
Complementary Feeding Indicators in Relation to Micronutrient Status of Ghanaian Children Aged 6–23 Months: Results from a National Survey

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data Collection Procedures
2.3. Infant and Young Child Feeding Indicators
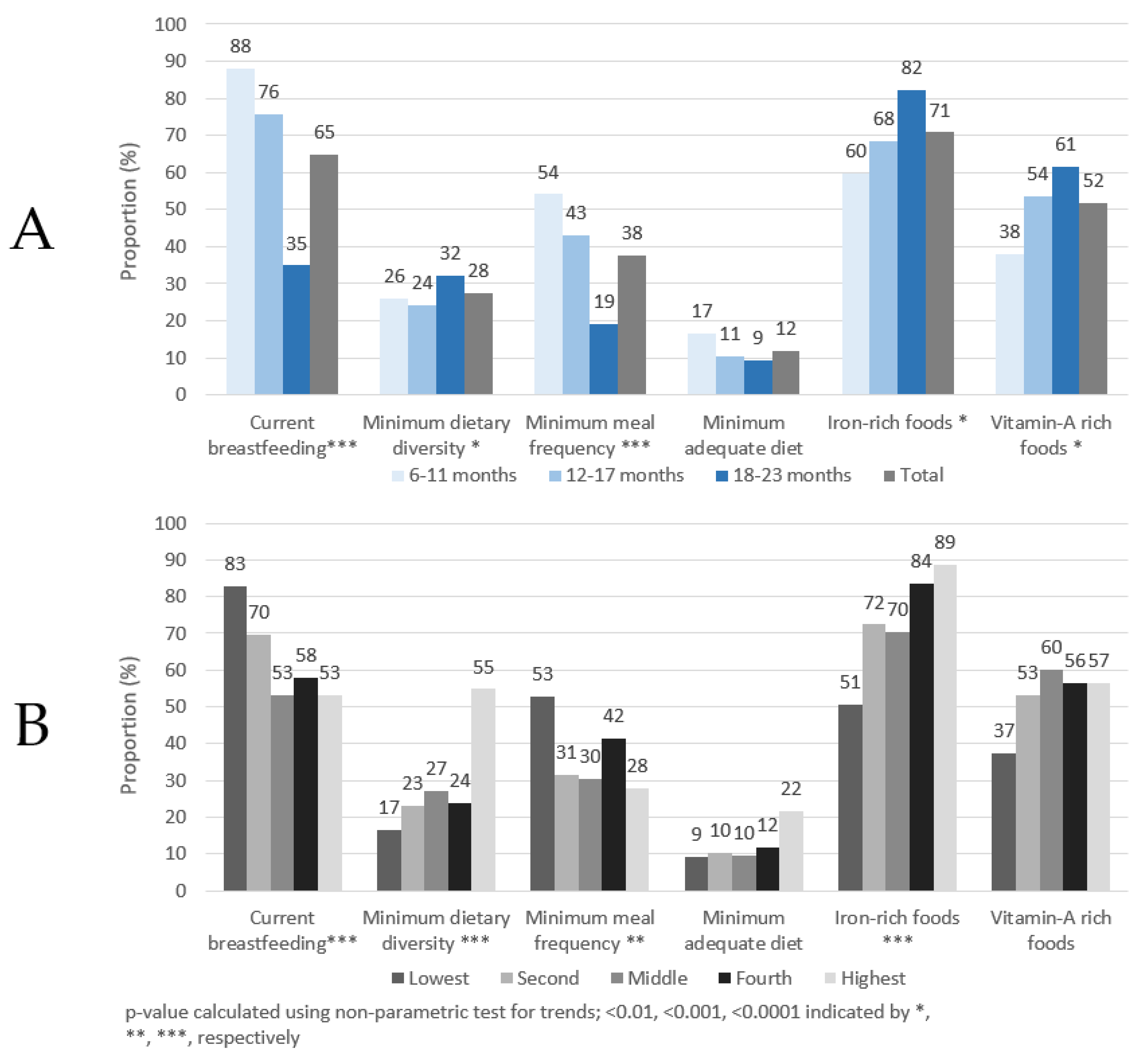
- Minimum dietary diversity (MDD): Proportion of children 6–23 months of age who receive foods from 5 or more food groups out of eight food groups in the previous 24 h.
- Minimum meal frequency (MMF): Proportion of children 6–23 months of age who receive solid, semi-solid, or soft foods (but also including milk feeds for non-breastfed children) the minimum number of times or more. The minimum number of times as defined by the WHO for breastfed children is two times for children 6–8 months of age, three times for children 9–23 months of age, and four times for all non-breastfed children 6–23 months of age [15].
