
Polycystic Ovary Syndrome and Gut Microbiota: Phenotype Matters
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Methods
3. Results
3.1. The Study Participants’ Characteristics
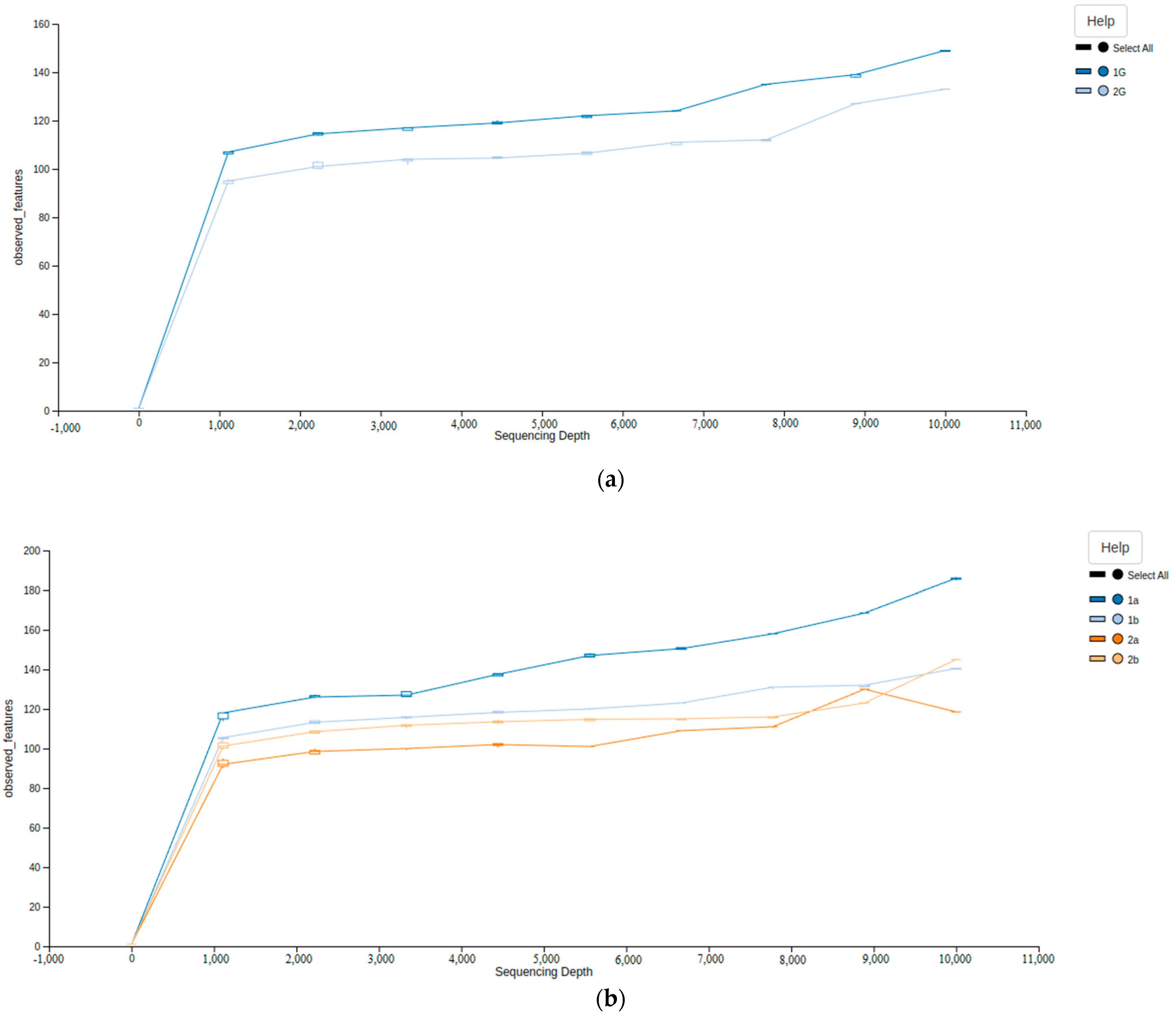
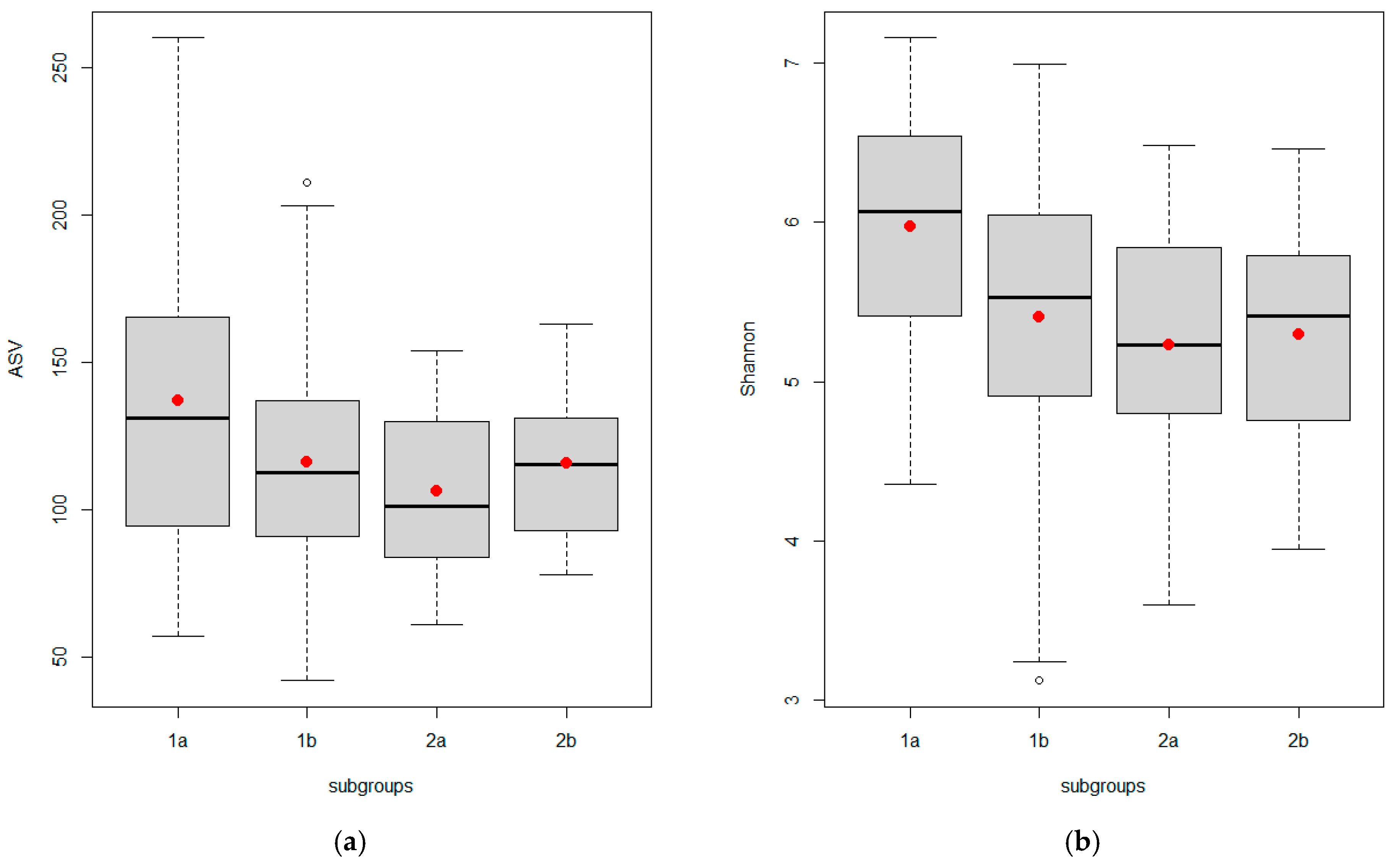
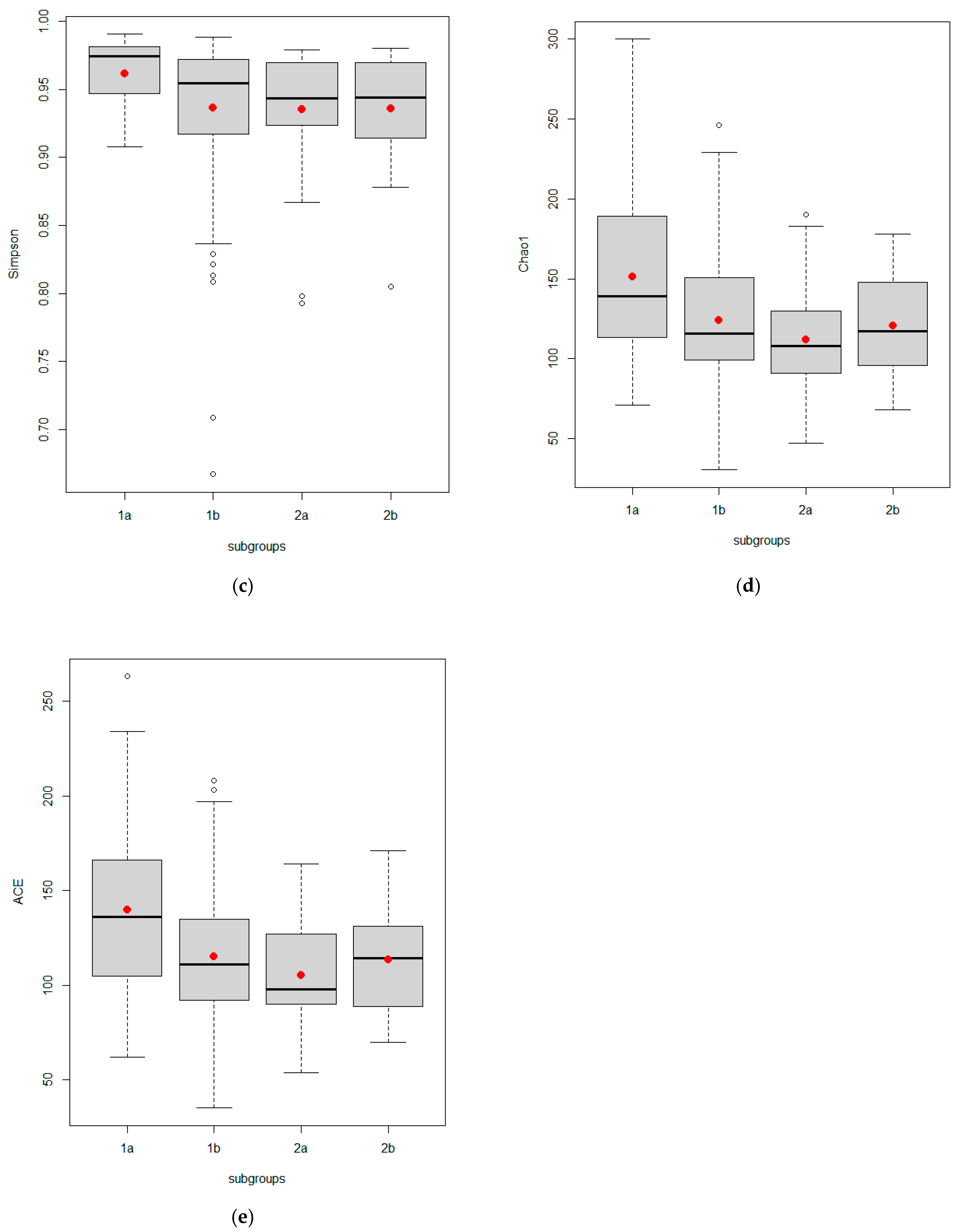
3.2. Differences in Alpha Diversity of Gut Microbiota According to Study Group and Subgroups
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 17-OHP | 17-hydroxyprogesterone |
| ACE | Abundance-based Coverage Estimator |
| AFC | Antral Follicle Count |
| AMH | Anti-Mullerian Hormone |
| ASV | Amplicon sequence variant |
| BMI | Body mass index |
| DHEAS | Dehydroepiandrosterone |
| DOGMA | Dysbiosis of gut microbiota |
| ESPEP | Eastern Siberia PCOS Epidemiology & Phenotype |
| FAI | Free Androgen Index |
| FSH | Follicle-Stimulating Hormone |
| HA | Hyperandrogenism |
| HRT | Hormone therapy |
| IFG | Impaired fasting glycaemia |
| IGT | Impaired glucose tolerance |
| LH | Luteinizing Hormone |
| LNG-IUD | Levonorgestrel intrauterine device |
| mF-G | modified Ferriman–Gallwey score for hirsutism |
| NC-CAH | Nonclassical congenital adrenal hyperplasia |
| OCP | Oral contraceptive pills |
| OUT | Operational Taxonomic Unit |
| PCOS | Polycystic ovary syndrome |
| PCOM | Polycystic ovarian morphology |
| REDCap | Research Electronic Data Capture |
| rRNA | ribosomal RNA |
| SHBG | Sex-Hormone-Binding Globulin |
| TSH | Thyroid-Stimulating Hormone |
| TT | Total Testosterone |
| U/S | Ultrasound |
| UNL | Upper Normal Limits |
| WC | Waist Circumference |
References
- Belenkaia, L.V.; Lazareva, L.M.; Walker, W.; Lizneva, D.V.; Suturina, L.V. Criteria, phenotypes and prevalence of polycystic ovary syndrome. Minerva Ginecol. 2019, 71, 211–223. [Google Scholar] [CrossRef]
- Suturina, L. The Epidemiology of Polycystic Ovary Syndrome. In Polycystic Ovary Syndrome, 3rd ed.; Kovacs, G.T., Fauser, B., Legro, R.S., Eds.; Cambridge University Press: Cambridge, UK, 2022; pp. 21–28. [Google Scholar] [CrossRef]
- Cho, I.; Blaser, M.J. The human microbiome: At the interface of health and disease. Nat. Rev. Genet. 2012, 13, 260–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kho, Z.Y.; Lal, S.K. The Human Gut Microbiome—A Potential Controller of Wellness and Disease. Front. Microbiol. 2018, 9, 1835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armour, C.R.; Nayfach, S.; Pollard, K.S.; Sharpton, T.J. A Metagenomic Meta-analysis Reveals Functional Signatures of Health and Disease in the Human Gut Microbiome. mSystems 2019, 4, e00332-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tremellen, K.; Pearce, K. Dysbiosis of gut microbiota (DOGMA)—A novel theory for the development of polycystic ovarian syndrome. Med. Hypotheses 2012, 79, 104–112. [Google Scholar] [CrossRef]
- Lindheim, L.; Bashir, M.; Münzker, J.; Trummer, C.; Zachhuber, V.; Leber, B.; Horvath, A.; Pieber, T.R.; Gorkiewicz, G.; Stadlbauer, V.; et al. Alterations in Gut Microbiome Composition and Barrier Function Are Associated with Reproductive and Metabolic Defects in Women with Polycystic Ovary Syndrome (PCOS): A Pilot Study. PLoS ONE 2017, 12, e0168390. [Google Scholar] [CrossRef] [Green Version]
