
Assessment of Eating Disorders and Eating Behavior to Improve Treatment Outcomes in Women with Polycystic Ovary Syndrome

Abstract
:1. Introduction
2. Eating Disorders in PCOS
2.1. Classification of Eating Disorders
2.2. Prevalence of Eating Disorders in PCOS
2.3. The Casual Link between Eating Disorders and PCOS
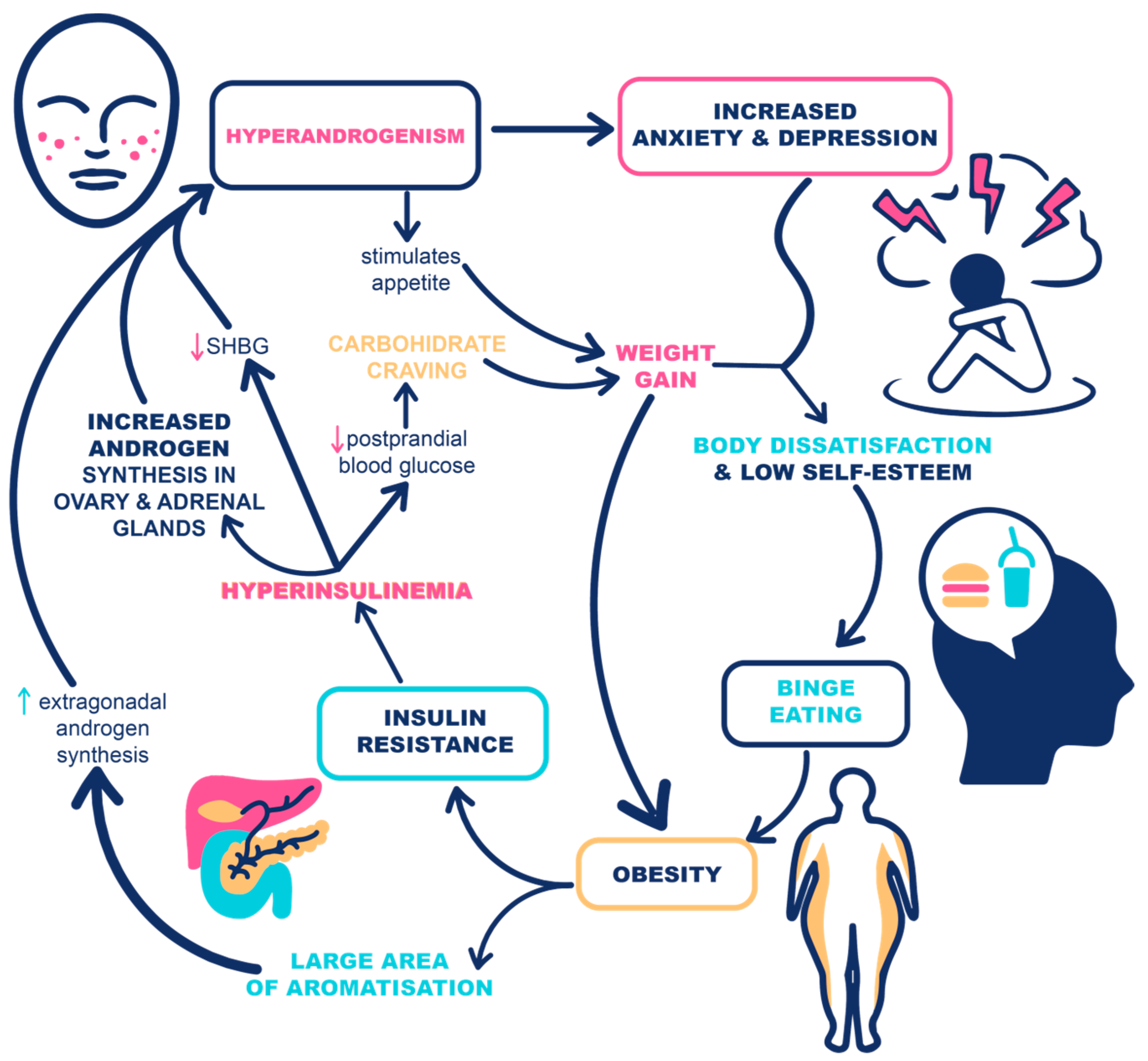
2.4. The Vicious Cycle of PCOS, Eating Disorders, and Obesity
3. Eating Behavior
3.1. Regulation of Eating Behavior
3.2. Assessment of Eating Behavior
4. Assessment of Eating Disorders and Behavior to Improve Anti-Obesity Treatment in PCOS
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Azziz, R.; Carmina, E.; Chen, Z.; Dunaif, A.; Laven, J.S.E.; Legro, R.S.; Yildiz, B.O.; Lizneva, D.; Natterson-Horowtiz, B.; Teede, H.J. Polycystic ovary syndrome. Nat. Rev. Dis. Primers 2016, 2, 16057. [Google Scholar] [CrossRef] [PubMed]
- Lizneva, D.; Suturina, L.; Walker, W.; Brakta, S.; Gavrilova-Jordan, L.; Azziz, R. Criteria, prevalence, and phenotypes of polycystic ovary syndrome. Fertil. Steril. 2016, 106, 6–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ilie, I.R. Advances in PCOS Pathogenesis and Progression-Mitochondrial Mutations and Dysfunction. Adv. Clin. Chem. 2018, 86, 127–155. [Google Scholar] [PubMed]
- Balen, A. The pathophysiology of polycystic ovary syndrome: Trying to understand PCOS and its endocrinology. Best Pract. Res. Clin. Obstet. Gynaecol. 2004, 18, 685–706. [Google Scholar] [CrossRef]
- Naderpoor, N.; Shorakae, S.; Joham, A.; Boyle, J.; De Courten, B.; Teede, H.J. Obesity and polycystic ovary syndrome. Minerva Endocrinol. 2015, 40, 37–51. [Google Scholar]
- Barber, T.M.; Franks, S. Obesity and polycystic ovary syndrome. Clin. Endocrinol. 2021, 95, 531–541. [Google Scholar] [CrossRef]
- Moran, L.; Gibson-Helm, M.; Teede, H.; Deeks, A. Polycystic ovary syndrome: A biopsychosocial understanding in young women to improve knowledge and treatment options. J. Psychosom. Obstet. Gynaecol. 2010, 31, 24–31. [Google Scholar] [CrossRef]
- Hart, R.; Doherty, D.A. The potential implications of a PCOS diagnosis on a woman’s long-term health using data linkage. J. Clin. Endocrinol. Metab. 2015, 100, 911–919. [Google Scholar] [CrossRef] [Green Version]
- Dokras, A.; Clifton, S.; Futterweit, W.; Wild, R. Increased prevalence of anxiety symptoms in women with polycystic ovary syndrome: Systematic review and meta-analysis. Fertil. Steril. 2012, 97, 225–230.e2. [Google Scholar] [CrossRef]
- Lee, I.; Cooney, L.G.; Saini, S.; Smith, M.E.; Sammel, M.D.; Allison, K.C.; Dokras, A. Increased risk of disordered eating in polycystic ovary syndrome. Fertil. Steril. 2017, 107, 796–802. [Google Scholar] [CrossRef] [Green Version]
- Jedel, E.; Waern, M.; Gustafson, D.; Landén, M.; Eriksson, E.; Holm, G.; Nilsson, L.; Lind, A.-K.; Janson, P.O.; Stener-Victorin, E. Anxiety and depression symptoms in women with polycystic ovary syndrome compared with controls matched for body mass index. Hum. Reprod. 2010, 25, 450–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azizi, M.; Elyasi, F. Psychosomatic Aspects of Polycystic Ovarian Syndrome: A Review. Iran. J. Psychiatry Behav. Sci. 2017, in press. [Google Scholar] [CrossRef]
