Primary Gastro-Intestinal Lymphoma and Gastro-Intestinal Adenocarcinoma: An Initial Study of CT Texture Analysis as Quantitative Biomarkers for Differentiation



Abstract
:1. Introduction
2. Materials and Methods
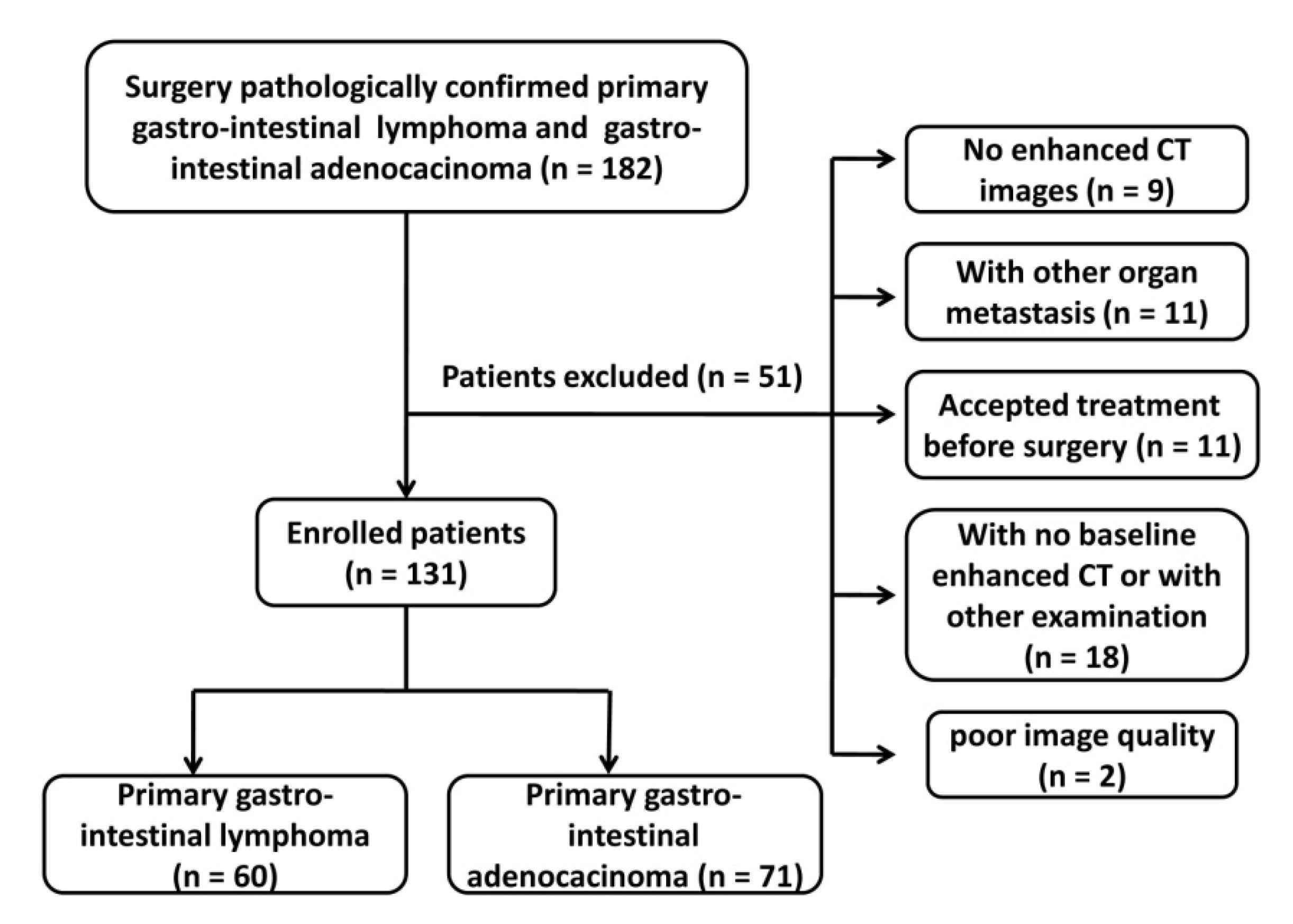
2.1. Patients Enrolled
2.2. Image Acquisition
2.3. Image Analysis
2.4. Statistical Analysis
3. Results
3.1. Clinical Features of the Patients with PGIL and Those with GIAC
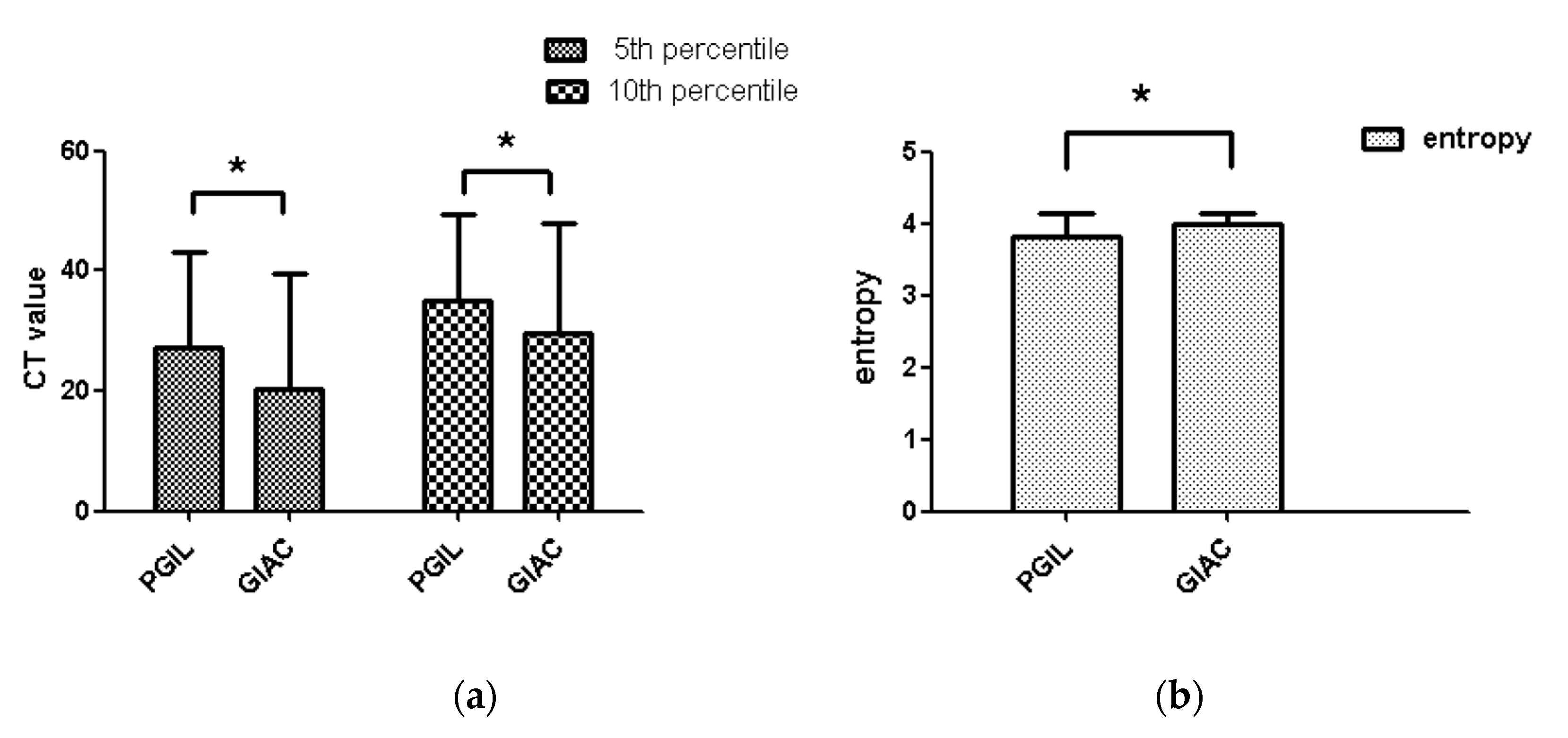
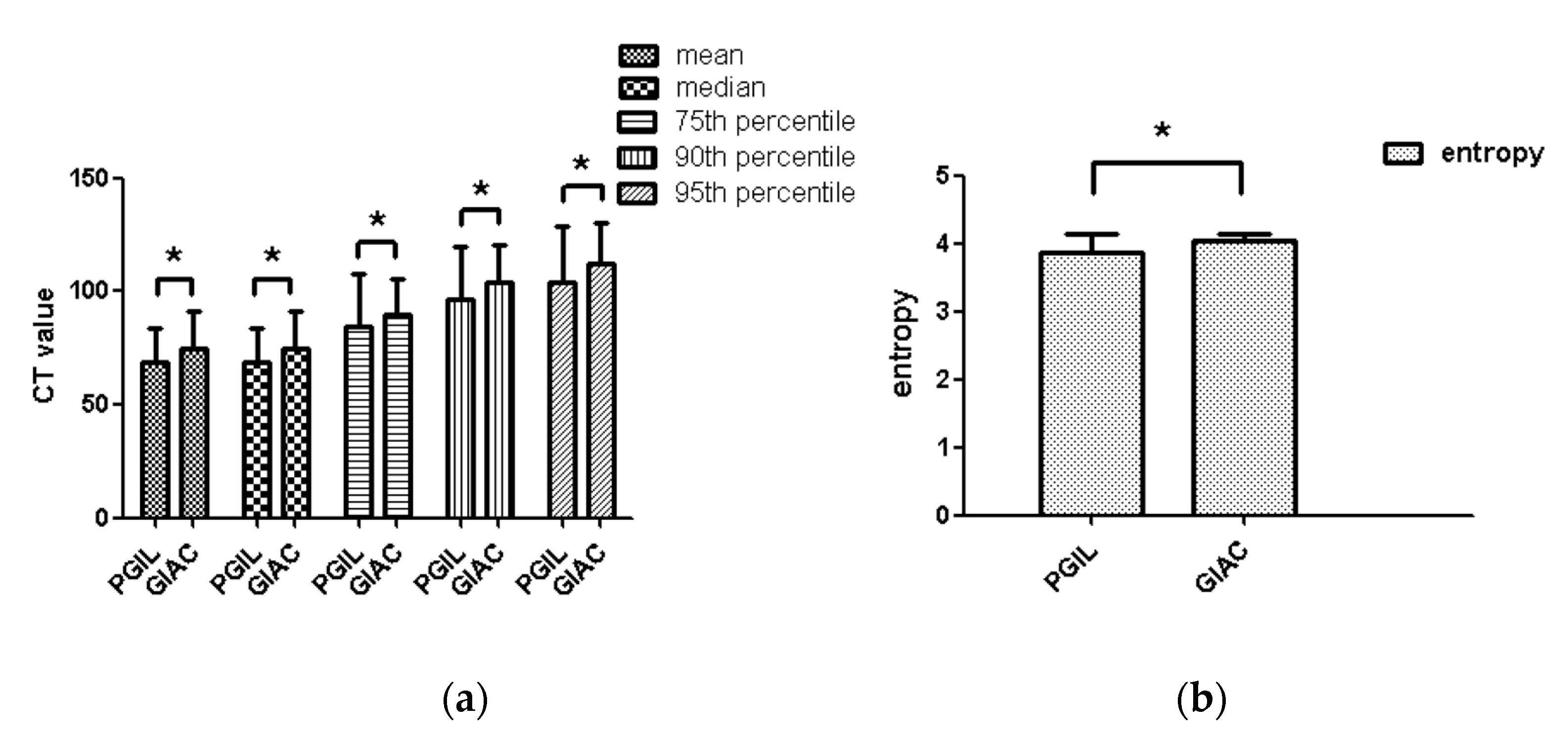
3.2. Histogram of the Comparison of Parameters Between the Patients with PGIL and Those with GIAC
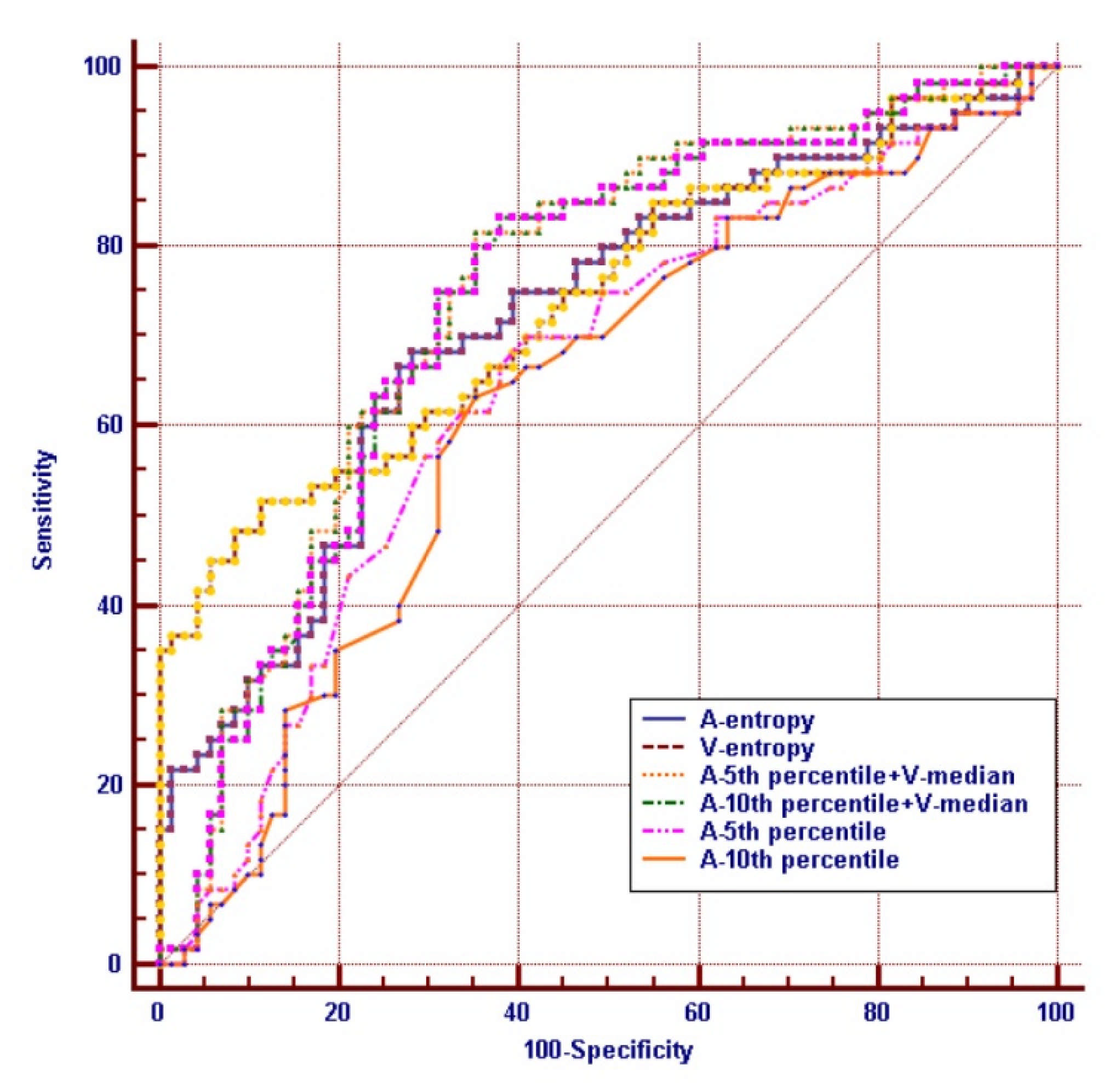
3.3. Prediction of Differentiation PGIL from GIAC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chang, S.T.; Menias, C.O. Imaging of Primary Gastrointestinal Lymphoma. Semin. Ultrasound CT MRI 2013, 34, 558–565. [Google Scholar] [CrossRef] [PubMed]
- Bautista-Quach, M.A.; Ake, C.D.; Chen, M.; Wang, J. Gastrointestinal lymphomas: Morphology, immunophenotype and molecular fea-tures. J. Gastrointest. Oncol. 2012, 3, 209–225. [Google Scholar] [PubMed]
- Schottenfeld, D.; Beebe-Dimmer, J.L.; Vigneau, F.D. The Epidemiology and Pathogenesis of Neoplasia in the Small Intestine. Ann. Epidemiol. 2009, 19, 58–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ugurlu, M.M.; Asoglu, O.; Potter, D.D.; Barnes, S.A.; Harmsen, W.S.; Donohue, J.H. Adenocarcinomas of the Jejunum and Ileum: A 25-Year Experience. J. Gastrointest. Surg. 2005, 9, 1182–1188. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.G.; Zhao, L.Y.; Liu, C.Q.; Pan, S.C.; Chen, X.L.; Liu, K.; Zhang, W.H.; Yang, K.; Chen, X.Z.; Hu, J.K. Clinical characteristics and prognostic factors of primary gastric lymphoma: A retrospective study with 165 cases. Medicine (Baltimore) 2016, 95, e4250. [Google Scholar] [CrossRef]
