
Genetic Lesions in Russian CLL Patients with the Most Common Stereotyped Antigen Receptors

 and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fais, F.; Ghiotto, F.; Hashimoto, S.; Sellars, B.; Valetto, A.; Allen, S.L.; Schulman, P.; Vinciguerra, V.P.; Rai, K.; Rassenti, L.Z.; et al. Chronic lymphocytic leukemia B cells express restricted sets of mutated and unmutated antigen receptors. J. Clin. Investig. 1998, 102, 1515–1525. [Google Scholar] [CrossRef] [Green Version]
- Damle, R.N.; Wasil, T.; Fais, F.; Ghiotto, F.; Valetto, A.; Allen, S.L.; Buchbinder, A.; Budman, D.; Dittmar, K.; Kolitz, J.; et al. Ig V gene mutation status and CD38 expression as novel prognostic indicators in chronic lymphocytic leukemia. Blood 1999, 94, 1840–1847. [Google Scholar] [CrossRef]
- Hamblin, T.J.; Davis, Z.; Gardiner, A.; Oscier, D.G.; Stevenson, F.K. Unmutated Ig V(H) genes are associated with a more aggressive form of chronic lymphocytic leukemia. Blood 1999, 94, 1848–1854. [Google Scholar] [CrossRef]
- Agathangelidis, A.; Chatzidimitriou, A.; Chatzikonstantinou, T.; Tresoldi, C.; Davis, Z.; Giudicelli, V.; Kossida, S.; Belessi, C.; Rosenquist, R.; Ghia, P.; et al. ERIC, the European Research Initiative on CLL. Immunoglobulin gene sequence analysis in chronic lymphocytic leukemia: The 2022 update of the recommendations by ERIC, the European Research Initiative on CLL. Leukemia 2022, 36, 1961–1968. [Google Scholar] [CrossRef]
- Agathangelidis, A.; Psomopoulos, F.; Stamatopoulos, K. Stereotyped B Cell Receptor Immunoglobulins in B Cell Lymphomas. Methods Mol. Biol. 2019, 1956, 139–155. [Google Scholar] [CrossRef]
- Rosenquist, R.; Ghia, P.; Hadzidimitriou, A.; Sutton, L.A.; Agathangelidis, A.; Baliakas, P.; Darzentas, N.; Giudicelli, V.; Lefranc, M.P.; Langerak, A.W.; et al. Immunoglobulin gene sequence analysis in chronic lymphocytic leukemia: Updated ERIC recommendations. Leukemia 2017, 31, 1477–1481. [Google Scholar] [CrossRef] [Green Version]
- Tobin, G.; Thunberg, U.; Johnson, A.; Eriksson, I.; Söderberg, O.; Karlsson, K.; Merup, M.; Juliusson, G.; Vilpo, J.; Enblad, G.; et al. Chronic lymphocytic leukemias utilizing the VH3-21 gene display highly restricted Vlambda 2-14 gene use and homologous CDR3s: Implicating recognition of a common antigen epitope. Blood 2003, 101, 4952–4957. [Google Scholar] [CrossRef] [Green Version]
- Tobin, G.; Thunberg, U.; Karlsson, K.; Murray, F.; Laurell, A.; Willander, K.; Enblad, G.; Merup, M.; Vilpo, J.; Juliusson, G.; et al. Subsets with restricted immunoglobulin gene rearrangement features indicate a role for antigen selection in the development of chronic lymphocytic leukemia. Blood 2004, 104, 2879–2885. [Google Scholar] [CrossRef] [Green Version]
