
Associations of HLA Polymorphisms with Chronic Kidney Disease in Japanese Rheumatoid Arthritis Patients
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Controls
2.2. Genotyping
2.3. Statistical Analysis
3. Results
3.1. Clinical Characteristics of RA Patients
3.2. Association of HLA with CKD in RA Patients
3.3. PCA of the CKD(+)RA, CKD(−)RA, and Healthy Control Groups
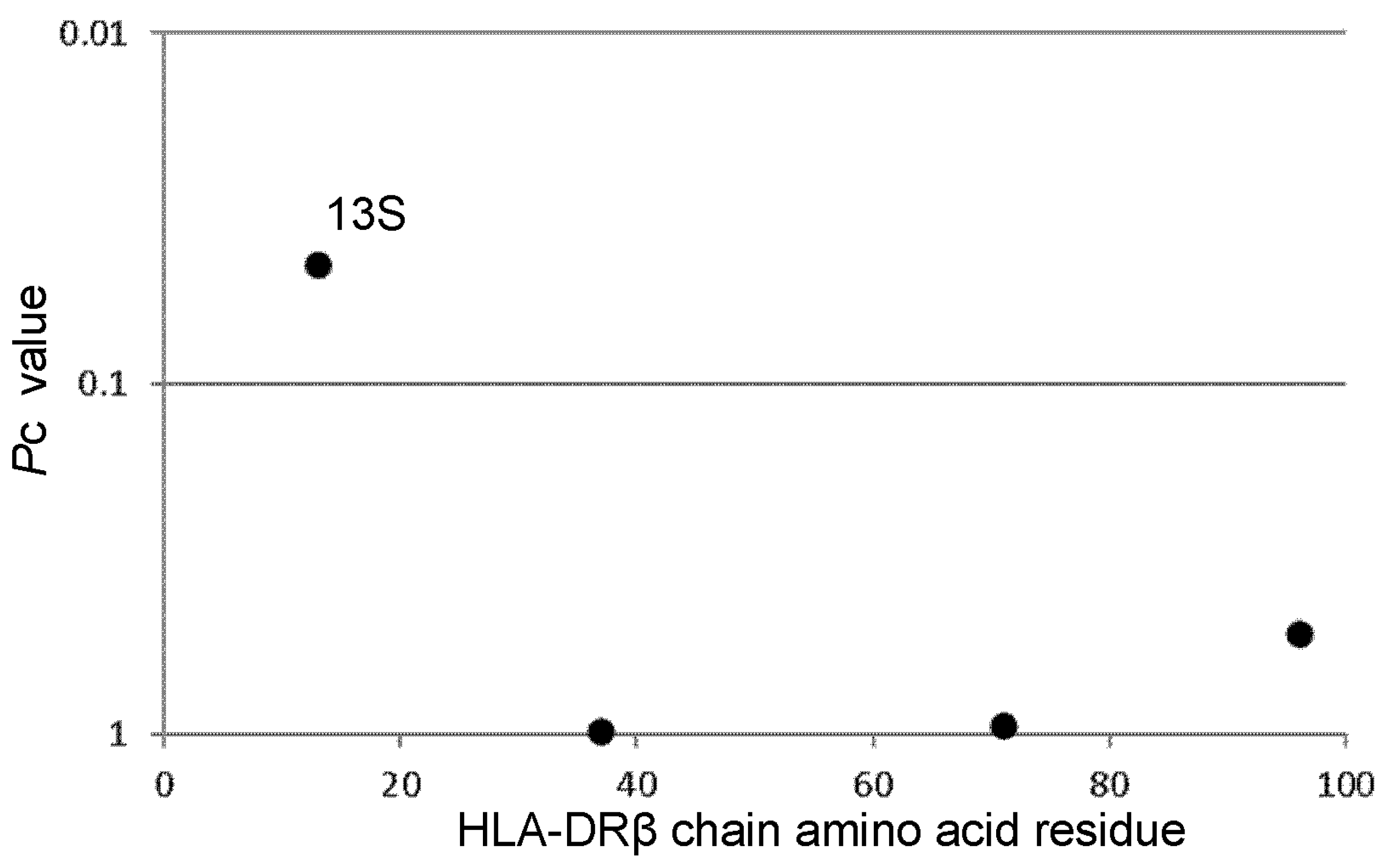
3.4. Associations of Amino Acid Residues in the DRβ Chain of RA Patients with CKD
3.5. Logistic Regression Analysis of DR6 and Clinical Characteristics of CKD
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Boers, M.; Dijkmans, B.A.; Breedveld, F.C.; Camps, J.A.; Chang, P.C.; van Brummelen, P.; Pauwels, E.K.; Cats, A. Subclinical renal dysfunction in rheumatoid arthritis. Arthritis Rheum. 1990, 33, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Koseki, Y.; Terai, C.; Moriguchi, M.; Uesato, M.; Kamatani, N. A prospective study of renal disease in patients with early rheumatoid arthritis. Ann. Rheum. Dis. 2001, 60, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Karstila, K.; Korpela, M.; Sihvonen, S.; Mustonen, J. Prognosis of clinical renal disease and incidence of new renal findings in patients with rheumatoid arthritis: Follow-up of a population-based study. Clin. Rheumatol. 2007, 26, 2089–2095. [Google Scholar] [CrossRef] [PubMed]
- Karie, S.; Gandjbakhch, F.; Janus, N.; Launay-Vacher, V.; Rozenberg, S.; Mai Ba, C.U.; Bourgeois, P.; Deray, G. Kidney disease in RA patients: Prevalence and implication on RA-related drugs management: The MATRIX study. Rheumatology 2008, 47, 350–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hill, A.J.; Thomson, R.J.; Hunter, J.A.; Traynor, J.P. The prevalence of chronic kidney disease in rheumatology outpatients. Scott. Med. J. 2009, 54, 9–12. [Google Scholar] [CrossRef]
- Hickson, L.J.; Crowson, C.S.; Gabriel, S.E.; McCarthy, J.T.; Matteson, E.L. Development of reduced kidney function in rheumatoid arthritis. Am. J. Kidney Dis. 2014, 63, 206–213. [Google Scholar] [CrossRef] [Green Version]
- Saisho, K.; Yoshikawa, N.; Sugata, K.; Hamada, H.; Tohma, S. Prevalence of chronic kidney disease and administration of RA-related drugs in patients with RA: The NinJa 2012 study in Japan. Mod. Rheumatol. 2016, 26, 331–335. [Google Scholar] [CrossRef]