- Nguyen, P.H.; Giraud, J.; Chambonnier, L.; Dubus, P.; Wittkop, L.; Belleannée, G.; Collet, D.; Soubeyran, I.; Evrard, S.; Rousseau, B.; et al. Characterization of Biomarkers of Tumorigenic and Chemoresistant Cancer Stem Cells in Human Gastric Carcinoma. Clin. Cancer Res. 2016, 23, 1586–1597. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, E.; Ezzat, A.A.; El-Weshi, A.N.; Martin, J.M.; Khafaga, Y.M.; Al Rabih, W.; Ajarim, D.S.; Al-Fouden, M.O.; Zucca, E. Primary intestinal diffuse large B-cell non-Hodgkin’s lymphoma: Clinical features, man-agement, and prognosis of 66 patients. Ann. Oncol. 2001, 12, 53–58. [Google Scholar] [CrossRef]
- Young, J.I.; Mongoue-Tchokote, S.; Wieghard, N.; Mori, M.; Vaccaro, G.M.; Sheppard, B.C.; Tsikitis, V.L. Treatment and Survival of Small-bowel Adenocarcinoma in the United States. Dis. Colon Rectum 2016, 59, 306–315. [Google Scholar] [CrossRef]
- El-Galaly, T.C.; Villa, D.; Gormsen, L.C.; Baech, J.; Lo, A.; Cheah, C.Y. FDG-PET/CT in the management of lymphomas: Current status and future directions. J. Intern. Med. 2018, 284, 358–376. [Google Scholar] [CrossRef] [Green Version]
- Galia, M.; Albano, D.; Narese, D.; Patti, C.; Chianca, V.; Di Pietto, F.; Mulè, A.; Grassedonio, E.; La Grutta, L.; Lagalla, R.; et al. Whole-body MRI in patients with lymphoma: Collateral findings. Radiol. Med. 2016, 121, 793–800. [Google Scholar] [CrossRef]
- Aleman, B.M.; Haas, R.L.; Van Der Maazen, R.W. Role of radiotherapy in the treatment of lymphomas of the gastrointestinal tract. Best Pract. Res. Clin. Gastroenterol. 2010, 24, 27–34. [Google Scholar] [CrossRef]
- Mishima, Y.; Terui, Y.; Yokoyama, M.; Nishimura, N.; Sakajiri, S.; Ueda, K.; Kuboki, Y.; Nakano, K.; Suzuki, K.; Nara, E.; et al. R-CHOP with dose-attenuated radiation therapy could induce good prognosis in gastric dif-fuse large B cell lymphoma. Exp. Hematol. Oncol. 2012, 1, 30. [Google Scholar] [CrossRef] [Green Version]
- Gollub, M.J. Imaging of Gastrointestinal Lymphoma. Radiol. Clin. N. Am. 2008, 46, 287–312. [Google Scholar] [CrossRef]
- Anzidei, M.; Napoli, A.; Zini, C.; A Kirchin, M.; Catalano, C.; Passariello, R. Malignant tumours of the small intestine: A review of histopathology, multidetector CT and MRI aspects. Br. J. Radiol. 2011, 84, 677–690. [Google Scholar] [CrossRef] [Green Version]
