
Molecular Effect of Variants in Toll-like Receptor 4 Gene in Saudi Patients with Type 2 Diabetes Mellitus

Abstract
:1. Introduction
2. Materials and Methods
2.1. Importance of Patients with T2DM
2.2. Sample Size
2.3. Ethical Issues
2.4. Subject Details
2.5. Sample Collection and Laboratory Investigation
2.6. Molecular Investigation
2.7. Statistical Analysis
3. Results
3.1. Demographic Profile for Performing Student t-Tests between T2DM and Control Subjects
3.2. Verification of Enrolled Population Analysis
3.3. Genetic Association of TLR4 Gene SNPs with T2DM and Controls
3.4. Allelic Association Studies
3.5. Association between TLR4 SNPs and T2DM Covariates
3.6. Analysis of ANOVA Examined between Dependent and Independent Variables
3.7. Haplotype Interference Analysis
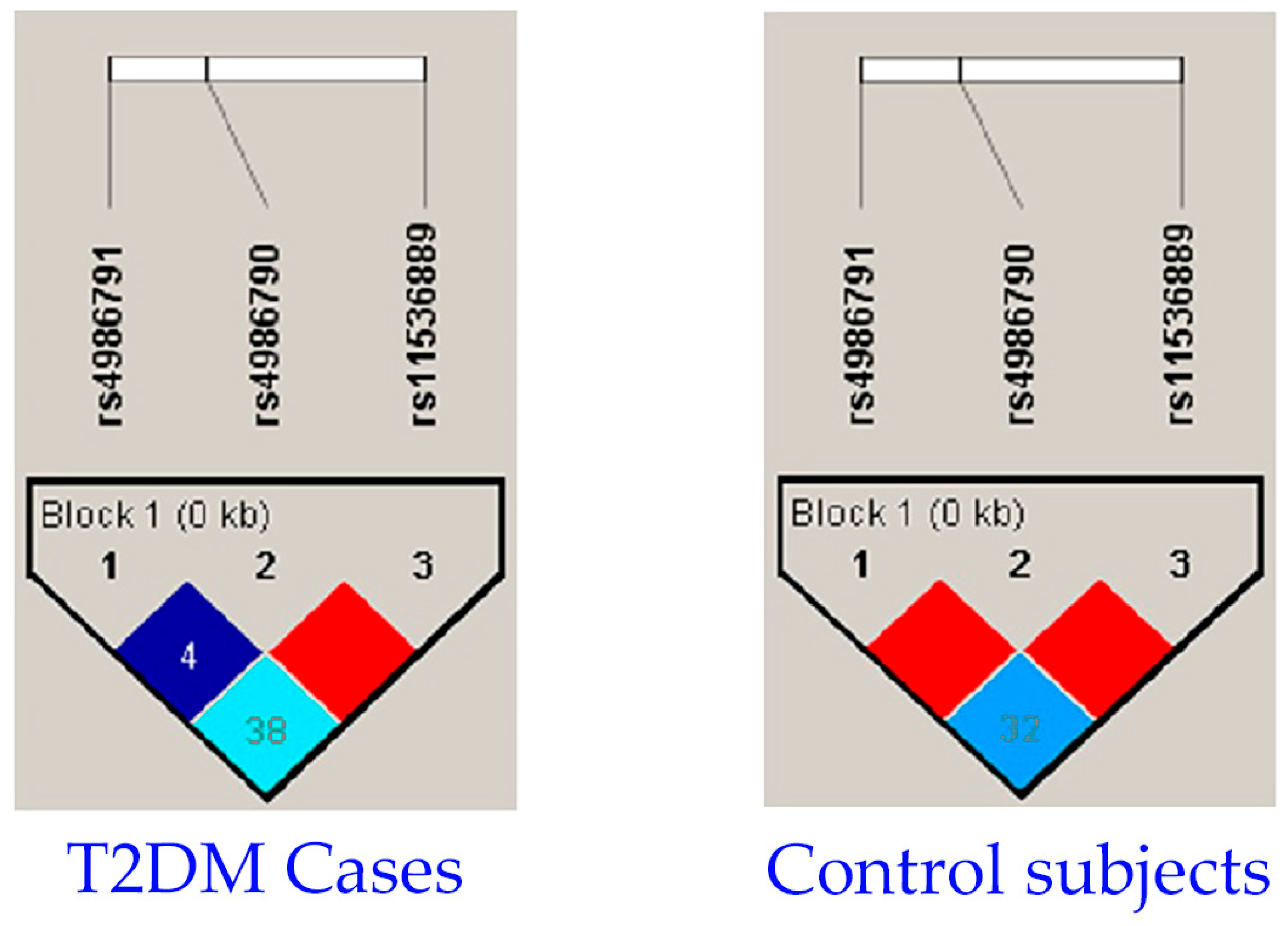
3.8. Association of Linkage Disequilibrium
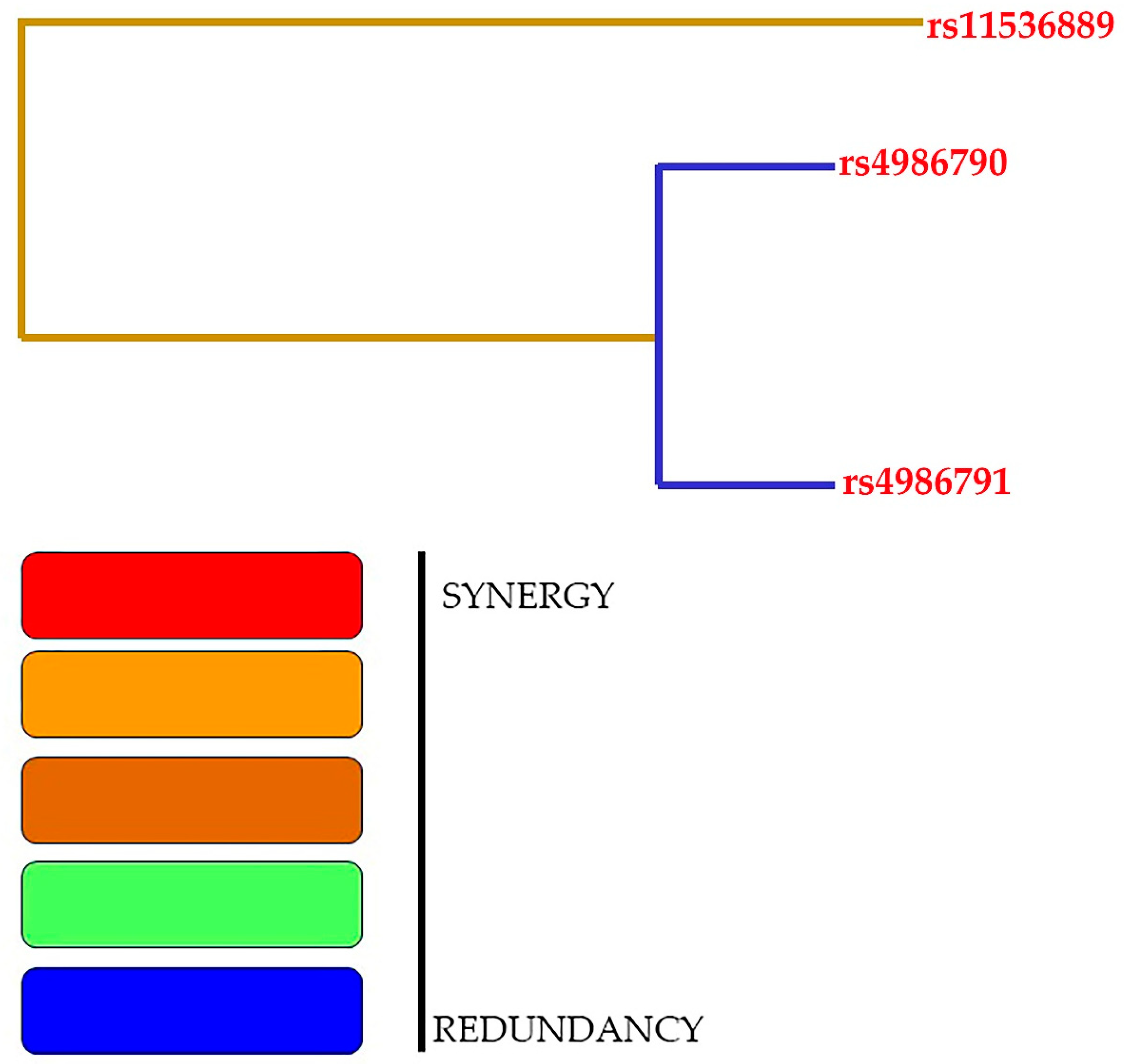
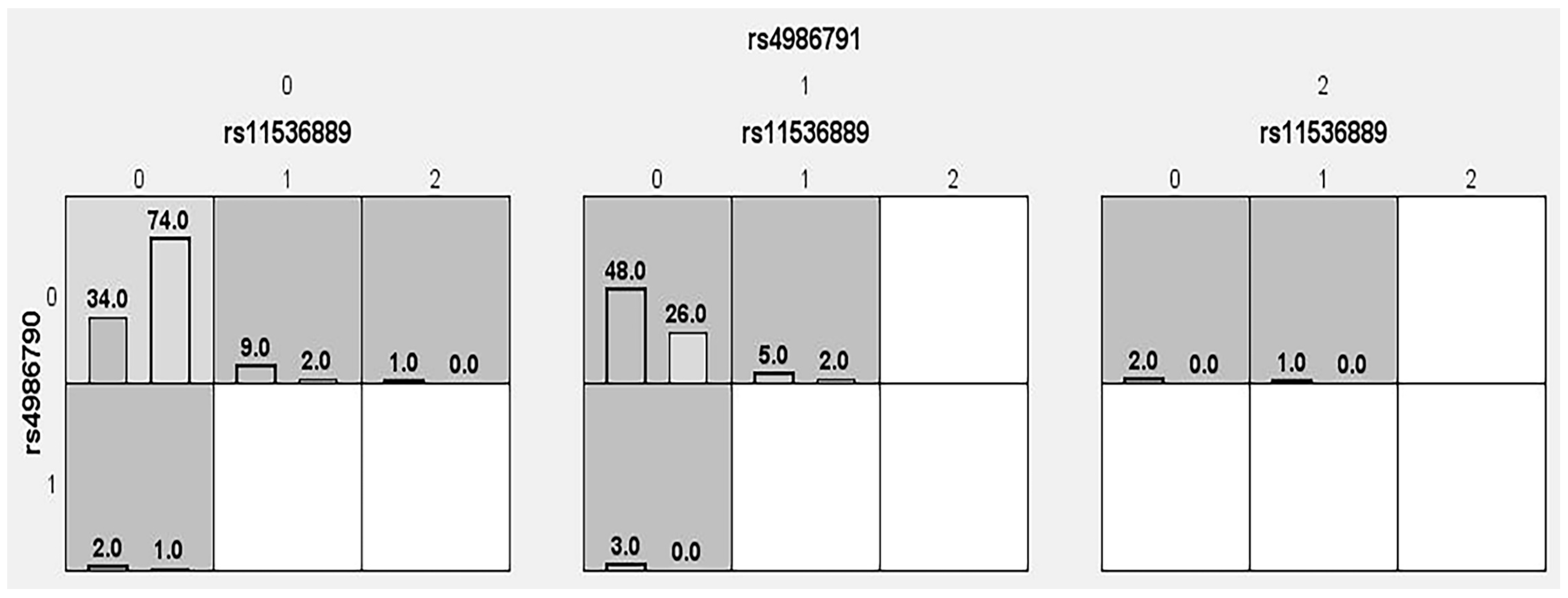
3.9. Association of Gene–Gene Interaction Analysis Studied via GMDR Model
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sheykhhasan, M. Towards standardized stem cell therapy in type 2 diabetes mellitus: A systematic review. Curr. Stem Cell Res. Ther. 2019, 14, 75–76. [Google Scholar] [CrossRef]
- Xiong, F.; Wang, J.; Nierenberg, J.L.; Van Blarigan, E.L.; Kenfield, S.A.; Chan, J.M.; Schmajuk, G.; Huang, C.-Y.; Graff, R.E. Diabetes mellitus and risk of breast cancer: A large-scale, prospective, population-based study. Br. J. Cancer 2023, 129, 648–655. [Google Scholar] [CrossRef]
- Ruze, R.; Song, J.; Yin, X.; Chen, Y.; Xu, R.; Wang, C.; Zhao, Y. Mechanisms of obesity-and diabetes mellitus-related pancreatic carcinogenesis: A comprehensive and systematic review. Signal Transduct. Target. Ther. 2023, 8, 139. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.M. History of diabetes mellitus. Saudi Med. J. 2002, 23, 373–378. [Google Scholar]
- Landgraf, R.; Heinemann, L.; Schleicher, E.; Gerdes, C.; Petersmann, A.; Müller-Wieland, D.; Müller, U.A.; Freckmann, G.; Thaler, M.; Ziegler, A.-G. Definition, Klassifikation, Diagnostik und Differenzialdiagnostik des Diabetes mellitus: Update 2022. Die Diabetol. 2023, 19, 44–55. [Google Scholar] [CrossRef]
- Karamanou, M.; Protogerou, A.; Tsoucalas, G.; Androutsos, G.; Poulakou-Rebelakou, E. Milestones in the history of diabetes mellitus: The main contributors. World J. Diabetes 2016, 7, 1. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Salgado, A.; Coyotl-Santiago, N.; Moreno-Vazquez, R.; Lopez-Teyssier, M.; Garcia-Carrasco, M.; Moccia, F.; Berra-Romani, R. Alterations of the Ca2+ clearing mechanisms by type 2 diabetes in aortic smooth muscle cells of Zucker diabetic fatty rat. Front. Physiol. 2023, 14, 771. [Google Scholar] [CrossRef] [PubMed]
- Alguwaihes, A.M.; Alhozali, A.; Yahia, M.M.; Abdel-Nabi, T.; Hatahet, M.H.; Albalkhi, N.I.; Al Sifri, S. The prevalence of cardiovascular disease in adults with type 2 diabetes mellitus in Saudi Arabia-CAPTURE study. Saudi Med. J. 2023, 44, 57. [Google Scholar] [CrossRef]
- Aljulifi, M.Z. Prevalence and reasons of increased type 2 diabetes in Gulf Cooperation Council Countries. Saudi Med. J. 2021, 42, 481. [Google Scholar] [CrossRef]
- Silva, M.J.A.; Santana, D.S.; de Oliveira, L.G.; Monteiro, E.O.L.; Lima, L.N.G.C. The relationship between 896A/G (rs4986790) polymorphism of TLR4 and infectious diseases: A meta-analysis. Front. Genet. 2022, 13, 1045725. [Google Scholar] [CrossRef]
