
Can Fetuin A Be Utilized in the Evaluation of Elderly Patients with Acute Myocardial Infarction?

 ,
, 
Abstract
:1. Introduction
- (1)
- To measure FA plasma concentrations in patients with AMI after PCI and to test the correlation with other parameters (cardiovascular risk factors, NT-proBNP, troponin);
- (2)
- To test the cut-off value of FA which might predict incomplete STR in patients with STEMI.
2. Materials and Methods
2.1. Study Population
2.2. Biological Measurements
2.3. Electrocardiographic, Echocardiographic and Angiographic Data
2.4. Statistical Analysis
3. Results
3.1. Patient Characterstics
3.2. Correlation of FA with Other Parameters
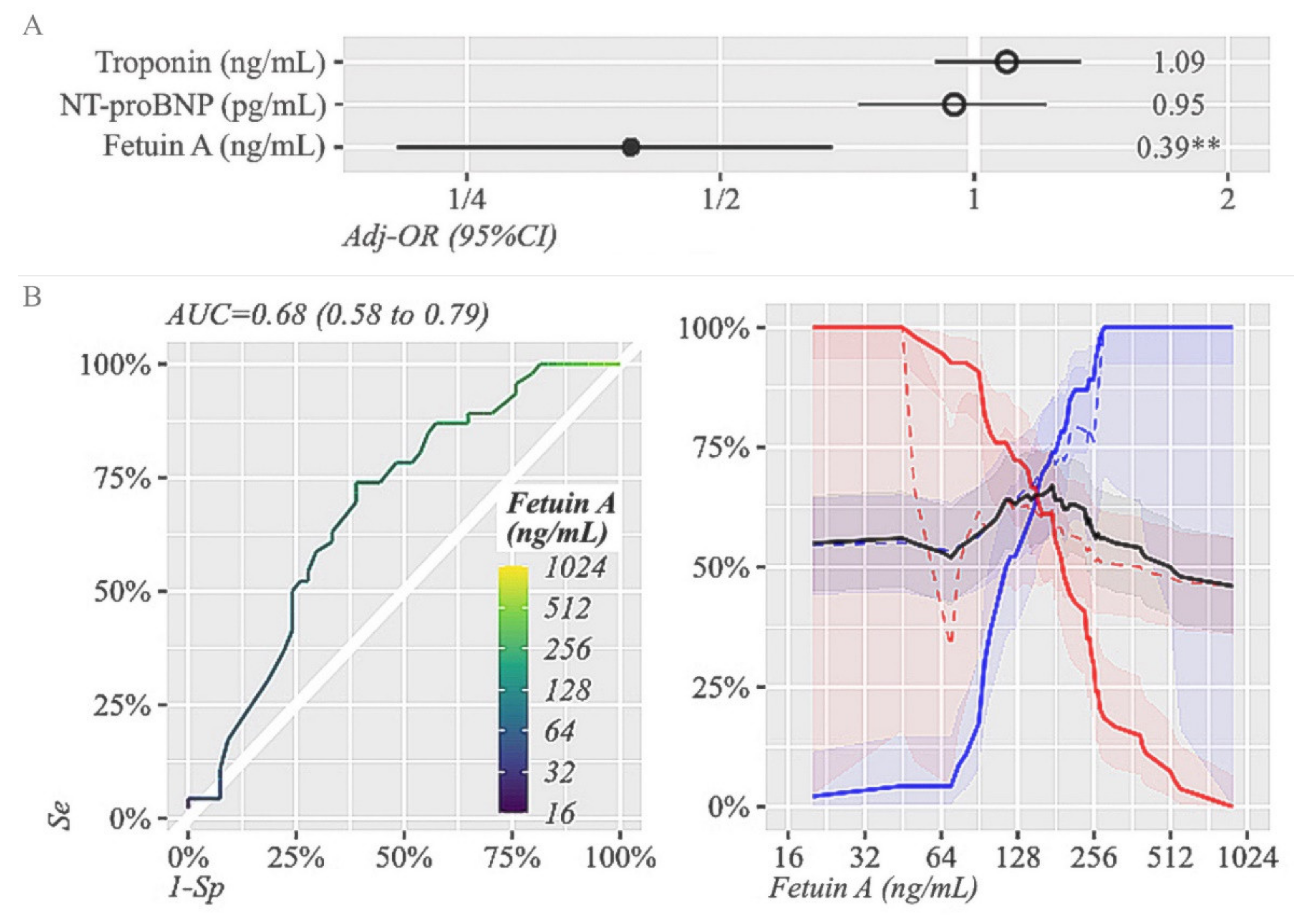
3.3. Prognostic Sensitivity and Specificity of FA with Regard to STR at 90 Min after PCI
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D.; on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction. Fourth Universal Definition of Myocardial Infarction. J. Am. Coll. Cardiol. 2018, 72, 237–269. [Google Scholar] [CrossRef]
- Anchidin, O.I.; Nemes, A.; Molnar, A.; Rosianu, A.; Rosianu, S.H.; Pop, D. Are cardiovascular rehabilitation programs implemented in young patients with acute coronary syndromes following revascularization procedures? Balneo Res. J. 2020, 1, 133–140. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; ESC Scientific Document Group; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2017, 39, 119–177,. [Google Scholar] [CrossRef] [Green Version]
- Schroder, R. Prognostic Impact of Early ST-Segment Resolution in Acute ST-Elevation Myocardial Infarction. Circulation 2004, 110, e506–e510. [Google Scholar] [CrossRef] [Green Version]
- Ombrellino, M.; Wang, H.; Yang, H.; Zhang, M.; Vishnubhakat, J.; Frazier, A.; Scher, L.A.; Friedman, S.G.; Tracey, K.J. Fetuin, a negative acute phase protein, attenuates TNF synthesis and the innate inflammatory response to carrageenan. Shock 2001, 15, 181–185. [Google Scholar] [CrossRef]
- Wang, H.; Zhang, M.; Bianchi, M.; Sherry, B.; Sama, A.; Tracey, K.J. Fetuin (alpha2-HS-glycoprotein) opsonizes cationic macrophage deactivating molecules. Proc. Natl. Acad. Sci. USA 1998, 95, 14429–14434. [Google Scholar] [CrossRef] [Green Version]
- Feistritzer, H.-J.; Klug, G.; Reinstadler, S.J.; Reindl, M.; Mayr, A.; Mair, J.; Metzler, B. Novel biomarkers predicting cardiac function after acute myocardial infarction. Br. Med. Bull. 2016, 119, 63–74. [Google Scholar] [CrossRef] [Green Version]
- Lebreton, J.P.; Joisel, F.; Raoult, J.P.; Lannuzel, B.; Rogez, J.P.; Humbert, G. Serum concentration of human alpha 2 HS glycoprotein during the inflammatory process: Evidence that alpha 2 HS glycoprotein is a negative acute-phase reactant. J. Clin. Investig. 1979, 64, 1118–1129. [Google Scholar] [CrossRef] [PubMed]
