

Evaporation Affects the In Vitro Deposition of Nebulized Droplet in an Idealized Mouth-Throat Model
Abstract
:1. Introduction
2. Methods
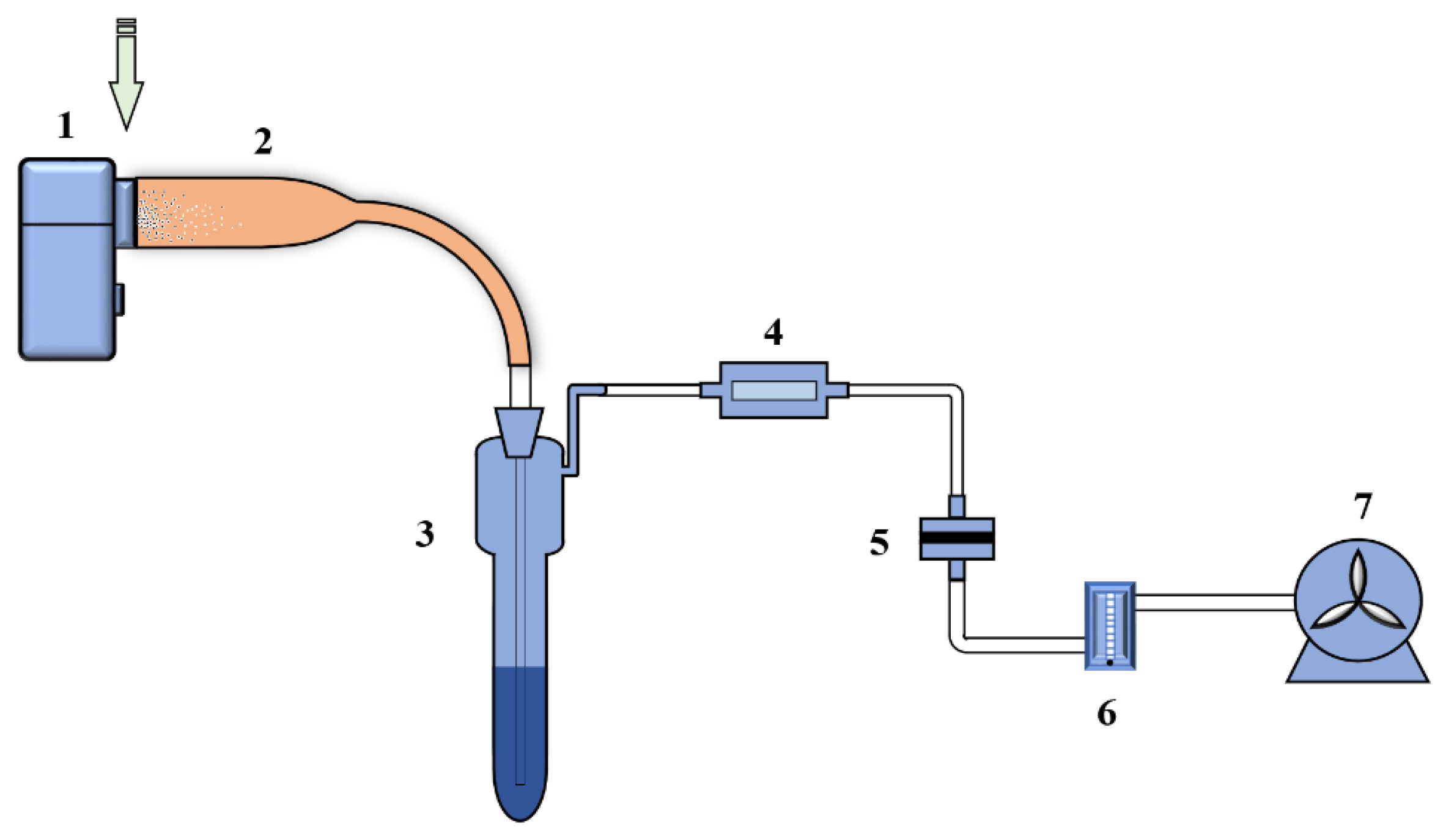
2.1. Experimental Environment and Setup
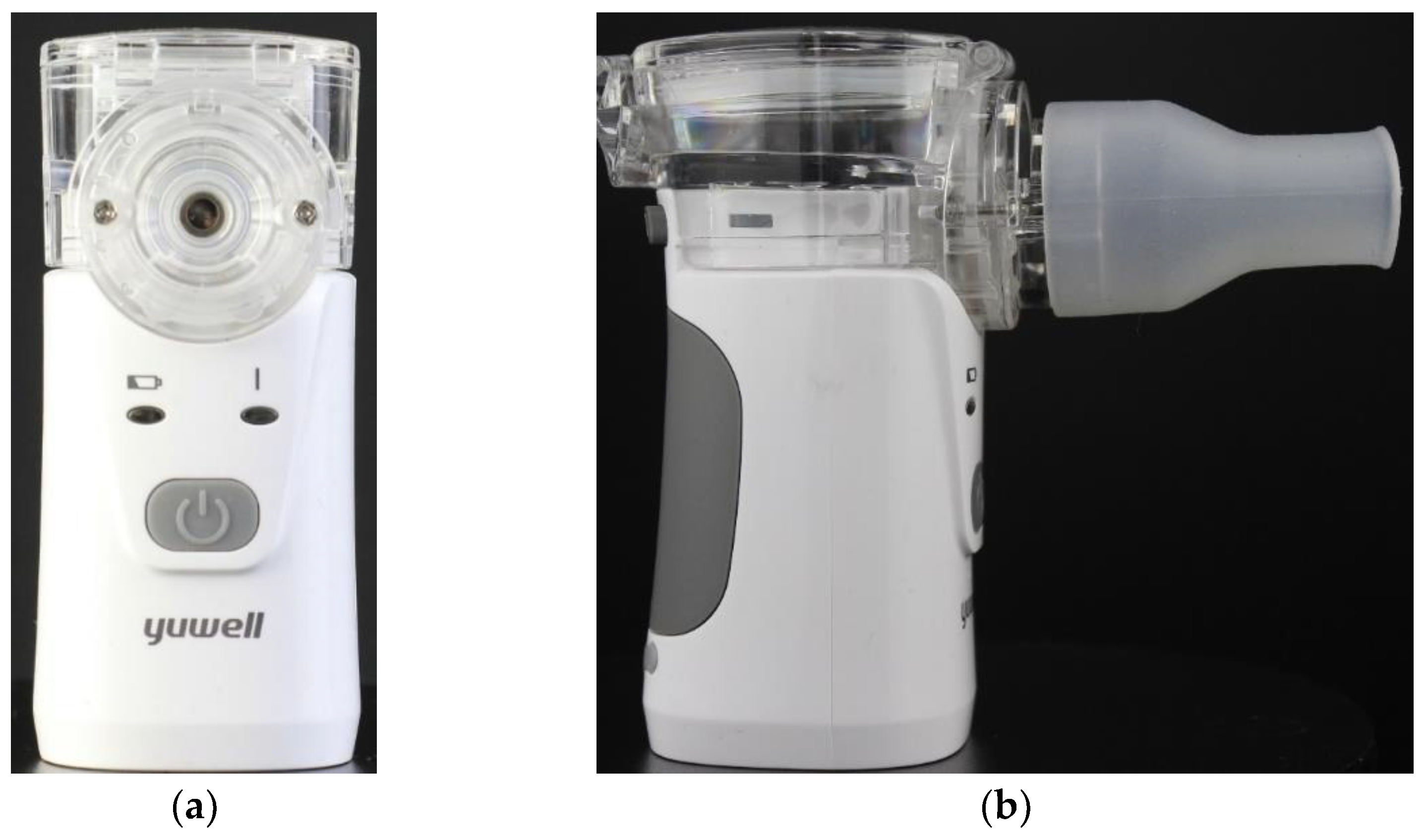
2.2. Vibrating Mesh Nebulizer (VMN)
2.3. Idealized MT Airway Model
2.4. In Vitro Nebulization Test
2.5. DF
3. Results and Discussion
3.1. Effect of Inhalation Flow Rate
3.2. Effect of NaCl Solution Concentration
4. Conclusions
- The DF of nebulized droplets first decreases with the increase in inhalation flow rate and then increases with the inhalation flow rate again. This deposition characteristic significantly differs from the experiments for solid particles or DEHS droplets;
- The high DF of VMN nebulized droplets at 15 L/min is caused by the humidification of inhaled air due to droplet evaporation. The increase in air RH handicaps the droplet evaporation, if the RH is higher than the threshold for the hygroscopic growth of NaCl;
- Droplets nebulized from a solution with a higher NaCl concentration have a higher DF in the MT airway.