- Widhopf, G.F.; Rassenti, L.Z.; Toy, T.L.; Gribben, J.G.; Wierda, W.G.; Kipps, T.J. Chronic lymphocytic leukemia B cells of more than 1% of patients express virtually identical immunoglobulins. Blood 2004, 104, 2499–2504. [Google Scholar] [CrossRef]
- Messmer, B.T.; Albesiano, E.; Efremov, D.G.; Ghiotto, F.; Allen, S.L.; Kolitz, J.; Foa, R.; Damle, R.N.; Fais, F.; Messmer, D.; et al. Multiple distinct sets of stereotyped antigen receptors indicate a role for antigen inpromoting chronic lymphocytic leukemia. J. Exp. Med. 2004, 200, 519–525. [Google Scholar] [CrossRef]
- Stamatopoulos, K.; Belessi, C.; Hadzidimitriou, A.; Smilevska, T.; Kalagiakou, E.; Hatzi, K.; Stavroyianni, N.; Athanasiadou, A.; Tsompanakou, A.; Papadaki, T.; et al. Immunoglobulin light chain repertoire in chronic lymphocytic leukemia. Blood 2005, 106, 3575–3583. [Google Scholar] [CrossRef] [Green Version]
- Agathangelidis, A.; Chatzidimitriou, A.; Gemenetzi, K.; Giudicelli, V.; Karypidou, M.; Plevova, K.; Davis, Z.; Yan, X.J.; Jeromin, S.; Schneider, C.; et al. Higher-order onnections between stereotyped subsets: Implications for improved patient classification in CLL. Blood 2021, 137, 1365–1376. [Google Scholar] [CrossRef]
- Malcikova, J.; Stalika, E.; Davis, Z.; Plevova, K.; Trbusek, M.; Mansouri, L.; Scarfo, L.; Baliakas, P.; Gardiner, A.; Sutton, L.A.; et al. The frequency of TP53 gene defects differs between chronic lymphocytic leukaemia subgroups harbouring distinct antigen receptors. Br. J. Haematol. 2014, 166, 621–625. [Google Scholar] [CrossRef]
- Strefford, J.C.; Sutton, L.A.; Baliakas, P.; Agathangelidis, A.; Malčíková, J.; Plevova, K.; Scarfo, L.; Davis, Z.; Stalika, E.; Cortese, D.; et al. Distinct patterns of novel gene mutations in poor-prognostic stereotyped subsets of chronic lymphocytic leukemia: The case of SF3B1 and subset #2. Leukemia 2013, 27, 2196–2199. [Google Scholar] [CrossRef] [Green Version]
- Kanduri, M.; Marincevic, M.; Halldorsdottir, A.M.; Mansouri, L.; Junevik, K.; Ntoufa, S.; Kultima, H.G.; Isaksson, A.; Juliusson, G.; Andersson, P.O.; et al. Distinct transcriptional control in major immunogenetic subsets of chronic lymphocytic leukemia exhibiting subset-biased global DNA methylation profiles. Epigenetics 2012, 7, 1435–1442. [Google Scholar] [CrossRef]
- Marincevic, M.; Mansouri, M.; Kanduri, M.; Isaksson, A.; Göransson, H.; Smedby, K.E.; Jurlander, J.; Juliusson, G.; Davi, F.; Stamatopoulos, K.; et al. Distinct gene expression profiles in subsets of chronic lymphocytic leukemia expressing stereotyped IGHV4-34 B-cell receptors. Haematologica 2010, 95, 2072–2079. [Google Scholar] [CrossRef] [Green Version]
