Metallothioneins in Failure of Dental Implants and Periodontitis Down Syndrome Patients

 ,
,  ,
, 
Abstract
:1. Introduction
- Down syndrome patients who have suffered aggressive periodontitis and for whom implant treatment has failed.
- Down syndrome patients who have not suffered aggressive periodontitis and have a positive experience of implant treatment (more than two years’ follow-up without bone loss problems (grade 1 on the Lavergall and Jansson scale) [14].
2. Experimental Section
2.1. Type of Study
2.2. Selection of Patients and Study Groups
- Non-Down syndrome patients
- Patients receiving treatment that could possibly affect bone metabolism, such as long-term corticosteroids, bisphosphonates, or monoclonal antibodies.
- Patients treated with short implants, or with immediate loading implants.
- Patients with active or untreated periodontal disease.
- Patients with implants inserted less than two years ago.
- Grade 0: implants with no marginal bone loss.
- Grade 1: marginal bone loss of one-third or less of the total length of the implant.
- Grade 2: one-third, but less than two-thirds, of the total length of the implant.
- Grade 3: marginal bone loss greater than two-thirds of the total length of the implant.
- A fifth group (Grade 4) was added of those patients where the implant was lost.
2.3. Sampling and Total RNA Isolation
2.4. Gene Expression
3. Results
3.1. Participants
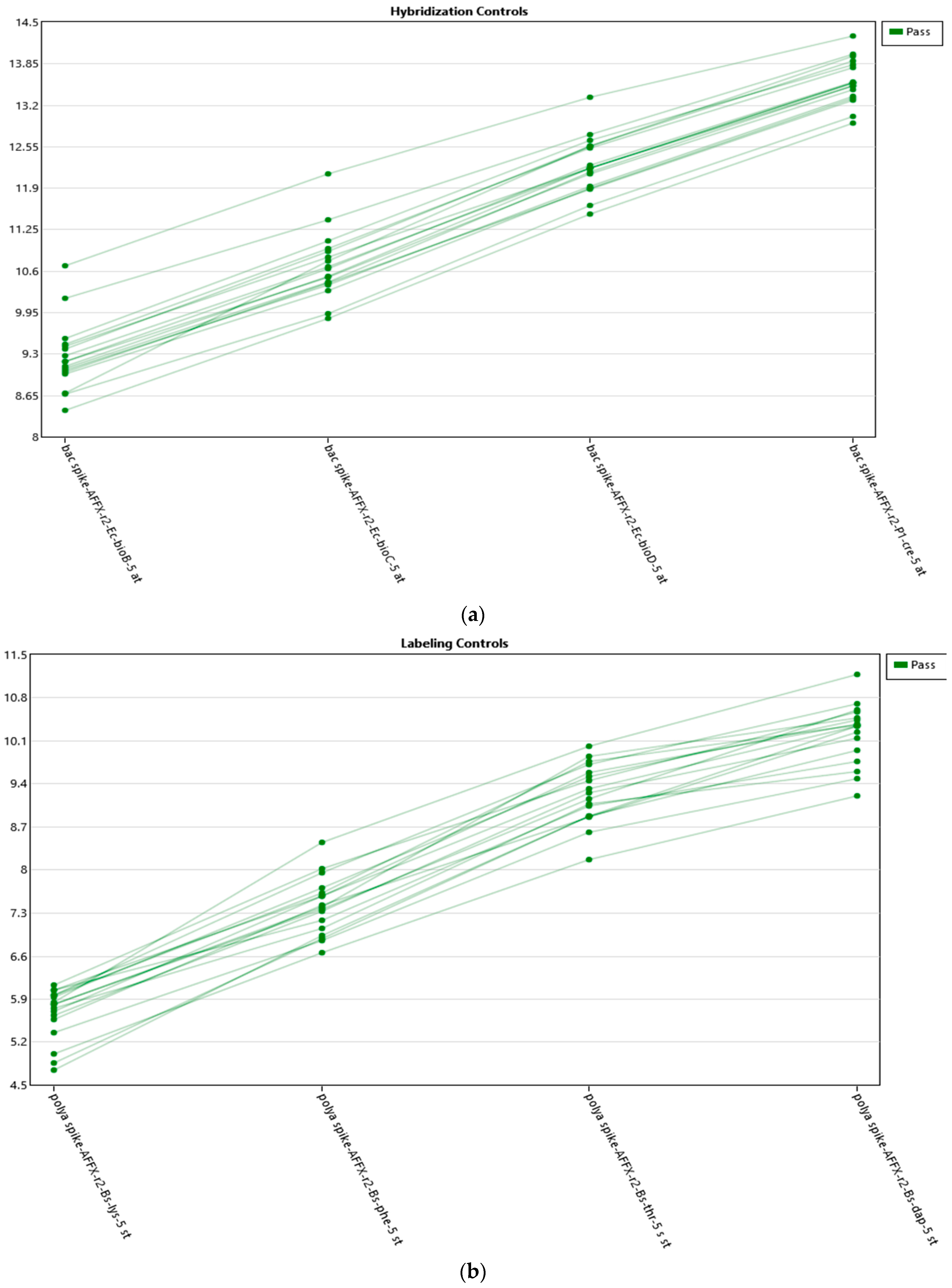
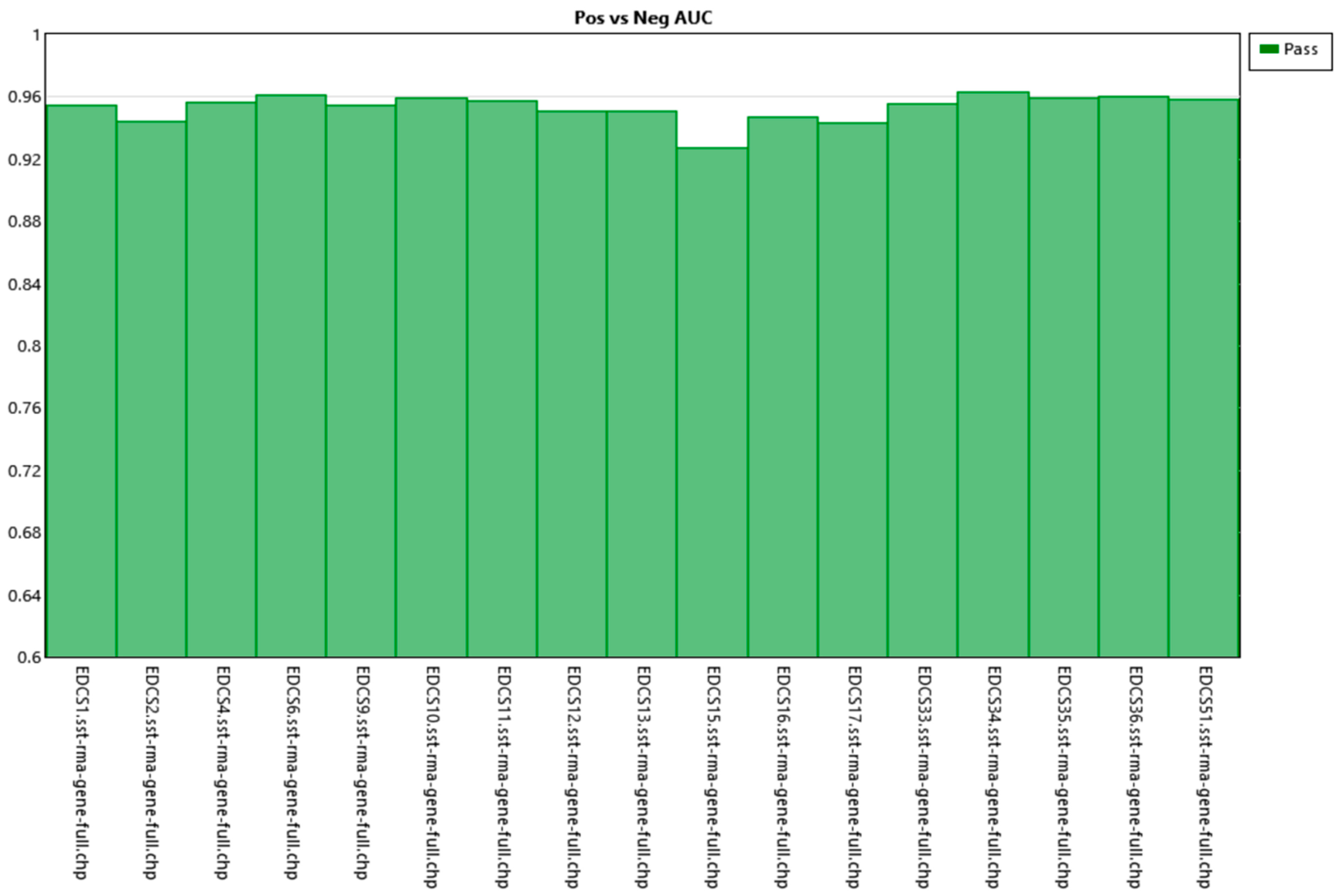
3.2. RNA Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hoffman, W., Jr.; Bomberg, T.J. Removable partial denture variations for the elderly patient. Gerodontics 1986, 2, 47–49. [Google Scholar] [PubMed]
- Bhansali, S.; Tripathi, A.; Tiwari, S.C.; Singh, S.V. A study of the prosthodontic and oral health needs of an ageing psychiatric population. Gerodontology 2008, 25, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Visser, A.; de Baat, C.; Hoeksema, A.R.; Vissink, A. Oral implants in dependent elderly persons: Blessing or burden? Gerodontology 2011, 28, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Romero-Pérez, M.J.; Mang-de la Rosa, M.R.; López-Jimenez, J.; Fernández-Feijoo, J.; Cutando-Soriano, A. Implants in disabled patients: A review and update. Med. Oral Patol Oral Cir Bucal 2014, 19, e478–e482. [Google Scholar]
