
Sex Differences on Mitotane Concentration and Treatment Outcome in Patients with Adrenocortical Carcinoma

 ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Inclusion Criteria
2.2. HPLC Analysis
2.3. Statistical Analysis
3. Results
3.1. Study Population
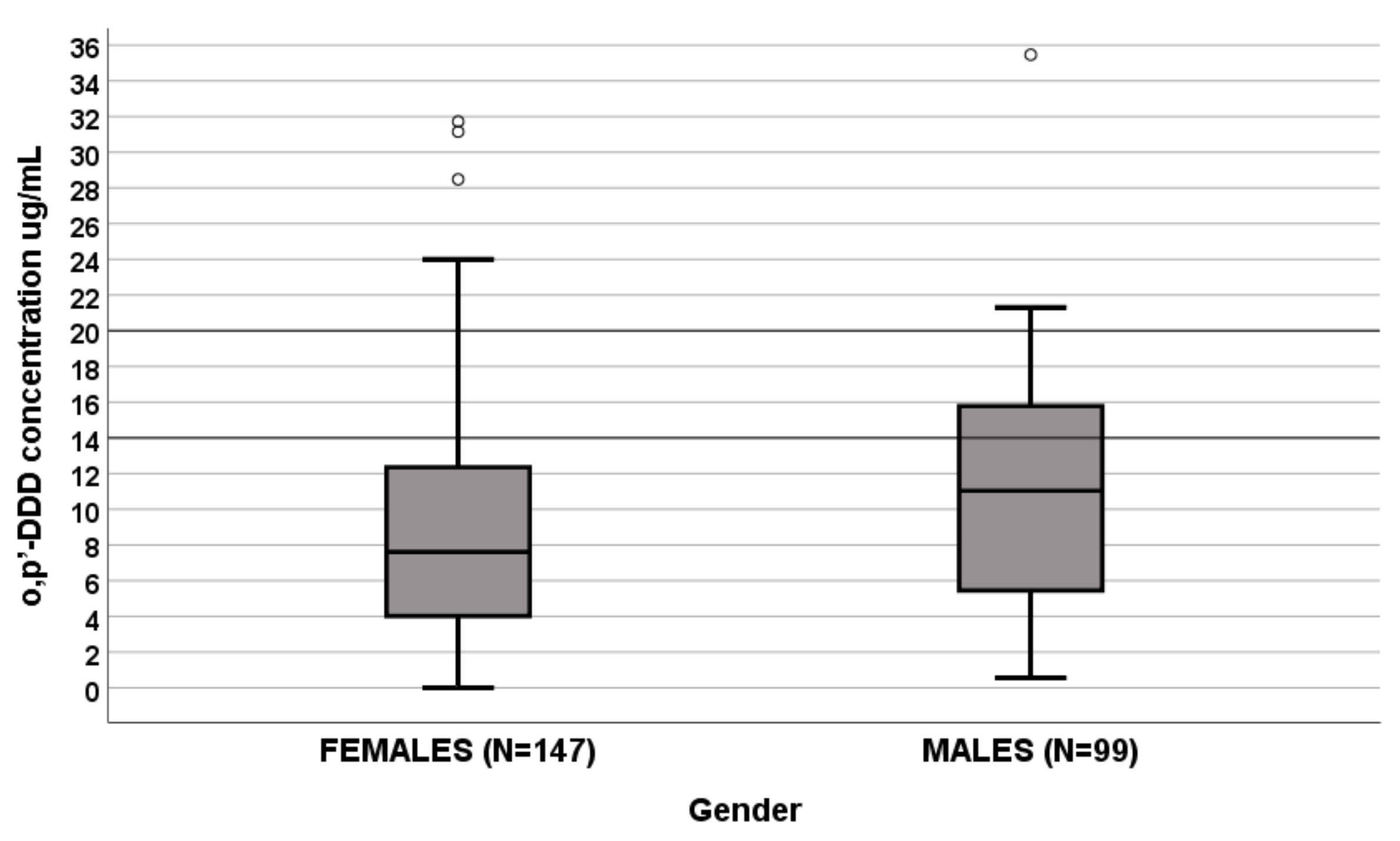
3.2. Effect of Sex on Plasma o,p′-DDD Concentrations
- Females (N = 147): median o,p′-DDD of 7.604 μg/mL (IQR 3.971–12.353 μg/mL);
- Males (N = 99): median o,p′-DDD 11.029 μg/mL (IQR 5.052–15.779 μg/mL).