- Casqueiro, J.; Casqueiro, J.; Alves, C. Infections in patients with diabetes mellitus: A review of pathogenesis. Indian J. Endocrinol. Metab. 2012, 16, S27. [Google Scholar] [PubMed]
- Wheat, L.J. Infection and diabetes mellitus. Diabetes Care 1980, 3, 187–197. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, A.C.M.; Dos Santos, B.R.C.; Dos Santos, B.B.; de Moura, E.L.; Ferreira, J.M.; Dos Santos, L.K.C.; Oliveira, S.P.; Dias, R.B.F.; e Silva, A.C.P.; de Farias, K.F. Genetic polymorphisms as multi-biomarkers in severe acute respiratory syndrome (SARS) by coronavirus infection: A systematic review of candidate gene association studies. Infect. Genet. Evol. 2021, 93, 104846. [Google Scholar] [CrossRef] [PubMed]
- Jan, A.; Zakiullah; Ali, S.; Muhammad, B.; Arshad, A.; Shah, Y.; Bahadur, H.; Khan, H.; Khuda, F.; Akbar, R. Decoding type 2 diabetes mellitus genetic risk variants in Pakistani Pashtun ethnic population using the nascent whole exome sequencing and MassARRAY genotyping: A case-control association study. PLoS ONE 2023, 18, e0281070. [Google Scholar] [CrossRef]
- Berdeli, A.; Emingil, G.; Han Saygan, B.; Gürkan, A.; Atilla, G.; Köse, T.; Baylas, H. TLR2 Arg753Gly, TLR4 Asp299Gly and Thr399Ile gene polymorphisms are not associated with chronic periodontitis in a Turkish population. J. Clin. Periodontol. 2007, 34, 551–557. [Google Scholar] [CrossRef]
- Khaghanzadeh, N.; Naderi, N.; Pournasrollah, N.; Farahbakhsh, E.; Kheirandish, M.; Samiei, A. TLR4 polymorphisms (896A> G and 1196C> T) affect the predisposition to diabetic nephropathy in type 2 diabetes mellitus. Diabetes Metab. Syndr. Obes. 2020, 13, 1015–1021. [Google Scholar] [CrossRef]
- Fu, X.; Sun, X.; Wang, H.; Guo, J.; Zhang, G.; Xu, Q. Genetic polymorphisms of the TLR4 gene and their association with susceptibility to type 2 diabetes mellitus in the Chinese population. Genet. Mol. Res. 2013, 12, 3813–3820. [Google Scholar] [CrossRef]
- Rodríguez-García, R.; Vazquez-Villamar, M.; Aparicio-Ozores, G.; Parra-Rojas, I.; Radilla-Vázquez, R.; Castro-Alarcón, N. TLR4 polymorphism and haplotype are associated with obesity and lipid profile in young population: A pilot study. J. Endocrinol. Investig. 2023, 46, 903–913. [Google Scholar] [CrossRef]
- Association, A.D. American Diabetes Association Standards of medical care in diabetes–2017. Diabetes Care 2017, 40, S1. [Google Scholar]
- Rosner, B. Fundamentals of Biostatistics; Cengage Learning: Boston, MA, USA, 2015. [Google Scholar]
- Smail, S.W.; Babaei, E.; Amin, K. Demographic, clinical and genetic factors associated with COVID-19 disease susceptibility and mortality in a Kurdish population. Ann. Saudi Med. 2023, 43, 125–142. [Google Scholar] [CrossRef]
- Solé, X.; Guinó, E.; Valls, J.; Iniesta, R.; Moreno, V. SNPStats: A web tool for the analysis of association studies. Bioinformatics 2006, 22, 1928–1929. [Google Scholar] [CrossRef] [PubMed]
- Barrett, J.C.; Fry, B.; Maller, J.; Daly, M.J. Haploview: Analysis and visualization of LD and haplotype maps. Bioinformatics 2005, 21, 263–265. [Google Scholar] [CrossRef] [PubMed]
- Lou, X.-Y.; Chen, G.-B.; Yan, L.; Ma, J.Z.; Zhu, J.; Elston, R.C.; Li, M.D. A generalized combinatorial approach for detecting gene-by-gene and gene-by-environment interactions with application to nicotine dependence. Am. J. Hum. Genet. 2007, 80, 1125–1137. [Google Scholar] [CrossRef] [PubMed]
