
The Role of Ionizing Radiation for Diagnosis and Treatment against COVID-19: Evidence and Considerations

 ,
,  , , ,
, , ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Ionizing Radiation for Diagnostic and Therapeutic Purposes
2.3. Ionizing Radiation for Diagnostic Purposes of COVID-19
2.3.1. Τhe Role of Chest X-ray (CXR)
2.3.2. The Role of Chest CT
2.3.3. Scanning Considerations
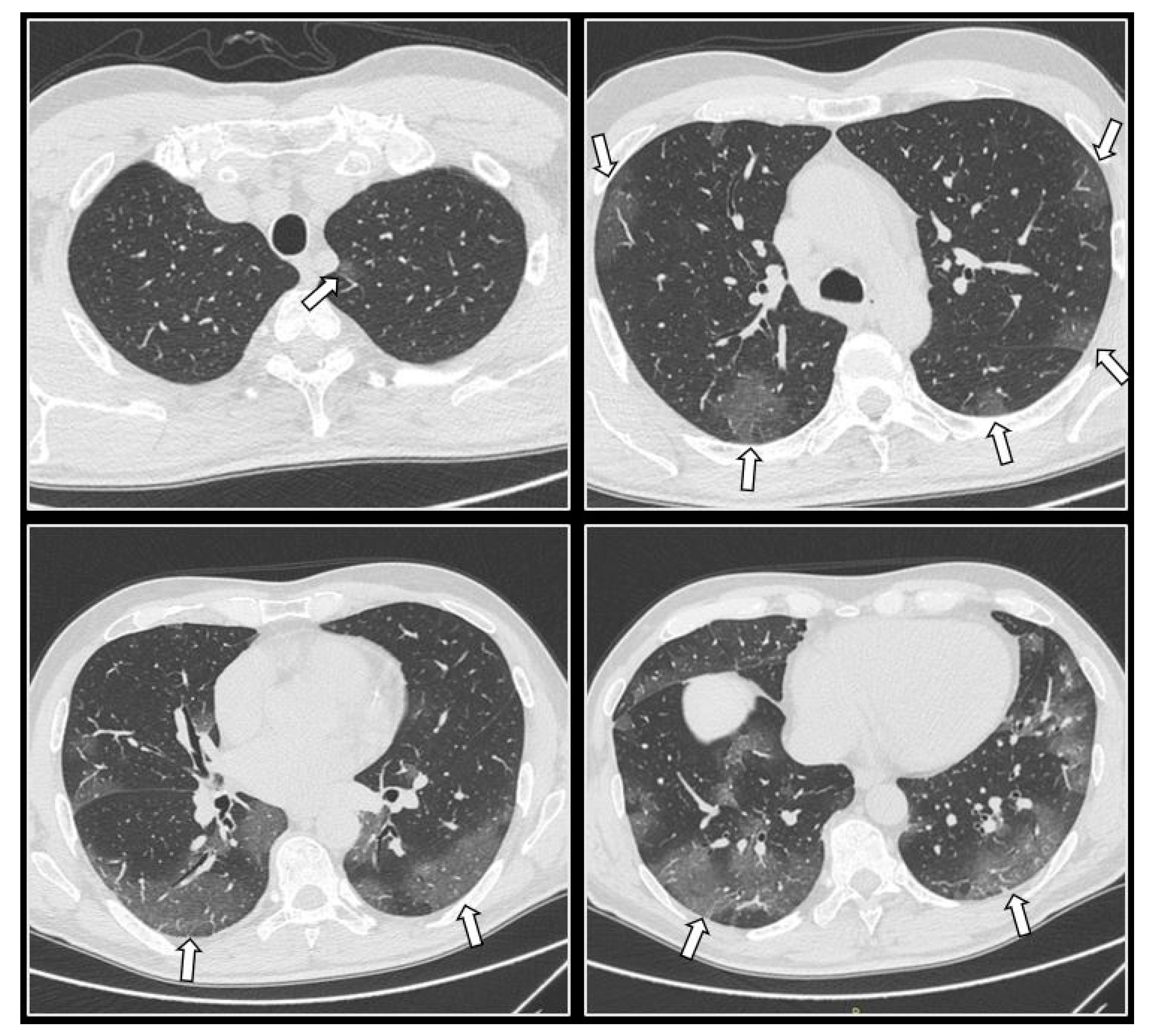
2.3.4. CT Imaging Findings
2.4. Ionizing Radiation for Treatment Purposes of COVID-19
2.4.1. Low-Dose Radiation Therapy (LDRT) for COVID-19: Modulatory Effects
2.4.2. LDRT Clinical Trials
2.4.3. Cancer Risks Due to Whole Lungs LDRT with Different Techniques
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Study | No of pts | Protocol | Effective Dose (mSv) |
|---|---|---|---|
| Tabatabaei et al., 2020 [21] | 20 | HDCT/LDCT | 6.60/1.80 |
| Mohan et al., 2020 [99] | 141 | HDCT/LDCT | 6.33/1.45 |
| Bahrami et al., 2021 [43] | 163 | HDCT/LDCT | 5.8/0.91 |
| Desmet et al., 2021 [77] | 610 | LDCT | 0.74 |
| Leger et al., 2020 [39] | 80 | LDCT | 0.60 |
| Samir et al., 2021 [100] | 250 | uldCT | 0.59 |
| Zarei et al., 2020 [101] | 36 | uldCT | 0.50 |
| Name | Author | Country | Type of Study | Dose (cGy/fx) | Clinical Benefit as per Primary Endpoint |
|---|---|---|---|---|---|
| LOWRAD | Sanmamed [17] | Spain | I-II single-arm | 100/1 | yes |
| - | Ameri [18] | Iran | I-II, single-arm | 50/1 ± 50/2 or 100/1 | yes |
| RESCUE 1–19 (elderly) | Hess [71] | USA | I-II, transitioned to III | 150/1 | yes |
| COVID-RT-01 (critically ill) | Papachristofilou [72] | Switzerland | II, double-arm | 100/1 | no |
| IPACOVID (not ITU candidates) | Arenas [73] | Spain | I, transitioned to II | 50/1 ± 50/2 | yes |
| Trials | Dose Scheme (cGy) | Est Completion/Update |
|---|---|---|
| COLOR 19 Brescia Italy N: 30, Monocentric single arm [102] | 70 | August 2022 |
| PREVENT Ohio, USA N: 100, phase II NCT04466683 [103] | 35 100 | 2022 |
| COVRTE-19 Spain (bad prognosis pts) N: 41, single-arm NCT04414293 [104] | unknown | unknown |
| LOCORAD India N: 20, case control study NCT04904783 [105] | 50 | December 2021 |
| RESCUE 1-19 USA N: 52, phase III NCT04433949 [106] | 150 | 2022 |
| ULTRA-COVID Spain N: 15, single arm NCT04394182 [107] | 80 | 2021 |
| Lancashire, UK, phase I N: 13, Feasibility NCT04572412 [108] | 50 ± 50 | 2021 |
| VENTED COVID Ohio, USA N: 24, phase II NCT04427566 [109] | 80 | December 2021 |
| Madrid, Spain N: 96, phase II, LDRT vs. pharmacological Rx NCT04380818 [110] | 50 ± 50 | 2021 |
| Anti-inflammatory effect Mexico N: 30, randomized double-blinded NCT04534790 [111] | 100 | completed/not published |
| Study | No of pts | Age | RT Technique | Calculated | Estimated | Organs Taken into Account | Prescribed Dose (cGy) | Risk Factors |
|---|---|---|---|---|---|---|---|---|
| Banaei [75] | 32 COVID pts | 32–74 y | 3D-CRT AP-PA | organ mean/max doses | RIC risks | lungs | 100 | cancer site |
| heart | ||||||||
| 3D-CRT 8 fields | CI | breast | gender | |||||
| liver | ||||||||