- Lie Fong, S.; Douma, A.; Verhaeghe, J. Implementing the international evidence-based guideline of assessment and management of polycystic ovary syndrome (PCOS): How to achieve weight loss in overweight and obese women with PCOS? J. Gynecol. Obstet. Hum. Reprod. 2021, 50, 101894. [Google Scholar] [CrossRef] [PubMed]
- Treasure, J.; Duarte, T.A.; Schmidt, U. Eating disorders. Lancet 2020, 395, 899–911. [Google Scholar] [CrossRef]
- Hollinrake, E.; Abreu, A.; Maifeld, M.; Van Voorhis, B.J.; Dokras, A. Increased risk of depressive disorders in women with polycystic ovary syndrome. Fertil. Steril. 2007, 87, 1369–1376. [Google Scholar] [CrossRef]
- Månsson, M.; Holte, J.; Landin-Wilhelmsen, K.; Dahlgren, E.; Johansson, A.; Landén, M. Women with polycystic ovary syndrome are often depressed or anxious--a case control study. Psychoneuroendocrinology 2008, 33, 1132–1138. [Google Scholar] [CrossRef]
- Tay, C.T.; Teede, H.J.; Hill, B.; Loxton, D.; Joham, A.E. Increased prevalence of eating disorders, low self-esteem, and psychological distress in women with polycystic ovary syndrome: A community-based cohort study. Fertil. Steril. 2019, 112, 353–361. [Google Scholar] [CrossRef]
- Annagür, B.B.; Kerimoglu, Ö.S.; Tazegül, A.; Gündüz, Ş.; Gençoglu, B.B. Psychiatric comorbidity in women with polycystic ovary syndrome. J. Obstet. Gynaecol. Res. 2015, 41, 1229–1233. [Google Scholar] [CrossRef]
- Kerchner, A.; Lester, W.; Stuart, S.P.; Dokras, A. Risk of depression and other mental health disorders in women with polycystic ovary syndrome: A longitudinal study. Fertil. Steril. 2009, 91, 207–212. [Google Scholar] [CrossRef]
- Jeanes, Y.M.; Reeves, S.; Gibson, E.L.; Piggott, C.; May, V.A.; Hart, K.H. Binge eating behaviours and food cravings in women with Polycystic Ovary Syndrome. Appetite 2017, 109, 24–32. [Google Scholar] [CrossRef] [Green Version]
- Asdaq, S.M.B.; Jomah, S.; Hasan, R.; Al-Baroudi, D.; Alharbi, M.; Alsubaie, S.; Buhamad, M.H.; Alyahya, B.; Al-Yamani, M.J. Impact of polycystic ovary syndrome on eating behavior, depression and health related quality of life: A cross-sectional study in Riyadh. Saudi J. Biol. Sci. 2020, 27, 3342–3347. [Google Scholar] [CrossRef] [PubMed]
- Bernadett, M. Prevalence of eating disorders among women with polycystic ovary syndrome. Psychiatr Hung. 2016, 31, 136–145. [Google Scholar]
- Thannickal, A.; Brutocao, C.; Alsawas, M.; Morrow, A.; Zaiem, F.; Murad, M.H.; Chattha, A.J. Eating, sleeping and sexual function disorders in women with polycystic ovary syndrome (PCOS): A systematic review and meta-analysis. Clin. Endocrinol. 2020, 92, 338–349. [Google Scholar] [CrossRef] [PubMed]
- Morgan, J.; Scholtz, S.; Lacey, H.; Conway, G. The prevalence of eating disorders in women with facial hirsutism: An epidemiological cohort study. Int. J. Eat. Disord. 2008, 41, 427–431. [Google Scholar] [CrossRef]
- American Psychiatric Association Division of Research. Highlights of Changes from DSM-IV to DSM-5. FOCUS 2013, 11, 525–527. [Google Scholar] [CrossRef]
