Figure 1.
Traditional community life circle to an aging-friendly community life circle.
Figure 1.
Traditional community life circle to an aging-friendly community life circle.
Figure 2.
Scope of the study area.
Figure 2.
Scope of the study area.
Figure 3.
Community population distribution in the study area.
Figure 3.
Community population distribution in the study area.
Figure 4.
Schematic diagram of the health characteristics of the elderly.
Figure 4.
Schematic diagram of the health characteristics of the elderly.
Figure 5.
Schematic diagram of the hierarchical division of the life circle of the elderly.
Figure 5.
Schematic diagram of the hierarchical division of the life circle of the elderly.
Figure 6.
Evaluation framework.
Figure 6.
Evaluation framework.
Figure 7.
The distribution of the elderly population.
Figure 7.
The distribution of the elderly population.
Figure 8.
The distribution of the elderly population after community rasterization (600 m × 600 m).
Figure 8.
The distribution of the elderly population after community rasterization (600 m × 600 m).
Figure 9.
Distribution of medical and health facilities in the study area. (a) 5-min life circle level, (b) 10-min life circle level, (c) 15-min life circle level.
Figure 9.
Distribution of medical and health facilities in the study area. (a) 5-min life circle level, (b) 10-min life circle level, (c) 15-min life circle level.
Figure 10.
The distribution map of pension service facilities in the study area. (a) 5-min life circle level, (b) 10-min life circle level, (c) 15-min life circle level.
Figure 10.
The distribution map of pension service facilities in the study area. (a) 5-min life circle level, (b) 10-min life circle level, (c) 15-min life circle level.
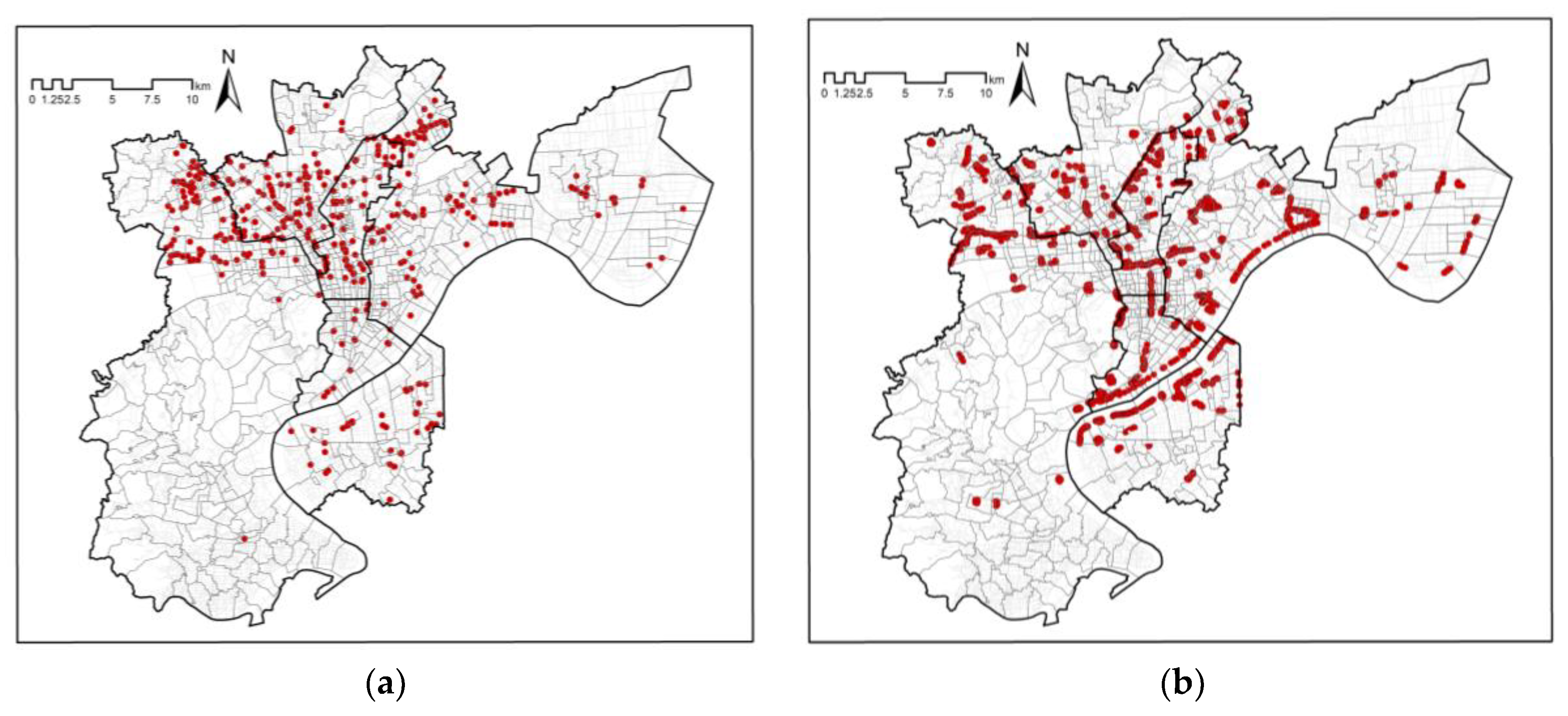
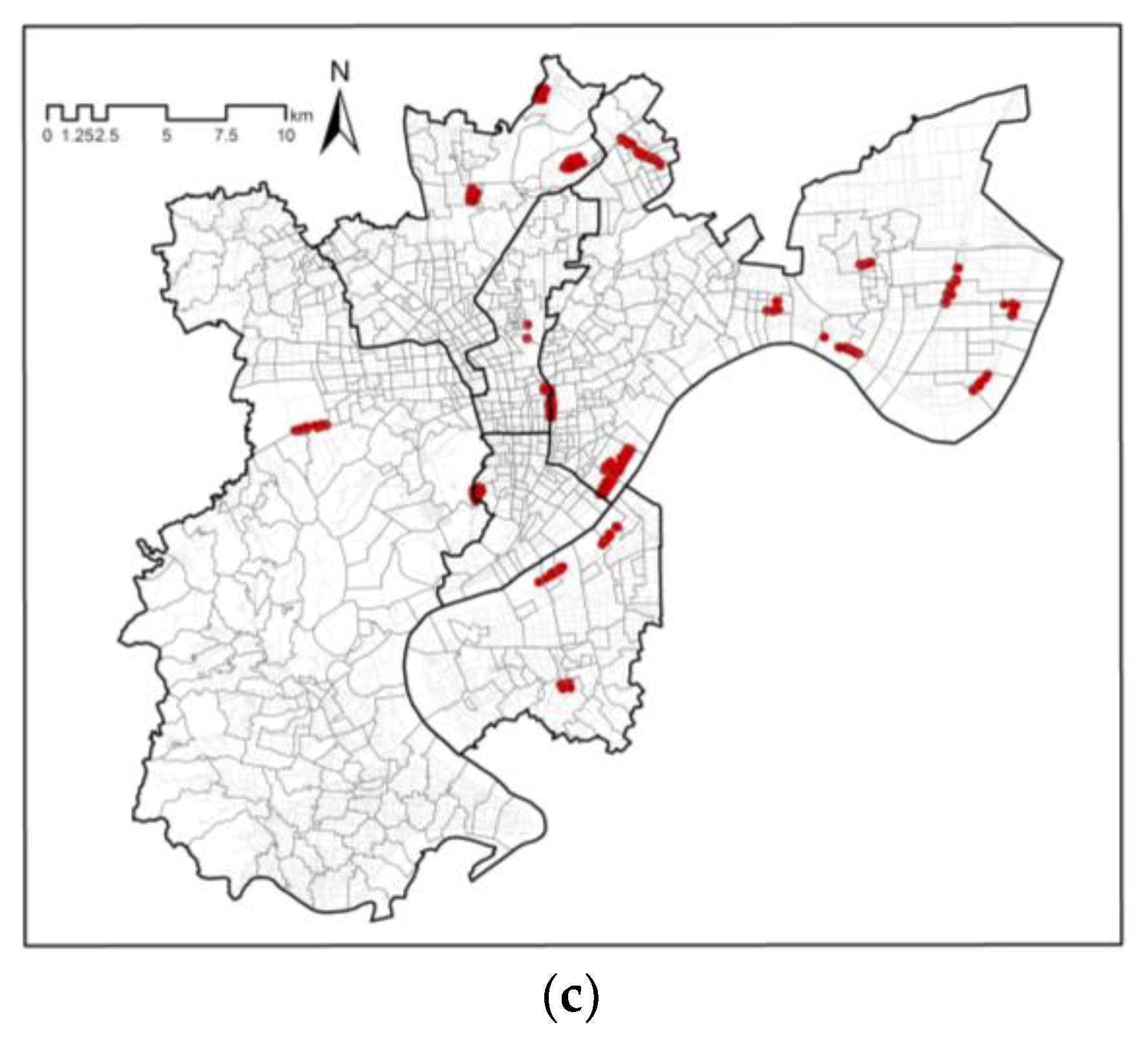
Figure 11.