| IMRT- 8 fields | radiation induced mortality risks | stomach | age at exposure | |||||
| HI | thyroid | |||||||
| VMAT- 2 full arcs | esophagus | time elapsed after exposure | ||||||
| spinal cord | ||||||||
| Arruda [8] | simulation from a median female body | 20–80 y | 3D-CRT AP-PA | organ mean doses | lifetime RIC risks | lung | 50 | cancer site |
| breast | 70 | |||||||
| IMRT- 7 fields | cardiovascular REID due to ischemic heart disease | liver | 100 | gender | ||||
| esophagus | ||||||||
| heart | 150 | age at exposure | ||||||
| Hernandez [76] | reference male and female ICRP phantoms | Adults | 3D-CRT AP-PA | effective dose as the tissue-weighted sum of the equivalent dose in all specified tissues and organs | RIC incidence by cancer site | lungs | 50 | cancer site |
| heart | ||||||||
| breast | ||||||||
| liver | ||||||||
| stomach | 70 | gender | ||||||
| thyroid | ||||||||
| esophagus | ||||||||
| spinal cord | ||||||||
| total RIC obtained by effective dose | brain | |||||||
| salivary glands | ||||||||
| colon | 100 in 2 fx | age at exposure | ||||||
| gonads | ||||||||
| bladder | ||||||||
| skin | ||||||||
| prostate | ||||||||
| uterus | ||||||||
| Shuryak [74] | 24 | 50–85 y | whole-lung irradiation | - | lifetime RIC risk | lung | 50 | gender |
| age at exposure | ||||||||
| heart disease risks | heart | 100 | cigarette smoking | |||||
| 150 | baseline heart disease |
| Study | Organs with Highest Radiation Doses | Organ Dose Differences between Males and Females | Highest RIC Risk | RIC Risk for Other Organs | LAR vs. Age | LAR vs. Sex | Other |
|---|---|---|---|---|---|---|---|
| Banaei [75] | lung | small (except the breast) | lung (for all delivery techniques statistically similar) | breast, and stomach significantly higher in 3D-CRT techniques compared to IMRT or VMAT | at lower ages: | female > male | CI: similar in all techniques |
| heart | higher LAR values | ||||||
| breast (for females) | higher differences among different techniques | HI: IMRT ≈ VMAT (better) <3D-CRT | |||||
| Arruda [8] | lung | - | lung | second highest for females: breast | at lower ages: higher LAR values | female > male (except for liver) | Dose > 100 cGy unacceptable or cautionary |
| heart | |||||||
| breast (for females) | |||||||
| Hernandez [76] | lung | small (except the breast) | lung | second highest for females: breast | at lower ages: higher LAR values | female > male | fractionation scheme: negligible effect on RIC risk |
| heart | second highest for males: heart | ||||||
| breast (for females) | |||||||
| Shuryak [74] | lung | - | lung | second highest: heart | at lower ages: higher LAR values | female > male | lung RIC and heart disease risks higher in: smoking patients & patients with cardiac risk factors |
| heart |
References
- WHO. Estimate of Influenza Deaths Due to Respiratory Disease. Available online: https://www.who.int/teams/global-influenza-programme/surveillance-and-monitoring/burden-of-disease (accessed on 15 January 2022).
- WHO. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/table (accessed on 15 January 2022).