- Lai, S.; Yan, D.; Xu, J.; Yu, X.; Guo, J.; Fang, X.; Tang, M.; Zhang, R.; Zhang, H.; Jia, W. Genetic variants in epoxyeicosatrienoic acid processing and degradation pathways are associated with gestational diabetes mellitus. Nutr. J. 2023, 22, 31. [Google Scholar] [CrossRef]
- Mambiya, M.; Shang, M.; Wang, Y.; Li, Q.; Liu, S.; Yang, L.; Zhang, Q.; Zhang, K.; Liu, M.; Nie, F. The play of genes and non-genetic factors on type 2 diabetes. Front. Public Health 2019, 7, 349. [Google Scholar] [CrossRef]
- Mahdy, S.H.; Abd Elkader, N.M.; Kassim, N.A.; ElHady, M.M. Genetic variation in toll-like receptor 4 gene with primary antiphospholipid syndrome susceptibility: A cohort of Egyptian patients. Egypt. J. Med. Hum. Genet. 2022, 23, 148. [Google Scholar] [CrossRef]
- Rees, D.C.; Krieg, A.M.; Titball, R.W. Nonspecific Immunomodulator Therapy: CpG. In Biological Weapons Defense: Infectious Diseases and Counterbioterrorism; Humana Press: Totowa, NJ, USA, 2005; pp. 317–331. [Google Scholar]
- Yehualashet, A.S. Toll-like receptors as a potential drug target for diabetes mellitus and diabetes-associated complications. Diabetes Metab. Syndr. Obes. 2020, 13, 4763–4777. [Google Scholar] [CrossRef]
- Abu-Amero, K.K.; Jaeger, M.; Plantinga, T.; Netea, M.G.; Hassan, H.Y. Genetic variation of TLR2 and TLR4 among the Saudi Arabian population: Insight into the evolutionary dynamics of the Arabian Peninsula. Genet. Test. Mol. Biomark. 2013, 17, 166–169. [Google Scholar] [CrossRef]
- Al-Qahtani, A.A.; Al-Anazi, M.R.; Al-Zoghaibi, F.; Abdo, A.A.; Sanai, F.M.; Khan, M.Q.; Albenmousa, A.; Al-Ashgar, H.I.; Al-Ahdal, M.N. The association of toll-like receptor 4 polymorphism with hepatitis C virus infection in Saudi Arabian patients. BioMed Res. Int. 2014, 2014, 357062. [Google Scholar] [CrossRef]
- Fouad, N.A.; Saeed, A.M.; Mahedy, A.W. Toll like receptor-4 gene polymorphism and susceptibility to pulmonary tuberculosis. Egypt. J. Immunol. 2019, 26, 1–10. [Google Scholar]
- AlKhulaifi, F.M.; Alkhuriji, A.; Mansour, L.; Al-jurayyan, A.; Al-Mulhim, N.M.; Tashkandy, Y.A.; Aldossari, G.S.; Alomar, S. Association between Toll-like receptor 4 polymorphism and Acute Lymphoblastic Leukemia susceptibility in Saudi Arabian patients. J. King Saud Univ.-Sci. 2022, 34, 101985. [Google Scholar] [CrossRef]
- Mousa, A.; Kondkar, A.A.; Al-Obeidan, S.A.; Azad, T.A.; Sultan, T.; Osman, E.A.; Abu-Amero, K.K. Lack of association between polymorphism rs4986791 in TLR4 and primary open-angle glaucoma in a Saudi cohort. Genet. Test. Mol. Biomark. 2016, 20, 556–559. [Google Scholar] [CrossRef] [PubMed]
- Semlali, A.; Jalouli, M.; Parine, N.R.; Al Amri, A.; Arafah, M.; Al Naeem, A.; Abdullah Ajaj, S.; Rouabhia, M.; Alanazi, M.S. Toll-like receptor 4 as a predictor of clinical outcomes of estrogen receptor-negative breast cancer in Saudi women. OncoTargets Ther. 2017, 10, 1207–1216. [Google Scholar] [CrossRef]
- Abu-Amero, K.K.; Kondkar, A.A.; Mousa, A.; Azad, T.A.; Sultan, T.; Osman, E.A.; Al-Obeidan, S.A. Analysis of toll-like receptor rs4986790 polymorphism in Saudi patients with primary open angle glaucoma. Ophthalmic Genet. 2017, 38, 133–137. [Google Scholar] [CrossRef] [PubMed]
