
Modeling the Endothelial Glycocalyx Layer in the Human Conventional Aqueous Outflow Pathway
 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Finite Element Reconstruction, Volume Meshing, Material Models, and Boundary Conditions
2.2. Electrical–Fluid–Structure Interaction
3. Results
4. Discussion
Limitations
5. Conclusions
- (a)
- The endothelial glycocalyx layer in the healthy human outflow pathway was modeled using EFSI.
- (b)
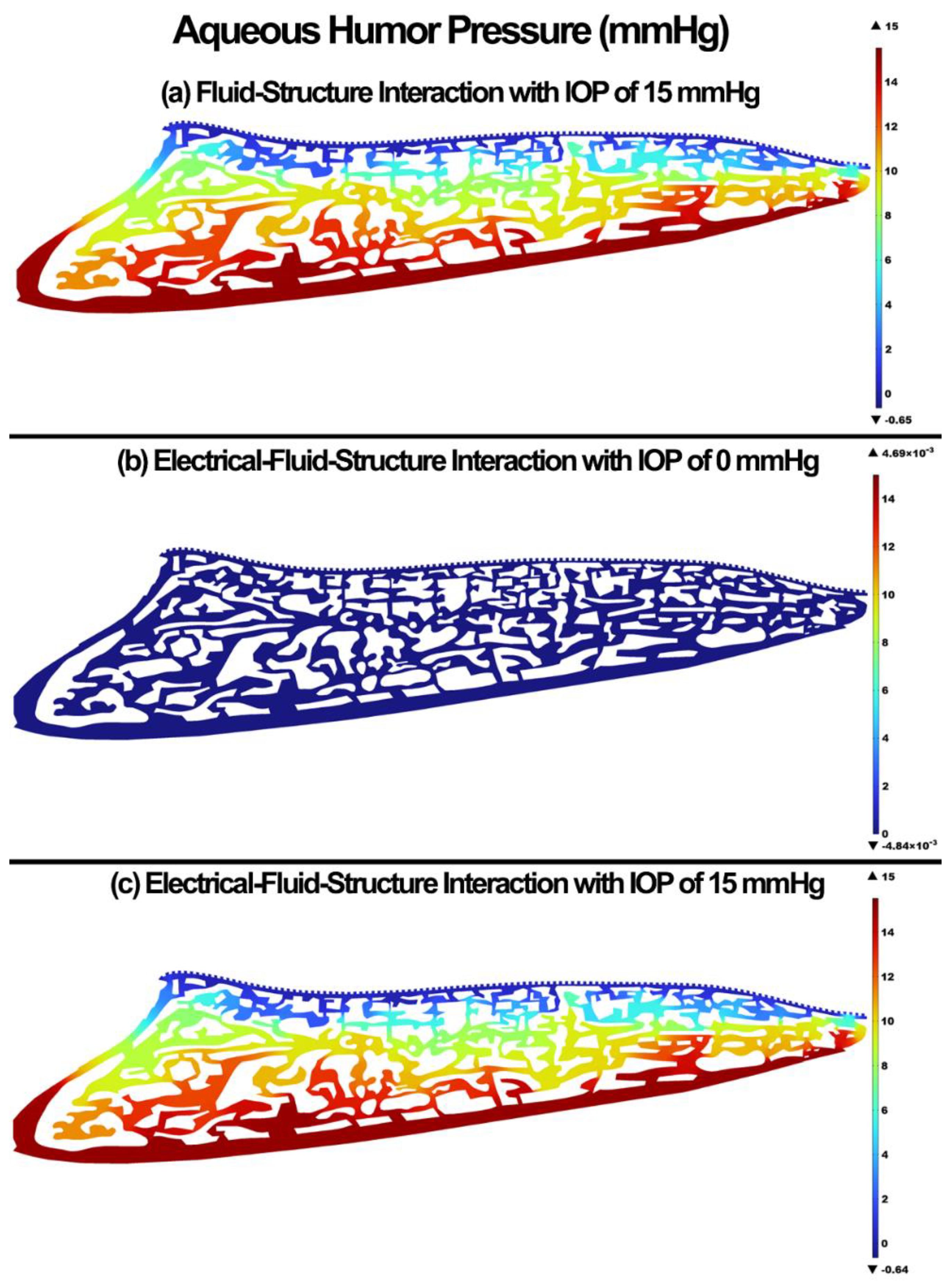
- The positively charged aqueous humor can flow in the negatively outflow pathway with no IOP.