- Corcuera-Flores, J.R.; López-Giménez, J.; López-Jiménez, J.; López-Giménez, A.; Silvestre-Rangil, J.; Machuca-Portillo, G. Four years survival and marginal bone loss of implants in patients with down syndrome and cerebral palsy. Clin. Oral Investig. 2017, 21, 1667–1674. [Google Scholar] [CrossRef] [PubMed]
- Marín-Berná, M.; Velázquez-Cayón, R.T.; Torres-Lagares, D.; Hita-Iglesias, P.; Bouferrache, K.; Madrid, C.; Gutiérrez-Pérez, J.L. Failure in implant rehabilitation in a patient with severe congenital neutropenia (Kostmann syndrome). J. Oral Maxillofac. Surg. 2012, 70, e260–e263. [Google Scholar] [CrossRef] [PubMed]
- Culebras-Atienza, E.; Silvestre, F.J.; Silvestre-Rangil, J. Possible association between obesity and periodontitis in patients with Down syndrome. Med. Oral Patol Oral Cir. Bucal. 2018, 23, e335–e343. [Google Scholar] [CrossRef] [PubMed]
- Ballesta-Mudarra, S.; Machuca-Portillo, G.; Torres-Lagares, D.; Rodríguez-Caballero, A.; Yáñez-Vico, R.M.; Solano-Reina, E.; Perea-Pérez, E. Determination of periodontopathogens in patients with Cri du chat síndrome. Med. Oral Patol. Oral Cir. Bucal. 2013, 18, e883–e887. [Google Scholar] [CrossRef] [PubMed]
- Corcuera-Flores, J.R.; Castellanos-Cosano, L.; Torres-Lagares, D.; Serrera-Figallo, M.A.; Rodríguez-Caballero, A.; Machuca-Portillo, G. A systematic review of the oral and craniofacial manifestations of cri du chat syndrome. Clin. Anat. 2016, 29, 555–560. [Google Scholar] [CrossRef] [PubMed]
- Maroni, G.; Wise, J.; Young, J.E.; Otto, E. Metallothionein gene duplications and metal tolerance in natural populations of drosophila melanogaster. Genetics 1987, 117, 739–744. [Google Scholar] [PubMed]
- Egli, D.; Domènech, J.; Selvaraj, A.; Balamurugan, K.; Hua, H.; Capdevila, M.; Georgiev, O.; Schaffner, W.; Atrian, S. The four members of the drosophila metallothionein family exhibit distinct yet overlapping roles in heavy metal homeostasis and detoxification. Genes Cells 2006, 11, 647–658. [Google Scholar] [CrossRef] [PubMed]
- Moleirinho, A.; Carneiro, J.; Matthiesen, R.; Silva, R.M.; Amorim, A.; Azevedo, L. Gains, losses and changes of function after gene duplication: Study of the metallothionein family. PLoS ONE 2011, 6, e18487. [Google Scholar] [CrossRef] [PubMed]