Distribution map of park green space facilities in the study area. (a) 5-min life circle level, (b) 10-min life circle level, (c) 15-min life circle level.
Figure 11.
Distribution map of park green space facilities in the study area. (a) 5-min life circle level, (b) 10-min life circle level, (c) 15-min life circle level.
Figure 12.
Distribution map of sports facilities in the study area. (a) 5-min life circle level, (b) 10-min life circle level, (c) 15-min life circle level.
Figure 12.
Distribution map of sports facilities in the study area. (a) 5-min life circle level, (b) 10-min life circle level, (c) 15-min life circle level.
Figure 13.
Distribution of cultural service facilities in the study area. (a) 5-min life circle level, (b) 15-min life circle level.
Figure 13.
Distribution of cultural service facilities in the study area. (a) 5-min life circle level, (b) 15-min life circle level.
Figure 14.
Spatial distribution map of the accessibility evaluation of medical and health facilities at each life circle level. (a) 5-min life circle level, (b) 10-min life circle level, (c) 15-min life circle level, (d) Comprehensive community life circle level.
Figure 14.
Spatial distribution map of the accessibility evaluation of medical and health facilities at each life circle level. (a) 5-min life circle level, (b) 10-min life circle level, (c) 15-min life circle level, (d) Comprehensive community life circle level.
Figure 15.
Spatial distribution map of the accessibility evaluation of elderly public service facilities at each life circle level. (a) 5-min life circle level, (b) 10-min life circle level, (c) 15-min life circle level, (d) Comprehensive community life circle level.
Figure 15.
Spatial distribution map of the accessibility evaluation of elderly public service facilities at each life circle level. (a) 5-min life circle level, (b) 10-min life circle level, (c) 15-min life circle level, (d) Comprehensive community life circle level.
Figure 16.
Spatial distribution map of the accessibility evaluation of park facilities at each life circle level. (a) 5-min life circle level, (b) 10-min life circle level, (c) 15-min life circle level, (d) Comprehensive community life circle level.
Figure 16.
Spatial distribution map of the accessibility evaluation of park facilities at each life circle level. (a) 5-min life circle level, (b) 10-min life circle level, (c) 15-min life circle level, (d) Comprehensive community life circle level.
Figure 17.
Spatial distribution map of the accessibility evaluation of sports facilities at each life circle level. (a) 5-min life circle level, (b) 10-min life circle level, (c) 15-min life circle level, (d) Comprehensive community life circle level.
Figure 17.
Spatial distribution map of the accessibility evaluation of sports facilities at each life circle level. (a) 5-min life circle level, (b) 10-min life circle level, (c) 15-min life circle level, (d) Comprehensive community life circle level.
Figure 18.
Spatial distribution map of accessibility evaluation of cultural facilities at each life circle level. (a) 5-min life circle level, (b) 15-min life circle level, (c) Comprehensive community life circle level.
Figure 18.
Spatial distribution map of accessibility evaluation of cultural facilities at each life circle level. (a) 5-min life circle level, (b) 15-min life circle level, (c) Comprehensive community life circle level.
Figure 19.
The spatial distribution of facility layout comprehensive evaluation. (a) “Health Care for the Elderly”, (b) “Providing for the Elderly”, (c) “Achieving for the Elderly”.