- Farrell, K.; Antoni, M.H. Insulin resistance, obesity, inflammation, and depression in polycystic ovary syndrome: Biobehavioral mechanisms and interventions. Fertil. Steril. 2010, 94, 1565–1574. [Google Scholar] [CrossRef] [Green Version]
- Setji, T.L.; Brown, A.J. Comprehensive clinical management of polycystic ovary syndrome. Minerva Med. 2007, 98, 175–189. [Google Scholar]
- Teede, H.J.; Misso, M.L.; Costello, M.F.; Dokras, A.; Laven, J.; Moran, L.; Piltonen, T.; Norman, R.J.; International PCOS Network. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Hum. Reprod. 2018, 33, 1602–1618. [Google Scholar] [CrossRef] [Green Version]
- Moghetti, P.; Tosi, F. Insulin resistance and PCOS: Chicken or egg? J. Endocrinol. Investig. 2021, 44, 233–244. [Google Scholar] [CrossRef]
- Sadeeqa, S.; Mustafa, T.; Latif, S. Polycystic Ovarian Syndrome-Related Depression in Adolescent Girls: A Review. J. Pharm. Bioallied. Sci. 2018, 10, 55–59. [Google Scholar] [CrossRef]
- Baker, J.H.; Girdler, S.S.; Bulik, C.M. The role of reproductive hormones in the development and maintenance of eating disorders. Expert Rev. Obstet. Gynecol. 2012, 7, 573–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sundblad, C.; Bergman, L.; Eriksson, E. High levels of free testosterone in women with bulimia nervosa. Acta Psychiatr. Scand. 1994, 90, 397–398. [Google Scholar] [CrossRef] [PubMed]
- Sundblad, C.; Landén, M.; Eriksson, T.; Bergman, L.; Eriksson, E. Effects of the Androgen Antagonist Flutamide and the Serotonin Reuptake Inhibitor Citalopram in Bulimia Nervosa. J. Clin. Psychopharmacol. 2005, 25, 85–88. [Google Scholar] [CrossRef] [PubMed]
- Krug, I.; Giles, S.; Paganini, C. Binge eating in patients with polycystic ovary syndrome: Prevalence, causes, and management strategies. Neuropsychiatr. Dis. Treat. 2019, 15, 1273–1285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garvey, W.T. Is Obesity or Adiposity-Based Chronic Disease Curable: The Set Point Theory, the Environment, and Second-Generation Medications. Endocr. Pract. Off. J. Am. Coll. Endocrinol. Am. Assoc. Clin. Endocrinol. 2022, 28, 214–222. [Google Scholar] [CrossRef] [PubMed]
- Karacan, E.; Caglar, G.S.; Gürsoy, A.Y.; Yilmaz, M.B. Body satisfaction and eating attitudes among girls and young women with and without polycystic ovary syndrome. J. Pediatr. Adolesc. Gynecol. 2014, 27, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Frisch, R.E.; Revelle, R. Height and weight at menarche and a hypothesis of critical body weights and adolescent events. Science 1970, 169, 397–399. [Google Scholar] [CrossRef]
- Biro, F.M.; Galvez, M.P.; Greenspan, L.C.; Succop, P.A.; Vangeepuram, N.; Pinney, S.M.; Teitelbaum, S.; Windham, G.C.; Kushi, L.H.; Wolff, M.S. Pubertal assessment method and baseline characteristics in a mixed longitudinal study of girls. Pediatrics 2010, 126, e583–e590. [Google Scholar] [CrossRef] [Green Version]
- Durda-Masny, M.; Hanć, T.; Czapla, Z.; Szwed, A. BMI at menarche and timing of growth spurt and puberty in Polish girls-longitudinal study. Anthropol. Anz. Ber. Uber Biol.-Anthropol. Lit. 2019, 76, 37–47. [Google Scholar] [CrossRef]