- Schafer, C.; Heiss, A.; Schwarz, A.; Westenfeld, R.; Ketteler, M.; Floege, J.; Müller-Esterl, W.; Schinke, T.; Jahnen-Dechent, W. The serum protein alpha 2-Heremans-Schmid glycoprotein/fetuin-A is a systemically acting inhibitor of ectopic calcification. J. Clin. Investig. 2003, 112, 357–366. [Google Scholar] [CrossRef] [PubMed]
- Fisher, E.; Stefan, N.; Saar, K.; Drogan, D.; Schulze, M.B.; Fritsche, A.; Joost, H.-G.; Häring, H.-U.; Hubner, N.; Boeing, H.; et al. Association of AHSG gene polymorphisms with fetuin-A plasma levels and cardiovascular diseases in the EPIC-potsdam study. Circ. Cardiovasc. Genet. 2009, 2, 607–613. [Google Scholar] [CrossRef] [Green Version]
- Ix, J.H.; Barrett-Connor, E.; Wassel, C.L.; Cummins, K.; Bergstrom, J.; Daniels, L.B.; Laughlin, G.A. The associations of fetuin-A with subclinical cardiovascular disease in community-dwelling persons: The Rancho Bernardo Study. J. Am. Coll. Cardiol. 2011, 58, 2372–2379. [Google Scholar] [CrossRef] [Green Version]
- Afsar, C.U.; Uzun, H.; Yurdakul, S.; Muderrisoglu, C.; Ergüney, M.; Demir, B.; Aslan, A.; Aral, H.; Ozyazgan, S. Association of serum fetuin-A levels with heart valve calcification and other biomarkers of inflammation among persons with acute coronary syndrome. Clin. Investig. Med. 2012, 35, E206–E215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cubedo, J.; Padro, T.; Badimon, L. Coordinated proteomic signature changes in immune response and complement proteins in acute myocardial infarction: The implication of serum amyloid P-component. Int. J. Cardiol. 2013, 168, 5196–5204. [Google Scholar] [CrossRef]
- Feistritzer, H.-J.; Klug, G.; Reinstadler, S.J.; Gröber, M.-T.; Mair, J.; Kirchmair, R.; Henninger, B.; Franz, W.-M.; Metzler, B. Fetuin-A is related to infarct size, left ventricular function and remodeling after acute STEMI. Open Heart 2015, 2, e000244. [Google Scholar] [CrossRef] [Green Version]
- Mayr, A.; Klug, G.; Schocke, M.; Trieb, T.; Mair, J.; Pedarnig, K.; Pachinger, O.; Jaschke, W.; Metzler, B. Late microvascular obstruction after acute myocardial infarction: Relation with cardiac and inflammatory markers. Int. J. Cardiol. 2012, 157, 391–396. [Google Scholar] [CrossRef]
- Chen, X.; Zhang, Y.; Chen, Q.; Li, Q.; Li, Y.; Ling, W. Lower Plasma Fetuin-A Levels Are Associated With a Higher Mortality Risk in Patients With Coronary Artery Disease. Arterioscler. Thromb. Vasc. Biol. 2017, 37, 2213–2219. [Google Scholar] [CrossRef] [Green Version]
- Ren, J.; Davidoff, A.J. Alpha2-Heremans Schmid glycoprotein, a putative inhibitor of tyrosine kinase, prevents glucose toxicity associated with cardiomyocyte dysfunction. Diabetes Metab. Res. Rev. 2002, 18, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Weikert, C.; Stefan, N.; Schulze, M.B.; Pischon, T.; Berger, K.; Joost, H.-G.; Häring, H.-U.; Boeing, H.; Fritsche, A. Plasma fetuin-A levels and the risk of myocardial infarction and ischemic stroke. Circulation 2008, 118, 2555–2562. [Google Scholar] [CrossRef] [Green Version]