- Vašák, M.; Meloni, G. Chemistry and biology of mammalian metallothioneins. J. Biol. Inorg. Chem. 2011, 16, 1067–1078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lagervall, M.; Jansson, L.E. Treatment outcome in patients with peri-implantitis in a periodontal clinic: A retrospective study. J. Periodontol. 2013, 84, 1365–1373. [Google Scholar] [CrossRef] [PubMed]
- Corcuera-Flores, J.R.; Alonso-Domínguez, A.M.; Serrera-Figallo, M.A.; Torres-Lagares, D.; Castellanos-Cosano, L.; Machuca-Portillo, G. Relationship between osteoporosis and marginal bone loss in osseointegrated implants: A 2-year retrospective study. J. Periodontol. 2016, 87, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Liu, A.L.; Zhang, Z.M.; Zhu, B.F.; Liao, Z.H.; Liu, Z. Metallothionein protects bone marrow stromal cells against hydrogen peroxide-induced inhibition of osteoblastic differentiation. Cell Biol Int. 2004, 28, 905–911. [Google Scholar] [CrossRef]
- Ruttkay-Nedecky, B.; Nejdl, L.; Gumulec, J.; Zitka, O.; Masarik, M.; Eckschlager, T.; Stiborova, M.; Adam, V.; Kizek, R. The role of metallothionein in oxidative stress. Int. J. Mol. Sci. 2013, 14, 6044–6066. [Google Scholar] [CrossRef]
- Dohi, Y.; Shimaoka, H.; Ikeuchi, M.; Ohgushi, H.; Yonemasu, K.; Minami, T. Role of metallothionein isoforms in bone formation processes in rat marrow mesenchymal stem cells in culture. Biol Trace Elem. Res. 2005, 104, 57–70. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Group | Age | Sex | Smoker | Drinker | History of Controlled Periodontal Disease | Implants Placed | Bone Regeneration | Result after Two Years of Follow-up |
|---|---|---|---|---|---|---|---|---|---|
| 1 | +PD+FI | 41 | Female | No | No | Yes | 2 implants | No | 1 implant lost and 1 implants with severe peri-implantitis |
| 2 | +PD+FI | 39 | Female | No | No | Yes | 3 implants | No | 1 implant lost and 2 implants with severe peri-implantitis |
| 3 | +PD+FI | 33 | Male | No | No | Yes | 4 implants | No | 2 implants with severe peri-implantitis |
| 4 | +PD+FI | 35 | Male | No | No | Yes | 12 implants | No | 3 implants lost |
| 5 | -PD-FI | 40 | Female | No | No | No | 3 implants | No | No implant failure or peri-implantitis |
| 6 | -PD-FI | 34 | Female | No | No | No | 2 implants | No | No implant failure or peri-implantitis |
| 7 | -PD-FI | 43 | Female | No | No | No | 3 implants | No | No implant failure or peri-implantitis |
| 8 | -PD-FI | 48 | Female | No | No | No | 2 implants | No | No implant failure or peri-implantitis |