- (c)
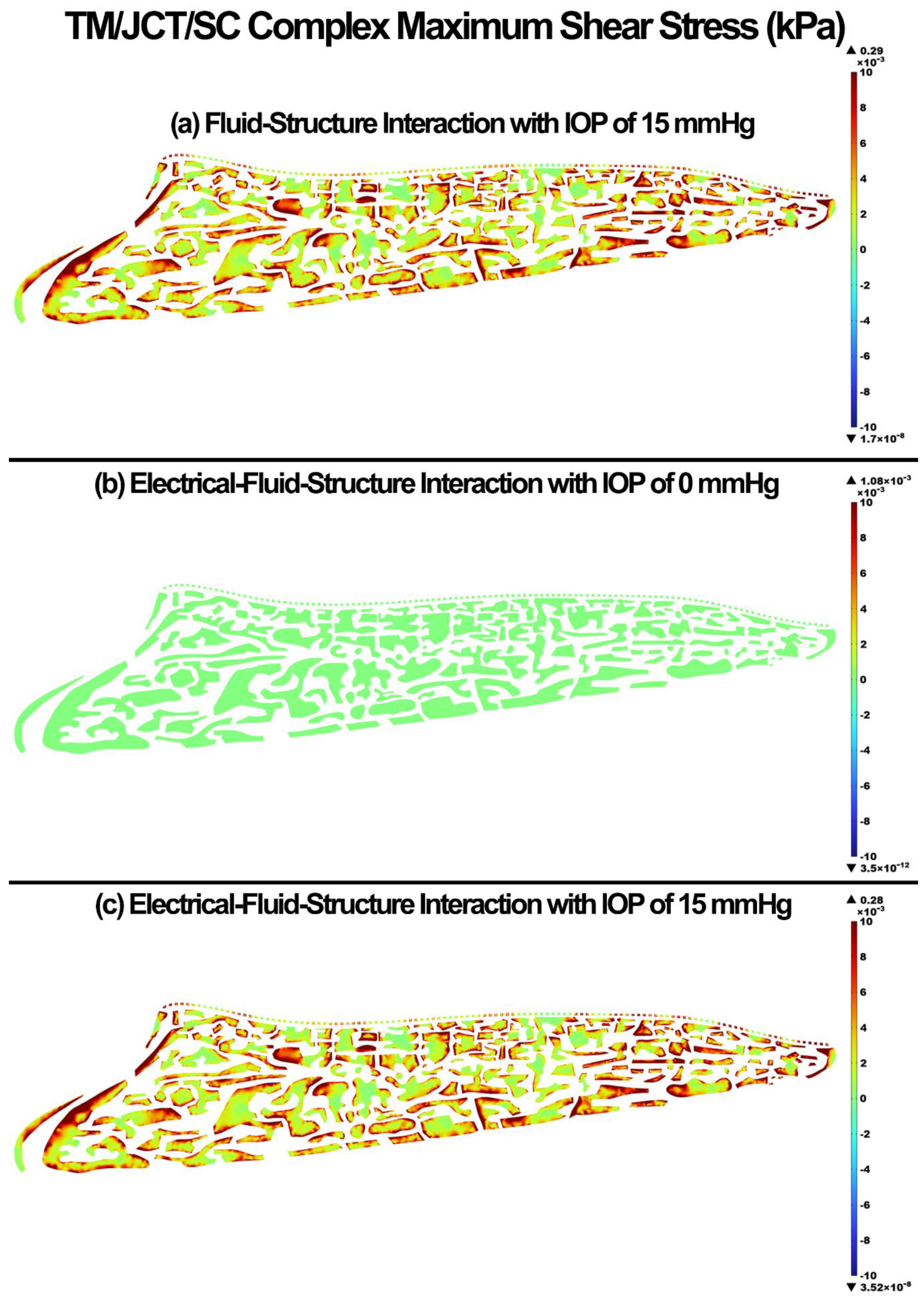
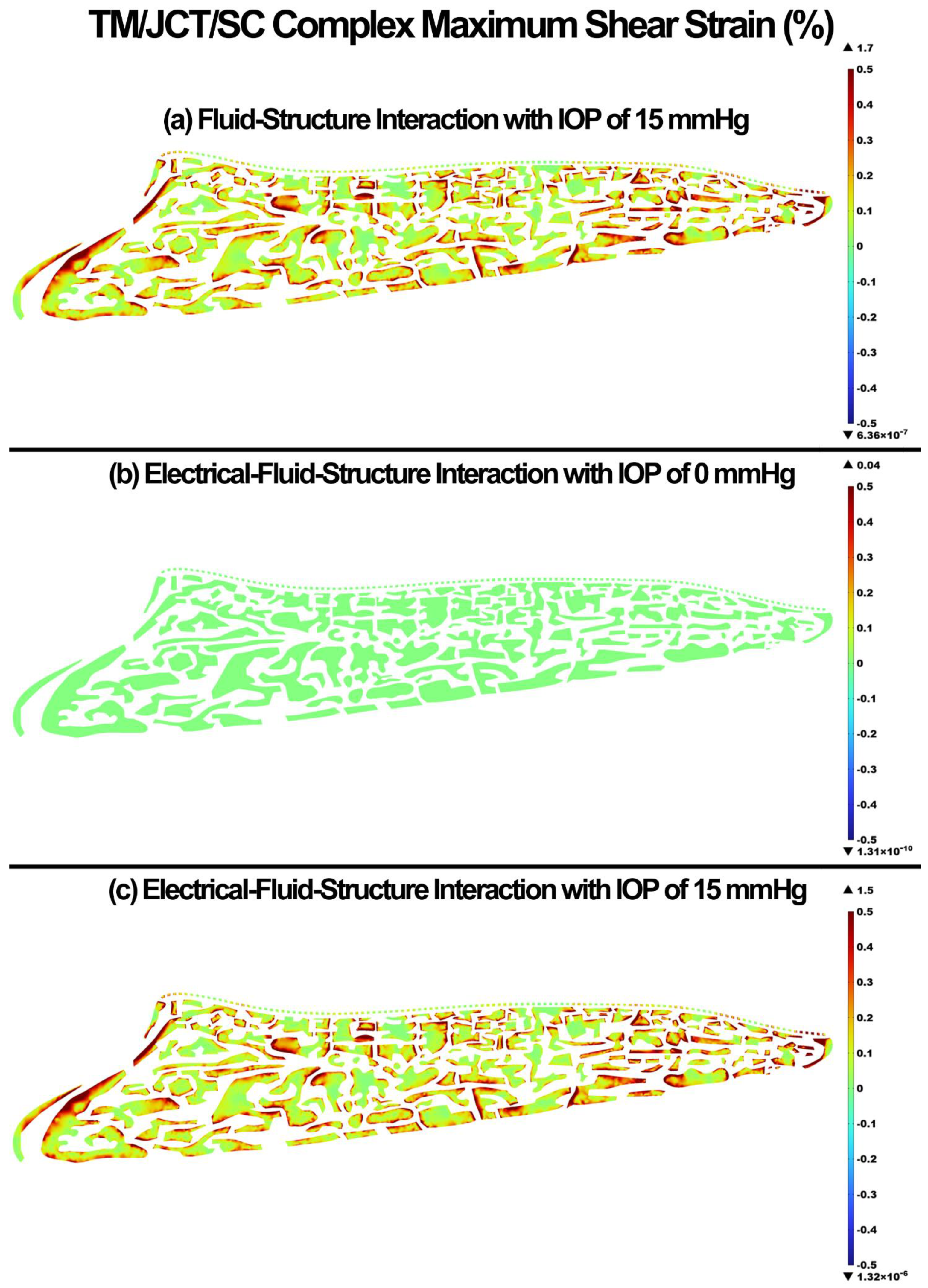
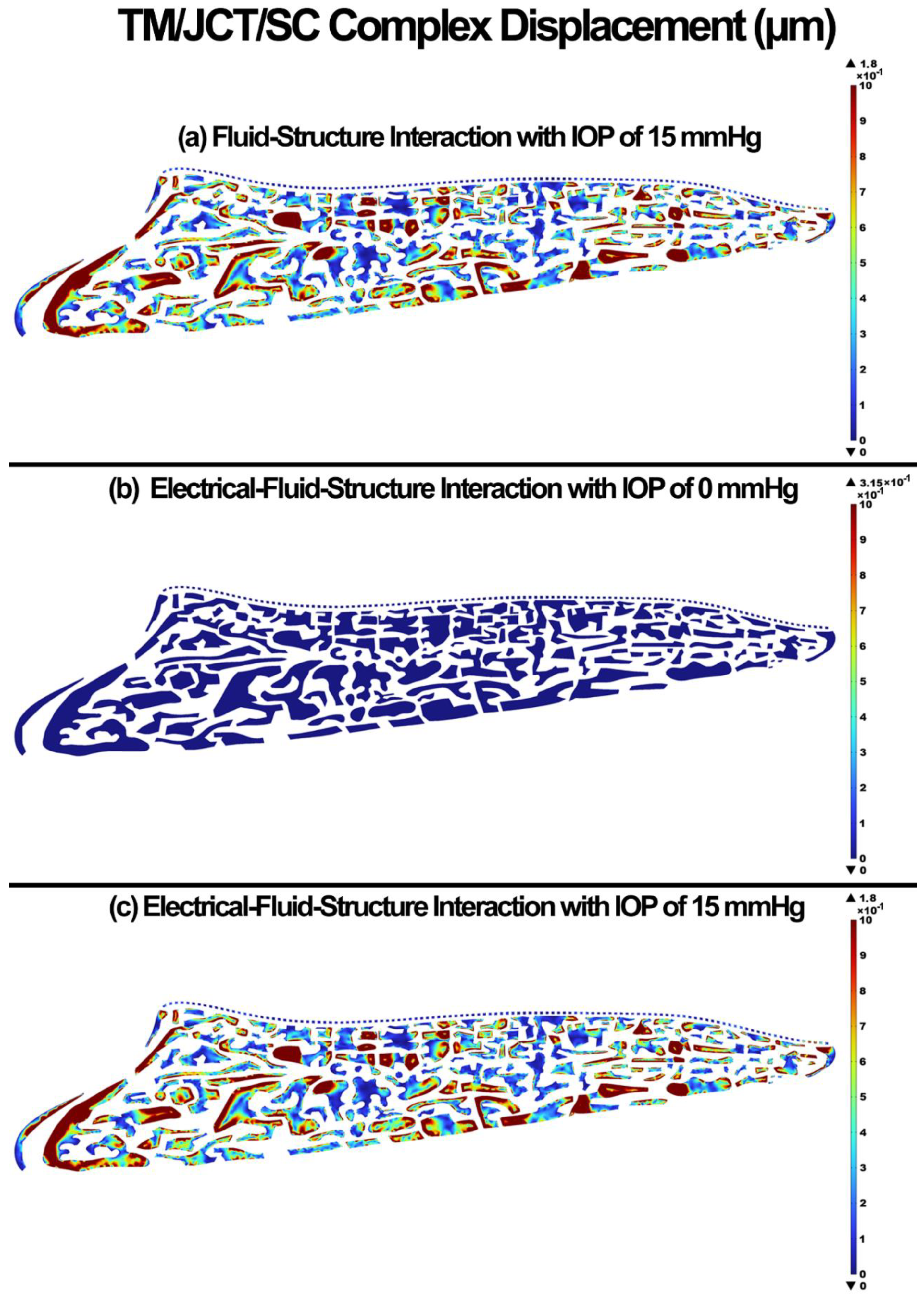
- The glycocalyx plays a minor role in the biomechanics and hydrodynamics of the outflow pathway.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ellingsen, B.A.; Grant, W.M. The relationship of pressure and aqueous outflow in enucleated human eyes. Investig. Ophthalmol. 1971, 10, 430–437. [Google Scholar]
- Moses, R.A. The effect of intraocular pressure on resistance to outflow. Surv. Ophthalmol. 1977, 22, 88–100. [Google Scholar] [CrossRef]
- Johnson, M.C.; Kamm, R.D. The role of Schlemm’s canal in aqueous outflow from the human eye. Investig. Ophthalmol. Vis. Sci. 1983, 24, 320–325. [Google Scholar]
- Johnson, D.H.; Johnson, M. How does nonpenetrating glaucoma surgery work? Aqueous outflow resistance and glaucoma surgery. J. Glaucoma 2001, 10, 55–67. [Google Scholar] [CrossRef] [PubMed]
- Kitazawa, Y.; Horie, T. Diurnal variation of intraocular pressure in primary open-angle glaucoma. Am. J. Ophthalmol. 1975, 79, 557–566. [Google Scholar] [CrossRef] [PubMed]
- Sommer, A.; Tielsch, J.M.; Katz, J.; Quigley, H.A.; Gottsch, J.D.; Javitt, J.; Singh, K. Relationship between intraocular pressure and primary open angle glaucoma among white and black Americans. The Baltimore Eye Survey. Arch. Ophthalmol. 1991, 109, 1090–1095. [Google Scholar] [CrossRef] [PubMed]
- Fautsch, M.P.; Johnson, D.H.; Second ARVO/Pfizer Research Institute Working Group. Aqueous humor outflow: What do we know? Where will it lead us? Investig. Ophthalmol. Vis. Sci. 2006, 47, 4181–4187. [Google Scholar] [CrossRef] [Green Version]
- Kwon, Y.H.; Fingert, J.H.; Kuehn, M.H.; Alward, W.L. Primary open-angle glaucoma. N. Engl. J. Med. 2009, 360, 1113–1124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stamer, W.D.; Acott, T.S. Current understanding of conventional outflow dysfunction in glaucoma. Curr. Opin. Ophthalmol. 2012, 23, 135–143. [Google Scholar] [CrossRef] [Green Version]
- Tamm, E. Glaucoma opinion: A unifying concept for trabecular meshwork pathology in primary open angle glaucoma. Int. Glaucoma Rev. 2013, 15, 45–47. [Google Scholar]
- Goel, M.; Picciani, R.G.; Lee, R.K.; Bhattacharya, S.K. Aqueous humor dynamics: A review. Open Ophthalmol. J. 2010, 4, 52–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carreon, T.; van der Merwe, E.; Fellman, R.L.; Johnstone, M.; Bhattacharya, S.K. Aqueous outflow—A continuum from trabecular meshwork to episcleral veins. Prog. Retin. Eye Res. 2017, 57, 108–133. [Google Scholar] [CrossRef] [PubMed]
- Dvorak-Theobald, G.; Kirk, H.Q. Aqueous pathways in some cases of glaucoma. Trans. Am. Ophthalmol. Soc. 1955, 53, 301. [Google Scholar] [PubMed]
- Johnstone, M.A. The aqueous outflow system as a mechanical pump: Evidence from examination of tissue and aqueous movement in human and non-human primates. J. Glaucoma 2004, 13, 421–438. [Google Scholar] [CrossRef] [PubMed]
- Johnstone, M.; Jamil, A.; Martin, E. Aqueous veins and open angle glaucoma. In The Glaucoma Book; Springer: Berlin/Heidelberg, Germany, 2010; pp. 65–78. [Google Scholar]
- Johnstone, M.A. Intraocular pressure regulation: Findings of pulse-dependent trabecular meshwork motion lead to unifying concepts of intraocular pressure homeostasis. J. Ocul. Pharmacol. Ther. 2014, 30, 88–93. [Google Scholar] [CrossRef]