- de Siqueira Barros, B.; Kuschnir, M.C.M.C.; Bloch, K.V.; da Silva, T.L.N. ERICA: Age at menarche and its association with nutritional status. J. Pediatr. 2019, 95, 106–111. [Google Scholar] [CrossRef]
- Quennell, J.H.; Mulligan, A.C.; Tups, A.; Liu, X.; Phipps, S.J.; Kemp, C.J.; Herbison, A.; Grattan, D.; Anderson, G.M. Leptin Indirectly Regulates Gonadotropin-Releasing Hormone Neuronal Function. Endocrinology 2009, 150, 2805–2812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, M.L.; Ong, K.K.; Dunger, D.B. Childhood obesity and the timing of puberty. Trends Endocrinol. Metab. 2009, 20, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Heras, V.; Castellano, J.M.; Fernandois, D.; Velasco, I.; Rodríguez-Vazquez, E.; Roa, J.; Vazquez, M.J.; Ruiz-Pino, F.; Rubio, M.; Pineda, R.; et al. Central Ceramide Signaling Mediates Obesity-Induced Precocious Puberty. Cell Metab. 2020, 32, 951–966.e8. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Shen, S.; Tan, Y.; Xia, D.; Xia, Y.; Cao, Y.; Wang, W.; Wu, X.; Wang, H.; Yi, L.; et al. The correlation of aromatase activity and obesity in women with or without polycystic ovary syndrome. J. Ovarian Res. 2015, 8, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Apter, D.; Bützow, T.; Laughlin, G.A.; Yen, S.S. Metabolic features of polycystic ovary syndrome are found in adolescent girls with hyperandrogenism. J. Clin. Endocrinol. Metab. 1995, 80, 2966–2973. [Google Scholar] [PubMed]
- Wei, S.; Schmidt, M.D.; Dwyer, T.; Norman, R.J.; Venn, A.J. Obesity and menstrual irregularity: Associations with SHBG, testosterone, and insulin. Obes. Silver Spring Md. 2009, 17, 1070–1076. [Google Scholar] [CrossRef]
- Diamanti-Kandarakis, E.; Papavassiliou, A.G. Molecular mechanisms of insulin resistance in polycystic ovary syndrome. Trends Mol. Med. 2006, 12, 324–332. [Google Scholar] [CrossRef]
- Tosi, F.; Bonora, E.; Moghetti, P. Insulin resistance in a large cohort of women with polycystic ovary syndrome: A comparison between euglycaemic-hyperinsulinaemic clamp and surrogate indexes. Hum. Reprod. 2017, 32, 2515–2521. [Google Scholar] [CrossRef] [Green Version]
- Itriyeva, K. The effects of obesity on the menstrual cycle. Curr. Probl. Pediatr. Adolesc. Health Care 2022, 52, 101241. [Google Scholar] [CrossRef]
- Sam, S. Obesity and Polycystic Ovary Syndrome. Obes. Manag. 2007, 3, 69–73. [Google Scholar] [CrossRef]
- Grimm, E.R.; Steinle, N.I. Genetics of eating behavior: Established and emerging concepts. Nutr Rev. 2011, 69, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Badman, M.K.; Flier, J.S. The gut and energy balance: Visceral allies in the obesity wars. Science 2005, 307, 1909–1914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klok, M.D.; Jakobsdottir, S.; Drent, M.L. The role of leptin and ghrelin in the regulation of food intake and body weight in humans: A review. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2007, 8, 21–34. [Google Scholar] [CrossRef] [PubMed]