- Eed, E.M.; Hawash, Y.A.; Khalifa, A.S.; Alsharif, K.F.; Alghamdi, S.A.; Almalki, A.A.; Almehmadi, M.M.; Ismail, K.A.; Taha, A.A.; Saber, T. Association of toll-like receptors 2, 4, 9 and 10 genes polymorphisms and Helicobacter pylori-related gastric diseases in Saudi patients. Indian J. Med. Microbiol. 2020, 38, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Semlali, A.; Reddy Parine, N.; Arafah, M.; Mansour, L.; Azzi, A.; Al Shahrani, O.; Al Amri, A.; Shaik, J.P.; Aljebreen, A.M.; Alharbi, O. Expression and polymorphism of toll-like receptor 4 and effect on NF-κB mediated inflammation in colon cancer patients. PLoS ONE 2016, 11, e0146333. [Google Scholar] [CrossRef] [PubMed]
- Semlali, A.; Al Mutairi, M.; Oqla Alanazi, I.; Awad Aljohi, H.; Reddy Parine, N.; Alhadheq, A.; Al-Jafari, A.A.; Mobeirek, A.F.; Al Amri, A.; Shaik, J.P. Toll-like receptor 4 polymorphisms in Saudi population with cardiovascular diseases. Mol. Genet. Genom. Med. 2019, 7, e852. [Google Scholar] [CrossRef]
- Wang, X.; Ma, A.; Han, X.; Chen, L.; Liang, H.; Litifu, A.; Ablez, A.; Xue, F. Relationship between Toll-like receptor 4 and type-2 diabetes mellitus complicated by tuberculosis. Int. J. Tuberc. Lung Dis. 2017, 21, 910–915. [Google Scholar] [CrossRef]
- Huang, W.; Nie, L.; Zhang, L.; Jing, L.; Dong, F.; Wang, M.; Zhang, N.; Liu, Y.; Zhang, B.; Chen, C. Association of TLR2 and TLR4 non-missense single nucleotide polymorphisms with type 2 diabetes risk in a southern Chinese population: A case-control study. Genet. Mol. Res. 2015, 14, 8694–8705. [Google Scholar] [CrossRef]
- Peng, D.; Jiang, F.; Zhang, R.; Tang, S.; Chen, M.; Yan, J.; Sun, X.; Luo, Y.; Hu, C.; Jia, W. Association of T oll-like R eceptor 4 G ene polymorphisms with susceptibility to type 2 diabetes mellitus in the C hinese population Toll. J. Diabetes 2015, 7, 485–492. [Google Scholar] [CrossRef]
- Li, Y.; Li, D.; Zhang, J.; Liu, S.; Chen, H.; Wu, K. Association between Toll-like receptor 4 and occurrence of type 2 diabetes mellitus susceptible to pulmonary tuberculosis in Northeast China. Stem Cells Int. 2016, 2016, 8160318. [Google Scholar] [CrossRef] [PubMed]
- Singh, K.; Singh, V.K.; Agrawal, N.K.; Gupta, S.K.; Singh, K. Association of Toll-like receptor 4 polymorphisms with diabetic foot ulcers and application of artificial neural network in DFU risk assessment in type 2 diabetes patients. BioMed Res. Int. 2013, 2013, 318686. [Google Scholar] [CrossRef] [PubMed]
- Gond, D.P.; Singh, S.; Agrawal, N. Testing an association between TLR4 and CXCR1 gene polymorphisms with susceptibility to urinary tract infection in type 2 diabetes in north Indian population. Gene 2018, 641, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Buraczynska, M.; Baranowicz-Gaszczyk, I.; Tarach, J.; Ksiazek, A. Toll-like receptor 4 gene polymorphism and early onset of diabetic retinopathy in patients with type 2 diabetes. Hum. Immunol. 2009, 70, 121–124. [Google Scholar] [CrossRef]
- Illig, T.; Bongardt, F.; Schopfer, A.; Holle, R.; Muller, S.; Rathmann, W.; Koenig, W.; Meisinger, C.; Wichmann, H.-E.; Kolb, H. The endotoxin receptor TLR4 polymorphism is not associated with diabetes or components of the metabolic syndrome. Diabetes 2003, 52, 2861–2864. [Google Scholar] [CrossRef]
- Kolek, M.J.; Carlquist, J.F.; Muhlestein, J.B.; Whiting, B.M.; Horne, B.D.; Bair, T.L.; Anderson, J.L. Toll–like receptor 4 gene Asp299Gly polymorphism is associated with reductions in vascular inflammation, angiographic coronary artery disease, and clinical diabetes. Am. Heart J. 2004, 148, 1034–1040. [Google Scholar] [CrossRef]