- Johnstone, M.; Xin, C.; Tan, J.; Martin, E.; Wen, J.; Wang, R.K. Aqueous outflow regulation—21st century concepts. Prog. Retin. Eye Res. 2020, 83, 100917. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.Y.; Huynh, T.; Johnson, M.; Gong, H. Endothelial glycocalyx layer in the aqueous outflow pathway of bovine and human eyes. Exp. Eye Res. 2014, 128, 27–33. [Google Scholar] [CrossRef] [Green Version]
- Sosnowik, S.; Swain, D.L.; Liu, N.; Fan, S.; Toris, C.B.; Gong, H. Endothelial Glycocalyx Morphology in Different Flow Regions of the Aqueous Outflow Pathway of Normal and Laser-Induced Glaucoma Monkey Eyes. Cells 2022, 11, 2452. [Google Scholar] [CrossRef]
- Ethier, C.R.; Read, A.T.; Chan, D. Biomechanics of Schlemm’s canal endothelial cells: Influence on F-actin architecture. Biophys. J. 2004, 87, 2828–2837. [Google Scholar] [CrossRef] [Green Version]
- McDonnell, F.; Dismuke, W.M.; Overby, D.R.; Stamer, W.D. Pharmacological regulation of outflow resistance distal to Schlemm’s canal. Am. J. Physiol. Cell Physiol. 2018, 315, C44–C51. [Google Scholar] [CrossRef]
- Stamer, W.D.; Lei, Y.; Boussommier-Calleja, A.; Overby, D.R.; Ethier, C.R. eNOS, a pressure-dependent regulator of intraocular pressure. Investig. Ophthalmol. Vis. Sci. 2011, 52, 9438–9444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pries, A.R.; Secomb, T.W.; Gaehtgens, P. The endothelial surface layer. Pflug. Arch. 2000, 440, 653–666. [Google Scholar] [CrossRef] [PubMed]
- Weinbaum, S.; Tarbell, J.M.; Damiano, E.R. The structure and function of the endothelial glycocalyx layer. Annu. Rev. Biomed. Eng. 2007, 9, 121–167. [Google Scholar] [CrossRef]
- Collins, S.R.; Blank, R.S.; Deatherage, L.S.; Dull, R.O. Special article: The endothelial glycocalyx: Emerging concepts in pulmonary edema and acute lung injury. Anesth. Analg. 2013, 117, 664–674. [Google Scholar] [CrossRef] [Green Version]
- Vincent, P.E.; Weinberg, P.D. Flow-dependent concentration polarization and the endothelial glycocalyx layer: Multi-scale aspects of arterial mass transport and their implications for atherosclerosis. Biomech. Model. Mechanobiol. 2014, 13, 313–326. [Google Scholar] [CrossRef] [PubMed]
- Dewey, C., Jr. Effects of fluid flow on living vascular cells. J. Biomech. Eng. 1984, 106, 31–35. [Google Scholar] [CrossRef]
- Yao, Y.; Rabodzey, A.; Dewey, C.F., Jr. Glycocalyx modulates the motility and proliferative response of vascular endothelium to fluid shear stress. Am. J. Physiol. Heart Circ. Physiol. 2007, 293, H1023–H1030. [Google Scholar] [CrossRef]
- Tarbell, J.M.; Weinbaum, S.; Kamm, R.D. Cellular fluid mechanics and mechanotransduction. Ann. Biomed. Eng. 2005, 33, 1719–1723. [Google Scholar] [CrossRef]
- Florian, J.A.; Kosky, J.R.; Ainslie, K.; Pang, Z.; Dull, R.O.; Tarbell, J.M. Heparan sulfate proteoglycan is a mechanosensor on endothelial cells. Circ. Res. 2003, 93, e136–e142. [Google Scholar] [CrossRef] [Green Version]
- Mochizuki, S.; Vink, H.; Hiramatsu, O.; Kajita, T.; Shigeto, F.; Spaan, J.A.; Kajiya, F. Role of hyaluronic acid glycosaminoglycans in shear-induced endothelium-derived nitric oxide release. Am. J. Physiol. Heart Circ. Physiol. 2003, 285, H722–H726. [Google Scholar] [CrossRef] [Green Version]
- Zeng, L.; He, X.; Wang, Y.; Tang, Y.; Zheng, C.; Cai, H.; Liu, J.; Wang, Y.; Fu, Y.; Yang, G.Y. MicroRNA-210 overexpression induces angiogenesis and neurogenesis in the normal adult mouse brain. Gene Ther. 2014, 21, 37–43. [Google Scholar] [CrossRef]