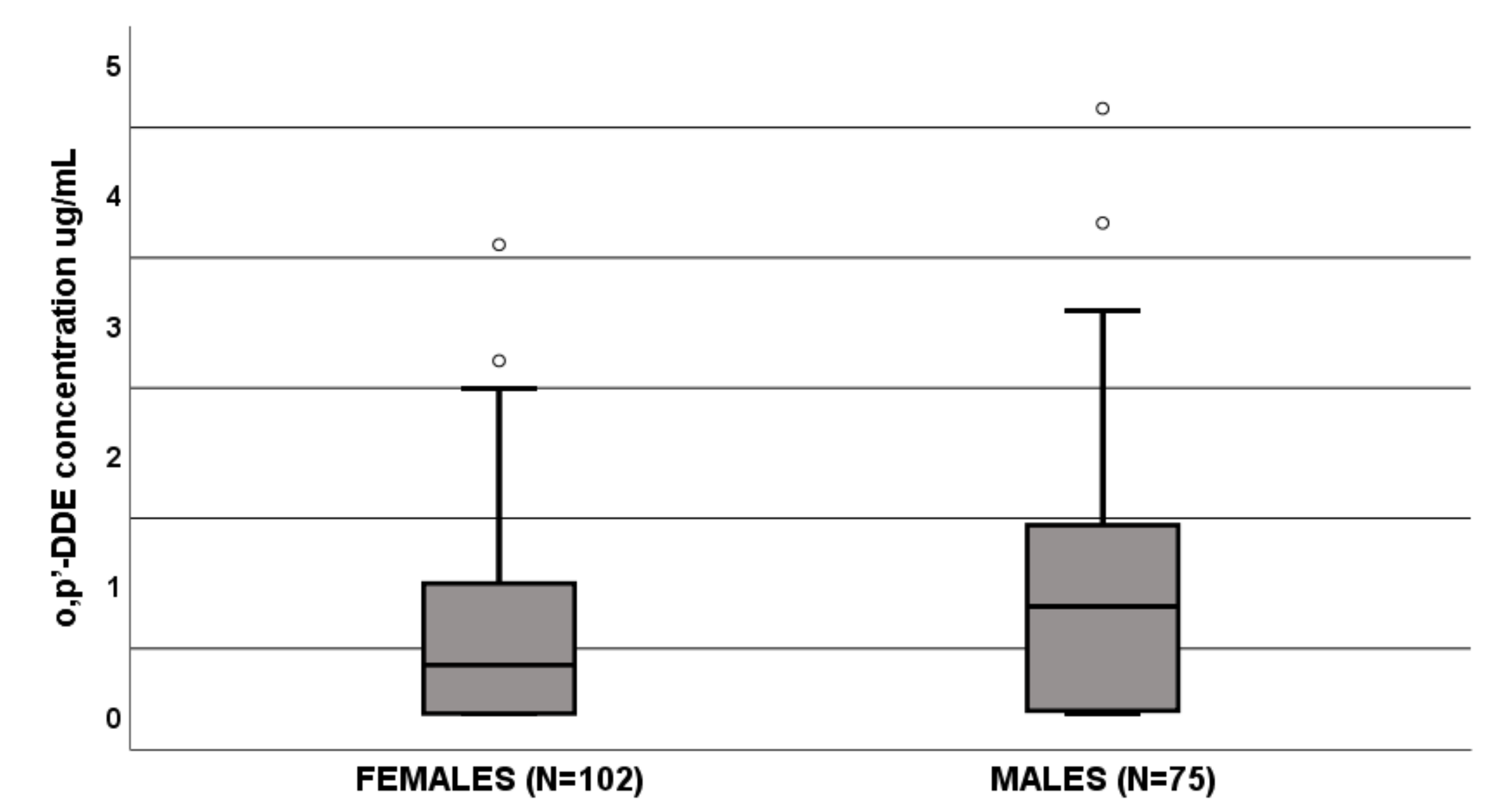
3.3. Effect of Sex on Plasma o,p′-DDE Concentrations
- Females (N = 102): median o,p′-DDE of 0.373 μg/mL (IQR 0–1 μg/mL);
- Males (N = 75): median o,p′-DDE 0.823 μg/mL (IQR 0.21–1.5 μg/mL).
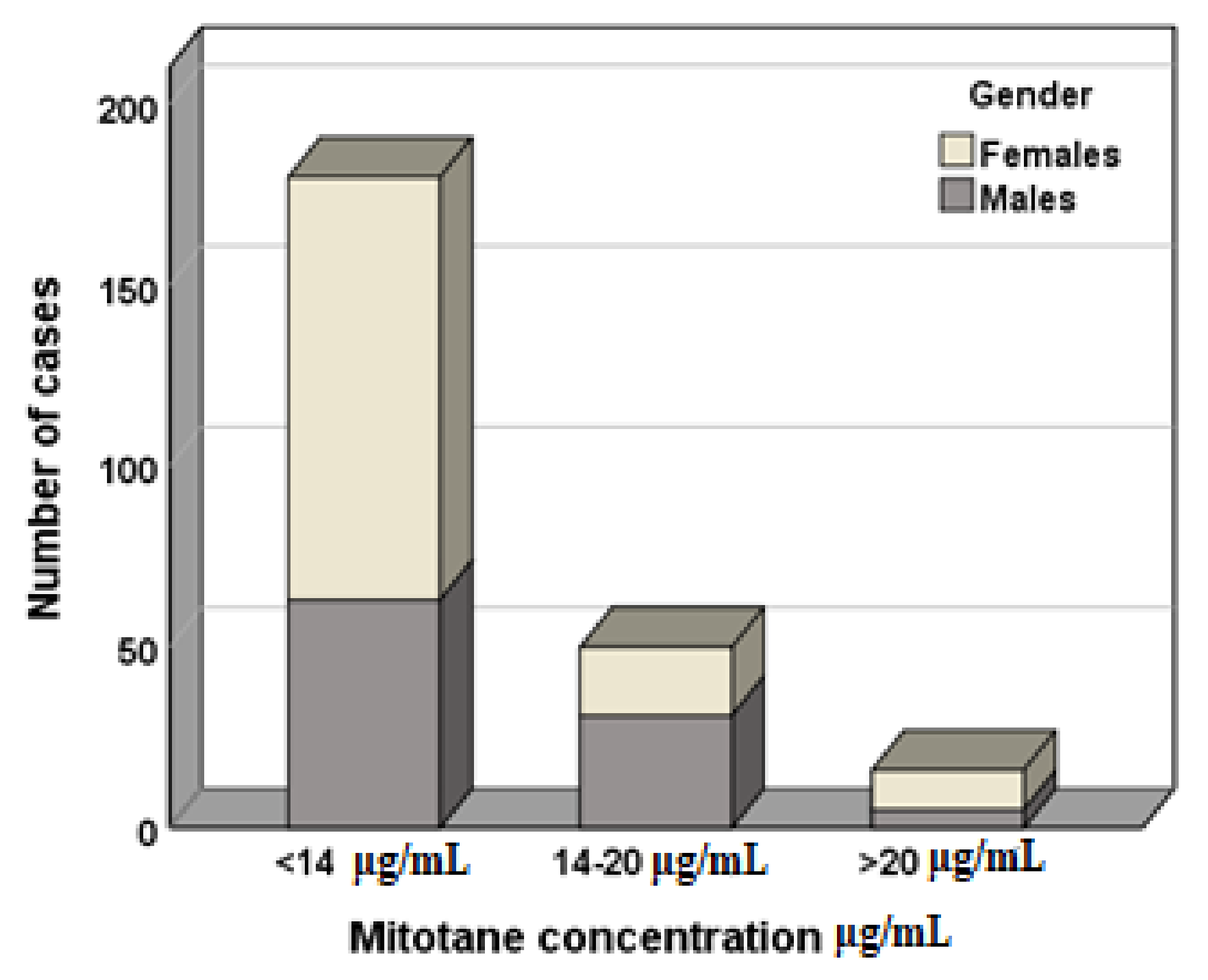
3.4. Effect of Sex on Mitotane Concentration Therapeutic Range
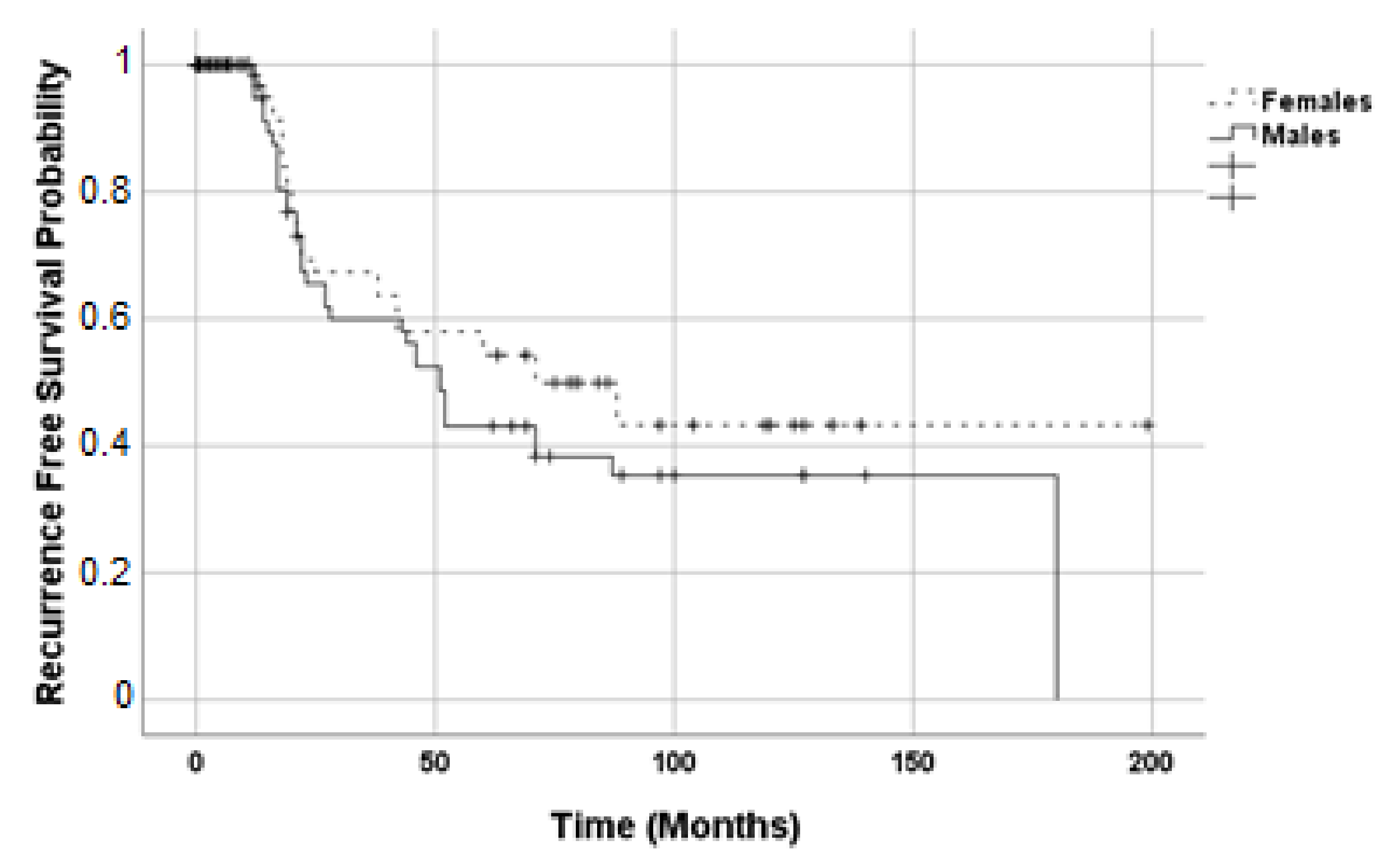
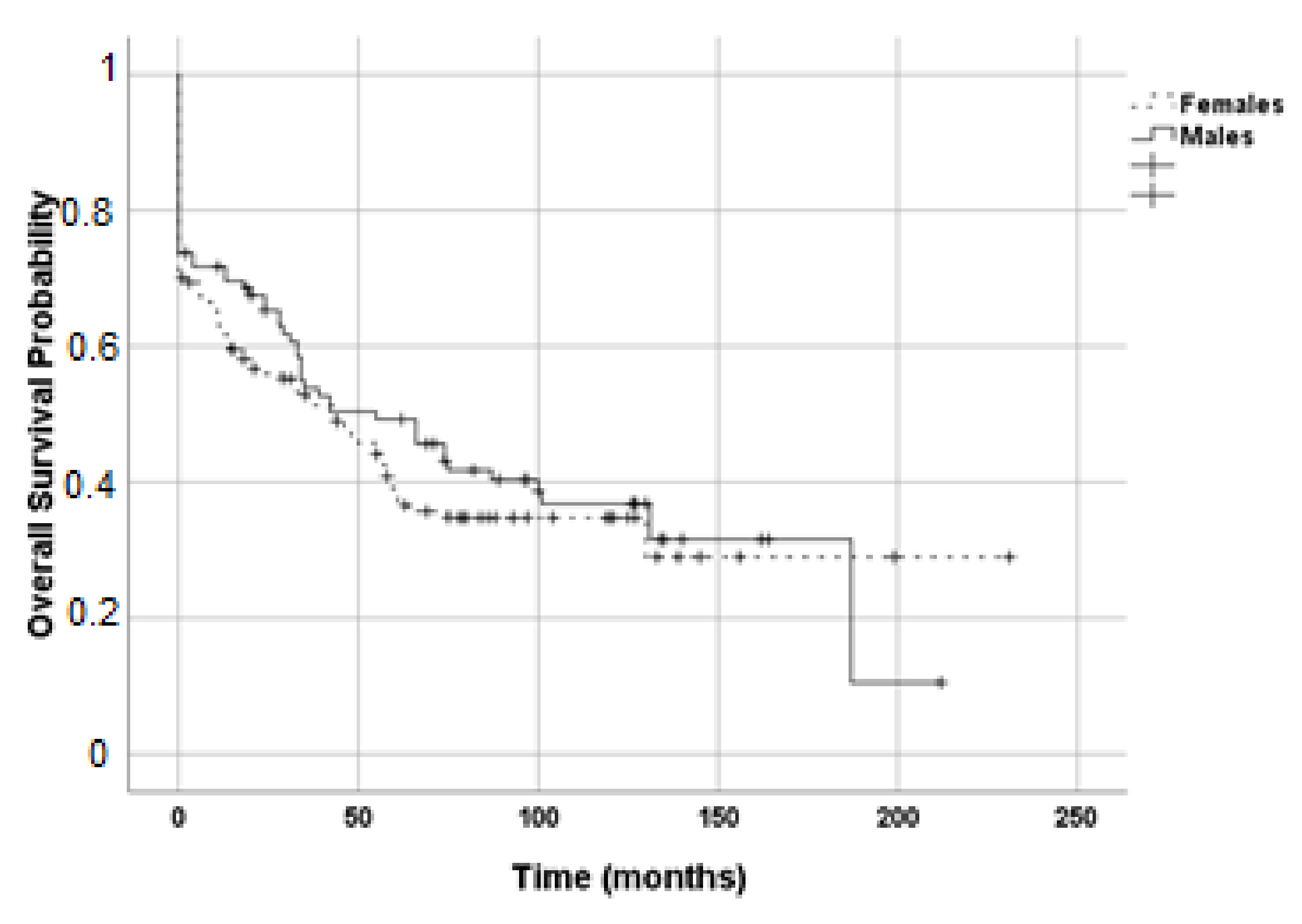
3.5. Effect of Sex on Recurrence Free and Overall Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Libé, R. Adrenocortical carcinoma (ACC): Diagnosis, prognosis, and treatment. Front. Cell Dev. Biol. 2015, 3, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaujoux, S.; Weinandt, M.; Bonnet, S.; Reslinger, V.; Bertherat, J.; Dousset, B. Surgical treatment of adrenal carcinoma. J. Visc. Surg. 2017, 154, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Fassnacht, M.; Dekkers, O.M.; Else, T.; Baudin, E.; Berruti, A.; de Krijger, R.; Haak, H.R.; Mihai, R.; Assie, G.; Terzolo, M. European Society of Endocrinology Clinical Practice Guidelines on the management of adrenocortical carcinoma in adults, in collaboration with the European Network for the Study of Adrenal Tumors. Eur. J. Endocrinol. 2018, 179, G1–G46. [Google Scholar] [CrossRef] [PubMed]
- Terzolo, M.; Angeli, A.; Fassnacht, M.; Daffara, F.; Tauchmanova, L.; Conton, P.A.; Rossetto, R.; Buci, L.; Sperone, P.; Grossrubatscher, E.; et al. Adjuvant mitotane treatment for adrenocortical carcinoma. N. Engl. J. Med. 2007, 356, 2372–2380. [Google Scholar] [CrossRef] [Green Version]
- Calabrese, A.; Basile, V.; Puglisi, S.; Perotti, P.; Pia, A.; Saba, L.; Berchialla, P.; Porpiglia, F.; Veltri, A.; Volante, M.; et al. Adjuvant mitotane therapy is beneficial in non-metastatic adrenocortical carcinoma at high risk of recurrence. Eur. J. Endocrinol. 2019, 180, 387–396. [Google Scholar] [CrossRef]
- Puglisi, S.; Perotti, P.; Cosentini, D.; Roca, E.; Basile, V.; Berruti, A.; Terzolo, M. Decision-making for adrenocortical carcinoma: Surgical, systemic, and endocrine management options. Expert Rev. Anticancer. Ther. 2018, 18, 1125–1133. [Google Scholar] [CrossRef]