- Berridge, K.C.; Ho, C.Y.; Richard, J.M.; DiFeliceantonio, A.G. The tempted brain eats: Pleasure and desire circuits in obesity and eating disorders. Brain Res. 2010, 1350, 43–64. [Google Scholar] [CrossRef] [Green Version]
- Vallis, M. Sustained behaviour change in healthy eating to improve obesity outcomes: It is time to abandon willpower to appreciate wanting. Clin. Obes. 2019, 9, e12299. [Google Scholar] [CrossRef] [Green Version]
- Brzechffa, P.R.; Jakimiuk, A.J.; Agarwal, S.K.; Weitsman, S.R.; Buyalos, R.P.; Magoffin, D.A. Serum immunoreactive leptin concentrations in women with polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 1996, 81, 4166–4169. [Google Scholar]
- Blüher, S.; Mantzoros, C.S. Leptin in humans: Lessons from translational research. Am. J. Clin. Nutr. 2009, 89, 991S–997S. [Google Scholar] [CrossRef] [Green Version]
- Kieffer, T.J.; Heller, R.S.; Leech, C.A.; Holz, G.G.; Habener, J.F. Leptin suppression of insulin secretion by the activation of ATP-sensitive K+ channels in pancreatic beta-cells. Diabetes 1997, 46, 1087–1093. [Google Scholar] [CrossRef] [Green Version]
- Casabiell, X.; Piñeiro, V.; Vega, F.; De La Cruz, L.F.; Diéguez, C.; Casanueva, F.F. Leptin, reproduction and sex steroids. Pituitary 2001, 4, 93–99. [Google Scholar] [CrossRef]
- Erturk, E.; Kuru, N.; Savcı, V.; Tuncel, E.; Ersoy, C.; Imamoglu, S. Serum leptin levels correlate with obesity parameters but not with hyperinsulinism in women with polycystic ovary syndrome. Fertil. Steril. 2004, 82, 1364–1368. [Google Scholar] [CrossRef]
- Morin-Papunen, L.C.; Koivunen, R.M.; Tomás, C.; Ruokonen, A.; Martikainen, H.K. Decreased serum leptin concentrations during metformin therapy in obese women with polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 1998, 83, 2566–2568. [Google Scholar] [CrossRef] [PubMed]
- Romualdi, D.; Campagna, G.; Selvaggi LJr Cento, R.; Proto, C.; Lanzone, A.; Guido, M. Metformin treatment does not affect total leptin levels and free leptin index in obese patients with polycystic ovary syndrome. Fertil. Steril. 2008, 89, 1273–1276. [Google Scholar] [CrossRef] [PubMed]
- Romualdi, D.; Immediata, V.; De Cicco, S.; Tagliaferri, V.; Lanzone, A. Neuroendocrine Regulation of Food Intake in Polycystic Ovary Syndrome. Reprod. Sci. 2018, 25, 644–653. [Google Scholar]
- Acosta, A.; Camilleri, M.; Abu Dayyeh, B.; Calderon, G.; Gonzalez, D.; McRae, A.; Rossini, W.; Singh, S.; Burton, D.; Clark, M.M. Selection of Antiobesity Medications Based on Phenotypes Enhances Weight Loss: A Pragmatic Trial in an Obesity Clinic. Obes. Silver Spring Md. 2021, 29, 662–671. [Google Scholar] [CrossRef] [PubMed]
- Barrea, L.; Verde, L.; Vetrani, C.; Savastano, S.; Colao, A.; Muscogiuri, G. Chronotype: A Tool to Screen Eating Habits in Polycystic Ovary Syndrome? Nutrients 2022, 14, 955. [Google Scholar] [CrossRef] [PubMed]
- Eleftheriadou, M.; Stefanidis, K.; Lykeridou, K.; Iliadis, I.; Michala, L. Dietary habits in adolescent girls with polycystic ovarian syndrome. Gynecol. Endocrinol. Off. J. Int. Soc. Gynecol. Endocrinol. 2015, 31, 269–271. [Google Scholar] [CrossRef]
