
Benefits of Binaural Integration in Cochlear Implant Patients with Single-Sided Deafness and Residual Hearing in the Implanted Ear



Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
4.1. Contribution of Preserved LF Hearing to Integration Benefit of Redundancy and Squelch
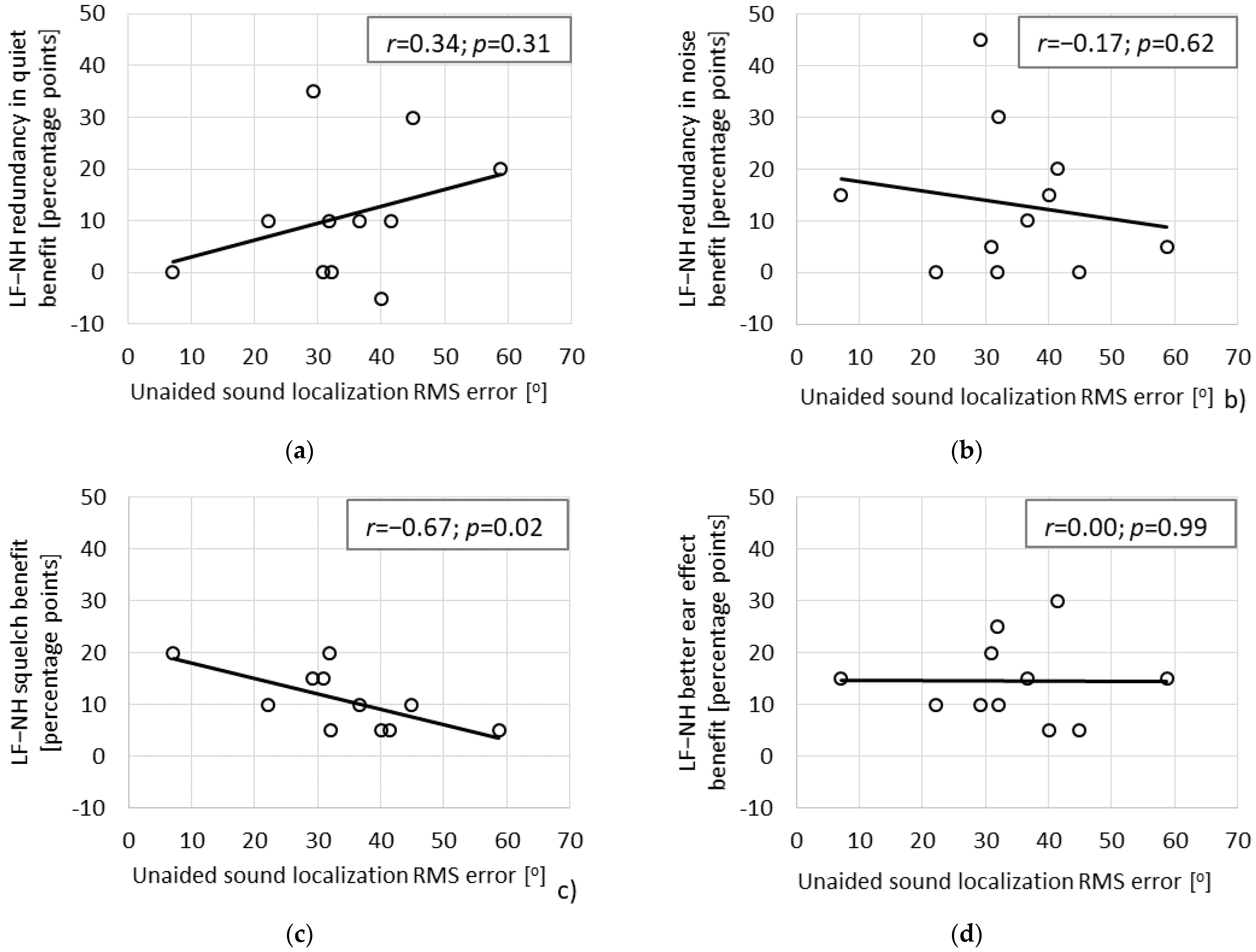
4.2. Relation between Binaural Effects and Localization Ability
4.3. Clinical Relevance
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lorens, A.; Kruszyńska, M.; Obrycka, A.; Skarzynski, P.H.; Wilson, B.; Skarzynski, H. Binaural advantages in using a cochlear implant for adults with profound unilateral hearing loss. Acta Otolaryngol. 2019, 139, 153–161. [Google Scholar] [CrossRef]
- Távora-Vieira, D.; Marino, R.; Acharya, A.; Rajan, G.P. The impact of cochlear implantation on speech understanding, subjective hearing performance, and tinnitus perception in patients with unilateral severe to profound hearing loss. Otol. Neurotol. 2015, 36, 430–436. [Google Scholar] [CrossRef]
- Skarzynski, H.; Lorens, A.; Kruszynska, M.; Obrycka, A.; Pastuszak, D.; Skarzynski, P.H. The hearing benefit of cochlear implantation for individuals with unilateral hearing loss, but no tinnitus. Acta Otolaryngol. 2017, 137, 723–729. [Google Scholar] [CrossRef]
- Mertens, G.; Punte, A.K.; De Bodt, M.; Van de Heyning, P. Binaural auditory outcomes in patients with postlingual profound unilateral hearing loss: 3 years after cochlear implantation. Audiol. Neurotol. 2015, 20, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Távora-Vieira, D.; De Ceulaer, G.; Govaerts, P.J.; Rajan, G.P. Cochlear implantation improves localization ability in patients with unilateral deafness. Ear Hear. 2015, 36, 93–98. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food and Drug Administration, Center for Devices and Radiological Health. MED-EL Cochlear Implant System PMA P000025. Available online: https://www.fda.gov/medical-devices/recently-approved-devices/med-el-cochlear-implant-system-p000025s104 (accessed on 19 July 2019).
- Lorens, A.; Polak, M.; Piotrowska, A.; Skarzynski, H. Outcomes of treatment of partial deafness with cochlear implantation: A DUET study. Laryngoscope 2008, 118, 288–294. [Google Scholar] [CrossRef] [Green Version]
- Skarzynski, P.H.; Skarzynski, H.; Dziendziel, B.; Rajchel, J.J.; Gos, E.; Lorens, A. Hearing preservation with the use of Flex20 and Flex24 electrodes in patients with partial deafness. Otol Neurotol. 2019, 40, 1153–1159. [Google Scholar] [CrossRef] [PubMed]
