
Adult and Pediatric Nail Unit Melanoma: Epidemiology, Diagnosis, and Treatment


Abstract
:1. Etiology
2. Risk Factors
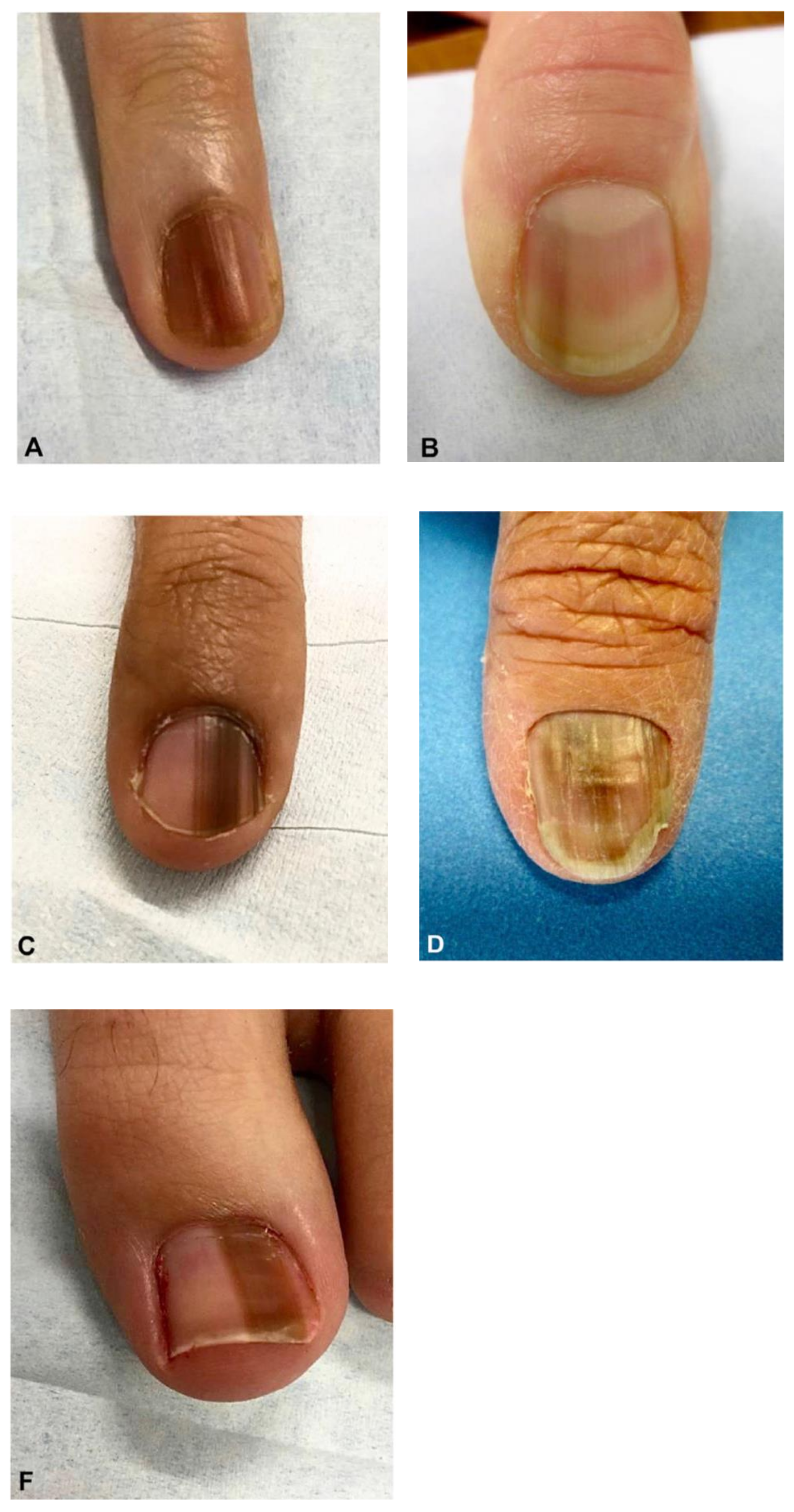
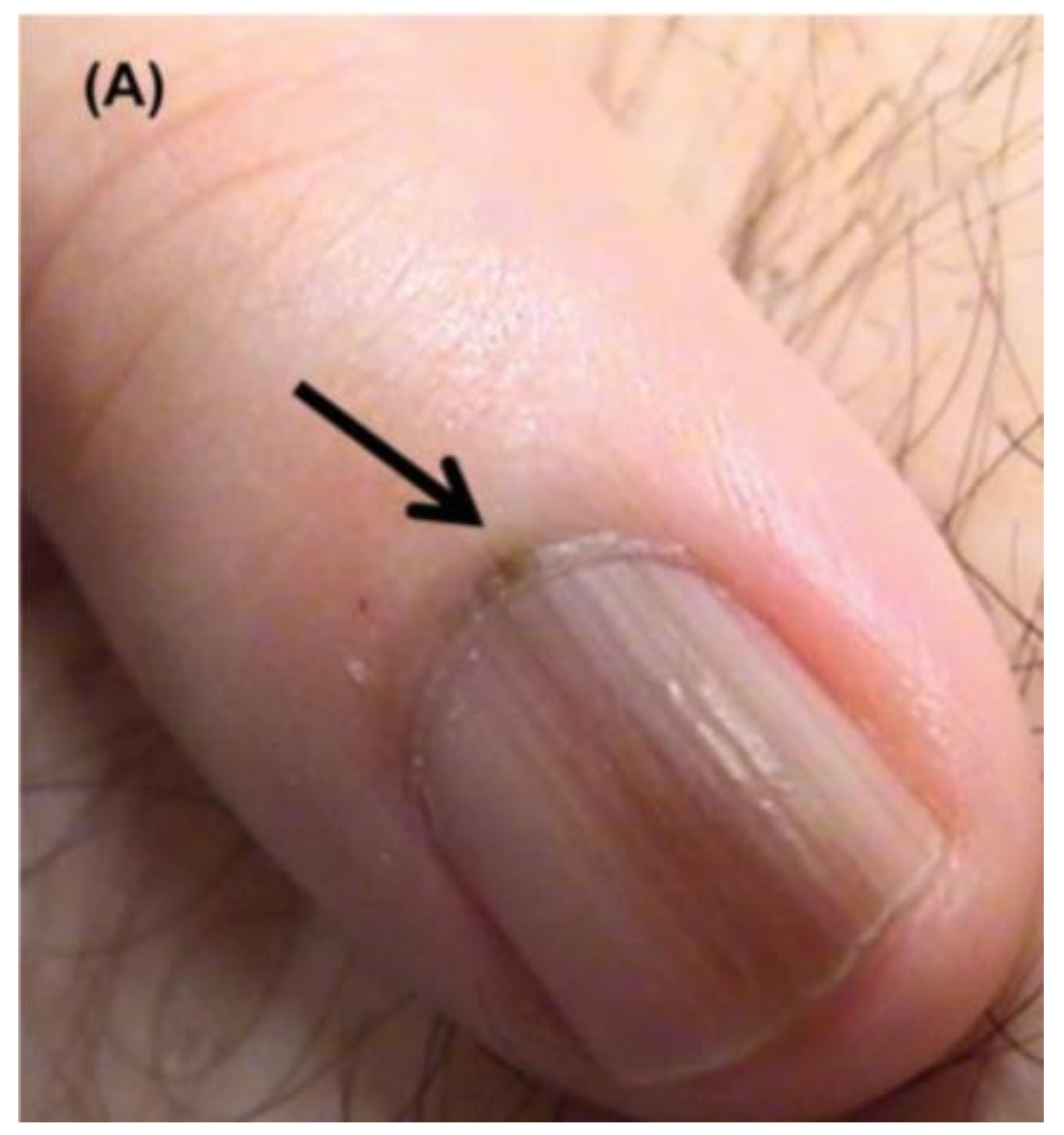
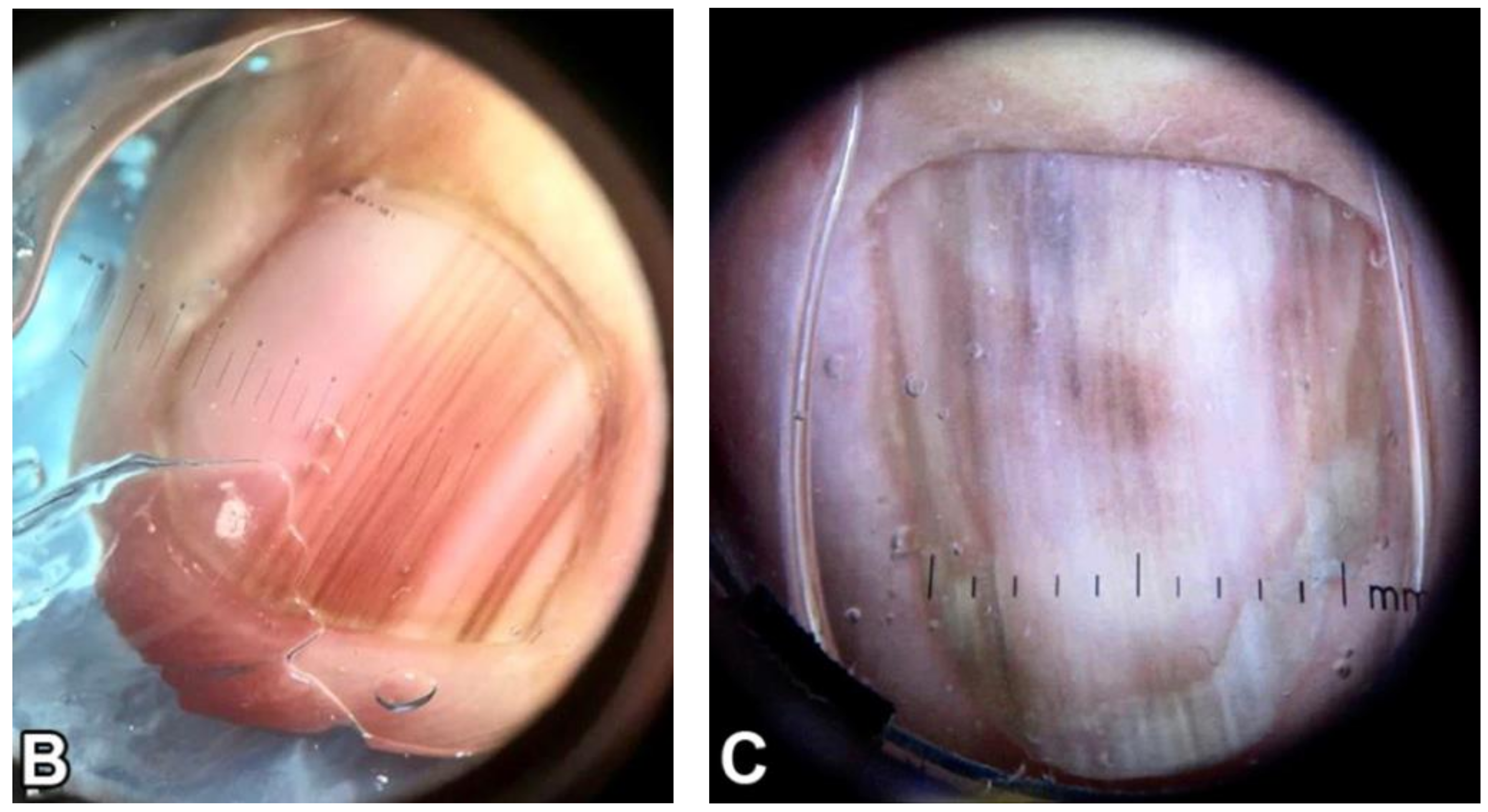
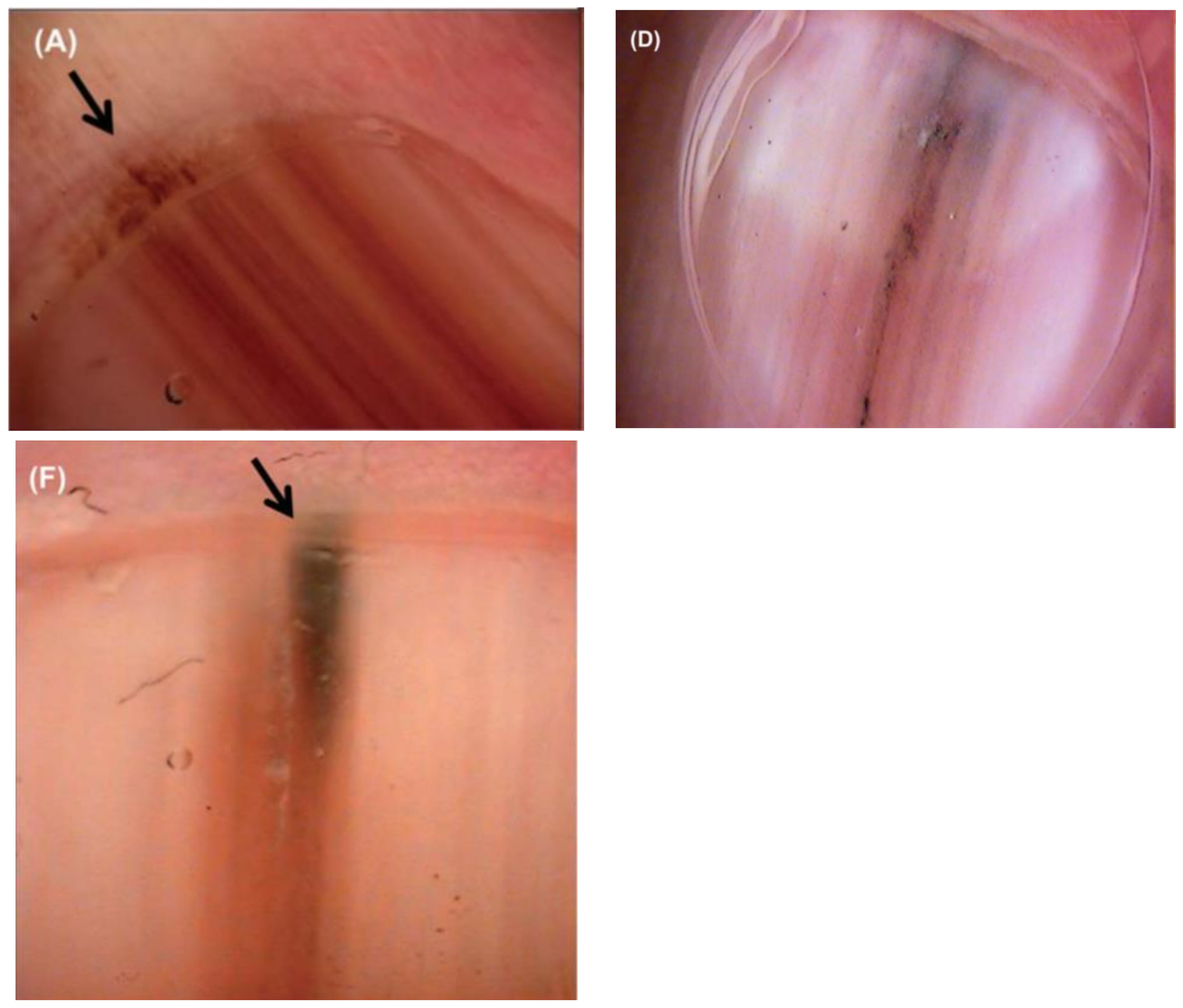
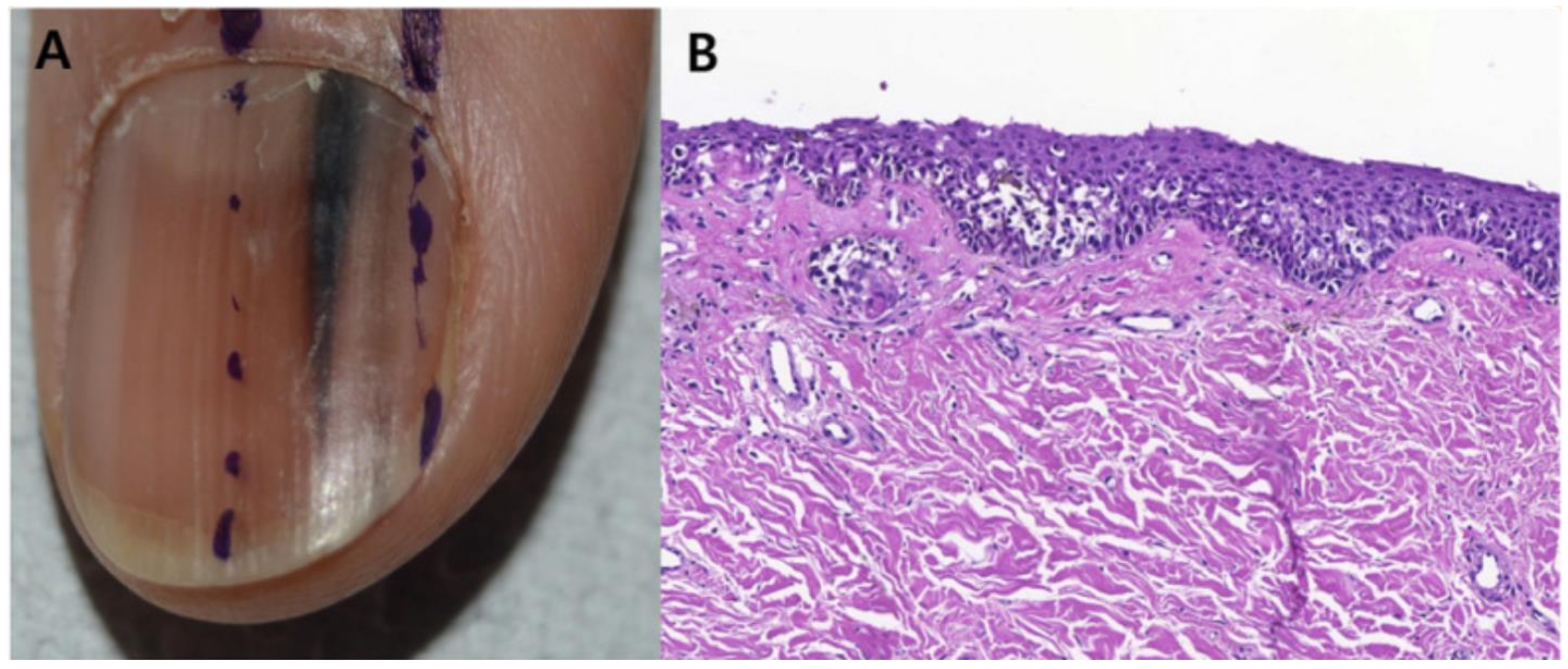
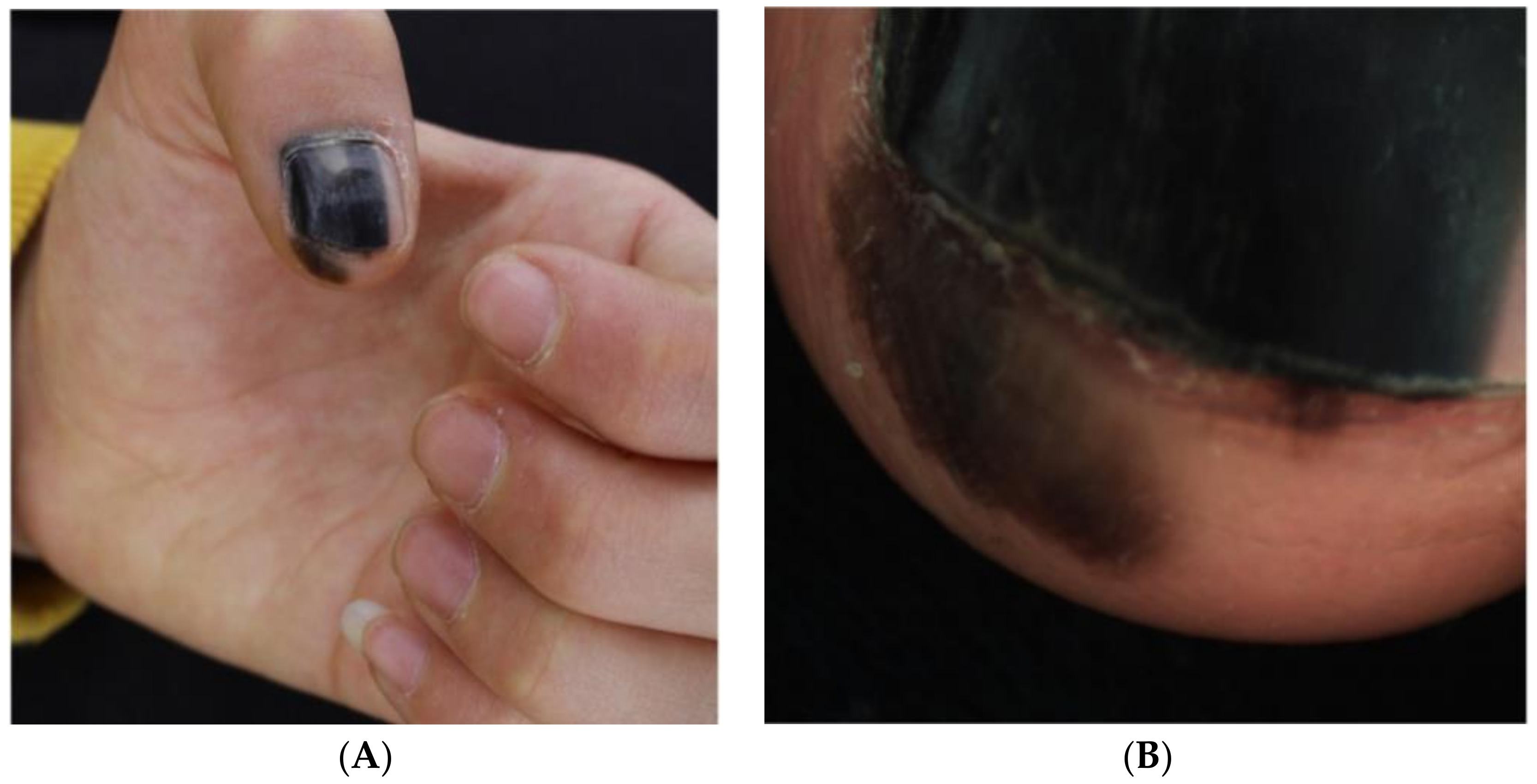
3. Clinical Presentation & Dermoscopy
4. Diagnosis
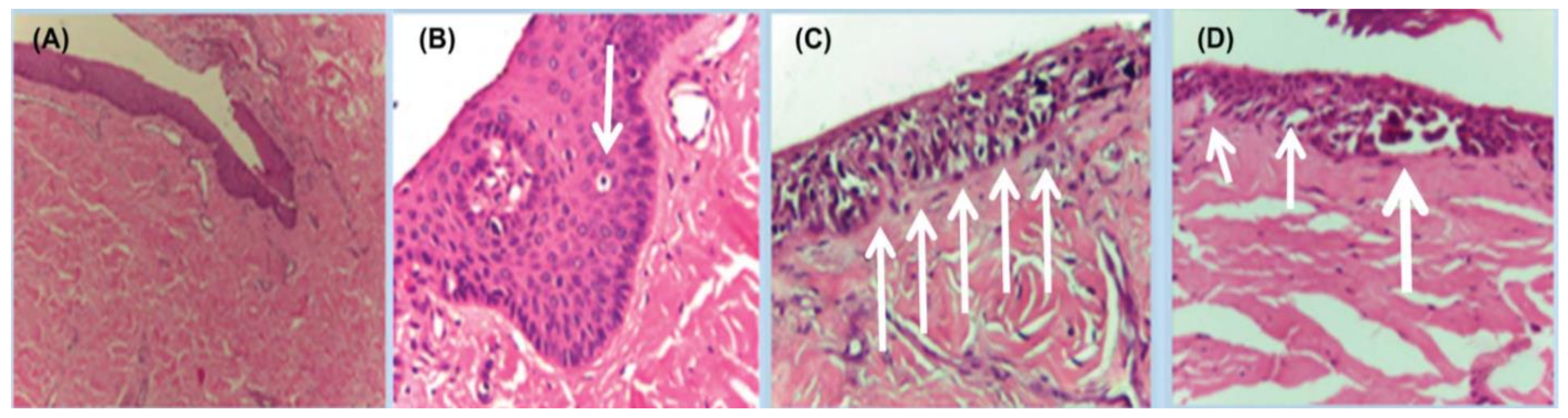
5. Histopathology
6. Management
6.1. Management: Surgery
6.2. Management: Adjuvant Therapy
6.2.1. Targeted Therapies
6.2.2. Immunotherapies
6.3. Management: Neoadjuvant Therapy
6.4. Prognosis by Location
7. Pediatric NUM
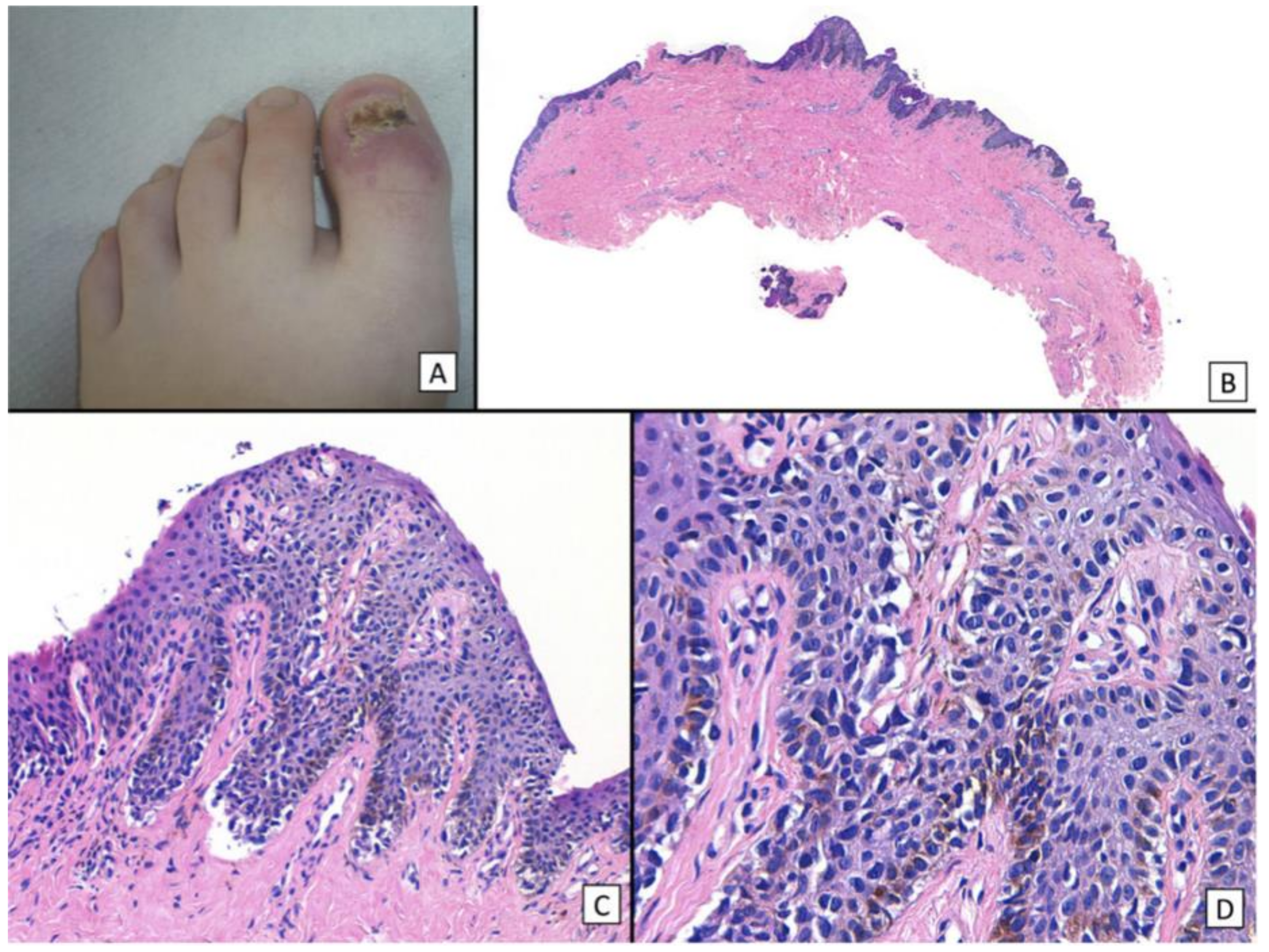
7.1. Pediatric NUM: Clinical Presentation & Dermoscopy
7.2. Diagnosis
7.3. Histopathology
7.4. Management
8. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bradford, P.T.; Goldstein, A.M.; McMaster, M.L.; Tucker, M.A. Acral lentiginous melanoma: Incidence and survival patterns in the United States, 1986–2005. Arch. Dermatol. 2009, 145, 427–434. [Google Scholar] [CrossRef]
- Basurto-Lozada, P.; Molina-Aguilar, C.; Castaneda-Garcia, C.; Vázquez-Cruz, M.E.; Garcia-Salinas, O.I.; Álvarez-Cano, A.; Martínez-Said, H.; Roldán-Marín, R.; Adams, D.J.; Possik, P.A.; et al. Acral lentiginous melanoma: Basic facts, biological characteristics and research perspectives of an understudied disease. Pigment. Cell Melanoma Res. 2021, 34, 59–71. [Google Scholar] [CrossRef] [Green Version]
- Duarte, A.F.; Correia, O.; Barros, A.M.; Ventura, F.; Haneke, E. Nail melanoma in situ: Clinical, dermoscopic, pathologic clues, and steps for minimally invasive treatment. Dermatol. Surg. 2015, 41, 59–68. [Google Scholar] [CrossRef] [Green Version]
- Kazi, R.; Moghaddam, S.; Chu, P.; Marghoob, A.A. Histologic Evidence of Melanocytes Isolated to the Nail Matrix. JAMA Dermatol. 2016, 152, 573–575. [Google Scholar] [CrossRef] [Green Version]
- Lee, D.J.R.; Arbache, S.T.; Quaresma, M.V.; Nico, M.M.S.; Gabbi, T.V.B. Nail Apparatus Melanoma: Experience of 10 Years in a Single Institution. Ski. Appendage Disord. 2018, 5, 20–26. [Google Scholar] [CrossRef]
- Saida, T. Heterogeneity of the site of origin of malignant melanoma in ungual areas: ‘subungual’ malignant melanoma may be a misnomer. Br. J. Dermatol. 1992, 126, 529. [Google Scholar] [CrossRef]
- Haneke, E. Ungual melanoma—Controversies in diagnosis and treatment. Dermatol. Ther. 2012, 25, 510–524. [Google Scholar] [CrossRef]
- Möhrle, M.; Häfner, H. Is subungual melanoma related to trauma? Dermatology 2002, 204, 259–261. [Google Scholar] [CrossRef]
- Choi, M.E.; Cho, H.; Won, C.H.; Chang, S.E.; Lee, M.W.; Lee, W.J. Clinicopathologic Characteristics of Trauma-Related Nail Apparatus Melanoma: A Comparative Study according to the Presence of Trauma prior to Melanoma Development. Dermatology 2022, 239, 165–173. [Google Scholar] [CrossRef]
