an ACE inhibitor are synergistic [171,172]. In 2014/2015, a statin/ARB combination appeared to dramatically reduce Ebola mortality in Sierra Leone [21,22,173]. Combination treatment is also discussed below.
For people who live in LMICs, COVID-19 treatments licensed in wealthy countries may be too expensive or they are simply unavailable. Hospital beds for those with critical illness may be few or unavailable [174]. Moreover, statin use itself might be limited [175]. (There are no data on the extent to which ACE inhibitors/ARBs or other generic drugs are used in LMICs.) Nonetheless, in resource-poor countries inexpensive generic drugs like statins, ACE inhibitors, and ARBs might be the only practical way to save the lives of patients with severe COVID-19 [176]. These drugs will be available in all countries on the first pandemic day. In addition. because they target the host response to infection, they could be used to save lives during any pandemic [16,17,18,19,22]. They might even be used to save the lives of those with other forms of acute critical illness like sepsis and ARDS [177].
9. Statin and ACE Inhibitor/ARB Withdrawal
Investigators have known for many years that statin treatment is associated with reduced mortality due to several infectious diseases [178]. Cardiovascular investigators know that statins are clearly beneficial in preventing cardiovascular diseases in people less than 75 years in age [179]. Moreover, research published 15–20 years ago showed that statin treatment reduced morbidity and mortality in patients with acute myocardial infarction [180]. It made no difference whether outpatient statins were continued after hospital admission or were started in the hospital. Furthermore, statin withdrawal was associated with an increase in cardiovascular mortality. The importance of statin withdrawal and its probable mechanisms of action were extensively reviewed in 2006 [181]. For COVID-19, similar findings have been published for ACE inhibitor and ARB withdrawal [164,165,166,167,168].
Most studies showing that statins are associated with reduced COVID-19 mortality are based on outpatient treatment [27]. The point estimates for mortality reduction in these studies (e.g., Ref. [157]) are unreliable because they do not document whether statin treatment was continued or withdrawn after hospital admission. Thus, accurate estimates for mortality reduction can only be obtained from evidence of inpatient statin treatment.
10. Inpatient Statin Treatment
In 2021, an observational study by Belgian investigators reported that inpatient statin treatment was associated with reduced COVID-19 mortality [26]. At least 24 observational studies have reported similar results [26,158,169,182,183,184,185,186,187,188,189,190,191,192,193,194,195,196,197,198]. The results of six RCTs of inpatient statin treatment have also been reported [199,200,201,202,203,204]. All of these results are summarized in Table 4.
A meta-analysis of five of the six RCTs of inpatient statin treatment has been published [206]. The relative risk of death was 0.90 (95% CI = 0.73–1.11; p value = 0.33). Daily statin treatment had no effect on mortality, but three of the six studies were very small [199,200,204], four used what was probably too low a dose of atorvastatin (20 mg instead of 40 mg) [199,200,201,202], and one dealt only with ICU patients [202], which may have been too late in the course of illness. Two RCTs examined simultaneous treatment with several drugs [200,203]. One additional RCT reported the results of statin/aspirin treatment on mortality [207]. In this study, ten days of atorvastatin treatment (40 mg) reduced in-hospital mortality, but no statistical results were reported. An earlier meta-analysis of “inpatient” statin treatment included eight RCTs [208]. Unfortunately, one of the eight observational studies of statin effects on mortality in this meta-analysis reported on chronic (i.e., outpatient) but not inpatient statin treatment.
Of the 22 observational studies of inpatient statin treatment, 12 used propensity score matching to minimize confounding [26,158,182,185,187,189,191,193,194,196,197,205], five reported treating >1000 patients [170,182,184,189,197], and many of the remaining studies included hundreds of subjects. All but one observational study [194] showed that statins significantly reduced COVID-19 mortality. Almost all observational studies recommended that they be followed by RCTs.
Thus, as shown in Table 4, there was a distinct difference in the results of RCTs and observational studies of inpatient statin treatment. Almost all of the observational studies showed mortality reductions, whereas all of the RCTs failed to show these reductions. The REMAP-CAP investigators should soon report findings from a large RCT of inpatient statin treatment. It is hoped these widely anticipated results will help resolve this difference.
11. Combination Treatment
In 2021, Belgian investigators published an observational study showing that inpatient treatment with a combination of a statin and either an ACE inhibitor or an ARB was associated with a threefold reduction in 28-day COVID-19 mortality [26]. Combination treatment was more effective in reducing COVID-19 mortality than statin treatment alone.
Combination treatment for pandemics was suggested in 2008 [17]. For COVID-19, combinations of repurposed drugs have been very effective [209]. Earlier studies had shown that a statin/ACE inhibitor combination was effective in reducing morbidity after coronary artery bypass surgery [171]. A statin/ARB combination appeared effective in reducing mortality during the Ebola outbreak in Sierra Leone [21,22,173]. Combination treatment is not unusual; combinations of antivirals and dexamethasone had been reported earlier [210]. Combinations of baricitinib with remdesivir [211] and with dexamethasone [212] have been reported for COVID-19.
The Belgian study is the only report of inpatient combination statin and ACEi or ARB treatment of COVID-19, although this combination has probably been widely used by clinicians (e.g., Ref. [169]). The success of combination polypill treatment for the prevention of cardiovascular disease [21,213,214] suggests the potential for using an inexpensive generic drug combination for treating patients affected by any pandemic. A pragmatic combination could contain two or more generic drugs (a statin, an ACEi/ARB, metformin, or a PPARα or PPARγ agonist). Each of these individual drugs is known to be safe in patients with critical illness and in those requiring long-term treatment. A combination polypill-like treatment could be especially important for pandemic-affected patients in LMICs.
12. Why Have There Been No RCTs of Combination Treatment with Statins and ACEis/ARBs?
Other than the Belgian hospital study [26], it is surprising that no studies of combination treatment with statins and ACE inhibitor/ARB treatment have been undertaken. Other combination studies for COVID-19 have been reported [211,212]. One can only speculate about the reasons for the absence of these combination studies.
No pharmaceutical company would make money from advocating generic drug treatment for COVID-19 (although the health benefits for people in LMICs could be substantial [18,25]). Leadership for the global response to the COVID-19 pandemic, especially the rapid development of effective vaccines, has come from WHO, international institutions and prestigious national health agencies. Many of those who have favored vaccines have not been elected by the people in high-income countries who have benefitted most [215]. Nonetheless, global estimates of COVID-19′s excess mortality (at least 20 million excess deaths [1]) strongly suggest that the success of vaccine development has come too late for most of the world’s people.
Inexpensive generic drugs like statins affect many aspects of the host response to infection [216,217]. Three RCTs published more than a decade ago showed that statins alone were ineffective in improving survival in patients with sepsis and ARDS, especially in those admitted to ICUs [218]. These results may have persuaded some health officials and investigators that it would be useless to test statins against COVID-19. In addition, failure to understand the importance of subphenotypes in determining responses to statin treatment may have led many to conclude that statins were ineffective [219]. Moreover, social influences and behavioral biases may have led some to overlook or dismiss the idea that statins might be helpful [220,221]. The advice of scientific experts about COVID-19 was generally accepted (despite uncertainties) by most people. Support for political leaders was initially high, but distrust soon arose because political decisions often differed from the views of scientists [222]. This lack of trust led to difficulties with vaccination programs and might have led some to conclude that host response treatments had nothing to offer.
13. The Way Forward—The Next Pandemic
The COVID-19 pandemic might be on the decline, but the SARS-CoV-2 virus is not going to go away [223]. Most virologists predict it will become endemic. A few regions of the world might be able to eliminate the virus but only if herd immunity levels (induced by vaccination or previous infection) are very high. No one can predict how the virus will evolve, but its evolution is certain [224]. Future ‘variant waves” might be characterized by increased mortality or be benign like those of other coronaviruses that humans have experienced for several decades. Whether affordable and effective treatments will eventually be discovered and widely implemented to blunt these waves is uncertain [225]. In the meantime, the burden of the current pandemic must not be forgotten—more than 20 million excess deaths worldwide [1] and more than an estimated 10 million orphans [226]. This burden has fallen heavily on LMICs [227].
The Lancet recently published the findings and recommendations of its COVID-19 Commission [228]. The findings were predictable and unremarkable—the pandemic’s origin remains unknown, the reactions of WHO and national governments were too slow, public opposition to advice indicated a lack of trust, widespread inequities occurred everywhere (especially access to rapidly developed vaccines in LMICs). Social and economic progress were set back in all countries. Many of the Commission’s recommendations are self-evident—strengthening national health systems, expanding national pandemic preparedness planning and improving “mass vaccination, availability and affordability of testing, treatment for new infections and long COVID (test and treat), complementary public health and social measures (including the wearing of face masks in some contexts), promotion of safe workplaces, and economic and social support for self-isolation” [228]. However, other recommendations such as establishing a WHO Science Council, a World Health Assembly-sponsored Global Health Board and a new WHO-based Global Health Fund, if implemented, are unlikely to make a difference when the next pandemic arrives.
An agenda for pandemic research by clinicians is shown in Table 5 [16,17,18,19,22,28,229]. It is unlikely that arguments regarding the primacy of RCTs over observational studies will be settled anytime soon, although the concept of “real world evidence” (RWE) and the availability of electronic health records (EHRs) have allowed the utility of observational studies (i.e., most RWE studies) to be more widely discussed [69,230,231,232,233,234,235,236,237,238,239,240]. In contrast, critics of RWE have written about why they favor RCTs over observational studies [241,242]. Those who favor RWE studies say that having to choose between the two is a ‘myth’. Although neither method is perfect, the two are synergistic and they complement each other [233]. While “early observational studies and small randomized trials may cause spurious claims of effectiveness”, this conclusion is based on an examination of antiviral agents, not host response treatments [243]. Sometimes, clinicians are justified in undertaking innovative treatment before conducting definitive research [244] as long as it is supported by other RWE data [238]. The goal of all research “must be actionable data—data that are sufficient for clinical and public health—that have been derived openly and objectively and that enable us to say, “’Here’s what we recommend and why’” [245]. As I wrote more than ten years ago, “Sadly, the arithmetic for pandemic vaccines and antivirals is unforgiving. WHO is focused on vaccines and antivirals that will only be available to people who can afford them, and that’s ten percent of the world’s population. Consequently, it doesn’t matter that arguments for their use are scientifically well grounded; in practical terms they are pointless, in the same way that it is pointless to tell a starving man he should eat if there’s no food in the kitchen. For pandemic vaccines and antiviral agents, the kitchen is empty. We should stop talking about things that people in developing countries will never have, and start talking about things they’ve already got” [246].
Research on acute and long COVID-19 [247,248] will continue. In addition to pathophysiological studies (Figure 1) related to endothelial dysfunction, innate and adaptive immunity, interferon and abnormal coagulation, observational studies will continue to examine host response treatments [249,250], especially target trial studies that emulate RCTs [127]. The unexplained “tolerance” of children compared with adults will still require explanation [23,251,252,253]. In addition, energy metabolism, epigenetic changes, and the contributions of the microbiome and circadian rhythms to COVID-19 pathogenesis will come to the fore. New treatments and treatment combinations will receive more attention. Moreover, clinical and epidemiological studies will begin to document outpatient drug treatments that might influence COVID-19 hospitalizations and outcomes as much as high-risk conditions and abnormal laboratory findings.
Research for pandemic preparedness must consider the needs of people who live in LMICs, recognizing that every life-saving discovery will also help those who live in rich countries. As discussed in this review, treating pandemic patients with generic drugs like statins and ACEis/ARBs could “nudge” the host response back toward self-regulating homeostasis. It might not have much effect on the infection itself, but it might save lives. There is no guarantee it would work, but good science demands it be tried. A journalist has recently written about the challenge we face. “We should see science as something people do: as a way of solving problems, a project that does not just describe the world but brashly wants to change it. A science that people will follow must lead. If in the next pandemic we want something else from our public health leaders—to save lives and not tear the country apart in the process—we must learn to see science as a vehicle, not a dodge, for human agency: something we are right to make demands of, right at times to get angry at, whose terrible failures it must own along with its triumphs” [254].
Funding
This research received no external funding.
Institutional Review Board Statement
This review article required no informed consent or institutional review statements.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The author declares no conflict of interest.
References
- Adam, D. COVID’s true death toll: Much higher than official records. Nature 2022, 603, 562. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Ruhm, C.J.; Puac-Polanco, V.; Hwang, I.H.; Lee, S.; Petukhova, M.V.; Sampson, N.A.; Ziobrowski, H.N.; Zaslavsky, A.M.; Zubizarreta, J.R. Estimated Prevalence of and Factors Associated with Clinically Significant Anxiety and Depression Among US Adults During the First Year of the COVID-19 Pandemic. JAMA Netw. Open 2022, 5, e2217223. [Google Scholar] [CrossRef] [PubMed]
- Egger, D.; Miguel, E.; Warren, S.S.; Shenoy, A.; Collins, E.; Karlan, D.; Parkerson, D.; Mobarak, A.M.; Fink, G.; Udry, C.; et al. Falling living standards during the COVID-19 crisis: Quantitative evidence from nine developing countries. Sci. Adv. 2021, 7, eabe0997. [Google Scholar] [CrossRef] [PubMed]
- Bok, K.; Sitar, S.; Graham, B.S.; Mascola, J.R. Accelerated COVID-19 vaccine development: Milestones, lessons, and prospects. Immunity 2021, 54, 1636–1651. [Google Scholar] [CrossRef] [PubMed]
- Watson, O.J.; Barnsley, G.; Toor, J.; Hogan, A.B.; Winskill, P.; Ghani, A.C. Global impact of the first year of COVID-19 vaccination: A mathematical modelling study. Lancet Infect. Dis. 2022, 22, 1293–1302. [Google Scholar] [CrossRef]
- World Health Organisation. Vaccine Equity Declaration. 2021. Available online: https://www.who.int/campaigns/vaccine-equity/vaccine-equity-declaration (accessed on 20 March 2022).