- Madekurozwa, M.; Stamer, W.D.; Reina-Torres, E.; Sherwood, J.M.; Overby, D.R. The ocular pulse decreases aqueous humor outflow resistance by stimulating nitric oxide production. Am. J. Physiol. Cell Physiol. 2021, 320, C652–C665. [Google Scholar] [CrossRef]
- McDonnell, F.; Perkumas, K.M.; Ashpole, N.E.; Kalnitsky, J.; Sherwood, J.M.; Overby, D.R.; Stamer, W.D. Shear Stress in Schlemm’s Canal as a Sensor of Intraocular Pressure. Sci. Rep. 2020, 10, 5804. [Google Scholar] [CrossRef] [PubMed]
- Reina-Torres, E.; De Ieso, M.L.; Pasquale, L.R.; Madekurozwa, M.; van Batenburg-Sherwood, J.; Overby, D.R.; Stamer, W.D. The vital role for nitric oxide in intraocular pressure homeostasis. Prog. Retin. Eye Res. 2021, 83, 100922. [Google Scholar] [CrossRef] [PubMed]
- Schouten, M.; Wiersinga, W.J.; Levi, M.; van der Poll, T. Inflammation, endothelium, and coagulation in sepsis. J. Leukoc. Biol. 2008, 83, 536–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zharikov, S.I.; Sigova, A.A.; Chen, S.; Bubb, M.R.; Block, E.R. Cytoskeletal regulation of the L-arginine/NO pathway in pulmonary artery endothelial cells. Am. J. Physiol. Lung Cell. Mol. Physiol. 2001, 280, L465–L473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vranka, J.A.; Acott, T.S. Pressure-induced expression changes in segmental flow regions of the human trabecular meshwork. Exp. Eye Res. 2017, 158, 67–72. [Google Scholar] [CrossRef]
- Vranka, J.A.; Bradley, J.M.; Yang, Y.F.; Keller, K.E.; Acott, T.S. Mapping molecular differences and extracellular matrix gene expression in segmental outflow pathways of the human ocular trabecular meshwork. PLoS ONE 2015, 10, e0122483. [Google Scholar] [CrossRef] [Green Version]
- Keller, K.E.; Bradley, J.M.; Vranka, J.A.; Acott, T.S. Segmental versican expression in the trabecular meshwork and involvement in outflow facility. Investig. Ophthalmol. Vis. Sci. 2011, 52, 5049–5057. [Google Scholar] [CrossRef] [Green Version]
- Yang, C.Y.; Liu, Y.; Lu, Z.; Ren, R.; Gong, H. Effects of Y27632 on aqueous humor outflow facility with changes in hydrodynamic pattern and morphology in human eyes. Investig. Ophthalmol. Vis. Sci. 2013, 54, 5859–5870. [Google Scholar] [CrossRef]
- Van den Berg, B.M.; Spaan, J.A.; Vink, H. Impaired glycocalyx barrier properties contribute to enhanced intimal low-density lipoprotein accumulation at the carotid artery bifurcation in mice. Pflug. Arch. 2009, 457, 1199–1206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van den Berg, B.M.; Vink, H.; Spaan, J.A. The endothelial glycocalyx protects against myocardial edema. Circ. Res. 2003, 92, 592–594. [Google Scholar] [CrossRef] [Green Version]
- Brindley, G.S. A New Interaction of Light and Electricity in Stimulating the Human Retina. J. Physiol. 1964, 171, 514–520. [Google Scholar] [CrossRef]
- Kouwenhoven, W.B. Effects of electricity on the human body. Ind. Med. Surg. 1949, 18, 269. [Google Scholar] [CrossRef] [PubMed]
- Karimi, A.; Rahmati, S.M.; Razaghi, R.; Crawford Downs, J.; Acott, T.S.; Wang, R.K.; Johnstone, M. Biomechanics of human trabecular meshwork in healthy and glaucoma eyes via dynamic Schlemm’s canal pressurization. Comput. Methods Programs Biomed. 2022, 221, 106921. [Google Scholar] [CrossRef] [PubMed]