Figure 19.
The spatial distribution of facility layout comprehensive evaluation. (a) “Health Care for the Elderly”, (b) “Providing for the Elderly”, (c) “Achieving for the Elderly”.
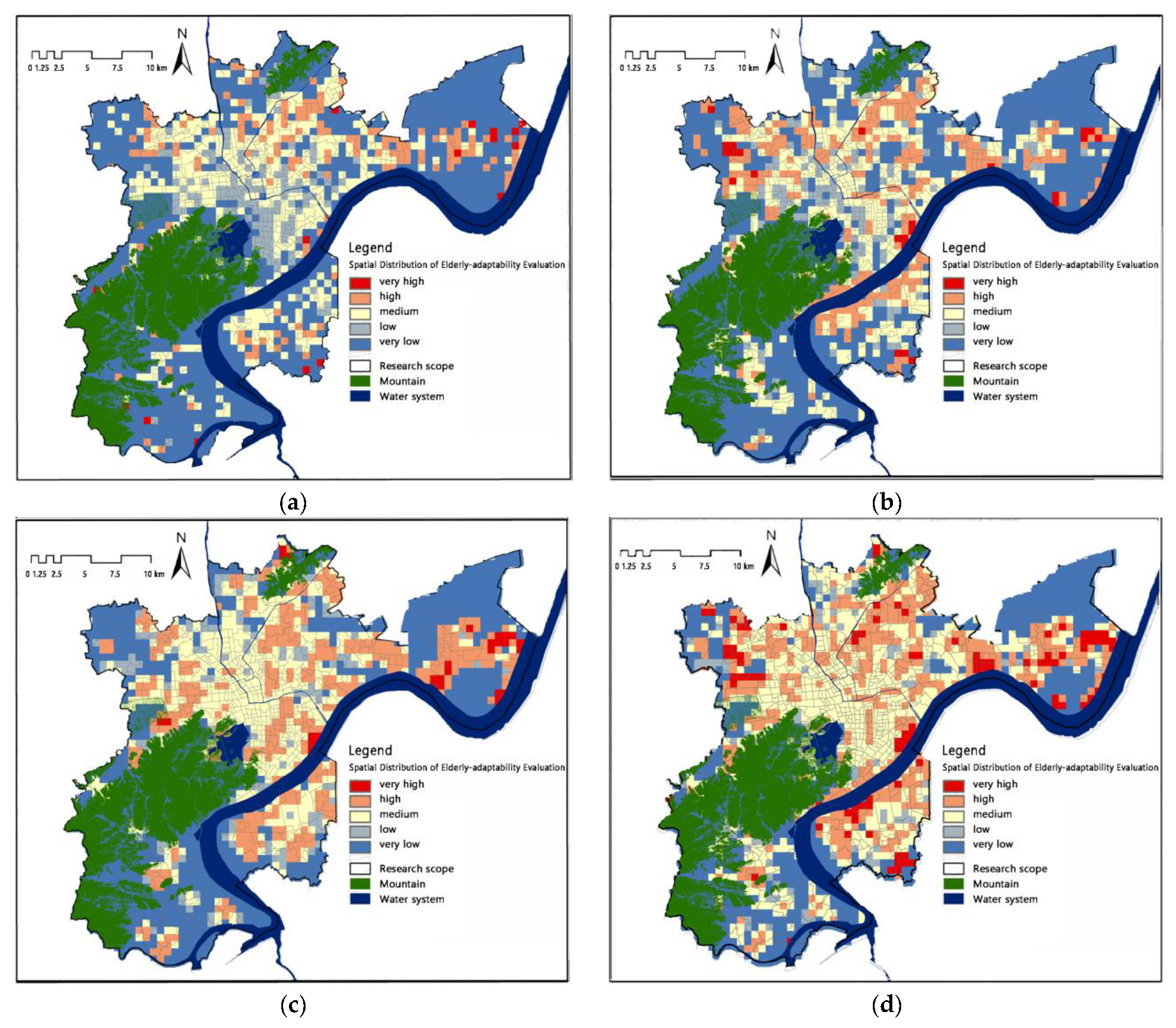
Figure 20.