- Hunter, D.J.; Karim, S.S.A.; Baden, L.R.; Farrar, J.J.; Hamel, M.B.; Longo, D.L.; Morrissey, S.; Rubin, E.J. Addressing Vaccine Inequity—Covid-19 Vaccines as a Global Public Good. N. Engl. J. Med. 2022, 386, 1176–1179. [Google Scholar] [CrossRef]
- Batista, C.; Shoham, S.; Ergonul, O.; Hotez, P.; Bottazzi, M.E.; Figueroa, J.P.; Gilbert, S.; Gursel, M.; Hassanain, M.; Kang, G.; et al. Urgent needs to accelerate the race for COVID-19 therapeutics. Eclinicalmedicine 2021, 36, 100911. [Google Scholar] [CrossRef]
- Dolgin, E. The race for antiviral drugs to beat COVID—And the next pandemic. Nature 2021, 592, 340–343. [Google Scholar] [CrossRef]
- Usher, A.D. The global COVID-19 treatment divide. Lancet 2022, 399, 779–782. [Google Scholar] [CrossRef]
- Nelson, F. Billion-dollar project aims to prep drugs before the next pandemic. Nature 2022, 31. [Google Scholar] [CrossRef]
- Lurie, N.; Keusch, G.T.; Dzau, V.J. Urgent lessons from COVID-19: Why the world needs a standing, coordinated system and sustainable financing for global research and development. Lancet 2021, 397, 1229–1236. [Google Scholar] [CrossRef] [PubMed]
- Dupont, S.C.; Galea, S. Science, Competing Values, and Trade-offs in Public Health—The Example of COVID-19 and Masking. N. Engl. J. Med. 2022, 387, 865–867. [Google Scholar] [CrossRef] [PubMed]
- Fedson, D.S. Pandemic influenza vaccines: Obstacles and opportunities. In The Threat of Pandemic Infuenza. Are We Ready? Knobler, S.L., Mack, A., Mahmoud, A., Lemon, S.M., Eds.; The National Academies Press: Washington, DC, USA, 2005; pp. 184–194. [Google Scholar] [CrossRef]
- Fedson, D.S. Pandemic Influenza: A Potential Role for Statins in Treatment and Prophylaxis. Clin. Infect. Dis. 2006, 43, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Fedson, D.S.; Dunnill, P. Commentary: From Scarcity to Abundance: Pandemic Vaccines and Other Agents for “Have Not” Countries. J. Public Health Policy 2007, 28, 322–340. [Google Scholar] [CrossRef]
- Fedson, D.S. Confronting an influenza pandemic with inexpensive generic agents: Can it be done? Lancet Infect. Dis. 2008, 8, 571–576. [Google Scholar] [CrossRef]
- Fedson, D.S. Meeting the Challenge of Influenza Pandemic Preparedness in Developing Countries. Emerg. Infect. Dis. 2009, 15, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Fedson, D.S. Treating influenza with statins and other immunomodulatory agents. Antivir. Res. 2013, 99, 417–435. [Google Scholar] [CrossRef]
- Fedson, D.S. How Will Physicians Respond to the Next Influenza Pandemic? Clin. Infect. Dis. 2014, 58, 233–237. [Google Scholar] [CrossRef] [Green Version]
- Fedson, D.S.; Jacobson, J.R.; Rordam, O.M.; Opal, S.M. Treating the Host Response to Ebola Virus Disease with Generic Statins and Angiotensin Receptor Blockers. MBio 2015, 6, e00716-15. [Google Scholar] [CrossRef] [Green Version]
- Fedson, D.S. Treating the host response to emerging virus diseases: Lessons learned from sepsis, pneumonia, influenza and Ebola. Ann. Transl. Med. 2016, 4, 421. [Google Scholar] [CrossRef] [Green Version]
- Fedson, D.S. Influenza, evolution, and the next pandemic. Evol. Med. Public Health 2018, 2018, 260–269. [Google Scholar] [CrossRef] [PubMed]
- Fedson, D.S.; Opal, S.M.; Rordam, O.M. Hiding in Plain Sight: An Approach to Treating Patients with Severe COVID-19 Infection. MBio 2020, 11, e00398-20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fedson, D.S. COVID-19, host response treatment, and the need for political leadership. J. Public Health Policy 2020, 42, 6–14. [Google Scholar] [CrossRef]
- Byttebier, G.; Belmans, L.; Alexander, M.; Saxberg, B.E.H.; De Spiegeleer, B.; De Spiegeleer, A.; Devreker, N.; Van Praet, J.T.; Vanhove, K.; Reybrouck, R.; et al. Hospital mortality in COVID-19 patients in Belgium treated with statins, ACE inhibitors and/or ARBs. Hum. Vaccines Immunother. 2021, 17, 2841–2850. [Google Scholar] [CrossRef]
- Fedson, D.S. Statin withdrawal and treating COVID-19 patients. Pharmacol. Res. Perspect. 2021, 9, e00861. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharya, J.; Booy, R.; Casadevall, A.; Cruz, C.D.; Fedson, D.S.; Garcia, J.G.N.; Grohmann, G.; Hung, I.F.N.; Jacobson, J.R.; Jennings, L.C.; et al. A practical treatment for COVID-19 and the next pandemic. Pharmacol. Res. Perspect. 2022, 10, e00988. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.G.; Simpson, L.J.; Ferreira, A.-M.; Rustagi, A.; Roque, J.; Asuni, A.; Ranganath, T.; Grant, P.M.; Subramanian, A.; Rosenberg-Hasson, Y.; et al. Cytokine profile in plasma of severe COVID-19 does not differ from ARDS and sepsis. J. Clin. Investig. 2020, 5, e140289. [Google Scholar] [CrossRef]
- Lowery, S.A.; Sariol, A.; Perlman, S. Innate immune and inflammatory responses to SARS-CoV-2: Implications for COVID-19. Cell Host Microbe 2021, 29, 1052–1062. [Google Scholar] [CrossRef]
- Wilk, A.J.; Lee, M.J.; Wei, B.; Parks, B.; Pi, R.; Martínez-Colón, G.J.; Ranganath, T.; Zhao, N.Q.; Taylor, S.; Becker, W.; et al. Multi-omic profiling reveals widespread dysregulation of innate immunity and hematopoiesis in COVID-19. J. Exp. Med. 2021, 218, e20210582. [Google Scholar] [CrossRef]
- O’Carroll, S.M.; O’Neill, L.A.J. Targeting immunometabolism to treat COVID-19. Immunother. Adv. 2021, 1, ltab013. [Google Scholar] [CrossRef]
- Merad, M.; Blish, C.A.; Sallusto, F.; Iwasaki, A. The immunology and immunopathology of COVID-19. Science 2022, 375, 1122–1127. [Google Scholar] [CrossRef] [PubMed]
- Lamers, M.M.; Haagemans, B.L. SARS-CoV-2 pathogenesis. Nat. Rev. Microbiol. 2022, 20, 270–284. [Google Scholar] [CrossRef]
- Roquilly, A.; Jacqueline, C.; Davieau, M.; Mollé, A.; Sadek, A.; Fourgeux, C.; Rooze, P.; Broquet, A.; Misme-Aucouturier, B.; Chaumette, T.; et al. Alveolar macrophages are epigenetically altered after inflammation, leading to long-term lung immunoparalysis. Nat. Immunol. 2020, 21, 636–648. [Google Scholar] [CrossRef] [PubMed]
- Muri, J.; Kopf, M. Redox regulation of immunometabolism. Nat. Rev. Immunol. 2020, 21, 363–381. [Google Scholar] [CrossRef] [PubMed]
- Sposito, B.; Broggi, A.; Pandolfi, L.; Crotta, S.; Clementi, N.; Ferrarese, R.; Sisti, S.; Criscuolo, E.; Spreafico, R.; Long, J.M.; et al. The interferon landscape along the respiratory tract impacts the severity of COVID-19. Cell 2021, 184, 4953–4968.e16. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, T.S.; de Sá, K.S.; Ishimoto, A.Y.; Becerra, A.; Oliveira, S.; Almeida, L.; Gonçalves, A.V.; Perucello, D.B.; Andrade, W.A.; Castro, R.; et al. Inflammasomes are activated in response to SARS-CoV-2 infection and are associated with COVID-19 severity in patients. J. Exp. Med. 2020, 218, e20201707. [Google Scholar] [CrossRef]
- Giamarellos-Bourbolis, E.J.; Netea, M.G.; Rovina, N.; Akinoissoglou, K.; Antoniadou, A.; Antonakos, N.; Damoraki, G.; Gkavogianni, T.; Adami, M.-E.; Katsaounou, P.; et al. Complex immune dysregulation function in COVID-19 patients with severe respiratory failure. Cell Host Microbe. 2020, 27, 1–9. [Google Scholar] [CrossRef]
- Kontaridis, M.I.; Chennappan, S. Mitochondria and the future of RASopathies: The emergence of bioenergetics. J. Clin. Investig. 2022, 132, 1–5. [Google Scholar] [CrossRef]
- Hough, R.F.; Islam, M.N.; Gusarova, G.A.; Jin, G.; Das, S.; Bhattacharya, J. Endothelial mitochondria determine rapid barrier failure in chemical lung injury. JCI Insight 2019, 4, e124329. [Google Scholar] [CrossRef] [Green Version]
- Libby, P.; Lüscher, T. COVID-19 is, in the end, an endothelial disease. Eur. Heart J. 2020, 41, 3038–3044. [Google Scholar] [CrossRef]
- Nicosia, R.F.; Ligresti, G.; Caporarello, N.; Akilesh, S.; Ribatti, D. COVID-19 Vasculopathy: Mounting Evidence for an Indirect Mechanism of Endothelial Injury. Am. J. Pathol. 2021, 191, 1374–1384. [Google Scholar] [CrossRef] [PubMed]
- Bonaventura, A.; Vecchié, A.; Dagna, L.; Martinod, K.; Dixon, D.L.; Van Tassell, B.W.; Dentali, F.; Montecucco, F.; Massberg, S.; Levi, M.; et al. Endothelial dysfunction and immunothrombosis as key pathogenic mechanisms in COVID-19. Nat. Rev. Immunol. 2021, 21, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Gu, S.X.; Tyagi, T.; Jain, K.; Gu, V.W.; Lee, S.H.; Hwa, J.M.; Kwan, J.M.; Krause, D.S.; Lee, A.I.; Halene, S.; et al. Thrombocytopathy and endotheliopathy: Crucial contributors to COVID-19 thromboinflammation. Nat. Rev. Cardiol. 2020, 18, 194–209. [Google Scholar] [CrossRef] [PubMed]
- Shao, Y.; Saredy, J.; Xu, K.; Sun, Y.; Saaoud, F.; Drummer, C.I.; Lu, Y.; Luo, J.J.; Lopez-Pastrana, J.; Choi, E.T.; et al. Endothelial Immunity Trained by Coronavirus Infections, DAMP Stimulations and Regulated by Anti-Oxidant NRF2 May Contribute to Inflammations, Myelopoiesis, COVID-19 Cytokine Storms and Thromboembolism. Front. Immunol. 2021, 12, 653110. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, C.; Luque, N.; Blanco, I.; Sebastian, L.; Barberà, J.A.; Peinado, V.I.; Tura-Ceide, O. Pulmonary Endothelial Dysfunction and Thrombotic Complications in Patients with COVID-19. Am. J. Respir. Cell Mol. Biol. 2021, 64, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Leisman, D.E.; Mehta, A.; Thompson, B.T.; Charland, N.C.; Gonye, A.L.K.; Gushterova, I.; Kays, K.R.; Khanna, H.K.; LaSalle, T.J.; Lavin-Parsons, K.M.; et al. Alveolar, Endothelial, and Organ Injury Marker Dynamics in Severe COVID-19. Am. J. Respir. Crit. Care Med. 2022, 205, 507–519. [Google Scholar] [CrossRef] [PubMed]
- Hui, K.P.-Y.; Cheung, M.-C.; Lai, K.-L.; Ng, K.-C.; Ho, J.C.-W.; Peiris, M.; Nicholls, J.M.; Chan, M.C.-W. Role of Epithelial–Endothelial Cell Interaction in the Pathogenesis of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection. Clin. Infect. Dis. 2021, 74, 199–209. [Google Scholar] [CrossRef] [PubMed]
- Joffre, J.; Rodriguez, L.; Matthay, Z.A.; Lloyd, E.; Fields, A.T.; Bainton, R.J.; Kurien, P.; Sil, A.; Calfee, C.S.; Woodruff, P.G.; et al. COVID-19–associated Lung Microvascular Endotheliopathy: A “From the Bench” Perspective. Am. J. Respir. Crit. Care Med. 2022, 206, 961–972. [Google Scholar] [CrossRef]
- Patterson, E.K.; Cepinskas, G.; Fraser, D.D. Endothelial Glycocalyx Degradation in Critical Illness and Injury. Front. Med. 2022, 9, 898592. [Google Scholar] [CrossRef]
- Ambrosino, P.; Calcaterra, I.L.; Mosella, M.; Formisano, R.; D’Anna, S.E.; Bachetti, T.; Marcuccio, G.; Galloway, B.; Mancini, F.P.; Papa, A.; et al. Endothelial Dysfunction in COVID-19: A Unifying Mechanism and a Potential Therapeutic Target. Biomedicines 2022, 10, 812. [Google Scholar] [CrossRef]
- Price, D.R.; Benedetti, E.; Hoffman, K.L.; Gomez-Escobar, L.; Alvarez-Mulett, S.; Capili, A.; Sarwath, H.; Parkhurst, C.N.; Lafond, E.; Weidman, K.; et al. Angiopoietin 2 Is Associated with Vascular Necroptosis Induction in Coronavirus Disease 2019 Acute Respiratory Distress Syndrome. Am. J. Pathol. 2022, 192, 1001–1015. [Google Scholar] [CrossRef] [PubMed]
- Ashour, L. Roles of the ACE/Ang II/AT1R pathway, cytokine release, and alteration of tight junctions in COVID-19 pathogenesis. Tissue Barriers 2022, 2090792. [Google Scholar] [CrossRef] [PubMed]
- Sinha, P.; Calfee, C.S.; Cherian, S.; Brealey, D.; Cutler, S.; King, C.; Killick, C.; Richards, O.; Cheema, Y.; Bailey, C.; et al. Prevalence of phenotypes of acute respiratory distress syndrome in critically ill patients with COVID-19: A prospective observational study. Lancet Respir. Med. 2020, 8, 1209–1218. [Google Scholar] [CrossRef] [PubMed]