- Lubner, M.G.; Smith, A.D.; Sandrasegaran, K.; Sahani, D.V.; Pickhardt, P.J. CT Texture Analysis: Definitions, Applications, Biologic Correlates, and Challenges. Radiographics 2017, 37, 1483–1503. [Google Scholar] [CrossRef]
- Lu, J.; Hu, D.; Tang, H.; Hu, X.; Shen, Y.; Li, Z.; Peng, Y.; Kamel, I. Assessment of tumor heterogeneity: Differentiation of periampullary neoplasms based on CT whole-lesion histogram analysis. Eur. J. Radiol. 2019, 115, 1–9. [Google Scholar] [CrossRef]
- Dawson, I.M.P.; Cornes, J.S.; Morson, B.C. Primary malignant lymphoid tumours of the intestinal tract. Report of 37 cases with a study of factors influencing prognosis. BJS 1961, 49, 80–89. [Google Scholar] [CrossRef]
- Yip, C.; Landau, D.; Kozarski, R.; Ganeshan, B.; Thomas, R.; Michaelidou, A.; Goh, V. Primary Esophageal Cancer: Heterogeneity as Potential Prognostic Biomarker in Patients Treated with Definitive Chemotherapy and Radiation Therapy. Radiology 2014, 270, 141–148. [Google Scholar] [CrossRef]
- Feng, C.; Lu, F.; Shen, Y.; Li, A.; Yu, H.; Tang, H.; Li, Z.; Hu, D. Tumor heterogeneity in gastrointestinal stromal tumors of the small bowel: Volumetric CT texture analysis as a potential biomarker for risk stratification. Cancer Imaging 2018, 18, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Choi, I.Y.; Yeom, S.K.; Cha, J.; Cha, S.H.; Lee, S.H.; Chung, H.H.; Lee, C.M.; Choi, J. Feasibility of using computed tomography texture analysis parameters as imaging biomarkers for predicting risk grade of gastrointestinal stromal tumors: Comparison with visual inspection. Abdom. Radiol. 2019, 44, 2346–2356. [Google Scholar] [CrossRef]
- Ng, F.; Ganeshan, B.; Kozarski, R.; Miles, K.A.; Goh, V. Assessment of Primary Colorectal Cancer Heterogeneity by Using Whole-Tumor Texture Analysis: Contrast-enhanced CT Texture as a Biomarker of 5-year Survival. Radiology 2013, 266, 177–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersen, I.R.; Thorup, K.; Andersen, M.B.; Olesen, R.; Mortensen, F.V.; Nielsen, D.T.; Rasmussen, F. Texture in the monitoring of regorafenib therapy in patients with colorectal liver metas-tases. Acta Radiol. 2019, 60, 1084–1093. [Google Scholar] [CrossRef]