Spatial distribution of the elderly-adaptability evaluation. (a) 5-min life circle, (b) 10-min life circle, (c) 15-min life circle, (d) Comprehensive evaluation of community life circle.
Figure 20.
Spatial distribution of the elderly-adaptability evaluation. (a) 5-min life circle, (b) 10-min life circle, (c) 15-min life circle, (d) Comprehensive evaluation of community life circle.
Figure 21.
Comparison of elderly-adaptability evaluation results and satisfaction evaluation.
Figure 21.
Comparison of elderly-adaptability evaluation results and satisfaction evaluation.
Figure 22.
Diagram of supply and demand differential pattern.
Figure 22.
Diagram of supply and demand differential pattern.
Figure 23.
Spatial distribution of demand and supply matching patterns.
Figure 23.
Spatial distribution of demand and supply matching patterns.
Table 1.
Summary of the research focus of “Health Equity”.
Table 1.
Summary of the research focus of “Health Equity”.
| Study Classification | Research Focus |
|---|
| Age-friendly design | Architectural design, public spaces, public facility structures, etc. |
| Age-friendly community | Public service facilities, community internal environment, road traffic planning, settlement conditions, etc. |
| Age-friendly city | Ecological environment, material living environment, spiritual and cultural environment, healthy environment, etc. |
Table 2.
Public service facilities related to the health of the elderly and the corresponding life circle levels.
Table 2.
Public service facilities related to the health of the elderly and the corresponding life circle levels.
| The Demands of the Elderly | Category | Subclass | Life Circle Level |
|---|
| Health Care for the Elderly | Medical and Health Facilities | Community health service centers, outpatient departments | 15-min |
| Clinics | 10-min |
| Community health service stations, pharmacies | 5-min |
| Providing for the Elderly | Elderly Public Service Facilities | Nursing institutions, nursing homes (200–500 beds) | 15-min |
| Home care service centers, Starlight Home for the Elderly (5–200 beds) | 10-min |
| Community canteen for the elderly | 5-min |
| Achieving for the Elderly | Sports Facilities | Comprehensive gymnasiums, fitness centers | 15-min |
| Medium-sized sports pitches (including a variety of pitches) | 10-min |
| Outdoor fitness points, chess and card rooms | 5-min |
| Park Facilities | Large park green spaces (integrated parks) (5–10 ha) | 15-min |
| Medium-sized parkland (community parks) (1–5 ha) | 10-min |
| Small park green spaces (community amusement parks) (0.4–1 ha) | 5-min |
| Cultural Facilities | Community cultural activity centers | 15-min |
| Community cultural activity stations (library, activity room) | 5-min |
Table 3.
Weight coefficient table of the importance of health public service facilities.
Table 3.
Weight coefficient table of the importance of health public service facilities.
| Category | Weight
Coefficient | Subcategories | Importance | Weight
Coefficient | Normalized Weight |
|---|
| Medical and Health Facilities | 0.23 | Community health service centers, outpatient departments | 3.90 | 0.58 | 0.13 |
| Clinics | 2.40 | 0.11 | 0.03 |
| Community health service stations, pharmacies | 3.50 | 0.31 | 0.07 |
| Elderly Public Service Facilities | 0.15 | Nursing institutions, nursing homes (200–500 beds) | 2.30 | 0.10 | 0.01 |
| Home care service centers, Starlight Home for the Elderly (5–200 beds) | 3.30 | 0.60 | 0.09 |
| Community canteens for the elderly | 2.50 | 0.30 | 0.04 |
| Sports Facilities | 0.10 | Comprehensive gymnasiums, fitness centers | 2.10 | 0.08 | 0.01 |
| Medium-sized sports pitches (including a variety of pitches) | 2.20 | 0.15 | 0.02 |
| Outdoor fitness points, chess and card rooms | 3.00 | 0.77 | 0.08 |
| Park Facilities | 0.46 | Large park green spaces (integrated parks) (5–10 ha) | 3.00 | 0.16 | 0.08 |
| Medium-sized parkland (community parks) (1–5 ha) | 3.80 | 0.54 | 0.25 |
| Small park green space (community amusement parks) (0.4–1 ha) | 3.40 | 0.30 | 0.14 |
| Cultural Facilities | 0.05 | Community cultural activity centers | 2.80 | 0.80 | 0.04 |
| Community cultural activity stations (library, activity room) | 2.00 | 0.20 | 0.01 |
Table 4.