- Stern, D.K.; Creasey, A.A.; Quijije, J.; Lebwohl, M.G. UV-A and UV-B penetration of normal human cadaveric fingernail plate. Arch. Dermatol. 2011, 147, 439–441. [Google Scholar] [CrossRef] [Green Version]
- Holman, B.N.; Van Gulick, R.J.; Amato, C.M.; Macbeth, M.L.; Davies, K.D.; Aisner, D.L.; Robinson, W.A.; Couts, K.L. Clinical and molecular features of subungual melanomas are site-specific and distinct from acral melanomas. Melanoma Res. 2020, 30, 562–573. [Google Scholar] [CrossRef] [PubMed]
- Yeh, I.; Jorgenson, E.; Shen, L.; Xu, M.; North, J.P.; Shain, A.H.; Reuss, D.; Wu, H.; Robinson, W.A.; Olshen, A.; et al. Targeted Genomic Profiling of Acral Melanoma. J. Natl. Cancer Inst. 2019, 111, 1068–1077. [Google Scholar] [CrossRef] [PubMed]
- Shi, K.; Zhang, B.; Kong, B.Y.; Zhang, Y.; Igartua, C.; Mohan, L.S.; Quan, V.L.; Panah, E.; Isales, M.C.; Beaubier, N.; et al. Distinct Genomic Features in a Retrospective Cohort of Mucosal, Acral and Vulvovaginal Melanomas. J. Am. Acad. Dermatol. 2019. [Google Scholar] [CrossRef]
- Duarte, A.F.; Correia, O.; Barros, A.M.; Azevedo, R.; Haneke, E. Nail matrix melanoma in situ: Conservative surgical management. Dermatology 2010, 220, 173–175. [Google Scholar] [CrossRef]
- Ruben, B.S. Pigmented lesions of the nail unit: Clinical and histopathologic features. Semin. Cutan. Med. Surg. 2010, 29, 148–158. [Google Scholar] [CrossRef]
- Mannava, K.A.; Mannava, S.; Koman, L.A.; Robinson-Bostom, L.; Jellinek, N. Longitudinal melanonychia: Detection and management of nail melanoma. Hand Surg. 2013, 18, 133–139. [Google Scholar] [CrossRef]
- Zhang, J.; Yun, S.J.; McMurray, S.L.; Miller, C.J. Management of Nail Unit Melanoma. Dermatol. Clin. 2021, 39, 269–280. [Google Scholar] [CrossRef]
- Lipner, S.R. Ulcerated Nodule of the Fingernail. JAMA 2018, 319, 713–714. [Google Scholar] [CrossRef] [Green Version]
- Ko, D.; Oromendia, C.; Scher, R.; Lipner, S.R. Retrospective single-center study evaluating clinical and dermoscopic features of longitudinal melanonychia, ABCDEF criteria, and risk of malignancy. J. Am. Acad. Dermatol. 2019, 80, 1272–1283. [Google Scholar] [CrossRef]
- Jellinek, N.J.; Lipner, S.R. Longitudinal Erythronychia: Retrospective Single-Center Study Evaluating Differential Diagnosis and the Likelihood of Malignancy. Dermatol. Surg. 2016, 42, 310–319. [Google Scholar] [CrossRef]
- Black, A.T.; Lahouti, A.H.; Genco, I.S.; Yagudayev, M.; Markinson, B.C.; Spielfogel, W.D. A Rare Case of Osteoinvasive Amelanotic Melanoma of the Nail Unit. Ski. Appendage Disord. 2021, 7, 139–143. [Google Scholar] [CrossRef]
- Levit, E.K.; Kagen, M.H.; Scher, R.K.; Grossman, M.; Altman, E. The ABC rule for clinical detection of subungual melanoma. J. Am. Acad. Dermatol. 2000, 42, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Ríos-Viñuela, E.; Nájera-Botello, L.; Requena, L.; Nagore, E.; Requena, C. Subungual Melanocytic Lesions: Key Clinical and Pathologic Concepts and Biopsy Techniques. Actas. Dermosifiliogr. 2021, 112, 573–585. [Google Scholar] [CrossRef]