- Ganeshan, B.; Miles, K.A.; Babikir, S.; Shortman, R.; Afaq, A.; Ardeshna, K.M.; Groves, A.M.; Kayani, I. CT-based texture analysis potentially provides prognostic information complementary to interim fdg-pet for patients with hodgkin’s and aggressive non-hodgkin’s lymphomas. Eur. Radiol. 2017, 27, 1012–1020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, C.-B.; Yu, N.; Jian, Y.-J.; Yu, Y.; Duan, H.-F.; Zhang, X.-R.; Ma, G.-M.; Guo, Y.; Duan, X. Spectral CT Imaging in the Differential Diagnosis of Small Bowel Adenocarcinoma From Primary Small Intestinal Lymphoma. Acad. Radiol. 2019, 26, 878–884. [Google Scholar] [CrossRef] [PubMed]
- Goh, V.; Sanghera, B.; Wellsted, D.M.; Sundin, J.; Halligan, S. Assessment of the spatial pattern of colorectal tumour perfusion estimated at perfusion CT using two-dimensional fractal analysis. Eur. Radiol. 2009, 19, 1358–1365. [Google Scholar] [CrossRef] [PubMed]
- Yardimci, A.H.; Sel, I.; Bektas, C.T.; Yarikkaya, E.; Dursun, N.; Bektas, H.; Afsar, C.U.; Gursu, R.U.; Yardimci, V.H.; Ertas, E.; et al. Computed tomography texture analysis in patients with gastric cancer: A quantitative imaging biomarker for preoperative evaluation before neoadjuvant chemotherapy treatment. Jpn. J. Radiol. 2020, 38, 553–560. [Google Scholar] [CrossRef]
- Prezzi, D.; Owczarczyk, K.; Bassett, P.; Siddique, M.; Breen, D.J.; Cook, G.J.R.; Goh, V. Adaptive statistical iterative reconstruction (ASIR) affects CT radiomics quantification in primary colorectal cancer. Eur. Radiol. 2019, 29, 5227–5235. [Google Scholar] [CrossRef] [Green Version]
- Giganti, F.; Antunes, S.; Salerno, A.; Ambrosi, A.; Marra, P.; Nicoletti, R.; Orsenigo, E.; Chiari, D.; Albarello, L.; Staudacher, C.; et al. Gastric cancer: Texture analysis from multidetector computed tomography as a potential preoperative prognostic biomarker. Eur. Radiol. 2016, 27, 1831–1839. [Google Scholar] [CrossRef]