Accessibility statistics of medical and health facilities by level of life circle.
Table 4.
Accessibility statistics of medical and health facilities by level of life circle.
| Medical and Health Facilities | Very High Reachability Cells (pcs) | Percentage (%) | Higher Accessibility Cells (pcs) | Percentage (%) | Highly Accessible Cells (pcs) |
|---|
| 5-min life circle (community health service station, pharmacy) | 27 | 1.3 | 263 | 12.7 | 14 |
| 10-min life circle (clinic) | 54 | 2.6 | 86 | 4.1 | 6.7 |
| 15-min life circle (community health service center, outpatient department) | 19 | 0.9 | 136 | 6.6 | 7.5 |
| Integrated community life circle | 34 | 1.6 | 301 | 14.5 | 16.1 |
Table 5.
Accessibility statistics for elderly public service facilities at each life circle level.
Table 5.
Accessibility statistics for elderly public service facilities at each life circle level.
| Elderly Public Service Facilities | Very High Reachability Cells (pcs) | Percentage (%) | Higher Accessibility Cells (pcs) | Percentage (%) | Highly Accessible Cells (pcs) |
|---|
| 5-min life circle (community senior cafeteria) | 7 | 0.3 | 6 | 0.3 | 0.6 |
| 10-min life circle (5–200 bed home care service center) | 6 | 0.3 | 108 | 5.2 | 5.5 |
| 15-min life circle (200–500 bed elderly care institution) | 13 | 0.6 | 44 | 2.1 | 2.7 |
| Integrated community life circle | 6 | 0.3 | 110 | 5.3 | 5.6 |
Table 6.
Accessibility statistics of park facilities at each life circle level.
Table 6.
Accessibility statistics of park facilities at each life circle level.
| Park Facilities | Very High Reachability Cells (pcs) | Percentage (%) | Higher Accessibility Cells (pcs) | Percentage (%) | Highly Accessible Cells (pcs) |
|---|
| 5-min life circle (small green space) | 10 | 0.5 | 75 | 3.6 | 4.1 |
| 10-min life circle (medium-sized green space) | 25 | 1.2 | 275 | 13.3 | 14.5 |
| 15-min life circle (large green space) | 27 | 1.2 | 107 | 5.1 | 6.4 |
| Integrated community life circle | 26 | 1.3 | 282 | 13.6 | 14.9 |
Table 7.
Accessibility statistics of sports facilities by level of life circle.
Table 7.
Accessibility statistics of sports facilities by level of life circle.
| Sports Facilities | Very High Reachability Cells (pcs) | Percentage (%) | Higher Accessibility Cells (pcs) | Percentage (%) | Highly Accessible Cells (pcs) |
|---|
| 5-min life circle (outdoor fitness spots, small activity venues) | 6 | 0.3 | 74 | 3.6 | 3.9 |
| 10-min life circle (medium-sized sports activity sites) | 17 | 0.8 | 86 | 4.1 | 4.9 |
| 15-min life circle (comprehensive gymnasium, national fitness center) | 10 | 0.5 | 123 | 5.9 | 6.4 |
| Integrated community life circle | 14 | 0.7 | 269 | 13 | 13.7 |
Table 8.
Accessibility statistics of cultural facilities by life circle level.
Table 8.
Accessibility statistics of cultural facilities by life circle level.
| Cultural Facilities | Very High Reachability Cells (pcs) | Percentage (%) | Higher Accessibility Cells (pcs) | Percentage (%) | Highly Accessible Cells (pcs) |
|---|
| 5-min life circle (community cultural activity station (library, activity room)) | 6 | 0.3 | 23 | 1.1 | 1.4 |
| 15-min life circle (community cultural activity center) | 20 | 1 | 288 | 13.9 | 14.9 |
| Integrated community life circle | 24 | 1.2 | 302 | 14.6 | 15.8 |
Table 9.