- Minimum acceptable diet (MAD): Proportion of children 6–23 months of age who receive a minimum acceptable diet (apart from breast milk). This is a composite indicator and is defined as the proportion of children 6–23 months of age who achieved both minimum dietary diversity and minimum meal frequency [15].
- Consumption of iron-rich or iron-fortified foods (IRF): Proportion of children 6–23 months of age who receive an iron-rich food or iron-fortified food that is specially designed for infants and young children, or that is fortified in the home. Iron-rich foods include red meat, poultry, fish and shellfish, organ meats, iron-fortified complementary foods or biscuits, iron-fortified infant formula, and iron-fortified lipid-based nutrient supplements [15].
- Consumption of vitamin A-rich food, foods fortified with vitamin A (VARF): The proportion of children (6–23 months of age) consuming vitamin A-rich foods or foods fortified with vitamin A. Vitamin A-rich foods include sweet potatoes that are orange or yellow inside, red palm oil, and foods made with red palm oil or palm nuts (“red-red”, palm nut soup, palava sauce: white-seed melon + taro leaves stew).
2.4. Data Management and Statistical Analysis
2.5. Ethics and Consent
3. Results
3.1. Infant and Young Child Feeding Indicators and Anemia and Micronutrient Status
3.2. Determinants of Anemia and Micronutrient Status of Children Aged 6–23 Months
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alderman, H.; Headey, D. The timing of growth faltering has important implications for observational analyses of the underlying determinants of nutrition outcomes. PLoS ONE 2018, 13, e0195904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Essential Nutrition Actions: Improving Maternal, Newborn, Infant and Young Child Health and Nutrition. Interv Target Infants Young Child (6–23 Mon Age); World Health Organization: Geneva, Switzerland, 2013; Volume 2. [Google Scholar]
- WHO. Indicators for Assessing Infant and Young Child Feeding Practices PART 1; World Health Organization: Geneva, Switzerland, 2007; Volume 2007, pp. 1–19. ISBN 9789240018389. [Google Scholar]
- Lutter, C.K.; Daelmans, B.M.E.G.; De Onis, M.; Kothari, M.T.; Ruel, M.; Arimond, M.; Deitchler, M.; Dewey, K.G.; Blössner, M.; Borghi, E. Undernutrition, poor feeding practices, and low coverage of key nutrition interventions. Pediatrics 2011, 128, e1418–e1427. [Google Scholar] [CrossRef]
- Dewey, K.G. The Challenge of Meeting Nutrient Needs of Infants and Young Children during the Period of Complementary Feeding: An Evolutionary Perspective. J. Nutr. 2013, 143, 2050–2054. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akombi, B.J.; Agho, K.E.; Hall, J.J.; Merom, D.; Astell-Burt, T.; Renzaho, A.M.N. Stunting and severe stunting among children under-5 years in Nigeria: A multilevel analysis. BMC Pediatr. 2017, 17, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danaei, G.; Andrews, K.G.; Sudfeld, C.; Fink, G.; McCoy, D.C.; Peet, E.; Sania, A.; Fawzi, M.C.S.; Ezzati, M.; Fawzi, W.W. Risk Factors for Childhood Stunting in 137 Developing Countries: A Comparative Risk Assessment Analysis at Global, Regional, and Country Levels. PLoS Med. 2016, 13, e1002164. [Google Scholar] [CrossRef] [Green Version]
- Simondon, K.B.; Simondon, F.; Costes, R.; Delaunay, V.; Diallo, A. Breast-feeding is associated with improved growth in length, but not weight, in rural senegalese toddlers. Am. J. Clin. Nutr. 2001, 73, 959–967. [Google Scholar] [CrossRef] [Green Version]