- Karimi, A.; Razaghi, R.; Padilla, S.; Rahmati, S.M.; Crawford Downs, J.; Acott, T.S.; Kelley, M.J.; Wang, R.K.; Johnstone, M. Viscoelastic Biomechanical Properties of the Conventional Aqueous Outflow Pathway Tissues in Healthy and Glaucoma Human Eyes. J. Clin. Med. 2022, 11, 6049. [Google Scholar] [CrossRef]
- Karimi, A.; Rahmati, S.M.; Razaghi, R.; Girkin, C.A.; Crawford Downs, J. Finite element modeling of the complex anisotropic mechanical behavior of the human sclera and pia mater. Comput. Methods Programs Biomed. 2022, 215, 106618. [Google Scholar] [CrossRef] [PubMed]
- Karimi, A.; Razaghi, R.; Rahmati, S.M.; Downs, J.C.; Acott, T.S.; Wang, R.K.; Johnstone, M. Modeling the biomechanics of the conventional aqueous outflow pathway microstructure in the human eye. Comput. Methods Programs Biomed. 2022, 221, 106922. [Google Scholar] [CrossRef] [PubMed]
- Karimi, A.; Razaghi, R.; Rahmati, S.M.; Downs, J.C.; Acott, T.S.; Kelley, M.J.; Wang, R.K.; Johnstone, M. The Effect of Intraocular Pressure Load Boundary on the Bio-mechanics of the Human Conventional Aqueous Outflow Pathway. Bioengineering 2022, 9, 672. [Google Scholar] [CrossRef] [PubMed]
- Khosravi, A.; Shirazi, H.A.; Asnafi, A.; Karimi, A. A fully analytical approach to investigate the electro-viscous effect of the endothelial glycocalyx layer on the microvascular blood flow. Clin. Chim. Acta 2017, 472, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Girkin, C.A.; Fazio, M.A.; Yang, H.; Reynaud, J.; Burgoyne, C.F.; Smith, B.; Wang, L.; Downs, J.C. Variation in the three-dimensional histomorphometry of the normal human optic nerve head with age and race: Lamina cribrosa and peripapillary scleral thickness and position. Investig. Ophthalmol. Vis. Sci. 2017, 58, 3759–3769. [Google Scholar] [CrossRef]
- Karimi, A.; Razaghi, R.; Rahmati, S.M.; Girkin, C.A.; Downs, J.C. Relative Contributions of Intraocular and Cerebrospinal Fluid Pressures to the Biomechanics of the Lamina Cribrosa and Laminar Neural Tissues. Investig. Ophthalmol. Vis. Sci. 2022, 63, 14. [Google Scholar] [CrossRef]
- Karimi, A.; Rahmati, S.M.; Grytz, R.G.; Girkin, C.A.; Downs, J.C. Modeling the biomechanics of the lamina cribrosa microstructure in the human eye. Acta Biomater. 2021, 134, 357–378. [Google Scholar] [CrossRef]
- Ten Hulzen, R.D.; Johnson, D.H. Effect of fixation pressure on juxtacanalicular tissue and Schlemm’s canal. Investig. Ophthalmol. Vis. Sci. 1996, 37, 114–124. [Google Scholar]
- Johnson, M.; Chan, D.; Read, A.T.; Christensen, C.; Sit, A.; Ethier, C.R. The pore density in the inner wall endothelium of Schlemm’s canal of glaucomatous eyes. Investig. Ophthalmol. Vis. Sci. 2002, 43, 2950–2955. [Google Scholar]
- Overby, D.; Gong, H.; Qiu, G.; Freddo, T.F.; Johnson, M. The mechanism of increasing outflow facility during washout in the bovine eye. Investig. Ophthalmol. Vis. Sci. 2002, 43, 3455–3464. [Google Scholar]
- Ethier, C.R.; Coloma, F.M.; Sit, A.J.; Johnson, M. Two pore types in the inner-wall endothelium of Schlemm’s canal. Investig. Ophthalmol. Vis. Sci. 1998, 39, 2041–2048. [Google Scholar]
- Karimi, A.; Grytz, R.; Rahmati, S.M.; Girkin, C.A.; Downs, J.C. Analysis of the effects of finite element type within a 3D biomechanical model of a human optic nerve head and posterior pole. Comput. Methods Programs Biomed. 2021, 198, 105794. [Google Scholar] [CrossRef] [PubMed]