- Starace, M.; Dika, E.; Fanti, P.; Patrizi, A.; Misciali, C.; Alessandrini, A.; Bruni, F.; Piraccini, B. Nail apparatus melanoma: Dermoscopic and histopathologic correlations on a series of 23 patients from a single centre. J. Eur. Acad. Dermatol. Venereol. 2017, 32, 164–173. [Google Scholar] [CrossRef]
- Lipner, S.R.; Scher, R.K. Evaluation of nail lines: Color and shape hold clues. Cleve Clin. J. Med. 2016, 83, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.K.; Lipner, S.R. Optimal diagnosis and management of common nail disorders. Ann. Med. 2022, 54, 694–712. [Google Scholar] [CrossRef]
- Ohn, J.; Jo, G.; Cho, Y.; Sheu, S.L.; Cho, K.H.; Mun, J.-H. Assessment of a Predictive Scoring Model for Dermoscopy of Subungual Melanoma In Situ. JAMA Dermatol. 2018, 154, 890–896. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, D.K.; Chang, M.J.; Desai, A.D.; Lipner, S.R. Clinical and dermoscopic findings of benign longitudinal melanonychia due to melanocytic activation differ by skin type and predict likelihood of nail matrix biopsy. J. Am. Acad. Dermatol. 2022, 87, 792–799. [Google Scholar] [CrossRef]
- Lieberherr, S.; Cazzaniga, S.; Haneke, E.; Hunger, R.E.; Jafari, S.M.S. Melanoma of the nail apparatus: A systematic review and meta-analysis of current challenges and prognosis. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 967–976. [Google Scholar] [CrossRef]
- Gatica-Torres, M.; Nelson, C.A.; Lipoff, J.B.; Miller, C.J.; Rubin, A.I. Nail clipping with onyzhengmycosis and surprise clue to the diagnosis of nail unit melanoma. J. Cutan. Pathol. 2018, 45, 803–806. [Google Scholar] [CrossRef]
- Das De, S.; Tan, K.B.; Ho, S.-A.J.E.; Athanasian, E.A.; Puhaindran, M.E. Pigmented Nail Lesions: When to Observe, When to Biopsy, When to Widely Excise, and When to Amputate? J. Hand Surg. Am. 2022, 47, 988–997. [Google Scholar] [CrossRef]
- Halteh, P.; Scher, R.; Artis, A.; Lipner, S.R. A survey-based study of management of longitudinal melanonychia amongst attending and resident dermatologists. J. Am. Acad. Dermatol. 2017, 76, 994–996. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halteh, P.; Scher, R.; Artis, A.; Lipner, S. Assessment of Patient Knowledge of Longitudinal Melanonychia: A Survey Study of Patients in Outpatient Clinics. Ski. Appendage Disord. 2017, 2, 156–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, R.; Lipner, S. Assessment of internet sources on subungual melanoma. Melanoma Res. 2020, 30, 416–419. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.C.; Stewart, C.R.; Lipner, S.R. Retrospective study of trends in dermatology telemedicine and in-person visits at an academic center during COVID-19. J. Am. Acad. Dermatol. 2021, 84, 777–779. [Google Scholar] [CrossRef]
