
An Updated Review of Hypertrophic Scarring

 , and
, and
Abstract
:1. Introduction
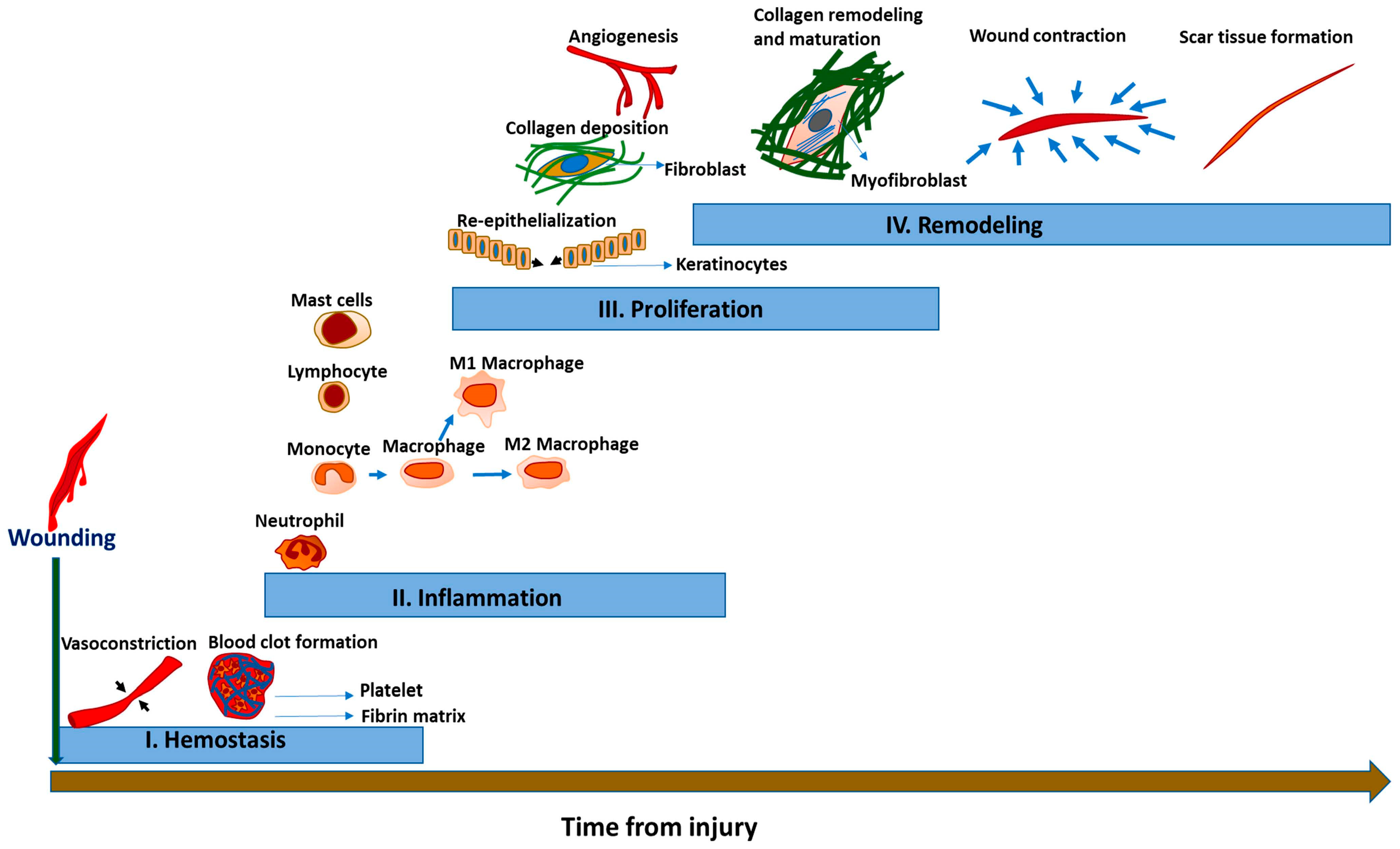
2. Overview of Normal Wound Healing
2.1. Phase 1: Hemostasis
2.2. Phase 2: Inflammation
2.3. Phase 3: Proliferation
2.4. Phase 4: Remodeling
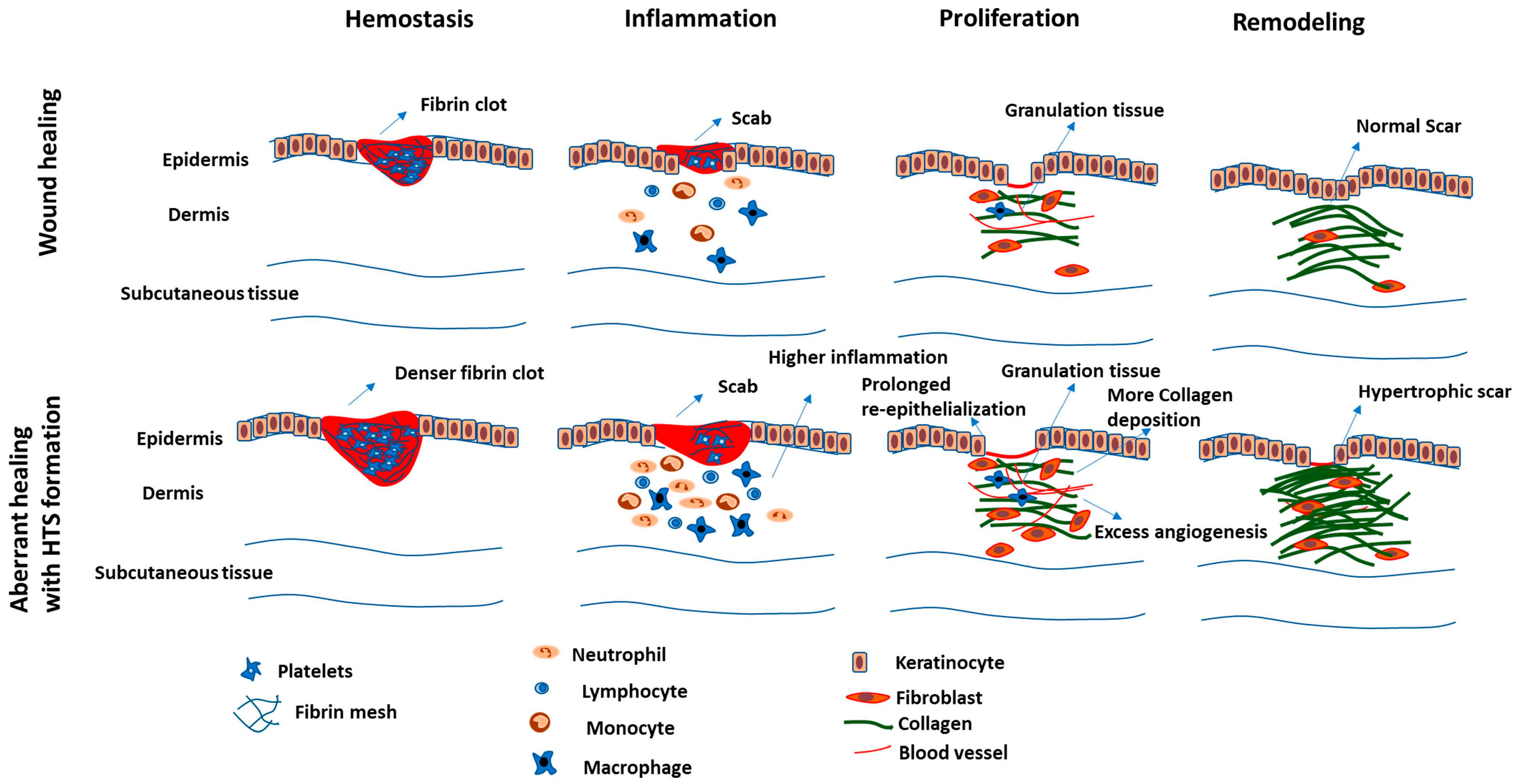
3. Hypertrophic Scarring Associated with Wound Healing Phases
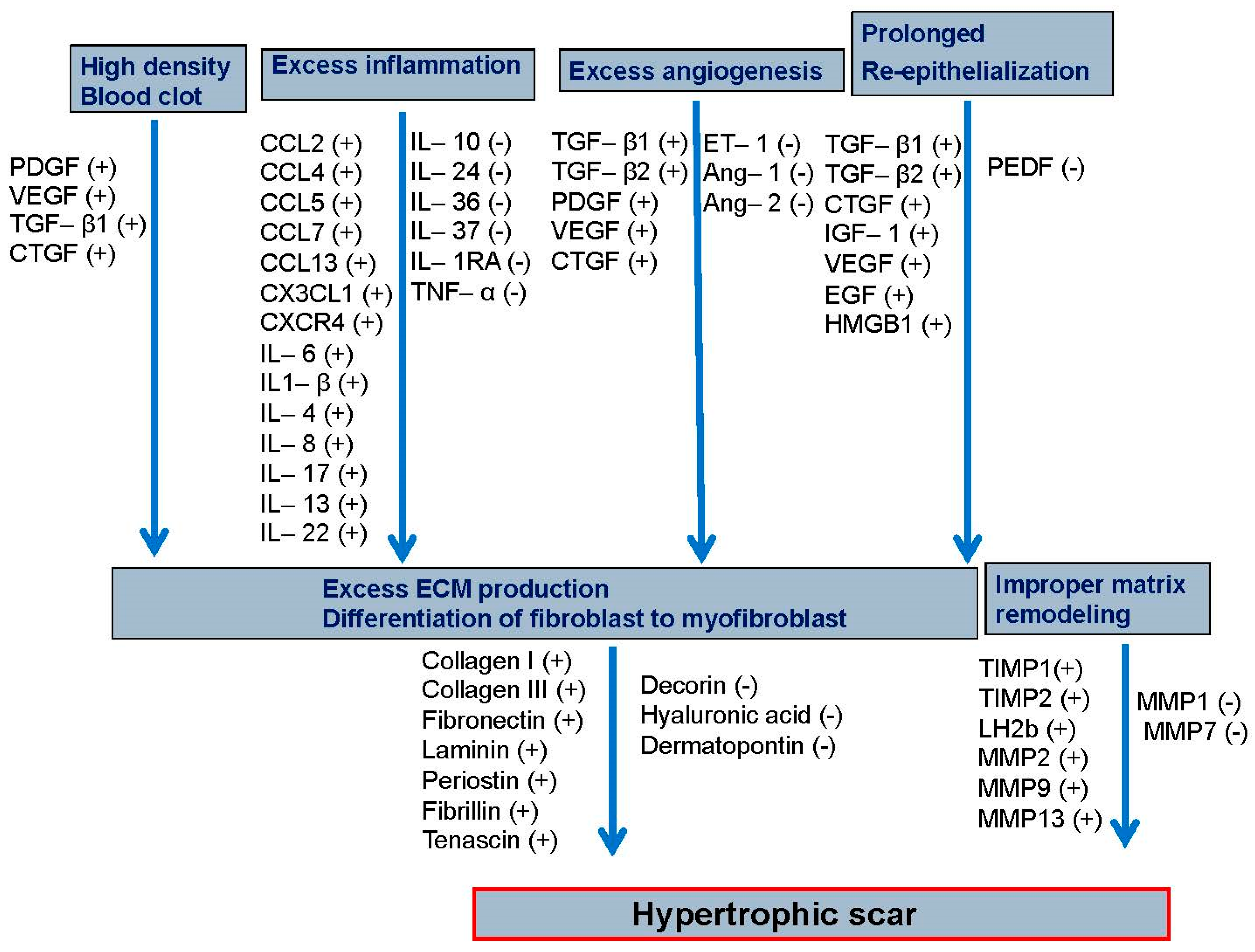
3.1. Phase 1: Hemostasis
3.2. Phase 2: Inflammation
3.3. Phase 3: Proliferation
3.4. Phase 4: Remodeling
4. Animal Models of Hypertrophic Scarring
5. Conventional and Emerging Treatments for Hypertrophic Scarring
5.1. Conventional Therapies
5.2. Emerging Treatments
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gurtner, G.C.; Werner, S.; Barrandon, Y.; Longaker, M.T. Wound repair and regeneration. Nature 2008, 453, 314–321. [Google Scholar] [CrossRef]
- Diegelmann, R.F.; Evans, M.C. Wound healing: An overview of acute, fibrotic and delayed healing. Front. Biosci. 2004, 9, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, R.; Akita, S.; Akaishi, S.; Aramaki-Hattori, N.; Dohi, T.; Hayashi, T.; Kishi, K.; Kono, T.; Matsumura, H.; Muneuchi, G. Diagnosis and treatment of keloids and hypertrophic scars—Japan scar workshop consensus document 2018. Burn. Trauma 2019, 7, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Limandjaja, G.C.; Niessen, F.B.; Scheper, R.J.; Gibbs, S. Hypertrophic scars and keloids: Overview of the evidence and practical guide for differentiating between these abnormal scars. Exp. Dermatol. 2021, 30, 146–161. [Google Scholar] [CrossRef] [PubMed]
- Marshall, C.D.; Hu, M.S.; Leavitt, T.; Barnes, L.A.; Lorenz, H.P.; Longaker, M.T. Cutaneous scarring: Basic science, current treatments, and future directions. Adv. Wound Care 2018, 7, 29–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawrence, J.W.; Mason, S.T.; Schomer, K.; Klein, M.B. Epidemiology and impact of scarring after burn injury: A systematic review of the literature. J. Burn. Care Res. 2012, 33, 136–146. [Google Scholar] [CrossRef] [PubMed]
- Gauglitz, G.G.; Korting, H.C.; Pavicic, T.; Ruzicka, T.; Jeschke, M.G. Hypertrophic scarring and keloids: Pathomechanisms and current and emerging treatment strategies. Mol. Med. 2011, 17, 113–125. [Google Scholar] [CrossRef]
- Thompson, C.M.; Hocking, A.M.; Honari, S.; Muffley, L.A.; Ga, M.; Gibran, N.S. Genetic risk factors for hypertrophic scar development. J. Burn. Care Res. 2013, 34, 477–482. [Google Scholar] [CrossRef] [Green Version]
- Shu, F.; Liu, H.; Lou, X.; Zhou, Z.; Zhao, Z.; Liu, Y.; Bai, X.; Luo, P.; Zheng, Y.; Xiao, S.; et al. Analysis of the predictors of hypertrophic scarring pain and neuropathic pain after burn. Burns 2022, 48, 1425–1434. [Google Scholar] [CrossRef]
- Mahdavian Delavary, B.; van der Veer, W.M.; Ferreira, J.A.; Niessen, F.B. Formation of hypertrophic scars: Evolution and susceptibility. J. Plast. Surg. Hand Surg. 2012, 46, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Brissett, A.E.; Sherris, D.A. Scar contractures, hypertrophic scars, and keloids. Facial Plast. Surg. 2001, 17, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wu, Z.; Du, Y.; Ogawa, R. The epidemiology of keloids. In Textbook on Scar Management; Springer: Cham, Switzerland, 2020; pp. 29–35. [Google Scholar]
- Kouotou, E.A.; Nansseu, J.R.; Omona Guissana, E.; Mendouga Menye, C.R.; Akpadjan, F.; Tounkara, T.M.; Zoung-Kanyi Bissek, A.C.; Ndjitoyap Ndam, E.C. Epidemiology and clinical features of keloids in Black Africans: A nested case–control study from Yaoundé, Cameroon. Int. J. Derm. 2019, 58, 1135–1140. [Google Scholar] [CrossRef]
- Kwan, P.; Hori, K.; Ding, J.; Tredget, E.E. Scar and contracture: Biological principles. Hand Clin 2009, 25, 511–528. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, H.; Herndon, D. Total Burn Care; Saunders Elsevier: Philadelphia, PA, USA; American Medical Association: Chicago, IL, USA, 2007; pp. 608–619. [Google Scholar]
- Wurzer, P.; Forbes, A.A.; Hundeshagen, G.; Andersen, C.R.; Epperson, K.M.; Meyer, W.J.; Kamolz, L.P.; Branski, L.K.; Suman, O.E.; Herndon, D.N.; et al. Two-year follow-up of outcomes related to scarring and distress in children with severe burns. Disabil. Rehabil. 2017, 39, 1639–1643. [Google Scholar] [CrossRef]
- Aarabi, S.; Longaker, M.T.; Gurtner, G.C. Hypertrophic scar formation following burns and trauma: New approaches to treatment. PLoS Med. 2007, 4, e234. [Google Scholar] [CrossRef]
- Atiyeh, B.; Ibrahim, A. Nonsurgical management of hypertrophic scars: Evidence-based therapies, standard practices, and emerging methods: An update. Aesthetic Plast. Surg. 2020, 44, 1345–1347. [Google Scholar] [CrossRef] [PubMed]
- Brusselaers, N.; Pirayesh, A.; Hoeksema, H.; Verbelen, J.; Blot, S.; Monstrey, S. Burn scar assessment: A systematic review of different scar scales. J. Surg. Res. 2010, 164, e115–e123. [Google Scholar] [CrossRef] [Green Version]
- Elrefaie, A.M.; Salem, R.M.; Faheem, M.H. High-resolution ultrasound for keloids and hypertrophic scar assessment. Lasers Med. Sci. 2020, 35, 379–385. [Google Scholar] [CrossRef]
- Rodrigues, M.; Kosaric, N.; Bonham, C.A.; Gurtner, G.C. Wound Healing: A Cellular Perspective. Physiol. Rev. 2019, 99, 665–706. [Google Scholar] [CrossRef]
- Gale, A.J. Continuing education course #2: Current understanding of hemostasis. Toxicol. Pathol. 2011, 39, 273–280. [Google Scholar] [CrossRef] [Green Version]
- Palta, S.; Saroa, R.; Palta, A. Overview of the coagulation system. Indian J. Anaesth. 2014, 58, 515. [Google Scholar] [CrossRef] [PubMed]
- Martin, P. Wound healing--aiming for perfect skin regeneration. Science 1997, 276, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Singer, A.J.; Clark, R.A. Cutaneous wound healing. N. Engl. J. Med. 1999, 341, 738–746. [Google Scholar] [CrossRef] [PubMed]
- Ellis, S.; Lin, E.J.; Tartar, D. Immunology of wound healing. Curr. Dermatol. Rep. 2018, 7, 350–358. [Google Scholar] [CrossRef] [Green Version]
- Turabelidze, A.; Dipietro, L.A. Inflammation and wound healing. Endod. Top. 2011, 24, 26–38. [Google Scholar] [CrossRef]
- Kolaczkowska, E.; Kubes, P. Neutrophil recruitment and function in health and inflammation. Nat. Rev. Immunol. 2013, 13, 159–175. [Google Scholar] [CrossRef]
- Mittal, M.; Nepal, S.; Tsukasaki, Y.; Hecquet, C.M.; Soni, D.; Rehman, J.; Tiruppathi, C.; Malik, A.B. Neutrophil activation of endothelial cell-expressed TRPM2 mediates transendothelial neutrophil migration and vascular injury. Circ. Res. 2017, 121, 1081–1091. [Google Scholar] [CrossRef]