Limitations and Future Work
- Nebulization rate of VMN, which may change the water vapor transfer between the droplets and surrounding air;
- Structure of VMN air inlet, which may change the trajectory of droplet;
- A realistic inhalation waveform instead of a steady inhalation flow rate, which may change the DF and deposition pattern of the droplets;
- Environmental temperature and humidity may also change the water vapor transfer between the droplets and air.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arpinelli, F.; Carone, M.; Riccardo, G.; Bertolotti, G. Health-related quality of life measurement in asthma and chronic obstructive pulmonary disease: Review of the 2009–2014 literature. Multidiscip. Respir. Med. 2016, 11, 1–7. [Google Scholar] [CrossRef]
- WHO. 10 Facts on Asthma. Available online: https://www.who.int/features/factfiles/asthma/en/ (accessed on 4 January 2022).
- WHO. Chronic Respiratory Diseases-Burden of COPD. Available online: https://www.who.int/respiratory/copd/burden/en/ (accessed on 4 January 2022).
- Ehrmann, S. Vibrating mesh nebulisers–can greater drug delivery to the airways and lungs improve respiratory outcomes. Eur. Respir. Pulmon. Dis. 2018, 4, 33–43. [Google Scholar] [CrossRef]
- Dhand, R.; Dolovich, M.; Chipps, B.R.; Myers, T.; Restrepo, R.; Rosen Farrar, J. The role of nebulized therapy in the management of COPD: Evidence and recommendations. COPD J. Chronic Obstr. Pulm. Dis. 2012, 9, 58–72. [Google Scholar] [CrossRef] [PubMed]
- Di Cristo, L.; Maguire, C.M.; Mc Quillan, K.; Aleardi, M.; Volkov, Y.; Movia, D.; Prina-Mello, A. Towards the identification of an in vitro tool for assessing the biological behavior of aerosol supplied nanomaterials. Int. J. Environ. Res. Public Health 2018, 15, 563. [Google Scholar] [CrossRef] [Green Version]
- Wu, S.; Huang, J.; Zhang, Z.; Wu, J.; Zhang, J.; Hu, H.; Zhu, T.; Zhang, J.; Luo, L.; Fan, P. Safety, tolerability, and immunogenicity of an aerosolised adenovirus type-5 vector-based COVID-19 vaccine (Ad5-nCoV) in adults: Preliminary report of an open-label and randomised phase 1 clinical trial. Lancet Infect. Dis. 2021, 21, 1654–1664. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.S.; Paul, G.; Ong, H.X.; Young, P.M.; Gu, Y.T.; Saha, S.C. A review of respiratory anatomical development, air flow characterization and particle deposition. Int. J. Environ. Res. Public Health 2020, 17, 380. [Google Scholar] [CrossRef] [Green Version]
- Singh, P.; Raghav, V.; Padhmashali, V.; Paul, G.; Islam, M.S.; Saha, S.C. Airflow and particle transport prediction through stenosis airways. Int. J. Environ. Res. Public Health 2020, 17, 1119. [Google Scholar] [CrossRef] [Green Version]
- Islam, M.S.; Larpruenrudee, P.; Hossain, S.I.; Rahimi-Gorji, M.; Gu, Y.; Saha, S.C.; Paul, G. Polydisperse aerosol transport and deposition in upper airways of age-specific lung. Int. J. Environ. Res. Public Health 2021, 18, 6239. [Google Scholar] [CrossRef]