- Arimond, M.; Ruel, M.T. Dietary diversity is associated with child nutritional status: Evidence from 11 demographic and health surveys. J. Nutr. 2004, 134, 2579–2585. [Google Scholar] [CrossRef] [Green Version]
- Moursi, M.M.; Arimond, M.; Dewey, K.G.; Trèche, S.; Ruel, M.T.; Delpeuch, F. Dietary diversity is a good predictor of the micronutrient density of the diet of 6- to 23-month-old children in Madagascar. J. Nutr. 2008, 138, 2448–2453. [Google Scholar] [CrossRef]
- Black, R. Micronutrient deficiency—An underlying cause of morbidity and mortality. Bull. World Health Organ. 2003, 81, 79. [Google Scholar] [CrossRef]
- World Health Organization. UNICEF, US Agency for International Development, Academy for Educational Development–Food and Nutrition Technical Assistance-2, University of California at Davis. In International Food Policy Research Institute. Indicators for Assessing Infant and Young Child Feeding Practices: Part 1: Definitions; WHO: Geneva, Switzerland, 2008. [Google Scholar]
- FANTA. Developing and Validating Simple Indicators of Dietary Quality and Energy Intake of Infants and Young Children in Developing Countries: Summary of Findings from Analysis of 10 Data Sets; FANTA: Washington, DC, USA, 2006. [Google Scholar]
- FANTA. Developing and Validating Simple Indicators of Dietary Quality of Infants and Young Children in Developing Countries: Additional Analysis of 10 Data Sets; FANTA: Washington, DC, USA, 2007. [Google Scholar]
- WHO; UNICEF. Indicators for Assessing Infant and Young Child Feeding Practices: Definitions and Measurement Methods; World Health Organization and United Nations Children’s Fund: Geneva, Switzerland, 2021. [Google Scholar]
- Heidkamp, R.A.; Ayoya, M.A.; Teta, I.N.; Stoltzfus, R.J.; Marhone, J.P. Complementary feeding practices and child growth outcomes in Haiti: An analysis of data from Demographic and Health Surveys. Matern. Child. Nutr. 2015, 11, 815–828. [Google Scholar] [CrossRef] [PubMed]
- Saaka, M.; Wemakor, A.; Abizari, A.R.; Aryee, P. How well do WHO complementary feeding indicators relate to nutritional status of children aged 6–23 months in rural Northern Ghana? BMC Public. Health 2015, 15, 1157. [Google Scholar] [CrossRef] [Green Version]
- Obbagy, J.E.; English, L.K.; Psota, T.L.; Wong, Y.P.; Butte, N.F.; Dewey, K.G.; Fox, M.K.; Greer, F.R.; Krebs, N.F.; Scanlon, K.S.; et al. Complementary feeding and micronutrient status: A systematic review. Am. J. Clin. Nutr. 2019, 109, 852S–871S. [Google Scholar] [CrossRef] [Green Version]
- Molla, A.; Egata, G.; Mesfin, F.; Arega, M.; Getacher, L. Prevalence of Anemia and Associated Factors among Infants and Young Children Aged 6–23 Months in Debre Berhan Town, North Shewa, Ethiopia. J. Nutr. Metab. 2020, 2020, 2956129. [Google Scholar] [CrossRef]
- University of Ghana; GroundWork; University of Wisconsin-Madison; KEMRI-Wellcome; UNICEF. Ghana Micronutrient Survey GMS 2017. Open Science Framework; UNICEF: Charlottesville, VA, USA, 2017. [Google Scholar] [CrossRef]
- Wegmüller, R.; Bentil, H.; Wirth, J.P.; Petry, N.; Tanumihardjo, S.A.; Allen, L.; Williams, T.N.; Selenje, L.; Mahama, A.; Amoaful, E.; et al. Anemia, micronutrient deficiencies, malaria, hemoglobinopathies and malnutrition in young children and non-pregnant women in Ghana: Findings from a national survey. PLoS ONE 2020, 15, e0228258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, C.K.; Gasser, R.A., Jr.; Magill, A.J.; Miller, R.S. Update on rapid diagnostic testing for malaria. Clin. Microbiol. Rev. 2008, 21, 97–110. [Google Scholar] [CrossRef] [Green Version]