- Helin, H.J.; Korpela, M.M.; Mustonen, J.T.; Pasternack, A.I. Renal biopsy findings and clinicopathologic correlations in rheumatoid arthritis. Arthritis Rheum. 1995, 38, 242–247. [Google Scholar] [CrossRef]
- Nakano, M.; Ueno, M.; Nishi, S.; Shimada, H.; Hasegawa, H.; Watanabe, T.; Kuroda, T.; Sato, T.; Maruyama, Y.; Arakawa, M. Analysis of renal pathology and drug history in 158 Japanese patients with rheumatoid arthritis. Clin. Nephrol. 1998, 50, 154–160. [Google Scholar]
- Kochi, M.; Kohagura, K.; Shiohira, Y.; Iseki, K.; Ohya, Y. Inflammation as a Risk of Developing Chronic Kidney Disease in Rheumatoid Arthritis. PLoS ONE 2016, 11, e0160225. [Google Scholar] [CrossRef]
- Sumida, K.; Molnar, M.Z.; Potukuchi, P.K.; Hassan, F.; Thomas, F.; Yamagata, K.; Kalantar-Zadeh, K.; Kovesdy, C.P. Treatment of rheumatoid arthritis with biologic agents lowers the risk of incident chronic kidney disease. Kidney Int. 2018, 93, 1207–1216. [Google Scholar] [CrossRef]
- Reveille, J.D. The genetic contribution to the pathogenesis of rheumatoid arthritis. Curr. Opin. Rheumatol. 1998, 10, 187–200. [Google Scholar] [CrossRef]
- Oka, S.; Furukawa, H.; Kawasaki, A.; Shimada, K.; Sugii, S.; Hashimoto, A.; Komiya, A.; Fukui, N.; Ito, S.; Nakamura, T.; et al. Protective effect of the HLA-DRB1*13:02 allele in Japanese rheumatoid arthritis patients. PLoS ONE 2014, 9, e99453. [Google Scholar] [CrossRef] [Green Version]
- Furukawa, H.; Oka, S.; Shimada, K.; Hashimoto, A.; Tohma, S. Human leukocyte antigen polymorphisms and personalized medicine for rheumatoid arthritis. J. Hum. Genet. 2015, 60, 691–696. [Google Scholar] [CrossRef]
- Le Pham, N.M.; Ong, T.P.; Vuong, N.L.; Van Tran, B.; Nguyen, T.T.H. HLA types and their association with end-stage renal disease in Vietnamese patients: A cross-sectional study. Medicine 2022, 101, e31856. [Google Scholar] [CrossRef]
- Lowe, M.; Jervis, S.; Payton, A.; Poulton, K.; Worthington, J.; Gemmell, I.; Verma, A. Systematic review of associations between HLA and renal function. Int. J. Immunogenet. 2022, 49, 46–62. [Google Scholar] [CrossRef]
- Arnett, F.C.; Edworthy, S.M.; Bloch, D.A.; McShane, D.J.; Fries, J.F.; Cooper, N.S.; Healey, L.A.; Kaplan, S.R.; Liang, M.H.; Luthra, H.S.; et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988, 31, 315–324. [Google Scholar] [CrossRef]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O., 3rd; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef]