- Calfee, C.S.; Delucchi, K.L.; Sinha, P.; Matthay, M.A.; Hackett, J.; Shankar-Hari, M.; McDowell, C.; Laffey, J.G.; O’Kane, C.M.; McAuley, D.F.; et al. Acute respiratory distress syndrome subphenotypes and differential response to simvastatin: Secondary analysis of a randomised controlled trial. Lancet Respir. Med. 2018, 6, 691–698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joachim, R.; Suber, F.; Kobzik, L. Characterising Pre-pubertal Resistance to Death from Endotoxemia. Sci. Rep. 2017, 7, 16541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suber, F.; Kobzik, L. Childhood tolerance of severe influenza: A mortality analysis in mice. Am. J. Physiol. Cell. Mol. Physiol. 2017, 313, L1087–L1095. [Google Scholar] [CrossRef]
- Joachim, R.B.; Altschuler, G.M.; Hutchinson, J.N.; Wong, H.R.; A Hide, W.; Kobzik, L. The relative resistance of children to sepsis mortality: From pathways to drug candidates. Mol. Syst. Biol. 2018, 14, e7998. [Google Scholar] [CrossRef]
- Kell, D.B.; Laubscher, G.J.; Pretorius, E. A central role for amyloid fibrin microclots in long COVID/PASC: Origins and therapeutic implications. Biochem. J. 2022, 479, 537–559. [Google Scholar] [CrossRef]
- Ahamed, J.; Laurence, J. Long COVID endotheliopathy: Hypothesized mechanisms and potential therapeutic approaches. J. Clin. Investig. 2022, 132, e161167. [Google Scholar] [CrossRef]
- Puntmann, V.O.; Martin, S.; Shchendrygina, A.; Hoffmann, J.; Ka, M.M.; Giokoglu, E.; Vanchin, B.; Holm, N.; Karyou, A.; Laux, G.S.; et al. Long-term cardiac pathology in individuals with mild initial COVID-19 illness. Nat. Med. 2022, 28, 2117–2123. [Google Scholar] [CrossRef]
- Gyöngyösi, M.; Alcaide, P.; Asselbergs, F.W.; Brundel, B.J.J.M.; Camici, G.G.; Martins, P.D.C.; Ferdinandy, P.; Fontana, M.; Girao, H.; Gnecchi, M.; et al. Long COVID and the cardiovascular system—Elucidating causes and cellular mechanisms in order to develop targeted diagnostic and therapeutic strategies: A joint Scientific Statement of the ESC Working Groups on Cellular Biology of the Heart and Myocardial and Pericardial Diseases. Cardiovasc. Res. 2022, cvac115. [Google Scholar] [CrossRef]
- Munblit, D.; Nicholson, T.; Akrami, A.; Apfelbacher, C.; Chen, J.; De Groote, W.; Diaz, J.V.; Gorst, S.L.; Harman, N.; Kokorina, A.; et al. A core outcome set for post-COVID-19 condition in adults for use in clinical practice and research: An international Delphi consensus study. Lancet Respir. Med. 2022, 10, 715–724. [Google Scholar] [CrossRef] [PubMed]
- Department of Health and Human Services, Office of the Assistant Secretary for Health. National Research Action Plan on Long COVID; Department of Health and Human Services: Washington, DC, USA, 2021. [Google Scholar]
- Ayres, J.S. A metabolic handbook for the COVID-19 pandemic. Nat Metab. 2020, 2, 572–585. [Google Scholar] [CrossRef] [PubMed]
- Concato, J. Study Design and “Evidence” in Patient-oriented Research. Am. J. Respir. Crit. Care Med. 2013, 187, 1167–1172. [Google Scholar] [CrossRef]
- Gershon, A.S.; Lindenauer, P.K.; Wilson, K.C.; Rose, L.; Walkey, A.J.; Sadatsafavi, M.; Anstrom, K.J.; Au, D.H.; Bender, B.G.; Brookhart, M.A.; et al. Informing Healthcare Decisions with Observational Research Assessing Causal Effect. An Official American Thoracic Society Research Statement. Am. J. Respir. Crit. Care Med. 2021, 203, 14–23. [Google Scholar] [CrossRef]
- Concato, J.; Corrigan-Curay, J. Real-World Evidence—Where Are We Now? N. Engl. J. Med. 2022, 386, 1680–1682. [Google Scholar] [CrossRef]
- Abel, U.; Koch, A. Discussion. J. Clin. Epidemiol. 1999, 52, 487–497. [Google Scholar] [CrossRef] [PubMed]
- Deaton, A.; Cartwright, N. Understanding and misunderstanding randomized controlled trials. Soc. Sci. Med. 2017, 210, 2–21. [Google Scholar] [CrossRef]
- Paneth, N.S.; Joyner, M.J.; Casadevall, A. The fossilization of randomized clinical trials. J. Clin. Investig. 2022, 132, e158499. [Google Scholar] [CrossRef]
- Itaya, T.; Isobe, Y.; Suzuki, S.; Koike, K.; Nishigaki, M.; Yamamoto, Y. The Fragility of Statistically Significant Results in Randomized Clinical Trials for COVID-19. JAMA Netw. Open 2022, 5, e222973. [Google Scholar] [CrossRef]
- Kitsios, G.D.; Dahabreh, I.J.; Callahan, S.; Paulus, J.K.; Campagna, A.C.; Dargin, J.M. Can We Trust Observational Studies Using Propensity Scores in the Critical Care Literature? A Systematic Comparison with Randomized Clinical Trials. Crit. Care Med. 2015, 43, 1870–1879. [Google Scholar] [CrossRef] [PubMed]
- Sturmberg, J.; Paul, E.; Van Damme, W.; Ridde, V.; Brown, G.W.; Kalk, A. The danger of the single storyline obfuscating the complexities of managing SARS-CoV-2/COVID-19. J. Eval. Clin. Pract. 2021, 28, 1173–1186. [Google Scholar] [CrossRef] [PubMed]
- Vandenbroucke, J.P.; Broadbent, A.; Pearce, N. Causality and causal inference in epidemiology: The need for a pluralistic approach. Int. J. Epidemiol. 2016, 45, 1776–1786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institutes of Health. COVID-19 Treatment Guidelines; Anti-SARS-CoV-2 Antibody Products. 2022. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 10 September 2022).
- Roche, N.; Crichton, M.L.; Goeminne, P.C.; Cao, B.; Humbert, M.; Shteinberg, M.; Antoniou, K.M.; Ulrik, C.S.; Parks, H.; Wang, C.; et al. Update June 2022: Management of hospitalised adults with coronavirus disease 2019 (COVID-19): A European Respiratory Society living guideline. Eur. Respir. J. 2022, 60, 2200803. [Google Scholar] [CrossRef]
- Crichton, M.L.; Goeminne, P.C.; Tuand, K.; Vandendriessche, T.; Tonia, T.; Roche, N.; Chalmers, J.D. The impact of therapeutics on mortality in hospitalised patients with COVID-19: Systematic review and meta-analyses informing the European Respiratory Society living guideline. Eur. Respir. Rev. 2021, 30, 210171. [Google Scholar] [CrossRef]
- World Health Organization. Clinical Management of COVID-19: Living Guideline, 15 September 2022; (WHO/2019-nCoV/Clinical/2022.2. Licence: CC BY-NC-SA 3.0 IGO); World Health Organization: Geneva, Switzerland, 2022; Available online: https://apps.who.int/iris/handle/10665/362783 (accessed on 30 January 2023).
- Axfors, C.; Schmitt, A.M.; Janiaud, P.; Hooft, J.V.; Abd-Elsalam, S.; Abdo, E.F.; Abella, B.S.; Akram, J.; Amaravadi, R.K.; Angus, D.C.; et al. Mortality outcomes with hydroxychloroquine and chloroquine in COVID-19 from an international collaborative meta-analysis of randomized trials. Nat. Commun. 2021, 12, 2349. [Google Scholar] [CrossRef]
- Cui, X.; Sun, J.; Minkove, S.J.; Li, Y.; Cooper, D.; Couse, Z.; Eichacker, P.Q.; Torabi-Parizi, P. Effects of chloroquine or hydroxychloroquine treatment on non-SARS-CoV2 viral infections: A systematic review of clinical studies. Rev. Med. Virol. 2021, 31, e2228. [Google Scholar] [CrossRef]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of COVID-19—Preliminary report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef]
- Ohl, M.E.; Miller, D.R.; Lund, B.C.; Kobayashi, T.; Miell, K.R.; Beck, B.F.; Alexander, B.; Crothers, K.; Sarrazin, M.S.V. Association of Remdesivir Treatment with Survival and Length of Hospital Stay Among US Veterans Hospitalized With COVID-19. JAMA Netw. Open 2021, 4, e2114741. [Google Scholar] [CrossRef]
- Olender, S.A.; Walunas, T.L.; Martinez, E.; Perez, K.K.; Castagna, A.; Wang, S.; Kurbegov, D.; Goyal, P.; Ripamonti, D.; Balani, B.; et al. Remdesivir Versus Standard-of-Care for Severe Coronavirus Disease 2019 Infection: An Analysis of 28-Day Mortality. Open Forum Infect. Dis. 2021, 8, ofab278. [Google Scholar] [CrossRef]
- Gottlieb, R.L.; Vaca, C.E.; Paredes, R.; Mera, J.; Webb, B.J.; Perez, G.; Oguchi, G.; Ryan, P.; Nielsen, B.U.; Brown, M.; et al. Early Remdesivir to Prevent Progression to Severe COVID-19 in Outpatients. N. Engl. J. Med. 2022, 386, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Diaz, G.A.; Christensen, A.B.; Pusch, T.; Goulet, D.; Chang, S.-C.; Grunkemeier, G.L.; A McKelvey, P.; Robicsek, A.; French, T.; Parsons, G.T.; et al. Remdesivir and Mortality in Patients with Coronavirus Disease 2019. Clin. Infect. Dis. 2021, 74, 1812–1820. [Google Scholar] [CrossRef] [PubMed]
- Chuah, C.H.; Chow, T.S.; Hor, C.P.; Cheng, J.T.; Ker, H.B.; Lee, H.G.; Lee, K.S.; Nordin, N.; Ng, T.K.; Zaid, M.; et al. Efficacy of Early Treatment with Favipiravir on Disease Progression Among High-Risk Patients with Coronavirus Disease 2019 (COVID-19): A Randomized, Open-Label Clinical Trial. Clin. Infect. Dis. 2021, 75, e432–e439. [Google Scholar] [CrossRef] [PubMed]
- AlQahtani, M.; Kumar, N.; Aljawder, D.; Abdulrahman, A.; Mohamed, M.W.; Alnashaba, F.; Abu Fayyad, M.; Alshaikh, F.; Alsahaf, F.; Saeed, S.; et al. Randomized controlled trial of favipiravir, hydroxychloroquine, and standard care in patients with mild/moderate COVID-19 disease. Sci. Rep. 2022, 12, 4925. [Google Scholar] [CrossRef]
- López-Medina, E.; López, P.; Hurtado, I.C.; Dávalos, D.M.; Ramirez, O.; Martínez, E.; Díazgranados, J.A.; Oñate, J.M.; Chavarriaga, H.; Herrera, S.; et al. Effect of Ivermectin on Time to Resolution of Symptoms Among Adults with Mild COVID-19. JAMA 2021, 325, 1426. [Google Scholar] [CrossRef]
- Reis, G.; Silva, E.A.; Silva, D.C.; Thabane, L.; Milagres, A.C.; Ferreira, T.S.; dos Santos, C.V.; Campos, V.H.; Nogueira, A.M.; de Almeida, A.P.; et al. Effect of Early Treatment with Ivermectin among Patients with COVID-19. N. Engl. J. Med. 2022, 386, 1721–1731. [Google Scholar] [CrossRef]
- Kerr, L.; Cadegiani, F.A.; Baldi, F.; Lobo, R.B.; Assagra, W.L.O.; Proença, F.C.; Kory, P.; Hibberd, J.A.; Chamie-Quintero, J.J. Ivermectin Prophylaxis Used for COVID-19: A Citywide, Prospective, Observational Study of 223,128 Subjects Using Propensity Score Matching. Cureus 2022, 14, e21272. [Google Scholar] [CrossRef]
- Izcovich, A.; Peiris, S.; Ragusa, M.; Tortosa, F.; Rada, G.; Aldighieri, S.; Reveiz, L. Bias as a source of inconsistency in ivermectin trials for COVID-19: A systematic review. Ivermectin’s suggested benefits are mainly based on potentially biased results. J. Clin. Epidemiol. 2021, 144, 43–55. [Google Scholar] [CrossRef]
- Tardif, J.-C.; Bouabdallaoui, N.; L’Allier, P.L.; Gaudet, D.; Shah, B.; Pillinger, M.H.; Lopez-Sendon, J.; da Luz, P.; Verret, L.; Audet, S.; et al. Colchicine for community-treated patients with COVID-19 (COLCORONA): A phase 3, randomised, double-blinded, adaptive, placebo-controlled, multicentre trial. Lancet Respir. Med. 2021, 9, 924–932. [Google Scholar] [CrossRef]
- Recovery Collaborative Group. Colchicine in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet Respir. Med. 2021, 9, 1419–1426. [Google Scholar] [CrossRef]
- Klassen, S.A.; Senefeld, J.W.; Johnson, P.W.; Carter, R.E.; Wiggins, C.C.; Shoham, S.; Grossman, B.J.; Henderson, J.P.; Musser, J.; Salazar, E.; et al. The Effect of Convalescent Plasma Therapy on Mortality Among Patients With COVID-19: Systematic Review and Meta-analysis. Mayo Clin. Proc. 2021, 96, 1262–1275. [Google Scholar] [CrossRef] [PubMed]
- Bégin, P.; Callum, J.; Jamula, E.; Cook, R.; Heddle, N.M.; Tinmouth, A.; Zeller, M.P.; Beaudoin-Bussières, G.; Amorim, L.; Bazin, R.; et al. Convalescent plasma for hospitalized patients with COVID-19: An open-label, randomized controlled trial. Nat. Med. 2021, 27, 2012–2024. [Google Scholar] [CrossRef] [PubMed]
- Joyner, M.J.; Carter, R.E.; Senefeld, J.W.; Klassen, S.A.; Mills, J.R.; Johnson, P.W.; Theel, E.S.; Wiggins, C.C.; Bruno, K.A.; Klompas, A.M.; et al. Convalescent Plasma Antibody Levels and the Risk of Death from COVID-19. N. Engl. J. Med. 2021, 384, 1015–1027. [Google Scholar] [CrossRef] [PubMed]
- Park, A.S.; Iwasaki, A. Type I and Type III Interferons—Induction, Signaling, Evasion, and Application to Combat COVID-19. Cell Host Microbe 2020, 27, 870–878. [Google Scholar] [CrossRef] [PubMed]
- Zanoni, I. Interfering with SARS-CoV-2: Are interferons friends or foes in COVID-19. Curr. Opin. Virol. 2021, 50, 119–127. [Google Scholar] [CrossRef] [PubMed]