- Erhardt, J.G.; Estes, J.E.; Pfeiffer, C.M.; Biesalski, H.K.; Craft, N.E. Combined measurement of ferritin, soluble transferrin receptor, retinol binding protein, and C-reactive protein by an inexpensive, sensitive, and simple sandwich enzyme-linked immunosorbent assay technique. J. Nutr. 2004, 134, 3127–3132. [Google Scholar] [CrossRef] [Green Version]
- Atkinson, S.H.; Rockett, K.; Sirugo, G.; Bejon, P.A.; Fulford, A.; O’Connell, M.A.; Bailey, R.; Kwiatkowski, D.; Prentice, A.M. Seasonal childhood anaemia in West Africa is associated with the haptoglobin 2-2 genotype. PLoS Med. 2006, 3, 652–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chong, S.S.; Boehm, C.D.; Higgs, D.R.; Cutting, G.R. Single-tube multiplex-PCR screen for common deletional determinants of alpha-thalassemia. Blood 2000, 95, 360–362. [Google Scholar] [CrossRef]
- Waterfall, C.M.; Cobb, B.D. Single tube genotyping of sickle cell anaemia using PCR-based SNP analysis. Nucleic. Acids Res. 2001, 29, E119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filmer, D.; Pritchett, L.H. Estimating Wealth Effects Without Expenditure Data—Or Tears: An Application To Educational Enrollments In States Of India. Demography 2001, 38, 115–132. [Google Scholar] [PubMed] [Green Version]
- Namaste, S.M.; Rohner, F.; Huang, J.; Bhushan, N.L.; Flores-Ayala, R.; Kupka, R.; Mei, Z.; Rawat, R.; Williams, A.M.; Raiten, D.J.; et al. Adjusting ferritin concentrations for inflammation: Biomarkers Reflecting Inflammation and Determinants of Anemia (BRINDA) project. Am. J. Clin. Nutr. 2017, 106, 359S–371S. [Google Scholar] [CrossRef]
- Larson, L.M.; Namaste, S.M.; Williams, A.M.; Engle-Stone, R.; Addo, O.Y.; Suchdev, P.S.; Wirth, J.P.; Temple, V.; Serdula, M. Adjusting retinol-binding protein concentrations for inflammation: Biomarkers Reflecting Inflammation and Nutritional Determinants of Anemia (BRINDA) project. Am. J. Clin. Nutr. 2017, 106, 390S–401S. [Google Scholar] [CrossRef] [PubMed]
- Tanumihardjo, S.A.; Russell, R.M.; Stephensen, C.B.; Gannon, B.M.; Craft, N.E.; Haskell, M.J.; Lietz, G.; Schulze, K.; Raiten, D.J. Biomarkers of Nutrition for Development (BOND)—Vitamin A Review. J. Nutr. 2016, 146, 1816S–1848S. [Google Scholar] [CrossRef] [Green Version]
- Cuzick, J. A Wilcoxon-type test for trend. Stat. Med. 1985, 4, 87–90. [Google Scholar] [CrossRef] [PubMed]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis Seventh Edition. Pearson New International; Pearson Education Limited Harlow: Hoboken, HJ, USA, 2014. [Google Scholar] [CrossRef]
- Clark, K.M.; Li, M.; Zhu, B.; Liang, F.; Shao, J.; Zhang, Y.; Ji, C.; Zhao, Z.; Kaciroti, N.; Lozoff, B. Breastfeeding, mixed, or formula feeding at 9 months of age and the prevalence of iron deficiency and iron deficiency anemia in two cohorts of infants in China. J. Pediatr. 2017, 181, 56–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simondon, K.B.; Costes, R.; Delaunay, V.; Diallo, A.; Simondon, F. Children’s height, health and appetite influence mothers’ weaning decisions in rural Senegal. Int. J. Epidemiol. 2001, 30, 476–481. [Google Scholar] [CrossRef] [PubMed]
- Stadlmayr, B.; Charrondiere, U.R.; Enujiugha, V.N.; Bayili, R.G.; Fagbohoun, E.G.; Samb, B.; Addy, P.; Barikmo, I.; Ouattara, F.; Oshaug, A.; et al. West African Food Composition Table; West African Health Organization: Rome, Iatly, 2012. [Google Scholar]