- Wilson, G.D.; Mehta, M.P.; Welsh, J.S.; Chakravarti, A.; Rogers, L.; Fontanesi, J. Investigating Low-Dose Thoracic Radiation as a Treatment for COVID-19 Patients to Prevent Respiratory Failure. Radiat. Res. 2020, 194, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Cao, X. COVID-19: Immunopathology and its implications for therapy. Nat. Rev. Immunol. 2020, 20, 269–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cascella, M.; Rajnik, M.; Cuomo, A.; Dulebohn, S.; Di Napoli, R. Features, Evaluation and Treatment Coronavirus (COVID-19); StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Kirkby, C.; Mackenzie, M. Is low dose radiation therapy a potential treatment for COVID-19 pneumonia? Radiother. Oncol. 2020, 147, 221. [Google Scholar] [CrossRef] [PubMed]
- Ghadimi-Moghadam, A.; Haghani, M.; Bevelacqua, J.E.A. COVID-19 tragic pandemic: Concerns over unintentional “directed accelerated evolution” of novel coronavirus (SARS-CoV-2) and introducing a modified treatment method for ARDS. J. Biomed. Phys. Eng. 2020, 10, 241–246. [Google Scholar]
- Arruda, G.V.; Weber, R.; Bruno, A.C.; Pavoni, J.F. The risk of induced cancer and ischemic heart disease following low dose lung irradiation for COVID-19: Estimation based on a virtual case. Int. J. Radiat. Biol. 2021, 97, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Calabrese, E.J.; Dhawan, G. How radiotherapy was historically used to treat pneumonia: Could it be useful today? Yale J. Biol. Med. 2013, 86, 555–570. [Google Scholar]
- Salomaa, S.; Bouffler, S.D.; Atkinson, M.J.; Cardis, E.; Hamada, N. Is there any supportive evidence for low dose radiotherapy for COVID-19 pneumonia? Int J Radiat Biol 2020, 96, 1228–1235. [Google Scholar] [CrossRef]
- WHO. Ionizing Radiation, Health Effects and Protective Measures. Available online: https://www.who.int/news-room/fact-sheets/detail/ionizing-radiation-health-effects-and-protective-measures (accessed on 15 January 2022).
- American College of Radiology. ACR–SPR–STR Practice Parameter for the Performance of Chest Radiography. Available online: https://www.acr.org/-/media/ACR/Files/Practice-Parameters/ChestRad.pdf (accessed on 16 January 2022).
- Patel, P.; De Jesus, O. CT Scan; StatPearls Publishing LLC: Treasure Island, FL, USA, 2022. [Google Scholar]
- Kazerooni, E.A. High-resolution CT of the lungs. AJR Am. J. Roentgenol. 2001, 177, 501–519. [Google Scholar] [CrossRef]
- ICRP. Application of Ionising Radiation in Healthcare. Available online: http://icrpaedia.org/Application_of_ionising_radiation_in_healthcare (accessed on 17 January 2022).
- Taylor, R.E.; Hatfield, P.; McKeown, S.R.; Prestwich, R.J.; Shaffer, R. Radiotherapy for Benign Disease: Current Evidence, Benefits and Risks. Clin. Oncol. R Coll. Radiol. 2015, 27, 433–435. [Google Scholar] [CrossRef]
- Sanmamed, N.; Alcantara, P.; Cerezo, E.; Gaztañaga, M.; Cabello, N.; Gómez, S.; Bustos, A.; Doval, A.; Corona, J.; Rodriguez, G.; et al. Low-Dose Radiation Therapy in the Management of Coronavirus Disease 2019 (COVID-19) Pneumonia (LOWRAD-Cov19): Preliminary Report. Int. J. Radiat. Oncol. Biol. Phys. 2021, 109, 880–885. [Google Scholar] [CrossRef]
- Ameri, A.; Ameri, P.; Rahnama, N.; Mokhtari, M.; Sedaghat, M.; Hadavand, F.; Bozorgmehr, R.; Haghighi, M.; Taghizadeh-Hesary, F. Low-Dose Whole-Lung Irradiation for COVID-19 Pneumonia: Final Results of a Pilot Study. Int. J. Radiat. Oncol. Biol. Phys. 2021, 109, 859–866. [Google Scholar] [CrossRef] [PubMed]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.; Bleicker, T.; Brünink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. EuroSurveillance 2020, 25, 2000045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Böger, B.; Fachi, M.M.; Vilhena, R.O.; Cobre, A.F.; Tonin, F.S.; Pontarolo, R. Systematic review with meta-analysis of the accuracy of diagnostic tests for COVID-19. Am. J. Infect. Control. 2021, 49, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Tabatabaei, S.M.H.; Talari, H.; Gholamrezanezhad, A.; Farhood, B.; Rahimi, H.; Razzaghi, R.; Mehri, N.; Rajebi, H. A low-dose chest CT protocol for the diagnosis of COVID-19 pneumonia: A prospective study. Emerg. Radiol. 2020, 27, 607–615. [Google Scholar] [CrossRef]
- Azadbakht, J.; Khoramian, D.; Lajevardi, Z.H.; Elikaii, F.; Aflatoonian, A.H.; Farhood, B.; Najafi, M.; Bagher, H. A review on chest CT scanning parameters implemented in COVID-19 patiehts: Bringing low dose CT protocols into play. Egypt. J. Radiol. Nucl. Med. 2021, 52, 13. [Google Scholar] [CrossRef]
- Rubin, G.D.; Ryerson, C.J.; Haramati, L.B.; Sverzellati, N.; Kanne, J.P.; Raoof, S.; Schluger, N.W.; Volpi, A.; Yim, J.J.; Martin, I.B.K.; et al. The Role of Chest Imaging in Patient Management During the COVID-19 Pandemic: A Multinational Consensus Statement from the Fleischner Society. Chest 2020, 158, 106–116. [Google Scholar] [CrossRef]