- Tornblom, N. Administration of DDD (2,2-bis (parachlorophenyl)-1,1-dichloroethane) to diabetics with hyaline vascular changes and hyperpolysaccharidemia. Acta Med. Scand. 1959, 164, 23–37. [Google Scholar] [CrossRef]
- Young, R.B.; Bryson, M.J.; Sweat, M.L.; Street, J.C. Complexing of DDT and o,p′DDD with adrenal cytochrome P-450 hydroxylating systems. J. Steroid Biochem. 1973, 4, 585–591. [Google Scholar] [CrossRef]
- Puglisi, S.; Perotti, P.; Pia, A.; Reimondo, G.; Terzolo, M. Adrenocortical Carcinoma with Hypercortisolism. Endocrinol. Metab. Clin. N. Am. 2018, 47, 395–407. [Google Scholar] [CrossRef]
- Berruti, A.; Baudin, E.; Gelderblom, H.; Haak, H.R.; Porpiglia, F.; Fassnacht, M.; Pentheroudakis, G.; Group, E.G.W. Adrenal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2012, 23 (Suppl. 7), vii131–vii138. [Google Scholar] [CrossRef]
- Hermsen, I.G.; Fassnacht, M.; Terzolo, M.; Houterman, S.; den Hartigh, J.; Leboulleux, S.; Daffara, F.; Berruti, A.; Chadarevian, R.; Schlumberger, M.; et al. Plasma concentrations of o,p′DDD, o,p′DDA, and o,p′DDE as predictors of tumor response to mitotane in adrenocortical carcinoma: Results of a retrospective ENS@T multicenter study. J. Clin. Endocrinol. Metab. 2011, 96, 1844–1851. [Google Scholar] [CrossRef] [Green Version]
- Megerle, F.; Herrmann, W.; Schloetelburg, W.; Ronchi, C.L.; Pulzer, A.; Quinkler, M.; Beuschlein, F.; Hahner, S.; Kroiss, M.; Fassnacht, M.; et al. Mitotane Monotherapy in Patients With Advanced Adrenocortical Carcinoma. J. Clin. Endocrinol. Metab. 2018, 103, 1686–1695. [Google Scholar] [CrossRef]
- Terzolo, M.; Baudin, A.E.; Ardito, A.; Kroiss, M.; Leboulleux, S.; Daffara, F.; Perotti, P.; Feelders, R.A.; deVries, J.H.; Zaggia, B.; et al. Mitotane levels predict the outcome of patients with adrenocortical carcinoma treated adjuvantly following radical resection. Eur. J. Endocrinol. 2013, 169, 263–270. [Google Scholar] [CrossRef]
- Terzolo, M.; Pia, A.; Berruti, A.; Osella, G.; Alì, A.; Carbone, V.; Testa, E.; Dogliotti, L.; Angeli, A. Low-dose monitored mitotane treatment achieves the therapeutic range with manageable side effects in patients with adrenocortical cancer. J. Clin. Endocrinol. Metab. 2000, 85, 2234–2238. [Google Scholar] [CrossRef]