- Choi, J.; Tawhai, M.H.; Hoffman, E.A.; Lin, C.-L. On intra-and intersubject variabilities of airflow in the human lungs. Phys. Fluids 2009, 21, 101901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, Y.; Dong, J.; Tian, L.; Inthavong, K.; Tu, J. Numerical and experimental analysis of inhalation airflow dynamics in a human pharyngeal airway. Int. J. Environ. Res. Public Health 2020, 17, 1556. [Google Scholar] [CrossRef]
- Zhang, Z.; Kleinstreuer, C. Transient airflow structures and particle transport in a sequentially branching lung airway model. Phys. Fluids 2002, 14, 862–880. [Google Scholar] [CrossRef]
- Kleinstreuer, C.; Zhang, Z. Airflow and particle transport in the human respiratory system. Annu. Rev. Fluid Mech. 2010, 42, 301–334. [Google Scholar] [CrossRef]
- Grgic, B.; Finlay, W.; Heenan, A. Regional aerosol deposition and flow measurements in an idealized mouth and throat. J. Aerosol Sci. 2004, 35, 21–32. [Google Scholar] [CrossRef]
- Golshahi, L.; Noga, M.L.; Finlay, W.H. Deposition of inhaled micrometer-sized particles in oropharyngeal airway replicas of children at constant flow rates. J. Aerosol Sci. 2012, 49, 21–31. [Google Scholar] [CrossRef]
- Xi, J.; Wang, Z.; Si, X.A.; Zhou, Y. Nasal dilation effects on olfactory deposition in unilateral and bi-directional deliveries: In vitro tests and numerical modeling. Eur. J. Pharm. Sci. 2018, 118, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Kleinstreuer, C.; Kim, C. Micro-particle transport and deposition in a human oral airway model. J. Aerosol Sci. 2002, 33, 1635–1652. [Google Scholar] [CrossRef]
- Feng, Y.; Zhao, J.; Hayati, H.; Sperry, T.; Yi, H. Tutorial: Understanding the transport, deposition, and translocation of particles in human respiratory systems using Computational Fluid-Particle Dynamics and Physiologically Based Toxicokinetic models. J. Aerosol Sci. 2021, 151, 105672. [Google Scholar] [CrossRef]
- Waldrep, J.; Dhand, R. Advanced nebulizer designs employing vibrating mesh/aperture plate technologies for aerosol generation. Curr. Drug Deliv. 2008, 5, 114–119. [Google Scholar] [CrossRef]
- Galindo-Filho, V.C.; Ramos, M.E.; Rattes, C.S.; Barbosa, A.K.; Brandão, D.C.; Brandão, S.C.S.; Fink, J.B.; de Andrade, A.D. Radioaerosol pulmonary deposition using mesh and jet nebulizers during noninvasive ventilation in healthy subjects. Respir. Care. 2015, 60, 1238–1246. [Google Scholar] [CrossRef] [Green Version]
- Dugernier, J.; Hesse, M.; Vanbever, R.; Depoortere, V.; Roeseler, J.; Michotte, J.-B.; Laterre, P.-F.; Jamar, F.; Reychler, G. SPECT-CT comparison of lung deposition using a system combining a vibrating-mesh nebulizer with a valved holding chamber and a conventional jet nebulizer: A randomized cross-over study. Pharm. Res. 2017, 34, 290–300. [Google Scholar] [CrossRef]
- Pitance, L.; Vecellio, L.; Leal, T.; Reychler, G.; Reychler, H.; Liistro, G. Delivery efficacy of a vibrating mesh nebulizer and a jet nebulizer under different configurations. J. Aerosol Med. Pulm. Deliv. 2010, 23, 389–396. [Google Scholar] [CrossRef]
- Rezaei, M.; Netz, R.R. Water evaporation from solute-containing aerosol droplets: Effects of internal concentration and diffusivity profiles and onset of crust formation. Phys. Fluids 2021, 33, 091901. [Google Scholar] [CrossRef]