- Hernesniemi, J.; Lehtimäki, T.; Rontu, R.; Islam, M.; Eklund, C.; Mikkelsson, J.; Ilveskoski, E.; Kajander, O.; Goebeler, S.; Viiri, L. Toll-like receptor 4 polymorphism is associated with coronary stenosis but not with the occurrence of acute or old myocardial infarctions. Scand. J. Clin. Lab. Investig. 2006, 66, 667–676. [Google Scholar] [CrossRef]
- Kim, Y.S.; Hwang, Y.J.; Kim, S.Y.; Yang, S.M.; Lee, K.Y.; Park, I.B. Rarity of TLR4 Asp299Gly and Thr399Ile polymorphisms in the Korean population. Yonsei Med. J. 2008, 49, 58–62. [Google Scholar] [CrossRef]
- Bagarolli, R.A.; Saad, M.J.A.; Saad, S.T.O. Toll-like receptor 4 and inducible nitric oxide synthase gene polymorphisms are associated with Type 2 diabetes. J. Diabetes Complicat. 2010, 24, 192–198. [Google Scholar] [CrossRef]
- Beijk, M.A.; Boekholdt, S.M.; Rittersma, S.Z.; Pons, D.; Zwinderman, A.H.; Doevendans, P.A.; Tio, R.A.; Tijssen, J.G.; Jukema, J.W.; de Winter, R.J. Toll-like receptor 4 gene polymorphisms show no association with the risk of clinical or angiographic restenosis after percutaneous coronary intervention. Pharmacogenetics Genom. 2010, 20, 544–552. [Google Scholar] [CrossRef]
- Cai, H.; Cai, J.; Tao, G. Association of toll-like receptor 4 polymorphisms with type 2 diabetes mellitus. Apmis 2013, 121, 605–611. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Z.-S.; Wang, S.-X.; Jia, H.-X.; Wang, J.; Liu, Y.-T. Association of toll-like receptor 4 polymorphisms with type 2 diabetes mellitus. Inflammation 2013, 36, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Singh, K.; Kant, S.; Singh, V.K.; Agrawal, N.K.; Gupta, S.K.; Singh, K. Toll-like receptor 4 polymorphisms and their haplotypes modulate the risk of developing diabetic retinopathy in type 2 diabetes patients. Mol. Vis. 2014, 20, 704. [Google Scholar]
- Buraczynska, M.; Zukowski, P.; Ksiazek, K.; Wacinski, P.; Dragan, M. The effect of Toll-like receptor 4 gene polymorphism on vascular complications in type 2 diabetes patients. Diabetes Res. Clin. Pract. 2016, 116, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Doody, N.E.; Dowejko, M.M.; Akam, E.C.; Cox, N.J.; Bhatti, J.S.; Singh, P.; Mastana, S.S. The role of TLR4, TNF-α and IL-1β in type 2 diabetes mellitus development within a North Indian population. Ann. Hum. Genet. 2017, 81, 141–146. [Google Scholar] [CrossRef]
- Zaharieva, E.; Kamenov, Z.; Savov, A. TLR4 polymorphisms seem not to be associated with prediabetes and type 2 diabetes but predispose to diabetic retinopathy; TLR4 polymorphisms in glucose continuum. Endocr. Regul. 2017, 51, 137–144. [Google Scholar] [CrossRef]
- Aioanei, C.; Ilies, R.; Bala, C.; Petrisor, M.; Porojan, M.; Popp, R.; Catana, A. The role of adiponectin and toll-like receptor 4 gene polymorphisms on non-proliferative retinopathy in type 2 diabetes mellitus patients. A case-control study in Romanian Caucasians patients. Acta Endocrinol. 2019, 15, 32. [Google Scholar] [CrossRef]
- Degirmenci, I.; Ozbayer, C.; Kebapci, M.N.; Kurt, H.; Colak, E.; Gunes, H.V. Common variants of genes encoding TLR4 and TLR4 pathway members TIRAP and IRAK1 are effective on MCP1, IL6, IL1β, and TNFα levels in type 2 diabetes and insulin resistance. Inflamm. Res. 2019, 68, 801–814. [Google Scholar] [CrossRef]
- Assmann, T.; Lemos, N.; Brondani, L.; Carlessi, R.; Canani, L.H.; Crispim, D. Association between Asp299Gly and Thr399Ile polymorphisms in TLR4 gene and type 2 diabetes mellitus: Case-control study and meta-analysis. Endocr. Abstr. 2014, 35, 353. [Google Scholar] [CrossRef]