- D’Avolio, A.; De Francia, S.; Basile, V.; Cusato, J.; De Martino, F.; Pirro, E.; Piccione, F.; Ardito, A.; Zaggia, B.; Volante, M.; et al. Influence of the CYP2B6 polymorphism on the pharmacokinetics of mitotane. Pharm. Genom. 2013, 23, 293–300. [Google Scholar] [CrossRef] [Green Version]
- Cusato, J.; De Francia, S.; Allegra, S.; Carrella, S.; Pirro, E.; Piccione, F.M.; De Martino, F.; Ferrero, A.; Daffara, F.C.; Terzolo, M.; et al. Circannual variation of mitotane and its metabolites plasma levels in patients with adrenocortical carcinoma. J. Pharm. Pharmacol. 2017, 69, 1524–1530. [Google Scholar] [CrossRef]
- Ronchi, C.L.; Sbiera, S.; Volante, M.; Steinhauer, S.; Scott-Wild, V.; Altieri, B.; Kroiss, M.; Bala, M.; Papotti, M.; Deutschbein, T.; et al. CYP2W1 is highly expressed in adrenal glands and is positively associated with the response to mitotane in adrenocortical carcinoma. PLoS ONE 2014, 9, e105855. [Google Scholar] [CrossRef]
- Puglisi, S.; Calabrese, A.; Basile, V.; Ceccato, F.; Scaroni, C.; Simeoli, C.; Torlontano, M.; Cannavò, S.; Arnaldi, G.; Stigliano, A.; et al. Mitotane Concentrations Influence the Risk of Recurrence in Adrenocortical Carcinoma Patients on Adjuvant Treatment. J. Clin. Med. 2019, 8, 1850. [Google Scholar] [CrossRef] [Green Version]
- Anderson, G.D. Gender differences in pharmacological response. Int. Rev. Neurobiol. 2008, 83, 1–10. [Google Scholar] [CrossRef]
- Weiss, L.M.; Medeiros, L.J.; Vickery, A.L. Pathologic features of prognostic significance in adrenocortical carcinoma. Am. J. Surg. Pathol. 1989, 13, 202–206. [Google Scholar] [CrossRef]
- Terzolo, M.; Ardito, A.; Zaggia, B.; Laino, F.; Germano, A.; De Francia, S.; Daffara, F.; Berruti, A. Management of adjuvant mitotane therapy following resection of adrenal cancer. Endocrine 2012, 42, 521–525. [Google Scholar] [CrossRef] [Green Version]
- Fassnacht, M.; Johanssen, S.; Quinkler, M.; Bucsky, P.; Willenberg, H.S.; Beuschlein, F.; Terzolo, M.; Mueller, H.H.; Hahner, S.; Allolio, B.; et al. Limited prognostic value of the 2004 International Union Against Cancer staging classification for adrenocortical carcinoma: Proposal for a Revised TNM Classification. Cancer 2009, 115, 243–250. [Google Scholar] [CrossRef]