- WHO Solidarity Trial Consortium. Repurposed Antiviral Drugs for COVID-19—Interim WHO Solidarity Trial Results. N. Engl. J. Med. 2021, 384, 497–511. [Google Scholar] [CrossRef]
- Kumar, S.; Saurabh, M.K.; Narasimha, V.L.; Maharshi, V. Efficacy of Interferon-β in Moderate-to-Severe Hospitalised Cases of COVID-19: A Systematic Review and Meta-analysis. Clin. Drug Investig. 2021, 41, 1037–1046. [Google Scholar] [CrossRef]
- Feld, J.J.; Kandel, C.; Biondi, M.J.; A Kozak, R.; Zahoor, M.A.; Lemieux, C.; Borgia, S.M.; Boggild, A.K.; Powis, J.; McCready, J.; et al. Peginterferon lambda for the treatment of outpatients with COVID-19: A phase 2, placebo-controlled randomised trial. Lancet Respir. Med. 2021, 9, 498–510. [Google Scholar] [CrossRef]
- Corti, D.; Purcell, L.A.; Snell, G.; Veesler, D. Tackling COVID-19 with neutralizing monoclonal antibodies. Cell 2021, 184, 3086–3108. [Google Scholar] [CrossRef]
- Hirsch, C.; Park, Y.S.; Piechotta, V.; Chai, K.L.; Estcourt, L.J.; Monsef, I.; Salomon, S.; Wood, E.M.; So-Osman, C.; McQuilten, Z.; et al. SARS-CoV-2-neutralising monoclonal antibodies to prevent COVID-19. Cochrane Database Syst. Rev. 2022, 2022, CD014945. [Google Scholar] [CrossRef]
- Kim, J.Y.; Săndulescu, O.; Preotescu, L.L.; E Rivera-Martínez, N.; Dobryanska, M.; Birlutiu, V.; Miftode, E.G.; Gaibu, N.; Caliman-Sturdza, O.; Florescu, S.A.; et al. A Randomized Clinical Trial of Regdanvimab in High-Risk Patients with Mild-to-Moderate COVID-19. Open Forum Infect. Dis. 2022, 9, ofac406. [Google Scholar] [CrossRef] [PubMed]
- Anderson, T.S.; O’Donoghue, A.; Mechanic, O.; Dechen, T.; Stevens, J. Administration of Anti–SARS-CoV-2 Monoclonal Antibodies After US Food and Drug Administration Deauthorization. JAMA Netw. Open 2022, 5, e2228997. [Google Scholar] [CrossRef] [PubMed]
- Hentzien, M.; Autran, B.; Piroth, L.; Yazdanpanah, Y.; Calmy, A. A monoclonal antibody stands out against omicron subvariants: A call to action for a wider access to bebtelovimab. Lancet Infect. Dis. 2022, 22, 1278. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.K.H.; Au, I.C.H.; Lau, K.T.K.; Lau, E.H.Y.; Cowling, B.J.; Leung, G.M. Real-world effectiveness of early molnupiravir or nirmatrelvir–ritonavir in hospitalised patients with COVID-19 without supplemental oxygen requirement on admission during Hong Kong’s omicron BA.2 wave: A retrospective cohort study. Lancet Infect. Dis. 2022, 22, 1681–1693. [Google Scholar] [CrossRef]
- Jayk Bernal, A.; Gomes da Silva, M.M.; Musungaie, D.B.; Kovalchuk, E.; Gonzalez, A.; Delos Reyes, V.; Martín-Quirós, A.; Caraco, Y.; Williams-Diaz, A.; Brown, M.L.; et al. Molnupiravir for Oral Treatment of COVID-19 in Nonhospitalized Patients. N. Engl. J. Med. 2022, 386, 509–520. [Google Scholar] [CrossRef]
- Arbel, R.; Sagy, Y.W.; Hoshen, M.; Battat, E.; Lavie, G.; Sergienko, R.; Friger, M.; Waxman, J.G.; Dagan, N.; Balicer, R.; et al. Nirmatrelvir Use and Severe Covid-19 Outcomes during the Omicron Surge. N. Engl. J. Med. 2022, 387, 790–798. [Google Scholar] [CrossRef]
- Epling, B.P.; Rocco, J.M.; Boswell, K.L.; Laidlaw, E.; Galindo, F.; Kellogg, A.; Das, S.; Roder, A.; Ghedin, E.; Kreitman, A.; et al. Clinical, Virologic, and Immunologic Evaluation of Symptomatic Coronavirus Disease 2019 Rebound Following Nirmatrelvir/Ritonavir Treatment. Clin. Infect. Dis. 2022, ciac663. [Google Scholar] [CrossRef]
- Wang, L.; Volkow, N.D.; Davis, P.B.; Berger, N.A.; Kaelber, D.C.; Xu, R. COVID-19 rebound after Paxlovid treatment during Omicron BA.5 and BA2.12.1 subvariant predominance period. medRxiv 2022. [Google Scholar] [CrossRef]
- Anderson, A.S.; Caubel, P.; Rusnak, J.M. Nirmatrelvir–Ritonavir and Viral Load Rebound in COVID-19. N. Engl. J. Med. 2022, 387, 1047–1049. [Google Scholar] [CrossRef]
- Pitre, T.; Van Alstine, R.; Chick, G.; Leung, G.; Mikhail, D.; Cusano, E.; Khalid, F.; Zeraatkar, D. Antiviral drug treatment for nonsevere COVID-19: A systematic review and network meta-analysis. Can. Med. Assoc. J. 2022, 194, E969–E980. [Google Scholar] [CrossRef]
- Dal-Ré, R.; Becker, S.L.; Bottieau, E.; Holm, S. Availability of oral antivirals against SARS-CoV-2 infection and the requirement for an ethical prescribing approach. Lancet Infect. Dis. 2022, 22, e231–e238. [Google Scholar] [CrossRef] [PubMed]
- Burki, T.K. The role of antiviral treatment in the COVID-19 pandemic. Lancet Respir. Med. 2022, 10, e18. [Google Scholar] [CrossRef]
- Recovery Collaborative Group. Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- Annane, D.; Bellissant, E.; Bollaert, P.E.; Briegel, J.; Keh, D.; Kupfer, Y.; Pirracchio, R.; Rochwerg, B. Corticosteroids for treating sepsis in children and adults. Cochrane Database Syst. Rev. 2019, 2019, CD002243. [Google Scholar] [CrossRef] [PubMed]
- Liang, H.; Song, H.; Zhai, R.; Song, G.; Li, H.; Ding, X.; Kan, Q.; Sun, T. Corticosteroids for Treating Sepsis in Adult Patients: A Systematic Review and Meta-Analysis. Front. Immunol. 2021, 12, 709155. [Google Scholar] [CrossRef] [PubMed]
- Villar, J.; Ferrando, C.; Martínez, D.; Ambrós, A.; Muñoz, T.; Soler, J.A.; Aguilar, G.; Alba, F.; González-Higueras, E.; Conesa, L.A.; et al. Dexamethasone treatment for the acute respiratory distress syndrome: A multicentre, randomised controlled trial. Lancet Respir. Med. 2020, 8, 267–276. [Google Scholar] [CrossRef]
- Tomazini, B.M.; Maia, I.S.; Cavalcanti, A.B.; Berwanger, O.; Rosa, R.G.; Veiga, V.C.; Avezum, A.; Lopes, R.D.; Bueno, F.R.; Silva, M.V.A.O.; et al. Effect of Dexamethasone on Days Alive and Ventilator-Free in Patients with Moderate or Severe Acute Respiratory Distress Syndrome and COVID-19: The CoDEX Randomized Clinical Trial. JAMA 2020, 324, 1307–1316. [Google Scholar] [CrossRef]
- The WHO Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group; Sterne, J.A.C.; Murthy, S.; Diaz, J.V.; Slutsky, A.S.; Villar, J.; Angus, D.C.; Annane, D.; Azevedo, L.C.P.; Berwanger, O.; et al. Association Between Administration of Systemic Corticosteroids and Mortality Among Critically Ill Patients With COVID-19: A Meta-analysis. JAMA 2020, 324, 1330–1341. [Google Scholar] [CrossRef]
- Kim, W.-Y.; Kweon, O.J.; Cha, M.J.; Baek, M.S.; Choi, S.-H. Dexamethasone may improve severe COVID-19 via ameliorating endothelial injury and inflammation: A preliminary pilot study. PLoS ONE 2021, 16, e0254167. [Google Scholar] [CrossRef]
- Martínez-Martínez, M.; Plata-Menchaca, E.P.; Nuvials, F.X.; Roca, O.; Ferrer, R. Risk factors and outcomes of ventilator-associated pneumonia in COVID-19 patients: A propensity score matched analysis. Crit. Care 2021, 25, 235. [Google Scholar] [CrossRef]
- Bradley, M.C.; Perez-Vilar, S.; Chillarige, Y.; Dong, D.; Martinez, A.I.; Weckstein, A.R.; Pan, G.J.D. Systemic Corticosteroid Use for COVID-19 in US Outpatient Settings from April 2020 to August 2021. JAMA 2022, 327, 2015. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, K.L.; Schenck, E.J.; Satlin, M.J.; Whalen, W.; Pan, D.; Williams, N.; Díaz, I. Comparison of a Target Trial Emulation Framework vs Cox Regression to Estimate the Association of Corticosteroids With COVID-19 Mortality. JAMA Netw. Open 2022, 5, e2234425. [Google Scholar] [CrossRef] [PubMed]
- Winkler, M.S.; Osuchowski, M.F.; Payen, D.; Torres, A.; Dickel, S.; Skirecki, T. Renaissance of glucocorticoids in critical care in the era of COVID-19: Ten urging questions. Crit. Care 2022, 26, 308. [Google Scholar] [CrossRef] [PubMed]
- CORIMUNO-19 Collaborative Group. Effect of anakinra versus usual care in adults in hospital with COVID-19 and mild-to-moderate pneumonia (CORIMUNO-ANA-1): A randomised controlled trial. Lancet Respir. Med. 2021, 9, 295–304. [Google Scholar] [CrossRef]
- Recovery Collaborative Group. Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2021, 397, 1637–1645. [Google Scholar] [CrossRef]
- Gordon, A.C.; Mouncey, P.R.; Al-Beidh, F.; Rowan, K.M.; Nichol, A.D.; Arabi, Y.M.; Annane, D.; Beane, A.; Van Bentum-Puijk, W.; Berry, L.R.; et al. Interleukin-6 Receptor Antagonists in Critically Ill Patients with COVID-19. N. Engl. J. Med. 2021, 384, 1491–1502. [Google Scholar] [CrossRef] [PubMed]
- The WHO Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group; Shankar-Hari, M.; Vale, C.L.; Godolphin, P.J.; Fisher, D.; Higgins, J.P.T.; Spiga, F.; Savović, J.; Tierney, J.; Baron, G.; et al. Association Between Administration of IL-6 Antagonists and Mortality Among Patients Hospitalized for COVID-19: A Meta-analysis. JAMA 2021, 326, 499–518. [Google Scholar] [CrossRef]
- Lenze, E.J.; Mattar, C.; Zorumski, C.F.; Stevens, A.; Schweiger, J.; Nicol, G.E.; Miller, J.P.; Yang, L.; Yingling, M.; Avidan, M.S.; et al. Fluvoxamine vs Placebo and Clinical Deterioration in Outpatients with Symptomatic COVID-19. JAMA 2020, 324, 2292–2300. [Google Scholar] [CrossRef]
- Oskotsky, T.; Marić, I.; Tang, A.; Oskotsky, B.; Wong, R.J.; Aghaeepour, N.; Sirota, M.; Stevenson, D.K. Mortality Risk Among Patients With COVID-19 Prescribed Selective Serotonin Reuptake Inhibitor Antidepressants. JAMA Netw. Open 2021, 4, e2133090. [Google Scholar] [CrossRef]
- Lee, T.C.; Vigod, S.; Bortolussi-Courval, É.; Hanula, R.; Boulware, D.R.; Lenze, E.J.; Reiersen, A.M.; McDonald, E.G. Fluvoxamine for Outpatient Management of COVID-19 to Prevent Hospitalization. JAMA Netw. Open 2022, 5, e226269. [Google Scholar] [CrossRef]
- Reis, G.; Moreira-Silva, E.A.D.S.; Silva, D.C.M.; Thabane, L.; Milagres, A.C.; Ferreira, T.S.; dos Santos, C.V.Q.; Campos, V.H.d.S.; Nogueira, A.M.R.; de Almeida, A.P.F.G.; et al. Effect of early treatment with fluvoxamine on risk of emergency care and hospitalisation among patients with COVID-19: The TOGETHER randomised, platform clinical trial. Lancet Glob. Health 2021, 10, e42–e51. [Google Scholar] [CrossRef] [PubMed]
- Bramante, C.T.; Huling, J.D.; Tignanelli, C.J.; Buse, J.B.; Liebovitz, D.M.; Nicklas, J.M.; Cohen, K.; Puskarich, M.A.; Belani, H.K.; Proper, J.L.; et al. Randomized Trial of Metformin, Ivermectin, and Fluvoxamine for COVID-19. N. Engl. J. Med. 2022, 387, 599–610. [Google Scholar] [CrossRef]
- Bronte, V.; Ugel, S.; Tinazzi, E.; Vella, A.; De Sanctis, F.; Canè, S.; Batani, V.; Trovato, R.; Fiore, A.; Petrova, V.; et al. Baricitinib restrains the immune dysregulation in patients with severe COVID-19. J. Clin. Investig. 2020, 130, 6409–6416. [Google Scholar] [CrossRef]
- Guimarães, P.O.; Quirk, D.; Furtado, R.H.; Maia, L.N.; Saraiva, J.F.; Antunes, M.O.; Filho, R.K.; Junior, V.M.; Soeiro, A.M.; Tognon, A.P.; et al. Tofacitinib in Patients Hospitalized with COVID-19 Pneumonia. N. Engl. J. Med. 2021, 385, 406–415. [Google Scholar] [CrossRef]
- Walz, L.; Cohen, A.J.; Rebaza, A.P.; Vanchieri, J.; Slade, M.D.; Cruz, C.S.D.; Sharma, L. JAK-inhibitor and type I interferon ability to produce favorable clinical outcomes in COVID-19 patients: A systematic review and meta-analysis. BMC Infect. Dis. 2021, 21, 47. [Google Scholar] [CrossRef]
- Ely, E.W.; Ramanan, A.V.; E Kartman, C.; de Bono, S.; Liao, R.; Piruzeli, M.L.B.; Goldman, J.D.; Saraiva, J.F.K.; Chakladar, S.; Marconi, V.C.; et al. Efficacy and safety of baricitinib plus standard of care for the treatment of critically ill hospitalised adults with COVID-19 on invasive mechanical ventilation or extracorporeal membrane oxygenation: An exploratory, randomised, placebo-controlled trial. Lancet Respir. Med. 2022, 10, 327–336. [Google Scholar] [CrossRef] [PubMed]
- Aman, J.; Duijvelaar, E.; Botros, L.; Kianzad, A.; Schippers, J.R.; Smeele, P.J.; Azhang, S.; Bartelink, I.H.; A Bayoumy, A.; Bet, P.M.; et al. Imatinib in patients with severe COVID-19: A randomised, double-blind, placebo-controlled, clinical trial. Lancet Respir. Med. 2021, 9, 957–968. [Google Scholar] [CrossRef] [PubMed]