- Bettinger, D.A.; Pellicane, J.V.; Tarry, W.C.; Yager, D.R.; Diegelmann, R.F.; Lee, R.; Cohen, I.; DeMaria, E.J. The role of inflammatory cytokines in wound healing: Accelerated healing in endotoxin-resistant mice. J. Trauma 1994, 36, 810–813; discussion 813. [Google Scholar] [CrossRef]
- Nosenko, M.; Ambaryan, S.; Drutskaya, M. Proinflammatory cytokines and skin wound healing in mice. Mol. Biol. 2019, 53, 653–664. [Google Scholar] [CrossRef]
- Kim, S.Y.; Nair, M.G. Macrophages in wound healing: Activation and plasticity. Immunol. Cell Biol. 2019, 97, 258–267. [Google Scholar] [CrossRef]
- Kloc, M.; Ghobrial, R.M.; Wosik, J.; Lewicka, A.; Lewicki, S.; Kubiak, J.Z. Macrophage functions in wound healing. J. Tissue Eng. Regen. Med. 2019, 13, 99–109. [Google Scholar] [CrossRef] [Green Version]
- Eming, S.A.; Martin, P.; Tomic-Canic, M. Wound repair and regeneration: Mechanisms, signaling, and translation. Sci. Transl. Med. 2014, 6, 265sr266. [Google Scholar] [CrossRef] [Green Version]
- Kotwal, G.J.; Chien, S. Macrophage differentiation in normal and accelerated wound healing. Macrophages 2017, 62, 353–364. [Google Scholar]
- Demidova-Rice, T.N.; Hamblin, M.R.; Herman, I.M. Acute and impaired wound healing: Pathophysiology and current methods for drug delivery, part 1: Normal and chronic wounds: Biology, causes, and approaches to care. Adv. Ski. Wound Care 2012, 25, 304. [Google Scholar] [CrossRef] [Green Version]
- Duncan, M.R.; Frazier, K.S.; Abramson, S.; Williams, S.; Klapper, H.; Huang, X.; Grotendorst, G.R. Connective tissue growth factor mediates transforming growth factor beta-induced collagen synthesis: Down-regulation by cAMP. FASEB J. 1999, 13, 1774–1786. [Google Scholar] [CrossRef] [Green Version]
- Barker, T.H.; Engler, A.J. The provisional matrix: Setting the stage for tissue repair outcomes. Matrix Biol. 2017, 60, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Broughton, G.; Janis, J.E.; Attinger, C.E. The basic science of wound healing. Plast Reconstr Surg 2006, 117, 12S–34S. [Google Scholar] [CrossRef] [PubMed]
- Häkkinen, L.; Larjava, H.; Koivisto, L. Granulation tissue formation and remodeling. Endod. Top. 2011, 24, 94–129. [Google Scholar] [CrossRef]
- Rousselle, P.; Braye, F.; Dayan, G. Re-epithelialization of adult skin wounds: Cellular mechanisms and therapeutic strategies. Adv. Drug Deliv. Rev. 2019, 146, 344–365. [Google Scholar] [CrossRef]
- Pastar, I.; Stojadinovic, O.; Yin, N.C.; Ramirez, H.; Nusbaum, A.G.; Sawaya, A.; Patel, S.B.; Khalid, L.; Isseroff, R.R.; Tomic-Canic, M. Epithelialization in Wound Healing: A Comprehensive Review. Adv. Wound Care 2014, 3, 445–464. [Google Scholar] [CrossRef] [Green Version]
- DiPietro, L.A. Angiogenesis and wound repair: When enough is enough. J. Leukoc. Biol. 2016, 100, 979–984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grotendorst, G.; Grotendorst, C.; Gilman, T. Production of growth factors (PDGF & TGF-beta) at the site of tissue repair. Prog. Clin. Biol. Res. 1988, 266, 47–54. [Google Scholar] [PubMed]
- Uutela, M.; Wirzenius, M.; Paavonen, K.; Rajantie, I.; He, Y.; Karpanen, T.; Lohela, M.; Wiig, H.; Salven, P.; Pajusola, K. PDGF-D induces macrophage recruitment, increased interstitial pressure, and blood vessel maturation during angiogenesis. Blood 2004, 104, 3198–3204. [Google Scholar] [CrossRef] [PubMed]
- Nissen, N.N.; Polverini, P.J.; Gamelli, R.L.; DiPietro, L.A. Basic fibroblast growth factor mediates angiogenic activity in early surgical wounds. Surgery 1996, 119, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Pardali, E.; Goumans, M.-J.; ten Dijke, P. Signaling by members of the TGF-β family in vascular morphogenesis and disease. Trends Cell Biol. 2010, 20, 556–567. [Google Scholar] [CrossRef] [PubMed]
- Sorg, H.; Tilkorn, D.J.; Hager, S.; Hauser, J.; Mirastschijski, U. Skin wound healing: An update on the current knowledge and concepts. Eur. Surg. Res. 2017, 58, 81–94. [Google Scholar] [CrossRef]
- Diller, R.B.; Tabor, A.J. The role of the extracellular matrix (ECM) in wound healing: A review. Biomimetics 2022, 7, 87. [Google Scholar] [CrossRef]
- Xue, M.; Jackson, C.J. Extracellular matrix reorganization during wound healing and its impact on abnormal scarring. Adv. Wound Care 2015, 4, 119–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reinke, J.M.; Sorg, H. Wound repair and regeneration. Eur. Surg. Res. 2012, 49, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Shanmugam, V.K.; Fernandez, S.J.; Evans, K.K.; McNish, S.; Banerjee, A.N.; Couch, K.S.; Mete, M.; Shara, N. Postoperative wound dehiscence: Predictors and associations. Wound Repair Regen. 2015, 23, 184–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spiliotis, J.; Tsiveriotis, K.; Datsis, A.D.; Vaxevanidou, A.; Zacharis, G.; Giafis, K.; Kekelos, S.; Rogdakis, A. Wound dehiscence: Is still a problem in the 21th century: A retrospective study. World J. Emerg. Surg. 2009, 4, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Li, B.; Wang, J.H.-C. Fibroblasts and myofibroblasts in wound healing: Force generation and measurement. J. Tissue Viability 2011, 20, 108–120. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.C.; Zhao, W.Y.; Cao, Y.; Liu, Y.Q.; Sun, Q.; Shi, P.; Cai, J.Q.; Shen, X.Z.; Tan, W.Q. The Roles of Inflammation in Keloid and Hypertrophic Scars. Front. Immunol. 2020, 11, 603187. [Google Scholar] [CrossRef]
- Bellemare, J.; Roberge, C.J.; Bergeron, D.; Lopez-Vallé, C.A.; Roy, M.; Moulin, V.J. Epidermis promotes dermal fibrosis: Role in the pathogenesis of hypertrophic scars. J. Pathol. A J. Pathol. Soc. Great Br. Irel. 2005, 206, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Molina, E.A.; Hartmann, B.; Oliver, M.A.; Kirkpatrick, L.D.; Keyloun, J.W.; Moffatt, L.T.; Shupp, J.W.; Travis, T.E.; Carney, B.C. Angiogenic gene characterization and vessel permeability of dermal microvascular endothelial cells isolated from burn hypertrophic scar. Sci. Rep. 2022, 12, 12222. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, P.; Calitz, C.; Pavlović, N.; Binet, F.; Solbak, S.M.Ø.; Danielson, U.H.; Kreuger, J.; Heindryckx, F.; Gerwins, P. Fibrin fragment E potentiates TGF-β-induced myofibroblast activation and recruitment. Cell. Signal. 2020, 72, 109661. [Google Scholar] [CrossRef]
- Wang, Y.; Guerrero-Juarez, C.F.; Qiu, Y.; Du, H.; Chen, W.; Figueroa, S.; Plikus, M.V.; Nie, Q. A multiscale hybrid mathematical model of epidermal-dermal interactions during skin wound healing. Exp. Derm. 2019, 28, 493–502. [Google Scholar] [CrossRef] [PubMed]