- De Francia, S.; Pirro, E.; Zappia, F.; De Martino, F.; Sprio, A.E.; Daffara, F.; Terzolo, M.; Berruti, A.; Di Carlo, F.; Ghezzo, F. A new simple HPLC method for measuring mitotane and its two principal metabolites Tests in animals and mitotane-treated patients. J. Chromatogr. B 2006, 837, 69–75. [Google Scholar] [CrossRef]
- Lane, J.R.; Connor, J.D. The influence of endogenous and exogenous sex hormones in adolescents with attention to oral contraceptives and anabolic steroids. J. Adolesc. Health 1994, 15, 630–634. [Google Scholar] [CrossRef]
- Parish, R.C.; Spivey, C. Influence of menstrual cycle phase on serum concentrations of alpha 1-acid glycoprotein. Br. J. Clin. Pharmacol. 1991, 31, 197–199. [Google Scholar] [CrossRef] [Green Version]
- Flores Pérez, J.; Juárez Olguín, H.; Flores Pérez, C.; Pérez Guillé, G.; Guillé Pérez, A.; Camacho Vieyra, A.; Toledo López, A.; Carrasco Portugal, M.; Lares Asseff, I. Effects of gender and phase of the menstrual cycle on the kinetics of ranitidine in healthy volunteers. Chronobiol. Int. 2003, 20, 485–494. [Google Scholar]
- Wilson, J.T. Developmental pharmacology: A review of its application to clinical and basic science. Annu. Rev. Pharmacol. 1972, 12, 423–457. [Google Scholar] [CrossRef]
- Blackham, A.; Spencer, P.S. The effects of oestrogens and progestins on the response of mice to barbiturates. Br. J. Pharmacol. 1969, 37, 129–139. [Google Scholar] [CrossRef] [Green Version]
- Keskin, S.; Taş, F.; Vatansever, S. Adrenocortical carcinoma: Clinicopathological features, prognostic factors and outcome. Urol Int. 2013, 90, 435–438. [Google Scholar] [CrossRef]
- Luton, J.P.; Cerdas, S.; Billaud, L.; Thomas, G.; Guilhaume, B.; Bertagna, X.; Laudat, M.H.; Louvel, A.; Chapuis, Y.; Blondeau, P. Clinical features of adrenocortical carcinoma, prognostic factors, and the effect of mitotane therapy. N. Engl. J. Med. 1990, 322, 1195–1201. [Google Scholar] [CrossRef]
- Michalkiewicz, E.; Sandrini, R.; Figueiredo, B.; Miranda, E.C.; Caran, E.; Oliveira-Filho, A.G.; Marques, R.; Pianovski, M.A.; Lacerda, L.; Cristofani, L.M.; et al. Clinical and outcome characteristics of children with adrenocortical tumors: A report from the International Pediatric Adrenocortical Tumor Registry. J. Clin. Oncol. 2004, 22, 838–845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, X.; Shu, C.; Chen, L.; Yao, B. Impact of sex, body mass index and initial pathologic diagnosis age on the incidence and prognosis of different types of cancer. Oncol. Rep. 2018, 40, 1359–1369. [Google Scholar] [CrossRef] [PubMed]