- Duijvelaar, E.; Schippers, J.R.; Smeele, P.J.; de Raaf, M.A.; Vanhove, A.L.E.M.; Blok, S.G.; Twisk, J.W.R.; Noordegraaf, A.V.; de Man, F.S.; Bogaard, H.J.; et al. Long-term clinical outcomes of COVID-19 patients treated with imatinib. Lancet Respir. Med. 2022, 10, e34–e35. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.-L.; Levi, M.; Hunt, B.J. Prevention and management of thrombosis in hospitalised patients with COVID-19 pneumonia. Lancet Respir. Med. 2021, 10, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Flumignan, R.L.; Civile, V.T.; Tinôco, J.D.D.S.; Pascoal, P.I.; Areias, L.L.; Matar, C.F.; Tendal, B.; Trevisani, V.F.; Atallah, N.; Nakano, L.C. Anticoagulants for people hospitalised with COVID-19. Cochrane Database Syst. Rev. 2022, 2022. [Google Scholar] [CrossRef]
- Lopes, R.D.; de Barros E Silva, P.G.M.; Furtado, R.H.M.; Macedo, A.V.S.; Bronhara, B.; Damiani, L.P.; Barbosa, L.M.; de Aveiro Morata, J.; Ramacciotti, E.; de Aquino Martins, P.; et al. Therapeutic versus prophylactic anticoagulation for patients admitted to hospital with COVID-19 and elevated D-dimer concentration (ACTION): An open-label, multicentre, randomised, controlled trial. Lancet 2021, 397, 2253–2263. [Google Scholar] [CrossRef] [PubMed]
- Lawler, P.R.; Goligher, E.C.; Berger, J.S.; Neal, M.D.; McVerry, B.J.; Nicolau, J.C. Therapeutic Anticoagulation with Heparin in Noncritically Ill Patients with COVID-19. N. Engl. J. Med. 2021, 385, 790–802. [Google Scholar] [CrossRef] [PubMed]
- Goligher, E.C.; Bradbury, C.A.; McVerry, B.J.; Lawler, P.R.; Berger, J.S.; Gong, M.N. Therapeutic Anticoagulation with Heparin in Critically Ill Patients with COVID-19. N. Engl. J. Med. 2021, 385, 777–789. [Google Scholar] [CrossRef] [PubMed]
- Ionescu, F.; Jaiyesimi, I.; Petrescu, I.; Lawler, P.R.; Castillo, E.; Munoz-Maldonado, Y.; Imam, Z.; Narasimhan, M.; Abbas, A.E.; Konde, A.; et al. Association of anticoagulation dose and survival in hospitalized COVID-19 patients: A retrospective propensity score-weighted analysis. Eur. J. Haematol. 2020, 106, 165–174. [Google Scholar] [CrossRef] [PubMed]
- INSPIRATION Investigators; Sadeghipour, P.; Talasaz, A.H.; Mazloomzadeh, S.; Khaleghparast, S.; Ghadrdoost, B.; Mousavizadeh, M.; Baay, M.R.; Noohi, F. Effect of Intermediate-Dose vs Standard-Dose Prophylactic Anticoagulation on Thrombotic Events, Extracorporeal Membrane Oxygenation Treatment, or Mortality Among Patients With COVID-19 Admitted to the Intensive Care Unit: The INSPIRATION Randomized Clinical Trial. JAMA 2021, 325, 1620–1630. [Google Scholar]
- Nguyen, N.N.; Ho, D.S.; Nguyen, H.S.; Ho, D.K.N.; Li, H.-Y.; Lin, C.-Y.; Chiu, H.-Y.; Chen, Y.-C. Preadmission use of antidiabetic medications and mortality among patients with COVID-19 having type 2 diabetes: A meta-analysis. Metabolism 2022, 131, 155196. [Google Scholar] [CrossRef]
- Alkhayyat, S.S.; Al-Kuraishy, H.M.; Al-Gareeb, A.I.; El-Bouseary, M.M.; AboKamer, A.M.; Batiha, G.E.-S.; Simal-Gandara, J. Fenofibrate for COVID-19 and related complications as an approach to improve treatment outcomes: The missed key for Holy Grail. Inflamm. Res. 2022, 71, 1159–1167. [Google Scholar] [CrossRef]
- Chirinos, J.A.; Lopez-Jaramillo, P.; Giamarellos-Bourboulis, E.J.; Dávila-Del-Carpio, G.H.; Bizri, A.R.; Andrade-Villanueva, J.F.; Salman, O.; Cure-Cure, C.; Rosado-Santander, N.R.; Giraldo, M.P.C.; et al. A randomized clinical trial of lipid metabolism modulation with fenofibrate for acute coronavirus disease 2019. Nat. Metab. 2022, 4, 1847–1857. [Google Scholar] [CrossRef]
- Vallée, A.; Lecarpentier, Y.; Vallée, J.-N. Interplay of Opposing Effects of the WNT/β-Catenin Pathway and PPARγ and Implications for SARS-CoV2 Treatment. Front. Immunol. 2021, 12, 666693. [Google Scholar] [CrossRef]
- Zhao, Q.; Yu, Z.; Zhang, S.; Shen, X.-R.; Yang, H.; Xu, Y.; Liu, Y.; Yang, L.; Zhang, Q.; Chen, J.; et al. Metabolic modeling of single bronchoalveolar macrophages reveals regulators of hyperinflammation in COVID-19. Iscience 2022, 25, 105319. [Google Scholar] [CrossRef]
- Fajgenbaum, D.C.; Rader, D.J. Teaching Old Drugs New Tricks: Statins for COVID-19? Cell Metab. 2020, 32, 145–147. [Google Scholar] [CrossRef] [PubMed]
- Daniels, L.B.; Ren, J.; Kumar, K.; Bui, Q.M.; Zhang, J.; Zhang, X.; Sawan, M.A.; Eisen, H.; Longhurst, C.A.; Messer, K. Relation of prior statin and anti-hypertensive use to severity of disease among patients hospitalized with COVID-19: Findings from the American Heart Association’s COVID-19 Cardiovascular Disease Registry. PLoS ONE 2021, 16, e0254635. [Google Scholar] [CrossRef] [PubMed]
- Al Harbi, S.; Kensara, R.; Aljuhani, O.; Korayem, G.B.; Altebainawi, A.F.; Al Harthi, A.; Vishwakarma, R.; Alenazi, A.M.; Almutairi, A.; Alshaya, O.; et al. Statins and Risk of Thrombosis in Critically ill Patients with COVID-19: A Multicenter Cohort Study. Clin. Appl. Thromb. 2022, 28, 10760296221103864. [Google Scholar] [CrossRef] [PubMed]
- Audrey, J.; Wisnu, W.; Tahapary, D.L. Association Between Statin Use and Poor Outcomes in COVID-19 Patients with Diabetes Mellitus: A Systematic Review. Curr. Diabetes Rev. 2022, 18, 73–78. [Google Scholar] [CrossRef]
- Aparisi, Á.; Catalá, P.; Amat-Santos, I.J.; Marcos-Mangas, M.; López-Otero, D.; Veras, C.; López-Pais, J.; Cabezón-Villalba, G.; Antonio, C.E.C.; Candela, J.; et al. Chronic use of renin–angiotensin–aldosterone inhibitors in hypertensive COVID-19 patients: Results from a Spanish registry and meta-analysis. Med. Clin. 2021, 158, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Lumbers, E.R.; Head, R.; Smith, G.R.; Delforce, S.J.; Jarrott, B.; Martin, J.H.; Pringle, K.G. The interacting physiology of COVID-19 and the renin-angiotensin-aldosterone system: Key agents for treatment. Pharmacol. Res. Perspect. 2022, 10, e00917. [Google Scholar] [CrossRef]
- Duarte, M.; Pelorosso, F.; Nicolosi, L.N.; Salgado, M.V.; Vetulli, H.; Aquieri, A.; Azzato, F.; Castro, M.; Coyle, J.; Davolos, I.; et al. Telmisartan for treatment of COVID-19 patients: An open multicenter randomized clinical trial. Eclinicalmedicine 2021, 37, 100962. [Google Scholar] [CrossRef]
- Lam, K.W.; Chow, K.W.; Vo, J.; Hou, W.; Li, H.; Richman, P.S.; Mallipattu, S.K.; A Skopicki, H.; Singer, A.J.; Duong, T.Q. Continued In-Hospital Angiotensin-Converting Enzyme Inhibitor and Angiotensin II Receptor Blocker Use in Hypertensive COVID-19 Patients Is Associated with Positive Clinical Outcome. J. Infect. Dis. 2020, 222, 1256–1264. [Google Scholar] [CrossRef]
- Roy-Vallejo, E.; Purificación, A.S.; Peña, J.D.T.; Moreno, B.S.; Arnalich, F.; Blanco, M.J.G.; Miranda, J.L.; Romero-Cabrera, J.L.; Gil, C.R.H.; Bascunana, J.; et al. Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor Blockers Withdrawal Is Associated with Higher Mortality in Hospitalized Patients with COVID-19. J. Clin. Med. 2021, 10, 2642. [Google Scholar] [CrossRef]
- Cohen, J.B.; Hanff, T.C.; William, P.; Sweitzer, N.; Rosado-Santander, N.R.; Medina, C.; E Rodriguez-Mori, J.; Renna, N.; I Chang, T.; Corrales-Medina, V.; et al. Continuation versus discontinuation of renin–angiotensin system inhibitors in patients admitted to hospital with COVID-19: A prospective, randomised, open-label trial. Lancet Respir. Med. 2021, 9, 275–284. [Google Scholar] [CrossRef]
- Bauer, A.; Schreinlechner, M.; Sappler, N.; Dolejsi, T.; Tilg, H.; A Aulinger, B.; Weiss, G.; Bellmann-Weiler, R.; Adolf, C.; Wolf, D.; et al. Discontinuation versus continuation of renin-angiotensin-system inhibitors in COVID-19 (ACEI-COVID): A prospective, parallel group, randomised, controlled, open-label trial. Lancet Respir. Med. 2021, 9, 863–872. [Google Scholar] [CrossRef] [PubMed]
- Oddy, C.; Allington, J.; McCaul, J.; Keeling, P.; Senn, D.; Soni, N.; Morrison, H.; Mawella, R.; Samuel, T.; Dixon, J. Inpatient Omission of Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor Blockers Is Associated With Morbidity and Mortality in Coronavirus Disease 2019. Clin. Ther. 2021, 43, e97–e110. [Google Scholar] [CrossRef] [PubMed]
- Theurl, F.; Sappler, N.; Rizas, K.D.; Massberg, S.; Bauer, A.; Schreinlechner, M. Long-term effects of discontinuing renin–angiotensin system inhibitors in COVID-19. Respirology 2022, 27, 788–790. [Google Scholar] [CrossRef]
- Memel, Z.N.; Lee, J.J.; Foulkes, A.S.; Chung, R.T.; Thaweethai, T.; Bloom, P.P. Association of Statins and 28-Day Mortality Rates in Patients Hospitalized with Severe Acute Respiratory Syndrome Coronavirus 2 Infection. J. Infect. Dis. 2021, 225, 19–29. [Google Scholar] [CrossRef] [PubMed]
- Andrews, L.; Goldin, L.; Shen, Y.; Korwek, K.; Kleja, K.; Poland, R.E.; Guy, J.; Sands, K.E.; Perlin, J.B. Discontinuation of atorvastatin use in hospital is associated with increased risk of mortality in COVID-19 patients. J. Hosp. Med. 2022, 17, 169–175. [Google Scholar] [CrossRef]
- Radaelli, A.; Loardi, C.; Cazzaniga, M.; Balestri, G.; de Carlini, C.; Cerrito, M.G.; Cusa, E.N.; Guerra, L.; Garducci, S.; Santo, D.; et al. Inflammatory Activation During Coronary Artery Surgery and Its Dose-Dependent Modulation by Statin/ACE-Inhibitor Combination. Arter. Thromb. Vasc. Biol. 2007, 27, 2750–2755. [Google Scholar] [CrossRef]
- Borghi, C.; Levy, B.I. Synergistic actions between angiotensin-converting enzyme inhibitors and statins in atherosclerosis. Nutr. Metab. Cardiovasc. Dis. 2021, 32, 815–826. [Google Scholar] [CrossRef]
- Fedson, D.S.; Rordam, O.M. Treating Ebola patients: A ‘bottom up’ approach using generic statins and angiotensin receptor blockers. Int. J. Infect. Dis. 2015, 36, 80–84. [Google Scholar] [CrossRef] [Green Version]
- Vukoja, M.; Riviello, E.; Gavrilovic, S.; Adhikari, N.K.; Kashyap, R.; Bhagwanjee, S.; Gajic, O.; Kilickaya, O.; CERTAIN Investigators. A Survey on Critical Care Resources and Practices in Low- and Middle-Income Countries. Glob. Heart 2014, 9, 337–342.e1. [Google Scholar] [CrossRef]
- Marcus, M.E.; Manne-Goehler, J.; Theilmann, M.; Farzadfar, F.; Moghaddam, S.S.; Keykhaei, M.; Hajebi, A.; Tschida, S.; Lemp, J.M.; Aryal, K.K.; et al. Use of statins for the prevention of cardiovascular disease in 41 low-income and middle-income countries: A cross-sectional study of nationally representative, individual-level data. Lancet Glob. Health 2022, 10, e369–e379. [Google Scholar] [CrossRef]
- Fedson, D.S. Influenza pandemic preparedness: A special challenge for India. Indian J. Med. Res. 2019, 150, 217–220. [Google Scholar] [CrossRef] [PubMed]
- Mota, S.; Bensalel, J.; Park, D.H.; Gonzalez, S.; Rodriguez, A.; Gallego-Delgado, J. Treatment Reducing Endothelial Activation Protects against Experimental Cerebral Malaria. Pathogens 2022, 11, 643. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Wen, X.; Peng, J.; Lu, Y.; Guo, Z.; Lu, J. Systematic Review and Meta-Analysis on the Association between Outpatient Statins Use and Infectious Disease-Related Mortality. PLoS ONE 2012, 7, e51548. [Google Scholar] [CrossRef] [PubMed]
- Yebyo, H.G.; Aschmann, H.; Menges, D.; Boyd, C.M.; Puhan, M.A. Net benefit of statins for primary prevention of cardiovascular disease in people 75 years or older: A benefit-harm balance modeling study. Ther. Adv. Chronic Dis. 2019, 10, 2040622319877745. [Google Scholar] [CrossRef]
- Fonarow, G.C.; Wright, R.S.; Spencer, F.A.; Fredrick, P.D.; Dong, W.; Every, N.; French, W.J. Effect of Statin Use Within the First 24 Hours of Admission for Acute Myocardial Infarction on Early Morbidity and Mortality. Am. J. Cardiol. 2005, 96, 611–616. [Google Scholar] [CrossRef] [PubMed]
- Cubeddu, L.X.; Seamon, M.J. Statin Withdrawal: Clinical Implications and Molecular Mechanisms. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2006, 26, 1288–1296. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.-J.; Qin, J.-J.; Cheng, X.; Shen, L.; Zhao, Y.-C.; Yuan, Y.; Lei, F.; Chen, M.-M.; Yang, H.; Bai, L.; et al. In-Hospital Use of Statins Is Associated with a Reduced Risk of Mortality among Individuals with COVID-19. Cell Metab. 2020, 32, 176–187.e4. [Google Scholar] [CrossRef]