- Werner, S.; Grose, R. Regulation of wound healing by growth factors and cytokines. Physiol. Rev. 2003, 83, 835–870. [Google Scholar] [CrossRef] [Green Version]
- Nam, S.M.; Kim, Y.B. The effects of platelet-rich plasma on hypertrophic scars fibroblasts. Int. Wound J. 2018, 15, 547–554. [Google Scholar] [CrossRef]
- Agrawal, A.; Ding, J.; Agrawal, B.; Kwan, P.O.; Tredget, E.E. Stimulation of toll-like receptor pathways by burn eschar tissue as a possible mechanism for hypertrophic scarring. Wound Repair Regen. 2021, 29, 810–819. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Hori, K.; Ding, J.; Huang, Y.; Kwan, P.; Ladak, A.; Tredget, E.E. Toll-like receptors expressed by dermal fibroblasts contribute to hypertrophic scarring. J. Cell Physiol. 2011, 226, 1265–1273. [Google Scholar] [CrossRef]
- Williams, H.; Suda, S.; Dervish, S.; Yap, Y.T.; Holland, A.J.; Medbury, H.J. Monocyte M1/M2 profile is altered in paediatric burn patients with hypertrophic scarring. Wound Repair Regen. 2021, 29, 996–1005. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.; Li, H.; Xia, W. The role of Th1/Th2 cell chemokine expression in hypertrophic scar. Int. Wound J. 2020, 17, 197–205. [Google Scholar] [CrossRef] [PubMed]
- van den Broek, L.J.; van der Veer, W.M.; de Jong, E.H.; Gibbs, S.; Niessen, F.B. Suppressed inflammatory gene expression during human hypertrophic scar compared to normotrophic scar formation. Exp. Derm. 2015, 24, 623–629. [Google Scholar] [CrossRef]
- Ding, J.; Hori, K.; Zhang, R.; Marcoux, Y.; Honardoust, D.; Shankowsky, H.A.; Tredget, E.E. Stromal cell-derived factor 1 (SDF-1) and its receptor CXCR4 in the formation of postburn hypertrophic scar (HTS). Wound Repair Regen. 2011, 19, 568–578. [Google Scholar] [CrossRef] [PubMed]
- Henry, G.; Garner, W.L. Inflammatory mediators in wound healing. Surg. Clin. N. Am. 2003, 83, 483–507. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Li, B.; Zhao, M. Therapeutic Strategies by Regulating Interleukin Family to Suppress Inflammation in Hypertrophic Scar and Keloid. Front. Pharm. 2021, 12, 667763. [Google Scholar] [CrossRef]
- Butzelaar, L.; Schooneman, D.P.; Soykan, E.A.; Talhout, W.; Ulrich, M.M.; van den Broek, L.J.; Gibbs, S.; Beelen, R.H.; Mink van der Molen, A.B.; Niessen, F.B. Inhibited early immunologic response is associated with hypertrophic scarring. Exp. Derm. 2016, 25, 797–804. [Google Scholar] [CrossRef]
- Roy, R.; Zayas, J.; Mohamed, M.F.; Aboonabi, A.; Delgado, K.; Wallace, J.; Bayat, M.; Kuzel, T.M.; Reiser, J.; Shafikhani, S.H. IL-10 Dysregulation Underlies Chemokine Insufficiency, Delayed Macrophage Response, and Impaired Healing in Diabetic Wounds. J. Investig. Dermatol. 2022, 142, 692–704.e614. [Google Scholar] [CrossRef]
- Roy, R.; Zayas, J.; Singh, S.K.; Delgado, K.; Wood, S.J.; Mohamed, M.F.; Frausto, D.M.; Estupinian, R.; Giurini, E.F.; Kuzel, T.M.; et al. Overriding impaired FPR chemotaxis signaling in diabetic neutrophil stimulates infection control in murine diabetic wound. eLife 2022, 11, e72071. [Google Scholar] [CrossRef]
- Wood, S.; Jayaraman, V.; Huelsmann, E.J.; Bonish, B.; Burgad, D.; Sivaramakrishnan, G.; Qin, S.; Dipietro, L.A.; Zloza, A.; Zhang, C.; et al. Pro-inflammatory chemokine CCL2 (MCP-1) promotes healing in diabetic wounds by restoring the macrophage response. PLoS ONE 2014, 9, e91574. [Google Scholar] [CrossRef] [Green Version]
- Goldufsky, J.; Wood, S.J.; Jayaraman, V.; Majdobeh, O.; Chen, L.; Qin, S.; Zhang, C.; DiPietro, L.A.; Shafikhani, S.H. Pseudomonas aeruginosa uses T3SS to inhibit diabetic wound healing. Wound Repair Regen. 2015, 23, 557–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaplanski, G.; Marin, V.; Montero-Julian, F.; Mantovani, A.; Farnarier, C. IL-6: A regulator of the transition from neutrophil to monocyte recruitment during inflammation. Trends Immunol. 2003, 24, 25–29. [Google Scholar] [CrossRef]
- Fernando, M.R.; Reyes, J.L.; Iannuzzi, J.; Leung, G.; McKay, D.M. The pro-inflammatory cytokine, interleukin-6, enhances the polarization of alternatively activated macrophages. PLoS ONE 2014, 9, e94188. [Google Scholar] [CrossRef] [Green Version]
- Juhl, P.; Bondesen, S.; Hawkins, C.L.; Karsdal, M.A.; Bay-Jensen, A.C.; Davies, M.J.; Siebuhr, A.S. Dermal fibroblasts have different extracellular matrix profiles induced by TGF-β, PDGF and IL-6 in a model for skin fibrosis. Sci. Rep. 2020, 10, 17300. [Google Scholar] [CrossRef] [PubMed]
- Xue, H.; McCauley, R.L.; Zhang, W.; Martini, D.K. Altered interleukin-6 expression in fibroblasts from hypertrophic burn scars. J. Burn. Care Rehabil. 2000, 21, 142–146. [Google Scholar] [CrossRef]
- Ray, S.; Ju, X.; Sun, H.; Finnerty, C.C.; Herndon, D.N.; Brasier, A.R. The IL-6 trans-signaling-STAT3 pathway mediates ECM and cellular proliferation in fibroblasts from hypertrophic scar. J. Investig. Dermatol. 2013, 133, 1212–1220. [Google Scholar] [CrossRef] [Green Version]
- Kwan, P.O.; Ding, J.; Tredget, E.E. Serum Decorin, Interleukin-1β, and Transforming Growth Factor-β Predict Hypertrophic Scarring Postburn. J. Burn Care Res. 2016, 37, 356–366. [Google Scholar] [CrossRef]
- Zhang, J.; Qiao, Q.; Liu, M.; He, T.; Shi, J.; Bai, X.; Zhang, Y.; Li, Y.; Cai, W.; Han, S.; et al. IL-17 Promotes Scar Formation by Inducing Macrophage Infiltration. Am. J. Pathol. 2018, 188, 1693–1702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, J.K.; Austin, E.; Huang, A.; Mamalis, A.; Jagdeo, J. The IL-4/IL-13 axis in skin fibrosis and scarring: Mechanistic concepts and therapeutic targets. Arch. Dermatol. Res. 2020, 312, 81–92. [Google Scholar] [CrossRef]
- Shi, J.; Li, J.; Guan, H.; Cai, W.; Bai, X.; Fang, X.; Hu, X.; Wang, Y.; Wang, H.; Zheng, Z.; et al. Anti-fibrotic actions of interleukin-10 against hypertrophic scarring by activation of PI3K/AKT and STAT3 signaling pathways in scar-forming fibroblasts. PLoS ONE 2014, 9, e98228. [Google Scholar] [CrossRef]
- Shi, J.; Shi, S.; Xie, W.; Zhao, M.; Li, Y.; Zhang, J.; Li, N.; Bai, X.; Cai, W.; Hu, X.; et al. IL-10 alleviates lipopolysaccharide-induced skin scarring via IL-10R/STAT3 axis regulating TLR4/NF-κB pathway in dermal fibroblasts. J. Cell Mol. Med. 2021, 25, 1554–1567. [Google Scholar] [CrossRef]
- Ma, L.; Hua, L.; Yu, W.; Ke, L.; Li, L. TSG-6 inhibits hypertrophic scar fibroblast proliferation by regulating IRE1α/TRAF2/NF-κB signalling. Int. Wound J. 2022. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.-X.; Li, S.-Y.; Chen, M.-L.; He, L.-R. The role of altered fatty acid in pathological scars and their dermal fibroblasts. Chin. J. Traumatol. 2022, 25, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Chen, M.; He, L. To Explore Ideas From the Altered Metabolites: The Metabolomics of Pathological Scar. J. Craniofacial Surg. 2022, 33, 1619–1625. [Google Scholar] [CrossRef] [PubMed]