- Rahane, C.S.; Kutzner, A.; Heese, K. Establishing a human adrenocortical carcinoma (ACC)-specific gene mutation signature. Cancer Genet. 2019, 230, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barzon, L.; Masi, G.; Pacenti, M.; Trevisan, M.; Fallo, F.; Remo, A.; Martignoni, G.; Montanaro, D.; Pezzi, V.; Palù, G. Expression of aromatase and estrogen receptors in human adrenocortical tumors. Virchows Arch. 2008, 452, 181–191. [Google Scholar] [CrossRef]
- Felizola, S.J.; Nakamura, Y.; Hui, X.G.; Satoh, F.; Morimoto, R.; McNamara, K.M.; Midorikawa, S.; Suzuki, S.; Rainey, W.E.; Sasano, H. Estrogen-related receptor α in normal adrenal cortex and adrenocortical tumors: Involvement in development and oncogenesis. Mol. Cell. Endocrinol. 2013, 365, 207–211. [Google Scholar] [CrossRef] [Green Version]
- Scollo, C.; Russo, M.; Trovato, M.A.; Sambataro, D.; Giuffrida, D.; Manusia, M.; Sapuppo, G.; Malandrino, P.; Vigneri, R.; Pellegriti, G. Prognostic Factors for Adrenocortical Carcinoma Outcomes. Front. Endocrinol. (Lausanne) 2016, 7, 99. [Google Scholar] [CrossRef] [Green Version]
- Sirianni, R.; Zolea, F.; Chimento, A.; Ruggiero, C.; Cerquetti, L.; Fallo, F.; Pilon, C.; Arnaldi, G.; Carpinelli, G.; Stigliano, A.; et al. Targeting estrogen receptor-α reduces adrenocortical cancer (ACC) cell growth in vitro and in vivo: Potential therapeutic role of selective estrogen receptor modulators (SERMs) for ACC treatment. J. Clin. Endocrinol. Metab. 2012, 97, E2238–E2250. [Google Scholar] [CrossRef] [Green Version]
- Wajchenberg, B.L.; Albergaria Pereira, M.A.; Medonca, B.B.; Latronico, A.C.; Campos Carneiro, P.; Alves, V.A.; Zerbini, M.C.; Liberman, B.; Carlos Gomes, G.; Kirschner, M.A. Adrenocortical carcinoma: Clinical and laboratory observations. Cancer 2000, 88, 711–736. [Google Scholar] [CrossRef]
