
Polycystic Ovary Syndrome and Endocrine Disruptors (Bisphenols, Parabens, and Triclosan)—A Systematic Review

Abstract
:1. Introduction
2. Materials and Methods
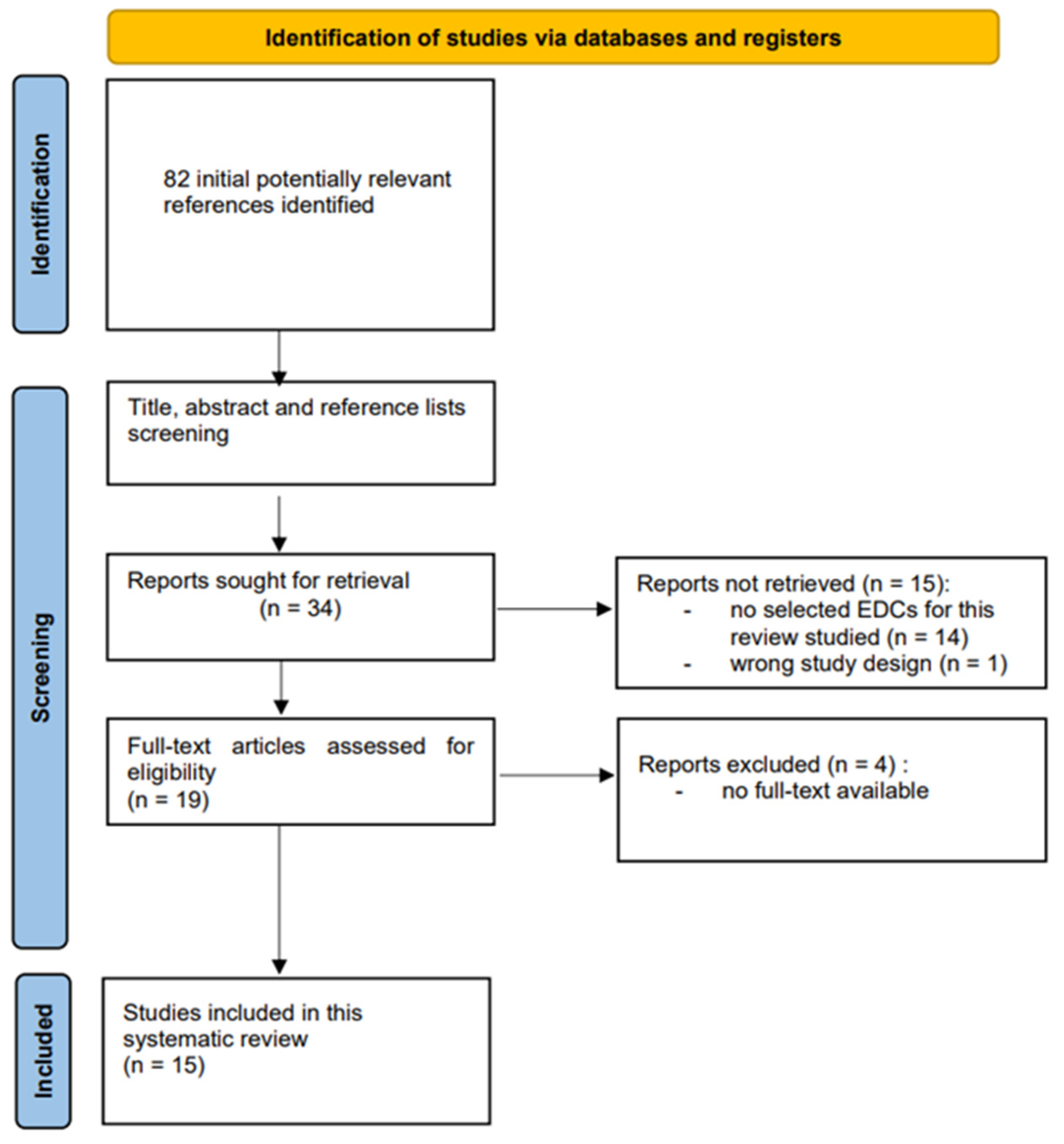
2.1. Literature Identification
2.2. The Inclusion and Exclusion Criteria
2.3. Data Extraction
3. Results
3.1. Bisphenol A (BPA)
3.2. Parabens
3.3. Triclosan (TCS)
3.4. Literature Search
3.5. Association of Endocrine-Disrupting Chemicals with Polycystic Ovary Syndrome
3.5.1. Bisphenol A and PCOS
3.5.2. Parabens and PCOS
3.5.3. Triclosan and PCOS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Karwacka, A.; Zamkowska, D.; Radwan, M.; Jurewicz, J. Exposure to modern, widespread environmental endocrine disrupting chemicals and their effect on the reproductive potential of women: An overview of current epidemiological evidence. Hum. Fertil. 2017, 22, 2–25. [Google Scholar] [CrossRef] [PubMed]
- Colborn, T.; Clement, C. Wingspread Consensus Statement. Chemically-Induced Alterations in Sexual and Functional Development: The Wildlife/Human Connection; Princeton Scientific Publishing Company: Princeton, NJ, USA, 1992; pp. 1–8. [Google Scholar]
- Damstra, T.; Barlow, S.; Berman, A.; Kavlock, R.; van der Kraak, G. Global Assessment of the State-of-the-Science of Endocrine Disruptors. World Health Organization, the International Labour Organisation, and the United Nations Environment Programme. 2002. Available online: https://www.who.int/publications/i/item/WHO_PCS_EDC_02.2 (accessed on 8 October 2022).