- Yin, Y.-W.; Wang, Q.; Sun, Q.-Q.; Hu, A.-M.; Liu, H.-L. Toll-like receptor 4 gene Asp299Gly and Thr399Ile polymorphisms in type 2 diabetes mellitus: A meta-analysis of 15,059 subjects. Diabetes Res. Clin. Pract. 2015, 107, 338–347. [Google Scholar] [CrossRef]
- Fan, J.; Liang, R. Quantitative assessment of TLR4 gene polymorphisms and T2DM risk: A meta-analysis. Mol. Genet. Genom. Med. 2020, 8, e1466. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Li, H.; Wang, C.; Lv, H.; Fu, S. Toll like receptor 4 gene Asp299Gly polymorphism increases the risk of diabetic microvascular complications: A meta analysis. Diabetol. Metab. Syndr. 2022, 14, 79. [Google Scholar] [CrossRef] [PubMed]
- Kolz, M.; Baumert, J.; Müller, M.; Khuseyinova, N.; Klopp, N.; Thorand, B.; Meisinger, C.; Herder, C.; Koenig, W.; Illig, T. Association between variations in the TLR4gene and incident type 2 diabetes is modified by the ratio of total cholesterol to HDL-cholesterol. BMC Med. Genet. 2008, 9, 9. [Google Scholar] [CrossRef] [PubMed]
- Van Linthout, S.; Spillmann, F.; Graiani, G.; Miteva, K.; Peng, J.; Van Craeyveld, E.; Meloni, M.; Tölle, M.; Escher, F.; Subasigüller, A. Down-regulation of endothelial TLR4 signalling after apo AI gene transfer contributes to improved survival in an experimental model of lipopolysaccharide-induced inflammation. J. Mol. Med. 2011, 89, 151–160. [Google Scholar] [CrossRef]
- Naeem, Z. Burden of diabetes mellitus in Saudi Arabia. Int. J. Health Sci. 2015, 9, V–VI. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Covariates | T2DM Cases (n = 105) | Controls (n = 105) | p Value |
|---|---|---|---|
| Age (year) | 63.68 ± 8.43 | 52.85 ± 7.97 | <0.0001 |
| Gender (male:female) | 50 (47.62%):55 (52.38%) | 66 (62.86%):39 (37.14%) | 0.78 |
| Weight (kilograms) | 79.65 ± 13.66 | 76.48 ± 11.97 | 0.07 |
| Height (centimeters) | 159.72 ± 8.42 | 161.23 ± 7.13 | 0.16 |
| BMI (kg/m2) | 31.16 ± 5.13 | 29.44 ± 4.39 | 0.009 |
| Waist | 96.59 ± 16.77 | 98.81 ± 18.83 | 0.36 |
| Hip | 103.88 ± 15.57 | 105.90 ± 16.79 | 0.38 |
| SBP (mmHg) | 126.50 ± 10.66 | 116.60 ± 6.26 | <0.0001 |
| DBP (mmHg) | 79.82 ± 6.27 | 77.22 ± 5.43 | 0.001 |
| FBG (mmol/L) | 12.91 ± 4.32 | 5.44 ± 0.47 | <0.0001 |
| Hb1Ac (%) | 7.22 ± 0.89 | 5.36 ± 0.41 | <0.0001 |
| TG (mmol/L) | 2.09 ± 5.75 | 1.80 ± 0.99 | 0.61 |
| TC (mmol/L) | 5.75 ± 1.18 | 5.17 ± 0.92 | 0.01 |
| HDL-c (mmol/L) | 1.39 ± 1.17 | 0.67 ± 0.30 | <0.0001 |
| LDL-c (mmol/L) | 3.81 ± 0.97 | 3.68 ± 0.80 | 0.29 |
| Family History of T2DM | 105 (100%) | 46 (43.8%) | <0.0001 |
| SNPs | Minor Allele | Controls (n = 105) | T2DM (n = 105) | ||||
|---|---|---|---|---|---|---|---|
| VAF | χ2 | p Value | VAF | χ2 | p Value | ||
| rs11536889 | A | 0.02 | 0.03 | 0.84 | 0.08 | 0.16 | 0.68 |
| rs4986790 | G | 0.00 | 0.002 | 0.96 | 0.02 | 0.06 | 0.80 |
| rs4986791 | T | 0.13 | 2.48 | 0.11 | 0.30 | 8.32 | 0.003 |
| Gene (rs Number) | Genotypes | T2DM Cases (n = 105) | Controls (n = 105) | OR (95%CI) and p Value |
|---|---|---|---|---|
| TLR4 (rs11536889) | GG | 89 (84.7%) | 101 (96.2%) | Reference |
| GC | 15 (14.3%) | 04 (3.8%) | OR—4.25 (95%CI: 1.36–13.29); p = 0.007 | |
| CC | 01 (0.9%) | 00 (00%) | OR—3.41 (95%CI: 0.13–84.56); p = 0.42 * | |
| GC + CC Vs GG | 16 (15.2%) | 04 (3.8%) | OR—4.53 (95%CI: 1.46–14.08); p = 0.004 | |
| GG + CC Vs GC | 90 (85.7%) | 101 (96.2%) | OR—0.23 (95%CI: 0.07–0.74); p = 0.008 | |
| GG + GC Vs CC | 104 (99.1%) | 105 (100%) | OR—0.49 (95%CI: 0.01–14.92); p = 0.67 * | |