- Abiven, G.; Coste, J.; Groussin, L.; Anract, P.; Tissier, F.; Legmann, P.; Dousset, B.; Bertagna, X.; Bertherat, J. Clinical and biological features in the prognosis of adrenocortical cancer: Poor outcome of cortisol-secreting tumors in a series of 202 consecutive patients. J. Clin. Endocrinol. Metab. 2006, 91, 2650–2655. [Google Scholar] [CrossRef]
- Zheng, S.; Cherniack, A.D.; Dewal, N.; Moffitt, R.A.; Danilova, L.; Murray, B.A.; Lerario, A.M.; Else, T.; Knijnenburg, T.A.; Ciriello, G.; et al. Comprehensive Pan-Genomic Characterization of Adrenocortical Carcinoma. Cancer Cell 2016, 30, 363. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | N = 246 |
|---|---|
| Male, n (%) | 147 (59.8) |
| Female, n (%) | 99 (40.2) |
| Median age, years (IQR) | 45.5 (35.2–57.1) |
| Median body mass index (BMI), kg/m2 (IQR) | 23.4 (21.6–27.5) |
| Margins, R status | |
| R0, n (%) | 89 (36.8) |
| R1, n (%) | 57 (23.6) |
| RX, n (%) | 8 (3.3) |
| Median size, cm (IQR) | 7.00 (1.00–12.00) |
| Median Ki67 index, % (IQR) | 25.50 (14.00–40.00) |
| Median mitotic count (IQR) | 12.50 (6.00–25.00) |
| Tumor stage | |
| I, n (%) | 16 (6.6) |
| II, n (%) | 82 (33.9) |
| III, n (%) | 38 (15.7) |
| IV, n (%) | 28 (11.6) |
| Hormone secretion | |
| No secretion, n (%) | 73 (30.2) |
| Secretion, n (%) | 82 (33.9) |
| Cortisol/cortisol + other steroids, n (%) | 66 (27.3) |
| No hormone work up, n (%) | 17 (7.0) |
| Median Weiss score (IQR) | 7 (5–8) |
| Death, n (%) | 83 (34.3) |
| Median recurrence-free survival, months (IQR) | 19.00 (7.00–69.00) |
| Median overall survival, months (IQR) | 60.50 (28.25–100.75) |
| Median o,p′-DDD concentration, µg/mL (IQR) | 8.82 (4.36–14.37) |
| Median o,p′-DDE concentration, µg/mL (IQR) (N = 178) | 0.90 (0.48–1.50) |
| Mitotane therapeutic range | |
| <14 µg/mL | 180 (73.2) |
| 14–20 µg/mL | 50 (20.3) |
| >20 µg/mL | 16 (6.5) |
| o,p′-DDD Concentration | o,p′-DDE Concentration | |||
|---|---|---|---|---|
| Univariate | Multivariate | Univariate | Multivariate | |
| FACTOR | p β (IC95%) | p β (IC95%) | P β (IC95%) | P β (IC95%) |
| Age | 0.004 −0.185 (−0.147; −0.029) | 0.088 −0.123 (−0.123; 0.009) | <0.001 −0.298 (−0.026; −0.009) | 0.029 −0.200 (−0.023; −0.001) |
| Gender | 0.032 0.137 (0.168; 3.699) | 0.010 0.189 (0.644; 4.573) | 0.004 0.216 (0.124; 0.629) | 0.029 0.199 (0.034; 0.628) |
| BMI | 0.616 −0.053 (−0.386; 0.230) | 0.978 −0.004 (−0.033; 0.032) | ||