- Gore, A.C.; Chappell, V.A.; Fenton, S.E.; Flaws, J.A.; Nadal, A.; Prins, G.S.; Toppari, J.; Zoeller, R.T. EDC-2: The Endocrine Society’s Second Scientific Statement on Endocrine-Disrupting Chemicals. Endocr. Rev. 2015, 36, E1–E150. [Google Scholar] [CrossRef] [PubMed]
- Scsukova, S.; Rollerova, E.; Mlynarcikova, A.B. Impact of endocrine disrupting chemicals on onset and development of female reproductive disorders and hormone-related cancer. Reprod. Biol. 2016, 16, 243–254. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, B.; Terekeci, H.; Sandal, S.; Kelestimur, F. Endocrine disrupting chemicals: Exposure, effects on human health, mechanism of action, models for testing and strategies for prevention. Rev. Endocr. Metab. Disord. 2020, 21, 127–147. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.-R.; Jeung, E.-B.; Cho, M.-H.; Kim, T.-H.; Leung, P.; Choi, K.-C. Molecular mechanism(s) of endocrine-disrupting chemicals and their potent oestrogenicity in diverse cells and tissues that express oestrogen receptors. J. Cell. Mol. Med. 2013, 17, 1–11. [Google Scholar] [CrossRef]
- Neier, K.; Marchlewicz, E.H.; Dolinoy, D.C.; Padmanabhan, V. Assessing human health risk to endocrine disrupting chemicals: A focus on prenatal exposures and oxidative stress. Endocr. Disruptors 2015, 3, e1069916. [Google Scholar] [CrossRef] [Green Version]
- Xin, F.; Susiarjo, M.; Bartolomei, M.S. Multigenerational and transgenerational effects of endocrine disrupting chemicals: A role for altered epigenetic regulation? Semin. Cell Dev. Biol. 2015, 43, 66–75. [Google Scholar] [CrossRef] [Green Version]
- Uzumcu, M.; Zama, A.M.; Oruc, E. Epigenetic Mechanisms in the Actions of Endocrine-disrupting Chemicals: Gonadal Effects and Role in Female Reproduction. Reprod. Domest. Anim. 2012, 47 (Suppl. 4), 338–347. [Google Scholar] [CrossRef]
- Rattan, S.; Zhou, C.; Chiang, C.; Mahalingam, S.; Brehm, E.; Flaws, J.A. Exposure to endocrine disruptors during adulthood: Consequences for female fertility. J. Endocrinol. 2017, 233, R109–R129. [Google Scholar] [CrossRef] [Green Version]
- Patel, S.; Zhou, C.; Rattan, S.; Flaws, J.A. Effects of Endocrine-Disrupting Chemicals on the Ovary1. Biol. Reprod. 2015, 93, 20. [Google Scholar] [CrossRef]
- Gibson, D.A.; Saunders, P.T.K. Endocrine disruption of oestrogen action and female reproductive tract cancers. Endocr.-Relat. Cancer 2013, 21, T13–T31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rutkowska, A.Z.; Diamanti-Kandarakis, E. Polycystic ovary syndrome and environmental toxins. Fertil. Steril. 2016, 106, 948–958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azziz, R.; Woods, K.S.; Reyna, R.; Key, T.J.; Knochenhauer, E.S.; Yildiz, B.O. The Prevalence and Features of the Polycystic Ovary Syndrome in an Unselected Population. J. Clin. Endocrinol. Metab. 2004, 89, 2745–2749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agrawal, R.; Sharma, S.; Bekir, J.; Conway, G.; Bailey, J.; Balen, A.; Prelevic, G. Prevalence of polycystic ovaries and polycystic ovary syndrome in lesbian women compared with heterosexual women. Fertil. Steril. 2004, 82, 1352–1357. [Google Scholar] [CrossRef] [PubMed]
- Sobolewski, M.; Barrett, E.S. Polycystic Ovary Syndrome: Do Endocrine-Disrupting Chemicals Play a Role? Semin. Reprod. Med. 2014, 32, 166–176. [Google Scholar] [CrossRef] [Green Version]
- Kechagias, K.S.; Semertzidou, A.; Athanasiou, A.; Paraskevaidi, M.; Kyrgiou, M. Bisphenol-A and polycystic ovary syndrome: A review of the literature. Rev. Environ. Health 2020, 35, 323–331. [Google Scholar] [CrossRef]
- Hu, Y.; Wen, S.; Yuan, D.; Peng, L.; Zeng, R.; Yang, Z.; Liu, Q.; Xu, L.; Kang, D. The association between the environmental endocrine disruptor bisphenol A and polycystic ovary syndrome: A systematic review and meta-analysis. Gynecol. Endocrinol. 2018, 34, 370–377. [Google Scholar] [CrossRef]
- Vandenberg, L.N.; Chahoud, I.; Heindel, J.J.; Padmanabhan, V.; Paumgartten, F.J.R.; Schönfelder, G. Urinary, Circulating, and Tissue Biomonitoring Studies Indicate Widespread Exposure to Bisphenol A. Ciência Saúde Coletiva 2012, 17, 407–434. [Google Scholar] [CrossRef]
- Eladak, S.; Grisin, T.; Moison, D.; Guerquin, M.-J.; N’Tumba-Byn, T.; Pozzi-Gaudin, S.; Benachi, A.; Livera, G.; Rouiller-Fabre, V.; Habert, R. A new chapter in the bisphenol A story: Bisphenol S and bisphenol F are not safe alternatives to this compound. Fertil. Steril. 2015, 103, 11–21. [Google Scholar] [CrossRef] [Green Version]