- Ascer, E.; Bertolami, M.C.; Venturinelli, M.L.; Buccheri, V.; Souza, J.; Nicolau, J.; Ramires, J.A.F.; Serrano, C.V. Atorvastatin reduces proinflammatory markers in hypercholesterolemic patients. Atherosclerosis 2004, 177, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Tomoaia, R.; Beyer, R.S.; Simu, G.; Serban, A.M.; Pop, D. Understanding the role of echocardiography in remodeling after acute myocardial infarction and development of heart failure with preserved ejection fraction—New aspects of interest. Med. Ultrason 2019, 21, 69–76. [Google Scholar] [CrossRef] [Green Version]
- Aurelian, S.V.; Adrian, M.; Andercou, O.; Bruno, S.; Alexandru, O.; Catalin, T.; Dan, B. Neutrophil-to-Lymphocyte Ratio: A Comparative Study of Rupture to Nonruptured Infrarenal Abdominal Aortic Aneurysm. Ann. Vasc. Surg. 2019, 58, 270–275. [Google Scholar] [CrossRef]
- Kelly, R.A.; Smith, T.W. Cytokines and cardiac contractile function. Circulation 1997, 95, 778–781. [Google Scholar] [CrossRef] [PubMed]
- Abbate, A.; Bonanno, E.; Mauriello, A.; Bussani, R.; Biondi-Zoccai, G.G.; Liuzzo, G.; Leone, A.M.; Silvestri, F.; Dobrina, A.; Baldi, F.; et al. Widespread myocardial inflammation and infarct related artery patency. Circulation 2004, 110, 46–50. [Google Scholar] [CrossRef] [Green Version]
- Keçebaş, M.; Güllülü, S.; Sağ, S.; Beşli, F.; Açikgöz, E.; Sarandöl, E.; Aydinlar, A. Serum fetuin-A levels in patients with systolic heart failure. Acta Cardiol. 2014, 69, 399–405. [Google Scholar] [CrossRef]
- Tsutamoto, T.; Hisanaga, T.; Wada, A.; Maeda, K.; Ohnishi, M.; Fukai, D.; Mabuchi, N.; Sawaki, M.; Kinoshita, M. Interleukin-6 spillover in the peripheral circulation increases with the severity of heart failure, and the high plasma level of Interleukin-6 is an important prognostic predictor in patients with congestive heart failure. J. Am. Coll. Cardiol. 1998, 31, 391–398. [Google Scholar] [CrossRef] [Green Version]
- Rauchhaus, M.; Doehner, W.; Francis, D.P.; Davos, C.; Kemp, M.; Liebenthal, C.; Niebauer, J.; Hooper, J.; Volk, H.-D.; Coats, A.S.; et al. Plasma cytokine parameters and mortality in patients with chronic heart failure. Circulation 2000, 102, 3060–3067. [Google Scholar] [CrossRef] [Green Version]
- Lim, P.; Collet, J.-P.; Moutereau, S.; Guigui, N.; Mitchell-Heggs, L.; Loric, S.; Bernard, M.; Benhamed, S.; Montalescot, G.; Randé, J.-L.D.; et al. Fetuin-A is an independent predictor of death after ST-elevation myocardial infarction. Clin. Chem. 2007, 53, 1835–1840. [Google Scholar] [CrossRef]