- Yoon, S.H.; Lee, K.H.; Kim, J.Y.; Lee, Y.K.; Ko, H.; Kim, K.H.; Park, C.M.; Kim, Y.H. Chest Radiographic and CT Findings of the 2019 Novel Coronavirus Disease (COVID-19): Analysis of Nine Patients Treated in Korea. Korean J. Radiol. 2020, 21, 494–500. [Google Scholar] [CrossRef]
- Wong, H.Y.F.; Lam, H.Y.S.; Fong, A.H.; Leung, S.T.; Chin, T.W.; Lo, C.S.Y.; Lui, M.M.; Lee, J.C.Y.; Chiu, K.W.; Chung, T.W.; et al. Frequency and Distribution of Chest Radiographic Findings in Patients Positive for COVID-19. Radiology 2020, 296, E72–E78. [Google Scholar] [CrossRef] [Green Version]
- Ng, M.Y.; Lee, E.Y.P.; Yang, J.; Yang, F.; Li, X.; Wang, H.; Lui, M.M.; Lo, C.S.; Leung, B.; Khong, P.L.; et al. Imaging Profile of the COVID-19 Infection: Radiologic Findings and Literature Review. Radiol. Cardiothorac. Imaging 2020, 2, e200034. [Google Scholar] [CrossRef] [Green Version]
- Cellina, M.; Orsi, M.; Toluian, T.; Valenti Pittino, C.; Oliva, G. False negative chest X-Rays in patients affected by COVID-19 pneumonia and corresponding chest CT findings. Radiography 2020, 26, e189–e194. [Google Scholar] [CrossRef]
- Revel, M.P.; Parkar, A.P.; Prosch, H.; Silva, M.; Sverzellati, N.; Gleeson, F.; Brady, A. COVID-19 patients and the radiology department—Advice from the European Society of Radiology (ESR) and the European Society of Thoracic Imaging (ESTI). Eur. Radiol. 2020, 30, 4903–4909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, X.; Zhong, Z.; Zhao, W.; Zheng, C.; Wang, F.; Liu, J. Chest CT for Typical Coronavirus Disease 2019 (COVID-19) Pneumonia: Relationship to Negative RT-PCR Testing. Radiology 2020, 296, E41–E45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ai, T.; Yang, Z.; Hou, H.; Zhan, C.; Chen, C.; Lv, W.; Tao, Q.; Sun, Z.; Xia, L. Correlation of Chest CT and RT-PCR Testing for Coronavirus Disease 2019 (COVID-19) in China: A Report of 1014 Cases. Radiology 2020, 296, E32–E40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simpson, S.; Kay, F.U.; Abbara, S.; Bhalla, S.; Chung, J.H.; Chung, M.; Henry, T.S.; Kanne, J.P.; Kligerman, S.; Ko, J.P.; et al. Radiological Society of North America Expert Consensus Statement on Reporting Chest CT Findings Related to COVID-19. Endorsed by the Society of Thoracic Radiology, the American College of Radiology, and RSNA—Secondary Publication. J. Thorac. Imaging 2020, 35, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Salehi, S.; Abedi, A.; Balakrishnan, S.; Gholamrezanezhad, A. Coronavirus Disease 2019 (COVID-19): A Systematic Review of Imaging Findings in 919 Patients. AJR Am. J. Roentgenol. 2020, 215, 87–93. [Google Scholar] [CrossRef]
- Kalra, M.K.; Homayounieh, F.; Arru, C.; Holmberg, O.; Vassileva, J. Chest CT practice and protocols for COVID-19 from radiation dose management perspective. Eur. Radiol. 2020, 30, 6554–6560. [Google Scholar] [CrossRef] [PubMed]
- American College of Radiology. ACR Recommendations for the Use of Chest Radiography and Computed Tomography (CT) for Suspected COVID-19 Infection. Available online: https://psnet.ahrq.gov/issue/acr-recommendations-use-chest-radiography-and-computed-tomography-ct-suspected-covid-19 (accessed on 25 October 2021).
- Centers for Disease Control and Prevention. Interim Clinical Guidance for Management of Patients with Confirmed Coronavirus Disease (COVID-19). Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-guidance-management-patients.html (accessed on 8 October 2021).
- Society of Thoracic Radiology & American Society of Emergency Radiology. STR/ASER COVID-19 Position Statement. Available online: https://thoracicrad.org/?page_id=2879#accordion-1-1 (accessed on 20 October 2021).
- Sverzellati, N.; Milanese, G.; Milone, F.; Balbi, M.; Ledda, R.E.; Silva, M. Integrated Radiologic Algorithm for COVID-19 Pandemic. J. Thorac. Imaging 2020, 35, 228–233. [Google Scholar] [CrossRef]
- Argentieri, G.; Bellesi, L.; Pagnamenta, A.; Vanini, G.; Presilla, S.; Del Grande, F.; Marando, M.; Gianella, P. Diagnostic yield, safety, and advantages of ultra-low dose chest CT compared to chest radiography in early stage suspected SARS-CoV-2 pneumonia: A retrospective observational study. Medicine 2021, 100, e26034. [Google Scholar] [CrossRef]
- Leger, T.; Jacquier, A.; Barral, P.A.; Castelli, M.; Finance, J.; Lagier, J.C.; Million, M.; Parola, P.; Brouqui, P.; Raoult, D.; et al. Low-dose chest CT for diagnosing and assessing the extent of lung involvement of SARS-CoV-2 pneumonia using a semi quantitative score. PLoS ONE 2020, 15, e0241407. [Google Scholar] [CrossRef]
- Agostini, A.; Floridi, C.; Borgheresi, A.; Badaloni, M.; Esposto Pirani, P.; Terilli, F.; Ottaviani, L.; Giovagnoni, A. Proposal of a low-dose, long-pitch, dual-source chest CT protocol on third-generation dual-source CT using a tin filter for spectral shaping at 100 kVp for CoronaVirus Disease 2019 (COVID-19) patients: A feasibility study. Radiol. Med. 2020, 125, 365–373. [Google Scholar] [CrossRef] [Green Version]