- Karimi, A.; Razaghi, R.; Girkin, C.A.; Downs, J.C. Ocular biomechanics due to ground blast reinforcement. Comput. Methods Programs Biomed. 2021, 211, 106425. [Google Scholar] [CrossRef]
- Karimi, A.; Rahmati, S.M.; Razaghi, R.; Downs, J.C.; Wang, R.K.; Johnstone, M.A. Biomechanics of Human Trabecular Meshwork in Healthy and Glaucoma Eyes via Dynamic Schlemm’s Canal Pressurization. Investig. Ophthalmol. Vis. Sci. 2022, 63, 2728. [Google Scholar]
- Karimi, A.; Razaghi, R.; Girkin, C.A.; Downs, J.C. Ocular biomechanics during improvised explosive device blast: A computational study using eye-specific models. Injury 2022, 53, 1401–1415. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Read, A.T.; Sulchek, T.; Ethier, C.R. Trabecular meshwork stiffness in glaucoma. Exp. Eye Res. 2017, 158, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Vahabikashi, A.; Gelman, A.; Dong, B.; Gong, L.; Cha, E.D.K.; Schimmel, M.; Tamm, E.R.; Perkumas, K.; Stamer, W.D.; Sun, C.; et al. Increased stiffness and flow resistance of the inner wall of Schlemm’s canal in glaucomatous human eyes. Proc. Natl. Acad. Sci. USA 2019, 116, 26555–26563. [Google Scholar] [CrossRef] [PubMed]
- Zhao, G.; Joca, H.C.; Nelson, M.T.; Lederer, W.J. ATP- and voltage-dependent electro-metabolic signaling regulates blood flow in heart. Proc. Natl. Acad. Sci. USA 2020, 117, 7461–7470. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Bai, H.; Wang, E.; Forrester, J.V.; McCaig, C.D. Electrical stimulation directly induces pre-angiogenic responses in vascular endothelial cells by signaling through VEGF receptors. J. Cell Sci. 2004, 117, 397–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lepple-Wienhues, A.; Stahl, F.; Wiederholt, M. Differential smooth muscle-like contractile properties of trabecular meshwork and ciliary muscle. Exp. Eye Res. 1991, 53, 33–38. [Google Scholar] [CrossRef]
- Halabian, M.; Beigzadeh, B.; Siavashi, M. A numerical study on the effect of osmotic pressure on stress and strain in intercellular structures of tumor tissue in the poro-elastic model. Meccanica 2021, 56, 2471–2486. [Google Scholar] [CrossRef]
- Mansouri, A.; Vali, A.; Kostiuk, L.W. Electrokinetic power generation of non-Newtonian fluids in a finite length microchannel. Microfluid. Nanofluid. 2016, 20, 71. [Google Scholar] [CrossRef]
- Razaghi, R.; Biglari, H.; Karimi, A. Risk of rupture of the cerebral aneurysm in relation to traumatic brain injury using a patient-specific fluid-structure interaction model. Comput. Methods Programs Biomed. 2019, 176, 9–16. [Google Scholar] [CrossRef]
- Vass, C.; Hirn, C.; Unger, E.; Mayr, W.; Georgopoulos, M.; Rainer, G.; Richter-Maksch, S. Human aqueous humor viscosity in cataract, primary open angle glaucoma and pseudoexfoliation syndrome. Investig. Ophthalmol. Vis. Sci. 2004, 45, 5030. [Google Scholar]
- Kalam, M.A.; Alshamsan, A.; Aljuffali, I.A.; Mishra, A.K.; Sultana, Y. Delivery of gatifloxacin using microemulsion as vehicle: Formulation, evaluation, transcorneal permeation and aqueous humor drug determination. Drug Deliv. 2016, 23, 896–907. [Google Scholar] [CrossRef] [PubMed]