- Gifford, R.H.; Dorman, M.F.; Skarzynski, H.; Lorens, A.; Polak, M.; Driscoll, C.L.W.; Roland, P.; Buchman, C.A. Cochlear implantation with hearing preservation yields significant benefit for speech recognition in complex listening environments. Ear Hear. 2013, 34, 413–425. [Google Scholar] [CrossRef] [Green Version]
- Wanna, G.B.; Gifford, R.H.; McRackan, T.R.; Rivas, A.; Haynes, D.S. Bilateral cochlear implantation. Otolaryngol. Clin. N. Am. 2012, 45, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Schafer, E.C.; Amlani, A.M.; Paiva, D.; Nozari, L.; Verret, S. A meta-analysis to compare speech recognition in noise with bilateral cochlear implants and bimodal stimulation. Int. J. Audiol. 2011, 50, 871–880. [Google Scholar] [CrossRef]
- Laszig, R.; Aschendorff, A.; Stecker, M.; Müller-Deile, J.; Maune, S.; Dillier, N.; Weber, B.; Hey, M.; Begall, K.; Lenarz, T.; et al. Benefits of bilateral electrical stimulation with the Nucleus cochlear implant in adults: 6-month postoperative results. Otol. Neurotol. 2004, 25, 958–968. [Google Scholar] [CrossRef]
- Williges, B.; Dietz, M.; Hohmann, V.; Jürgens, T. Spatial release from masking in simulated cochlear implant users with and without access to low-frequency acoustic hearing. Trends Hear. 2015, 19, 1–14. [Google Scholar] [CrossRef] [Green Version]
- van Hoesel, R.; Böhm, M.; Pesch, J.; Vandali, A.; Battmer, R.D.; Lenarz, T. Binaural speech unmasking and localization in noise with bilateral cochlear implants using envelope and fine-timing based strategies. J. Acoust. Soc. Am. 2008, 123, 2249–2263. [Google Scholar] [CrossRef]
- Gifford, R.H.; Dorman, M.F.; Sheffield, S.W.; Teece, K.; Olund, A.P. Availability of binaural cues for bilateral implant recipients and bimodal listeners with and without preserved hearing in the implanted ear. Audiol. Neurootol. 2014, 19, 57–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gifford, R.H.; Stecker, G.C. Binaural cue sensitivity in cochlear implant recipients with acoustic hearing preservation. Hear. Res. 2020, 390, 107929. [Google Scholar] [CrossRef] [PubMed]
- Gifford, R.H.; Grantham, D.W.; Sheffield, S.W.; Davis, T.J.; Dwyer, R.; Dorman, M.F. Localization and inter-aural time difference (ITD) thresholds for cochlear implant recipients with preserved acoustic hearing in the implanted ear. Hear. Res. 2014, 312, 8–37. [Google Scholar] [CrossRef] [Green Version]
- Loiselle, L.H.; Dorman, M.F.; Yost, W.A.; Cook, S.J.; Gifford, R.H. Using ILD or ITD Cues for Sound Source Localization and Speech Understanding in a Complex Listening Environment by Listeners With Bilateral and With Hearing-Preservation Cochlear Implants. J. Speech Lang. Hear. Res. 2016, 59, 810–818. [Google Scholar] [CrossRef] [PubMed]