- Ehrlich, S.; Calafat, A.M.; Humblet, O.; Smith, T.; Hauser, R. Handling of Thermal Receipts as a Source of Exposure to Bisphenol A. JAMA 2014, 311, 859–860. [Google Scholar] [CrossRef]
- Liao, C.; Kannan, K. Widespread Occurrence of Bisphenol A in Paper and Paper Products: Implications for Human Exposure. Environ. Sci. Technol. 2011, 45, 9372–9379. [Google Scholar] [CrossRef] [PubMed]
- Milanović, M.; Milošević, N.; Sudji, J.; Stojanoski, S.; Krstonošić, M.A.; Bjelica, A.; Milić, N.; Stojanoska, M.M. Can environmental pollutant bisphenol A increase metabolic risk in polycystic ovary syndrome? Clin. Chim. Acta 2020, 507, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Włodarczyk, E. Occurrence of bisphenol A and its effects on the human body. Arch. Physiother. Glob. Res. 2015, 19, 13–26. [Google Scholar] [CrossRef] [Green Version]
- Souter, I.; Smith, K.W.; Dimitriadis, I.; Ehrlich, S.; Williams, P.L.; Calafat, A.M.; Hauser, R. The association of bisphenol-A urinary concentrations with antral follicle counts and other measures of ovarian reserve in women undergoing infertility treatments. Reprod. Toxicol. 2013, 42, 224–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziv-Gal, A.; Flaws, J.A. Evidence for bisphenol A-induced female infertility: A review (2007–2016). Fertil. Steril. 2016, 106, 827–856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yokota, H.; Iwano, H.; Endo, M.; Kobayashi, T.; Inoue, H.; Ikushiro, S.; Yuasa, A. Glucuronidation of the environmental oes-trogen bisphenol A by an isoform of UDP-glucuronosyltransferase, UGT2B1, in the rat liver. Biochem. J. 1999, 340, 405–409. [Google Scholar] [CrossRef] [PubMed]
- Matuszczak, E.; Komarowska, M.D.; Debek, W.; Hermanowicz, A. The Impact of Bisphenol A on Fertility, Reproductive System, and Development: A Review of the Literature. Int. J. Endocrinol. 2019, 2019, 4068717. [Google Scholar] [CrossRef] [Green Version]
- Santangeli, S.; Maradonna, F.; Olivotto, I.; Piccinetti, C.C.; Gioacchini, G.; Carnevali, O. Effects of BPA on female reproductive function: The involvement of epigenetic mechanism. Gen. Comp. Endocrinol. 2017, 245, 122–126. [Google Scholar] [CrossRef]
- Czubacka, E.; Wielgomas, B.; Klimowska, A.; Radwan, M.; Radwan, P.; Karwacka, A.; Kałużny, P.; Jurewicz, J. Urinary Bisphenol A Concentrations and Parameters of Ovarian Reserve among Women from a Fertility Clinic. Int. J. Environ. Res. Public Health 2021, 18, 8041. [Google Scholar] [CrossRef]
- Commision Directive 2011/8/EU amending Directive 2002/72/EC aa Regards the Restriction of Use of Bisphenol A in Plastic Infant Feeding Bottles. Off. J. Eur. Union 2011, L26/11–L26/14. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32011L0008&qid=1669142783080&from=EN (accessed on 22 November 2022).
- Rochester, J.R.; Bolden, A.L. Bisphenol S and F: A Systematic Review and Comparison of the Hormonal Activity of Bisphenol A Substitutes. Environ. Health Perspect. 2015, 123, 643–650. [Google Scholar] [CrossRef]
- Jurewicz, J.; Majewska, J.; Berg, A.; Owczarek, K.; Zajdel, R.; Kaleta, D.; Wasik, A.; Rachoń, D. Serum bisphenol A analogues in women diagnosed with the polycystic ovary syndrome—Is there an association? Environ. Pollut. 2021, 272, 115962. [Google Scholar] [CrossRef] [PubMed]
- Rutkowska, A.; Rachoń, D. Bisphenol A (BPA) and its potential role in the pathogenesis of the polycystic ovary syndrome (PCOS). Gynecol. Endocrinol. 2014, 30, 260–265. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, M.; Bourguignon, N.; Lux-Lantos, V.; Libertun, C. Neonatal Exposure to Bisphenol A and Reproductive and Endocrine Alterations Resembling the Polycystic Ovarian Syndrome in Adult Rats. Environ. Health Perspect. 2010, 118, 1217–1222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palioura, E.; Diamanti-Kandarakis, E. Polycystic ovary syndrome (PCOS) and endocrine disrupting chemicals (EDCs). Rev. Endocr. Metab. Disord. 2015, 16, 365–371. [Google Scholar] [CrossRef]
- Zhou, W.; Liu, J.; Liao, L.; Han, S.; Liu, J. Effect of bisphenol A on steroid hormone production in rat ovarian theca-interstitial and granulosa cells. Mol. Cell. Endocrinol. 2008, 283, 12–18. [Google Scholar] [CrossRef]
- Nilsson, E.; Larsen, G.; Manikkam, M.; Guerrero-Bosagna, C.; Savenkova, M.I.; Skinner, M.K. Environmentally Induced Epigenetic Transgenerational Inheritance of Ovarian Disease. PLoS ONE 2012, 7, e36129. [Google Scholar] [CrossRef] [Green Version]