- Gromovsky, A.D.; Schugar, R.C.; Brown, A.L.; Helsley, R.N.; Burrows, A.C.; Ferguson, D.; Zhang, R.; Sansbury, B.E.; Lee, R.G.; Morton, R.E. Δ-5 fatty acid desaturase FADS1 impacts metabolic disease by balancing proinflammatory and proresolving lipid mediators. Arterioscler. Thromb. Vasc. Biol. 2018, 38, 218–231. [Google Scholar] [CrossRef] [Green Version]
- Fritsche, K.L. The science of fatty acids and inflammation. Adv. Nutr. 2015, 6, 293S–301S. [Google Scholar] [CrossRef] [Green Version]
- Vinolo, M.A.; Rodrigues, H.G.; Nachbar, R.T.; Curi, R. Regulation of inflammation by short chain fatty acids. Nutrients 2011, 3, 858–876. [Google Scholar] [CrossRef] [Green Version]
- van der Veer, W.M.; Niessen, F.B.; Ferreira, J.A.; Zwiers, P.J.; de Jong, E.H.; Middelkoop, E.; Molema, G. Time course of the angiogenic response during normotrophic and hypertrophic scar formation in humans. Wound Repair Regen. 2011, 19, 292–301. [Google Scholar] [CrossRef]
- Machesney, M.; Tidman, N.; Waseem, A.; Kirby, L.; Leigh, I. Activated keratinocytes in the epidermis of hypertrophic scars. Am J. Pathol. 1998, 152, 1133–1141. [Google Scholar]
- Ma, L.; Gan, C.; Huang, Y.; Wang, Y.; Luo, G.; Wu, J. Comparative proteomic analysis of extracellular matrix proteins secreted by hypertrophic scar with normal skin fibroblasts. Burn. Trauma 2014, 2, 76–83. [Google Scholar] [CrossRef] [Green Version]
- Lian, N.; Li, T. Growth factor pathways in hypertrophic scars: Molecular pathogenesis and therapeutic implications. Biomed Pharm. 2016, 84, 42–50. [Google Scholar] [CrossRef]
- Eremenko, E.; Ding, J.; Kwan, P.; Tredget, E.E. The Biology of Extracellular Matrix Proteins in Hypertrophic Scarring. Adv. Wound Care 2022, 11, 234–254. [Google Scholar] [CrossRef]
- Varkey, M.; Ding, J.; Tredget, E.E. Differential collagen-glycosaminoglycan matrix remodeling by superficial and deep dermal fibroblasts: Potential therapeutic targets for hypertrophic scar. Biomaterials 2011, 32, 7581–7591. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Gu, S.; Liu, C.; Zhang, L.; Zhang, Z.; Zhao, Y.; Khoong, Y.; Li, H.; Gao, Y.; Liu, Y. CD39+ fibroblasts enhance myofibroblast activation by promoting IL-11 secretion in hypertrophic scars. J. Investig. Dermatol. 2022, 142, 1065–1076.e1019. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Wang, X.F.; Wang, Z.C.; Lou, D.; Fang, Q.Q.; Hu, Y.Y.; Zhao, W.Y.; Zhang, L.Y.; Wu, L.H.; Tan, W.Q. Current potential therapeutic strategies targeting the TGF-β/Smad signaling pathway to attenuate keloid and hypertrophic scar formation. Biomed. Pharm. 2020, 129, 110287. [Google Scholar] [CrossRef] [PubMed]
- Fang, X.; Hu, X.; Zheng, Z.; Tao, K.; Wang, H.; Guan, H.; Shi, J.; Ji, P.; Cai, W.; Bai, X.; et al. Smad interacting protein 1 influences transforming growth factor-β. J. Mol. Histol. 2019, 50, 503–514. [Google Scholar] [CrossRef]
- Li, X.P.; Liu, P.; Li, Y.F.; Zhang, G.L.; Zeng, D.S.; Liu, D.L. LPS induces activation of the TLR4 pathway in fibroblasts and promotes skin scar formation through collagen I and TGF-β in skin lesions. Int. J. Clin. Exp. Pathol. 2019, 12, 2121–2129. [Google Scholar]
- Ogawa, R.; Akaishi, S. Endothelial dysfunction may play a key role in keloid and hypertrophic scar pathogenesis–keloids and hypertrophic scars may be vascular disorders. Med. Hypotheses 2016, 96, 51–60. [Google Scholar] [CrossRef]
- Laberge, A.; Merjaneh, M.; Arif, S.; Larochelle, S.; Moulin, V.J. Shedding of proangiogenic microvesicles from hypertrophic scar myofibroblasts. Exp. Derm. 2021, 30, 112–120. [Google Scholar] [CrossRef]
- Wilgus, T.A. Vascular endothelial growth factor and cutaneous scarring. Adv. Wound Care 2019, 8, 671–678. [Google Scholar] [CrossRef]
- Li, B.; Gao, C.; Diao, J.S.; Wang, D.L.; Chu, F.F.; Li, Y.; Wang, G.; Guo, S.Z.; Xia, W. Aberrant Notch signalling contributes to hypertrophic scar formation by modulating the phenotype of keratinocytes. Exp Derm. 2016, 25, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Yuan, F.L.; Sun, Z.L.; Feng, Y.; Liu, S.Y.; Du, Y.; Yu, S.; Yang, M.L.; Lv, G.Z. Epithelial-mesenchymal transition in the formation of hypertrophic scars and keloids. J. Cell Physiol. 2019, 234, 21662–21669. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Yu, J.; Xu, Y.; Chen, L.; Zhou, F.; Zhai, Q.; Wu, J.; Shu, B.; Qi, S. Epidermal HMGB1 activates dermal fibroblasts and causes hypertrophic scar formation in reduced hydration. J. Investig. Dermatol. 2018, 138, 2322–2332. [Google Scholar] [CrossRef] [Green Version]
- Ma, D.; Chen, L.; Shi, J.; Zhao, Y.; Vasani, S.; Chen, K.; Romana-Souza, B.; Henkin, J.; DiPietro, L.A. Pigment epithelium-derived factor attenuates angiogenesis and collagen deposition in hypertrophic scars. Wound Repair Regen. 2020, 28, 684–695. [Google Scholar] [CrossRef] [PubMed]
- Eto, H.; Suga, H.; Aoi, N.; Kato, H.; Kuno, S.; Tabata, Y.; Yoshimura, K. Therapeutic potential of fibroblast growth factor-2 for hypertrophic scars: Upregulation of MMP-1 and HGF expression. Lab. Investig. 2012, 92, 214–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spyrou, G.E.; Naylor, I.L. The effect of basic fibroblast growth factor on scarring. Br. J. Plast. Surg. 2002, 55, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Ulrich, D.; Ulrich, F.; Unglaub, F.; Piatkowski, A.; Pallua, N. Matrix metalloproteinases and tissue inhibitors of metalloproteinases in patients with different types of scars and keloids. J. Plast. Reconstr. Aesthetic Surg. 2010, 63, 1015–1021. [Google Scholar] [CrossRef]
- Oliveira, G.V.; Hawkins, H.K.; Chinkes, D.; Burke, A.; Tavares, A.L.; Ramos-e-Silva, M.; Albrecht, T.B.; Kitten, G.T.; Herndon, D.N. Hypertrophic versus non hypertrophic scars compared by immunohistochemistry and laser confocal microscopy: Type I and III collagens. Int. Wound J. 2009, 6, 445–452. [Google Scholar] [CrossRef]
- Moulin, V.; Larochelle, S.; Langlois, C.; Thibault, I.; Lopez-Vallé, C.A.; Roy, M. Normal skin wound and hypertrophic scar myofibroblasts have differential responses to apoptotic inductors. J. Cell Physiol. 2004, 198, 350–358. [Google Scholar] [CrossRef]
- Sidgwick, G.P.; Bayat, A. Extracellular matrix molecules implicated in hypertrophic and keloid scarring. J. Eur. Acad Derm. Venereol. 2012, 26, 141–152. [Google Scholar] [CrossRef] [PubMed]