- Rodriguez-Nava, G.; Trelles-Garcia, D.P.; Yanez-Bello, M.A.; Chung, C.W.; Trelles-Garcia, V.P.; Friedman, H.J. Atorvastatin associated with decreased hazard for death in COVID-19 patients admitted to an ICU: A retrospective cohort study. Crit. Care 2020, 24, 429. [Google Scholar] [CrossRef]
- Mallow, P.J.; Belk, K.W.; Topmiller, M.; Hooker, E.A. Outcomes of Hospitalized COVID-19 Patients by Risk Factors: Results from a United States Hospital Claims Database. J. Health Econ. Outcomes Res. 2020, 7, 165–175. [Google Scholar] [CrossRef]
- Saeed, O.; Castagna, F.; Agalliu, I.; Xue, X.; Patel, S.R.; Rochlani, Y.; Kataria, R.; Vukelic, S.; Sims, D.B.; Alvarez, C.; et al. Statin Use and In-Hospital Mortality in Patients With Diabetes Mellitus and COVID-19. J. Am. Heart Assoc. 2020, 9, e018475. [Google Scholar] [CrossRef]
- Lala, A.; Johnson, K.W.; Januzzi, J.L.; Russak, A.J.; Paranjpe, I.; Richter, F.; Zhao, S.; Somani, S.; Van Vleck, T.; Vaid, A.; et al. Prevalence and Impact of Myocardial Injury in Patients Hospitalized With COVID-19 Infection. J. Am. Coll. Cardiol. 2020, 76, 533–546. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Guo, T.; Yan, F.; Gong, M.; Zhang, X.A.; Li, C.; He, T.; Luo, H.; Zhang, L.; Chen, M.; et al. Association of Statin Use with the In-Hospital Outcomes of 2019-Coronavirus Disease Patients: A Retrospective Study. Front. Med. 2020, 7, 584870. [Google Scholar] [CrossRef]
- Rossi, R.; Talarico, M.; Coppi, F.; Boriani, G. Protective role of statins in COVID-19 patients: Importance of pharmacokinetic characteristics rather than intensity of action. Intern. Emerg. Med. 2020, 15, 1573–1576. [Google Scholar] [CrossRef] [PubMed]
- Torres-Peña, J.D.; Pérez-Belmonte, L.M.; Fuentes-Jiménez, F.; Carmona, M.D.L.; Pérez-Martinez, P.; López-Miranda, J.; Sánchez, F.J.C.; Núñez, J.A.V.; Beamonte, E.D.C.; Gamboa, J.O.M.; et al. Prior Treatment with Statins is Associated with Improved Outcomes of Patients with COVID-19: Data from the SEMI-COVID-19 Registry. Drugs 2021, 81, 685–695. [Google Scholar] [CrossRef] [PubMed]
- Terlecki, M.; Wojciechowska, W.; Klocek, M.; Olszanecka, A.; Stolarz-Skrzypek, K.; Grodzicki, T.; Małecki, M.; Katra, B.; Garlicki, A.; Bociąga-Jasik, M.; et al. Association between cardiovascular disease, cardiovascular drug therapy, and in-hospital outcomes in patients with COVID-19: Data from a large single-center registry in Poland. Kardiologia Polska 2021, 79, 773–780. [Google Scholar] [CrossRef]
- Lohia, P.; Kapur, S.; Benjaram, S.; Cantor, Z.; Mahabadi, N.; Mir, T.; Badr, M.S. Statins and clinical outcomes in hospitalized COVID-19 patients with and without Diabetes Mellitus: A retrospective cohort study with propensity score matching. Cardiovasc. Diabetol. 2021, 20, 140. [Google Scholar] [CrossRef]
- Choi, D.; Chen, Q.; Goonewardena, S.N.; Pacheco, H.; Mejia, P.; Smith, R.L.; Rosenson, R.S. Efficacy of Statin Therapy in Patients with Hospital Admission for COVID-19. Cardiovasc. Drugs Ther. 2021, 36, 1165–1173. [Google Scholar] [CrossRef]
- Shen, L.; Qiu, L.; Wang, L.; Huang, H.; Liu, D.; Xiao, Y.; Liu, Y.; Jin, J.; Liu, X.; Wang, D.W.; et al. Statin Use and In-hospital Mortality in Patients with COVID-19 and Coronary Heart Disease. Sci. Rep. 2021, 11, 1–12. [Google Scholar] [CrossRef]
- Ayeh, S.K.; Abbey, E.J.; Khalifa, B.A.A.; Nudotor, R.D.; Osei, A.D.; Chidambaram, V.; Osuji, N.; Khan, S.; Salia, E.L.; Oduwole, M.O.; et al. Statins use and COVID-19 outcomes in hospitalized patients. PLoS ONE 2021, 16, e0256899. [Google Scholar] [CrossRef]
- Masana, L.; Correig, E.; Rodríguez-Borjabad, C.; Anoro, E.; Arroyo, J.A.; Jericó, C.; Pedragosa, A.; Miret, M.; Näf, S.; Pardo, A.; et al. Effect of statin therapy on SARS-CoV-2 infection-related mortality in hospitalized patients. Eur. Heart J. Cardiovasc. Pharmacother. 2020, 8, 157–164. [Google Scholar] [CrossRef]
- Kuno, T.; So, M.; Iwagami, M.; Takahashi, M.; Egorova, N.N. The association of statins use with survival of patients with COVID-19. J. Cardiol. 2021, 79, 494–500. [Google Scholar] [CrossRef]
- Li, W.; Rios, S.; Nagraj, S.; Hajra, A.; Saralidze, T.; Varrias, D.; Mathai, S.V.; Novakovic, M.; Hupart, K.H.; Miles, J.A.; et al. Statin Use in Hospitalized Patients with COVID-19: A Comprehensive Analysis of the New York City Public Hospital System. Am. J. Med. 2022, 135, 897–905. [Google Scholar] [CrossRef]
- Kouhpeikar, H.; Tabasi, H.K.; Khazir, Z.; Naghipour, A.; Moghadam, H.M.; Forouzanfar, H.; Abbasifard, M.; Kirichenko, T.V.; Reiner, Z.; Banach, M.; et al. Statin Use in COVID-19 Hospitalized Patients and Outcomes: A Retrospective Study. Front. Cardiovasc. Med. 2022, 9, 175. [Google Scholar] [CrossRef]
- Davoodi, L.; Jafarpour, H.; Oladi, Z.; Zakariaei, Z.; Tabarestani, M.; Ahmadi, B.M.; Razavi, A.; Hessami, A. Atorvastatin therapy in COVID-19 adult inpatients: A double-blind, randomized controlled trial. IJC Hear. Vasc. 2021, 36, 100875. [Google Scholar] [CrossRef]
- Matli, K.; Al Kotob, A.; Jamaleddine, W.; Al Osta, S.; Salameh, P.; Tabbikha, R.; Chamoun, N.; Moussawi, A.; Saad, J.; Atwi, G.; et al. Managing endothelial dysfunction in COVID -19 with statins, beta blockers, nicorandil, and oral supplements: A pilot, double-blind, placebo-controlled, randomized clinical trial. Clin. Transl. Sci. 2022, 15, 2323–2330. [Google Scholar] [CrossRef]
- Ghafoori, M.; Saadati, H.; Taghavi, M.; Azimian, A.; Alesheikh, P.; Mohajerzadeh, M.S.; Behnamfar, M.; Pakzad, M.; Rameshrad, M. Survival of the hospitalized patients with COVID-19 receiving atorvastatin: A randomized clinical trial. J. Med. Virol. 2022, 94, 3160–3168. [Google Scholar] [CrossRef]
- INSPIRATION-S Investigators Atorvastatin versus placebo in patients with COVID-19 in intensive care: Randomized controlled trial. BMJ 2022, 376, e068407. [CrossRef]
- Gaitán-Duarte, H.; Álvarez-Moreno, C.; Rincón-Rodríguez, C.; Yomayusa-González, N.; Cortés, J.; Villar, J.; Bravo-Ojeda, J.; García-Peña, A.; Adarme-Jaimes, W.; Rodríguez-Romero, V.; et al. Effectiveness of rosuvastatin plus colchicine, emtricitabine/tenofovir and combinations thereof in hospitalized patients with COVID-19: A pragmatic, open-label randomized trial. Eclinicalmedicine 2021, 43, 101242. [Google Scholar] [CrossRef]
- Hejazi, S.; Mircheraghi, F.; Elyasi, S.; Davoodian, N.; Salarbashi, D.; Majd, H.M. Atorvastatin efficacy in the management of mild to moderate hospitalized COVID-19: A pilot randomized triple-blind placebo-controlled clinical trial. Recent Adv. Anti-Infect. Drug Discov. 2022, 17, 212–222. [Google Scholar] [CrossRef]
- Al Sulaiman, K.; Aljuhani, O.; Korayem, G.B.; Altebainawi, A.F.; Al Harbi, S.; Al Shaya, A.; Badreldin, H.A.; Kensara, R.; Alharthi, A.F.; Alghamdi, J.; et al. The impact of HMG-CoA reductase inhibitors use on the clinical outcomes in critically ill patients with COVID-19: A multicenter, cohort study. Front. Public Health 2022, 10, 877944. [Google Scholar] [CrossRef]
- Martins-Filho, P.R.; Barreto-Filho, J.A.S.; Sousa, A.C.S. Effects of statins on clinical outcomes in hospitalized patients with COVID-19. Eur. J. Intern. Med. 2022, 104, 113–115. [Google Scholar] [CrossRef]
- Ghati, N.; Bhatnagar, S.; Mahendran, M.; Thakur, A.; Prasad, K.; Kumar, D.; Dwivedi, T.; Mani, K.; Tiwari, P.; Gupta, R.; et al. Statin and aspirin as adjuvant therapy in hospitalised patients with SARS-CoV-2 infection: A randomised clinical trial (RESIST trial). BMC Infect. Dis. 2022, 22, 606. [Google Scholar] [CrossRef]
- Permana, H.; Huang, I.; Purwiga, A.; Kusumawardhani, N.Y.; Sihite, T.A.; Martanto, E.; Wisaksana, R.; Soetedjo, N.N.M. In-hospital use of statins is associated with a reduced risk of mortality in coronavirus-2019 (COVID-19): Systematic review and meta-analysis. Pharmacol. Rep. 2021, 73, 769–780. [Google Scholar] [CrossRef]
- Chakraborty, C.; Sharma, A.R.; Bhattacharya, M.; Agoramoorthy, G.; Lee, S.-S. The Drug Repurposing for COVID-19 Clinical Trials Provide Very Effective Therapeutic Combinations: Lessons Learned from Major Clinical Studies. Front. Pharmacol. 2021, 12, 2942. [Google Scholar] [CrossRef]
- Zhang, W.; Wang, X.; Hu, W.; Liu, L.; Li, X.; Han, J.; Chen, Y.; Duan, Y. Co-treatment of Pitavastatin and Dexamethasone Exacerbates the High-fat Diet–induced Atherosclerosis in apoE-deficient Mice. J. Cardiovasc. Pharmacol. 2015, 66, 189–195. [Google Scholar] [CrossRef]
- Kalil, A.C.; Patterson, T.F.; Mehta, A.K.; Tomashek, K.M.; Wolfe, C.R.; Ghazaryan, V.; Marconi, V.C.; Ruiz-Palacios, G.M.; Hsieh, L.; Kline, S.; et al. Baricitinib plus Remdesivir for Hospitalized Adults with COVID-19. N. Engl. J. Med. 2021, 384, 795–807. [Google Scholar] [CrossRef]
- Wolfe, C.R.; Tomashek, K.M.; Patterson, T.F.; Gomez, C.A.; Marconi, V.C.; Jain, M.K.; Yang, O.O.; I Paules, C.; Palacios, G.M.R.; Grossberg, R.; et al. Baricitinib versus dexamethasone for adults hospitalised with COVID-19 (ACTT-4): A randomised, double-blind, double placebo-controlled trial. Lancet Respir. Med. 2022, 10, 888–899. [Google Scholar] [CrossRef]
- Chow, C.K.; Atkins, E.R.; Hillis, G.S.; Nelson, M.R.; Reid, C.M.; Schlaich, M.P.; Hay, P.; Rogers, K.; Billot, L.; Burke, M.; et al. Initial treatment with a single pill containing quadruple combination of quarter doses of blood pressure medicines versus standard dose monotherapy in patients with hypertension (QUARTET): A phase 3, randomised, double-blind, active-controlled trial. Lancet 2021, 398, 1043–1052. [Google Scholar] [CrossRef]
- Castellano, J.M.; Pocock, S.J.; Bhatt, D.L.; Quesada, A.J.; Owen, R.; Fernandez-Ortiz, A.; Sanchez, P.L.; Ortuño, F.M.; Rodriguez, J.M.V.; Domingo-Fernández, A.; et al. Polypill Strategy in Secondary Cardiovascular Prevention. N. Engl. J. Med. 2022, 387, 967–977. [Google Scholar] [CrossRef]
- Basco, E.; Furlong, A.; Pfahler, L. Four health organizations, working closely together, spent almost $10 billion on responding to COVID across the world. But they lacked the scrutiny of governments and fell short of their own goals, a POLITICO and WELT investigation found. Politico 2022. [Google Scholar] [CrossRef]
- Pawlos, A.; Niedzielski, M.; Gorzelak-Pabiś, P.; Broncel, M.; Woźniak, E. COVID-19: Direct and Indirect Mechanisms of Statins. Int. J. Mol. Sci. 2021, 22, 4177. [Google Scholar] [CrossRef] [PubMed]
- Silva, L.F.; Ravi, R.; Vangipurapu, J.; Laakso, M. Metabolite Signature of Simvastatin Treatment Involves Multiple Metabolic Pathways. Metabolites 2022, 12, 753. [Google Scholar] [CrossRef] [PubMed]
- Thomas, G.; Hraiech, S.; Loundou, A.; Truwit, J.; Kruger, P.; McAuley, D.; Papazian, L.; Roch, A. Statin therapy in critically-ill patients with severe sepsis: A review and meta-analysis of randomized clinical trials. Minerva Anestesiol. 2015, 81, 921–930. [Google Scholar] [PubMed]
- McAuley, D.F.; Laffey, J.G.; O’Kane, C.M.; Perkins, G.D.; Mullan, B.; Trinder, T.J.; Johnston, P.; A Hopkins, P.; Johnston, A.J.; Murphy, L.; et al. Simvastatin to reduce pulmonary dysfunction in patients with acute respiratory distress syndrome: The HARP-2 RCT. Effic. Mech. Eval. 2018, 5, 1–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baddeley, M. Herding, social influences and behavioural bias in scientific research. EMBO Rep. 2015, 16, 902–905. [Google Scholar] [CrossRef] [Green Version]
- Baddeley, M. Experts in policy land–insights from behavioural economics on improving experts’ advice for policy-makers. J. Behav. Econ. Policy 2017, 1, 27–31. Available online: http://sabeconomics.org/journal/RePEc/beh/JBEPv1/articles/ (accessed on 23 September 2019).