- WHO; FAO. Guidelines on Food Fortification with Micronutrients; Allen, L., Benoist, B., de Dary, O., Hurrell, R., Eds.; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Kuypers, F.A. Red cell membrane lipids in hemoglobinopathies. Curr. Mol. Med. 2008, 8, 633–638. [Google Scholar] [CrossRef]
- FAO. Food Balance Sheets; FAOSTAT: Rome, Italy, 2021. [Google Scholar]
- Petry, N.; Egli, I.; Gahutu, J.B.; Tugirimana, P.L.; Boy, E.; Hurrell, R. Stable iron isotope studies in Rwandese women indicate that the common bean has limited potential as a vehicle for iron biofortification. J. Nutr. 2012, 142, 492–497. [Google Scholar] [CrossRef] [Green Version]
- Petry, N.; Boy, E.; Wirth, J.P.; Hurrell, R.F. Review: The potential of the common bean (phaseolus vulgaris) as a vehicle for iron biofortification. Nutrients 2015, 7, 1144–1173. [Google Scholar] [CrossRef] [Green Version]
- Petry, N.; Egli, I.; Gahutu, J.B.; Tugirimana, P.L.; Boy, E.; Hurrell, R. Phytic Acid Concentration Influences Iron Bioavailability from Biofortified Beans in Rwandese Women with Low Iron Status. J. Nutr. 2014, 144, 1681–1687. [Google Scholar] [CrossRef] [Green Version]
- Xu, B.J.; Yuan, S.H.; Chang, S.K.C. Comparative analyses of phenolic composition, antioxidant capacity, and color of cool season legumes and other selected food legumes. J. Food Sci. 2007, 72, S167–S177. [Google Scholar] [CrossRef] [PubMed]
- ElMaki, H.B.; AbdelRahaman, S.M.; Idris, W.H.; Hassan, A.B.; Babiker, E.E.; Tinay, A.H.E. Content of antinutritional factors and HCl-extractability of minerals from white bean (Phaseolus vulgaris) cultivars: Influence of soaking and/or cooking. Food Chem. 2007, 100, 362–368. [Google Scholar] [CrossRef]
- Nergiz, C.; Gökgöz, E. Effects of traditional cooking methods on some antinutrients and in vitro protein digestibility of dry bean varieties (Phaseolus vulgaris L.) grown in Turkey. Int. J. Food Sci Technol. 2007, 42, 868–873. [Google Scholar] [CrossRef]
- Ramírez-Cárdenas, L.; Leonel, A.J.; Costa, N.M.B. Efeito do processamento doméstico sobre o teor de nutrientes e de fatores antinutricionais de diferentes cultivares de feijão comum. Cienc. E Tecnol. Aliment. 2008, 28, 200–213. [Google Scholar] [CrossRef] [Green Version]
- Luthria, D.L.; Pastor-Corrales, M.A. Phenolic acids content of fifteen dry edible bean (Phaseolus vulgaris L.) varieties. J. Food Compos. Anal. 2006, 19, 205–211. [Google Scholar] [CrossRef]
- Akhwale, W.S.; Lum, J.; Kaneko, A.; Eto, H.; Obonyo, C.; Björkman, A.; Kobayakawa, T. Anemia and malaria at different altitudes in the western highlands of Kenya. Acta Trop. 2004, 91, 167–175. [Google Scholar] [CrossRef]
- Ehrhardt, S.; Burchard, G.D.; Mantel, C.; Cramer, J.P.; Kaiser, S.; Kubo, M.; Otchwemah, R.N.; Bienzle, U.; Mockenhaupt, F. Malaria, anemia, and malnutrition in African children—Defining intervention priorities. J. Infect. Dis. 2006, 194, 108–114. [Google Scholar] [CrossRef] [Green Version]
- Korenromp, E.L.; Armstrong-Schellenberg, J.R.M.; Williams, B.G.; Nahlen, B.L.; Snow, R.W. Impact of malaria control on childhood anaemia in Africa—A quantitative review. Trop. Med. Int. Health 2004, 9, 1050–1065. [Google Scholar] [CrossRef]