- Gabbiani, G. The myofibroblast in wound healing and fibrocontractive diseases. J. Pathol. 2003, 200, 500–503. [Google Scholar] [CrossRef] [PubMed]
- Junker, J.P.; Kratz, C.; Tollbäck, A.; Kratz, G. Mechanical tension stimulates the transdifferentiation of fibroblasts into myofibroblasts in human burn scars. Burns 2008, 34, 942–946. [Google Scholar] [CrossRef] [PubMed]
- Darby, I.A.; Laverdet, B.; Bonté, F.; Desmoulière, A. Fibroblasts and myofibroblasts in wound healing. Clin. Cosmet. Investig. Dermatol. 2014, 7, 301. [Google Scholar] [PubMed] [Green Version]
- Lee, D.E.; Trowbridge, R.M.; Ayoub, N.T.; Agrawal, D.K. High-mobility Group Box Protein-1, Matrix Metalloproteinases, and Vitamin D in Keloids and Hypertrophic Scars. Plast. Reconstr. Surg. Glob. Open 2015, 3, e425. [Google Scholar] [CrossRef]
- Travis, T.E.; Ghassemi, P.; Prindeze, N.J.; Moffatt, L.T.; Carney, B.C.; Alkhalil, A.; Ramella-Roman, J.C.; Shupp, J.W. Matrix Metalloproteinases Are Differentially Regulated and Responsive to Compression Therapy in a Red Duroc Model of Hypertrophic Scar. Eplasty 2018, 18, e1. [Google Scholar]
- Keskin, E.S.; Keskin, E.R.; Öztürk, M.B.; Çakan, D. The Effect of MMP-1 on Wound Healing and Scar Formation. Aesthetic Plast Surg. 2021, 45, 2973–2979. [Google Scholar] [CrossRef]
- McArdle, C.; Abbah, S.A.; Bhowmick, S.; Collin, E.; Pandit, A. Localized temporal co-delivery of interleukin 10 and decorin genes using amediated by collagen-based biphasic scaffold modulates the expression of TGF-β1/β2 in a rabbit ear hypertrophic scarring model. Biomater. Sci. 2021, 9, 3136–3149. [Google Scholar] [CrossRef]
- Ying, M.; Chen, Y.; Yuan, B. Knockdown of lysyl oxidase like 1 inhibits the proliferation and pro-fibrotic effects of transforming growth factor-β1-induced hypertrophic scar fibroblasts. Can. J. Physiol. Pharm. 2021, 99, 1272–1279. [Google Scholar] [CrossRef]
- Raktoe, R.S.; Rietveld, M.H.; Out-Luiting, J.J.; Kruithof-de Julio, M.; van Zuijlen, P.P.; van Doorn, R.; El Ghalbzouri, A. The effect of TGFβRI inhibition on fibroblast heterogeneity in hypertrophic scar 2D in vitro models. Burns 2021, 47, 1563–1575. [Google Scholar] [CrossRef]
- Moulin, V.J. Three-dimensional model of hypertrophic scar using a tissue-engineering approach. In Myofibroblasts; Springer: Berlin/Heidelberg, Germany, 2021. [Google Scholar]
- Sun, Q.; Yu, E.T.; Zhou, Y.; Tong, S.; Sun, X.; Li, K.Z.; Lv, M.Z.; Guo, S. The Effects of Timing of Postoperative Radiotherapy on Hypertrophic Scar in a Rabbit Model. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2020, 26, e921263. [Google Scholar] [CrossRef]
- Huang, J.; Chen, J.; Wo, Y.; Wang, X.; Zhang, Y.; Chen, X.; Zhang, Z.; Biskup, E. CO2 Fractional Laser Combined with 5-Fluorouracil Ethosomal Gel Treatment of Hypertrophic Scar Macro-, Microscopic, and Molecular Mechanism of Action in a Rabbit Animal Model. Rejuvenation Res. 2021, 24, 131–138. [Google Scholar] [CrossRef]
- Tunca, M.; Gamsızkan, M.; Yürekli, A.; Alp Göksel, B.; Fuat Çiçek, A.; Çalışkan, E. Cryosurgery to remove perichondrium for the rabbit ear hypertrophic scar model: A simplified method. Acta Dermatovenerol. Alp. Pannonica Adriat. 2019, 28, 57–59. [Google Scholar] [CrossRef]
- Friedrich, E.E.; Niknam-Bienia, S.; Xie, P.; Jia, S.X.; Hong, S.J.; Mustoe, T.A.; Galiano, R.D. Thermal injury model in the rabbit ear with quantifiable burn progression and hypertrophic scar. Wound Repair Regen. 2017, 25, 327–337. [Google Scholar] [CrossRef]
- Zu, W.; Jiang, B.; Liu, H. Establishment of a long-term hypertrophic scar model by injection of anhydrous alcohol: A rabbit model. Int. J. Exp. Pathol. 2021, 102, 105–112. [Google Scholar] [CrossRef]
- Alrobaiea, S.M.; Ding, J.; Ma, Z.; Tredget, E.E. A novel nude mouse model of hypertrophic scarring using scratched full thickness human skin grafts. Adv. Wound Care 2016, 5, 299–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davidson, J.M.; Yu, F.; Opalenik, S.R. Splinting Strategies to Overcome Confounding Wound Contraction in Experimental Animal Models. Adv. Wound Care 2013, 2, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Son, D.O.; Hinz, B. A Rodent Model of Hypertrophic Scarring: Splinting of Rat Wounds. Methods Mol. Biol. 2021, 2299, 405–417. [Google Scholar] [CrossRef] [PubMed]
- Naldaiz-Gastesi, N.; Bahri, O.A.; López de Munain, A.; McCullagh, K.J.A.; Izeta, A. The panniculus carnosus muscle: An evolutionary enigma at the intersection of distinct research fields. J. Anat. 2018, 233, 275–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aarabi, S.; Bhatt, K.A.; Shi, Y.; Paterno, J.; Chang, E.I.; Loh, S.A.; Holmes, J.W.; Longaker, M.T.; Yee, H.; Gurtner, G.C. Mechanical load initiates hypertrophic scar formation through decreased cellular apoptosis. FASEB J. 2007, 21, 3250–3261. [Google Scholar] [CrossRef] [Green Version]
- Sylakowski, K.; Hwang, M.P.; Justin, A.; Whaley, D.; Wang, Y.; Wells, A. The matricellular protein decorin delivered intradermally with coacervate improves wound resolution in the CXCR3-deficient mouse model of hypertrophic scarring. Wound Repair Regen. 2022, 30, 436–447. [Google Scholar] [CrossRef] [PubMed]
- Yates, C.C.; Krishna, P.; Whaley, D.; Bodnar, R.; Turner, T.; Wells, A. Lack of CXC chemokine receptor 3 signaling leads to hypertrophic and hypercellular scarring. Am. J. Pathol. 2010, 176, 1743–1755. [Google Scholar] [CrossRef]
- Yates, C.C.; Whaley, D.; Kulasekeran, P.; Hancock, W.W.; Lu, B.; Bodnar, R.; Newsome, J.; Hebda, P.A.; Wells, A. Delayed and deficient dermal maturation in mice lacking the CXCR3 ELR-negative CXC chemokine receptor. Am. J. Pathol. 2007, 171, 484–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jimi, S.; Saparov, A.; Koizumi, S.; Miyazaki, M.; Takagi, S. A novel mouse wound model for scar tissue formation in abdominal muscle wall. J. Vet. Med. Sci. 2021, 83, 1933–1942. [Google Scholar] [CrossRef]
- Li, Y.; Shan, X.; Mao, Q.; Xiang, R.; Cai, Z. Botulinum toxin type a intralesional monotherapy for treating human hypertrophic scar in a dose-dependent manner: In an animal model. J. Plast. Reconstr. Aesthetic Surg. 2021, 74, 3186–3195. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Li, S.; Li, K.; Jiang, X.; Zhang, J.; Liu, H. A highly simulated scar model developed by grafting human thin split-thickness skin on back of nude mouse: The remodeling process, histological characteristics of scars. Biochem. Biophys Res. Commun. 2020, 526, 744–750. [Google Scholar] [CrossRef] [PubMed]