- Gudjonsdottir, J.; Svensson, J.R.; Campling, S.; Brennan, P.C.; Jonsdottir, B. Efficient use of automatic exposure control systems in computed tomography requires correct patient positioning. Acta Radiol. 2009, 50, 1035–1041. [Google Scholar] [CrossRef] [PubMed]
- Homayounieh, F.; Holmberg, O.; Umairi, R.A.; Aly, S.; Basevičius, A.; Costa, P.R.; Darweesh, A.; Gershan, V.; Ilves, P.; Kostova-Lefterova, D.; et al. Variations in CT Utilization, Protocols, and Radiation Doses in COVID-19 Pneumonia: Results from 28 Countries in the IAEA Study. Radiology 2021, 298, E141–E151. [Google Scholar] [CrossRef] [PubMed]
- Bahrami-Motlagh, H.; Abbasi, S.; Haghighimorad, M.; Salevatipour, B.; Alavi Darazam, I. Performance of Low-Dose Chest CT Scan for Initial Triage of COVID-19. Iran. J. Radiol. 2020, 17, e104950. [Google Scholar] [CrossRef]
- Pan, F.; Ye, T.; Sun, P.; Gui, S.; Liang, B.; Li, L.; Zheng, D.; Wang, J.; Hesketh, R.L.; Yang, L.; et al. Time Course of Lung Changes at Chest CT during Recovery from Coronavirus Disease 2019 (COVID-19). Radiology 2020, 295, 715–721. [Google Scholar] [CrossRef] [Green Version]
- Arkoudis, N.A.; Tsochatzis, A.; Argentos, S.; Kontopoulou, C.; Mademli, M.; Spiliopoulos, S.; Oikonomopoulos, N. CT in patients with COVID-19: Imaging patterns, disease extent and evolution; our experience in a Greek reference University Hospital. Hell. J. Radiol. 2021, 6, 1. [Google Scholar] [CrossRef]
- Guan, C.S.; Lv, Z.B.; Li, J.J.; Du, Y.N.; Chen, H.; Cui, T.; Guo, N.; Chen, B.D.; Xie, R.M. CT appearances, patterns of progression, and follow-up of COVID-19: Evaluation on thin-section CT. Insights Imaging 2021, 12, 73. [Google Scholar] [CrossRef]
- Li, K.; Fang, Y.; Li, W.; Pan, C.; Qin, P.; Zhong, Y.; Liu, X.; Huang, M.; Liao, Y.; Li, S. CT image visual quantitative evaluation and clinical classification of coronavirus disease (COVID-19). Eur. Radiol. 2020, 30, 4407–4416. [Google Scholar] [CrossRef] [Green Version]
- Yang, R.; Li, X.; Liu, H.; Zhen, Y.; Zhang, X.; Xiong, Q.; Luo, Y.; Gao, C.; Zeng, W. Chest CT Severity Score: An Imaging Tool for Assessing Severe COVID-19. Radiol. Cardiothorac. Imaging 2020, 2, e200047. [Google Scholar] [CrossRef] [Green Version]
- Guillo, E.; Bedmar Gomez, I.; Dangeard, S.; Bennani, S.; Saab, I.; Tordjman, M.; Jilet, L.; Chassagnon, G.; Revel, M.P. COVID-19 pneumonia: Diagnostic and prognostic role of CT based on a retrospective analysis of 214 consecutive patients from Paris, France. Eur. J. Radiol. 2020, 131, 109209. [Google Scholar] [CrossRef]
- Colombi, D.; Bodini, F.C.; Petrini, M.; Maffi, G.; Morelli, N.; Milanese, G.; Silva, M.; Sverzellati, N.; Michieletti, E. Well-aerated Lung on Admitting Chest CT to Predict Adverse Outcome in COVID-19 Pneumonia. Radiology 2020, 296, E86–E96. [Google Scholar] [CrossRef] [Green Version]
- Grégory, J.; Raynaud, L.; Galy, A.; Corre, F.; Bijot, J.C.; Nguyen, Y.; Vilgrain, V. Extension of COVID-19 pulmonary parenchyma lesions based on real-life visual assessment on initial chest CT is an independent predictor of poor patient outcome. Infect. Dis. 2020, 52, 838–840. [Google Scholar] [CrossRef] [PubMed]
- Ahlstrand, E.; Cajander, S.; Cajander, P.; Ingberg, E.; Löf, E.; Wegener, M.; Lidén, M. Visual scoring of chest CT at hospital admission predicts hospitalization time and intensive care admission in COVID-19. Infect. Dis. 2021, 53, 622–632. [Google Scholar] [CrossRef] [PubMed]
- Rödel, F.; Frey, B.; Manda, K.; Hildebrandt, G.; Hehlgans, S.; Keilholz, L.; Seegenschmiedt, M.H.; Gaipl, U.S.; Rödel, C. Immunomodulatory properties and molecular effects in inflammatory diseases of low-dose x-irradiation. Front. Oncol 2012, 2, 120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rousseau, J.; Johnson, W.; Harrell, G. The value of roentgen therapy in pneumonia which fails to respond to the sulfonamides. Radiology 1942, 38, 281–289. [Google Scholar] [CrossRef]
- Seegenschmiedt, M.H.; Micke, O.; Muecke, R. Radiotherapy for non-malignant disorders: State of the art and update of the evidence-based practice guidelines. Br. J. Radiol 2015, 88, 20150080. [Google Scholar] [CrossRef]
- Torres Royo, L.; Antelo Redondo, G.; Árquez Pianetta, M.; Arenas Prat, M. Low-Dose radiation therapy for benign pathologies. Rep. Pract. Oncol. Radiother. 2020, 25, 250–254. [Google Scholar] [CrossRef]
- Tufan, A.; Avanoğlu Güler, A.; Matucci-Cerinic, M. COVID-19, immune system response, hyperinflammation and repurposing antirheumatic drugs. Turk. J. Med. Sci. 2020, 50, 620–632. [Google Scholar] [CrossRef]
- Blot, M.; Bour, J.-B.; Quenot, J.P.; Bourredjem, A.; Nguyen, M.; Guy, J.; Monier, S.; Georges, M.; Large, A.; Dargent, A.; et al. The dysregulated innate immune response in severe COVID-19 pneumonia that could drive poorer outcome. J. Transl. Med. 2020, 18, 457. [Google Scholar] [CrossRef]