- Papakonstantinou, N.; Ntoufa, S.; Chartomatsidou, E.; Papadopoulos, G.; Hatzigeorgiou, A.; Anagnostopoulos, A.; Chlichlia, K.; Ghia, P.; Muzio, M.; Belessi, C.; et al. Differential microRNA profiles and their functional implications in different immunogenetic subsets of chronic lymphocytic leukemia. Mol. Med. 2013, 19, 115–123. [Google Scholar] [CrossRef]
- Maura, F.; Cutrona, G.; Mosca, L.; Matis, S.; Lionetti, M.; Fabris, S.; Agnelli, L.; Colombo, M.; Massucco, C.; Ferracin, M.; et al. Association between gene and miRNA expression profiles and stereotyped subset #4 B-cell receptor in chronic lymphocytic leukemia. Leuk. Lymphoma 2015, 56, 3150–3158. [Google Scholar] [CrossRef]
- Rossi, D.; Spina, V.; Bomben, R.; Rasi, S.; Dal-Bo, M.; Bruscaggin, A.; Rossi, F.M.; Monti, S.; Degan, M.; Ciardullo, C.; et al. Association between molecular lesions and specific B-cell receptor subsets in chronic lymphocytic leukemia. Blood 2013, 121, 4902–4905. [Google Scholar] [CrossRef]
- Sutton, L.A.; Young, E.; Baliakas, P.; Hadzidimitriou, A.; Moysiadis, T.; Plevova, K.; Rossi, D.; Kminkova, J.; Stalika, E.; Pedersen, L.B.; et al. Different spectra of recurrent gene mutations in subsets of chronic lymphocytic leukemia harboring stereotyped B-cell receptors. Haematologica 2016, 101, 959–967. [Google Scholar] [CrossRef]
- Biderman, B.V.; Severina, N.A.; Likold, E.B.; Obukhova, T.N.; Sudarikov, A.B.; Savchenko, V.G. Genetic lesions in Russian CLL patients with the most common stereotyped antigen receptors. Blood 2020, 136 (Suppl. S1), 16–17. [Google Scholar] [CrossRef]
- Baliakas, P.; Moysiadis, T.; Hadzidimitriou, A.; Xochelli, A.; Jeromin, S.; Agathangelidis, A.; Mattsson, M.; Sutton, L.A.; Minga, E.; Scarfò, L.; et al. Tailored approaches grounded on immunogenetic features for refined prognostication in chronic lymphocytic leukemia. Haematologica 2019, 104, 360. [Google Scholar] [CrossRef] [Green Version]
- The International Agency for Research on Cancer (IARC). Mature B-cell neoplasms. In WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, 4th ed.; Swerdlow, S.H., Campo, E., Harris, N.L., Jaffe, E.S., Pileri, S.A., Stein, H., Thiele, J., Eds.; WHO: Lyon, France, 2017; pp. 215–342. [Google Scholar]
- Biderman, B.V.; Likold, E.B.; Smirnova, S.Y.; Nikitin, E.A.; Koroleva, D.A.; Zvonkov, E.E.; Al-Radi, L.S.; Julhakyan, H.L.; Sudarikov, A.B. Repertoire of Rearranged Immunoglobulin Heavy Chain Genes in Russian Patients With B-Cell Lymphoproliferative Diseases. Clin. Lymphoma Myeloma Leuk. 2021, 21, e938–e945. [Google Scholar] [CrossRef]
- DNA Prep For Eukaryotic Cells. Available online: http://www.bio.net/bionet/mm/methods-and-reagents/1995-July/031231.html (accessed on 31 July 1995).
- Campbell, M.J.; Zelenetz, A.D.; Levy, S.; Levy, R. Use of family specific leader region primers for PCR amplification of the human heavy chain variable region repertoire. Mol. Immunol. 1992, 29, 193–203. [Google Scholar] [CrossRef]