- Kulshreshtha, B.; Sharma, N.; Pant, S.; Sharma, L.; Pahuja, B.; Singh, P. PCOS patients differ in meal timings rather than total caloric or macronutrient intake in comparison to weight matched controls. Eur. J. Obstet. Gynecol. Reprod. Biol. 2022, 270, 11–16. [Google Scholar] [CrossRef]
- De Giuseppe, R.; Braschi, V.; Bosoni, D.; Biino, G.; Stanford, F.C.; Nappi, R.E.; Cena, H. Dietary underreporting in women affected by polycystic ovary syndrome: A pilot study. Nutr. Diet J. Dietit. Assoc. Aust. 2019, 76, 560–566. [Google Scholar] [CrossRef]
- Cetik, S.; Acikgoz, A.; Yildiz, B.O. Investigation of taste function and eating behavior in women with polycystic ovary syndrome. Appetite 2022, 168, 105776. [Google Scholar] [CrossRef]
- Jensterle, M.; Ferjan, S.; Battelino, T.; Kovač, J.; Battelino, S.; Šuput, D.; Vovk, A.; Janež, A. Does intervention with GLP-1 receptor agonist semaglutide modulate perception of sweet taste in women with obesity: Study protocol of a randomized, single-blinded, placebo-controlled clinical trial. Trials 2021, 22, 464. [Google Scholar] [CrossRef]
- Jensterle, M.; Herman, R.; Janež, A. Therapeutic Potential of Glucagon-like Peptide-1 Agonists in Polycystic Ovary Syndrome: From Current Clinical Evidence to Future Perspectives. Biomedicines 2022, 10, 1989. [Google Scholar] [CrossRef] [PubMed]
- Ornstein, R.M.; Copperman, N.M.; Jacobson, M.S. Effect of weight loss on menstrual function in adolescents with polycystic ovary syndrome. J. Pediatr. Adolesc. Gynecol. 2011, 24, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Ozgen Saydam, B.; Yildiz, B.O. Weight management strategies for patients with PCOS: Current perspectives. Expert Rev. Endocrinol. Metab. 2021, 16, 49–62. [Google Scholar] [CrossRef]
- Jarrett, B.Y.; Lujan, M.E. Impact of hypocaloric dietary intervention on ovulation in obese women with PCOS. Reproduction 2017, 153, R15–R27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barrea, L.; Arnone, A.; Annunziata, G.; Muscogiuri, G.; Laudisio, D.; Salzano, C.; Pugliese, G.; Colao, A.; Savastano, S. Adherence to the Mediterranean Diet, Dietary Patterns and Body Composition in Women with Polycystic Ovary Syndrome (PCOS). Nutrients 2019, 11, 2278. [Google Scholar] [CrossRef]
- Barrea, L.; Muscogiuri, G.; Macchia, P.E.; Di Somma, C.; Falco, A.; Savanelli, M.C.; Colao, A.; Savastano, S. Mediterranean Diet and Phase Angle in a Sample of Adult Population: Results of a Pilot Study. Nutrients 2017, 9, 151. [Google Scholar] [CrossRef] [Green Version]
- Toosy, S.; Sodi, R.; Pappachan, J.M. Lean polycystic ovary syndrome (PCOS): An evidence-based practical approach. J. Diabetes Metab. Disord. 2018, 17, 277–285. [Google Scholar] [CrossRef]
- Patten, R.K.; Boyle, R.A.; Moholdt, T.; Kiel, I.; Hopkins, W.G.; Harrison, C.L.; Stepto, N.K. Exercise Interventions in Polycystic Ovary Syndrome: A Systematic Review and Meta-Analysis. Front. Physiol. 2020, 11, 606. [Google Scholar] [CrossRef]
- Stahl, J.M.; Malhotra, S. Obesity Surgery Indications and Contraindications. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: http://www.ncbi.nlm.nih.gov/books/NBK513285/ (accessed on 15 October 2022).