- Noble, W.; Byrne, D.; Lepage, B. Effects on sound localization of configuration and type of hearing impairment. J. Acoust. Soc. Am. 1994, 95, 992–1005. [Google Scholar] [CrossRef]
- Noble, W.; Byrne, D.; Ter-Horst, K. Auditory localization, detection of spatial separateness, and speech hearing in noise by hearing impaired listeners. J. Acoust. Soc. Am. 1997, 102, 2343–2352. [Google Scholar] [CrossRef]
- Lorenzi, C.; Gatehouse, S.; Lever, C. Sound localization in noise in hearing-impaired listeners. J. Acoust. Soc. Am. 1999, 105, 3454–3463. [Google Scholar] [CrossRef] [PubMed]
- Skarżyński, H.; Lorens, A.; Piotrowska, A.; Podskarbi-Fayette, R. Results of partial deafness cochlear implantation using various electrode designs. Audiol. Neurotol. 2009, 14, 39–45. [Google Scholar] [CrossRef]
- Galletti, F.; Freni, F.; Gazia, F.; Galletti, B. Endomeatal approach in cochlear implant surgery in a patient with small mastoid cavity and procident lateral sinus. BMJ Case Rep. 2019, 12, e229518. [Google Scholar] [CrossRef] [Green Version]
- Arndt, S.; Aschendorff, A.; Laszig, R.; Beck, R.; Schild, C.; Kroeger, S.; Ihorst, G.; Wesarg, T. Comparison of pseudobinaural hearing to real binaural hearing rehabilitation after cochlear implantation in patients with unilateral deafness and tinnitus. Otol. Neurotol. 2011, 32, 39–47. [Google Scholar] [CrossRef] [Green Version]
- Kitterick, P.T.; Smith, S.N.; Lucas, L. Hearing Instruments for Unilateral Severe-to-Profound Sensorineural Hearing Loss in Adults: A Systematic Review and Meta-Analysis. Ear Hear. 2016, 37, 495–507. [Google Scholar] [CrossRef] [Green Version]
- Bernstein, J.G.; Schuchman, G.I.; Rivera, A.L. Head Shadow and Binaural Squelch for Unilaterally Deaf Cochlear Implantees. Otol. Neurotol. 2017, 38, 195–202. [Google Scholar] [CrossRef]
- Sullivan, C.B.; Al-Qurayshi, Z.; Zhu, V.; Liu, A.; Dunn, C.; Gantz, B.J.; Hansen, M.R. Long-term audiologic outcomes after cochlear implantation for single-sided deafness. Laryngoscope 2020, 130, 1805–1811. [Google Scholar] [CrossRef] [PubMed]
- Poncet-Wallet, C.; Mamelle, E.; Godey, B.; Truy, E.; Guevara, N.; Ardoint, M.; Gnansia, D.; Hoen, M.; Saaï, S.; Mosnier, I.; et al. Prospective Multicentric Follow-up Study of Cochlear Implantation in Adults With Single-Sided Deafness: Tinnitus and Audiological Outcomes. Otol. Neurotol. 2020, 41, 458–466. [Google Scholar] [CrossRef] [PubMed]
- Nuetzel, J.M.; Hafter, E.R. Discrimination of interaural delays in complex waveforms: Spectral effects. J. Acoust. Soc. Am. 1981, 69, 1112–1118. [Google Scholar] [CrossRef]