- Ud-Din, S.; Bayat, A. Classification of distinct endotypes in human skin scarring: SCAR—A novel perspective on dermal fibrosis. Adv. Wound Care 2022, 11, 109–120. [Google Scholar] [CrossRef] [PubMed]
- Nast, A.; Eming, S.; Fluhr, J.; Fritz, K.; Gauglitz, G.; Hohenleutner, S.; Panizzon, R.G.; Sebastian, G.; Sporbeck, B.; Koller, J.; et al. German S2k guidelines for the therapy of pathological scars (hypertrophic scars and keloids). J. Dtsch Derm. Ges. 2012, 10, 747–762. [Google Scholar] [CrossRef]
- Ogawa, R.; Akaishi, S.; Huang, C.; Dohi, T.; Aoki, M.; Omori, Y.; Koike, S.; Kobe, K.; Akimoto, M.; Hyakusoku, H. Clinical applications of basic research that shows reducing skin tension could prevent and treat abnormal scarring: The importance of fascial/subcutaneous tensile reduction sutures and flap surgery for keloid and hypertrophic scar reconstruction. J. Nippon Med. Sch. 2011, 78, 68–76. [Google Scholar] [CrossRef] [Green Version]
- Ogawa, R.; Akaishi, S.; Kuribayashi, S.; Miyashita, T. Keloids and Hypertrophic Scars Can Now Be Cured Completely: Recent Progress in Our Understanding of the Pathogenesis of Keloids and Hypertrophic Scars and the Most Promising Current Therapeutic Strategy. J. Nippon Med. Sch. 2016, 83, 46–53. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.H.; Huang, T.; Hsu, Y.; Chen, H. Prospective clinical trial comparing barbed dermal suture and interrupted suture closure of the anterolateral thigh flap donor site in a Taiwanese population based on the Vancouver scar scale and the patient and observer scar assessment scale. J. Plast. Reconstr. Aesthet. Surg. 2021, 74, 3196–3211. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, R. Keloid and Hypertrophic Scars Are the Result of Chronic Inflammation in the Reticular Dermis. Int. J. Mol. Sci. 2017, 18, 606. [Google Scholar] [CrossRef] [Green Version]
- Macintyre, L.; Baird, M. Pressure garments for use in the treatment of hypertrophic scars--a review of the problems associated with their use. Burns 2006, 32, 10–15. [Google Scholar] [CrossRef]
- Engrav, L.H.; Heimbach, D.M.; Rivara, F.P.; Moore, M.L.; Wang, J.; Carrougher, G.J.; Costa, B.; Numhom, S.; Calderon, J.; Gibran, N.S. 12-Year within-wound study of the effectiveness of custom pressure garment therapy. Burns 2010, 36, 975–983. [Google Scholar] [CrossRef]
- Moortgat, P.; Meirte, J.; Maertens, K.; Lafaire, C.; De Cuyper, L.; Anthonissen, M. Can a Cohesive Silicone Bandage Outperform an Adhesive Silicone Gel Sheet in the Treatment of Scars? A Randomized Comparative Trial. Plast. Reconstr. Surg. 2019, 143, 902–911. [Google Scholar] [CrossRef] [PubMed]
- Rogers, N.T.; Fancourt, D. Cultural Engagement Is a Risk-Reducing Factor for Frailty Incidence and Progression. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2020, 75, 571–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.J.; Jang, Y.J. Recent Understandings of Biology, Prophylaxis and Treatment Strategies for Hypertrophic Scars and Keloids. Int. J. Mol. Sci. 2018, 19, 711. [Google Scholar] [CrossRef] [Green Version]
- Kalasho, B.D.; Kikuchi, R.; Zoumalan, C.I. Silicone-Based Scar Cream for Post Upper Eyelid Blepharoplasty-associated Cicatricial and Hypertrophic Scarring. J. Drugs Dermatol. 2019, 18, 440–446. [Google Scholar]
- Kim, S.H.; Lee, S.J.; Lee, J.W.; Jeong, H.S.; Suh, I.S. Clinical trial to evaluate the efficacy of botulinum toxin type A injection for reducing scars in patients with forehead laceration: A double-blinded, randomized controlled study. Medicine 2019, 98, e16952. [Google Scholar] [CrossRef]
- Huang, R.L.; Ho, C.K.; Tremp, M.; Xie, Y.; Li, Q.; Zan, T. Early Postoperative Application of Botulinum Toxin Type A Prevents Hypertrophic Scarring after Epicanthoplasty: A Split-Face, Double-Blind, Randomized Trial. Plast. Reconstr. Surg. 2019, 144, 835–844. [Google Scholar] [CrossRef]
- Abedini, R.; Mehdizade Rayeni, N.; Haddady Abianeh, S.; Rahmati, J.; Teymourpour, A.; Nasimi, M. Botulinum Toxin Type A Injection for Mammoplasty and Abdominoplasty Scar Management: A Split-Scar Double-Blinded Randomized Controlled Study. Aesthetic Plast. Surg. 2020, 44, 2270–2276. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Pang, R.; Wei, Z.; Zhang, H.; Liu, W.; Li, G. The effect of botulinum toxin injection dose on the appearance of surgical scar. Sci. Rep. 2021, 11, 13670. [Google Scholar] [CrossRef] [PubMed]
- Park, G.S.; An, M.K.; Yoon, J.H.; Park, S.S.; Koh, S.H.; Mauro, T.M.; Cho, E.B.; Park, E.J.; Kim, K.H.; Kim, K.J. Botulinum toxin type A suppresses pro-fibrotic effects via the JNK signaling pathway in hypertrophic scar fibroblasts. Arch. Dermatol. Res. 2019, 311, 807–814. [Google Scholar] [CrossRef]
- Shin, J.U.; Park, J.; Lee, J.H.; Lee, K.H.; Kim, Y.O.; Yun, C.O.; Lee, W.J. Extramarginal excision is preferable for hypertrophic scars. Int. J. Derm. 2014, 53, 1138–1144. [Google Scholar] [CrossRef]
- Schweinfurth, J.M.; Fedok, F. Avoiding pitfalls and unfavorable outcomes in scar revision. Facial Plast. Surg. 2001, 17, 273–278. [Google Scholar] [CrossRef]
- Vijaya Lakshmi, Y.; Swetha Reddy, L.; Naga Neelima Devi, K.; Phani Kumar, K.; Guru Karthik, G.; Srinivas Chakravarthy, P.; Nageswar Rao, K. Evaluation of Microneedling Therapy in Management of Facial Scars. J. Craniofacial Surg. 2020, 31, e214–e217. [Google Scholar] [CrossRef]
- Esmat, S.; Shokeir, H.A.; Samy, N.A.; Mahmoud, S.B.; Sayed, S.S.E.D.; Shaker, E.; Hilal, R.F. Automated Microneedling Versus Fractional CO2 Laser in Treatment of Traumatic Scars: A Clinical and Histochemical Study. Dermatol. Surg. 2021, 47, 1480–1485. [Google Scholar] [CrossRef] [PubMed]
- El Mofty, M.; Esmat, S.; Hunter, N.; Mashaly, H.M.; Dorgham, D.; Shaker, O.; Ibrahim, S. Effect of different types of therapeutic trauma on vitiligo lesions. Dermatol. Ther. 2017, 30, e12447. [Google Scholar] [CrossRef] [PubMed]
- Wong, T.-S.; Li, J.Z.-H.; Chen, S.; Chan, J.Y.-W.; Gao, W. The efficacy of triamcinolone acetonide in keloid treatment: A systematic review and meta-analysis. Front. Med. 2016, 3, 71. [Google Scholar] [CrossRef] [Green Version]
- Zhuang, Z.; Li, Y.; Wei, X. The safety and efficacy of intralesional triamcinolone acetonide for keloids and hypertrophic scars: A systematic review and meta-analysis. Burns 2021, 47, 987–998. [Google Scholar] [CrossRef]