- Lipner, S.R.; Iorizzo, M.; Jellinek, N.; Piraccini, B.M.; Scher, R.K. Considerations for management of longitudinal melanonychia during the coronavirus disease 2019 (COVID-19) pandemic: An international perspective. J. Am. Acad. Dermatol. 2020, 83, e159–e161. [Google Scholar] [CrossRef]
- Rodriguez, O.; Elenitsas, R.; Jiang, A.J.; Abbott, J.; Rubin, A.I. A call for nail clipping histopathology to become an essential component of the routine evaluation of melanonychia: Benefitting patients as a triage and surgical planning maneuver. J. Cutan. Pathol. 2022, 50, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Stephen, S.; Tosti, A.; Rubin, A.I. Diagnostic Applications of Nail Clippings. Dermatol. Clin. 2015, 33, 289–301. [Google Scholar] [CrossRef] [PubMed]
- Braun, R.P.; Baran, R.; Le Gal, F.A.; Dalle, S.; Ronger, S.; Pandolfi, R.; Gaide, O.; French, L.E.; Laugier, P.; Saurat, J.H.; et al. Diagnosis and management of nail pigmentations. J. Am. Acad. Dermatol. 2007, 56, 835–847. [Google Scholar] [CrossRef]
- Rich, P. Nail biopsy: Indications and methods. J. Dermatol. Surg. Oncol. 1992, 18, 673–682. [Google Scholar] [CrossRef]
- Jellinek, N. Nail matrix biopsy of longitudinal melanonychia: Diagnostic algorithm including the matrix shave biopsy. J. Am. Acad. Dermatol. 2007, 56, 803–810. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Jung, C.J.; Na, H.; Lee, W.J.; Chang, S.E.; Lee, M.W.; Park, C.S.; Lim, Y.; Won, C.H. Cyclin D1 and PRAME expression in distinguishing melanoma in situ from benign melanocytic proliferation of the nail unit. Diagn. Pathol. 2022, 17, 41. [Google Scholar] [CrossRef]
- Parra, O.; Linos, K.; Li, Z.; Yan, S. PRAME expression in melanocytic lesions of the nail. J. Cutan. Pathol. 2022, 49, 610–617. [Google Scholar] [CrossRef]
- Ren, M.; Ren, J.; Cai, X.; Shen, X.; Kong, J.; Dai, B.; Kong, Y. Clinicopathological, immunohistochemical and fluorescence in-situ hybridisation features of early subungual melanoma: An analysis of 65 cases. Histopathology 2021, 78, 717–726. [Google Scholar] [CrossRef]
- Rubin, A.I. Commentary on Mohs Micrographic Surgery Using MART-1 Immunostaining for Nail Unit Melanoma in Situ. Dermatol. Surg. 2021, 47, 263. [Google Scholar] [CrossRef] [PubMed]
- Mundada, P.; Becker, M.; Lenoir, V.; Stefanelli, S.; Rougemont, A.-L.; Beaulieu, J.Y.; Boudabbous, S. High resolution MRI of nail tumors and tumor-like conditions. Eur. J. Radiol. 2019, 112, 93–105. [Google Scholar] [CrossRef] [PubMed]
- Yun, S.J.; Bastian, B.C.; Duncan, L.M.; Haneke, E.U.H. Acral melanoma. In WHO Classification of Skin Tumours WHO Classification of Tumours, 4th ed.; Elder, D.E., Massi, D., Scolyer, R.A.W.R., Eds.; IARC Publications: Lyon, France, 2018; Volume 11, p. 116e118. [Google Scholar]