- Ehrlich, S.; Williams, P.L.; Missmer, S.A.; Flaws, J.A.; Berry, K.F.; Calafat, A.M.; Ye, X.; Petrozza, J.C.; Wright, D.; Hauser, R. Urinary Bisphenol A Concentrations and Implantation Failure among Women Undergoing In Vitro Fertilization. Environ. Health Perspect. 2012, 120, 978–983. [Google Scholar] [CrossRef] [Green Version]
- Déchaud, H.; Ravard, C.; Claustrat, F.; de la Perrière, A.B.; Pugeat, M. Xenoestrogen interaction with human sex hormone-binding globulin (hSHBG)1. Steroids 1999, 64, 328–334. [Google Scholar] [CrossRef]
- González, F.; Rote, N.S.; Minium, J.; Kirwan, J.P. Evidence of proatherogenic inflammation in polycystic ovary syndrome. Metabolism 2009, 58, 954–962. [Google Scholar] [CrossRef] [Green Version]
- Phrakonkham, P.; Viengchareun, S.; Belloir, C.; Lombès, M.; Artur, Y.; Canivenc-Lavier, M.-C. Dietary xenoestrogens differentially impair 3T3-L1 preadipocyte differentiation and persistently affect leptin synthesis. J. Steroid Biochem. Mol. Biol. 2008, 110, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Somm, E.; Schwitzgebel, V.M.; Toulotte, A.; Cederroth, C.R.; Combescure, C.; Nef, S.; Aubert, M.L.; Hüppi, P.S. Perinatal Exposure to Bisphenol A Alters Early Adipogenesis in the Rat. Environ. Health Perspect. 2009, 117, 1549–1555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wada, K.; Sakamoto, H.; Nishikawa, K.; Sakuma, S.; Nakajima, A.; Fujimoto, Y.; Kamisaki, Y. Life Style-Related Diseases of the Digestive System: Endocrine Disruptors Stimulate Lipid Accumulation in Target Cells Related to Metabolic Syndrome. J. Pharmacol. Sci. 2007, 105, 133–137. [Google Scholar] [CrossRef] [Green Version]
- Alonso-Magdalena, P.; Morimoto, S.; Ripoll, C.; Fuentes, E.; Nadal, A. The Estrogenic Effect of Bisphenol A Disrupts Pancreatic β-Cell Function In Vivo and Induces Insulin Resistance. Environ. Health Perspect. 2006, 114, 106–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, I.A.; Galloway, T.S.; Scarlett, A.; Henley, W.E.; Depledge, M.; Wallace, R.B.; Melzer, D. Association of Urinary Bisphenol A Concentration with Medical Disorders and Laboratory Abnormalities in Adults. JAMA 2008, 300, 1303–1310. [Google Scholar] [CrossRef] [PubMed]
- Hewlett, M.; Chow, E.; Aschengrau, A.; Mahalingaiah, S. Prenatal Exposure to Endocrine Disruptors: A Developmental Etiology for Polycystic Ovary Syndrome. Reprod. Sci. 2017, 24, 19–27. [Google Scholar] [CrossRef]
- Jayashree, S.; Indumathi, D.; Akilavalli, N.; Sathish, S.; Selvaraj, J.; Balasubramanian, K. Effect of Bisphenol-A on insulin signal transduction and glucose oxidation in liver of adult male albino rat. Environ. Toxicol. Pharmacol. 2013, 35, 300–310. [Google Scholar] [CrossRef]
- Nandi, A.; Sinha, N.; Ong, E.; Sonmez, H.; Poretsky, L. Is there a role for vitamin D in human reproduction? Horm. Mol. Biol. Clin. Investig. 2016, 25, 15–28. [Google Scholar] [CrossRef]
- Yaoi, T.; Itoh, K.; Nakamura, K.; Ogi, H.; Fujiwara, Y.; Fushiki, S. Genome-wide analysis of epigenomic alterations in fetal mouse forebrain after exposure to low doses of bisphenol A. Biochem. Biophys. Res. Commun. 2008, 376, 563–567. [Google Scholar] [CrossRef]
- Qu, F.; Wang, F.-F.; Yin, R.; Ding, G.-L.; El-Prince, M.; Gao, Q.; Shi, B.-W.; Pan, H.-H.; Huang, Y.-T.; Jin, M.; et al. A molecular mechanism underlying ovarian dysfunction of polycystic ovary syndrome: Hyperandrogenism induces epigenetic alterations in the granulosa cells. Klin. Wochenschr. 2012, 90, 911–923. [Google Scholar] [CrossRef]
- Virant-Klun, I.; Imamovic-Kumalic, S.; Pinter, B. From Oxidative Stress to Male Infertility: Review of the Associations of Endocrine-Disrupting Chemicals (Bisphenols, Phthalates, and Parabens) with Human Semen Quality. Antioxidants 2022, 11, 1617. [Google Scholar] [CrossRef] [PubMed]
- Braun, J.M.; Just, A.; Williams, P.L.; Smith, K.W.; Calafat, A.M.; Hauser, R. Personal care product use and urinary phthalate metabolite and paraben concentrations during pregnancy among women from a fertility clinic. J. Expo. Sci. Environ. Epidemiol. 2014, 24, 459–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matwiejczuk, N.; Galicka, A.; Brzóska, M.M. Review of the safety of application of cosmetic products containing parabens. J. Appl. Toxicol. 2020, 40, 176–210. [Google Scholar] [CrossRef]