- Weingart, P.; van Schalkwyk, F.; Guenther, L. Democratic and expert legitimacy: Science, politics and the public during the COVID-19 pandemic. Sci. Public Policy 2022, 49, 499–517. [Google Scholar] [CrossRef]
- Phillips, N. The coronavirus is here to stay–here’s what that means. Nature 2021, 590, 382–384. [Google Scholar] [CrossRef]
- Callaway, E. Beyond Omicron: What’s next for COVID’s viral evolution. Nature 2021, 600, 204–207. [Google Scholar] [CrossRef]
- Spicer, A.J.; Jalkanen, S. Why Haven’t We Found an Effective Treatment for COVID-19? Front. Immunol. 2021, 12, 644850. [Google Scholar] [CrossRef]
- Hillis, S.; N’Konzi, J.-P.N.; Msemburi, W.; Cluver, L.; Villaveces, A.; Flaxman, S.; Unwin, H.J.T. Orphanhood and Caregiver Loss Among Children Based on New Global Excess COVID-19 Death Estimates. JAMA Pediatr. 2022, 176, 1145. [Google Scholar] [CrossRef]
- Levin, A.T.; Owusu-Boaitey, N.; Pugh, S.; Fosdick, B.K.; Zwi, A.B.; Malani, A.; Soman, S.; Besançon, L.; Kashnitsky, I.; Ganesh, S.; et al. Assessing the burden of COVID-19 in developing countries: Systematic review, meta-analysis and public policy implications. BMJ Glob. Health 2022, 7, e008477. [Google Scholar] [CrossRef] [PubMed]
- Sachs, J.D.; Karim, S.S.A.; Aknin, L.; Allen, J.; Brosbøl, K.; Colombo, F.; Barron, G.C.; Espinosa, M.F.; Gaspar, V.; Gaviria, A.; et al. The Lancet Commission on lessons for the future from the COVID-19 pandemic. Lancet 2022, 400, 1224–1280. [Google Scholar] [CrossRef] [PubMed]
- Fedson, D.S. Clinician-initiated research on treating the host response to pandemic influenza. Hum. Vaccines Immunother. 2017, 14, 790–795. [Google Scholar] [CrossRef] [PubMed]
- Angus, D.C. Fusing Randomized Trials with Big Data. JAMA 2015, 314, 767–768. [Google Scholar] [CrossRef]
- Frakt, A.B. An Observational Study Goes Where Randomized Clinical Trials Have Not. JAMA 2015, 313, 1091–1092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lyman, G.H.; Kuderer, N.M. Randomized Controlled Trials Versus Real-World Data in the COVID-19 Era: A False Narrative. Cancer Investig. 2020, 38, 537–542. [Google Scholar] [CrossRef]
- Lim, H.-S.; Lee, S.; Kim, J.H. Real-world-evidence versus randomized controlled trials: Clinical research based on electronic medical records. J. Korean Med. Sci. 2018, 33, e213. [Google Scholar] [CrossRef]
- Randomization versus Real-World Evidence. N. Engl. J. Med. 2020, 383, e22351. [CrossRef]
- Forbes, S.P.; Dahabreh, I.J. Benchmarking Observational Analyses Against Randomized Trials: A Review of Studies Assessing Propensity Score Methods. J. Gen. Intern. Med. 2020, 35, 1396–1404. [Google Scholar] [CrossRef]
- Greenhalgh, T. Miasmas, mental models and preventive public health: Some philosophical reflections on science in the COVID-19 pandemic. Interface Focus 2021, 11, 20210017. [Google Scholar] [CrossRef] [PubMed]
- Hernán, M.A. Methods of Public Health Research—Strengthening Causal Inference from Observational Data. N. Engl. J. Med. 2021, 385, 1345–1348. [Google Scholar] [CrossRef] [PubMed]
- Greenhalgh, T.; Fisman, D.; Cane, D.J.; Oliver, M.; Macintyre, C.R. Adapt or die: How the pandemic made the shift from EBM to EBM+ more urgent. BMJ Evid.-Based Med. 2022, 27, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Franklin, J.M.; Platt, R.; Dreyer, N.A.; London, A.J.; Simon, G.E.; Watanabe, J.H.; Horberg, M.; Hernandez, A.; Califf, R.M. When Can Nonrandomized Studies Support Valid Inference Regarding Effectiveness or Safety of New Medical Treatments? Clin. Pharmacol. Ther. 2021, 111, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; E Pennini, M.; Bergmann, J.N.; Kozak, M.L.; Herring, K.; Sciarretta, K.L.; Armstrong, K.L. Applying Lessons Learned From COVID-19 Therapeutic Trials to Improve Future ALI/ARDS Trials. Open Forum Infect. Dis. 2022, 9, ofac381. [Google Scholar] [CrossRef] [PubMed]
- Gerstein, H.C.; McMurray, J.; Holman, R.R. Real-world studies no substitute for RCTs in establishing efficacy. Lancet 2019, 393, 210–211. [Google Scholar] [CrossRef]
- Collins, R.; Bowman, L.; Landray, M.; Peto, R. The Magic of Randomization versus the Myth of Real-World Evidence. N. Engl. J. Med. 2020, 382, 674–678. [Google Scholar] [CrossRef]
- Ioannidis, J.P. High-cited favorable studies for COVID-19 treatments ineffective in large trials. J. Clin. Epidemiol. 2022, 148, 1–9. [Google Scholar] [CrossRef]
- Wendler, D.; Anjum, S.; Williamson, P. Innovative treatment as a precursor to clinical research. J. Clin. Investig. 2021, 131, e152573. [Google Scholar] [CrossRef]
- Frieden, T.R. Evidence for Health Decision Making—Beyond Randomized, Controlled Trials. N. Engl. J. Med. 2017, 377, 465–475. [Google Scholar] [CrossRef]
- Fedson, D.S. The unforgiving arithmetic of pandemic. L’Osseratore Romano 2009, 28, 9. [Google Scholar]
- Hastie, C.E.; Lowe, D.J.; McAuley, A.; Winter, A.J.; Mills, N.L.; Black, C.; Scott, J.T.; O’Donnell, C.A.; Blane, D.N.; Browne, S.; et al. Outcomes among confirmed cases and a matched comparison group in the Long-COVID in Scotland study. Nat. Commun. 2022, 13, 5663. [Google Scholar] [CrossRef] [PubMed]
- Frere, J.J.; Serafini, R.A.; Pryce, K.D.; Zazhytska, M.; Oishi, K.; Golynker, I.; Panis, M.; Zimering, J.; Horiuchi, S.; Hoagland, D.A.; et al. SARS-CoV-2 infection in hamsters and humans results in lasting and unique systemic perturbations after recovery. Sci. Transl. Med. 2022, 14, abq3059. [Google Scholar] [CrossRef]
- Wallis, R.S.; O’Garra, A.; Sher, A.; Wack, A. Host-directed immunotherapy of viral and bacterial infections: Past, present and future. Nat. Rev. Immunol. 2022, 23, 121–133. [Google Scholar] [CrossRef] [PubMed]
- van de Veerdonk, F.L.; Giamarellos-Bourboulis, E.; Pickkers, P.; Derde, L.; Leavis, H.; van Crevel, R.; Engel, J.J.; Wiersinga, W.J.; Vlaar, A.P.J.; Shankar-Hari, M.; et al. A guide to immunotherapy for COVID-19. Nat. Med. 2022, 28, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Medzhitov, R.; Schneider, D.S.; Soares, M.P. Disease Tolerance as a Defense Strategy. Science 2012, 335, 936–941. [Google Scholar] [CrossRef] [Green Version]
- Yoshida, M.; Worlock, K.B.; Ni Huang, N.; Lindeboom, R.G.H.; Butler, C.R.; Kumasaka, N.; Conde, C.D.; Mamanova, L.; Bolt, L.; Richardson, L.; et al. Local and systemic responses to SARS-CoV-2 infection in children and adults. Nature 2021, 602, 321–327. [Google Scholar] [CrossRef]
- Maughan, E.F.; Hynds, R.E.; Pennycuick, A.; Nigro, E.; Gowers, K.H.; Denais, C.; Gómez-López, S.; Lazarus, K.A.; Orr, J.C.; Pearce, D.R.; et al. Cell-intrinsic differences between human airway epithelial cells from children and adults. iScience 2022, 25, 105409. [Google Scholar] [CrossRef]
- Schulman, A. Why Many Americans Turned on Anthony Fauci. The New York Times, 30 August 2022. [Google Scholar]
Figure 1.
The relationship between disease stage and treatment for patients with COVID-19. Adapted from Ref. [66]. After SARS-CoV2 infection, the virus replicates and reaches peak levels during stage 1, after which levels steadily decline. As they decline, the host inflammatory response increases (the hyperinflammatory phase). This response eventually decreases and recovery begins. The relationships among these factors and the clinical course of the infection dictates which of the two defence strategies will be more effective. Before infection, avoidance is the best defence strategy. After infection, patients will be in a presymptomatic phase of the infection, which is followed by stage 1 with fever, malaise and other mild symptoms. Virus levels peak and then decline as patients exit stage I, independently of whether they will recover or progress to a severe or critical stage of infection. Antiviral drugs are more effective for asymptomatic individuals and patients in stage 1. By stages 2 and 3, the host inflammatory response drives the disease. If patients survive, the host inflammatory response subsides, resolution begins, and patients proceed toward recovery in stage 4. Drugs that treat the host response are more effective for patients in stage 4. Patients whose disease severity peaks in stages 1 or 2 can bypass later stages and enter directly into the recovery phase.
Figure 1.
The relationship between disease stage and treatment for patients with COVID-19. Adapted from Ref. [66]. After SARS-CoV2 infection, the virus replicates and reaches peak levels during stage 1, after which levels steadily decline. As they decline, the host inflammatory response increases (the hyperinflammatory phase). This response eventually decreases and recovery begins. The relationships among these factors and the clinical course of the infection dictates which of the two defence strategies will be more effective. Before infection, avoidance is the best defence strategy. After infection, patients will be in a presymptomatic phase of the infection, which is followed by stage 1 with fever, malaise and other mild symptoms. Virus levels peak and then decline as patients exit stage I, independently of whether they will recover or progress to a severe or critical stage of infection. Antiviral drugs are more effective for asymptomatic individuals and patients in stage 1. By stages 2 and 3, the host inflammatory response drives the disease. If patients survive, the host inflammatory response subsides, resolution begins, and patients proceed toward recovery in stage 4. Drugs that treat the host response are more effective for patients in stage 4. Patients whose disease severity peaks in stages 1 or 2 can bypass later stages and enter directly into the recovery phase.


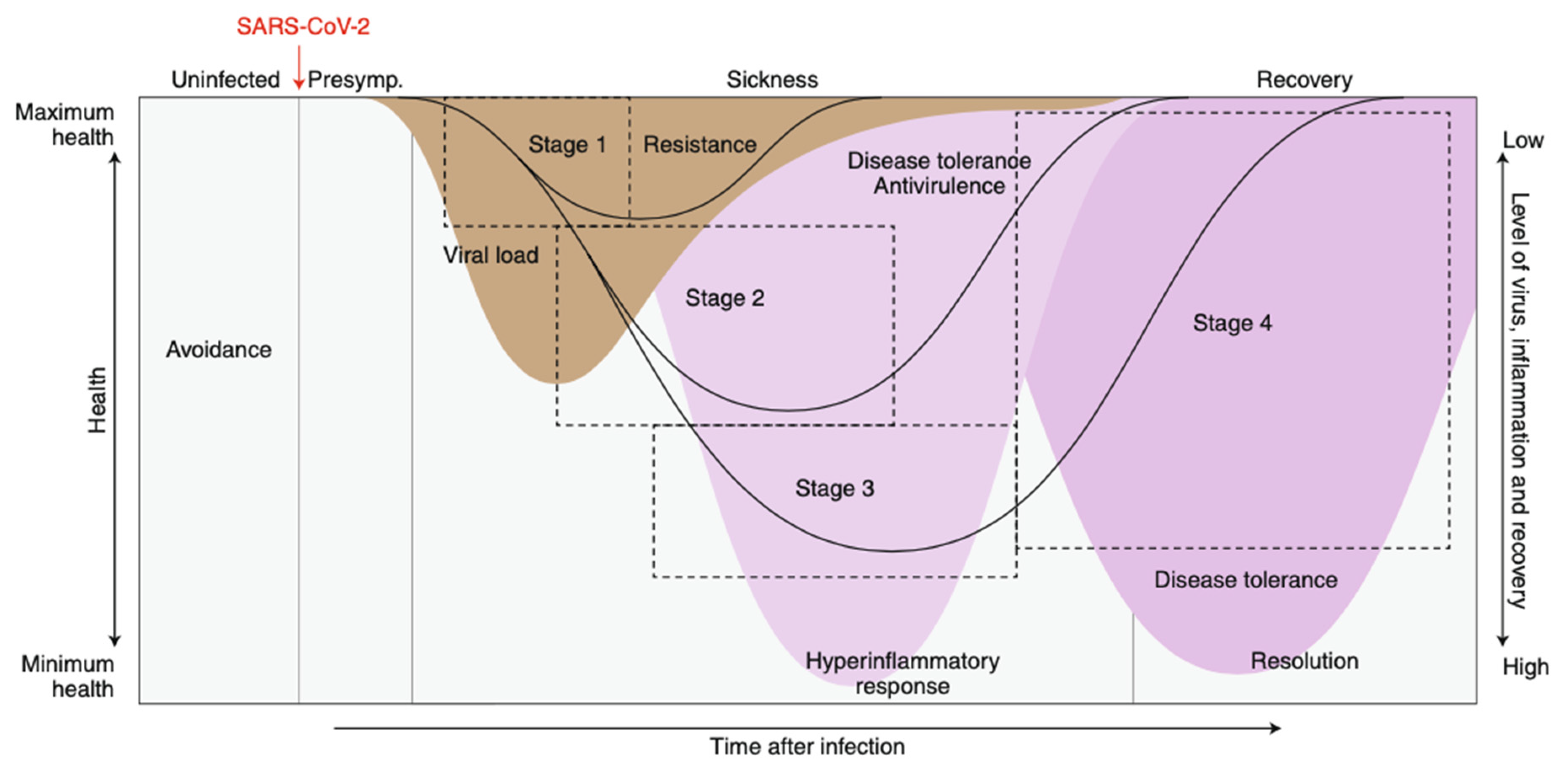{kind=link}
Table 1.