- Park, S.-W.; Jang, K.-T.; Lee, J.-H.; Park, J.-H.; Kwon, G.Y.; Mun, G.-H.; Lee, D.-Y.; Lee, J.B.; Park, K.K. Scattered atypical melanocytes with hyperchromatic nuclei in the nail matrix: Diagnostic clue for early subungual melanoma in situ. J. Cutan. Pathol. 2016, 43, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Izumi, M.; Ohara, K.; Hoashi, T.; Nakayama, H.; Chiu, C.-S.; Nagai, T.; Matsubayashi, J.; Iwaya, K.; Mukai, K. Subungual melanoma: Histological examination of 50 cases from early stage to bone invasion. J. Dermatol. 2008, 35, 695–703. [Google Scholar] [CrossRef]
- Tan, K.-B.; Moncrieff, M.; Thompson, J.F.; McCarthy, S.W.; Shaw, H.M.; Quinn, M.J.; Li, L.-X.L.; Crotty, K.A.; Stretch, J.R.; Scolyer, R.A. Subungual melanoma: A study of 124 cases highlighting features of early lesions, potential pitfalls in diagnosis, and guidelines for histologic reporting. Am. J. Surg. Pathol. 2007, 31, 1902–1912. [Google Scholar] [CrossRef]
- Amin, B.; Nehal, K.S.; Jungbluth, A.A.; Zaidi, B.; Brady, M.S.; Coit, D.C.; Zhou, Q.; Busam, K.J. Histologic distinction between subungual lentigo and melanoma. Am. J. Surg. Pathol. 2008, 32, 835–843. [Google Scholar] [CrossRef]
- Keung, E.Z.; Gershenwald, J.E. The eighth edition American Joint Committee on Cancer (AJCC) melanoma staging system: Implications for melanoma treatment and care. Expert Rev. Anticancer. Ther. 2018, 18, 775–784. [Google Scholar] [CrossRef]
- Chakera, A.H.; Quinn, M.J.; Lo, S.; Drummond, M.; Haydu, L.E.; Bond, J.S.; Stretch, J.R.; Saw, R.P.M.; Lee, K.J.; McCarthy, W.H.; et al. Subungual Melanoma of the Hand. Ann. Surg. Oncol. 2019, 26, 1035–1043. [Google Scholar] [CrossRef]
- Nakamura, Y.; Fujisawa, Y.; Teramoto, Y.; Sato, S.; Yamada, K.; Sekine, K.; Fujimoto, M.; Otsuka, F.; Yamamoto, A. Tumor-to-bone distance of invasive subungual melanoma: An analysis of 30 cases. J. Dermatol. 2014, 41, 872–877. [Google Scholar] [CrossRef]
- Cochran, A.M.; Buchanan, P.J.; Bueno, R.A., Jr.; Neumeister, M.W. Subungual melanoma: A review of current treatment. Plast. Reconstr. Surg. 2014, 134, 259–273. [Google Scholar] [CrossRef]
- Moehrle, M.; Metzger, S.; Schippert, W.; Garbe, C.; Rassner, G.; Breuninger, H. “Functional” surgery in subungual melanoma. Dermatol. Surg. 2003, 29, 366–374. [Google Scholar] [CrossRef]
- Sureda, N.; Phan, A.; Poulalhon, N.; Balme, B.; Dalle, S.; Thomas, L. Conservative surgical management of subungual (matrix derived) melanoma: Report of seven cases and literature review. Br. J. Dermatol. 2011, 165, 852–858. [Google Scholar] [CrossRef] [PubMed]
- Jo, G.; Cho, S.I.; Choi, S.; Mun, J.-H. Functional surgery versus amputation for in situ or minimally invasive nail melanoma: A meta-analysis. J. Am. Acad. Dermatol. 2019, 81, 917–922. [Google Scholar] [CrossRef] [PubMed]
- Swanson, G.G. The Upper Extremities. In Guides to the Evaluation of Permanent Impairment, 5th ed.; Cocchiarella, L., Andersson, G.B.J., Eds.; American Medical Associations: Chicago, IL, USA, 2001; pp. 433–522. [Google Scholar]