- Liu, R.; Zhang, C.; Shi, Y.; Zhang, F.; Li, L.; Wang, X.; Ling, Y.; Fu, H.; Dong, W.; Shen, J.; et al. Dysbiosis of Gut Microbiota Associated with Clinical Parameters in Polycystic Ovary Syndrome. Front. Microbiol. 2017, 8, 324. [Google Scholar] [CrossRef]
- Insenser, M.; Murri, M.; Del Campo, R.; Ángeles Martínez-García, M.; Fernández-Durán, E.; Escobar-Morreale, H.F. Gut Microbiota and the Polycystic Ovary Syndrome: Influence of Sex, Sex Hormones, and Obesity. J. Clin. Endocrinol. Metab. 2018, 103, 2552–2562. [Google Scholar] [CrossRef]
- Torres, P.J.; Siakowska, M.; Banaszewska, B.; Pawelczyk, L.; Duleba, A.J.; Kelley, S.T.; Thackray, V.G. Gut Microbial Diversity in Women With Polycystic Ovary Syndrome Correlates With Hyperandrogenism. J. Clin. Endocrinol. Metab. 2018, 103, 1502–1511. [Google Scholar] [CrossRef]
- Qi, X.; Yun, C.; Sun, L.; Xia, J.; Wu, Q.; Wang, L.; Wang, L.; Zhang, Y.; Liang, X.; Wang, L.; et al. Gut microbiota–bile acid–interleukin-22 axis orchestrates polycystic ovary syndrome. Nat. Med. 2019, 25, 1225–1233. [Google Scholar] [CrossRef]
- Zeng, B.; Lai, Z.; Sun, L.; Zhang, Z.; Yang, J.; Li, Z.; Lin, J.; Zhang, Z. Structural and functional profiles of the gut microbial community in polycystic ovary syndrome with insulin resistance (IR-PCOS): A pilot study. Res. Microbiol. 2019, 170, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Sun, Z.; Jiang, S.; Bai, X.; Ma, C.; Peng, Q.; Chen, K.; Chang, H.; Fang, T.; Zhang, H. Probiotic Bifidobacterium lactis V9 Regulates the Secretion of Sex Hormones in Polycystic Ovary Syndrome Patients through the Gut-Brain Axis. mSystems 2019, 4, e00017-19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, W.; Han, Q.; Xu, J.; Wang, J.; Sun, Y.; Li, W.; Chen, Z.J.; Du, Y. Metagenomic analysis identified microbiome alterations and pathological association between intestinal microbiota and polycystic ovary syndrome. Fertil. Steril. 2020, 113, 1286–1298.e4. [Google Scholar] [CrossRef] [PubMed]
- Eyupoglu, N.D.; Ergunay, K.; Acikgoz, A.; Akyon, Y.; Yilmaz, E.; Yildiz, B.O. Gut Microbiota and Oral Contraceptive Use in Overweight and Obese Patients with Polycystic Ovary Syndrome. J. Clin. Endocrinol. Metab. 2020, 105, dgaa600. [Google Scholar] [CrossRef]
- Haudum, C.; Lindheim, L.; Ascani, A.; Trummer, C.; Horvath, A.; Münzker, J.; Obermayer-Pietsch, B. Impact of Short-Term Isoflavone Intervention in Polycystic Ovary Syndrome (PCOS) Patients on Microbiota Composition and Metagenomics. Nutrients 2020, 12, 1622. [Google Scholar] [CrossRef]
- Jobira, B.; Frank, D.N.; Pyle, L.; Silveira, L.J.; Kelsey, M.M.; Garcia-Reyes, Y.; Robertson, C.E.; Ir, D.; Nadeau, K.J.; Cree-Green, M. Obese Adolescents With PCOS Have Altered Biodiversity and Relative Abundance in Gastrointestinal Microbiota. J. Clin. Endocrinol. Metab. 2020, 105, e2134–e2144. [Google Scholar] [CrossRef]
- Liang, Y.; Ming, Q.; Liang, J.; Zhang, Y.; Zhang, H.; Shen, T. Gut microbiota dysbiosis in polycystic ovary syndrome: Association with obesity—A preliminary report. Can. J. Physiol. Pharmacol. 2020, 98, 803–809. [Google Scholar] [CrossRef]
- Zhou, L.; Ni, Z.; Yu, J.; Cheng, W.; Cai, Z.; Yu, C. Correlation Between Fecal Metabolomics and Gut Microbiota in Obesity and Polycystic Ovary Syndrome. Front. Endocrinol. 2020, 11, 628. [Google Scholar] [CrossRef]