- Glinz, D.; Hurrell, R.F.; Righetti, A.A.; Zeder, C.; Adiossan, L.G.; Tjalsma, H.; Utzinger, J.; Zimmermann, M.B.; N’Goran, E.K.; Wegmüller, R. In Ivorian school-age children, infection with hookworm does not reduce dietary iron absorption or systemic iron utilization, whereas afebrile Plasmodium falciparum infection reduces iron absorption by half. Am. J. Clin. Nutr. 2015, 101, 462–470. [Google Scholar] [CrossRef] [Green Version]
- Wirth, J.P.; Rohner, F.; Woodruff, B.A.; Chiwile, F.; Yankson, H.; Koroma, A.S.; Russel, F.; Sesay, F.; Dominguez, E.; Petry, N.; et al. Anemia, Micronutrient Deficiencies, and Malaria in Children and Women in Sierra Leone Prior to the Ebola Outbreak—Findings of a Cross-Sectional Study. PLOS ONE 2016, 11, e0155031. [Google Scholar] [CrossRef] [Green Version]
- Prentice, A.M. Iron metabolism, malaria, and other infections: What is all the fuss about? J. Nutr. 2008, 138, 2537–2541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muriuki, J.M.; Mentzer, A.J.; Mitchell, R.; Webb, E.L.; Etyang, A.O.; Kyobutungi, C.; Morovat, A.; Kimita, W.; Ndungu, F.M.; Macharia, A.W.; et al. Malaria is a cause of iron deficiency in African children. Nat. Med. 2021, 27, 653–658. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | n | % | (95% CI) |
|---|---|---|---|
| Age group (in months) | |||
| 6–11 months | 127 | 29.7 | (24.4, 35.5) |
| 12–17 months | 145 | 34.7 | (29.4, 40.5) |
| 18–23 months | 147 | 35.6 | (30.1, 41.5) |
| Sex | |||
| Male | 211 | 50.6 | (45.2, 56.1) |
| Female | 208 | 49.4 | (43.9, 54.8) |
| Residence | |||
| Urban | 163 | 45.8 | (32.9, 59.3) |
| Rural | 256 | 54.2 | (40.7, 67.1) |
| Stratum/belt | |||
| Southern | 111 | 31.3 | (24.2, 39.4) |
| Middle | 178 | 47.5 | (39.8, 55.4) |
| Northern | 130 | 21.1 | (15.8, 27.7) |
| Wealth quintile | |||
| Lowest | 144 | 26.2 | (18.5, 35.8) |
| Second | 88 | 19.3 | (13.7, 26.5) |
| Middle | 69 | 22.4 | (15.3, 31.5) |
| Fourth | 61 | 16.3 | (11.5, 22.7) |
| Highest | 57 | 15.8 | (9.6, 24.8) |
| Food Groups | 6–11 Months | 12–17 Months | 18–23 Months | Total (6–23 Months) | p-Value c | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| % a | 95% CI b | % a | 95% CI b | % a | 95% CI b | % a | 95% CI b | |||
| 1 | Breast milk | 88.0 | (77.5, 93.9) | 75.7 | (65.6, 83.5) | 34.9 | (27.7, 43.0) | 64.8 | (57.8, 71.2) | <0.001 |
| 2 | Grains, roots and tubers | 85.5 | (77.8, 90.8) | 90.7 | (83.9, 94.9) | 94.4 | (88.6, 97.4) | 90.5 | (87, 93.1) | 0.07 |
| Thin porridge (e.g., koko) | 67.4 | (57.3, 76.1) | 61.0 | (51.2, 69.9) | 65.4 | (55.7, 73.9) | 64.4 | (58.5, 69.9) | 0.60 | |
| Foods made from grains | 74.9 | (64.6, 83) | 86.4 | (79.5, 91.2) | 91.1 | (84.9, 94.9) | 84.7 | (80.7, 88) | 0.011 | |
| White roots and tubers and plantains | 16.8 | (11, 24.7) | 26.6 | (19.1, 35.6) | 31.4 | (24, 39.9) | 25.4 | (21.3, 30.1) | 0.13 | |
| 3 | Legumes and nuts | 10.2 | (5.5, 18.1) | 13.9 | (8.3, 22.4) | 26.6 | (18.0, 37.4) | 17.3 | (13.1, 22.7) | 0.01 |
| 4 | Dairy products (milk, yogurt, cheese) | 37.9 | (28.3, 48.6) | 35.7 | (24.0, 49.4) | 46.9 | (35.3, 58.9) | 40.4 | (32.8, 48.5) | 0.30 |
| Infant formula or sweetened/flavored milk in tins or sachets (liquids module) | 15.5 | (9.2, 25) | 6.8 | (3.3, 13.3) | 4.4 | (1.8, 10.4) | 8.5 | (5.9, 12.2) | 0.017 | |
| Milk (tinned, powdered, or fresh animal milk) or Yogurt (liquids) | 10.4 | (5.9, 17.5) | 20.7 | (12.3, 32.8) | 24.9 | (17.1, 34.8) | 19.2 | (14.6, 24.7) | 0.08 | |
| Milk and milk products (food module) | 29.7 | (20.3, 41.3) | 28.3 | (18.3, 41.1) | 36.7 | (26.2, 48.6) | 31.7 | (24.9, 39.5) | 0.55 | |