- Ye, X.; Bishop, A.M.; Reidy, J.A.; Needham, L.L.; Calafat, A.M. Parabens as Urinary Biomarkers of Exposure in Humans. Environ. Health Perspect. 2006, 114, 1843–1846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azzouz, A.; Rascón, A.J.; Ballesteros, E. Simultaneous determination of parabens, alkylphenols, phenylphenols, bisphenol A and triclosan in human urine, blood and breast milk by continuous solid-phase extraction and gas chromatography-mass spectrometry. J. Pharm. Biomed. Anal. 2016, 119, 16–26. [Google Scholar] [CrossRef] [PubMed]
- Routledge, E.J.; Parker, J.; Odum, J.; Ashby, J.; Sumpter, J.P. Some Alkyl Hydroxy Benzoate Preservatives (Parabens) Are Estrogenic. Toxicol. Appl. Pharmacol. 1998, 153, 12–19. [Google Scholar] [CrossRef]
- Vo, T.T.; Yoo, Y.-M.; Choi, K.-C.; Jeung, E.-B. Potential estrogenic effect(s) of parabens at the prepubertal stage of a postnatal female rat model. Reprod. Toxicol. 2010, 29, 306–316. [Google Scholar] [CrossRef]
- Chen, J.; Ahn, K.C.; Gee, N.A.; Gee, S.J.; Hammock, B.D.; Lasley, B.L. Antiandrogenic properties of parabens and other phenolic containing small molecules in personal care products. Toxicol. Appl. Pharmacol. 2007, 221, 278–284. [Google Scholar] [CrossRef] [Green Version]
- Kang, K.-S.; Che, J.-H.; Ryu, D.-Y.; Kim, T.-W.; Li, G.-X.; Lee, Y.-S. Decreased Sperm Number and Motile Activity on the F1 Offspring Maternally Exposed to Butyl p-Hydroxybenzoic Acid(Butyl Paraben). J. Vet. Med. Sci. 2002, 64, 227–235. [Google Scholar] [CrossRef] [Green Version]
- Smith, K.W.; Souter, I.; Dimitriadis, I.; Ehrlich, S.; Williams, P.L.; Calafat, A.M.; Hauser, R. Urinary Paraben Concentrations and Ovarian Aging among Women from a Fertility Center. Environ. Health Perspect. 2013, 121, 1299–1305. [Google Scholar] [CrossRef] [Green Version]
- Jurewicz, J.; Radwan, M.; Wielgomas, B.; Karwacka, A.; Klimowska, A.; Kałużny, P.; Radwan, P.; Hanke, W. Parameters of ovarian reserve in relation to urinary concentrations of parabens. Environ. Health 2020, 19, 26. [Google Scholar] [CrossRef] [PubMed]
- Nishihama, Y.; Yoshinaga, J.; Iida, A.; Konishi, S.; Imai, H.; Yoneyama, M.; Nakajima, D.; Shiraishi, H. Association between paraben exposure and menstrual cycle in female university students in Japan. Reprod. Toxicol. 2016, 63, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Smarr, M.M.; Sundaram, R.; Honda, M.; Kannan, K.; Louis, G.B. Urinary Concentrations of Parabens and Other Antimicrobial Chemicals and Their Association with Couples’ Fecundity. Environ. Health Perspect. 2017, 125, 730–736. [Google Scholar] [CrossRef]
- Aker, A.M.; Watkins, D.J.; Johns, L.E.; Ferguson, K.K.; Soldin, O.P.; Del Toro, L.V.A.; Alshawabkeh, A.N.; Cordero, J.F.; Meeker, J.D. Phenols and parabens in relation to reproductive and thyroid hormones in pregnant women. Environ. Res. 2016, 151, 30–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mínguez-Alarcón, L.; Chiu, Y.-H.; Messerlian, C.; Williams, P.L.; Sabatini, M.E.; Toth, T.L.; Ford, J.B.; Calafat, A.M.; Hauser, R. Urinary paraben concentrations and in vitro fertilization outcomes among women from a fertility clinic. Fertil. Steril. 2016, 105, 714–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mínguez-Alarcón, L.; Messerlian, C.; Bellavia, A.; Gaskins, A.J.; Chiu, Y.-H.; Ford, J.B.; Azevedo, A.R.; Petrozza, J.C.; Calafat, A.M.; Hauser, R.; et al. Urinary concentrations of bisphenol A, parabens and phthalate metabolite mixtures in relation to reproductive success among women undergoing in vitro fertilization. Environ. Int. 2019, 126, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Maksymowicz, M.; Ręka, G.; Machowiec, P.; Piecewicz-Szczęsna, H. Impact of Triclosan on Female and Male Reproductive System and Its Consequences on Fertility; A Literature Review. J. Fam. Reprod. Health 2022, 16, 33–42. [Google Scholar] [CrossRef]
- Craig, Z.R.; Ziv-Gal, A. Pretty Good or Pretty Bad? The Ovary and Chemicals in Personal Care Products. Toxicol. Sci. 2017, 162, 349–360. [Google Scholar] [CrossRef] [Green Version]
- Derakhshan, A.; Shu, H.; Peeters, R.P.; Kortenkamp, A.; Lindh, C.H.; Demeneix, B.; Bornehag, C.-G.; Korevaar, T.I.M. Association of urinary bisphenols and triclosan with thyroid function during early pregnancy. Environ. Int. 2019, 133, 105123. [Google Scholar] [CrossRef]
- Commision Implementing Decision (EU) 2016/110 Not Approving Triclosan as an Existing Active Substance for Use in Biocidal Products Forproduct-Type 1. 2016. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32016D0110&from=PT (accessed on 8 October 2022).