- Zhou, L.; Ni, Z.; Cheng, W.; Yu, J.; Sun, S.; Zhai, D.; Yu, C.; Cai, Z. Characteristic gut microbiota and predicted metabolic functions in women with PCOS. Endocr. Connect. 2020, 9, 63–73. [Google Scholar] [CrossRef]
- Dong, S.; Jiao, J.; Jia, S.; Li, G.; Zhang, W.; Yang, K.; Wang, Z.; Liu, C.; Li, D.; Wang, X. 16S rDNA Full-Length Assembly Sequencing Technology Analysis of Intestinal Microbiome in Polycystic Ovary Syndrome. Front. Cell. Infect. Microbiol. 2021, 11, 634981. [Google Scholar] [CrossRef]
- Garcia-Beltran, C.; Malpique, R.; Carbonetto, B.; González-Torres, P.; Henares, D.; Brotons, P.; Muñoz-Almagro, C.; López-Bermejo, A.; de Zegher, F.; Ibáñez, L. Gut microbiota in adolescent girls with polycystic ovary syndrome: Effects of randomized treatments. Pediatr. Obes. 2021, 16, e12734. [Google Scholar] [CrossRef] [PubMed]
- He, F.; Li, Y. The gut microbial composition in polycystic ovary syndrome with insulin resistance: Findings from a normal-weight population. J. Ovarian. Res. 2021, 14, 50. [Google Scholar] [CrossRef]
- Jobira, B.; Frank, D.N.; Silveira, L.J.; Pyle, L.; Kelsey, M.M.; Garcia-Reyes, Y.; Robertson, C.E.; Ir, D.; Nadeau, K.J.; Cree-Green, M. Hepatic steatosis relates to gastrointestinal microbiota changes in obese girls with polycystic ovary syndrome. PLoS ONE 2021, 16, e0245219. [Google Scholar] [CrossRef] [PubMed]
- Liang, Z.; Di, N.; Li, L.; Yang, D. Gut microbiota alterations reveal potential gut-brain axis changes in polycystic ovary syndrome. J. Endocrinol. Investig. 2021, 44, 1727–1737. [Google Scholar] [CrossRef] [PubMed]
- Mammadova, G.; Ozkul, C.; Yilmaz Isikhan, S.; Acikgoz, A.; Yildiz, B.O. Characterization of gut microbiota in polycystic ovary syndrome: Findings from a lean population. Eur. J. Clin. Investig. 2021, 51, e13417. [Google Scholar] [CrossRef] [PubMed]
- Ni, Z.; Cheng, W.; Ding, J.; Yao, R.; Zhang, D.; Zhai, D.; Zhou, L.; Yu, C. Impact of Buzhong Yiqi Prescription on the Gut Microbiota of Patients with Obesity Manifesting Polycystic Ovarian Syndrome. Evid. Based Complement. Alternat. Med. 2021, 2021, 6671367. [Google Scholar] [CrossRef]
- Zhu, X.; Li, Y.; Jiang, Y.; Zhang, J.; Duan, R.; Liu, L.; Liu, C.; Xu, X.; Yu, L.; Wang, Q.; et al. Prediction of Gut Microbial Community Structure and Function in Polycystic Ovary Syndrome With High Low-Density Lipoprotein Cholesterol. Front. Cell. Infect. Microbiol. 2021, 11, 665406. [Google Scholar] [CrossRef]
- Hassan, S.; Kaakinen, M.A.; Draisma, H.; Zudina, L.; Ganie, M.A.; Rashid, A.; Balkhiyarova, Z.; Kiran, G.S.; Vogazianos, P.; Shammas, C.; et al. Bifidobacterium Is Enriched in Gut Microbiome of Kashmiri Women with Polycystic Ovary Syndrome. Genes 2022, 13, 379. [Google Scholar] [CrossRef]
- Li, G.; Liu, Z.; Ren, F.; Shi, H.; Zhao, Q.; Song, Y.; Fan, X.; Ma, X.; Qin, G. Alterations of Gut Microbiome and Fecal Fatty Acids in Patients With Polycystic Ovary Syndrome in Central China. Front. Microbiol. 2022, 13, 911992. [Google Scholar] [CrossRef]