| 5 | Flesh foods (meat, fish, poultry and liver/organ meats) | 41.8 | (30.7, 53.7) | 65.0 | (56.1, 73) | 76.8 | (68.0, 83.8) | 62.4 | (56.2, 68.2) | <0.001 |
| Organ meats | 0.2 | (0, 1.3) | 2.6 | (0.7, 8.8) | 5.0 | (2.3, 10.4) | 2.7 | (1.4, 5.3) | 0.28 | |
| Meat and poultry | 1.8 | (0.4, 8.3) | 10.2 | (5.7, 17.3) | 22.6 | (15.9, 31.1) | 12.1 | (9.1, 16) | <0.001 | |
| Fish and seafood | 40.4 | (29.7, 52.1) | 62.4 | (52.8, 71.1) | 67.9 | (59.3, 75.5) | 57.9 | (52.1, 63.4) | <0.001 | |
| 6 | Eggs | 11.9 | (6.6, 20.4) | 14.8 | (8.9, 23.7) | 25.4 | (18.6, 33.7) | 17.7 | (13.5, 23) | 0.02 |
| 7 | Vitamin A rich fruits and vegetables | 37.9 | (28.5, 48.4) | 53.6 | (43.2, 63.7) | 61.4 | (52.5, 69.5) | 51.8 | (45.5, 57.9) | 0.002 |
| Vitamin A-rich vegetables, roots and tubers | 1.8 | (0.5, 6.4) | 11.8 | (7.5, 18.2) | 3.4 | (1.3, 8.5) | 5.8 | (3.8, 8.9) | 0.011 | |
| Dark green leafy vegetables | 22.8 | (14.4, 34.1) | 31.1 | (22.8, 40.9) | 37.5 | (29.1, 46.7) | 31.0 | (24.9, 37.7) | 0.41 | |
| Vitamin A-rich fruits | 6.6 | (3.1, 13.6) | 11.3 | (6.2, 19.6) | 24.1 | (16.9, 33.1) | 14.5 | (10.4, 19.8) | 0.032 | |
| 8 | Other fruits and vegetables | 18.1 | (12.5, 25.6) | 16.1 | (10.9, 23) | 27.0 | (19.2, 36.5) | 20.6 | (16.7, 25.2) | 0.08 |
| 9 | Red palm oil | 24.1 | (16.5, 33.9) | 27.7 | (18, 40.1) | 28.6 | (21.1, 37.5) | 27.0 | (21.7, 33) | 0.91 |
| Mean dietary diversity score | 2.3 | (2.0, 2.7) | 2.8 | (2.6, 3.1) | 3.5 | (3.2, 3.8) | 2.9 | (2.7, 3.1) | <0.001 | |
| Proportion of children with minimum dietary diversity | 25.9 | (16.4, 38.5) | 24.2 | (16.4, 34.2) | 32.2 | (23.7, 42.2) | 27.6 | (22.2, 33.7) | 0.46 | |
| % Anemia (n = 398) a,c | p-Value b | Mean Hb (g/L) a | p-Value b | % Iron Def. (n = 398) a,c | p-Value b | Mean Ferritin (ug/L) a | p-Value b | % IDA a,c | p-Value b | % Vit A Def. (n = 398) a,c | p-Value b | Mean RBP (µmol/L) a | p-Value b | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Minimum Dietary Diversity | ||||||||||||||
| Yes | 34.7 | 0.027 | 111.8 | 0.025 | 44.5 | 0.89 | 18.0 | 0.62 | 19.3 | 0.12 | 8.1 | 0.49 | 1.09 | 0.22 |
| No | 49.1 | 108.0 | 45.2 | 19.1 | 28.3 | 11.2 | 1.05 | |||||||
| Minimum Meal Frequency | ||||||||||||||
| Yes | 48.2 | 0.47 | 108.5 | 0.63 | 54.8 | 0.013 | 17.3 | 0.23 | 37.5 | 0.002 | 9.3 | 0.64 | 1.05 | 0.72 |
| No | 43.7 | 109.5 | 39.5 | 19.8 | 20.3 | 11.0 | 1.07 | |||||||
| Minimum Acceptable Diet | ||||||||||||||
| Yes | 43.3 | 0.82 | 109.0 | 0.77 | 67.0 | 0.023 | 13.9 | 0.017 | 33.4 | 0.36 | 12.5 | 0.82 | 1.03 | 0.53 |
| No | 45.6 | 109.8 | 42.4 | 19.5 | 25.1 | 10.1 | 1.06 | |||||||
| Consumption of iron rich food, foods fortified with iron | ||||||||||||||
| Yes | 38.3 | <0.001 | 112.0 | <0.001 | 46.1 | 0.45 | 19.9 | 0.63 | 24.9 | 0.41 | 9.4 | 0.38 | 1.09 | 0.015 |
| No | 61.5 | 104.5 | 41.9 | 18.9 | 30.0 | 12.6 | 0.99 | |||||||
| Consumption of vitamin-A rich food, foods fortified with vitamin A | ||||||||||||||
| Yes | 40.0 | 0.07 | 109.4 | 0.61 | 44.9 | 0.99 | 18.2 | 0.54 | 22.2 | 0.24 | 12.0 | 0.96 | 1.06 | 0.86 |
| No | 50.7 | 108.5 | 44.9 | 19.5 | 30.9 | 8.7 | 1.07 | |||||||
| TOTAL | 45.7 | - | 108.8 | - | 45.1 | - | 18.7 | - | 26.7 | 10.3 | - | 1.06 | - | |
| Food Groups | Anemia | ID | IDA | VAD | |
|---|---|---|---|---|---|
| 1 | Breastmilk | O | ↑ | ↑ | O |
| 2 | Grains, roots and tubers | ↓ | O | ↓ | O |
| Thin porridge (e.g., koko) | ↓ | O | O | O | |
| Foods made from grains | ↓ | O | ↓ | O | |
| White roots and tubers and plantains | O | O | O | O | |
| 3 | Legumes and/or nuts | O | ↑ | ↑ | O |