- Kamatani, N.; Kawamoto, M.; Kitamura, Y.; Harigai, M.; Okumoto, T.; Sumino, Y. Establishment of B-cell lines derived from 996 Japanese individuals. Tissue Cult. Res. Commun. 2004, 23, 71–80. [Google Scholar]
- Kamitsuji, S.; Matsuda, T.; Nishimura, K.; Endo, S.; Wada, C.; Watanabe, K.; Hasegawa, K.; Hishigaki, H.; Masuda, M.; Kuwahara, Y.; et al. Japan PGx Data Science Consortium Database: SNPs and HLA genotype data from 2994 Japanese healthy individuals for pharmacogenomics studies. J. Hum. Genet. 2015, 60, 319–326. [Google Scholar] [CrossRef]
- Matsuo, S.; Imai, E.; Horio, M.; Yasuda, Y.; Tomita, K.; Nitta, K.; Yamagata, K.; Tomino, Y.; Yokoyama, H.; Hishida, A. Revised equations for estimated GFR from serum creatinine in Japan. Am. J. Kidney Dis. 2009, 53, 982–992. [Google Scholar] [CrossRef] [PubMed]
- Oka, S.; Furukawa, H.; Yasunami, M.; Kawasaki, A.; Nakamura, H.; Nakamura, M.; Komori, A.; Abiru, S.; Nagaoka, S.; Hashimoto, S.; et al. HLA-DRB1 and DQB1 alleles in Japanese type 1 autoimmune hepatitis: The predisposing role of the DR4/DR8 heterozygous genotype. PLoS ONE 2017, 12, e0187325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rousset, F. genepop’007: A complete re-implementation of the genepop software for Windows and Linux. Mol. Ecol. Resour. 2008, 8, 103–106. [Google Scholar] [CrossRef] [PubMed]
- Steinbrocker, O.; Traeger, C.H.; Batterman, R.C. Therapeutic criteria in rheumatoid arthritis. J. Am. Med. Assoc. 1949, 140, 659–662. [Google Scholar] [CrossRef]
- Oka, S.; Higuchi, T.; Furukawa, H.; Shimada, K.; Hashimoto, A.; Komiya, A.; Matsui, T.; Fukui, N.; Suematsu, E.; Ohno, S.; et al. Predisposition of HLA-DRB1*04:01/*15 heterozygous genotypes to Japanese mixed connective tissue disease. Sci. Rep. 2022, 12, 9916. [Google Scholar] [CrossRef]
- Furukawa, H.; Oka, S.; Shimada, K.; Sugii, S.; Hashimoto, A.; Komiya, A.; Fukui, N.; Miyashita, T.; Migita, K.; Suda, A.; et al. HLA-DRB1*08:02 is associated with bucillamine-induced proteinuria in Japanese rheumatoid arthritis patients. Biomark. Insights 2014, 9, 23–28. [Google Scholar] [CrossRef]


{kind=link}
| CKD(+)RA | CKD(−)RA | ||
|---|---|---|---|
| Number of patients | 351 | 959 | |
| Age, years (SD) | 73.5 (8.6) | 64.2 (12.4) | * 2.99 × 10−47 |
| Male, n (%) | 73 (20.8) | 161 (16.8) | 0.1033 |