- Tayachew, B.; Vanden Brink, H.; Garcia-Reyes, Y.; Rahat, H.; D’Alessandro, A.; Frank, D.N.; Robertson, C.E.; Silveira, L.; Kelsey, M.; Pyle, L.; et al. Combined Oral Contraceptive Treatment Does Not Alter the Gut Microbiome but Affects Amino Acid Metabolism in Sera of Obese Girls With Polycystic Ovary Syndrome. Front. Physiol. 2022, 13, 887077. [Google Scholar] [CrossRef]
- Wang, X.; Xu, T.; Liu, R.; Wu, G.; Gu, L.; Zhang, Y.; Zhang, F.; Fu, H.; Ling, Y.; Wei, X.; et al. High-Fiber Diet or Combined With Acarbose Alleviates Heterogeneous Phenotypes of Polycystic Ovary Syndrome by Regulating Gut Microbiota. Front. Endocrinol. 2022, 12, 806331. [Google Scholar] [CrossRef] [PubMed]
- Lüll, K.; Arffman, R.K.; Sola-Leyva, A.; Molina, N.M.; Aasmets, O.; Herzig, K.H.; Plaza-Díaz, J.; Franks, S.; Morin-Papunen, L.; Tapanainen, J.S.; et al. The Gut Microbiome in Polycystic Ovary Syndrome and Its Association with Metabolic Traits. J. Clin. Endocrinol. Metab. 2021, 106, 858–871. [Google Scholar] [CrossRef] [PubMed]
- Schloss, P.D.; Handelsman, J. Introducing DOTUR, a computer program for defining operational taxonomic units and estimating species richness. Appl. Environ. Microbiol. 2005, 71, 1501–1506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schloss, P.D.; Westcott, S.L.; Ryabin, T.; Hall, J.R.; Hartmann, M.; Hollister, E.B.; Lesniewski, R.A.; Oakley, B.B.; Parks, D.H.; Robinson, C.J.; et al. Introducing mothur: Open-source, platform-independent, community-supported software for describing and comparing microbial communities. Appl. Environ. Microbiol. 2009, 75, 7537–7541. [Google Scholar] [CrossRef] [Green Version]
- Chao, A.; Chazdon, R.L.; Colwell, R.K.; Shen, T.J. Abundance-based similarity indices and their estimation hen there are unseen species in samples. Biometrics 2006, 62, 361–371. [Google Scholar] [CrossRef]
- Kim, B.R.; Shin, J.; Guevarra, R.; Lee, J.H.; Kim, D.W.; Seol, K.H.; Lee, J.H.; Kim, H.B.; Isaacson, R. Deciphering Diversity Indices for a Better Understanding of Microbial Communities. J. Microbiol. Biotechnol. 2017, 27, 2089–2093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hughes, J.B.; Hellmann, J.J.; Ricketts, T.H.; Bohannan, B.J. Counting the uncountable: Statistical approaches to estimating microbial diversity. Appl. Environ. Microbiol. 2001, 67, 4399–4406. [Google Scholar] [CrossRef] [Green Version]
- Teede, H.J.; Misso, M.L.; Costello, M.F.; Dokras, A.; Laven, J.; Moran, L.; Piltonen, T.; Norman, R.J.; International PCOS Network. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Fertil. Steril. 2018, 110, 364–379. [Google Scholar] [CrossRef] [Green Version]
- Yildiz, B.O.; Bolour, S.; Woods, K.; Moore, A.; Azziz, R. Visually scoring hirsutism. Hum. Reprod. Update 2010, 16, 51–64. [Google Scholar] [CrossRef]
- Bolyen, E.; Rideout, J.R.; Dillon, M.R.; Bokulich, N.A.; Abnet, C.C.; Al-Ghalith, G.A.; Alexander, H.; Alm, E.J.; Arumugam, M.; Asnicar, F.; et al. Reproducible, interactive, scalable and extensible microbiome data science using QIIME 2. Nat. Biotechnol. 2019, 37, 852–857. [Google Scholar] [CrossRef]
- Naing, L.; Winn, T.; Rusli, B.N. Practical issues in calculating the sample size for prevalence studies. Med. Stat. 2006, 1, 9–14. [Google Scholar]
- Atalyan, A.V.; Kolesnikova, L.I.; Kolesnikov, S.I.; Grjibovski, A.M.; Suturina, L.V. Research Electronic Data Capture (REDCap) for Building and Managing Databases for Population-based Biomedical Studies. Ekol. Cheloveka (Hum. Ecol.) 2019, 2, 52–59. [Google Scholar] [CrossRef] [Green Version]