- Song, E.; Zhang, C.; Israelow, B.; Lu-Culligan, A.; Prado, A.V.; Skriabine, S.; Lu, P.; Weizman, O.-E.; Liu, F.; Dai, Y.; et al. Neuroinvasion of SARS-CoV-2 in human and mouse brain. bioRxiv 2020, 218, e20202135. [Google Scholar] [CrossRef]
- Murira, A.; Lamarre, A. Type-I Interferon Responses: From Friend to Foe in the Battle against Chronic Viral Infection. Front. Immunol. 2016, 7, 609. [Google Scholar] [CrossRef] [Green Version]
- Kindler, E.; Thiel, V. SARS-CoV and IFN: Too Little, Too Late. Cell Host Microbe 2016, 19, 139–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, Y.; Wang, Y.; Shao, C.; Huang, J.; Gan, J.; Huang, X.; Bucci, E.; Piacentini, M.; Ippolito, G.; Melino, G. COVID-19 infection: The perspectives on immune responses. Cell Death Differ. 2020, 27, 1451–1454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duan, K.; Liu, B.; Li, C.; Zhang, H.; Yu, T.; Qu, J.; Zhou, M.; Chen, L.; Meng, S.; Hu, Y.; et al. Effectiveness of convalescent plasma therapy in severe COVID-19 patients. Proc. Natl. Acad. Sci. USA 2020, 117, 9490–9496. [Google Scholar] [CrossRef] [Green Version]
- Yang, G.; Kong, Q.; Wang, G.; Jin, H.; Zhou, L.; Yu, D.; Niu, C.; Han, W.; Li, W.; Cui, J. Low-dose ionizing radiation induces direct activation of natural killer cells and provides a novel approach for adoptive cellular immunotherapy. Cancer Biother. Radiopharm. 2014, 29, 428–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thevarajan, I.; THi, H.; Koutsakos, M.; Druce, J.; Caly, L.; van de Sandt, C.; Jia, X.; Nicholson, S.; Catton, M.; Covie, B.; et al. Breadth of concomitant immune responses prior to patient recovery: A case report of non-severe COVID-19. Nat. Med. 2020, 26, 453–455. [Google Scholar] [CrossRef] [Green Version]
- Georgakilas, A.G.; O’Neill, P.; Stewart, R.D. Induction and Repair of Clustered DNA Lesions: What Do We Know So Far? Radiat. Res. 2013, 180, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Nikitaki, Z.; Nikolov, V.; Mavragani, I.V.; Mladenov, E.; Mangelis, A.; Laskaratou, D.A.; Fragkoulis, G.I.; Hellweg, C.E.; Martin, O.A.; Emfietzoglou, D.; et al. Measurement of complex DNA damage induction and repair in human cellular systems after exposure to ionizing radiations of varying linear energy transfer (LET). Free Radic Res. 2016, 50, S64–S78. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Z.; Li, H.; Wu, X.; Zhong, Y.; Zhang, K.; Zhang, Y.-P.; Boerwinkle, E.; Fu, Y.-X. Moderate mutation rate in the SARS coronavirus genome and its implications. BMC Evol. Biol. 2004, 4, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dos Santos, M.; Delorme, R.; Salmon, R.; Prezado, Y. Minibeam radiation therapy: A micro- and nano-dosimetry Monte Carlo study. Med. Phys. 2020, 47, 1379–1390. [Google Scholar] [CrossRef] [PubMed]
- Chung, M.; Bernheim, A.; Mei, X.; Zhang, N.; Huang, M.; Zeng, X.; Cui, J.; Xu, W.; Yang, Y.; Fayad, Z.A.; et al. CT Imaging Features of 2019 Novel Coronavirus (2019-nCoV). Radiology 2020, 295, 202–207. [Google Scholar] [CrossRef] [Green Version]
- Hess, C.B.; Nasti, T.H.; Dhere, V.R.; Kleber, T.J.; Switchenko, J.M.; Buchwald, Z.S.; Stokes, W.A.; Weinberg, B.D.; Rouphael, N.; Steinberg, J.P.; et al. Immunomodulatory Low-Dose Whole-Lung Radiation for Patients with Coronavirus Disease 2019-Related Pneumonia. Int. J. Radiat. Oncol. Biol. Phys. 2021, 109, 867–879. [Google Scholar] [CrossRef] [PubMed]
- Papachristofilou, A.; Finazzi, T.; Blum, A.; Zehnder, T.; Zellweger, N.; Lustenberger, J.; Bauer, T.; Dott, C.; Avcu, Y.; Kohler, G.; et al. Low-Dose Radiation Therapy for Severe COVID-19 Pneumonia: A Randomized Double-Blind Study. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 1274–1282. [Google Scholar] [CrossRef] [PubMed]
- Arenas, M.; Algara, M.; De Febrer, G.; Rubio, C.; Sanz, X.; de la Casa, M.A.; Vasco, C.; Marín, J.; Fernández-Letón, P.; Villar, J.; et al. Could pulmonary low-dose radiation therapy be an alternative treatment for patients with COVID-19 pneumonia? Preliminary results of a multicenter SEOR-GICOR nonrandomized prospective trial (IPACOVID trial). Strahlenther Onkol. 2021, 197, 1010–1020. [Google Scholar] [CrossRef] [PubMed]
- Shuryak, I.; Kachnic, L.A.; Brenner, D.J. Lung Cancer and Heart Disease Risks Associated with Low-Dose Pulmonary Radiotherapy to COVID-19 Patients with Different Background Risks. Int. J. Radiat. Oncol. Biol. Phys. 2021, 111, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Banaei, A.; Hashemi, B.; Bakhshandeh, M. Estimating Cancer Risks Due to Whole Lungs Low Treating COVID-19 Pneumonia. Radiat. Oncol. 2021, 17, 10. [Google Scholar] [CrossRef]
- García-Hernández, T.; Romero-Expósito, M.; Sánchez-Nieto, B. Low dose radiation therapy for COVID-19: Effective dose and estimation of cancer risk. Radiother. Oncol. 2020, 153, 289–295. [Google Scholar] [CrossRef]
- Desmet, J.; Biebaû, C.; De Wever, W.; Cockmartin, L.; Viktor, V.; Coolen, J.; Verschakelen, J.; Dubbeldam, A. Performance of Low-Dose Chest CT as a Triage Tool for Suspected COVID-19 Patients. J. Belg Soc. Radiol. 2021, 105, 9. [Google Scholar] [CrossRef]