| Disease duration, years (SD) | 17.7 (12.5) | 16.3 (11.3) | * 0.0632 |
| Steinbrocker stage III and IV, n (%) | 156 (45.3) | 418 (44.1) | 0.7043 |
| Steinbrocker class 3 and 4, n (%) | 61 (17.8) | 96 (10.1) | 0.0003 |
| Body mass index, kg/m2 (SD) | 22.3 (3.9) | 21.7 (3.5) | * 0.0171 |
| Rheumatoid factor positive, n (%) | 287 (82.0) | 766 (80.5) | 0.5782 |
| Anti-citrullinated peptide antibody positive, n (%) | 303 (86.6) | 823 (86.7) | 0.9269 |
| Serum creatinine, mg/dL (SD) | 0.96 (0.25) | 0.62 (0.12) | * 2.71 × 10−82 |
| CRP, mg/L (SD) | 4.6 (7.5) | 5.1 (11.8) | * 0.3548 |
| ESR, mm/h (SD) | 30.2 (21.0) | 26.2 (21.1) | * 0.0035 |
| DAS28 | 3.0 (1.0) | 2.8 (1.1) | * 0.0125 |
| DAS28-CRP | 2.2 (0.9) | 2.2 (0.9) | * 0.3548 |
| CKD(+)RA (n = 351) | CKD(−)RA (n = 959) | p | OR | pc | 95%CI | |
|---|---|---|---|---|---|---|
| DRB1*01:01 | 54 (15.4) | 136 (14.2) | 0.5955 | 1.10 | NS | (0.78–1.55) |
| DRB1*03:01 | 1 (0.3) | 0 (0.0) | 0.2679 | 8.21 | NS | (0.33–202.08) |
| DRB1*04:01 | 19 (5.4) | 75 (7.8) | 0.1478 | 0.67 | NS | (0.40–1.13) |
| DRB1*04:03 | 10 (2.8) | 28 (2.9) | 1.0000 | 0.98 | NS | (0.47–2.03) |
| DRB1*04:04 | 3 (0.9) | 5 (0.5) | 0.4483 | 1.64 | NS | (0.39–6.92) |
| DRB1*04:05 | 162 (46.2) | 487 (50.8) | 0.1513 | 0.83 | NS | (0.65–1.06) |
| DRB1*04:06 | 11 (3.1) | 45 (4.7) | 0.2799 | 0.66 | NS | (0.34–1.29) |
| DRB1*04:07 | 3 (0.9) | 4 (0.4) | 0.3934 | 2.06 | NS | (0.46–9.24) |
| DRB1*04:10 | 16 (4.6) | 39 (4.1) | 0.7557 | 1.13 | NS | (0.62–2.04) |
| DRB1*07:01 | 2 (0.6) | 5 (0.5) | 1.0000 | 1.09 | NS | (0.21–5.66) |
| DRB1*08:02 | 18 (5.1) | 29 (3.0) | 0.0917 | 1.73 | NS | (0.95–3.16) |
| DRB1*08:03 | 26 (7.4) | 81 (8.4) | 0.6487 | 0.87 | NS | (0.55–1.37) |
| DRB1*09:01 | 102 (29.1) | 252 (26.3) | 0.3258 | 1.15 | NS | (0.88–1.51) |
| DRB1*10:01 | 5 (1.4) | 18 (1.9) | 0.8123 | 0.76 | NS | (0.28–2.05) |
| DRB1*11:01 | 10 (2.8) | 30 (3.1) | 0.8584 | 0.91 | NS | (0.44–1.88) |
| DRB1*12:01 | 21 (6.0) | 70 (7.3) | 0.4625 | 0.81 | NS | (0.49–1.34) |
| DRB1*12:02 | 9 (2.6) | 27 (2.8) | 1.0000 | 0.91 | NS | (0.42–1.95) |
| DRB1*13:01 | 0 (0.0) | 2 (0.2) | 1.0000 | 0.54 | NS | (0.03–11.38) |
| DRB1*13:02 | 34 (9.7) | 57 (5.9) | 0.0265 | 1.70 | 0.7412 | (1.09–2.64) |
| DRB1*14:02 | 1 (0.3) | 2 (0.2) | 1.0000 | 1.37 | NS | (0.12–15.12) |
| DRB1*14:03 | 6 (1.7) | 21 (2.2) | 0.6672 | 0.78 | NS | (0.31–1.94) |
| DRB1*14:05 | 7 (2.0) | 18 (1.9) | 0.8237 | 1.06 | NS | (0.44–2.57) |