- Buckley, J.A.; Fishman, E.K. CT evaluation of small bowel neoplasms: Spectrum of disease. Radiographics 1998, 18, 379–392. [Google Scholar] [CrossRef] [Green Version]
- Gore, R.M.; Mehta, U.K.; Berlin, J.W.; Rao, V.; Newmark, G.M. Diagnosis and staging of small bowel tumours. Cancer Imaging 2006, 6, 209–212. [Google Scholar] [CrossRef] [Green Version]
- Chee, C.G.; Kim, Y.H.; Lee, K.H.; Lee, Y.J.; Park, J.H.; Lee, H.S.; Ahn, S.; Kim, B. CT texture analysis in patients with locally advanced rectal cancer treated with neoadjuvant chemoradiotherapy: A potential imaging biomarker for treatment response and prognosis. PLoS ONE 2017, 12, e0182883. [Google Scholar] [CrossRef] [Green Version]
- Alic, L.; Van Vliet, M.; Van Dijke, C.F.; Eggermont, A.M.M.; Veenland, J.F.; Niessen, W. Heterogeneity in DCE-MRI parametric maps: A biomarker for treatment response? Phys. Med. Biol. 2011, 56, 1601–1616. [Google Scholar] [CrossRef]
- Liu, S.; Ji, C.; Zheng, H.; Pan, X.; Zhang, Y.; Guan, W.; Chen, L.; Li, W.; He, J.; Ge, Y.; et al. Application of CT texture analysis in predicting histopathological characteristics of gastric cancers. Eur. Radiol. 2017, 27, 4951–4959. [Google Scholar] [CrossRef]
- Li, J.; Lu, J.; Liang, P.; Li, A.; Hu, Y.; Shen, Y.; Hu, D.; Li, Z. Differentiation of atypical pancreatic neuroendocrine tumors from pancreatic ductal adenocarcinomas: Using whole-tumor CT texture analysis as quantitative biomarkers. Cancer Med. 2018, 7, 4924–4931. [Google Scholar] [CrossRef]
- Miles, K.A.; Ganeshan, B.; Hayball, M.P. CT texture analysis using the filtration-histogram method: What do the measurements mean? Cancer Imaging 2013, 13, 400–406. [Google Scholar] [CrossRef] [Green Version]
- Moon, W.K.; Choi, J.W.; Cho, N.; Park, S.H.; Chang, J.M.; Jang, M.; Kim, K.G. Computer-aided analysis of ultrasound elasticity images for classification of benign and ma-lignant breast masses. AJR Am. J. Roentgenol. 2010, 195, 1460–1465. [Google Scholar] [CrossRef] [Green Version]