- van Dongen, J.J.; Langerak, A.W.; Bruggemann, M.; Evans, P.A.S.; Hummel, M.; Lavender, F.L.; Delabesse, E.; Davi, F.; Schuuring, E.; García-Sanz, R.; et al. Design and standardization of PCR primers and protocols for detection of clonal immunoglobulin and T-cell receptor gene recombinations in suspect lymphoproliferations: Report of the BIOMED-2 Concerted Action BMH4-CT98-3936. Leukemia 2003, 17, 2257–2317. [Google Scholar] [CrossRef] [Green Version]
- Brochet, X.; Lefranc, M.P.; Giudicelli, V. IMGT/V-QUEST: The highly customized and integrated system for IG and TR standardized V-J and V-D-J sequence analysis. Nucleic Acids Res. 2008, 36, W503–W508. [Google Scholar] [CrossRef] [Green Version]
- Bystry, V.; Agathangelidis, A.; Bikos, V.; Sutton, L.A.; Baliakas, P.; Hadzidimitriou, A.; Stamatopoulos, K.; Darzentas, N.; European Research Initiative on CLL. ARResT/AssignSubsets: A novel application for robust subclassification of chronic lymphocytic leukemia based on B cell receptor IG stereotypy. Bioinformatics 2015, 31, 3844–3846. [Google Scholar] [CrossRef] [Green Version]
- Campregher, P.V.; Petroni, R.C.; Muto, N.H.; Sitnik, R.; de Carvalho, F.P.; Bacal, N.S.; Velloso, E.D.; Oliveira, G.B.; Pinho, J.R.; Torres, D.C.; et al. A Novel Assay for the Identification of NOTCH1 PEST Domain Mutations in Chronic Lymphocytic Leukemia. Biomed. Res. Int. 2016, 2016, 4247908. [Google Scholar] [CrossRef] [Green Version]
- Pavlova, S.; Smardova, J.; Tom, N.; Trbusek, M. Detection and Functional Analysis of TP53 Mutations in CLL. Nat. Chronic Lymphocytic Leuk. Methods Protoc. Methods Mol. Biol. 2019, 1881, 63–81. [Google Scholar] [CrossRef]
- Hernández, J.A.; Hernández-Sánchez, M.; Rodríguez-Vicente, A.E.; Grossmann, V.; Collado, R.; Heras, C.; Puiggros, A.; Martín, A.A.; Puig, N.; Benito, R.; et al. A Low Frequency of Losses in 11q Chromosome Is Associated with Better Outcome and Lower Rate of Genomic Mutations in Patients with Chronic Lymphocytic Leukemia. PLoS ONE 2015, 10, e0143073. [Google Scholar] [CrossRef] [Green Version]
- Bolger, A.M.; Lohse, M.; Usadel, B. Trimmomatic: A flexible trimmer for Illumina Sequence Data. Bioinformatics 2014, 30, 2114–2120. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Durbin, R. Fast and accurate long-read alignment with Burrows-Wheeler transform. Bioinformatics 2010, 26, 589–595. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Handsaker, B.; Wysoker, A.; Fennell, T.; Ruan, J.; Homer, N.; Marth, G.; Abecasis, G.; Durbin, R.; 1000 Genome Project Data Processing Subgroup. The Sequence Alignment/Map format and SAMtools. Bioinformatics 2009, 25, 2078–2079. [Google Scholar] [CrossRef] [Green Version]