- Hu, L.; Ma, L.; Xia, X.; Ying, T.; Zhou, M.; Zou, S.; Yu, H.; Yin, J. Efficacy of Bariatric Surgery in the Treatment of Women With Obesity and Polycystic Ovary Syndrome. J. Clin. Endocrinol. Metab. 2022, 107, e3217–e3229. [Google Scholar] [CrossRef]
- Al-Najim, W.; Docherty, N.G.; le Roux, C.W. Food Intake and Eating Behavior After Bariatric Surgery. Physiol. Rev. 2018, 98, 1113–1141. [Google Scholar] [CrossRef] [Green Version]
- Grams, J.; Garvey, W.T. Weight Loss and the Prevention and Treatment of Type 2 Diabetes Using Lifestyle Therapy, Pharmacotherapy, and Bariatric Surgery: Mechanisms of Action. Curr. Obes. Rep. 2015, 4, 287–302. [Google Scholar] [CrossRef] [PubMed]
- Guerciolini, R. Mode of action of orlistat. Int. J. Obes. Relat. Metab. Disord. 1997, 21 (Suppl. S3), S12–S23. [Google Scholar] [PubMed]
- Fruzzetti, F.; Bersi, C.; Parrini, D.; Ricci, C.; Genazzani, A.R. Effect of long-term naltrexone treatment on endocrine profile, clinical features, and insulin sensitivity in obese women with polycystic ovary syndrome. Fertil. Steril. 2002, 77, 936–944. [Google Scholar] [CrossRef]
- Acosta, A.; Streett, S.; Kroh, M.D.; Cheskin, L.J.; Saunders, K.H.; Kurian, M.; Schofield, M.; Barlow, S.E.; Aronne, L. White Paper, AGA: POWER-Practice Guide on Obesity and Weight Management, Education, and Resources. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2017, 15, 631–649.e10. [Google Scholar] [CrossRef]
- Drucker, D.J. Mechanisms of Action and Therapeutic Application of Glucagon-like Peptide-1. Cell Metab. 2018, 27, 740–756. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.; Arora, S. Orlistat in polycystic ovarian syndrome reduces weight with improvement in lipid profile and pregnancy rates. J. Hum. Reprod. Sci. 2014, 7, 255–261. [Google Scholar] [CrossRef]
- Elkind-Hirsch, K.E.; Chappell, N.; Seidemann, E.; Storment, J.; Bellanger, D. Exenatide, Dapagliflozin, or Phentermine/Topiramate Differentially Affect Metabolic Profiles in Polycystic Ovary Syndrome. J. Clin. Endocrinol. Metab. 2021, 106, 3019–3033. [Google Scholar] [CrossRef] [PubMed]
- Shah, K.; Kulkarni, R.; Singh, R.; Pannu, H.S.; Kamrai, D. Role of Bupropion and Naltrexone in Managing Depression With Polycystic Ovary Syndrome: A Case Report and Literature Review. Cureus 2020, 12, e11343. [Google Scholar] [CrossRef]
- Ten Kulve, J.S.; Veltman, D.J.; Gerdes, V.E.A.; van Bloemendaal, L.; Barkhof, F.; Deacon, C.F.; Holst, J.J.; Drent, M.L.; Diamant, M.; Ijzerman, R.G. Elevated Postoperative Endogenous GLP-1 Levels Mediate Effects of Roux-en-Y Gastric Bypass on Neural Responsivity to Food Cues. Diabetes Care 2017, 40, 1522–1529. [Google Scholar] [CrossRef] [Green Version]
- van Bloemendaal, L.; IJzerman, R.G.; ten Kulve, J.S.; Barkhof, F.; Konrad, R.J.; Drent, M.L.; Veltman, D.J.; Diamant, M. GLP-1 Receptor Activation Modulates Appetite- and Reward-Related Brain Areas in Humans. Diabetes 2014, 63, 4186–4196. [Google Scholar] [CrossRef] [Green Version]
- Ten Kulve, J.S.; Veltman, D.J.; van Bloemendaal, L.; Barkhof, F.; Drent, M.L.; Diamant, M.; Ijzerman, R.G. Liraglutide Reduces CNS Activation in Response to Visual Food Cues Only After Short-term Treatment in Patients With Type 2 Diabetes. Diabetes Care 2016, 39, 214–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ten Kulve, J.S.; Veltman, D.J.; van Bloemendaal, L.; Groot, P.F.C.; Ruhé, H.G.; Barkhof, F.; Diamant, M.; Ijzerman, R.G. Endogenous GLP1 and GLP1 analogue alter CNS responses to palatable food consumption. J. Endocrinol. 2016, 229, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Bloemendaal, L.; Veltman, D.J.; ten Kulve, J.S.; Drent, M.L.; Barkhof, F.; Diamant, M.; Ijzerman, R.G. Emotional eating is associated with increased brain responses to food-cues and reduced sensitivity to GLP-1 receptor activation. Obes. Silver Spring Md. 2015, 23, 2075–2082. [Google Scholar] [CrossRef] [PubMed]
- Wharton, S.; Lau, D.C.W.; Vallis, M.; Sharma, A.M.; Biertho, L.; Campbell-Scherer, D.; Tytus, R.; Walji, S.; Walker, L.; Wicklum, S.; et al. Obesity in adults: A clinical practice guideline. CMAJ Can. Med. Assoc. J. 2020, 192, E875–E891. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Reference | Population Studied | Study Type | Eating Disorders | Prevalence in PCOS | Prevalence in Control Group | Questionnaire/ Interview | Other Remarks |