- Park, J.H.; Kim, H.-C.; Lee, J.H.; Kim, J.S.; Roh, S.Y.; Yi, C.H.; Kang, Y.K.; Kwon, B.S. Development of Korean Academy of Medical Sciences Guideline for rating physical disability of upper extremity. J. Korean Med. Sci. 2009, 24 (Suppl. S2), S288–S298. [Google Scholar] [CrossRef]
- Nguyen, J.T.; Bakri, K.; Nguyen, E.C.; Johnson, C.H.; Moran, S.L. Surgical management of subungual melanoma: Mayo clinic experience of 124 cases. Ann. Plast. Surg. 2013, 71, 346–354. [Google Scholar] [CrossRef] [PubMed]
- Brodland, D.G. The treatment of nail apparatus melanoma with Mohs micrographic surgery. Dermatol. Surg. 2001, 27, 269–273. [Google Scholar]
- Terushkin, V.; Brodland, D.G.; Sharon, D.J.; Zitelli, J.A. Digit-Sparing Mohs Surgery for Melanoma. Dermatol. Surg. 2016, 42, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, A.; Strickland, N.; Nijhawan, R.I.; Srivastava, D. Nail Unit Melanoma In Situ Treated With Mohs Micrographic Surgery. Dermatol. Surg. 2021, 47, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Falotico, J.M.; Lipner, S.R. The pharmacotherapeutic management of nail unit and acral melanomas. Expert Opin. Pharmacother. 2022, 23, 1273–1289. [Google Scholar] [CrossRef] [PubMed]
- Gellrich, F.; Schmitz, M.; Beissert, S.; Meier, F. Anti-PD-1 and Novel Combinations in the Treatment of Melanoma—An Update. J. Clin. Med. 2020, 9, 223. [Google Scholar] [CrossRef] [Green Version]
- Falotico, J.M.; Postow, M.A.; Lipner, S.R. Standardized guidelines for acral and nail unit melanoma treatment are lacking. J. Am. Acad. Dermatol. 2022, 87, e201–e202. [Google Scholar] [CrossRef]
- Cho, K.K.; Cust, A.E.; Foo, Y.M.; Long, G.V.; Menzies, A.M.; Eslick, G.D. Metastatic acral melanoma treatment outcomes: A systematic review and meta-analysis. Melanoma Res. 2021, 31, 482–486. [Google Scholar] [CrossRef]
- Zheng, Q.; Li, J.; Zhang, H.; Wang, Y.; Zhang, S. Immune Checkpoint Inhibitors in Advanced Acral Melanoma: A Systematic Review. Front. Oncol. 2020, 10, 602705. [Google Scholar] [CrossRef]
- Nakamura, Y.; Namikawa, K.; Yoshino, K.; Yoshikawa, S.; Uchi, H.; Goto, K.; Nakamura, Y.; Fukushima, S.; Kiniwa, Y.; Takenouchi, T.; et al. Anti-PD1 checkpoint inhibitor therapy in acral melanoma: A multicenter study of 193 Japanese patients. Ann. Oncol. 2020, 31, 1198–1206. [Google Scholar] [CrossRef]
- Zhang, Y.; Lan, S.; Wu, D. Advanced Acral Melanoma Therapies: Current Status and Future Directions. Curr. Treat. Options Oncol. 2022, 23, 1405–1427. [Google Scholar] [CrossRef]
- Dika, E.; Patrizi, A.; Fanti, P.A.; Chessa, M.A.; Reggiani, C.; Barisani, A.; Piraccini, B.M. The Prognosis of Nail Apparatus Melanoma: 20 Years of Experience from a Single Institute. Dermatology 2016, 232, 177–184. [Google Scholar] [CrossRef]
- LaRocca, C.J.; Lai, L.; Nelson, R.A.; Modi, B.; Crawford, B. Subungual Melanoma: A Single Institution Experience. Med. Sci. 2021, 9, 57. [Google Scholar] [CrossRef] [PubMed]