- Khalid, F.A.; Mehrose, M.Y.; Saleem, M.; Yousaf, M.A.; Mujahid, A.M.; Rehman, S.U.; Ahmad, S.; Tarar, M.N. Comparison of efficacy and safety of intralesional triamcinolone and combination of triamcinolone with 5-fluorouracil in the treatment of keloids and hypertrophic scars: Randomised control trial. Burns 2019, 45, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Bi, M.; Sun, P.; Li, D.; Dong, Z.; Chen, Z. Intralesional Injection of Botulinum Toxin Type A Compared with Intralesional Injection of Corticosteroid for the Treatment of Hypertrophic Scar and Keloid: A Systematic Review and Meta-Analysis. Med. Sci. Monit. 2019, 25, 2950–2958. [Google Scholar] [CrossRef]
- Elshahed, A.R.; Elmanzalawy, K.S.; Shehata, H.; ElSaie, M.L. Effect of botulinum toxin type A for treating hypertrophic scars: A split-scar, double-blind randomized controlled trial. J. Cosmet. Derm. 2020, 19, 2252–2258. [Google Scholar] [CrossRef] [PubMed]
- Henderson, D.L.; Cromwell, T.A.; Mes, L.G. Argon and carbon dioxide laser treatment of hypertrophic and keloid scars. Lasers Surg. Med. 1984, 3, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Nouri, K.; Rivas, M.P.; Stevens, M.; Ballard, C.J.; Singer, L.; Ma, F.; Vejjabhinanta, V.; Elsaie, M.L.; Elgart, G.W. Comparison of the effectiveness of the pulsed dye laser 585 nm versus 595 nm in the treatment of new surgical scars. Lasers Med. Sci. 2009, 24, 801–810. [Google Scholar] [CrossRef]
- Seago, M.; Shumaker, P.R.; Spring, L.K.; Alam, M.; Al-Niaimi, F.; Rox Anderson, R.; Artzi, O.; Bayat, A.; Cassuto, D.; Chan, H.H.; et al. Laser Treatment of Traumatic Scars and Contractures: 2020 International Consensus Recommendations. Lasers Surg. Med. 2020, 52, 96–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tawfic, S.; Sayed, S.; Nada, A.; Manaa, D.; Shalaby, S. High- Versus Low-Density Fractional Laser in the Treatment of Hypertrophic Postburn Scars: A Randomized Clinical Trial. Dermatol. Surg. 2020, 46, e38–e44. [Google Scholar] [CrossRef]
- Won, T.; Ma, Q.; Chen, Z.; Gao, Z.; Wu, X.; Zhang, R. The efficacy and safety of low-energy carbon dioxide fractional laser use in the treatment of early-stage pediatric hypertrophic scars: A prospective, randomized, split-scar study. Lasers Surg. Med. 2022, 54, 230–236. [Google Scholar] [CrossRef]
- Manuskiatti, W.; Kaewkes, A.; Yan, C.; Ng, J.N.; Glahn, J.Z.; Wanitphakdeedecha, R. Hypertrophic Scar Outcomes in Fractional Laser Monotherapy Versus Fractional Laser-Assisted Topical Corticosteroid Delivery: A Randomized Clinical Trial. Acta Derm. Venereol. 2021, 101, adv00416. [Google Scholar] [CrossRef]
- Babu, P.; Meethale Thiruvoth, F.; Chittoria, R.K. Intense pulsed light vs silicone gel sheet in the management of hypertrophic scars: An interventional comparative trial in the Indian population. J. Cosmet. Laser Ther. 2019, 21, 234–237. [Google Scholar] [CrossRef]
- Salem, S.A.M.; Abdel Hameed, S.M.; Mostafa, A.E. Intense pulsed light versus cryotherapy in the treatment of hypertrophic scars: A clinical and histopathological study. J. Cosmet. Derm. 2021, 20, 2775–2784. [Google Scholar] [CrossRef]
- Salameh, F.; Shumaker, P.R.; Goodman, G.J.; Spring, L.K.; Seago, M.; Alam, M.; Al-Niaimi, F.; Cassuto, D.; Chan, H.H.; Dierickx, C.; et al. Energy-based devices for the treatment of Acne Scars: 2022 International consensus recommendations. Lasers Surg. Med. 2022, 54, 10–26. [Google Scholar] [CrossRef]
- Daoud, A.A.; Gianatasio, C.; Rudnick, A.; Michael, M.; Waibel, J. Efficacy of Combined Intense Pulsed Light (IPL) With Fractional CO. Lasers Surg. Med. 2019, 51, 678–685. [Google Scholar] [CrossRef]
- Waibel, J.S.; Wulkan, A.J.; Rudnick, A.; Daoud, A. Treatment of hypertrophic scars using laser-assisted corticosteroid versus laser-assisted 5-fluorouracil delivery. Dermatol. Surg. 2019, 45, 423–430. [Google Scholar] [CrossRef]
- Shin, J.; Cho, J.T.; Park, S.I.; Jung, S.N. Combination therapy using non-ablative fractional laser and intralesional triamcinolone injection for hypertrophic scars and keloids treatment. Int. Wound J. 2019, 16, 1450–1456. [Google Scholar] [CrossRef]
- Rasaii, S.; Sohrabian, N.; Gianfaldoni, S.; Hadibarhaghtalab, M.; Pazyar, N.; Bakhshaeekia, A.; Lotti, T.; Ramirez-Pacheco, L.A.; Lange, C.S.; Matta, J.; et al. Intralesional triamcinolone alone or in combination with botulinium toxin A is ineffective for the treatment of formed keloid scar: A double blind controlled pilot study. Dermatol. Ther. 2019, 32, e12781. [Google Scholar] [CrossRef]
- Teplyi, V.; Grebchenko, K. THE USAGE OF RADIOFREQUENCY ABLATION FOR TREATMENT OF KELOIDS AND HYPERTROPHIC SCARS. Probl. Radiac Med. Radiobiol. 2019, 24, 561–573. [Google Scholar] [CrossRef] [Green Version]
- Murphy, A.; LeVatte, T.; Boudreau, C.; Midgen, C.; Gratzer, P.; Marshall, J.; Bezuhly, M. Angiotensin II Type I Receptor Blockade Is Associated with Decreased Cutaneous Scar Formation in a Rat Model. Plast. Reconstr. Surg. 2019, 144, 803e–813e. [Google Scholar] [CrossRef]
- Sobec, R.L.; Fodor, L.; Bodog, F. Topical Oxandrolone Reduces Ear Hypertrophic Scar Formation in Rabbits. Plast. Reconstr. Surg. 2019, 143, 481–487. [Google Scholar] [CrossRef]
- Wang, P.; Gu, L.; Yang, X.; An, Y.; Bi, H.; Zhao, Z.; Wang, Q.; Du, S.; Qin, Z. Dipeptidyl Peptidase-4 Inhibitor Reduces the Risk of Developing Hypertrophic Scars and Keloids following Median Sternotomy in Diabetic Patients: A Nationwide Retrospective Cohort Study Using the National Database of Health Insurance Claims of Japan. Plast. Reconstr. Surg. 2021, 147, 1067e–1068e. [Google Scholar] [CrossRef]
- Dolynchuk, K.N.; Tredget, E.E. A Preliminary Report of the Biochemical and Clinical Effects of 1,4-Diaminobutane on Prevention of Human Hypertrophic Scars. Plast. Reconstr. Surg. 2020, 145, 76e–84e. [Google Scholar] [CrossRef] [PubMed]
- Hoerst, K.; van den Broek, L.; Sachse, C.; Klein, O.; von Fritschen, U.; Gibbs, S.; Hedtrich, S. Regenerative potential of adipocytes in hypertrophic scars is mediated by myofibroblast reprogramming. J. Mol. Med. 2019, 97, 761–775. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Ziemer, M.; Stojanovic, I.; Saksida, T.; Maksimovic-Ivanic, D.; Mijatovic, S.; Djmura, G.; Gajic, D.; Koprivica, I.; Krajnovic, T. Mesenchymal Stem Cells From Mouse Hair Follicles Reduce Hypertrophic Scarring in a Murine Wound Healing Model. Stem Cell Rev. Rep. 2022, 18, 2028–2044. [Google Scholar] [CrossRef] [PubMed]
- Joo, S.Y.; Cho, Y.S.; Lee, S.Y.; Seo, C.H. Regenerative effect of combined laser and human stem cell-conditioned medium therapy on hypertrophic burn scar. Burns 2022, in press. [CrossRef]