|---|---|---|---|---|---|---|---|
| [15] | 103 women with PCOS, 103 controls | Cohort Study | Binge eating disorder | 12.6% § | 1.9% | Primary Care Evaluation of Mental Disorders (PRIME-MD PHQ) and the Beck Depression Inventory | Risk of depressive disorders, in general, was significantly higher in PCOS group; 30.5% of depressed women had binge eating disorder. |
| [18] | 44 women with untreated PCOS | Cross-sectional study | Binge eating disorder | 6.8% | - | Structured Clinical Interview (SCID-I) for the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV) | A total of 50% had psychiatric disorders, 33% major depression, and 13.6% generalized anxiety disorder. |
| Bulimia nervosa | 2.3% | ||||||
| Anorexia nervosa | 0% | ||||||
| [19] | 60 women with PCOS | Prospective longitudinal study | Binge eating disorder | 25% in PCOS group with depression (n = 24) and 22% in PCOS without depression (n = 36) ƛ | - | Primary Care Evaluation of Mental Disorders Patient Health Questionnaire (PRIME-MD PHQ), Beck Depression Inventory–II (BDI), Beck Anxiety Inventory (BAI) | Overall prevalence of depression was 40%. |
| [20] | 455 women with PCOS | Cross-sectional study | Binge eating behavior | 67% | - | Bulimia Investigatory test, Edinburgh (BITE), Food Cravings Questionnaire-Trait (FCQ-T), Three-Factor Eating Questionnaire-Revised 18 (TFEQ-18) | In total, 99% of PCOS patients reported food cravings. |
| High-degree binge eating behavior | 39% | ||||||
| Eating disorder | 2% | ||||||
| [21] | 116 women with PCOS, 378 controls | Cross-sectional study | Binge eating disorder | 93.1% § | 82.5% | Arabic version of DASS-21 with 4 sections: demographics information, eating behaviors in past 2 weeks, depression subscale, health-related quality of life. | Risk of depression in PCOS was higher than in controls (p = 0.000). |
| Health-related quality of life was impaired in PCOS group. | |||||||
| [22] | 95 women with PCOS | Cross-sectional study | Bulimia nervosa | 5.3% | - | Eating Attitudes Test (EAT); Eating Behavior Severity Scale (EBSS) | |
| Subclinical anorexia nervosa | 1.1% | ||||||
| Subclinical bulimia nervosa | 10.5% | ||||||
| [10] | 148 women with PCOS, 106 controls | Cross-sectional study | All eating disorders | 28.38% ƛ | 18.87% | Eating Disorder Examination-Questionnaire (EDE-Q), Night Eating Questionnaire (NEQ), Hospital Anxiety and Depression Scale, and Health-Related Quality of Life Questionnaire (PCOSQ). | Elevated scores were noted for body shape and weight concern, anxiety, and depression in PCOS group. |
| Anorexia nervosa | 0% ƛ | 0% | |||||
| Bulimia nervosa | 6.1% ƛ | 5.66% | |||||
| Binge eating disorder | 17.6% ƛ | 10.38% | |||||
| Night eating syndrome | 12.9% ƛ | 12.38% | |||||
| [17] | 875 women with PCOS, 7592 controls | Community-based cohort study | All eating disorders | 11% § | 7.6% | Rosenberg Self-Esteem Scale, Kessler psychological distress scale. | Obesity was associated with increased odds of low self-esteem and moderate to severe psychological distress. |
| Anorexia nervosa | 3.5% ƛ | 3.4% | |||||
| Bulimia nervosa | 3.4% ƛ | 2.6% | Underweight women had increased odds of eating disorders (not specified), low self-esteem, and psychological distress. | ||||
| others | 6.4% § | 3.4% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kolnikaj, T.S.; Herman, R.; Janež, A.; Jensterle, M. Assessment of Eating Disorders and Eating Behavior to Improve Treatment Outcomes in Women with Polycystic Ovary Syndrome. Life 2022, 12, 1906. https://doi.org/10.3390/life12111906
Kolnikaj TS, Herman R, Janež A, Jensterle M. Assessment of Eating Disorders and Eating Behavior to Improve Treatment Outcomes in Women with Polycystic Ovary Syndrome. Life. 2022; 12(11):1906. https://doi.org/10.3390/life12111906
Chicago/Turabian StyleKolnikaj, Tea Shehu, Rok Herman, Andrej Janež, and Mojca Jensterle. 2022. "Assessment of Eating Disorders and Eating Behavior to Improve Treatment Outcomes in Women with Polycystic Ovary Syndrome" Life 12, no. 11: 1906. https://doi.org/10.3390/life12111906