- Lai, Z.; Markovets, A.; Ahdesmaki, M.; Chapman, B.; Hofmann, O.; McEwen, R.; Johnson, J.; Dougherty, B.; Barrett, J.C.; Dry, J.R. VarDict: A novel and versatile variant caller for next-generation sequencing in cancer research. Nucleic Acids Res. 2016, 44, e108. [Google Scholar] [CrossRef] [Green Version]
- Wang, K.; Li, M.; Hakonarson, H. ANNOVAR: Functional annotation of genetic variants from high-throughput sequencing data. Nucleic Acids Res. 2010, 38, e164. [Google Scholar] [CrossRef]
- Seshat. Available online: http://vps338341.ovh.net/ (accessed on 15 January 2022).
- COSMIC (Catalogue of Somatic Mutations in Cancer). Available online: https://cancer.sanger.ac.uk/cosmic (accessed on 15 January 2022).
- Franklin by Genoox. Available online: https://franklin.genoox.com/ (accessed on 15 January 2022).
- McGowan-Jordan, J.; Simons, A.; Schmid, M. (Eds.) ISCN: An International System for Human Cytogenomic Nomenclature; Karger: Basel, Switzerland, 2016. [Google Scholar]
- McGowan-Jordan, J.; Hastings, R.J.; Moore, S. (Eds.) ISCN 2020: An International System for Human Cytogenomic Nomenclature; Karger: Basel, Switzerland, 2020. [Google Scholar]
- Obukhova, T.N.; Kislitsyna, M.A.; Novikova, T.Y.; Biderman, B.V.; Orlova, A.A.; Seydalieva, K.R.; Sudarikov, A.B. Detection of deletion 17p13/tp53 in chronic lymphocytic leukemia by ARRAY-CGH method. Hematol. Transfusiology 2022, 67 (Suppl. S2), 130–131. (In Russian) [Google Scholar]
- Baliakas, P.; Jeromin, S.; Iskas, M.; Puiggros, A.; Plevova, K.; Nguyen-Khac, F.; Davis, Z.; Rigolin, G.M.; Visentin, A.; Xochelli, A.; et al. Cytogenetic complexity in chronic lymphocytic leukemia: Definitions, associations, and clinical impact. Blood 2019, 133, 1205–1216. [Google Scholar] [CrossRef] [Green Version]
- Rai, K.R.; Jain, P. Chronic lymphocytic leukemia (CLL)—Then and now. Am. J. Hematol. 2016, 91, 330–340. [Google Scholar] [CrossRef] [Green Version]
- Weissmann, S.; Roller, A.; Jeromin, S.; Hernández, M.; Abáigar, M.; Hernández-Rivas, J.M.; Grossmann, V.; Haferlach, C.; Kern, W.; Haferlach, T.; et al. Prognostic impact and landscape of NOTCH1 mutations in chronic lymphocytic leukemia (CLL): A study on 852 patients. Leukemia 2013, 27, 2393–2396. [Google Scholar] [CrossRef] [Green Version]
- Rossi, D.; Rasi, S.; Fabbri, G.; Spina, V.; Fangazio, M.; Forconi, F.; Marasca, R.; Laurenti, L.; Bruscaggin, A.; Cerri, M.; et al. Mutations of NOTCH1 are an independent predictor of survival in chronic lymphocytic leukemia. Blood 2012, 119, 521–529. [Google Scholar] [CrossRef] [Green Version]
- Jeromin, S.; Weissmann, S.; Haferlach, C.; Dicker, F.; Bayer, K.; Grossmann, V.; Alpermann, T.; Roller, A.; Kohlmann, A.; Haferlach, T.; et al. SF3B1 mutations correlated to cytogenetics andmutations in NOTCH1, FBXW7, MYD88,XPO1 and TP53 in 1160 untreated CLLpatients. Leukemia 2014, 28, 108–117. [Google Scholar] [CrossRef]