Strengths and limitations of RCTs and observational studies.
| RCTs | Observational Studies | |
|---|---|---|
| Strengths | Randomization balances baseline characteristics | Rigor is enhanced by specific methods |
| “Prospective” infrastructure collects pertinent data | Observational studies and RCTs with the same focus provide consistent results | |
| Analytic methods are simple and straightforward | Treatments evaluated in large populations can be shown to be safe and effective | |
| Limitations | Individual RCTs are often contradictory | Baseline characteristics are usually not well balanced |
| Meta-analyses and large trials often disagree | Data quality can be variable | |
| Limited generalizability | Analytical methods can be complex and obscure |
Adapted from Ref. [67].
Table 2.
Summary of guidelines for the use of treatments for acute COVID-19.
| Treatment Guidelines | NIH Guidelines | ERS Guidelines |
|---|---|---|
| Antiviral Treatments Targeting the SARS-CoV-2 Virus | ||
| HCQ/CQ | Not recommended | Strongly not recommended |
| Remdesivir | Recommended | Conditionally recommended |
| Favipiravir | Not mentioned | Not mentioned |
| Convalescent plasma | Not recommended | Not recommended |
| Ivermectin | Not recommended | Strongly not recommended |
| Interferon–1β | Not mentioned | Conditionally not recommended |
| Pegylated interferon-lambda | Not mentioned | Not mentioned |
| Monoclonal antibodies specific for the anti-SARS-CoV-2 spike protein | Not mentioned | Recommended |
| Paxlovid (Ritonavir-boosted nirmatrelvir | Recommended | Not mentioned |
| Molnupiravir | Weakly recommended | Not mentioned |
| Colchicine | Not recommended | Strongly not recommended |
| Immunomodulators targeting the host response to infection | ||
| Corticosteroids | Recommended, requiring O2 treatment only | Strongly recommended |
| mAb—IL-1 receptor antagonist | Not recommended * | Conditionally not recommended |
| mAb—IL-6 receptor antagonist | Recommended | Strongly recommended |
| Fluvoxamine (SSRI) | Not recommended * | Not mentioned |
| Janus kinase inhibitors | Strongly recommended | Strongly recommended |
| Tyrosine kinase inhibitors | Not recommended * | Not mentioned |
| Anticoagulation (LMWH) | Recommended | Strongly recommended |
| Azithromycin | Not recommended | Not mentioned |
| Azithromycin + HCQ | Not recommended | Not mentioned |
| Inexpensive generic drugs targeting the host response | ||
| Metformin | Not recommended * | Not mentioned |
| PPARα, PPARγ agonists | Not mentioned | Not mentioned |
| Statins, ACE inhibitors, ARBs | Not mentioned except for continuing treatment | Not mentioned |
Adapted from Refs. [77,78,79]. Abbreviations: NIH = National Institutes of Health; ERS = European Respiratory Society; HCQ = hydroxychloroquine; CQ = chloroquine; mAb = monoclonal antibody; Paxlovid = ritonavir-boosted nirmatrelvir; SSRI = selective serotonin uptake inhibitor; Not recommended * = Not recommended except when used in a clinical trial; LMWH = low molecular weight heparin; PPAR = peroxisome proliferator activator receptor; ACE = angiotensin converting enzyme; ARB = angiotensin receptor blocker.
Table 3.
Beneficial effects of statin, ACE inhibitor or ARB treatment on biomarkers of inflammation and endothelial barrier integrity.
Table 3.
Beneficial effects of statin, ACE inhibitor or ARB treatment on biomarkers of inflammation and endothelial barrier integrity.
| Biomarker | Improve Inflammation/ Endothelial Barrier Integrity | Biomarker | Improve Inflammation/ Endothelial Barrier Integrity | Biomarker | Improve Inflammation/ Endothelial Barrier Integrity | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Statin | ACEi | ARB | Statin | ACEi | ARB | Statin | ACEi | ARB | |||
| Tyrosine kinase | yes | yes | yes | PAF | yes | yes | yes | PPAR α | yes | yes | yes |
| Janus kinase | yes | yes | yes | PAR-1/PAR-2 | yes | yes | yes | PPAR γ | yes | yes | yes |
| IL-1 | yes | yes | yes | α7 nicotinic aCh receptor | yes | yes | yes | ||||
| IL-4 | yes | yes | yes | ROS | yes | yes | yes | RAGE | yes | yes | yes |
| IL-6 | yes | yes | yes | β-arrestin | yes | yes | yes | Ferritin | yes | yes | yes |
| IL-10 | yes | yes | yes | Inflammasome | yes | yes | yes | Mitochondria | yes | yes | yes |
| IL-17 | yes | yes | yes | AMPK | yes | yes | yes | HO-1 | yes | yes | yes |
| TNF | yes | yes | yes | MAPK/Akt | yes | yes | yes | KLF4 | yes | yes | yes |
| HMBG1 | yes | yes | yes | MCP-1 | yes | yes | yes | ||||
| Lipoxin A4 | yes | yes | yes | FOXP3 | yes | yes | yes | Angpt2/ Tie2 | yes | yes | yes |
| T regs | yes | yes | yes | ACE2 | yes | yes | yes | ||||
| HMBG1 | yes | yes | yes | NADPH oxidase | yes | yes | yes | eNOS/ iNOS | yes | yes | yes |
| Thrombomodulin | yes | yes | yes | Interferon | yes | yes | yes | VCAM-1/ ICAM-1 | yes | yes | yes |
| Thromboxane A2 | yes | yes | yes | TGF-β1 | yes | yes | yes | VE- cadherin | yes | yes | yes |
| t-PA | yes | yes | yes | hs CRP | yes | yes | yes | Actin cytoskeleton | yes | yes | yes |
| P-selectin/ E-selectin | yes | yes | yes | mTOR | yes | yes | yes | VEGF | yes | yes | yes |
| PAI-1 | yes | yes | yes | Adiponectin | yes | yes | yes | Bradykinin | yes | yes | yes |
Adapted from Ref. [22] and updated. The biomarkers shown in this table are representative and do not include all that affect inflammation or endothelial barrier integrity. Inflammatory biomarkers and endothelial barrier disruptors and protectors are signaling molecules or pathways. Beneficial treatment by statins, ACE inhibitors (ACEis) or angiotensin receptor blockers (ARBs) is defined as either up regulation or down regulation in cell signaling pathways that reduce inflammation and/or improve endothelial barrier integrity. This is indicated by “yes in the table. The literature for each agent on each biomarker in Table 3 is extensive and individual articles have not been cited. Three documents showing selected citations and abstracts for these articles are available from the author (davidsfedson@gmail.com). Abbreviations: α7 nicotinic aCh receptor = alpha7 nicotinic acetylcholinesterase receptor; ACE2 = angiotensin converting enzyme-2; Angpt = angiopoietin; AMPK = adenosine monophosphate kinase; C = complement; eNOS/iNOS = endothelial/inducible nitric oxide synthase; FOXP3 = fork head box P3; HMGB1 = high mobility group box 1; hsCRP = highly sensitive C-reactive protein; HO-1 = heme oxygenase-1; IL-1 = interleukin 1; IL-4 = interleukin 4; IL-6 = interleukin 6; IL-10 = interleukin 10; IL-17 = interleukin 17; KLF4 = Kruppel-like factor 4; MAPK/Akt = mitogen-activated protein kinase/three members of the serine/threonine protein kinase family; MCP-1 = monocyte chemoattractant protein-1; MMPs = matrix metalloproteinases; mTOR = mechanistic target of rapamycin kinase; PAF = platelet activating factor; PAI-1 = plasminogen activator inhibitor-1; PAR = protease activator receptor; PPARα = peroxisome proliferative activated receptor alpha; PPARγ = peroxisome proliferative activated receptor gamma; P-selectin = platelet selectin; E-selectin = endothelial selectin; RAGE = receptor for advanced glycation end products; ROS = reactive oxygen species; TGF-β1 = transforming growth factor-β1; tPA = tissue plasminogen activator; Treg = regulatory T cells; TNF = tumor necrosis factor; VCAM-1/ICAM-1 = vascular/intercellular adhesion molecule-1; VE-cadherin = vascular endothelial cadherin; VEGF = vascular endothelial growth factor.
Table 4.
Twenty-two observational studies and six RCTs of inpatient statin treatment and its effectiveness in reducing 28–30-day mortality.
Table 4.
Twenty-two observational studies and six RCTs of inpatient statin treatment and its effectiveness in reducing 28–30-day mortality.
| Study (Ref.) | Methods | No. of Statin Users | Adjusted OR/HR | 95% CI | p Value |
|---|---|---|---|---|---|
| Zhang [182] | PSM (4:1), CCS | 1219 | 0.58 | 0.43–0.80 | 0.001 |
| Rodriguez-Nava [183] | ICU only, cohort, Cox regression | ns | 0.38 | 0.18–0.77 | 0.008 |
| Mallow [184] | Cohort, multivariate regression | 5313 | 0.54 | 0.49–0.60 | <0.001 |
| Saeed [185] | Diabetes mellitus, multivariate regression | 982 | 0.51 | 0.43–0.61 | <0.001 |
| PSM (1:1), IPTW *, diabetes vs. no DM, | 0.88 | 0.84–0.91 | <0.001 | ||
| Lala [186] | Adjusted for HRC, ACEi/ARB | 984 | 0.57 | 0.47–0.69 | <0.001 |
| Fan [187] | PSM (1:1), cohort | 250 | 0.25 | 0.07–0.92 | 0.037 |
| Rossi [188] | Observational study, compares only lipophilic/hydrophilic statins; no adjustment for HRC or other risk variables | 42 | ns | - | 0.025 |
| Torres-Pena [189] | PSM (1:1), statins continued vs. withdrawal **, mixed effect logistic regression | 1130 | 0.67 | 0.54–0.84 | <0.001 |
| Byttebier [26] | PSM (1:1), CCS | 297 | 0.56 | 0.39–0.93 | 0.020 |
| Terleki [190] | Logistic regression | ns | 0.54 | 0.33–0.84 | 0.008 |
| Lohia [191] | PSM (1:1), cohort | 250 | 0.47 | 0.32–0.70 | <0.001 |
| Choi [192] | Cox regression, high intensity statin | 843 | 0.53 | 0.43–0.65 | not done |
| Davoodi [199] | RCT, atorvastatin, 20 mg for 5 days | 20 | no deaths | - | - |
| Shen [193] | PSM (1:1), logistic regression | 404 | 0.47 | 0.29–0.77 | <0.001 |
| Ayeh [194] | PSM (1:1), Cox regression | 594 | 0.92 | 0.53–1.59 | ns |
| Masana [195] | GM (1:1) | 336 | 0.60 | 0.39–0.92 | 0.020 |
| Memel [169] | marginal structural Cox regression, IPTW, statin treatment vs. no treatment | 777 | 0.57 | 0.37–0.86 | 0.008 |
| statins continued vs. withdrawal *** | - | 0.27 | 0.11–0.64 | 0.003 | |
| Matli [200] | RCT, Cox regression, atorvastatin 20 mg + other drugs | 17 | 1.43 | 0.28–13.16 | 0.644 |
| Ghafoori [201] | RCT, Cox regression, atorvastatin 20 mg | 76 | ns (multiple outcomes including ICU admissions and deaths | ns | 0.27 |
| I.S.Investigators [202] | RCT, ICU, atorvastatin 20 mg | 210 | 0.84 | 0.58–1.22 | 0.39 |
| Gaitan-Duarte [203] | RCT, rosuvastatin 40 mg + other drugs | 159 | 0.53 | 0.29–0.56 | 0.038 |
| Kuno [196] | PSM (1:1), statins continued vs. withdrawal | 671 | 0.53 | 0.41–0.62 | <0.001 |
| Li [197] | PSM (1:1) | 3359 | 0.72 | 0.64–0.80 | <0.001 |
| Kouhpeikar [198] | Cox regression, composite outcome (mortality, ICU, ventilation) | 162 | 0.57 | 0.33–0.99 | 0.048 |
| Andrews [170] | Logistic regression | 26,893 | 0.72 | 0.68–0.77 | <0.001 |
| Al Harbi [158] | PSM (1:1), ICU, Cox proportional hazard regression | 198 | 0.72 | 0.54–0.97 | 0.030 |
| Al-Sulaiman [205] | PSM (1:1), ICU, Cox proportional hazard regression | 251 | 0.75 | 0.58–0.98 | 0.03 |
| Hejazi [204] | RCT | 26 | ns (mortality was twice as high in control patients) | ns | ns |
Adapted from Ref. [27] and updated. Abbreviations: CCS = case-control study; CI = confidence interval; GM = genetics-matched; HR = hazard ratio; HRC = high risk conditions; ICU = intensive care unit; IPTW = inverse probability treatment weighted; ns = not stated or not significant; OR = odds ratio; PSM = propensity score-matched; RCT = randomized controlled trial. * The PS matched IPTW cohort analysis included demographic and comorbidity factors, clinical and laboratory test values, and the use of ACE inhibitors and angiotensin receptor blockers. ** Statin treatment continued after hospital admission versus statin withdrawal; conditional logistic regression. *** Statin treatment continued after hospital admission versus statin withdrawal; marginal structural Cox model.
Table 5.
A research agenda for clinicians in treating the host response to COVID-19 and other pandemic illnesses.
Table 5.
A research agenda for clinicians in treating the host response to COVID-19 and other pandemic illnesses.
| Choose Drugs That Are |
|
| Plan Clinical studies of Host Response Treatment |
|
| Plan What to Do with the Results |
|
Adapted from Ref. [25] and updated.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Fedson, D.S. Treating COVID-19: Targeting the Host Response, Not the Virus. Life 2023, 13, 712. https://doi.org/10.3390/life13030712
AMA Style
Fedson DS. Treating COVID-19: Targeting the Host Response, Not the Virus. Life. 2023; 13(3):712. https://doi.org/10.3390/life13030712
Chicago/Turabian StyleFedson, David S. 2023. "Treating COVID-19: Targeting the Host Response, Not the Virus" Life 13, no. 3: 712. https://doi.org/10.3390/life13030712
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.