- Zuur, A.F.; Ieno, E.N.; Elphick, C.S. A protocol for data exploration to avoid common statistical problems. Methods Ecol. Evol. 2010, 1, 3–14. [Google Scholar] [CrossRef]
- Lehmann, R. 3sigma-Rule for Outlier Detection from the Viewpoint of Geodetic Adjustment. J. Surv. Eng. 2013, 139, 157–165. [Google Scholar] [CrossRef] [Green Version]
- Martínez, I.; Muller, C.E.; Walter, J. Long-term temporal analysis of the human fecal microbiota revealed a stable core of dominant bacterial species. PLoS ONE 2013, 8, e69621. [Google Scholar] [CrossRef]
- Costa, M.; Weese, J.S. Methods and basic concepts for microbiota assessment. Vet. J. 2019, 249, 10–15. [Google Scholar] [CrossRef]
- Lindheim, L.; Bashir, M.; Münzker, J.; Trummer, C.; Zachhuber, V.; Pieber, T.R.; Gorkiewicz, G.; Obermayer-Pietsch, B. The Salivary Microbiome in Polycystic Ovary Syndrome (PCOS) and Its Association with Disease-Related Parameters: A Pilot Study. Front. Microbiol. 2016, 7, 1270. [Google Scholar] [CrossRef] [Green Version]
- Li, N.; Li, Y.; Qian, C.; Liu, Q.; Cao, W.; Ma, M.; He, R.; Chen, R.; Geng, R.; Liu, Y. Dysbiosis of the Saliva Microbiome in Patients With Polycystic Ovary Syndrome. Front. Cell. Infect. Microbiol. 2021, 10, 624504. [Google Scholar] [CrossRef]
- Hong, X.; Qin, P.; Huang, K.; Ding, X.; Ma, J.; Xuan, Y.; Zhu, X.; Peng, D.; Wang, B. Association between polycystic ovary syndrome and the vaginal microbiome: A case-control study. Clin. Endocrinol. 2020, 93, 52–60. [Google Scholar] [CrossRef]
- Tu, Y.; Zheng, G.; Ding, G.; Wu, Y.; Xi, J.; Ge, Y.; Gu, H.; Wang, Y.; Sheng, J.; Liu, X.; et al. Comparative Analysis of Lower Genital Tract Microbiome Between PCOS and Healthy Women. Front. Physiol. 2020, 11, 1108. [Google Scholar] [CrossRef]
- Lu, C.; Wang, H.; Yang, J.; Zhang, X.; Chen, Y.; Feng, R.; Qian, Y. Changes in Vaginal Microbiome Diversity in Women With Polycystic Ovary Syndrome. Front. Cell. Infect. Microbiol. 2021, 11, 755741. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Wang, Q.; Zhao, L.; Bin, Y.; Wang, L.; Wang, L.; Zhang, K.; Li, Q. Blood Bacterial 16S rRNA Gene Alterations in Women With Polycystic Ovary Syndrome. Front. Endocrinol. 2022, 13, 814520. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Wu, X.; Guo, S.; Lv, Y.; Zhou, P.; Huang, G.; Duan, Z.; Sun, W. Metagenomic-based characterization of the gut virome in patients with polycystic ovary syndrome. Front. Microbiol. 2022, 13, 951782. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameters | Non-PCOS n = 121 | PCOS n = 63 | p-Value |
|---|---|---|---|
| Age, years, Mean ± SD | 35.11 ± 5.71 | 29.48 ± 5.21 | <0.001 # |
| Height, cm, Mean ± SD | 163.71 ± 6.00 | 164.93 ± 6.57 | 0.07 # |
| Weight, kg, Mean ± SD | 71.95 ± 16.11 | 71.29 ± 14.73 | 0.98 # |
| BMI, kg/m2, Mean ± SD | 26.83 ± 5.83 | 26.24 ± 5.24 | 0.65 # |
| mFG score, M ± SD Me [25% Quartile; 75% Quartile] | 1.27 ± 1.91 0.00 [0.00; 2.00] | 3.67 ± 3.61 3.00 [0.00; 6.00] | <0.001 * |
| Waist circumference, cm Mean ± SD | 80.36 ± 12.91 | 79.29 ± 13.19 | 0.48 # |
| Hip circumference, cm, Mean ± SD | 101.62 ± 10.62 | 100.83 ± 9.44 | 0.73 # |