- Oksala, A.; Lehtinen, A. Comparative studies on the electrical conductivity of aqueous humour, vitreous body, cornea and sclera. Acta Ophthalmol. 1959, 37, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Mandel, Y.; Laufer, S.; Rubinsky, B. Measurement of corneal endothelial impedance with non-invasive external electrodes—A theoretical study. Med. Eng. Phys. 2012, 34, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Coleman, D.J.; Trokel, S. Direct-recorded intraocular pressure variations in a human subject. Arch. Ophthalmol. 1969, 82, 637–640. [Google Scholar] [CrossRef]
- Turner, D.C.; Edmiston, A.M.; Zohner, Y.E.; Byrne, K.J.; Seigfreid, W.P.; Girkin, C.A.; Morris, J.S.; Downs, J.C. Transient Intraocular Pressure Fluctuations: Source, Magnitude, Frequency, and Associated Mechanical Energy. Investig. Ophthalmol. Vis. Sci. 2019, 60, 2572–2582. [Google Scholar] [CrossRef] [Green Version]
- Gasiorowski, J.Z.; Russell, P. Biological properties of trabecular meshwork cells. Exp. Eye Res. 2009, 88, 671–675. [Google Scholar] [CrossRef] [Green Version]
- Sienkiewicz, A.E.; Rosenberg, B.N.; Edwards, G.; Carreon, T.A.; Bhattacharya, S.K. Aberrant glycosylation in the human trabecular meshwork. Proteom. Clin. Appl. 2014, 8, 130–142. [Google Scholar] [CrossRef] [Green Version]
- Arisaka, T.; Mitsumata, M.; Kawasumi, M.; Tohjima, T.; Hirose, S.; Yoshida, Y. Effects of shear stress on glycosaminoglycan synthesis in vascular endothelial cells. Ann. N. Y. Acad. Sci. 1995, 748, 543–554. [Google Scholar] [CrossRef]
- Gouverneur, M.; Berg, B.; Nieuwdorp, M.; Stroes, E.; Vink, H. Vasculoprotective properties of the endothelial glycocalyx: Effects of fluid shear stress. J. Intern. Med. 2006, 259, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Reitsma, S.; Slaaf, D.W.; Vink, H.; van Zandvoort, M.A.; oude Egbrink, M.G. The endothelial glycocalyx: Composition, functions, and visualization. Pflug. Arch. 2007, 454, 345–359. [Google Scholar] [CrossRef] [Green Version]
- Tarbell, J.M. Shear stress and the endothelial transport barrier. Cardiovasc. Res. 2010, 87, 320–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarbell, J.M.; Ebong, E.E. The endothelial glycocalyx: A mechano-sensor and -transducer. Sci. Signal. 2008, 1, pt8. [Google Scholar] [CrossRef] [PubMed]
- Pries, A.R.; Secomb, T.W. Microvascular blood viscosity in vivo and the endothelial surface layer. Am. J. Physiol. Heart Circ. Physiol. 2005, 289, H2657–H2664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pries, A.R.; Secomb, T.W. Blood flow in microvascular networks. In Microcirculation; Elsevier: Amsterdam, The Netherlands, 2008; pp. 3–36. [Google Scholar]
- Pries, A.R.; Secomb, T.W.; Jacobs, H.; Sperandio, M.; Osterloh, K.; Gaehtgens, P. Microvascular blood flow resistance: Role of endothelial surface layer. Am. J. Physiol. 1997, 273, H2272–H2279. [Google Scholar] [CrossRef]
- Kapellos, G.E.; Alexiou, T.S. Modeling Momentum and Mass Transport in Cellular Biological Media: From the Molecular to the Tissue Scale. In Transport in Biological Media; Becker, S.M., Kuznetsov, A.V., Eds.; Elsevier: Boston, MA, USA, 2013; pp. 1–40. [Google Scholar]
- Raviola, G.; Raviola, E. Paracellular route of aqueous outflow in the trabecular meshwork and canal of Schlemm. A freeze-fracture study of the endothelial junctions in the sclerocorneal angel of the macaque monkey eye. Investig. Ophthalmol. Vis. Sci. 1981, 21, 52–72. [Google Scholar]
- Koefoed-Johnsen, V.; Ussing, H.H. The nature of the frog skin potential. Acta Physiol. Scand. 1958, 42, 298–308. [Google Scholar] [CrossRef]