- Wang, F.; Zheng, F.; Liu, F. Effects of triclosan on antioxidant- and apoptosis-related genes expression in the gill and ovary of zebrafish. Exp. Anim. 2020, 69, 199–206. [Google Scholar] [CrossRef] [Green Version]
- Cao, X.-Y.; Hua, X.; Xiong, J.-W.; Zhu, W.-T.; Zhang, J.; Chen, L. Impact of Triclosan on Female Reproduction through Reducing Thyroid Hormones to Suppress Hypothalamic Kisspeptin Neurons in Mice. Front. Mol. Neurosci. 2018, 11, 6. [Google Scholar] [CrossRef]
- Du, Y.; Wang, B.; Cai, Z.; Zhang, H.; Wang, B.; Liang, W.; Zhou, G.; Ouyang, F.; Wang, W. The triclosan-induced shift from aerobic to anaerobic metabolism link to increased steroidogenesis in human ovarian granulosa cells. Ecotoxicol. Environ. Saf. 2021, 220, 112389. [Google Scholar] [CrossRef] [PubMed]
- Mínguez-Alarcón, L.; Christou, G.; Messerlian, C.; Williams, P.L.; Carignan, C.C.; Souter, I.; Ford, J.B.; Calafat, A.M.; Hauser, R.; Keller, M.G.; et al. Urinary triclosan concentrations and diminished ovarian reserve among women undergoing treatment in a fertility clinic. Fertil. Steril. 2017, 108, 312–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jurewicz, J.; Wielgomas, B.; Radwan, M.; Karwacka, A.; Klimowska, A.; Dziewirska, E.; Korczak, K.; Zajdel, R.; Radwan, P.; Hanke, W. Triclosan exposure and ovarian reserve. Reprod. Toxicol. 2019, 89, 168–172. [Google Scholar] [CrossRef] [PubMed]
- Hua, R.; Zhou, Y.; Wu, B.; Huang, Z.; Zhu, Y.; Song, Y.; Yu, Y.; Li, H.; Quan, S. Urinary triclosan concentrations and early outcomes of in vitro fertilization-embryo transfer. Reproduction 2017, 153, 319–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vélez, M.P.; Arbuckle, T.E.; Fraser, W.D. Female exposure to phenols and phthalates and time to pregnancy: The Maternal-Infant Research on Environmental Chemicals (MIREC) Study. Fertil. Steril. 2015, 103, 1011–1020. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Liu, X.F.; Liu, Y.; Xu, L.Z.; Zhou, L.L.; Tang, L.L.; Zhuang, J.; Li, T.T.; Guo, W.Q.; Hu, R.; et al. Environmental risk factors for women with polycystic ovary syndrome in China: A population-based case-control study. J. Biol. Regul. Homeost. Agents 2014, 28, 203–211. [Google Scholar]
- Akin, L.; Kendirci, M.; Narin, F.; Kurtoglu, S.; Saraymen, R.; Kondolot, M.; Kocak, S.O.; Hatipoglu, N.; Elmali, F. The Role of Bisphenol A in Etiopathogenesis of Polycystic Ovary Syndrome in Adolescent Girls; ESPE: Dublin, Ireland, 2014. [Google Scholar]
- Cunningham, T.; Allgar, V.; Atkin, S.; Kilpatrick, E.; Maguiness, S.; Sathyapalan, T. A Prospective Cohort Study Investigating Endocrine Disrupting Agents and Polycystic Ovary Syndrome within an IVF Setting; Society for Endocrinology BES 2016: Brighton, UK, 2016. [Google Scholar]
- Lazurova, Z.; Figurova, J.; Hubkova, B.; Lazurova, I. Relationship of urinary bisphenol A to metabolic and hormonal profile in PCOS women. In Proceedings of the 20th European Congress of Endocrinology, Barcelona, Spain, 19–22 May 2018. [Google Scholar]
- Akgül, S.; Sur, Ü.; Düzçeker, Y.; Balcı, A.; Kızılkan, M.P.; Kanbur, N.; Bozdağ, G.; Erkekoğlu, P.; Gümüş, E.; Kocer-Gumusel, B.; et al. Bisphenol A and phthalate levels in adolescents with polycystic ovary syndrome. Gynecol. Endocrinol. 2019, 35, 1084–1087. [Google Scholar] [CrossRef]
- Akın, L.; Kendirci, M.; Narin, F.; Kurtoglu, S.; Saraymen, R.; Kondolot, M.; Koçak, S.; Elmalı, F.; Elmali, F. The endocrine disruptor bisphenol A may play a role in the aetiopathogenesis of polycystic ovary syndrome in adolescent girls. Acta Paediatr. 2015, 104, e171–e177. [Google Scholar] [CrossRef]
- Gu, J.; Yuan, T.; Ni, N.; Ma, Y.; Shen, Z.; Yu, X.; Shi, R.; Tian, Y.; Zhou, W.; Zhang, J. Urinary concentration of personal care products and polycystic ovary syndrome: A case-control study. Environ. Res. 2019, 168, 48–53. [Google Scholar] [CrossRef]
- Rashidi, B.H.; Amanlou, M.; Lak, T.B.; Ghazizadeh, M.; Haghollahi, F.; Bagheri, M.; Eslami, B. The Association Between Bisphenol A and Polycystic Ovarian Syndrome: A Case-Control Study. Acta MEDICA Iran. 2017, 55, 759–764. [Google Scholar]
- Jędrzejuk, D.; Kuliczkowska-Płaksej, J.; Milewicz, A.; Wilczewska, K.; Namieśnik, J.; Rutkowska, A. Bisphenol A levels are inversely associated with serum vitamin D-binding protein and sex hormone-binding globulin levels in women with polycystic ovary syndrome: A pilot study. Pol. Arch. Intern. Med. 2019, 129, 133–136. [Google Scholar] [CrossRef] [Green Version]