- Sasaki, Y.; Hasegawa, K.; Kaneko, A.; Abe, Y. Heat and mass transfer characteristics of binary droplets in acoustic levitation. Phys. Fluids 2020, 32, 072102. [Google Scholar] [CrossRef]
- Zeng, G.; Chen, L.; Yuan, H.; Yamamoto, A.; Maruyama, S. Evaporation flow characteristics of airborne sputum droplets with solid fraction: Effects of humidity field evolutions. Phys. Fluids 2021, 33, 123308. [Google Scholar] [CrossRef]
- Dbouk, T.; Drikakis, D. On coughing and airborne droplet transmission to humans. Phys. Fluids 2020, 32, 053310. [Google Scholar] [CrossRef] [PubMed]
- Ju, W.; Wu, Y.; Lin, S.; Zhao, F.; Tan, S. Visual experimental study of droplet impinging on liquid film and analysis of droplet evolution characteristics. Exp. Comput. Multiph. Flow 2020, 4, 212–220. [Google Scholar] [CrossRef]
- Wang, Q.; Wang, Z.; Jiang, Y.; Yang, S. Experimental study of electro-spraying modes of deionized water in atmospheric environment. Exp. Comput. Multiph. Flow 2019, 3, 38–46. [Google Scholar] [CrossRef] [Green Version]
- Finlay, W.H. The Mechanics of Inhaled Pharmaceutical Aerosols: An Introduction; Academic Press: New York, NY, USA, 2001. [Google Scholar]
- Zhang, Z.; Kleinstreuer, C.; Kim, C.S. Isotonic and hypertonic saline droplet deposition in a human upper airway model. J. Aerosol Med. 2006, 19, 184–198. [Google Scholar] [CrossRef]
- Zhang, Z.; Kim, C.S.; Kleinstreuer, C. Water vapor transport and its effects on the deposition of hygroscopic droplets in a human upper airway model. Aerosol Sci. Technol. 2006, 40, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Feng, Y.; Zhong, W.; Kleinstreuer, C. Numerical investigation of the interaction, transport and deposition of multicomponent droplets in a simple mouth-throat model. J. Aerosol Sci. 2017, 105, 108–127. [Google Scholar] [CrossRef]
- Tu, H.; Ray, A.K. Measurement of activity coefficients from unsteady state evaporation and growth of microdroplets. Chem. Eng. Commun. 2005, 192, 474–498. [Google Scholar] [CrossRef]
- Chen, X.; Kleinstreuer, C.; Zhong, W.; Feng, Y.; Zhou, X. Effects of thermal airflow and mucus-layer interaction on hygroscopic droplet deposition in a simple mouth–throat model. Aerosol Sci. Technol. 2018, 52, 900–912. [Google Scholar] [CrossRef]
- Wu, D.; Tawhai, M.H.; Hoffman, E.A.; Lin, C.-L. A numerical study of heat and water vapor transfer in MDCT-based human airway models. Ann. Biomed. Eng. 2014, 42, 2117–2131. [Google Scholar] [CrossRef] [Green Version]
- Rajaraman, P.K.; Choi, J.; Hoffman, E.A.; O’Shaughnessy, P.T.; Choi, S.; Delvadia, R.; Babiskin, A.; Walenga, R.; Lin, C.-L. Transport and deposition of hygroscopic particles in asthmatic subjects with and without airway narrowing. J. Aerosol Sci. 2020, 146, 105581. [Google Scholar] [CrossRef]
- Xu, C.; Zheng, X.; Shen, S. A numerical study of the effects of ambient temperature and humidity on the particle growth and deposition in the human airway. Environ. Res. 2021, 200, 111751. [Google Scholar] [CrossRef]
- Winkler-Heil, R.; Pichelstorfer, L.; Hofmann, W. Aerosol dynamics model for the simulation of hygroscopic growth and deposition of inhaled NaCl particles in the human respiratory tract. J. Aerosol Sci. 2017, 113, 212–226. [Google Scholar] [CrossRef]