| 9 | -PD-FI | 44 | Male | No | No | No | No | No | No implant failure or peri-implantitis |
| 10 | -PD-FI | 38 | Male | No | No | No | No | No | No implant failure or peri-implantitis |
| 11 | -PD-FI | 44 | Male | No | No | No | No | No | No implant failure or peri-implantitis |
| ID | +PD+FI (Average, log 2) | -PD-FI (Average, log 2) | Fold Change | p Value | Fdr p Value | Genetic Symbol | Description |
|---|---|---|---|---|---|---|---|
| TC1600007959 | 8.05 | 9.49 | −2.71 | 0.0014 | 0.9997 | MT1E | Metallothionein 1E |
| TC1600007966 | 6.8 | 8.06 | −2.39 | 0.0018 | 0.9997 | MT1H | Metallothionein 1H |
| TC1600011399 | 10.73 | 12.36 | −3.09 | 0.0021 | 0.9997 | MT1X | Metallothionein 1X |
| TC1600007962 | 12.17 | 13.67 | −2.82 | 0.0023 | 0.9997 | MT1A | Metallothionein 1A |
| TC1600007964 | 11.7 | 13.38 | −2.95 | 0.0024 | 0.9997 | MT1B; MT1C | Metallothionein 1B; Metallothionein 1C, pseudogene |
| TC1600007958 | 11.58 | 12.93 | −2.55 | 0.0048 | 0.9997 | MT1L | Metallothionein 1L (gene/pseudogene) |
| TC1600007957 | 13.82 | 15.05 | −2.35 | 0.0072 | 0.9997 | MT2A | Metallothionein 2A |
| TC1600007960 | 9.03 | 10.39 | −2.37 | 0.0092 | 0.9997 | MT1M | Metallothionein 1M |
| TC1600010421 | 10.62 | 11.79 | −2.24 | 0.0118 | 0.9997 | MT1G | Metallothionein 1G |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baus-Domínguez, M.; Gómez-Díaz, R.; Corcuera-Flores, J.-R.; Torres-Lagares, D.; Ruiz-Villandiego, J.-C.; Machuca-Portillo, G.; Gutiérrez-Pérez, J.-L.; Serrera-Figallo, M.-A. Metallothioneins in Failure of Dental Implants and Periodontitis Down Syndrome Patients. Genes 2019, 10, 711. https://doi.org/10.3390/genes10090711
Baus-Domínguez M, Gómez-Díaz R, Corcuera-Flores J-R, Torres-Lagares D, Ruiz-Villandiego J-C, Machuca-Portillo G, Gutiérrez-Pérez J-L, Serrera-Figallo M-A. Metallothioneins in Failure of Dental Implants and Periodontitis Down Syndrome Patients. Genes. 2019; 10(9):711. https://doi.org/10.3390/genes10090711
Chicago/Turabian StyleBaus-Domínguez, Maria, Raquel Gómez-Díaz, Jose-Ramón Corcuera-Flores, Daniel Torres-Lagares, José-Cruz Ruiz-Villandiego, Guillermo Machuca-Portillo, José-Luis Gutiérrez-Pérez, and María-Angeles Serrera-Figallo. 2019. "Metallothioneins in Failure of Dental Implants and Periodontitis Down Syndrome Patients" Genes 10, no. 9: 711. https://doi.org/10.3390/genes10090711