| Margins | 0.313 −0.081 (−2.632; 0.8499 | 0.579 −0.050 (−0.342; 0.192) | ||
| Hormone secretion | 0.003 −0.222 (−2.639; −0.546) | 0.005 −0.207 (−2.508; −0.464) | 0.711 −0.371 (−0.189; 0.129) | |
| Tumor stage | 0.425 0.062 (−0.709; 1.673) | 0.143 0.128 (−0.044; 0.301) | 0.242 0.114 (−0.079; 0.311) | |
| Tumor size | 0.655 0.032 (−0.044; 0.070) | 0.267 −0.091 (−0.014; 0.004) | ||
| Weiss score | 0.876 −0.013 (−0.692; 0.590) | 0.585 0.052 (−0.076; 0.135) | ||
| Ki67 index | 0.803 −0.022 (−0.068; 0.053) | 0.010 −0.258 (−0.019; −0.003) | 0.059 −0.171 (−0.015; 0) | |
| Mitotic count | 0.630 −0.041 (−0.064; 0.039) | 0.089 0.168 (−0.001; 0.015) | 0.327 −0.124 (−0.015; 0.005) | |
| UNIVARIATE | MULTIVARIATE | |
|---|---|---|
| FACTOR | p OR (IC95%) | p OR (IC95%) |
| Age | 0.407 0.991 (0.970; 1.012) | |
| Gender | 0.001 0.326 (0.171; 0.619) | <0.001 4.829 (2.156; 10.814) |
| BMI | 0.709 0.977 (0.865; 1.104) | |
| Margins | 0.693 1.154 (0.635; 2.095) | |
| Hormone secretion | 0.001 0.422 (0.249; 0.716) | 0.005 0.484 (0.292; 0.801) |
| Tumour stage | 0.100 0.699 (0.455; 1.072) | 0.102 0.663 (0.405; 1.085) |
| Tumour size | 0.188 1.011 (0.994; 1.029) | 0.728 0.996 (0.976; 1.017) |
| Weiss score | 0.925 0.990 (0.799; 1.227) | |
| Ki67 index | 0.219 0.987 (0.967; 1.008) | |
| Mitotic count | 0.387 0.992 (0.974; 1.010) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Allegra, S.; Puglisi, S.; Brescia, I.; Chiara, F.; Basile, V.; Calabrese, A.; Reimondo, G.; De Francia, S. Sex Differences on Mitotane Concentration and Treatment Outcome in Patients with Adrenocortical Carcinoma. Life 2021, 11, 266. https://doi.org/10.3390/life11030266
Allegra S, Puglisi S, Brescia I, Chiara F, Basile V, Calabrese A, Reimondo G, De Francia S. Sex Differences on Mitotane Concentration and Treatment Outcome in Patients with Adrenocortical Carcinoma. Life. 2021; 11(3):266. https://doi.org/10.3390/life11030266
Chicago/Turabian StyleAllegra, Sarah, Soraya Puglisi, Irene Brescia, Francesco Chiara, Vittoria Basile, Anna Calabrese, Giuseppe Reimondo, and Silvia De Francia. 2021. "Sex Differences on Mitotane Concentration and Treatment Outcome in Patients with Adrenocortical Carcinoma" Life 11, no. 3: 266. https://doi.org/10.3390/life11030266