- Paolino, G.; Bekkenk, M.W.; Didona, D.; Eibenschutz, L.; Richetta, A.G.; Cantisani, C.; Viti, G.; Carbone, A.; Buccini, P.; De Simone, P.; et al. Is the prognosis and course of acral melanoma related to site-specific clinico-pathological features? Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 842–848. [Google Scholar] [PubMed]
- Ríos-Viñuela, E.; Manrique-Silva, E.; Nagore, E.; Nájera-Botello, L.; Requena, L.; Requena, C. Subungual Melanocytic Lesions in Pediatric Patients. Lesiones melanocíticas subungueales en la edad pediátri-ca. Actas Dermosifiliogr. 2022, 113, 388–400. [Google Scholar] [CrossRef]
- Yan, Y.; Huang, Y.; Wang, Y.; Chen, X.; Tu, P.; Li, H. The first Chinese case of pediatric subungual melanoma: A case report and literature review. Dermatol. Ther. 2020, 33, e13918. [Google Scholar] [CrossRef]
- Tosti, A.; Piraccini, B.M.; Cagalli, A.; Haneke, E. In situ melanoma of the nail unit in children: Report of two cases in fair-skinned Caucasian chil-dren. Pediatr. Dermatol. 2012, 29, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Scher, R.K.; Lipner, S.R. Pediatric melanomas often mimic benign skin lesions. J. Am. Acad. Dermatol. 2017, 76, e131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellet, J.S. Nail discoloration in pediatric skin of color patients. Pediatr. Dermatol. 2021, 38 (Suppl. S2), 37–41. [Google Scholar] [CrossRef] [PubMed]
- Iorizzo, M.; Tosti, A.; Di Chiacchio, N.; Hirata, S.H.; Misciali, C.; Michalany, N.; Domiguez, J.; Toussaint, S. Nail melanoma in children: Differential diagnosis and management. Dermatol. Surg. 2008, 34, 974–978. [Google Scholar] [CrossRef] [PubMed]
- Piraccini, B.M.; Dika, E.; Fanti, P.A. Tips for diagnosis and treatment of nail pigmentation with practical algorithm. Dermatol. Clin. 2015, 33, 185–195. [Google Scholar] [CrossRef]
- Bellet, J.S. Pediatric Nail Disorders. Dermatol. Clin. 2021, 39, 231–243. [Google Scholar] [CrossRef]
- Goettmann-Bonvallot, S.; André, J.; Belaich, S. Longitudinal melanonychia in children: A clinical and histopathologic study of 40 cases. J. Am. Acad. Dermatol. 1999, 41, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Cooper, C.; Arva, N.C.; Lee, C.; Yélamos, O.; Obregon, R.; Sholl, L.M.; Wagner, A.; Shen, L.; Guitart, J.; Gerami, P. A clinical, histopathologic, and outcome study of melanonychia striata in childhood. J. Am. Acad. Dermatol. 2015, 72, 773–779. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.K.; Seo, S.B.; Jung, J.Y.; Shin, Y.S.; Cho, E.B.; Park, E.J.; Kim, K.J. Longitudinal melanonychia in childhood: A clinical and histopathological review of Korean patients. Eur. J. Dermatol. 2017, 27, 275–280. [Google Scholar] [CrossRef]