| Systolic blood pressure, mm Hg, Mean ± SD | 126.02 ± 14.09 | 121.54 ± 12.37 | 0.03 # |
| Diastolic blood pressure, mm Hg Mean ± SD | 81.07 ± 9.39 | 78.86 ± 9.49 | 0.12 # |
| Pelvic U/S | M ± SD Me [25% Quartile; 75% Quartile] | ||
| AFC, right ovary | 7.88 ± 3.75 7.00 [5.00; 9.00] | 12.27 ± 3.87 12.00 [10.00; 14.00] | <0.001 * |
| AFC, left ovary | 7.16 ± 3.22 6.00 [5.00; 9.00] | 11.50 ± 3.53 12.00 [10.00; 13.00] | <0.001 * |
| Volume, right ovary, cm3 | 13.87 ± 52.08 6.92 [5.51; 9.06] | 13.71 ± 9.12 11.68 [10.01; 13.41] | <0.001 * |
| Volume, left ovary, cm3 | 8.38 ± 8.95 6.44 [5.05; 8.69] | 10.79 ± 4.64 9.37 [7.64; 12.91] | <0.001 * |
| Parameter | Non-PCOS n = 121 | PCOS n = 63 | p-Value | ||
|---|---|---|---|---|---|
| Control (1a) n = 19 | «Grey Zone» (1b) N = 102 | Phenotypes A, B, C (2a) n = 41 | Phenotype D (2b) n = 22 | ||
| Age, years, Mean ± SD | 34.3 ± 4.3 | 35.3 ± 5.9 | 29.8 ± 5.5 | 28.9 ± 4.7 | <0.001 * p1a-1b = 1.00 p1a-2a = 0.03 p1a-2b = 0.02 p1b-2a < 0.001 p1b-2b < 0.001 p2a-2b = 1.00 |
| Height, cm, Mean ± SD | 162.91 ± 5.9 | 163.9 ± 6.0 | 164.6 ± 7.3 | 165.7 ± 5.2 | 0.53 * |
| Weight, kg, Mean ± SD | 65.7 ± 12.4 | 73.1 ± 16.5 | 73.3 ± 16.4 | 67.7 ± 10.2 | 0.13 * |
| BMI, kg/m2, Mean ± SD | 24.6 ± 3.5 | 27.3 ± 6.1 | 27.1 ± 5.6 | 24.7 ± 4.1 | 0.08 * |
| mFG score, M ± SD Me [25% Quartile; 75% Quartile] | 0.42 ± 0.69 0.00 [0.00; 1.00] | 1.43 ± 2.02 0.50 [0.00; 2.00] | 5.05 ± 3.67 5.00 [2.00; 7.00] | 1.09 ± 1.48 0.00 [0.00; 2.00] | <0.001 # p1a-1b = 0.52 p1a-2a < 0.001 p1a-2b = 1.00 p1b-2a < 0.001 p1b-2b = 1.00 p2a-2b < 0.001 |
| Waist circumference, cm, Mean ± SD | 75.9 ± 8.9 | 81.2 ± 13.4 | 81.8 ± 13.6 | 74.6 ± 11.4 | 0.07 * |
| Hip circumference, cm, Mean ± SD | 98.1 ± 8.3 | 102.3 ± 10.9 | 102.4 ± 10.2 | 97.9±7.1 | 0.14 * |
| Systolic blood pressure, mm Hg, Mean ± SD | 117.3 ± 11.7 | 127.7 ± 13.9 | 123.8 ± 12.6 | 117.4±11.2 | <0.001 * p1a-1b= 0.008 p1a-2a = 0.47 p1a-2b = 1.00 p1b-2a = 0.52 p1b-2b = 0.005 p2a-2b = 0.41 |
| Diastolic blood pressure, mm Hg, Mean ± SD | 75.4 ± 7.3 | 82.1 ± 9.4 | 80.3 ± 9.3 | 76.1±9.4 | 0.002 * p1a-1b = 0.015 p1a-2a = 0.31 p1a-2b = 1.00 p1b-2a = 1.00 p1b-2b = 0.02 p2a-2b = 0.48 |
| Pelvic U/S | M ± SD Me [25% Quartile; 75% Quartile] | ||||
| AFC, right ovary | 6.63 ± 3.15 6.00 [5.00; 8.00] | 8.11 ± 3.82 7.00 [5.00; 10.00] | 12.02 ± 3.54 12.00 [11.00; 14.00] | 12.73 ± 4.47 12.00 [10.00; 13.00] | <0.001 # p1 a-1b = 0.26 p1a-2a < 0.001 p1a-2b < 0.001 p1b-2a < 0.001 p1b-2b < 0.001 p2a-2b = 1.00 |
| AFC, left ovary | 6.47 ± 2.46 6.00 [5.00; 8.00] | 7.29 ± 3.34 6.00 [5.00; 9.50] | 11.28 ± 3.95 12.00 [8.50; 13.00] | 11.91 ± 2.64 0.00 [0.00; 2.00] | <0.001 # p1a-1b = 1.00 p1a-2a = 0.006 p1a-2b < 0.001 p1b-2a = 0.009 p1b-2b < 0.001 p2a-2b = 0.18 |
| Volume, right ovary, cm3 | 6.40 ± 1.71 6.12 [4.85; 7.46] | 15.26 ± 56.65 7.40 [5.52; 9.49] | 12.56 ± 6.70 11.60 [9.54; 13.27] | 15.86 ± 12.36 11.81 [10.24; 13.41] | <0.001 # p1a-1b = 0.52 p1a-2a < 0.001 p1a-2b < 0.001 p1b-2a < 0.001 p1b-2b < 0.001 p2a-2b = 1.00 |
| Volume, left ovary, cm3 | 6.20 ± 2.00 6.44 [4.61; 7.18] | 8.80 ± 9.68 6.41 [5.17; 8.87] | 9.54 ± 3.91 8.79 [7.07; 12.60] | 13.06 ± 5.07 11.76 [8.84; 16.95] | <0.001 # p1 a-1b=1.000 p1a-2a < 0.001 p1a-2b < 0.001 p1b-2a < 0.001 p1b-2b < 0.001 p2a-2b = 1.000 |