- Tofighi, S.; Najafi, S.; Johnston, S.K.; Gholamrezanezhad, A. Low-dose CT in COVID-19 outbreak: Radiation safety, image wisely, and image gently pledge. Emerg Radiol 2020, 27, 601–605. [Google Scholar] [CrossRef]
- Kwee, T.C.; Kwee, R.M. Chest CT in COVID-19: What the Radiologist Needs to Know. Radiographics 2020, 40, 1848–1865. [Google Scholar] [CrossRef]
- Kang, Z.; Li, X.; Zhou, S. Recommendation of low-dose CT in the detection and management of COVID-2019. Eur. Radiol. 2020, 30, 4356–4357. [Google Scholar] [CrossRef] [Green Version]
- Cristofaro, M.; Fusco, N.; Petrone, A.; Albarello, F.; Di Stefano, F.; Pianura, E.; Schininà, V.; Ianniello, S.; Campioni, P. Increased Radiation Dose Exposure in Thoracic Computed Tomography in Patients with COVID-19. Radiation 2021, 1, 14. [Google Scholar] [CrossRef]
- Karam, M.; Althuwaikh, S.; Alazemi, M.; Abul, A.; Hayre, A.; Alsaif, A.; Barlow, G. Chest CT versus RT-PCR for the detection of COVID-19: Systematic review and meta-analysis of comparative studies. JRSM Open 2021, 12, 20542704211011837. [Google Scholar] [CrossRef] [PubMed]
- Dangis, A.; Gieraerts, C.; De Bruecker, Y.; Janssen, L.; Valgaeren, H.; Obbels, D.; Gillis, M.; Van Ranst, M.; Frans, J.; Demeyere, A.; et al. Accuracy and Reproducibility of Low-Dose Submillisievert Chest CT for the Diagnosis of COVID-19. Radiol. Cardiothorac. Imaging 2020, 2, e200196. [Google Scholar] [CrossRef] [Green Version]
- Jindal, H.; Jain, S.; Suvvari, T.K.; Kutikuppala, L.; Rackimuthu, S.; Rocha, I.C.N.; Goyal, S.; Radha. False-Negative RT-PCR Findings and Double Mutant Variant as Factors of an Overwhelming Second Wave of COVID-19 in India: An Emerging Global Health Disaster. SN Compr. Clin. Med. 2021, 3, 2383–2388. [Google Scholar] [CrossRef] [PubMed]
- Gökharman, F.D.; Ertem, G.T.; Aydın, S.; Büyükdemirci, A.; Yüksekkaya, E.; Tokur, O.; Koşar, P.N. Evaluation of thorax computed tomographic findings in COVID-19 variant cases. Respir. Investig. 2022, in press. [CrossRef]
- Cheng, Q.R.; Fan, M.X.; Hao, J.; Hu, X.C.; Ge, X.H.; Hu, Z.L.; Li, Z. Chest CT features of children infected by B.1.617.2 (Delta) variant of COVID-19. World J. Pediatr 2022, 18, 37–42. [Google Scholar] [CrossRef]
- Brakohiapa, E.K.K.; Sarkodie, B.D.; Botwe, B.O.; Dzefi-Tettey, K.; Anim, D.A.; Edzie, E.K.M.; Goleku, P.N.; Jimah, B.B.; Amankwa, A.T. Comparing radiological presentations of first and second strains of COVID-19 infections in a low-resource country. Heliyon 2021, 7, e07818. [Google Scholar] [CrossRef]
- Hautmann, M.G.; Rechner, P.; Neumaier, U.; Süß, C.; Dietl, B.; Putz, F.J.; Behr, M.; Kölbl, O.; Steger, F. Radiotherapy for osteoarthritis-an analysis of 295 joints treated with a linear accelerator. Strahlenther Onkol. 2020, 196, 715–724. [Google Scholar] [CrossRef]
- Álvarez, B.; Montero, Á.; Aramburu, F.; Calvo, E.; Ángel de la Casa, M.; Valero, J.; Hernando, O.; López, M.; Ciérvide, R.; García-Aranda, M.; et al. Radiotherapy for ostheoarticular degenerative disorders: When nothing else works. Osteoarthr. Cartil. Open 2020, 1, 100016. [Google Scholar] [CrossRef]
- Koc, B.B.; Schotanus, M.G.M.; Borghans, R.; Jong, B.; Maassen, M.E.; Buijsen, J.; Jansen, E.J.P. Short-term pain reduction after low-dose radiotherapy in patients with severe osteoarthritis of the hip or knee joint: A cohort study and literature review. Eur. J. Orthop. Surg. Traumatol. 2019, 29, 843–847. [Google Scholar] [CrossRef]
- Donaubauer, A.J.; Zhou, J.G.; Ott, O.J.; Putz, F.; Fietkau, R.; Keilholz, L.; Gaipl, U.S.; Frey, B.; Weissmann, T. Low Dose Radiation Therapy, Particularly with 0.5 Gy, Improves Pain in Degenerative Joint Disease of the Fingers: Results of a Retrospective Analysis. Int. J. Mol. Sci. 2020, 21, 5854. [Google Scholar] [CrossRef] [PubMed]
- Kirsch, D.G.; Diehn, M.; Cucinotta, F.A.; Weichselbaum, R. Lack of supporting data make the risks of a clinical trial of radiation therapy as a treatment for COVID-19 pneumonia unacceptable. Radiother. Oncol. 2020, 147, 217–220. [Google Scholar] [CrossRef] [PubMed]
- Little, M.P.; Zhang, W.; van Dusen, R.; Hamada, N. Pneumonia After Bacterial or Viral Infection Preceded or Followed by Radiation Exposure: A Reanalysis of Older Radiobiologic Data and Implications for Low-Dose Radiation Therapy for Coronavirus Disease 2019 Pneumonia. Int. J. Radiat. Oncol. Biol. Phys. 2021, 109, 849–858. [Google Scholar] [CrossRef] [PubMed]
- Salomaa, S.; Cardis, E.; Bouffler, S.D.; Atkinson, M.J.; Hamada, N. Low dose radiation therapy for COVID-19 pneumonia: Is there any supportive evidence? Int. J. Radiat. Biol. 2020, 96, 1224–1227. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.J.; Sun, J.G.; Sun, J.; Ming, H.; Wang, X.X.; Wu, L.; Chen, Z.T. Prediction of radiation pneumonitis in lung cancer patients: A systematic review. J. Cancer Res. Clin. Oncol. 2012, 138, 2103–2116. [Google Scholar] [CrossRef] [PubMed]