- Khatri, S.S.; Wang, M.; Harms, K.L.; Durham, A.B.; Johnson, T.M.; Nazarian, R.M.; Harms, P.W.; Fullen, D.R.; Andea, A.A.; Chan, M.P. Subungual atypical lentiginous melanocytic proliferations in children and adolescents: A clinicopathologic study. J. Am. Acad. Dermatol. 2018, 79, 327–336.e2. [Google Scholar] [CrossRef]
- Smith, R.J.; Rubin, A.I. Pediatric nail disorders: A review. Curr. Opin. Pediatr. 2020, 32, 506–515. [Google Scholar] [CrossRef]
- Bonamonte, D.; Arpaia, N.; Cimmino, A.; Vestita, M. In situ melanoma of the nail unit presenting as a rapid growing longitudinal melanonychia in a 9-year-old white boy. Dermatol. Surg. 2014, 40, 1154–1157. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Lim, Y.; Park, J.-H.; Lee, J.H.; Jang, K.-T.; Kwon, E.J.; Lee, D.-Y. Clinicopathologic features of 28 cases of nail matrix nevi (NMNs) in Asians: Comparison between children and adults. J. Am. Acad. Dermatol. 2018, 78, 479–489. [Google Scholar] [CrossRef] [PubMed]
- Ohn, J.; Choe, Y.S.; Mun, J.-H. Dermoscopic features of nail matrix nevus (NMN) in adults and children: A comparative analysis. J. Am. Acad. Dermatol. 2016, 75, 535–540. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Surgical |
| Digit Amputation |
| En Bloc Excision |
| Mohs Micrographic Surgery |
| Targeted Therapies |
| Tyrosine Kinase Inhibitors |
| Dasatinib |
| Imatinib mesylate |
| Nilotinib |
| Sunitinib |
| High-dose interferon alfa-2b |
| BRAF Inhibitors |
| Vemurafenib |
| Dabrafenib |
| Encorafenib |
| MEK Inhibitors |
| Trametinib |
| Cobimetinib |
| Immunotherapies |
| PD-1 Inhibitors |
| Nivolumab |
| Pembrolizumab |
| Toripalimab |
| CTLA-4 Inhibitors |
| Ipilimumab |
| Tremelimumab |
| Therapy | #Studies | ORR, % | DCR, % | mOS, Months | mPFS, Months |
|---|---|---|---|---|---|
| CTLA-4 Inhibitors | |||||
| Ipilimumab | 7 | 0–25.0 | 7.1–29.8 | 7.16–95.0 | 2.1–2.73 |
| Tremelimumab | 1 | 10.7 | UK | 12.6 | UK |
| PD-1 Inhibitors | |||||
| Nivolumab | 2 | 19.0 | UK | 14.03–25.8 | 6.56 |
| Pembrolizumab | 3 | 15.8–25.0 | 35.7–38.2 | 12.1 | 2.8 |
| Toripalimab | 2 | 14.0–23.1 | 46.2–57.5 | 16.9 | 3.2 |
| Tyrosine Kinase Inhibitors | |||||
| Dasatinib | 2 | UK | UK | 12.6–21.1 | 1.84–2.8 |
| Imatinib mesylate | 3 | 22.0 | 53.5 | 7.5–14.0 | 3.5 |
| Nilotinib | 5 | 16.7–26.2 | 47.6–77.8 | 4.3–18.0 | 2.5–4.2 |
| Sunitinib | 2 | 8.0 | 44.0 | 7.7 | UK |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conway, J.; Bellet, J.S.; Rubin, A.I.; Lipner, S.R. Adult and Pediatric Nail Unit Melanoma: Epidemiology, Diagnosis, and Treatment. Cells 2023, 12, 964. https://doi.org/10.3390/cells12060964
Conway J, Bellet JS, Rubin AI, Lipner SR. Adult and Pediatric Nail Unit Melanoma: Epidemiology, Diagnosis, and Treatment. Cells. 2023; 12(6):964. https://doi.org/10.3390/cells12060964
Chicago/Turabian StyleConway, Jade, Jane S. Bellet, Adam I. Rubin, and Shari R. Lipner. 2023. "Adult and Pediatric Nail Unit Melanoma: Epidemiology, Diagnosis, and Treatment" Cells 12, no. 6: 964. https://doi.org/10.3390/cells12060964