- Francart, T.; Wouters, J. Perception of across-frequency interaural level differences. J. Acoust. Soc. Am. 2007, 122, 2826–2831. [Google Scholar] [CrossRef] [Green Version]
- Lacher-Fougère, S.; Demany, L. Consequences of cochlear damage for the detection of interaural phase differences. J. Acoust. Soc. Am. 2005, 118, 2519–2526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorenzi, C.; Gilbert, G.; Carn, C.; Garnier, S.; Moore, B.C.J. Speech perception problems of the hearing impaired reflect inability to use temporal fine structure. Proc. Natl. Acad. Sci. USA 2006, 103, 1866–18869. [Google Scholar] [CrossRef] [Green Version]
- Hopkins, K.; Moore, B.C.J. Moderate cochlear hearing loss leads to a reduced ability to use temporal fine structure information. J. Acoust. Soc. Am. 2007, 122, 1055–1068. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, K.; Moore, B.C.J.; Stone, M.A. Effects of moderate cochlear hearing loss on the ability to benefit from temporal fine structure information in speech. J. Acoust. Soc. Am. 2008, 123, 1140–1153. [Google Scholar] [CrossRef] [PubMed]
- Lorenzi, C.; Debruille, L.; Garnier, S.; Fleuriot, P.; Moore, B.C.J. Abnormal processing of temporal fine structure in speech for frequencies where absolute thresholds are normal. J. Acoust. Soc. Am. 2009, 125, 27–30. [Google Scholar] [CrossRef]
- Sheffield, S.W.; Jahn, K.; Gifford, R.H. Preserved acoustic hearing in cochlear implantation improves speech perception. J. Am. Acad. Audiol. 2015, 26, 145–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ching, T.Y.C.; van Wanrooy, E.; Hill, M.; Dillon, H. Binaural redundancy and inter-aural time difference cues for patients wearing a cochlear implant and a hearing aid in opposite ears. Int. J. Audiol. 2005, 44, 513–521. [Google Scholar] [CrossRef] [PubMed]
- Strelcyk, O.; Dau, T. Relations between frequency selectivity, temporal fine-structure processing, and speech reception in impaired hearing. J. Acoust. Soc. Am. 2009, 125, 3328–3345. [Google Scholar] [CrossRef] [Green Version]
- Hopkins, K.; Moore, B.C.J. The effects of age and cochlear hearing loss on temporal fine structure sensitivity, frequency selectivity, and speech reception in noise. J. Acoust. Soc. Am. 2011, 130, 334–349. [Google Scholar] [CrossRef]
- Finke, M.; Bönitz, H.; Lyxell, B.; Illg, A. Cochlear implant effectiveness in postlingual single-sided deaf individuals: What’s the point? Int. J. Audiol. 2017, 56, 417–423. [Google Scholar] [CrossRef]