| TLR4 (rs4986790) | AA | 100 (95.2%) | 104 (99%) | Reference |
| AG | 05 (4.8%) | 01 (1.0%) | OR—5.21 (95%CI: 0.59–45.29); p = 0.09 | |
| GG | 00 (00%) | 00 (00%) | OR—1.00 (95%CI: 0.01–50.85); p = 0.99 | |
| AG + GG Vs AA | 05 (4.8%) | 01 (1.0%) | OR—1.00 (95%CI: 0.01–50.85); p = 0.99 | |
| AA + GG Vs AG | 100 (95.2%) | 104 (99%) | OR—0.19 (95%CI: 0.02–1.67); p = 0.09 | |
| AA + AG Vs GG | 105 (100%) | 105 (100%) | OR—1.00 (95%CI: 0.01–50.85); p = 0.99 | |
| TLR4 (rs4986791) | CC | 46 (43.8%) | 77 (73.3%) | Reference |
| CT | 56 (53.3%) | 28 (26.7%) | OR—3.34 (1.87–5.99); p = 0.0003 | |
| TT | 03 (2.9%) | 00 (0%) * | OR—11.67 (0.58–230.0); p = 0.04 * | |
| CT + TT Vs CC | 59 (56.2%) | 28 (26.7%) | OR—3.52 (1.97–6.29); p = 0.0001 | |
| CC + TT Vs CT | 49 (46.7%) | 77 (73.3%) | OR—0.31 (0.17–0.56); p = 0.0008 | |
| CC + CT Vs TT | 102 (97.1%) | 105 (100%) * | OR—0.31 (0.17–0.56); p = 0.13 |
| Gene (rs Number) | Alleles | T2DM Cases (n = 105) | Control (n = 105) | OR (95%CI) and p Value |
|---|---|---|---|---|
| TLR4 (rs11536889) | G | 193 (91.9%) | 206 (98.1%) | Reference |
| C | 17 (8.1%) | 04 (1.9%) | OR—4.53 (1.51–13.72); p = 0.003 | |
| TLR4 (rs4986790) | A | 205 (97.6%) | 209 (99.5%) | Reference |
| G | 05 (2.4%) | 01 (0.5%) | OR—5.09 (0.59–44.1); p = 0.100 | |
| TLR4 (rs4986791) | C | 148 (70.5%) | 182 (86.7%) | Reference |
| T | 62 (29.5%) | 28 (13.3%) | OR—2.72 (1.65–4.47); p = 0.00005 |
| Covariates | R-Value a | Adjusted R Square Value | Standardized β-Coefficient for rs11536889 | Standardized β-Coefficient for rs4986790 | Standardized β-Coefficient for rs4986791 | F | p Value b |
|---|---|---|---|---|---|---|---|
| Age | 0.067 | −0.025 | 0.033 | 0.064 | −0.004 | 0.154 | 0.927 |
| Gender | 0.066 | −0.025 | 0.002 | 0.066 | −0.007 | 0.149 | 0.930 |
| Weight | 0.130 | −0.012 | −0.039 | 0.119 | 0.023 | 0.581 | 0.629 |
| BMI | 0.069 | −0.025 | −0.002 | 0.053 | −0.038 | 0.159 | 0.924 |
| SBP | 0.084 | −0.022 | −0.011 | −0.004 | 0.084 | 0.241 | 0.868 |
| DBP | 0.110 | −0.017 | −0.029 | 0.082 | −0.052 | 0.410 | 0.746 |
| Waist | 0.119 | −0.015 | −0.075 | 0.079 | 0.035 | 0.482 | 0.696 |
| Hip | 0.238 | 0.029 | 0.039 | −0.058 | 0.219 | 2.029 | 0.115 |
| FBG | 0.253 | 0.036 | −0.021 | 0.188 | −0.146 | 2.298 | 0.082 |
| Hb1Ac | 0.112 | −0.017 | −0.026 | −0.112 | 0.008 | 0.427 | 0.734 |
| TC | 0.217 | 0.019 | −0.091 | −0.139 | 0.146 | 1.657 | 0.181 |
| TG | 0.122 | −0.014 | −0.106 | −0.078 | −0.010 | 0.506 | 0.679 |
| HDLc | 0.717 | 0.500 | 0.701 | −0.085 | −0.046 | 35.714 | <0.001 |
| LDLc | 0.149 | −0.007 | 0.031 | 0.129 | −0.068 | 1.409 | 0.162 |
| TLR4 (rs11536889) | TLR4 (rs4986790) | TLR4 (rs4986791) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| GG (n = 89) | GC (n = 15) | CC (n = 01) | p Value | AA (n = 100) | AG (n = 05) | GG (n = 00) | p Value | CC (n = 46) | CT (n = 56) | TT (n = 03) | p Value | |
| Age | 63.57 ± 8.64 | 63.53 ± 7.04 | 75.00 ± 1.00 | 0.11 | 63.69 ± 8.42 | 63.40 ± 9.81 | 00.00 ± 00.00 | 0.94 | 64.22 ± 9.94 | 63.22 ± 7.22 | 62.00 ± 5.20 | 0.79 |
| Weight | 78.91 ± 12.11 | 83.87 ± 21.01 | 82.5 ± 1.00 | 0.42 | 79.63 ± 13.02 | 80.20 ± 25.62 | 00.00 ± 00.00 | 0.92 | 79.30 ± 14.88 | 80.62 ± 12.52 | 67.00 ± 12.17 | 0.23 |
| BMI | 30.96 ± 4.79 | 32.36 ± 7.04 | 31.43 ± 1.00 | 0.66 | 31.14 ± 5.05 | 31.68 ± 7.18 | 00.00 ± 00.00 | 0.81 | 30.59 ± 5.79 | 31.92 ± 4.40 | 25.66 ± 3.60 | 0.07 |