- Reindl, M.; Eitel, I.; Reinstadler, S.J. Role of Cardiac Magnetic Resonance to Improve Risk Prediction following Acute ST-elevation Myocardial Infarction. J. Clin. Med. 2020, 9, 1041. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variable | Value |
|---|---|
| Age, years (mean ± SD) | 67 ± 13.1 |
| Arterial hypertension (%) | 76 |
| Smoking (%) | 39 |
| Diabetes (%) | 31 |
| Obesity (%) | 49 |
| Biological values (mean ± SD or median [IQR]) | |
| Total cholesterol, mg/dL | 183.1 ± 51.1 |
| LDL cholesterol, mg/dL | 109.5 ± 45.7 |
| HDL cholesterol, mg/dL | 42.7 ± 11.5 |
| Triglycerides, mg/dL | 155.4 ± 80.4 |
| Glucose, mg/dL | 137.1 ± 50 |
| GFR, ml/min/1.73 m2 | 58 ± 19.9 |
| ASAT, mg/dl | 36.5 (22.3–70.6) |
| ALAT, mg/dl | 24.5 (17–35.25) |
| Troponin, ng/mL | 0.24 (0.09–0.9) |
| NT-proBNP, pg/mL | 1750 (180–1638) |
| Fetuin-A, ng/mL | 155 (100–241.3) |
| Type of myocardial infarction | |
| STEMI (%) | 59 |
| NSTEMI (%) | 41 |
| Changes in ST segment elevation | |
| Maximum ST segment elevation, mm (mean ± SD) | 2.5 ± 2.5 |
| Complete STR after revascularization (%) | 52 |
| Culprit vessel | |
| LAD, (%) | 48 |
| CX, (%) | 14 |
| RCA, (%) | 35 |
| LM, (%) | 3 |
| >1 diseased vessel (n%) | 58 |
| TIMI grade flow grade < 3 after revascularization (%) | 30 |
| LVEF, % (mean ± SD) | 46 ± 10 |
| Causes of death Ventricular arrhythmias, n (%) | 9 (42.5) |
| Mechanical complications, n (%) | 2 (9.5) |
| Pump failure, n (%) | 10 (47.6) |
| Rhythm on cardiac arrest | |
| Ventricular tachycardia/ ventricular fibrillation, n (%) | 12 (57%) |
| Asistole, n (%) | 9 (43%) |
| Variable | Patients with CA (n = 21) | Survivors after AMI (n = 79) | p Value |
|---|---|---|---|
| Age, years (mean ± SD) | 72 ± 10.8 | 65.6 ± 13.4 | 0.03 * |
| Arterial hypertension (n, %) | 14 (66.6) | 62 (78.5) | 0.4 |
| Smoking (n, %) | 11 (52.4) | 28 (35.4) | 0.23 |
| Diabetes (n, %) | 4 (19) | 27 (34.2) | 0.3 |
| Obesity (n, %) | 9 (42.8) | 40 (50.6) | 0.07 |
| Biological values (mean ± SD or median (IQR)) | |||
| Total cholesterol, mg/dL | 169.2 ± 40.8 | 186.9 ± 53.2 | 0.25 |
| LDL cholesterol, mg/dL | 100.6 ± 35.4 | 111.8 ± 48 | 0.5 |
| HDL cholesterol, mg/dL | 40 ± 11.76 | 43.2 ± 11.4 | 0.12 |
| Triglycerides, mg/dL | 150.8 ± 67.6 | 156.6 ± 83.77 | 0.9 |
| Glucose, mg/dL | 160.3 ± 63 | 131 ± 33.2 | 0.01 * |
| GFR, mL/min/1.73 m2 | 55 ± 16.6 | 59.3 ± 18.8 | 0.45 |
| ASAT, mg/dL | 79 (37–130) | 28 (21–50) | 0.005 * |
| ALAT, mg/dL | 35 (18–67) | 23 (17–33.5) | <0.001 * |
| Troponin, ng/mL | 0.7 (0.15–2.1) | 0.2 (0.07–0.6) | 0.01 * |
| NT-proBNP, pg/mL | 1750 (800–3200) | 480 (155–945) | <0.001 * |
| Fetuin-A, ng/mL | 115 (95–175) | 180 (105–250) | 0.03 * |
| Electrocardiography | |||
| Type of myocardial infarction | |||
| STEMI, n (%) | 19 (90) | 50 (63) | 0.03 * |
| NSTEMI, n (%) | 2 (10) | 29 (37) | |
| Changes in ST segment elevation | |||