- Kandaraki, E.; Chatzigeorgiou, A.; Livadas, S.; Palioura, E.; Economou, F.; Koutsilieris, M.; Palimeri, S.; Panidis, D.; Diamanti-Kandarakis, E. Endocrine Disruptors and Polycystic Ovary Syndrome (PCOS): Elevated Serum Levels of Bisphenol A in Women with PCOS. J. Clin. Endocrinol. Metab. 2011, 96, E480–E484. [Google Scholar] [CrossRef]
- Konieczna, A.; Rachoń, D.; Owczarek, K.; Kubica, P.; Kowalewska, A.; Kudłak, B.; Wasik, A.; Namieśnik, J. Serum bisphenol A concentrations correlate with serum testosterone levels in women with polycystic ovary syndrome. Reprod. Toxicol. 2018, 82, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Lazúrová, Z.; Figurová, J.; Hubková, B.; Mašlanková, J.; Lazúrová, I. Urinary bisphenol A in women with polycystic ovary syndrome—A possible suppressive effect on steroidogenesis? Horm. Mol. Biol. Clin. Investig. 2021, 42, 303–309. [Google Scholar] [CrossRef]
- Luo, Y.; Nie, Y.; Tang, L.; Xu, C.C.; Xu, L. The correlation between UDP-glucuronosyltransferase polymorphisms and environmental endocrine disruptors levels in polycystic ovary syndrome patients. Medicine 2020, 99, e19444. [Google Scholar] [CrossRef] [PubMed]
- Šimková, M.; Vítků, J.; Kolátorová, L.; Vrbíková, J.; Vosátková, M.; Včelák, J.; Dušková, M. Endocrine Disruptors, Obesity, and Cytokines—How Relevant Are They to PCOS? Physiol. Res. 2020, 69, S279–S293. [Google Scholar] [CrossRef]
- Tarantino, G.; Valentino, R.; Di Somma, C.; D’Esposito, V.; Passaretti, F.; Pizza, G.; Brancato, V.; Orio, F.; Formisano, P.; Colao, A.; et al. Bisphenol A in polycystic ovary syndrome and its association with liver-spleen axis. Clin. Endocrinol. 2013, 78, 447–453. [Google Scholar] [CrossRef]
- Vagi, S.J.; Azziz-Baumgartner, E.; Sjödin, A.; Calafat, A.M.; Dumesic, D.; Gonzalez, L.; Kato, K.; Silva, M.J.; Ye, X.; Azziz, R. Exploring the potential association between brominated diphenyl ethers, polychlorinated biphenyls, organochlorine pesticides, perfluorinated compounds, phthalates, and bisphenol a in polycystic ovary syndrome: A case-control study. BMC Endocr. Disord. 2014, 14, 86. [Google Scholar] [CrossRef] [Green Version]
- Vahedi, M.; Saeedi, A.; Poorbaghi, S.L.; Sepehrimanesh, M.; Fattahi, M.R. Metabolic and endocrine effects of bisphenol A exposure in market seller women with polycystic ovary syndrome. Environ. Sci. Pollut. Res. 2016, 23, 23546–23550. [Google Scholar] [CrossRef]
- Wang, Y.; Zhu, Q.; Dang, X.; He, Y.; Li, X.; Sun, Y. Local effect of bisphenol A on the estradiol synthesis of ovarian granulosa cells from PCOS. Gynecol. Endocrinol. 2017, 33, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.; Fang, F.; Zhu, W.; Chen, Z.-J.; Du, Y.; Zhang, J. Bisphenol A and Ovarian Reserve among Infertile Women with Polycystic Ovarian Syndrome. Int. J. Environ. Res. Public Health 2016, 14, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takeuchi, T.; Tsutsumi, O.; Ikezuki, Y.; Takai, Y.; Taketani, Y. Positive Relationship between Androgen and the Endocrine Disruptor, Bisphenol A, in Normal Women and Women with Ovarian Dysfunction. Endocr. J. 2004, 51, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Hanioka, N.; Jinno, H.; Nishimura, T.; Ando, M. Suppression of male-specific cytochrome P450 isoforms by bisphenol A in rat liver. Arch. Toxicol. 1998, 72, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Li, D.-K.; Miao, M.; Zhou, Z.; Wu, C.; Shi, H.; Liu, X.; Wang, S.; Yuan, W. Urine Bisphenol-A Level in Relation to Obesity and Overweight in School-Age Children. PLoS ONE 2013, 8, e65399. [Google Scholar] [CrossRef] [Green Version]
- Palioura, E.; Kandaraki, E.; Diamanti-Kandarakis, E. Endocrine disruptors and polycystic ovary syndrome: A focus on Bisphenol A and its potential pathophysiological aspects. Horm. Mol. Biol. Clin. Investig. 2014, 17, 137–144. [Google Scholar] [CrossRef]
- Park, S.Y.; Jeon, J.H.; Jeong, K.; Chung, H.W.; Lee, H.; Sung, Y.-A.; Ye, S.; Ha, E.-H. The Association of Ovarian Reserve with Exposure to Bisphenol A and Phthalate in Reproductive-aged Women. J. Korean Med. Sci. 2021, 36, e1. [Google Scholar] [CrossRef]