- Leigh, J.R.; Moran, M.; Hollow, R.; Dowell, R.C. Evidence-based guidelines for recommending cochlear implantation for postlingually deafened adults. Int. J. Audiol. 2016, 55, 3–8. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| No. | Gender | Etiology | Hearing Loss Type | CI Type | Electrode Type | Processor Type | EAS System | CI Ear | Type | Post-Op PTA Non-CI Ear [dB] | Pre-Op PTA CI Ear [dB] | Post-Op PTA CI Ear [dB] | Tinnitus before CI? | Duration of Deafness [years] | Age at CI [years] | Extent of CI Use [hours/day] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | m | head trauma | sudden | Sonata | Flex 24 | Sonnet | yes | right | ssd | 9 | 80 | 111 | yes | 2 | 33 | 10 |
| 2 | m | SIHL | sudden | Sonata | Flex 20 | Sonnet | yes | left | ssd | 9 | 63 | 74 | yes | 12 | 61 | 14 |
| 3 | f | otosclerosis | progressive | Synchrony | Flex 20 | Sonnet | no | left | ssd | 20 | 80 | 103 | yes | 2 | 50 | 16 |
| 4 | m | head trauma | sudden | Sonata | Flex 24 | Sonnet | yes | right | ssd | 5 | 108 | 105 | yes | 3 | 23 | 12 |
| 5 | m | unknown | sudden | Concerto | Flex 20 | Sonnet | yes | right | ssd | 5 | 64 | 68 | yes | 13 | 35 | 16 |
| 6 | f | unknown | sudden | Sonata | Medium | Opus2 | no | left | ssd | 13 | 115 | 115 | yes | 31 | 53 | 10 |
| 7 | f | SIHL | sudden | Concerto | Flex 24 | Rondo | no | left | ssd | 11 | 96 | 116 | yes | 6 | 56 | 16 |
| 8 | m | after virus infection | sudden | Concerto | Flex 24 | Rondo | no | left | ssd | 5 | 103 | 114 | no | 7 | 18 | 12 |
| 9 | m | unknown | sudden | Sonata | Flex 24 | Sonnet | yes | right | ssd | 4 | 94 | 104 | yes | 4 | 40 | 12 |
| 10 | f | unknown | sudden | Concerto | Flex 24 | Sonnet | yes | right | ssd | 25 | 76 | 104 | yes | 3 | 52 | 16 |
| 11 | f | unknown | sudden | Sonata | Flex 28 | Sonnet | no | left | ssd | 11 | 105 | 106 | yes | 11 | 46 | 10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lorens, A.; Obrycka, A.; Skarzynski, P.H.; Skarzynski, H. Benefits of Binaural Integration in Cochlear Implant Patients with Single-Sided Deafness and Residual Hearing in the Implanted Ear. Life 2021, 11, 265. https://doi.org/10.3390/life11030265
Lorens A, Obrycka A, Skarzynski PH, Skarzynski H. Benefits of Binaural Integration in Cochlear Implant Patients with Single-Sided Deafness and Residual Hearing in the Implanted Ear. Life. 2021; 11(3):265. https://doi.org/10.3390/life11030265
Chicago/Turabian StyleLorens, Artur, Anita Obrycka, Piotr Henryk Skarzynski, and Henryk Skarzynski. 2021. "Benefits of Binaural Integration in Cochlear Implant Patients with Single-Sided Deafness and Residual Hearing in the Implanted Ear" Life 11, no. 3: 265. https://doi.org/10.3390/life11030265