| 4 | Dairy products (milk, yogurt, cheese) | ↓ | O | ↓ | O |
| Infant formula and/or sweetened/flavored milk products in tins or sachets (liquids module) | O | O | ↓ | O | |
| Milk (tinned, powdered, or fresh animal milk) or Yogurt (liquids module) | O | O | ↓ | O | |
| Milk and milk products (food module) | ↓ | O | O | O | |
| 5 | Flesh foods (meat, fish, poultry and liver/organ meats) | ↓ | ↑ | O | O |
| Organ meats | O | O | O | O | |
| Meat and poultry | O | O | O | O | |
| Fish and seafood | ↓ | O | O | O | |
| 6 | Eggs | ↓ | O | O | O |
| 7 | Vitamin A rich fruits and vegetables | O | O | O | O |
| Vitamin A-rich vegetables, roots and tubers | O | O | O | O | |
| Dark green leafy vegetables | O | O | O | O | |
| Vitamin A-rich fruits | O | O | O | O | |
| 8 | Other fruits and vegetables | O | O | O | O |
| 9 | Red palm oil | O | O | O | ↑ |
| Model | Characteristic | Category | Adjusted Relative Risk a | 95% CI |
|---|---|---|---|---|
| Anemia model (n = 372)b | Consumed iron-rich foods in past 24 h | Yes | 0.61 | (0.50, 0.75) |
| No | referent | - | ||
| Consumed eggs in past 24 h | Yes | 0.54 | (0.37, 0.80) | |
| No | referent | - | ||
| Iron status b | Sufficient | 0.52 | (0.42, 0.65) | |
| Deficient | referent | - | ||
| Malaria status c | Positive | 1.74 | (1.36, 2.21) | |
| Negative | referent | - | ||
| Iron deficiency model (n = 362)b | Currently breastfeeding | Yes | 1.58 | (1.21, 2.05) |
| No | referent | - | ||
| Consumed legumes and/or nuts in past 24 h | Yes | 1.26 | (1.03, 1.56) | |
| No | referent | |||
| Malaria status c | Positive | 0.26 | (0.14, 0.50) | |
| Negative | referent | - | ||
| Sickle cell status d | HbAS, HbSS | 0.68 | (0.47, 0.98) | |
| Normal | referent | - | ||
| Child Sex | Male | 1.27 | (1.05, 1.56) | |
| Female | referent | - | ||
| Iron deficiency anemia model (n = 362)b | Currently breastfeeding | Yes | 1.53 | (1.03, 2.31) |
| No | referent | - | ||
| Consumed grains, roots and tubers in past 24 h | Yes | 0.66 | (0.44, 0.99) | |
| No | referent | |||
| Consumed legumes and/or nuts in past 24 h | Yes | 1.43 | (1.02, 2.02) | |
| No | referent | |||
| Malaria status c | Positive | 0.38 | (0.19, 0.74) | |
| Negative | referent | - | ||
| Wealth quintile | First | referent | ||
| Second | 0.81 | (0.55, 1.20) | ||
| Middle | 0.59 | (0.36, 0.99) | ||
| Fourth | 0.63 | (0.38, 1.05) | ||
| Highest | 0.43 | (0.22, 0.82) | ||
| Vitamin A deficiency model (n = 398) | Child Sex | Male | 1.92 | (1.01, 3.65) |
| Female | referent | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Donkor, W.E.S.; Adu-Afarwuah, S.; Wegmüller, R.; Bentil, H.; Petry, N.; Rohner, F.; Wirth, J.P. Complementary Feeding Indicators in Relation to Micronutrient Status of Ghanaian Children Aged 6–23 Months: Results from a National Survey. Life 2021, 11, 969. https://doi.org/10.3390/life11090969
Donkor WES, Adu-Afarwuah S, Wegmüller R, Bentil H, Petry N, Rohner F, Wirth JP. Complementary Feeding Indicators in Relation to Micronutrient Status of Ghanaian Children Aged 6–23 Months: Results from a National Survey. Life. 2021; 11(9):969. https://doi.org/10.3390/life11090969
Chicago/Turabian StyleDonkor, William E. S., Seth Adu-Afarwuah, Rita Wegmüller, Helena Bentil, Nicolai Petry, Fabian Rohner, and James P. Wirth. 2021. "Complementary Feeding Indicators in Relation to Micronutrient Status of Ghanaian Children Aged 6–23 Months: Results from a National Survey" Life 11, no. 9: 969. https://doi.org/10.3390/life11090969