- Silvestris, E.; Cohen, M.; Cornet, D.; Jacquesson-Fournols, L.; Clement, P.; Chouteau, J.; Schneider, M.; Besnard, T.; Ménézo, Y. Supporting the One-Carbon Cycle Restores Ovarian Reserve in Subfertile Women: Absence of Correlation with Urinary Bisphenol A Concentration. BioRes. Open Access 2017, 6, 104–109. [Google Scholar] [CrossRef]
- Mok-Lin, E.; Ehrlich, S.; Williams, P.L.; Petrozza, J.; Wright, D.L.; Calafat, A.M.; Ye, X.; Hauser, R. Urinary bisphenol A concentrations and ovarian response among women undergoing IVF. Int. J. Androl. 2010, 33, 385–393. [Google Scholar] [CrossRef]
- Wu, L.-H.; Zhang, X.-M.; Wang, F.; Gao, C.-J.; Chen, D.; Palumbo, J.R.; Guo, Y.; Zeng, E.Y. Occurrence of bisphenol S in the environment and implications for human exposure: A short review. Sci. Total Environ. 2018, 615, 87–98. [Google Scholar] [CrossRef]
- Asimakopoulos, A.G.; Xue, J.; De Carvalho, B.P.; Iyer, A.; Abualnaja, K.O.; Yaghmoor, S.S.; Kumosani, T.A.; Kannan, K. Urinary biomarkers of exposure to 57 xenobiotics and its association with oxidative stress in a population in Jeddah, Saudi Arabia. Environ. Res. 2016, 150, 573–581. [Google Scholar] [CrossRef] [PubMed]
- Ye, J.; Zhu, W.; Liu, H.; Mao, Y.; Jin, F.; Zhang, J. Environmental exposure to triclosan and polycystic ovary syndrome: A cross-sectional study in China. BMJ Open 2018, 8, e019707. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Source | Study Design | Sample of Participants (No. of Women) | Sample Type | Exposure | Main Findings |
|---|---|---|---|---|---|
| Akgül et al. (2019), Turkey [84] | Case-control study | 95 aged 12–18 years: 62 with PCOS, 33 controls | Blood plasma, urine samples | BPA, phthalates |
|
| Akin et al. (2015), Turkey [85] | Cross-sectional study | 173 aged 13–19 years: 112 with PCOS, 61 controls | Blood serum | BPA |
|
| Gu et al. (2019) [86] | Case-control study | 123: 40 with PCOS, 83 controls | Urine sample | Organic UV filters, BPA, triclosan |
|
| Hossein Rashidi et al. (2017), Iran [87] | Case-control study | 102: 51 with PCOS, 51 controls | First morning urine sample | BPA |
|
| Jędrzejuk et al. (2019), Poland [88] | Pilot study | 63: 27 with PCOS, 36 controls | Blood sample | BPA |
|
| Kandaraki et al. (2011), United Kingdom, Greece [89] | Cross-sectional study | 171: 71 with PCOS, 100 controls | Blood serum | BPA |
|
| Konieczna et al. (2018), Poland [90] | Cross-sectional study | 186: 106 with PCOS, 80 controls | Blood serum | BPA |
|
| Lazúrová et al. (2021), Slovakia [91] | Case-control study | 118: 86 with PCOS, 32 controls | Fasting blood and morning urinary samples | BPA |
|
| Luo et al. (2020), China [92] | Case-control study | 357: 119 with PCOS, 238 controls | Blood plasma | BPA, polybrominated diphenyl ethers, phthalates |
|
| Šimková et al. (2020), Czech Republic [93] | Case-control study | 39: 19 with PCOS (9 normal-weight, 10 obese), 20 controls | Blood plasma | Parabens, BPA, BPS, BPF, BPAF |
|
| Tarantino et al. (2013), Italy [94] | Cross-sectional study | 60: 40 with PCOS, 20 controls | Blood serum | BPA |
|
| Vagi et al. (2014), USA [95] | Case-control study | 102: 52 with PCOS, 50 controls | Blood and urinary samples | Brominated diphenyl ethers, polychlorinated biphenyls, organochlorine pesticides, perfluorinated compounds, phthalates, and BPA |
|
| Vahedi et al. (2016), Iran [96] | Case-control study | 124: 62 with PCOS, 62 controls | Blood serum | BPA |
|
| Wang et al. (2017), China [97] | Case-control study | 38: 21 with PCOS, 17 controls | Follicular fluid and ovarian granulosa cells | BPA |
|
| Zhou et al. (2016), China [98] | Cross-sectional study | 268 infertile women diagnosed with PCOS | Urinary sample | BPA |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Srnovršnik, T.; Virant-Klun, I.; Pinter, B. Polycystic Ovary Syndrome and Endocrine Disruptors (Bisphenols, Parabens, and Triclosan)—A Systematic Review. Life 2023, 13, 138. https://doi.org/10.3390/life13010138
Srnovršnik T, Virant-Klun I, Pinter B. Polycystic Ovary Syndrome and Endocrine Disruptors (Bisphenols, Parabens, and Triclosan)—A Systematic Review. Life. 2023; 13(1):138. https://doi.org/10.3390/life13010138
Chicago/Turabian StyleSrnovršnik, Tinkara, Irma Virant-Klun, and Bojana Pinter. 2023. "Polycystic Ovary Syndrome and Endocrine Disruptors (Bisphenols, Parabens, and Triclosan)—A Systematic Review" Life 13, no. 1: 138. https://doi.org/10.3390/life13010138