| Parameter | Non-PCOS n = 121 | PCOS n = 63 | p-Value * |
|---|---|---|---|
| M ± SD Me [25%Quartile; 75% Quartile] | |||
| Prolactin, mIU/mL | 358 ± 249 292 [206; 436] | 314 ± 145 278 [221; 383] | 0.61 |
| TSH, mIU/mL | 1.96 ± 1.795222 1.50 [1.10; 2.10] | 1.57 ± 0.71 1.60 [1.00; 1.90] | 0.48 |
| LH, mIU/mL | 7.10 ± 7.74 5.25 [3.00; 7.65] | 10.82 ± 8.44 8.60 [5.40; 14.00] | <0.001 |
| follicule phase, mIU/mL | 8.28 ± 8.21 5.90 [4.90; 9.10] | 9.42 ± 4.94 7.45 [5.60; 13.20] | 0.09 |
| luteal phase, mIU/mL | 6.29 ± 7.09 5.00 [2.50; 7.40] | 10.61 ± 9.10 8.45 [4.85; 13.50] | 0.000 |
| FSH, mIU/mL | 6.01 ± 5.93 5.25 [3.75;6.55] | 5.44 ± 1.70 5.40 [3.90; 6.40] | 0.46 |
| follicule phase, mIU/mL | 7.09 ± 3.61 6.20 [5.45; 7.00] | 5.96 ± 1.02 5.85 [5.60; 6.80] | 0.521 |
| luteal phase, mIU/mL | 4.60 ± 4.60 4.10 [2.90; 5.70] | 5.06 ± 1.80 4.95 [3.55;6.15] | 0.122 |
| AMH, ng/mL | 3.13 ± 3.52 2.20 [0.80; 4.10] | 7.71 ± 6.10 5.60 [3.10; 8.80] | <0.001 |
| 17OHP, nmol/L | 2.57 ± 1.65 2.20 [1.40; 4.20] | 4.31 ± 1.33 4.60 [3.70; 5.00] | 0.005 |
| TT, ng/dL | 29.2 ± 23.8 26.0 [17.1; 36.5] | 46.3 ± 26.1 43.2 [27.5; 56.2] | <0.001 |
| follicule phase, ng/dL | 32.0 ± 32.3 25.7 [14.7; 37.1] | 41.3 ± 19.3 47.5 [25.5; 55.6] | 0.024 |
| luteal phase, ng/dL | 28.6 ± 16.1 27.4 [18.8; 36.6] | 50.2 ± 30.2 38.5 [28.6; 63.2] | 0.000 |
| SHBG, nmol/L | 80.4 ± 50.1 71.0 [45.9; 103.9] | 66.5 ± 52.1 45.6 [33.0; 89.5] | 0.008 |
| FAI | 1.96 ± 3.73 1.23 [0.68; 2.07] | 3.55 ± 3.01 2.68 [1.39; 4.65] | <0.001 |
| follicule phase | 2.33 ± 5.40 1.37 [0.80; 2.07] | 2.54 ± 1.76 2.01 [1.30; 3.22] | 0.029 |
| luteal phase | 1.77 ± 2.07 1.09 [0.66; 2.05] | 3.80 ± 3.04 3.22 [1.44; 5.06] | 0.000 |
| DHEAS, μg/dL | 168 ± 72.8 161 [116; 218] | 232 ± 114 200 [139; 319] | <0.001 |
| follicule phase, μg/dL | 176 ± 79.0 158 [114; 226] | 234 ± 107 218 [134; 311] | 0.046 |
| luteal phase, μg/dL | 165 ± 66.5 166 [119; 215] | 225 ± 116 194 [140; 294] | 0.016 |
| Parameter | Non-PCOS n = 121 | PCOS n = 63 | p-Value *,# | ||
|---|---|---|---|---|---|
| Control (1a) n = 19 | «Grey Zone» (1b) n = 102 | Phenotypes A, B, C (2a) n = 41 | Phenotype D (2b) n = 22 | ||
| M ± SD Me [25% Quartile; 75% Quartile] | |||||
| Prolactin, mIU/mL | 295 ± 131 248 [185; 436] | 370 ± 264 298 [217; 436] | 316 ± 144 284 [232; 384] | 309 ± 151 271 [199; 352] | 0.70 |
| TSH, mIU/mL | 1.55 ± 0.70 1.60 [0.90; 1.90] | 2.03 ± 1.93 1.50 [1.10; 2.10] | 1.64 ± 0.81 1.60 [1.00; 2.00] | 1.44 ± 0.45 1.45 [1.10; 0.80] | 0.75 |
| LH, mIU/mL | 6.55 ± 5.24 5.80 [3.90; 7.40] | 7.20 ± 8.14 5.20 [2.90; 7.90] | 12.0 ± 9.63 8.30 [5.90; 14.50] | 8.59 ± 5.05 8.90 [4.20; 11.80] | <0.001 p1a-1b = 1.00 p1a-2a = 0.04 p1a-2b = 1.00 p1b-2a < 0.001 p1b-2b = 0.29 p2a-2b = 1.00 |
| FSH, mIU/mL | 5.74 ± 1.85 6.10 [4.00; 6.90] | 6.06 ± 6.42 5.00 [3.70; 6.40] | 5.81 ± 1.89 5.90 [4.90; 7.20] | 4.75 ± 0.98 5.00 [3.70; 5.40] | 0.05 |
| AMH, ng/mL | 2.79 ± 2.06 2.00 [1.20; 4.60] | 3.20 ± 3.75 2.20 [0.70; 4.10] | 6.63 ± 5.48 4.70 [2.50; 8.70] | 9.72 ± 6.79 7.20 [5.20; 17.20] | <0.001 p1a-1b = 1.000 p1a-2a = 0.02 p1a-2b < 0.001 p1b-2a < 0.001 p1b-2b < 0.001 p2a-2b = 0.39 |