- Ganeshan, B.; Miles, K.A. Quantifying tumour heterogeneity with CT. Cancer Imaging 2013, 13, 140–149. [Google Scholar] [CrossRef] [Green Version]
- Giganti, F.; Tang, L.; Baba, H. Gastric cancer and imaging biomarkers: Part 1—A critical review of DW-MRI and CE-MDCT findings. Eur. Radiol. 2019, 29, 1743–1753. [Google Scholar] [CrossRef] [Green Version]
- Tang, L.; Wang, X.-J.; Baba, H.; Giganti, F. Gastric cancer and image-derived quantitative parameters: Part 2—a critical review of DCE-MRI and 18F-FDG PET/CT findings. Eur. Radiol. 2020, 30, 247–260. [Google Scholar] [CrossRef] [Green Version]
- Lim, C.H.; Hyun, S.H.; Moon, S.H.; Cho, Y.S.; Choi, J.Y.; Lee, K.-H. Comparison of the prognostic values of 18F-fluorodeoxyglucose parameters from colon and non-colon sites of involvement in diffuse large B-cell lymphoma of the colon. Sci. Rep. 2020, 10, 1–10. [Google Scholar] [CrossRef]
- North, J.H.; Pack, M.S. Malignant tumors of the small intestine: A review of 144 cases. Am. Surg. 2000, 66, 46–51. [Google Scholar] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PGIL | GIAC | |
|---|---|---|
| Number of patients | 60 | 71 |
| Age, y | 50.75 (24–74) | 56.1 (21–80) |
| Sex | ||
| Man | 38 (63.3%) | 41 (57.7%) |
| Woman | 22 (36.7%) | 30 (42.3%) |
| Primary mass location | ||
| Stomach | 35 (58.3%) | 16 (22.5%) |
| Duodenum | 3 (5%) | 24 (33.8%) |
| Small intestine | 10 (16.7%) | 14 (19.7%) |
| Colon | 5 (8.4%) | 12 (17.0%) |
| Cecus | 7 (11.6%) | 4 (5.6%) |
| Appendix | 0 (0%) | 1 (1.4%) |
| Maxium diameter (cm) | ||
| 2.49 (1.0–6.55) | 1.96 (1.0–4.0) |
| Lymphoma Classification | Stomach | Small Intestine | Colon | Total Number |
|---|---|---|---|---|
| Diffuse large B-cell lymphoma | 25 (41.67%) | 5 (8.33%) | 10 (16.67%) | 40 (66.67%) |
| Mucosa associated lymphoid tissue lymphoma | 9 (15%) | 3 (5%) | 0 (%) | 12 (20%) |
| Burkitt lymphoma | 0 (0%) | 1 (1.67%) | 0 (%) | 1 (1.67%) |