- Chiaretti, S.; Marinelli, M.; Del Giudice, I.; Bonina, S.; Piciocchi, A.; Messina, M.; Vignetti, M.; Rossi, D.; Di Maio, V.; Mauro, F.R.; et al. NOTCH1, SF3B1, BIRC3 and TP53 mutations in patients with chronic lymphocytic leukemia undergoing first-line treatment: Correlation with biological parameters and response to treatment. Leuk. Lymph. 2014, 55, 2785–2792. [Google Scholar] [CrossRef]
- Jondreville, L.; Krzisch, D.; Chapiro, E.; Nguyen-Khac, F. The complex karyotype and chronic lymphocytic leukemia: Prognostic value and diagnostic recommendations. Am. J. Hematol. 2020, 95, 1361–1367. [Google Scholar] [CrossRef]
- Landau, D.A.; Carter, S.L.; Stojanov, P.; McKenna, A.; Stevenson, K.; Lawrence, M.S.; Sougnez, C.; Stewart, C.; Sivachenko, A.; Wang, L.; et al. Evolution and impact of subclonal mutations in chronic lymphocytic leukemia. Cell 2013, 152, 714–726. [Google Scholar] [CrossRef] [Green Version]
- Zapatka, M.; Tausch, E.; Öztürk, S.; Yosifov, D.Y.; Seiffert, M.; Zenz, T.; Schneider, C.; Blöhdorn, J.; Döhner, H.; Mertens, D.; et al. Clonal evolution in chronic lymphocytic leukemia is scant in relapsed but accelerated in refractory cases after chemo(immune) therapy. Haematologica 2022, 107, 604–614. [Google Scholar] [CrossRef]
- Baliakas, P.; Mattsson, M.; Hadzidimitriou, A.; Minga, E.; Agathangelidis, A.; Sutton, L.A.; Scarfo, L.; Davis, Z.; Yan, X.J.; Plevova, K.; et al. No improvement in long-term survival over time for chronic lymphocytic leukemia patients in stereotyped subsets #1 and #2 treated with chemo(immuno)therapy. Haematologica 2018, 103, e158–e161. [Google Scholar] [CrossRef]
- Gerousi, M.; Laidou, S.; Gemenetzi, K.; Stamatopoulos, K.; Chatzidimitriou, A. Distinctive Signaling Profiles with Distinct biological and Clinical Implications in Aggressive CLL Subsets With Stereotyped B-Cell Receptor Immunoglobulin. Front. Oncol. 2021, 11, 771454. [Google Scholar] [CrossRef]
- Baliakas, P.; Hadzidimitriou, A.; Sutton, L.-A.; Minga, E.; Agathangelidis, A.; Nichelatti, M.; Tsanousa, A.; Scarfò, L.; Davis, Z.; Yan, X.J.; et al. Clinical Effect of Stereotyped B-Cell Receptor Immunoglobulins in Chronic Lymphocytic Leukaemia: A Retrospective Multicentre Study. Lancet Haematol. 2014, 1, e74–e84. [Google Scholar] [CrossRef]
- Maura, F.; Visco, C.; Falisi, E.; Reda, G.; Fabris, S.; Agnelli, L.; Tuana, G.; Lionetti, M.; Guercini, N.; Novella, E.; et al. B-cell receptor configuration and adverse cytogenetics are associated with autoimmune hemolytic anemia in chronic lymphocytic leukemia. Am. J. Hematol. 2013, 88, 32–36. [Google Scholar] [CrossRef]