- Wickert, D.; Prokop, G. Simulation of water evaporation under natural conditions—A state-of-the-art overview. Exp. Comput. Multiph. Flow. 2021, 3, 242–249. [Google Scholar] [CrossRef]
- Khamooshi, M.; Fletcher, D.F.; Salati, H.; Vahaji, S.; Gregory, S.; Inthavong, K. Computational assessment of the nasal air conditioning and paranasal sinus ventilation from nasal assisted breathing therapy. Phys. Fluids 2022, 34, 051912. [Google Scholar] [CrossRef]
- Zhang, Y.; Finlay, W.; Matida, E. Particle deposition measurements and numerical simulation in a highly idealized mouth–throat. J. Aerosol Sci. 2004, 35, 789–803. [Google Scholar] [CrossRef]
- Zhang, Y.; Chia, T.L.; Finlay, W.H. Experimental measurement and numerical study of particle deposition in highly idealized mouth-throat models. Aerosol Sci. Technol. 2006, 40, 361–372. [Google Scholar] [CrossRef]
- Kleinstreuer, C.; Zhang, Z.; Li, Z. Modeling airflow and particle transport/deposition in pulmonary airways. Resp. Physiol. Neurobiol. 2008, 163, 128–138. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Feng, Y.; Zhong, W.; Sun, B.; Tao, F. Numerical investigation of particle deposition in a triple bifurcation airway due to gravitational sedimentation and inertial impaction. Powder Technol. 2018, 323, 284–293. [Google Scholar] [CrossRef]
- Tang, I.; Munkelwitz, H.; Davis, J. Aerosol growth studies—II. Preparation and growth measurements of monodisperse salt aerosols. J. Aerosol Sci. 1977, 8, 149–159. [Google Scholar] [CrossRef]
- Robinson, R.A.; Stokes, R.H. Electrolyte Solutions; Butterworth: London, UK, 1970. [Google Scholar]
- Cruz, C.N.; Pandis, S.N. Deliquescence and hygroscopic growth of mixed inorganic-organic atmospheric aerosol. Environ. Sci. Technol. 2000, 34, 4313–4319. [Google Scholar] [CrossRef]
- Zhou, Y.; Brasel, T.L.; Kracko, D.; Cheng, Y.-S.; Ahuja, A.; Norenberg, J.P.; William Kelly, H. Influence of impactor operating flow rate on particle size distribution of four jet nebulizers. Pharm. Dev. Technol. 2007, 12, 353–359. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | 0.9% NaCl Solution | 10% NaCl Solution |
|---|---|---|
| Refractive index | 1.335 | 1.351 |
| MMAD | 5.82 μm | 5.91 μm |
| Geometric standard deviation | 1.447 | 1.602 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xia, X.; Ding, T.; Chen, X.; Tao, F.; Sun, B.; Lu, T.; Wang, J.; Huang, Y.; Xu, Y. Evaporation Affects the In Vitro Deposition of Nebulized Droplet in an Idealized Mouth-Throat Model. Atmosphere 2023, 14, 93. https://doi.org/10.3390/atmos14010093
Xia X, Ding T, Chen X, Tao F, Sun B, Lu T, Wang J, Huang Y, Xu Y. Evaporation Affects the In Vitro Deposition of Nebulized Droplet in an Idealized Mouth-Throat Model. Atmosphere. 2023; 14(1):93. https://doi.org/10.3390/atmos14010093
Chicago/Turabian StyleXia, Xueying, Ting Ding, Xiaole Chen, Feng Tao, Baobin Sun, Tong Lu, Jianwei Wang, Yu Huang, and Yin Xu. 2023. "Evaporation Affects the In Vitro Deposition of Nebulized Droplet in an Idealized Mouth-Throat Model" Atmosphere 14, no. 1: 93. https://doi.org/10.3390/atmos14010093