| Extranodal NK/T cell lymphoma | 0 (%) | 1 (1.67%) | 0 (%) | 1 (1.67%) |
| Follicular lymphoma | 1 (1.665%) | 1 (1.665%) | 0 (%) | 2 (3.33%) |
| Mantle cell lymphoma | 0 (%) | 1 (1.665%) | 1 (1.665%) | 2 (3.33%) |
| Peripheral T cell lymphoma | 0 (%) | 1 (1.665%) | 1 (1.665%) | 2 (3.33%) |
| Parameter | PGIL | GIAC | p Value |
|---|---|---|---|
| A-mean a | 60.00 ± 12.40 | 60.90 ± 17.48 | 0.681 |
| A-median a | 60.23 ± 12.65 | 61.10 ± 17.65 | 0.631 |
| A-5%th percentile a | 27.22 ± 15.78 | 20.31 ± 19.13 | 0.003 * |
| A-10%th percentile a | 34.88 ± 14.64 | 29.59 ± 18.27 | 0.011 * |
| A-25%th percentile a | 46.94 ± 14.07 | 44.14 ± 17.63 | 0.126 |
| A-50%th percentile a | 59.83 ± 14.57 | 59.84 ± 17.61 | 0.501 |
| A-75%th percentile a | 72.93 ± 16.66 | 75.62 ± 18.40 | 0.488 |
| A-90%th percentile a | 84.44 ± 18.70 | 89.27 ± 19.78 | 0.122 |
| A-95%th percentile a | 91.88 ± 20.83 | 97.48 ± 20.60 | 0.055 |
| A-skewness | −0.08 ± 0.18 | −0.12 ± 0.24 | 0.518 |
| A-kurtosis | 0.21 ± 0.27 | 0.29 ± 0.63 | 0.408 |
| A-entropy | 3.82 ± 0.31 | 4.00 ± 0.13 | 0.001 * |
| Parameter | PGIL | GIAC | p Value |
|---|---|---|---|
| V-mean a | 68.87 ± 14.84 | 74.60 ± 16.55 | 0.036 * |
| V-median a | 69.10 ± 14.85 | 75.06 ± 16.41 | 0.029 * |
| V-5%th percentile a | 37.87 ± 27.34 | 33.04 ± 21.10 | 0.550 |
| V-10%th percentile a | 45.47 ± 25.97 | 42.13 ± 20.12 | 0.824 |
| V-25%th percentile a | 58.13 ± 23.89 | 57.33 ± 18.07 | 0.521 |
| V-50%th percentile a | 71.57 ± 22.78 | 73.73 ± 16.41 | 0.087 |
| V-75%th percentile a | 84.73 ± 22.92 | 89.49 ± 16.21 | 0.007 * |
| V-90%th percentile a | 96.37 ± 23.26 | 103.87 ± 16.69 | 0.001 * |
| V-95%th percentile a | 103.9 ± 24.52 | 112.62 ± 17.96 | 0.001 * |
| V-skewness | −0.094 ± 0.211 | −0.105 ± 0.233 | 0.785 |
| V-kurtosis | 0.226 ± 0.463 | 0.127 ± 0.364 | 0.280 |
| V-entropy | 3.871 ± 0.275 | 4.035 ± 0.095 | 0.001 * |
| Parameters | AUC (95% Confidence Interval) | Cut-off | Sensitivity (%) | Specificity (%) | p-Value |
|---|---|---|---|---|---|
| A-5th percentile a | 0.649 (0.560–0.730) | 22 | 70 | 59.15 | 0.0023 |