- Xochelli, A.; Baliakas, P.; Kavakiotis, I.; Agathangelidis, A.; Sutton, L.A.; Minga, E.; Ntoufa, S.; Tausch, E.; Yan, X.J.; Shanafelt, T. Chronic Lymphocytic Leukemia with Mutated IGHV4-34 Receptors: Shared and Distinct Immunogenetic Features and Clinical Outcomes. Clin. Cancer. Res. 2017, 23, 5292–5301. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Subset | IGHV Mutational Status | Subset Size * | Cases in Analysis | IGHV | Motif [12,20] |
|---|---|---|---|---|---|
| CLL#1 | unmutated | 3.08% | 38 | Clan I | ARxQWLxxxxFDY |
| CLL#99 | unmutated | 0.10% | 22 | Clan I | ARxQWLxxxxxFDY |
| CLL#28 | unmutated | 0.77% | 15 | IGHV1-2 | ARx[YL]SGSYYYYYYGMDV |
| CLL#3 | unmutated | 1.45% | 22 | IGHV1-69 | ARxxxDIVVVPAAIx[YR]YYGMDV |
| CLL#6 | unmutated | 1.16% | 24 | IGHV1-69 | ARGGxYDY[VI]WGSYRxNDAFDI |
| CLL#5 | unmutated | 0.77% | 21 | IGHV1-69 | ARxxxxGV[IV]xxxYYYY[GY]MDV |
| CLL#7H | unmutated | 0.39% | 10 | IGHV1-69 | AxxxxxxDFW[ST]GYxxxxYYYxMDV |
| Total | 7.72% | 152 |
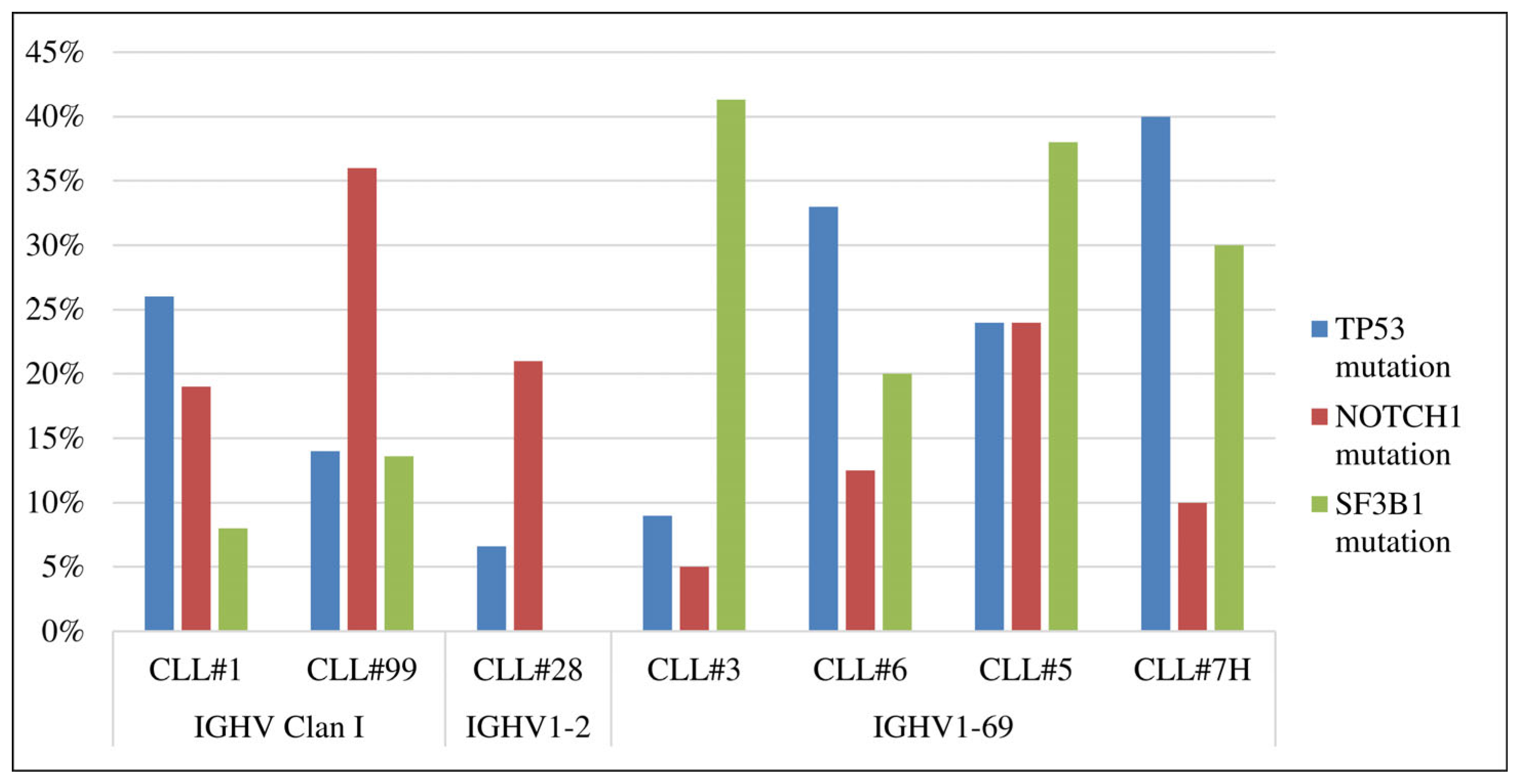
| CLL#1 | CLL#99 | CLL#28A | CLL#3 | CLL#6 | CLL#5 | CLL#7H | CLL in General [20,22,44] | |
|---|---|---|---|---|---|---|---|---|
| IGHV | Clan I | Clan I | IGHV1-2 | IGHV1-69 | IGHV1-69 | IGHV1-69 | IGHV1-69 | -- |
| U-CLL | 100% | 100% | 100% | 100% | 100% | 100% | 100% | 50–60% |
| TP53 mutation | 10/38, 26% | 3/22, 14% | 1/15, 7% | 2/22, 9% | 8/24, 33% | 5/21, 24% | 4/10, 40% | 7–10% |
| NOTCH1 mutation | 7/36, 19% | 8/22, 36% | 3/14, 21% | 1/20, 5% | 3/23, 13% | 5/21, 24% | 1/10, 10% | 4–10% |
| SF3B1 mutation | 3/35, 8% | 3/22, 13.6% | 0/15, 0% | 9/22, 41% | 4/21, 20% | 8/21, 38% | 3/10, 30% | 4–10% |
| del17p | 8/31, 26% | 2/18, 11% | 0/6, 0% ** | 1/17, 6% | 5/18, 28% | 5/16, 31% | 2/8, 25% | 4% |
| del11q | 7/20, 39% | -- | -- | -- | 1/11, 9% | -- | -- | 11% |
| del13q only | 0/20, 0% | -- | -- | -- | 1/11,9% | -- | -- | 50% |
| tris12 | 1/20, 5% | -- | -- | -- | 0/11, 0% | -- | -- | 11% |
| Complex kariotype | 6/10, 60% | -- | -- | -- | 4/7, 66% | -- | -- | 10–40% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biderman, B.V.; Likold, E.B.; Severina, N.A.; Obukhova, T.N.; Sudarikov, A.B. Genetic Lesions in Russian CLL Patients with the Most Common Stereotyped Antigen Receptors. Genes 2023, 14, 532. https://doi.org/10.3390/genes14020532
Biderman BV, Likold EB, Severina NA, Obukhova TN, Sudarikov AB. Genetic Lesions in Russian CLL Patients with the Most Common Stereotyped Antigen Receptors. Genes. 2023; 14(2):532. https://doi.org/10.3390/genes14020532
Chicago/Turabian StyleBiderman, Bella V., Ekaterina B. Likold, Nataliya A. Severina, Tatiana N. Obukhova, and Andrey B. Sudarikov. 2023. "Genetic Lesions in Russian CLL Patients with the Most Common Stereotyped Antigen Receptors" Genes 14, no. 2: 532. https://doi.org/10.3390/genes14020532