| DRB1*14:06 | 19 (5.4) | 30 (3.1) | 0.0691 | 1.77 | NS | (0.98–3.19) |
| DRB1*14:07 | 1 (0.3) | 1 (0.1) | 0.4642 | 2.74 | NS | (0.17–43.88) |
| DRB1*14:54 | 27 (7.7) | 46 (4.8) | 0.0559 | 1.65 | NS | (1.01–2.70) |
| DRB1*15:01 | 37 (10.5) | 116 (12.1) | 0.4967 | 0.86 | NS | (0.58–1.27) |
| DRB1*15:02 | 56 (16.0) | 163 (17.0) | 0.6769 | 0.93 | NS | (0.67–1.29) |
| DRB1*16:02 | 5 (1.4) | 14 (1.5) | 1.0000 | 0.98 | NS | (0.35–2.73) |
| DR6 (DRB1*13, *14) | 93 (26.5) | 172 (17.9) | 0.0008 | 1.65 | (1.24–2.20) |
| CKD(+)RA (n = 351) | CKD(−)RA (n = 959) | p | OR | 95%CI | |
|---|---|---|---|---|---|
| DR6/not DR6 | 89 (25.4) | 163 (17.0) | 0.0009 | 1.66 | (1.24–2.23) |
| DR6/DR6 | 4 (1.1) | 9 (0.9) | 0.7558 | 1.22 | (0.37–3.98) |
| Unconditioned | Conditioned on Other Clinical Manifestations | |||||
|---|---|---|---|---|---|---|
| Clinical Manifestations | OR | 95%CI | p | ORadjusted | 95%CI | padjusted |
| Age | 1.10 | (1.08–1.11) | 2.95 × 10−30 | 1.10 | (1.08–1.11) | 4.68 × 10−25 |
| Male | 1.30 | (0.96–1.77) | 0.0940 | 1.10 | (0.77–1.57) | 0.5978 |
| Disease duration | 1.01 | (1.00–1.02) | 0.0517 | 0.99 | (0.98–1.01) | 0.3772 |
| Steinbrocker class | 1.32 | (1.10–1.59) | 0.0024 | 1.24 | (1.00–1.52) | 0.0475 |
| Body mass index | 1.04 | (1.01–1.08) | 0.0126 | 1.05 | (1.01–1.09) | 0.0176 |
| ESR | 1.01 | (1.00–1.01) | 0.0040 | 1.00 | (0.99–1.01) | 0.7025 |
| DR6 | 1.55 | (1.19–2.03) | 0.0013 | 1.43 | (1.06–1.94) | 0.0196 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Higuchi, T.; Oka, S.; Furukawa, H.; Shimada, K.; Hashimoto, A.; Komiya, A.; Matsui, T.; Fukui, N.; Tohma, S. Associations of HLA Polymorphisms with Chronic Kidney Disease in Japanese Rheumatoid Arthritis Patients. Genes 2023, 14, 1470. https://doi.org/10.3390/genes14071470
Higuchi T, Oka S, Furukawa H, Shimada K, Hashimoto A, Komiya A, Matsui T, Fukui N, Tohma S. Associations of HLA Polymorphisms with Chronic Kidney Disease in Japanese Rheumatoid Arthritis Patients. Genes. 2023; 14(7):1470. https://doi.org/10.3390/genes14071470
Chicago/Turabian StyleHiguchi, Takashi, Shomi Oka, Hiroshi Furukawa, Kota Shimada, Atsushi Hashimoto, Akiko Komiya, Toshihiro Matsui, Naoshi Fukui, and Shigeto Tohma. 2023. "Associations of HLA Polymorphisms with Chronic Kidney Disease in Japanese Rheumatoid Arthritis Patients" Genes 14, no. 7: 1470. https://doi.org/10.3390/genes14071470