- Dai, Z.; Lou, X.; Shen, T.; Sun, Y.; Xiao, Y.; Zheng, X.; Wang, X.; Peng, Y.; Guo, Y.; Guo, Y. Combination of ablative fractional carbon dioxide laser and platelet-rich plasma treatment to improve hypertrophic scars: A retrospective clinical observational study. Burn. Trauma 2021, 9, tkab016. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimi, Z.; Alimohamadi, Y.; Janani, M.; Hejazi, P.; Kamali, M.; Goodarzi, A. Platelet-rich plasma in the treatment of scars, to suggest or not to suggest? A systematic review and meta-analysis. J. Tissue Eng. Regen. Med. 2022, 16, 875–899. [Google Scholar] [CrossRef] [PubMed]
- Kurachi, I.; Kurita, E.; Takushima, A.; Suga, H. Human CD206+ Macrophages Show Antifibrotic Effects on Human Fibroblasts through an IL-6-Dependent Mechanism In Vitro. Plast Reconstr Surg 2021, 147, 231e–239e. [Google Scholar] [CrossRef]
- Kanno, E.; Tanno, H.; Masaki, A.; Sasaki, A.; Sato, N.; Goto, M.; Shisai, M.; Yamaguchi, K.; Takagi, N.; Shoji, M. Defect of interferon γ leads to impaired wound healing through prolonged neutrophilic inflammatory response and enhanced MMP-2 activation. Int. J. Mol. Sci. 2019, 20, 5657. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Model | Scar Location | Advantages | Disadvantages |
|---|---|---|---|
| Rabbit ear HTS * model [124,125] | Ventral side of rabbit ear | Simple, reliable model Ease of handling Possibility of creating multiple wounds | Skin of the ventral side is too difficult to handle because of low thickness Involvement of cells other than skin cells during healing, such as chondrocytes Risk of damaging the underlying cartilage |
| Modified rabbit ear HTS model—use of cryosurgery [126] | Ventral side of rabbit ear | Low risk of damaging the cartilage | Skin of the ventral side is too difficult to handle because of low thickness Involvement of cells other than skin cells during healing, such as chondrocyte |
| Modified Rabbit ear HTS model—application of thermal injury [127] | Ventral side of rabbit ear | Elevated scar within short duration compared to the typical rabbit ear HTS model | Skin of the ventral side is too difficult to handle because of low thickness Involvement of cells other than skin cells during healing, such as chondrocytes Uncontrolled thermal injury can cause variability in scarring effect |
| HTS model on rabbit by injecting anhydrous alcohol [128] | Dorsal skin | HTS-like appearance comparable to the rabbit ear HTS model Low cost Ease of handling | Absence of healing response |
| Burn hypertrophic model on porcine skin [57] | Dorsal Skin | Elevated scar comparable to human scar | High cost Difficult to handle |
| HTS model by splinting of rat wound [131] | Dorsal skin | HTS-like features by reducing the formation of neo-epithelium Low cost Ease of handling | Splinting may create a higher and more persistent tensional state |
| Scar on CXCR3 * deficient mouse [134] | Dorsal skin | Simple, reliable model Ease of handling | The model requires further validation |
| HTS model produced by grafting human xenografts on nude mice [139] | Dorsal skin | Establishment of human scar on an animal model | Difficulty in maintaining nude mice Absence of immune response in mice |
| HTS model by resecting abdominal wall muscle on mice [137] | Ventral skin, abdominal region | Simple and reliable method Ease of handling | Not comparable with general scar development after burn injury or trauma |
| Treatment | Mechanism |
|---|---|
| Tensile reduction suture closure [142] | Reduces tension on the dermal layer when closing wound |
| Paper tape, silicone sheets [145,148] | Hydration, increased temperature, prevent dermal inflammation |
| Wound compression [146] | Reduces capillary perfusion, accelerated collagen maturation |
| Laser [169,170,171,172,173,174] | Destroys microvascularization, resulting in hypoperfusion and hypoxia |
| Silicone cream [150,151] | Hydration of the stratum corneum and cytokine-mediated signaling from keratinocytes to dermal fibroblasts |
| Flavonoids [150] | Anti-inflammatory, antioxidant, anti-bacterial |
| Botulinum toxin-A [152,153,154,155,156] | Decreases proliferation, migration, and secretion of pro-fibrotic factors from fibroblasts |
| Scar excision [157] | Removal of affected tissue |
| Microneedle [159,160,161] | Disruption of existing collagen, stimulation of MMP-9 * release |
| Corticosteroids [145,163] | Anti-inflammatory, local vasoconstriction |
| Botulinum toxin-A [163,165,166] | Decreases proliferation, migration, and secretion of pro-fibrotic factors from fibroblasts |
| Treatment | Proposed Mechanism |
|---|---|
| Corticosteroids + 5-Fluorouracil [163,164,177,178] | Anti-inflammatory, local vasoconstriction, inhibit fibroblasts proliferation, decrease collagen synthesis |
| Laser + Verapamil + 5-Fluorouracil or corticosteroids [180] | Destroy microvascularization resulting in hypoperfusion and hypoxia, inhibit fibroblast proliferation, decrease collagen synthesis, anti-inflammatory |
| CO2 * Laser + Intense Pulse Light [176] | Destroy microvascularization resulting in hypoperfusion and hypoxia, promote new dermal collagen formation and rapid differentiation of keratinocytes |
| Losartan [181] | Fibroblasts with decreased contractile activity, migration, and adhesion |
| Oxandolone + hyaluronic acid gel [182] | Decrease inflammation, collagen and fibroblast cellularity, vascularization, and myofibroblast activity |
| Dipeptidyl peptidase-4 inhibitors [183] | Attenuate collagen synthesis and deposition |
| 1,4-Diaminobutane [184] | Inhibits collagen cross-linking |
| Autologous fat grafting [185] | Decreases the expression of the myofibroblast marker α-SMA * and ECM * components |
| Stem cells [186,187] | Reduce inflammation, cellularity, and collagen filaments |
| Platelet-rich plasma [61,188,189] | Reduces expression of TGF-β1 * and CTGF mRNA |
| CD206 * + Macrophages and Fibroblasts [190] | Increase MMP-1 * and decrease expression of pro-fibrotic factors, COL1A1 *, COL2A1 *, α-SMA *, CTGF *, and TGF-β1 * |
| IL-6 * [190] | Increases expression of anti-fibrotic genes |
| IFN-γ * [191] | Increases expression of COL1A1 * and COL3A1 * mRNA and decreases expression of MMP-2 * (gelatinase) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mony, M.P.; Harmon, K.A.; Hess, R.; Dorafshar, A.H.; Shafikhani, S.H. An Updated Review of Hypertrophic Scarring. Cells 2023, 12, 678. https://doi.org/10.3390/cells12050678
Mony MP, Harmon KA, Hess R, Dorafshar AH, Shafikhani SH. An Updated Review of Hypertrophic Scarring. Cells. 2023; 12(5):678. https://doi.org/10.3390/cells12050678
Chicago/Turabian StyleMony, Manjula P., Kelly A. Harmon, Ryan Hess, Amir H. Dorafshar, and Sasha H. Shafikhani. 2023. "An Updated Review of Hypertrophic Scarring" Cells 12, no. 5: 678. https://doi.org/10.3390/cells12050678