| A-10th percentile a | 0.628 (0.540–0.711) | 33 | 63.3 | 64.8 | 0.0093 |
| A-entropy | 0.717 (0.631–0.792) | 3.96 | 68.33 | 71.83 | <0.0001 |
| V-mean a | 0.607 (0.517–0.691) | 76.05 | 80.0 | 47.9 | 0.0321 |
| V-median a | 0.611 (0.522–0.695) | 76.0 | 80.0 | 47.9 | 0.025 |
| V-75th percentile a | 0.636 (0.547–0.718) | 87.0 | 73.33 | 53.52 | 0.0059 |
| V-90th percentile a | 0.663 (0.575–0.743) | 92.8 | 58.33 | 70.42 | 0.0008 |
| V-95th percentile a | 0.671 (0.584–0.751) | 100 | 58.33 | 71.83 | 0.0004 |
| V-entropy | 0.739 (0.656–0.812) | 3.93 | 48.33 | 78.73 | <0.0001 |
| V-median+ A-5th percentile | 0.746 (0.663–0.818) | NS | 81.7 | 64.8 | <0.0001 |
| V-median+ A-10th percentile | 0.739 (0.650–0.832) | NS | 83.3 | 62.0 | <0.0001 |
| B | S.E. | Wals | df | P | Odds Ratio | 95%CI for Odds Ratio | ||
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| A-5% percentile | −0.057 | 0.015 | 15.163 | 1 | 0.000 | 0.944 | 0.918 | 0.972 |
| V-median | 0.065 | 0.017 | 14.661 | 1 | 0.000 | 1.067 | 1.032 | 1.103 |
| Constant | −3.124 | 1.021 | 9.360 | 1 | 0.002 | 0.044 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ding, L.; Wu, S.; Shen, Y.; Hu, X.; Hu, D.; Kamel, I.; Li, Z. Primary Gastro-Intestinal Lymphoma and Gastro-Intestinal Adenocarcinoma: An Initial Study of CT Texture Analysis as Quantitative Biomarkers for Differentiation. Life 2021, 11, 264. https://doi.org/10.3390/life11030264
Ding L, Wu S, Shen Y, Hu X, Hu D, Kamel I, Li Z. Primary Gastro-Intestinal Lymphoma and Gastro-Intestinal Adenocarcinoma: An Initial Study of CT Texture Analysis as Quantitative Biomarkers for Differentiation. Life. 2021; 11(3):264. https://doi.org/10.3390/life11030264
Chicago/Turabian StyleDing, Lin, Sisi Wu, Yaqi Shen, Xuemei Hu, Daoyu Hu, Ihab Kamel, and Zhen Li. 2021. "Primary Gastro-Intestinal Lymphoma and Gastro-Intestinal Adenocarcinoma: An Initial Study of CT Texture Analysis as Quantitative Biomarkers for Differentiation" Life 11, no. 3: 264. https://doi.org/10.3390/life11030264