- Curry, F.E.; Michel, C.C. A fiber matrix model of capillary permeability. Microvasc. Res. 1980, 20, 96–99. [Google Scholar] [CrossRef]
- Dewey, C. Orientation of endothelial cells in shear fields in vitro. Clin. Hemorheol. 1983, 3, 224. [Google Scholar]
- Remuzzi, A.; Dewey, C.F., Jr.; Davies, P.F.; Gimbrone, M.A., Jr. Orientation of endothelial cells in shear fields in vitro. Biorheology 1984, 21, 617–630. [Google Scholar] [CrossRef]
- Liu, M.; Yang, J. Electrokinetic effect of the endothelial glycocalyx layer on two-phase blood flow in small blood vessels. Microvasc. Res. 2009, 78, 14–19. [Google Scholar] [CrossRef]
- Hall, J.E.; Hall, M.E. Guyton and Hall Textbook of Medical Physiology e-Book; Elsevier Health Sciences: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Johnstone, M.A. Aqueous humor outflow system overview. In Becker-Shaffer’s Diagnosis and Therapy of the Glaucomas; Stamper, R.L., Lieberman, M.F., Drake, M.V., Eds.; Mosby: Edinburgh, UK, 2009; pp. 25–46. [Google Scholar]
- Li, P.; Reif, R.; Zhi, Z.; Martin, E.; Shen, T.T.; Johnstone, M.; Wang, R.K. Phase-sensitive optical coherence tomography characterization of pulse-induced trabecular meshwork displacement in ex vivo nonhuman primate eyes. J. Biomed. Opt. 2012, 17, 076026. [Google Scholar] [CrossRef]
- Grant, W.M. Experimental aqueous perfusion in enucleated human eyes. Arch. Ophthalmol. 1963, 69, 783–801. [Google Scholar] [CrossRef]
- Rosenquist, R.; Epstein, D.; Melamed, S.; Johnson, M.; Grant, W.M. Outflow resistance of enucleated human eyes at two different perfusion pressures and different extents of trabeculotomy. Curr. Eye Res. 1989, 8, 1233–1240. [Google Scholar] [CrossRef]
- Maepea, O.; Bill, A. Pressures in the juxtacanalicular tissue and Schlemm’s canal in monkeys. Exp. Eye Res. 1992, 54, 879–883. [Google Scholar] [CrossRef] [PubMed]
- Schuman, J.S.; Chang, W.; Wang, N.; de Kater, A.W.; Allingham, R.R. Excimer laser effects on outflow facility and outflow pathway morphology. Investig. Ophthalmol. Vis. Sci. 1999, 40, 1676–1680. [Google Scholar]
- Overby, D.R.; Stamer, W.D.; Johnson, M. The changing paradigm of outflow resistance generation: Towards synergistic models of the JCT and inner wall endothelium. Exp. Eye Res. 2009, 88, 656–670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vranka, J.A.; Staverosky, J.A.; Reddy, A.P.; Wilmarth, P.A.; David, L.L.; Acott, T.S.; Russell, P.; Raghunathan, V.K. Biomechanical Rigidity and Quantitative Proteomics Analysis of Segmental Regions of the Trabecular Meshwork at Physiologic and Elevated Pressures. Investig. Ophthalmol. Vis. Sci. 2018, 59, 246–259. [Google Scholar] [CrossRef]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karimi, A.; Halabian, M.; Razaghi, R.; Downs, J.C.; Kelley, M.J.; Acott, T.S. Modeling the Endothelial Glycocalyx Layer in the Human Conventional Aqueous Outflow Pathway. Cells 2022, 11, 3925. https://doi.org/10.3390/cells11233925
Karimi A, Halabian M, Razaghi R, Downs JC, Kelley MJ, Acott TS. Modeling the Endothelial Glycocalyx Layer in the Human Conventional Aqueous Outflow Pathway. Cells. 2022; 11(23):3925. https://doi.org/10.3390/cells11233925
Chicago/Turabian StyleKarimi, Alireza, Mahdi Halabian, Reza Razaghi, J. Crawford Downs, Mary J. Kelley, and Ted S. Acott. 2022. "Modeling the Endothelial Glycocalyx Layer in the Human Conventional Aqueous Outflow Pathway" Cells 11, no. 23: 3925. https://doi.org/10.3390/cells11233925