| Waist | 97.75 ± 14.45 | 88.89 ± 27.79 | 93.00 ± 1.00 | 0.17 | 95.42 ± 14.06 | 122.33 ± 45.71 | 00.00 ± 00.00 | 0.0005 | 98.53 ± 17.36 | 94.50 ± 16.73 | 94.33 ± 9.02 | 0.48 |
| Hip | 104.23 ±15.74 | 101.56 ± 15.07 | 120.00 ± 1.00 | 0.49 | 103.30 ± 15.67 | 116.67 ± 2.08 | 00.00 ± 00.00 | 0.06 | 99.64 ± 17.43 | 109.55 ± 11.94 | 98.00 ± 2.00 | 0.002 |
| SBP | 126.42 ± 10.70 | 125.15 ± 8.91 | 150.00 ± 1.00 | 0.07 | 126.38 ± 10.72 | 130.00 ± 10.00 | 00.00 ± 00.00 | 0.46 | 130.35 ± 10.34 | 123.18 ± 9.95 | 132.50 ± 10.61 | 0.001 |
| DBP | 79.27 ± 6.39 | 82.60 ± 5.17 | 80.00 ± 1.00 | 0.16 | 79.93 ± 6.29 | 76.67 ± 5.77 | 00.00 ± 00.00 | 0.25 | 82.54 ± 6.19 | 77.84 ± 5.80 | 80.00 ± 0.00 | 0.006 |
| FBG | 13.11 ± 4.43 | 11.83 ± 3.64 | 11.36 ± 1.00 | 0.53 | 12.90 ± 4.37 | 13.23 ± 3.32 | 00.00 ± 00.00 | 0.86 | 13.58 ± 4.64 | 12.47 ± 4.01 | 10.97 ± 4.45 | 0.31 |
| Hb1Ac | 7.27 ± 0.91 | 6.88 ± 0.77 | 7.20 ± 1.00 | 0.29 | 7.19 ± 0.90 | 7.82 ± 0.40 | 00.00 ± 00.00 | 0.12 | 7.39 ± 0.92 | 7.04 ± 0.82 | 7.77 ± 1.29 | 0.07 |
| TG | 2.15 ± 2.07 | 1.75 ± 1.00 | 2.25 ± 1.00 | 0.76 | 2.10 ± 1.98 | 2.01 ± 1.09 | 00.00 ± 00.00 | 0.92 | 1.71 ± 0.72 | 2.32 ± 2.51 | 3.64 ± 1.69 | 0.11 |
| TC | 5.85 ± 1.16 | 5.23 ± 1.18 | 5.13 ± 1.00 | 0.14 | 5.75 ± 1.20 | 5.80 ± 0.79 | 00.00 ± 00.00 | 0.93 | 5.77 ± 1.10 | 5.75 ± 1.26 | 5.60 ± 1.15 | 0.97 |
| HDL-c | 1.31 ± 0.97 | 1.88 ± 2.00 | 0.86 ± 1.00 | 0.19 | 1.41 ± 1.19 | 0.98 ± 0.91 | 00.00 ± 00.00 | 0.42 | 1.82 ± 1.41 | 1.05 ± 0.82 | 1.24 ± 0.78 | 0.003 |
| LDL-c | 3.87 ± 0.97 | 3.48 ± 0.94 | 3.24 ± 1.00 | 0.29 | 3.79 ± 0.97 | 4.09 ± 0.94 | 00.00 ± 00.00 | 0.51 | 3.77 ± 0.74 | 3.89 ± 1.09 | 2.72 ± 1.25 | 0.11 |
| S. No | rs11536889 | rs4986790 | rs4986791 | Freq | OR (95%CI) | p-Value |
|---|---|---|---|---|---|---|
| 1 | G | A | C | 0.7367 | 1.00 | 1.00 |
| 2 | G | A | T | 0.199 | 4.27 (2.02–9.01) | <0.0001 |
| 3 | A | A | C | 0.0325 | 8.46 (1.40–51.12) | 0.021 |
| 4 | A | A | T | 0.0127 | 6.42 (0.58–71.52) | 0.13 |
| Subjects | L1 | L2 | D’ | r2 |
|---|---|---|---|---|
| All cases | rs11536889 | rs4986790 | 0.217 | 0.014 |
| All cases | rs11536889 | rs4986791 | 0.029 | 0.02 |
| All cases | rs4986790 | rs4986791 | 0.126 | 0.001 |
| Model No | Best Combination of Genes | Training Accuracy | Testing Accuracy | CVC | p-Value | Total Sensitivity | Total Specificity | X2 | OR (95%CI) | F-Measure | Kappa |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | rs11536889 | 0.6476 | 0.6476 | 10/10 | <0.0001 | 0.5619 | 0.6476 | 18.86 | 3.52 (1.97–6.29) | 0.6146 | 0.2952 |
| 2 | rs11536889, rs4986791 | 0.6857 | 0.6857 | 10/10 | <0.0001 | 0.6571 | 0.7143 | 26.16 | 4.79 (2.67–8.59) | 0.6765 | 0.3714 |
| 3 | rs11536889, rs4986790, rs4986791 | 0.6905 | 0.6905 | 10/10 | <0.0001 | 0.6762 | 0.7048 | 30.51 | 4.98 (2.77–8.93) | 0.686 | 0.381 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alkudmani, Z.S.; Alshammary, A.F.; Ali Khan, I. Molecular Effect of Variants in Toll-like Receptor 4 Gene in Saudi Patients with Type 2 Diabetes Mellitus. Cells 2023, 12, 2340. https://doi.org/10.3390/cells12192340
Alkudmani ZS, Alshammary AF, Ali Khan I. Molecular Effect of Variants in Toll-like Receptor 4 Gene in Saudi Patients with Type 2 Diabetes Mellitus. Cells. 2023; 12(19):2340. https://doi.org/10.3390/cells12192340
Chicago/Turabian StyleAlkudmani, Zeina S., Amal F. Alshammary, and Imran Ali Khan. 2023. "Molecular Effect of Variants in Toll-like Receptor 4 Gene in Saudi Patients with Type 2 Diabetes Mellitus" Cells 12, no. 19: 2340. https://doi.org/10.3390/cells12192340