| Maximum ST segment elevation, mm (mean ± SD) | 2.5 ± 2.5 | 1.23 ± 1.4 | 0.04 * |
| Complete STR after revascularization (%) | 47.6 | 53 | 0.13 |
| Coronarography | |||
| Culprit vessel | |||
| LAD, n (%) | 11 (52) | 37 (47) | 0.55 |
| CX, n (%) | 1 (5) | 13 (6) | |
| RCA, n (%) | 8 (38) | 27 (34) | |
| LM, n (%) | 1 (5) | 2 (3) | |
| >1 diseased vessel (n, %) | 15 (71) | 43 (55) | 0.08 |
| TIMI grade flow grade < 3 after revascularization (n, %) | 11 (52) | 19 (24) | 0.03 * |
| LVEF, % (mean ± SD) | 40 ± 11 | 48 ± 9 | 0.006 * |
| Variable | All Patients | Patients with CA | Survivors after AMI |
|---|---|---|---|
| Age, years | −0.21 (p = 0.02) | NS | NS |
| Arterial hypertension, % | NS | NS | NS |
| Smoking, % | NS | NS | NS |
| Diabetes, % | NS | −0.51 (p = 0.02) | NS |
| BMI, kg/m2 | NS | NS | NS |
| Total cholesterol, mg/dL | NS | NS | NS |
| LDL cholesterol, mg/dL | NS | NS | NS |
| HDL cholesterol, mg/dL | NS | NS | NS |
| Triglycerides, mg/dL | 0.22 (p = 0.02) | 0.50 (p = 0.02) | NS |
| Glucose, mg/dL | 0.28 (p = 0.004) | NS | 0.40 (p < 0.01) |
| eGFR, mL/min/1.73 m2 | NS | NS | NS |
| ASAT, mg/dL | NS | NS | NS |
| ALAT, mg/dL | NS | NS | NS |
| Troponin, ng/mL | NS | NS | NS |
| NT-proBNP, pg/mL | −0.31 (p = 0.001) | −0.47 (p = 0.04) | NS |
| LVEF, % | NS | NS | NS |
| Variable | FA ≤ 175 ng/mL (n = 55) | FA > 175 ng/mL (n = 45) | p |
|---|---|---|---|
| Age, years | 68 ± 14 | 66 ± 12 | 0.40 |
| Male sex, n (%) | 33 (60%) | 24 (53%) | 0.50 |
| NT-proBNP, pg/ mL | 910 (320,2250) | 420 (130,700) | <0.001 * |
| Troponin, ng/ mL | 0.3 (0.13–1.1) | 0.22 (0.07–0.8) | 0.18 |
| LVEF, % | 44 ± 11 | 48 ± 8 | 0.07 |
| Number of diseased vessels > 1, n (%) | 36 (65) | 19 (42) | 0.02 * |
| TIMI flow grade < 3, n (%) | 20 (36%) | 10 (22%) | 0.12 |
| Number of patients with CA, n (%) | 16 (30) | 5 (11) | 0.03 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomoaia, R.; Beyer, R.Ș.; Zdrenghea, D.; Dădârlat-Pop, A.; Popescu, M.I.; Cismaru, G.; Gușetu, G.; Bodisz, G.; Chețan, M.I.; Pop, D. Can Fetuin A Be Utilized in the Evaluation of Elderly Patients with Acute Myocardial Infarction? Life 2021, 11, 968. https://doi.org/10.3390/life11090968
Tomoaia R, Beyer RȘ, Zdrenghea D, Dădârlat-Pop A, Popescu MI, Cismaru G, Gușetu G, Bodisz G, Chețan MI, Pop D. Can Fetuin A Be Utilized in the Evaluation of Elderly Patients with Acute Myocardial Infarction? Life. 2021; 11(9):968. https://doi.org/10.3390/life11090968
Chicago/Turabian StyleTomoaia, Raluca, Ruxandra Ștefana Beyer, Dumitru Zdrenghea, Alexandra Dădârlat-Pop, Mircea Ioachim Popescu, Gabriel Cismaru, Gabriel Gușetu, Gyorgy Bodisz, Maria Ioana Chețan, and Dana Pop. 2021. "Can Fetuin A Be Utilized in the Evaluation of Elderly Patients with Acute Myocardial Infarction?" Life 11, no. 9: 968. https://doi.org/10.3390/life11090968