- Schneider, U. Mechanistic model of radiation-induced cancer after fractionated radiotherapy using the linear-quadratic formula. Med. Phys. 2009, 36, 1138–1143. [Google Scholar] [CrossRef] [PubMed]
- Schneider, U.; Sumila, M.; Robotka, J. Site-specific dose-response relationships for cancer induction from the combined Japanese A-bomb and Hodgkin cohorts for doses relevant to radiotherapy. Biol Med. Model. 2011, 8, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sodickson, A.; Baeyens, P.F.; Andriole, K.P.; Prevedello, L.M.; Nawfel, R.D.; Hanson, R.; Khorasani, R. Recurrent CT, cumulative radiation exposure, and associated radiation-induced cancer risks from CT of adults. Radiology 2009, 251, 175–184. [Google Scholar] [CrossRef]
- Mohan, M.H.; Jobayr, M.R. Low-dose chest CT protocol to diagnose and discriminate COVID-19 from other infections compared to a standard dose. Ann. Rom. Soc. Cell Biol. 2021, 25, 4035–4044. [Google Scholar]
- Samir, A.; El-Husseiny, R.M.; Sweed, R.A.; El-Maaboud, N.A.E.-M.A.; Masoud, M. Ultra-low-dose chest CT protocol during the second wave of COVID-19 pandemic: A double-observer prospective study on 250 patients to evaluate its detection accuracy. Egypt. J. Radiol. Nucl. Med. 2021, 52, 136. [Google Scholar] [CrossRef]
- Zarei, F.; Lotfi, M.; Jalli, R.; Iranpour, P. Evaluation of Ultra Low Dose Chest CT Imaging for COVID-19 Diagnosis and Follow Up. Available online: https://arxiv.org/abs/2005.03347v1 (accessed on 2 October 2021).
- Magrini, S.M.; Azienda Socio Sanitaria Territoriale Degli Spedali Civili di Brescia. COVID-19 Pneumonitis Low Dose Lung Radiotherapy (COLOR-19). Available online: https://clinicaltrials.gov/ct2/show/NCT04377477 (accessed on 11 November 2021).
- Ohio State University Comprehensive Cancer Center. Low-Dose Radiotherapy for Patients with SARS-CoV-2 (COVID-19) Pneumonia (PREVENT). Available online: https://clinicaltrials.gov/ct2/show/NCT04466683 (accessed on 10 November 2021).
- Albiach, C.F.; Hospital Provincial de Castellon. Low Dose Pulmonary Irradiation in Patients with COVID-19 Infection of Bad Prognosis (COVRTE-19). Available online: https://clinicaltrials.gov/ct2/show/NCT04414293 (accessed on 10 November 2021).
- Datta, N.R.; Mahatma Gandhi Institute of Medical Sciences. Low-Dose Radiation Therapy to Lungs in Moderate COVID-19 Pneumonitis: A Case-Control Pilot Study (LOCORAD). Available online: https://clinicaltrials.gov/ct2/show/NCT04904783 (accessed on 10 November 2021).
- Khan, M.K.; Emory University. Best Supportive Care with or without Low Dose Whole Lung Radiation Therapy for the Treatment of COVID-19 (RESCUE1-19). Available online: https://clinicaltrials.gov/ct2/show/NCT04433949 (accessed on 10 November 2021).
- Fundacion GenesisCare. Ultra Low Doses of Therapy with Radiation Applicated to COVID-19 (ULTRA-COVID). Available online: https://clinicaltrials.gov/ct2/show/NCT04394182 (accessed on 10 November 2021).
- Lancashire Teaching Hospitals NHS Foundation Trust. Low Dose Lung Radiotherapy to Treat COVID-19 Pneumonia. Available online: https://clinicaltrials.gov/ct2/show/NCT04572412 (accessed on 10 November 2021).
- Chakravarti, A.; Ohio State University Comprehensive Cancer Center. Low Dose Whole Lung Radiation Therapy for Patients with COVID-19 and Respiratory Compromise (VENTED). Available online: https://clinicaltrials.gov/ct2/show/NCT04427566 (accessed on 10 November 2021).
- Grupo de Investigación Clínica en Oncología Radioterapia. Low Dose Anti-Inflammatory Radiotherapy for the Treatment of Pneumonia by COVID-19. Available online: https://clinicaltrials.gov/ct2/show/NCT04380818 (accessed on 10 November 2021).
- Guzmán, A.O.; Instituto Mexicano del Seguro Social. Anti-Inflammatory Effect of Low-Dose Whole-Lung Radiation for COVID-19 Pneumonia. Available online: https://clinicaltrials.gov/ct2/show/NCT04534790 (accessed on 10 November 2021).

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chalkia, M.; Arkoudis, N.-A.; Maragkoudakis, E.; Rallis, S.; Tremi, I.; Georgakilas, A.G.; Kouloulias, V.; Efstathopoulos, E.; Platoni, K. The Role of Ionizing Radiation for Diagnosis and Treatment against COVID-19: Evidence and Considerations. Cells 2022, 11, 467. https://doi.org/10.3390/cells11030467
Chalkia M, Arkoudis N-A, Maragkoudakis E, Rallis S, Tremi I, Georgakilas AG, Kouloulias V, Efstathopoulos E, Platoni K. The Role of Ionizing Radiation for Diagnosis and Treatment against COVID-19: Evidence and Considerations. Cells. 2022; 11(3):467. https://doi.org/10.3390/cells11030467
Chicago/Turabian StyleChalkia, Marina, Nikolaos-Achilleas Arkoudis, Emmanouil Maragkoudakis, Stamatis Rallis, Ioanna Tremi, Alexandros G. Georgakilas, Vassilis Kouloulias, Efstathios Efstathopoulos, and Kalliopi Platoni. 2022. "The Role of Ionizing Radiation for Diagnosis and Treatment against COVID-19: Evidence and Considerations" Cells 11, no. 3: 467. https://doi.org/10.3390/cells11030467