| 17OHP, nmol/L | 1.95 ± 1.54 2.00 [0.70; 2.80] | 2.83 ± 1.67 2.30 [1.50; 4.30] | 4.40 ± 0.70 4.40 [3.70; 5.00] | 4.20 ± 2.01 4.60 [3.00; 5.40] | 0.035 p1a-1b = 1.00 p1a-2a = 0.08 p1a-2b = 0.25 p1b-2a = 0.24 p1b-2b = 0.65 p2a-2b = 1.00 |
| TT, ng/dL | 23.5 ± 11.8 25.5 [14.9; 30.1] | 30.3 ± 25.3 27.4 [17.6; 37.3] | 53.3 ± 27.9 47.7 [31.8; 66.7] | 33.3 ± 15.8 30.8 [21.1; 39.6] | <0.001 p1a-1b = 1.00 p1a-2a < 0.001 p1a-2b = 0.50 p1b-2a < 0.001 p1b-2b = 1.00 p2a-2b = 0.05 |
| SHBG, nmol/L | 89.0±46.9 68.7 [57.2; 114.7] | 78.7 ± 50.8 71.2 [43.6; 102.9] | 61.2 ± 45.4 42.0 [32.9; 76.3] | 76.3 ± 62.5 66.9 [37.6; 94.3] | 0.018 p1a-1b = 1.00 p1a-2a = 0.03 p1a-2b = 1.00 p1b-2a = 0.05 p1b-2b = 1.00 p2a-2b = 1.00 |
| FAI | 1.10 ± 0.81 0.97 [0.49; 1.39] | 2.12 ± 4.03 1.31 [0.80; 2.10] | 4.33 ± 3.35 3.29 [2.06; 5.39] | 2.08 ± 1.36 1.67 [0.95; 3.23] | <0.001 p1a-1b = 0.54 p1a-2a < 0.001 p1a-2b = 0.12 p1b-2a < 0.001 p1b-2b = 1.00 p2a-2b = 0.03 |
| DHEAS, μg/dL | 173 ± 65.9 186 [118; 215] | 167 ± 73.6 153 [114; 219] | 256 ± 125 236 [141; 334] | 189 ± 75 189 [130; 221] | 0.001 p1a-1b = 1.00 p1a-2a = 0.15 p1a-2b = 1.00 p1b-2a < 0.001 p1b-2b = 1.00 p2a-2b = 0.55 |
| Indexes | Non-PCOS n = 121 (1) | PCOS n = 63 (2) | P1–2 * |
|---|---|---|---|
| ASV | 114 (91; 138) ** | 106 (87; 131) | 0.163 |
| Shannon | 5.57 (4.93; 6.07) | 5.28 (4.77; 5.84) | 0.039 |
| Simpson | 0.96 (0.92; 0.97) | 0.94 (0.92; 0.97) | 0.088 |
| Chao | 119 (100; 157) | 109 (92; 132) | 0.048 |
| ACE | 113 (93; 145) | 103 (89; 127) | 0.088 |
| Indexes | Non-PCOS n = 121 | PCOS n = 63 | p-Value * | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Control (1a) n = 19 | “Grey Zone” (1b) n = 102 | Phenotypes A, B, C (2a) n = 41 | Phenotype D (2b) n = 22 | 1a–1b | 2a–2b | 1a–2a | 1a–2b | 1b–2a | 1b–2b | |
| ASV | 131 ** [85; 166] | 113 [91; 137] | 101 [84; 130] | 116 [93; 131] | 0.140 | 0.108 | 0.045 | 0.248 | 0.127 | 0.823 |
| Shannon | 5.96 [5.36; 6.54] | 5.53 [4.91; 6.04] | 5.23 [4.80; 5.84] | 5.41 [4.76; 5.79] | 0.016 | 0.880 | 0.003 | 0.014 | 0.203 | 0.357 |
| Simpson | 0.97 [0.94; 0.98] | 0.95 [0.92; 0.97] | 0.94 [0.92;0.97] | 0.94 [0.91; 0.97] | 0.017 | 0.971 | 0.006 | 0.017 | 0.351 | 0.472 |
| Chao | 139 [111; 192] | 116 [99; 151] | 108 [91; 130] | 117 [96; 148] | 0.075 | 0.285 | 0.010 | 0.121 | 0.062 | 0.803 |
| ACE | 136 [99; 173] | 111 [92; 135] | 98 [90; 127] | 114 [89; 131] | 0.070 | 0.333 | 0.014 | 0.164 | 0.109 | 0.899 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suturina, L.; Belkova, N.; Igumnov, I.; Lazareva, L.; Danusevich, I.; Nadeliaeva, I.; Sholokhov, L.; Rashidova, M.; Belenkaya, L.; Belskikh, A.; et al. Polycystic Ovary Syndrome and Gut Microbiota: Phenotype Matters. Life 2023, 13, 7. https://doi.org/10.3390/life13010007
Suturina L, Belkova N, Igumnov I, Lazareva L, Danusevich I, Nadeliaeva I, Sholokhov L, Rashidova M, Belenkaya L, Belskikh A, et al. Polycystic Ovary Syndrome and Gut Microbiota: Phenotype Matters. Life. 2023; 13(1):7. https://doi.org/10.3390/life13010007
Chicago/Turabian StyleSuturina, Larisa, Natalia Belkova, Ilia Igumnov, Ludmila Lazareva, Irina Danusevich, Iana Nadeliaeva, Leonid Sholokhov, Maria Rashidova, Lilia Belenkaya, Aleksey Belskikh, and et al. 2023. "Polycystic Ovary Syndrome and Gut Microbiota: Phenotype Matters" Life 13, no. 1: 7. https://doi.org/10.3390/life13010007