“Health Care for the Elderly” evaluation of the suitability of the layout of facilities.
Table 9.
“Health Care for the Elderly” evaluation of the suitability of the layout of facilities.
| “Health Care for the Elderly” Evaluation of the Suitability of the Layout of Facilities | Very High Values | High Values | Medium Value | Low Value | Very Low Value |
|---|
| Population cell (pcs) | 34 | 301 | 417 | 112 | 1209 |
| Percentage of population cells (%) | 1.6 | 14.5 | 20.1 | 5.4 | 58.3 |
Table 10.
“Providing for the Elderly” evaluation of the suitability of the layout of facilities.
Table 10.
“Providing for the Elderly” evaluation of the suitability of the layout of facilities.
| “Providing for the Elderly” Evaluation of the Suitability of the Layout of Facilities | Very High Values | High Values | Medium Value | Low Value | Very Low Value |
|---|
| Population cell (pcs) | 6 | 110 | 226 | 37 | 1694 |
| Percentage of population cells (%) | 0.3 | 5.3 | 10.6 | 1.8 | 81.7 |
Table 11.
Evaluation results of the layout of facilities for the elderly.
Table 11.
Evaluation results of the layout of facilities for the elderly.
| “Achieving for the Elderly” Evaluation of the Suitability of the Layout of Facilities | Very High Values | High Values | Medium Value | Low Value | Very Low Value |
|---|
| Population cell (pcs) | 31 | 362 | 409 | 232 | 1039 |
| Percentage of population cells (%) | 1.5 | 17.5 | 19.8 | 11.2 | 50.1 |
Table 12.
5-min life circle elderly-adaptability evaluation results.
Table 12.
5-min life circle elderly-adaptability evaluation results.
| 5-Minute Life Circle Elderly-Adaptability Evaluation | Very High
Values | High Values | Medium Value | Low
Value | Very Low Value |
|---|
| Population cell (pcs) | 18 | 165 | 370 | 129 | 1391 |
| Percentage of population cells (%) | 0.9 | 8 | 17.8 | 6.2 | 67.1 |
Table 13.
10-min life circle elderly-adaptability evaluation results.
Table 13.
10-min life circle elderly-adaptability evaluation results.
| 10-Minute Life Circle Elderly-Adaptability Evaluation | Very High Values | High Values | Medium Value | Low Value | Very Low Value |
|---|
| Population cell (pcs) | 26 | 302 | 396 | 127 | 1222 |
| Percentage of population cells (%) | 1.3 | 14.6 | 19.1 | 6.1 | 58.9 |
Table 14.
15-min life circle elderly-adaptability evaluation results.
Table 14.
15-min life circle elderly-adaptability evaluation results.
| 15-Minute Life Circle Elderly-Adaptability Evaluation | Very High Values | High Values | Medium Value | Low
Value | Very Low Value |
|---|
| Population cell (pcs) | 36 | 405 | 418 | 147 | 1067 |
| Percentage of population cells (%) | 1.8 | 19.5 | 20.7 | 7.1 | 51.5 |
Table 15.
Results of comprehensive elderly-adaptability evaluation of the community life circle.
Table 15.
Results of comprehensive elderly-adaptability evaluation of the community life circle.
| Community Life Circle Elderly-Adaptability Evaluation | Very
High
Values | High Values | Medium Value | Low Value | Very Low Value |
|---|
| Population cell (pcs) | 106 | 444 | 553 | 44 | 926 |
| Percentage of population cells (%) | 5.1 | 21.4 | 26.7 | 2.1 | 44.7 |
Table 16.
Quantity statistics of different supply and demand matching patterns.
Table 16.
Quantity statistics of different supply and demand matching patterns.
| Supply and Demand Matching Patterns | Population Cell (pcs) | Percentage of Population Cells (%) |
|---|
| Balance between supply and demand (high demand-high supply) | 197 | 9.5 |
| Lack of supply (high demand-low supply) | 304 | 14.7 |
| Demand gap (low demand-high supply) | 352 | 17 |
| Low supply and demand (low demand-low supply) | 1219 | 58.8 |




























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}